Back to Journals » Journal of Asthma and Allergy » Volume 18
Severe Asthma and Sleep Disorders: A Severe Asthma Network Italy (SANI) Registry Analysis
Authors Ferri S ![]() , Marzio V, Cavaglià E, Valli N
, Marzio V, Cavaglià E, Valli N ![]() , Bagnardi V, Oriecuia C, Sala I, Cardini C, Sirena C, Paoletti G
, Bagnardi V, Oriecuia C, Sala I, Cardini C, Sirena C, Paoletti G ![]() , Blasi F
, Blasi F ![]() , Paggiaro P, Canonica GW
, Paggiaro P, Canonica GW ![]() , Heffler E
, Heffler E
Received 5 August 2025
Accepted for publication 30 October 2025
Published 1 December 2025 Volume 2025:18 Pages 1661—1673
DOI https://doi.org/10.2147/JAA.S558611
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Sebastian Ferri,1 Valentina Marzio,1 Edoardo Cavaglià,1 Nicolò Valli,1 Vincenzo Bagnardi,2 Chiara Oriecuia,3,4 Isabella Sala,2,5 Cristina Cardini,6 Concetta Sirena,6 Giovanni Paoletti,1,7 Francesco Blasi,8,9 Pierluigi Paggiaro,10 Giorgio Walter Canonica,1,7 Enrico Heffler,1,7 On behalf of the SANI study group
1Personalized Medicine Asthma and Allergy, IRCCS Humanitas Research Hospital, Rozzano, Italy; 2Department of Statistics and Quantitative Methods, University of Milano-Bicocca, Milan, Italy; 3Department of Clinical and Experimental Sciences, University of Brescia, Brescia, Italy; 4Department of Molecular and Translational Medicine, University of Brescia, Brescia, Italy; 5Department of Medicine and Surgery, University of Milano-Bicocca, Milan, Italy; 6Severe Asthma Network in Italy (SANI), Milan, Italy; 7Department of Biomedical Sciences, Humanitas University, Pieve Emanuele, Italy; 8Department of Pathophysiology and Transplantation, Università degli Studi di Milano, Milan, Italy; 9Internal Medicine Department, Respiratory Unit and Cystic Fibrosis Center, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico di Milano, Milan, Italy; 10Department of Surgery, Medicine, Molecular Biology and Critical Care, University of Pisa, Pisa, Italy
Correspondence: Enrico Heffler, Centro di Medicina Personalizzata, Asma e Allergologia, IRCCS Humanitas Research Center, Via Alessandro Manzoni 56, Rozzano (MI), 20089, Italy, Tel +39 0282247054, Email [email protected]
Purpose: This study aims to evaluate the link between sleep disorders and patients with severe asthma enrolled in the Severe Asthma Network Italy (SANI) registry. We investigated the prevalence and the overall disease burden sleep disorders in severe asthmatics, identifying their clinical features, risks factors and treatable traits.
Patients and Methods: We performed a retrospective analysis using data from the SANI registry, stratifying patients based on the presence or absence of sleep disorders at their baseline visit, to gather their clinical, functional, and demographic information.
Results: About 26.1% of severe asthmatics have concomitant sleep disorders, especially overweight patients. Severe asthmatic patients with sleep disorders have significantly more frequent rhinitis, chronic rhinosinusitis with (CRSwNP and without nasal polyps (CRSsNP), gastroesophageal reflux disease (GERD), cardiovascular disease (CVD) and type II diabetes. These patients more frequently use intranasal corticosteroids and show higher exacerbation rate needing systemic corticosteroids. They show less severe lung function impairment but worse asthma control and quality of life, increased asthma-related hospital admission and number of unscheduled medical visits. Multivariate analysis shows that overweight, moderate-to-severe rhinitis, CRSwNP, CRSsNP, GERD and CVD are independent risk factors for sleep disorders.
Conclusion: Sleep disorders are a common and relevant feature among patients with severe asthma. The two diseases influence each other worsening the severity of symptoms, quality of life and overall healthcare burden. These data suggest that, treating comorbidities, including sleep disorders, might result in a better management of asthma and so a better health outcome.
Keywords: comorbidities, real world evidence, registry, severe asthma, sleep disorders
Introduction
Asthma is a chronic inflammatory disease of the airways that affects up to 18% of people worldwide,1 characterized by dyspnea, wheezing, coughing, chest stiffness, variable airflow obstruction, bronchial hyperresponsiveness and recurrent exacerbations. According to Global Initiative for Asthma (GINA), severe asthma is defined as uncontrolled disease despite adherence with maximal optimized high dose of inhaled corticosteroids (ICS) plus long-acting beta2-agonists (LABA) treatment and management of contributing or worsening factors, or that worsen when high dose treatment is decreased.2 Currently, epidemiologic data on severe asthma are still limited. According to the European Network For Understanding Mechanisms Of Severe Asthma (ENFUMOSA), about 10% of the asthmatic population develops severe asthma.2 A poor asthma control leads to hospitalization, disability, and higher risk of death.3 Over the past ten years, it has been increasingly recognized that asthma can be linked with various disorders that influence the unique symptomatic experience of each patient and may lead to a condition that is challenging to manage.3 Patients with poorly controlled asthma frequently need long-term oral corticosteroids (LTOCS) resulting in potential oral corticosteroids (OCS)-related comorbidities (sleep apnea, hypertension, dyslipidemia, and adrenal insufficiency),3 moreover, they usually suffer from gastroesophageal reflux disease (GERD),4 chronic rhinitis and rhinosinusitis (with or without polyps),5,6 dysfunctional breathing, and obesity,7 among others. The combination between cough and/or asthma, obstructive sleep apnea (OSA), rhinosinusitis, and esophageal reflux generates a syndrome known as CORE (Cough/asthma, Obesity/OSA, Rhinosinusitis, and Esophageal reflux).8 Allergic rhinitis, a very common comorbidity in severe asthmatics3,5 and with unique pheno-endotypic characteristics,9 also has a direct impact on sleep disorders (SD),10 including OSA; when allergic rhinitis and asthma are comorbid, the risk of developing OSA further increases.11 Interestingly, many asthmatic patients refer SD such as frequent awakenings, snoring and daytime drowsiness, and these conditions have a relevant impact on the quality of life of patients with asthma, including those affected by severe asthma. The term sleep disorders embrace a spectrum of breathing abnormalities including mainly OSA, snoring, respiratory-related arousals and hypoventilation.12 OSA is a complex pathology influenced by numerous factors such as craniofacial structure, obesity, upper airway collapsibility, muscle tone reduction during sleep, lower arousal threshold and ventilatory control.13 Snoring and arousal are generally self-reported or reported by the partner with whom the patient shares the bed. The frequent coexistence of Asthma and Sleep disorders causes a significant impairment in health-related quality of life (HRQoL).14 In this study, we attempt to analyze the link between sleep disorders and patients with severe asthma enrolled in the Severe Asthma Network Italy (SANI),15 a registry designed to identify the prevalence and characteristics of within a real-world context.16 We want to investigate the prevalence and overall disease burden of patients affected by sleep disorders in this cohort and identify their clinical features, risk factors and treatable traits.
Materials and Methods
Study Population
Severe Asthma Network Italy (SANI)15 is a disease registry that gathers clinical, functional and demographic data on patients with severe asthma. Among the clinical features collected in the registry there are also several possible comorbidities of severe asthma, including allergic rhinitis, chronic rhinosinusitis with or without nasal polyps, cardiovascular diseases, gastroesophageal reflux and sleep disorders. All these comorbidities are tracked in the registry as individual variables, leaving the investigators at each center responsible for entering accurate information based on the diagnostic tests required by the guidelines of each single comorbidity. The inclusion criteria for being enrolled in the SANI registry are: a confirmed diagnosis of severe asthma according to European Respiratory Society (ERS)/American Thoracic Society (ATS) classification,17 being aged ≥12 years, and giving informed consent to participate in the study. Briefly, ERS/ATS recommendations define as severe asthmatic a patient that, despite high doses of ICS plus another controller or chronic oral corticosteroid therapy for at least 6 months in the previous year, is still clinically uncontrolled (altered Asthma Control Test and/or Asthma Control Questionnaire), or experiencing at least 2 acute asthma exacerbations per year (or at least one severe exacerbation requiring emergency department admission, or hospitalization or intubation), or is still having a compromised lung function (FEV1<80% predicted value).17 No exclusion criteria are foreseen to guarantee the most complete and real-life picture possible of patients affected by severe asthma in Italy.15 Patients are enrolled in certified centers spread throughout Italy. Every center was selected according to inclusion criteria involving staff and equipment standards, diagnostic and research criteria defined by protocol approved by the Central Ethics Committee (see below).
We performed a retrospective analysis on the data from SANI registry to investigate the prevalence of sleep disorders and the clinical features of this comorbidity in patients with severe asthma. Patients were stratified based on the presence or absence of sleep disorders at their baseline visit in the SANI registry. Symptoms of sleep disorders (snoring and clinical diagnosis of OSA) were confirmed by the investigators from the various clinical centres that support the SANI initiative.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation or median and interquartile range, as appropriate, while categorical variables were represented as counts and percentages. Differences in the distributions of demographic and clinical characteristics among subjects with or without sleep disorders were evaluated using Student’s t-test for means, Wilcoxon–Mann–Whitney for medians and Chi-squared test for proportions. For all variables with at least one expected count less than 5, Fisher’s exact test was used instead of a chi-squared test.
A multivariable logistic regression was performed to assess the association of demographic and clinical variables with the presence of sleep disorders (yes vs no). Variables having a significant univariate test (p-value <0.05) and with less than 10% of missing values were selected for the multivariable analysis. We excluded highly correlated variables (eg, if body mass index, BMI was selected, height and weight were excluded). Therapies were also excluded since they were directly related to predictors of disease severity and including them would result in biased estimates of the variables of interest (collider bias).
A two-tailed p-value <0.05 was considered statistically significant. Statistical analyses were performed using SAS statistical software version 9.4.
Ethical Issues
The study was carried out according to the declarations of Helsinki and Oviedo. The SANI registry12 was set up according to the 3rd Edition Recommendation on registries for evaluating patient outcomes published by the Effective Health Care Program of the Agency for Healthcare Research and Quality.18 The protocol was performed according to the principles and procedures of the Good Clinical Practice (ICH Harmonized Tripartite Guidelines for Good Clinical Practice 1996; Directive 91/507. EEC, The Rules Governing Medical Products in the European Community) and according to the Italian laws (Legislative Decree n.211, 24 June 2003; Legislative Decree n.200 6 November 2007; Health Ministry Decree, 21 December 2007). The Registry Protocol, with the Project Code OR00617 and the study number 1742, has been approved by the Central Ethics Committee; the enrolment in the other centres started upon approval of each local Ethics Committee. All enrolled patients signed an informed consent.
Results
Out of 2042 patients in the registry, 219 were excluded for lack of sleep data. Of the remaining 1823 patients, 475 (26.1%) patients had SD: 374 (20.5% of the entire study population, corresponding to 78.7% of patients with reported SD) with snoring and 101 (5.5% of the entire study population, corresponding to 21.3%) with OSA (Figure 1). Patients with SD were more frequently men (214, 45.1% vs 480, 35.6%, p<0.001) and overweight (median BMI [IQR]: 27.3 [23.9–31.6] vs 25.2 [22.3–28.2], p<0.001 (Table 1).
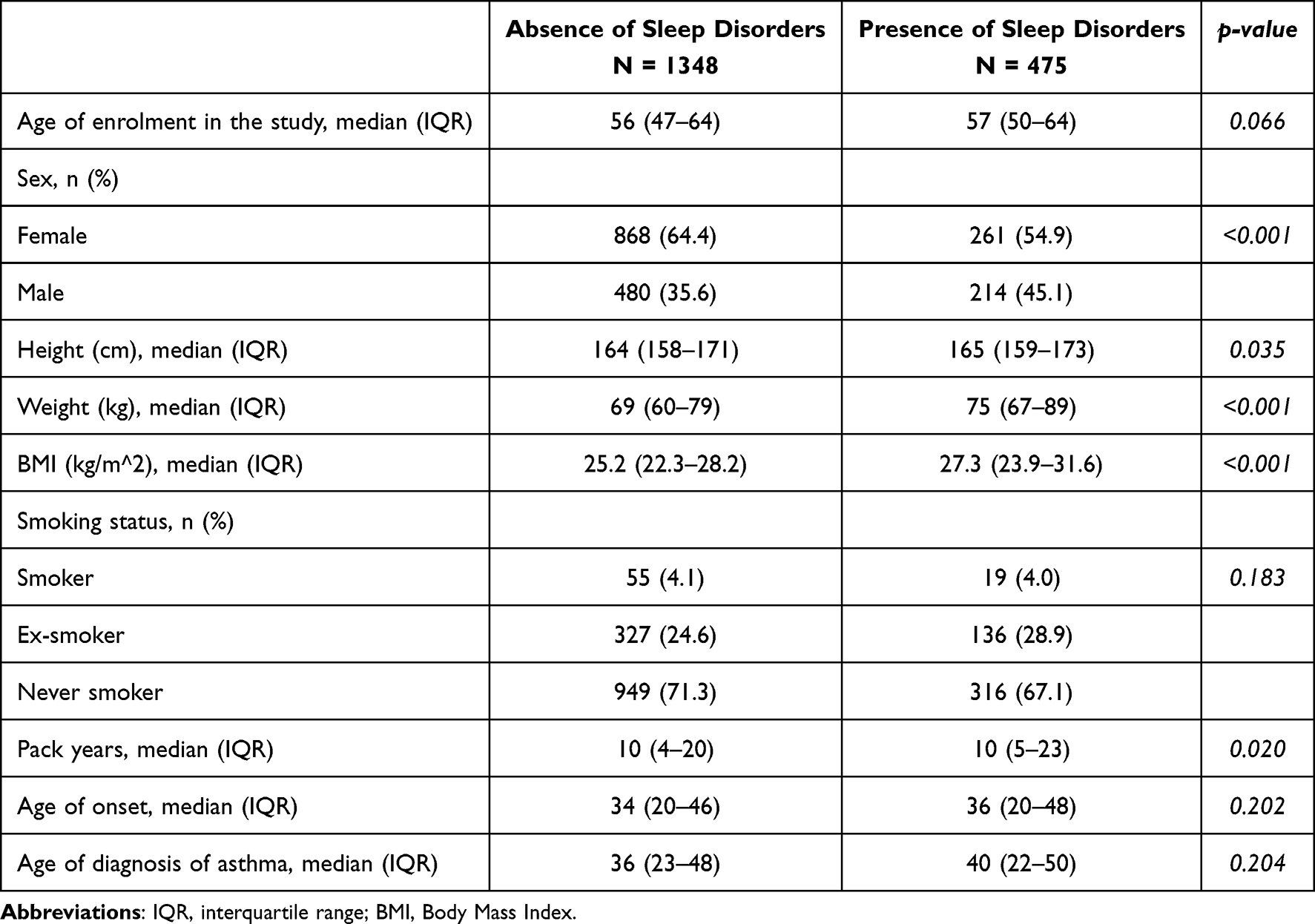 |
Table 1 Demographic Characteristics in Patients with and without Sleep Disorders |
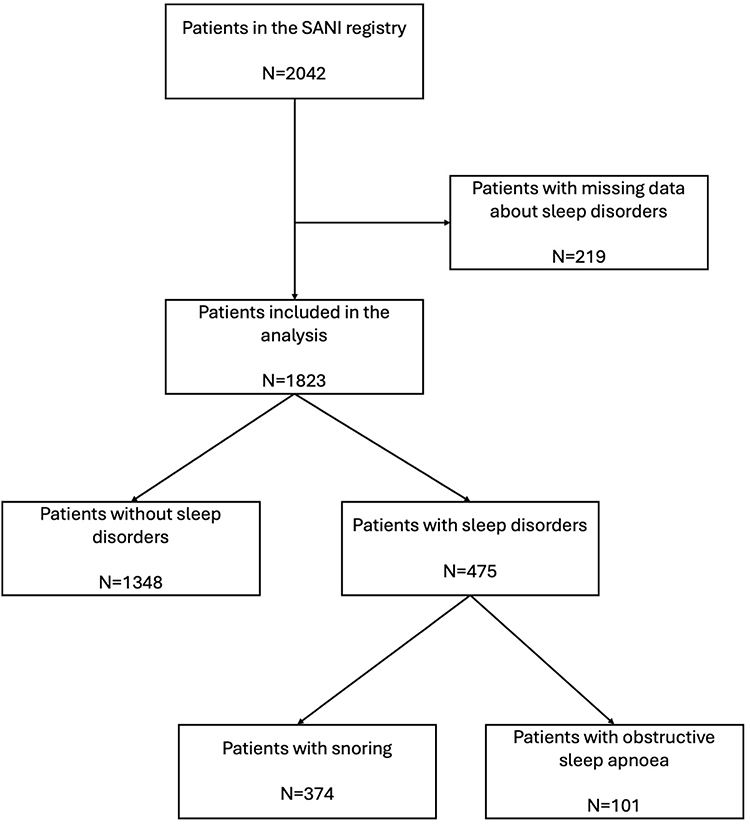 |
Figure 1 Flowchart of patients’ selection. |
Patients with SD had more frequently rhinitis ever in their lives (356, 75.6% vs 812, 60.8%, p<0.001). Moreover, patients with SD that experienced rhinitis were more prone to have moderate to severe disease (Table 2). Chronic rhinosinusitis without nasal polyps (CRSsNP) and with nasal polyps (CRSwNP) were more frequent in patients with SD (172, 37.1% vs 341, 26.3%, p<0.001 and 266, 56.2% vs 554, 41.3%, p<0.001, respectively). Patients with CRSwNP and SD had a higher extension of polyps in nasal cavities compared to those without SD as reported in Table 2. Moreover, the prevalence of gastroesophageal reflux disease (GERD) in patients suffering also from SD was higher than those without SD (251, 53.2% vs 467, 34.8%, p<0.001), as well as cardiovascular diseases (CVD) (181, 40.1% vs 293, 23.7%, p<0.001), and diabetes mellitus (37, 8.2% vs 55, 4.4%, p=0.004) (Table 2). The multivariable logistic regression confirmed that several factors were significantly associated with SD. Higher BMI was a significant predictor (OR = 1.10, 95% CI = 1.07–1.14, p < 0.001). Moderate-to-severe persistent rhinitis showed a strong association (OR = 2.52, 95% CI = 1.65–3.85, p < 0.001), as did a history of CRSsNP in the past (OR = 1.83, 95% CI = 1.15–2.89, p = 0.010). CRSwNP was also associated with increased risk (OR = 1.77, 95% CI = 1.28–2.45, p<0.001), along with confirmed GERD (OR = 1.81, 95% CI = 1.29–2.53, p <0.001) and suspected GERD (OR = 2.86, 95% CI = 1.87–4.40, p < 0.001). CVD was another significant factor (OR = 1.53, 95% CI = 1.09–2.13, p = 0.014) (Figure 2).
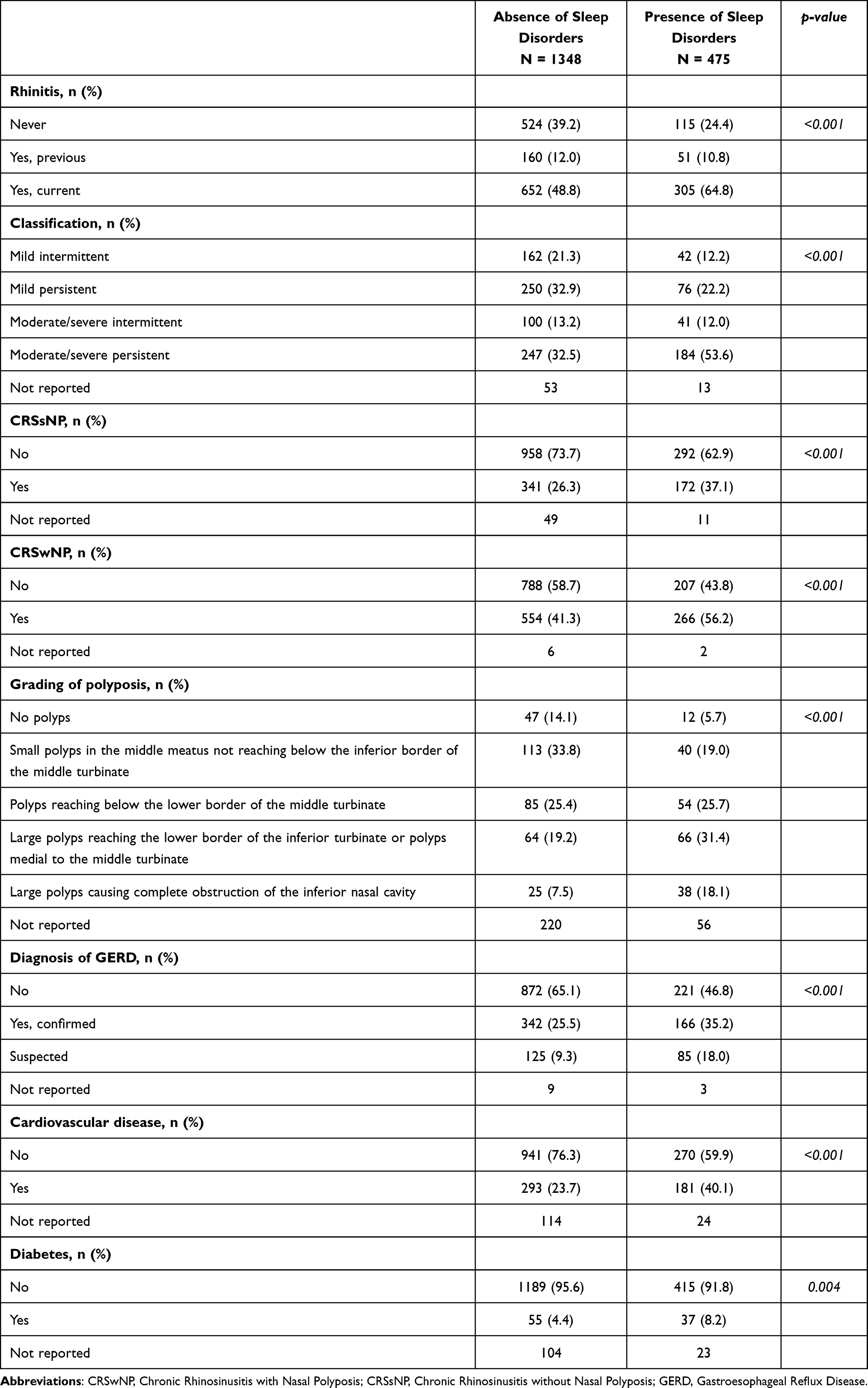 |
Table 2 Comorbidities in Patients with and without Sleep Disorders |
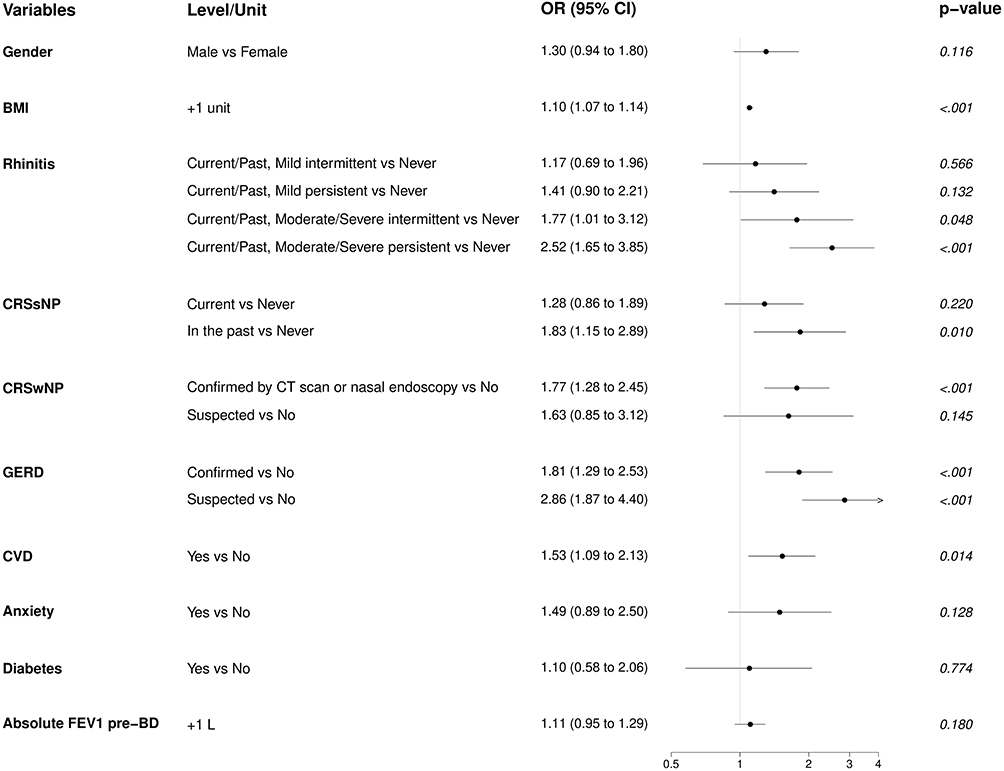 |
Figure 2 Results of multivariable logistic regression to assess the association of demographic and clinical variables with the presence of sleep disorders (yes vs no). Abbreviations: BD, bronchodilator; BMI, body mass index; CRSsNP, Chronic rhinosinusitis without nasal polyps; CRSwNP, Chronic rhinosinusitis with nasal polyps; CVD, cardiovascular disease; FEV1, forced expiratory volume in the first second; GERD, gastroesophageal reflux disease. |
Patients with SD, had higher mean Forced Expiratory Volume in the first second values (FEV1% 77.4±24% vs 73.9±21.8%, p=0.014) but worse Asthma Control Test (ACT: mean 16.8±5.3 vs 18±5.2, p<0.001) and quality of life (Asthma Quality of Life Questionnaire, AQLQ: mean 4.3±1.4 vs 4.7±1.4, p<0.001). Patients with SD had higher number of missed working days (median [IQR]: 0 [0–12] vs 0 [0–5], p<0.001) and, though statistically non-significant, an increase in disease-related hospital admissions (71, 15.7% vs 145, 11.5%, p 0.052). Additionally, a higher proportion of patients had at least an unscheduled medical visit (162, 40.5% vs 265, 26.0%, p<0.001) was observed in patients with SD. Moreover, patients with SD had a higher number of exacerbations needing systemic corticosteroid treatment (median [IQR]: 2 [0–4] vs 1 [0–3], p=0.002), as well as a generally higher occurrence of exacerbation needing oral corticosteroids (OCS) (300, 69.4% vs 729, 61.8%, p=0.005) (Table 3).
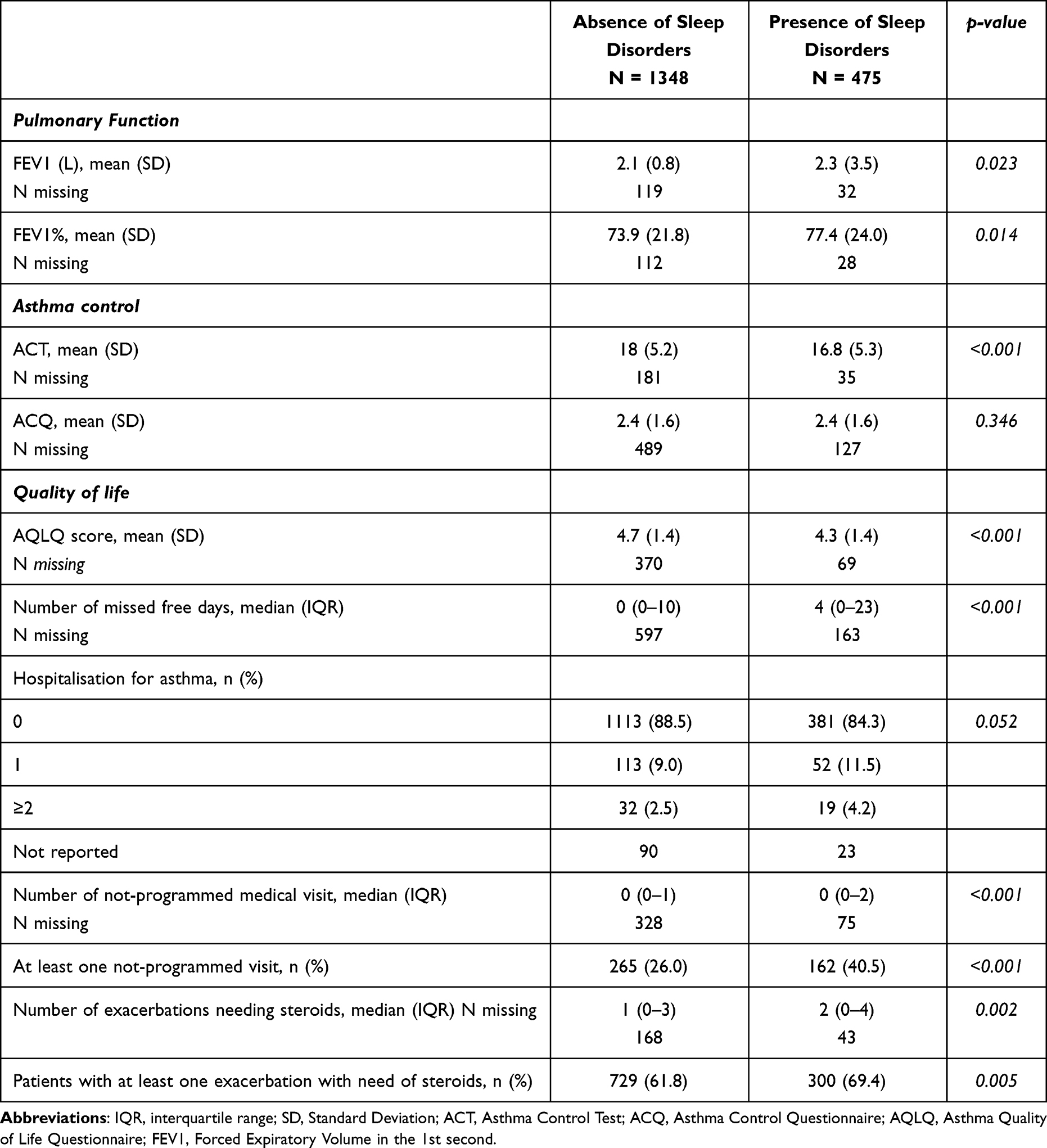 |
Table 3 Asthma Features in Patients with and without Sleep Disorders |
Furthermore, patients with SD used more frequently intranasal corticosteroids (139, 29.3% vs 247, 18.3% p<0.001). About biological therapies, no significative difference was found among the two populations of severe asthmatic patients with and without sleep disorders (189, 39.8% vs 597, 44.3%, p 0.099) (Table 4).
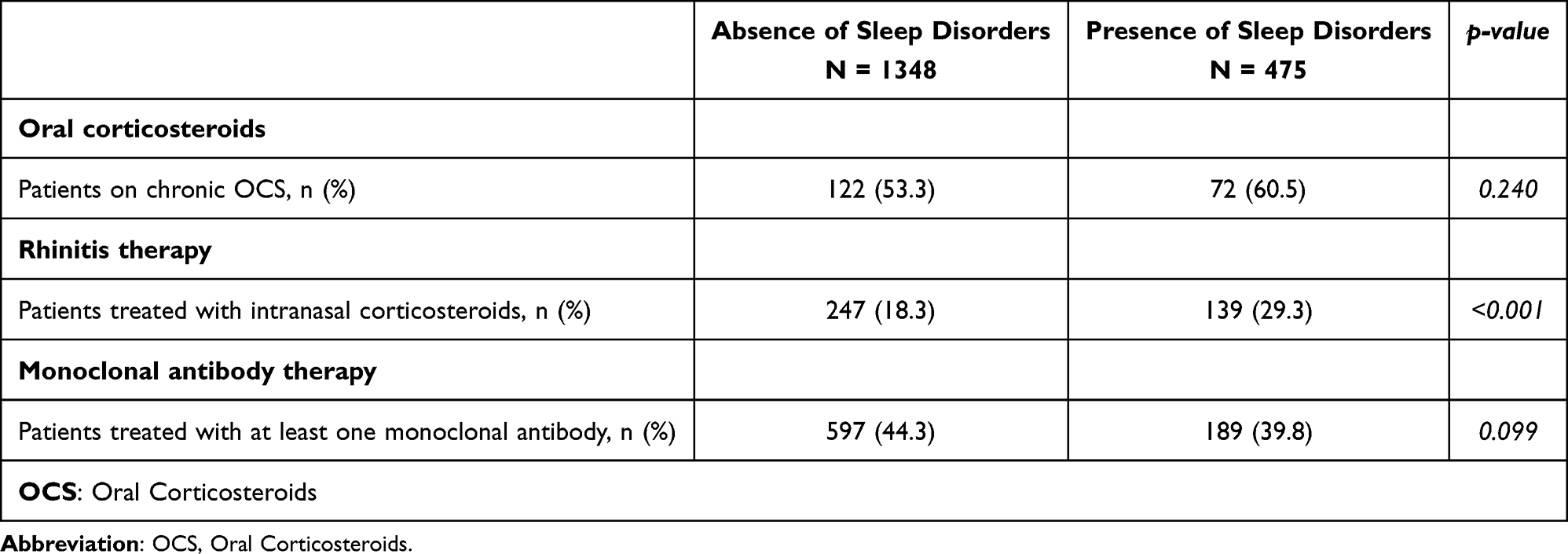 |
Table 4 Treatments Administered to Patients with and without Sleep Disorders |
Discussion
In this analysis of SANI registry data, we found that about one out of four patients with severe asthma suffer from SD. Asthma has been described to be more severe if sleep disorders coexist.19 The link between asthma and sleep disorders complicates the disease management and affects the severity of symptoms, quality of life and overall healthcare burden.20 Therefore, sleep disorders should be considered a treatable trait when assessing patients with severe asthma since the vicious cycle between the two diseases amplifies and destabilizes the pathologies taken individually.21 Our study is one of the first observational registry-based studies examining the prevalence of sleep disorders in a large population of adults with severe asthma. The high prevalence of sleep disorders in our cohort underscores the importance of considering sleep disorders as a comorbidity in patients with severe asthma.22 Considering the limit that not all the patients had performed a polysomnography, the discrepancy between snoring and OSA could reflect an underdiagnosed OSA or other respiratory-related sleep disorders. Furthermore, the relatively low number of patients with a diagnosis of sleep apnoea (that need confirmation by polysomnography) compared to patients who only reported snoring, could highlight the need of a more detailed screening protocol in all patients suffering from severe asthma.
In our study, SD were more frequent overweight patients, supporting the existing literature that identifies overweight as a common risk factor for sleep disorders such as obstructive sleep apnoea23 because it promotes upper airway collapse.24 The significantly higher mean BMI in patients with sleep disturbances suggests a potential area for intervention, as weight reduction has been shown to improve sleep apnoea symptoms. Interesting is the evidence showing no significant correlation between smoking and sleep disorders in this cohort, which contrasts with some previous studies that have suggested a potential link.25 It is important to consider this data in the context of the study’s demographic or the possibility that the impact of smoking might be overshadowed by the severity of the patients’ existing respiratory conditions.
Moreover, our study shows that rhinitis, especially the persistent moderate/severe type, and chronic rhinosinusitis (both with or without nasal polyps), are significantly more frequent in patients with severe asthma and sleep disorders. These conditions contribute to the breathing abnormalities, snoring, apnea and arousal typically found in sleep disorders.26 As seen in a previous SANI study6 patients affected by severe asthma and chronic rhinosinusitis with nasal polyps were more prone to be frequent exacerbators with a significantly higher oral corticosteroids exposure. These observations support the notion that CRSwNP may be a part of a distinctive clinical phenotype of asthma with shared inflammatory pathways and mechanical effects influencing both upper and lower airways. We can therefore speculate that treating the upper airways could ameliorate SD and asthma. This speculation is supported by a recent finding of very rapid improvement of SD in patients with CRSwNP (most of them with concomitant asthma) treated with Dupilumab.27
More than a half of our patients with severe asthma and SD also have GERD, in line with previous studies,3 and its presence is associated with higher risk to have SD. Although this is a common disease, this condition induces mucosal inflammation causing spasm of the upper-airway and oedema, which could worsen asthma and promoting SD.28 These mechanisms generate a vicious circle that perpetuates itself, amplifying and destabilizing the two diseases.29,30
The finding about higher rate of CVD in our patients with severe asthma and SD is supported by a previous study of by Xu M. et al,31 that links asthma and increased CVD rate by chronic systemic inflammation, an underlying condition in asthmatic state.32 Moreover, our population group suffering from SD is frequently overweight or obese. Obesity and an increased intra-abdominal adipose tissue are the leading causes of metabolic syndrome and type II diabetes,33,34 whose prevalence in our study is higher in patients with SD. It is also important not to underestimate the side effects of long-term oral corticosteroids therapy needed by patients with poorly controlled severe asthma. Indeed, several studies reported increased rates of diabetes mellitus, obesity, and CVD in patients with severe asthma and long-term OCS use compared with patients with milder disease and less or no OCS use.35–37
Interestingly, our patients with SD showed less severe lung function impairment but worse control and quality of life, with an increased number of asthma exacerbations, unscheduled medical visits and higher OCS exposure. The finding that these patients have worse asthma control and quality of life, despite less severe functional impairment based on FEV1, may indicate that sleep disturbances are an important factor in the overall management of asthma. As found by Teodorescu et al, individuals with OSAS are 3.6 times as likely to have uncontrolled asthma,38 that leads to a higher number of disease-related hospital admissions and the need of non-programmed medical visit.
As previously mentioned, patients with severe asthma and SD also presented a higher exacerbation rate needing steroid treatment and higher frequency of maintenance OCS therapy. These data define a more difficult-to-treat asthma phenotype that need to be further investigated, and it might be indicative of the complex interplay between sleep and asthma control, suggesting that treatment for sleep disorders might be an overlooked therapeutic target to reduce the need for intensive asthma therapy and improve outcomes. Based on this compelling data, physicians should be aware that treatment of patients with severe asthma and sleep disorders has the potential to improve patient outcomes and reduce healthcare burden.
Considering the overall results of our study, we confirm and strengthen the concept that sleep disorders are a common and relevant clinical feature among patients with severe asthma, and physicians should consider investigating patients’ sleep quality in their daily clinical practice. It is important to consider asthma and sleep disorders as two entities which can influence each other, and only treating properly both we could improve patient quality of life and reduce healthcare burden. Personalized therapeutical approaches, focused on modifying and treating comorbidities, including sleep disorders, are therefore necessary to guarantee a better management of asthma and so a better health outcome.
This study has some limitations that are intrinsic to the real-life nature of the registry from which the data derive: in particular, being a registry of patients with severe asthma, it is possible that not all patients were systematically evaluated for suspected sleep disorders and even fewer patients underwent a polysomnographic examination to confirm the suspicion of OSA; furthermore, it is also plausible that not all centers to which patients refer have equal expertise in the management of sleep disorders, leading to possible differences in the management of these comorbidities across the centers. However, we believe that, even taking these limitations into account, our results are relevant in highlighting the complicated relationship between severe asthma and sleep disturbances.
Further research should focus on examining the long-term impact of therapy for OSA on clinical outcomes in asthma. The known overlap of the two diseases, the shared risk factors and the fact that treating one improves symptoms and outcome of the other one, could make us think about the coexistence of asthma and OSA as a single disease or to consider the asthmatic patient with OSA as a particular patient phenotype.
Abbreviations
ACT, Asthma Control Test; AQLQ, Asthma Quality of Life Questionnaire; ATS, American Thoracic Society; BMI, Body mass index; CORE, Cough/asthma, Obesity/OSA, Rhinosinusitis, and Esophageal reflux; CRSsNP, Chronic rhinosinusitis without nasal polyps; CRSwNP, Chronic rhinosinusitis with nasal polyps; CVD, cardiovascular diseases; ENFUMOSA, European Network For Understanding Mechanisms Of Severe Asthma; ERS, European Respiratory Society; FEV1, Forced Expiratory Volume in the first second values; GERD, gastroesophageal reflux disease; GINA, Global Initiative for Asthma; HRQoL, health-related quality of life; ICS, inhaled corticosteroids; LABA, long-acting beta2-agonists; LTOCS, long-term oral corticosteroids; OCS, oral corticosteroids; OSA, obstructive sleep apnea; SANI, Severe Asthma Network Italy; SD, sleep disorders.
Acknowledgments
The abstract of this paper was presented at the European Respiratory Society (ERS) Annual Congress 2023 as a poster presentation with interim findings. The poster’s abstract was published in ‘Conference Abstracts’ in European Respiratory Journal: https://publications.ersnet.org/content/erj/62/suppl67/pa3053. The authors would like to thank all the SANI investigators for their valuable work.
Collaborators
SANI study group;
Luisa Brussino1, Cecilia Calabrese2, Gianna Camiciottoli3, Giovanna Elisiana Carpagnano4,5, Stefano Centanni6, Angelo Guido Corsico7, Maria Teresa Costantino8, Claudia Crimi9, Mirta Cavallini10, Simona D’Alo11, Maria D’Amato12, Corrado D’Andria13, Stefano Del Giacco14, Fabiano Di Marco15, Nicola Cosimo Facciolongo16, Alessandro Farsi17, Manuela Latorre18, Eustachio Nettis19, Eleonora Nucera20,21, Giovanni Passalacqua22, Girolamo Pelaia23, Laura Pini24, Luisa Ricciardi25, Fabio Luigi Massimo Ricciardolo26, Luca Richeldi27, Erminia Ridolo28, Pierachille Santus29, Nicola Scichilone30, Giulia Scioscia31, Gianenrico Senna32, Giuseppe Spadaro33, Antonio Spanevello34, Paolo Tarsia35
1S.S.D.D.U. Immunologia Clinica e Allergologia, Ospedale Mauriziano TorinoItaly; 2Department of Translational Medical Sciences, University of Campania “Luigi Vanvitelli” NaplesItaly; 3UNIT ASMA GRAVE - Ambulatorio Asma Grave Pneumologia e Fisiopatologia Toraco-Polmonare, Azienda Ospedaliera Universitaria Careggi (FI) FlorenceItaly; 4Department of Translational Biomedicine and Neuroscience “DiBraiN”, University of Bari Aldo Moro BariItaly; 5Section of Respiratory Diseases, Policlinico Hospital of Bari BariItaly; 6Respiratory Unit, ASST Santi Paolo e Carlo, San Paolo Hospital, Department of Health Sciences, University of Milan MilanItaly; 7Division of Respiratory Diseases, IRCCS Policlinico San Matteo, Foundation and Department of Internal Medicine and Therapeutics, University of Pavia PaviaItaly; 8Allergy and Clinical Immunology Unit, Department of Medicine, “Carlo Poma” Hospital MantovaItaly; 9Respiratory Medicine Unit, Policlinico “G. Rodolico-San Marco” University Hospital CataniaItaly; 10Broncopneumologia, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico MilanItaly; 11UOC Allergologia - PO Civitanova Marche - AREA VASTA 3 Civitanova MarcheItaly; 12Department of Respiratory Medicine, University “Federico II” of Naples NaplesItaly; 13Internal and Respiratory Medicine, SS Annunziata Hospital TarantoItaly; 14Unit of Allergy and Clinical Immunology, Department of Medical Sciences and Public Health, University of Cagliari CagliariItaly; 15Pulmonary Medicine Unit, ASST Papa Giovanni XXIII Hospital BergamoItaly; 16UOC di Pneumologia, Arcispedale S. Maria Nuova Azienda USL di Reggio Emilia Reggio EmiliaItaly; 17SOSD Allergology and Clinical Immunology, Ospedale S. Stefano, USL Toscana Centro PratoItaly; 18Pulmonary Unit, Nuovo Ospedale Apuano MassaItaly; 19Department of Emergency and Organ Transplantation, School and Chair of Allergology and Clinical Immunology, University of Bari - Aldo Moro BariItaly; 20Fondazione Policlinico Universitario Agostino Gemelli IRCCS - Università Cattolica del Sacro Cuore RomeItaly; 21UOSD Allergologia e Immunologia Clinica, Dipartimento Scienze Mediche e Chirurgiche, Fondazione Policlinico Universitario A. Gemelli IRCCS - Università Cattolica del Sacro Cuore RomeItaly; 22Clinica di Malattie Respiratorie e Allergologia, Dip. Medicina Interna, University of Genova, IRCCS-AOU San Martino GenoaItaly; 23U.O. Malattie dell’Apparato Respiratorio, A.O.U. Mater Domini CatanzaroItaly; 24Department of Clinical and Experimental Sciences, University of Brescia - ASST Spedali Civili di Brescia BresciaItaly; 25Allergologia e Immunologia Clinica, AOU Policlinico G. Martino - Università di Messina MessinaItaly; 26Department of Clinical and Biological Sciences, University of Turin, San Luigi Gonzaga University Hospital Orbassano, TurinItaly; 27Fondazione Policlinico Universitario A. Gemelli, IRCCS Catholic University of Rome RomeItaly; 28Department of Medicine and Surgery, University of Parma ParmaItaly; 29Department of Clinical and Biomedical Sciences, University of Milan, Respiratory Diseases, Sacco University Hospital, ASST Fatebenefratelli-Sacco MilanItaly; 30U.O.C. Pneumologia, Azienda Ospedaliera Universitaria Policlinico P. Giaccone di Palermo PalermoItaly; 31Malattie Apparato Respiratorio, Dipartimenti delle funzioni Mediche e Sanitarie, Azienda Ospedaliero Universitaria - Ospedali Riuniti FoggiaItaly; 32Department of Medicine, University of Verona, and Asthma Center and Allergy Unit, Verona University Hospital VeronaItaly; 33Center for Basic and Clinical Immunology Research (CISI), University of Naples Federico II NaplesItaly; 34Pneumologia Riabilitativa, ICS Maugeri IRCCS Tradate Tradate (VA)Italy; 35Pneumology Unit, Grande Ospedale Metropolitano Niguarda MilanItaly
Funding
This work was supported by unrestricted grants from Astrazeneca, Sanofi, GlaxoSmith & Kline.
Disclosure
Sebastian Ferri, Valentina Marzio, Edoardo Cavaglià, Nicolò Valli, Vincenzo Bagnardi, Chiara Oriecuia, Isabella Sala, Cristina Cardini, Concetta Sirena, and Giovanni Paoletti do not have any conflict of interest to declare for this work. Francesco Blasi reports grants and/or personal fees from AstraZeneca, Boehringer ingheleim, Bayer, Chiesi, GSK, Grifols, Guidotti, Insmed, Menarini, MSD, Novartis, OM Pharma, Pfizer, Sanofi, Zambon and Vertex, outside the submitted work.
Pierluigi Paggiaro reports grants and/or personal fees from AstraZeneca, Chiesi Farmaceutici, GSK, Guidotti, Lusofarmaco and Sanofi, outside the submitted work. Giorgio Walter Canonica reports grants and/or personal fees from A. Menarini, Anallergo, Allergy Therapeutics, AstraZeneca, Chiesi Farmaceutici, Faes, Firma, Genentech, Guidotti-Malesci, Glaxo Smith Kline, Hal Allergy, Innovacaremd, Novartis, OmPharma, RedMaple, Sanofi-Aventis, Sanofi-Genzyme, Stallergenes-Greer, and Uriach Pharma, outside the submitted work. Enrico Heffler reports grants and/or personal fees from Astrazeneca, GSK, Sanofi, Regeneron, Novartis, Chiesi, Stallergenes-Greer, Bosch, Celltrion-Healthcare, Almirall, Lofarma, and Apogee Therapeutics, outside the submitted work.
References
1. Global initiative for asthma (GINA). Available from: https://ginasthma.org/.
2. The ENFUMOSA cross-sectional European multicentre study of the clinical phenotype of chronic severe asthma. Eur Respir J. 2003;22(3):470–477. doi:10.1183/09031936.03.00261903
3. Scelo G, Torres-Duque CA, Maspero J, et al. Analysis of comorbidities and multimorbidity in adult patients in the International Severe Asthma Registry. Ann Allergy Asthma Immunol. 2024;132(1):42–53. doi:10.1016/j.anai.2023.08.021
4. Paoletti G, Melone G, Ferri S, et al. Gastroesophageal reflux and asthma: when, how, and why. Curr Opin Allergy Clin Immunol. 2021;21(1):52–58. doi:10.1097/ACI.0000000000000705
5. Nappi E, Paoletti G, Malvezzi L, et al. Comorbid allergic rhinitis and asthma: important clinical considerations. Expert Rev Clin Immunol. 2022;18(7):747–758. doi:10.1080/1744666X.2022.2089654
6. Canonica GW, Malvezzi L, Blasi F, et al. Chronic rhinosinusitis with nasal polyps impact in severe asthma patients: evidences from the Severe Asthma Network Italy (SANI) registry. Respir Med. 2020;166:105947. doi:10.1016/j.rmed.2020.105947
7. Sharma V, Cowan DC. Obesity, inflammation, and severe asthma: an update. Curr Allergy Asthma Rep. 2021;21(12):46. doi:10.1007/s11882-021-01024-9
8. Tondo P, Hoxhallari A, Lacedonia D, et al. The CORE syndrome: an overlap of severe asthma, obstructive sleep apnea, rhinosinusitis, and esophageal reflux. Sleep Breathing. 2024;28(4):1761–1765. doi:10.1007/s11325-024-03028-x
9. Chirakalwasan N, Ruxrungtham K. The linkage of allergic rhinitis and obstructive sleep apnea. Asian Pac J Allergy Immunol. 2014;32(4):276–286.
10. Berghi O, Dumitru M, Caragheorgheopol R, et al. The relationship between chemokine ligand 3 and allergic rhinitis. Cureus. 2020;12(4):e7783. doi:10.7759/cureus.7783
11. Ferreira NB, Ponte A, Grande AC, et al. Frequency of obstructive sleep apnea in patients with asthma or allergic rhinitis: a systematic review and meta-analysis. Sleep Med. 2025;134:106705. doi:10.1016/j.sleep.2025.106705
12. Dempsey JA, Veasey SC, Morgan BJ, O’Donnell CP. Pathophysiology of sleep apnea. Physiol Rev. 2010;90(1):47–112. doi:10.1152/physrev.00043.2008
13. Wang R, Mihaicuta S, Tiotiu A, Corlateanu A, Ioan IC, Bikov A. Asthma and obstructive sleep apnoea in adults and children – an up-to-date review. Sleep Med Rev. 2022;61:101564. doi:10.1016/j.smrv.2021.101564
14. Ekici A, Ekici M, Kurtipek E, et al. Association of asthma-related symptoms with snoring and apnea and effect on health-related quality of life. Chest. 2005;128(5):3358–3363. doi:10.1378/chest.128.5.3358
15. Senna G, Guerriero M, Paggiaro PL, et al. SANI-Severe asthma network in Italy: a way forward to monitor severe asthma. Clin Mol Allergy. 2017;15(1):9. doi:10.1186/s12948-017-0065-4
16. Heffler E, Blasi F, Latorre M, et al. The severe asthma network in italy: findings and perspectives. J Allergy Clin Immunol Pract. 2019;7(5):1462–1468. doi:10.1016/j.jaip.2018.10.016
17. Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43(2):343–373. doi:10.1183/09031936.00202013
18. Effective health care program of the agency for healthcare research and quality. Available from: https://effectivehealthcare.ahrq.gov/topics/registries-guide-3rd-edition/research/.
19. Shaker A. Study of obstructive sleep apnea (OSA) in asthmatics. Egypt J Chest Dis Tuberculosis. 2017;66(2):293–298. doi:10.1016/j.ejcdt.2017.04.002
20. Prasad B, Nyenhuis SM, Imayama I, Siddiqi A, Teodorescu M. Asthma and obstructive sleep apnea overlap: what has the evidence taught us? Am J Respir Crit Care Med. 2020;201(11):1345–1357. doi:10.1164/rccm.201810-1838TR
21. Damianaki A, Vagiakis E, Sigala I, et al. The co-existence of obstructive sleep apnea and bronchial asthma: revelation of a new asthma phenotype? J Clin Med. 2019;8(9):1476. doi:10.3390/jcm8091476
22. Liu X, Hong C, Liu Z, et al. Association of sleep disorders with asthma: a meta-analysis. BMJ Open Respir Res. 2023;10(1):e001661. doi:10.1136/bmjresp-2023-001661
23. Romero-Corral A, Caples SM, Lopez-Jimenez F, Somers VK. Interactions between obesity and obstructive sleep apnea. Chest. 2010;137(3):711–719. doi:10.1378/chest.09-0360
24. Isono S. Obesity and obstructive sleep apnoea: mechanisms for increased collapsibility of the passive pharyngeal airway. Respirology. 2012;17(1):32–42. doi:10.1111/j.1440-1843.2011.02093.x
25. Deleanu OC, Pocora D, Mihălcuţă S, Ulmeanu R, Zaharie AM, Mihălţan FD. Influence of smoking on sleep and obstructive sleep apnea syndrome. Pneumologia. 2016;65(1):28–35.
26. Braido F, Baiardini I, Ferrando M, et al. The prevalence of sleep impairments and predictors of sleep quality among patients with asthma. J Asthma. 2021;58(4):481–487. doi:10.1080/02770903.2019.1711391
27. Ferri S, Montagna C, Casini M, et al. Sleep quality burden in chronic rhinosinusitis with nasal polyps and its modulation by dupilumab. Ann Allergy Asthma Immunol. 2024;132(1):69–75. doi:10.1016/j.anai.2023.08.594
28. Taillé C, Rouvel-Tallec A, Stoica M, et al. Obstructive sleep apnoea modulates airway inflammation and remodelling in severe asthma. PLoS One. 2016;11(3):e0150042. doi:10.1371/journal.pone.0150042
29. Havemann BD, Henderson CA, El-Serag HB. The association between gastro-oesophageal reflux disease and asthma: a systematic review. Gut. 2007;56(12):1654–1664. doi:10.1136/gut.2007.122465
30. Orr WC, Robert JJT, Houck JR, Giddens CL, Tawk MM. The effect of acid suppression on upper airway anatomy and obstruction in patients with sleep apnea and gastroesophageal reflux disease. J Clin Sleep Med. 2009;5(4):330–334.
31. Xu M, Xu J, Yang X. Asthma and risk of cardiovascular disease or all-cause mortality: a meta-analysis. Ann Saudi Med. 2017;37(2):99–105. doi:10.5144/0256-4947.2017.99
32. Tattersall MC, Jarjour NN, Busse PJ. Systemic inflammation in asthma: what are the risks and impacts outside the airway? J Allergy Clin Immunol Pract. 2024;12(4):849–862. doi:10.1016/j.jaip.2024.02.004
33. Shinohara E, Kihara S, Yamashita S, et al. Visceral fat accumulation as an important risk factor for obstructive sleep apnoea syndrome in obese subjects. J Intern Med. 1997;241(1):11–18. doi:10.1046/j.1365-2796.1997.63889000.x
34. Vgontzas AN, Papanicolaou DA, Bixler EO, et al. Sleep apnea and daytime sleepiness and fatigue: relation to visceral obesity, insulin resistance, and hypercytokinemia. J Clin Endocrinol Metab. 2000;85(3):1151–1158. doi:10.1210/jcem.85.3.6484
35. Zazzali JL, Broder MS, Omachi TA, Chang E, Sun GH, Raimundo K. Risk of corticosteroid-related adverse events in asthma patients with high oral corticosteroid use. Allergy Asthma Proc. 2015;36(4):268–274. doi:10.2500/aap.2015.36.3863
36. Westerhof GA, de Groot JC, Amelink M, et al. Predictors of frequent exacerbations in (ex)smoking and never smoking adults with severe asthma. Respir Med. 2016;118:122–127. doi:10.1016/j.rmed.2016.08.006
37. Sullivan PW, Ghushchyan VH, Globe G, Schatz M. Oral corticosteroid exposure and adverse effects in asthmatic patients. J Allergy Clin Immunol. 2018;141(1):110–116.e7. doi:10.1016/j.jaci.2017.04.009
38. Teodorescu M, Polomis DA, Hall SV, et al. Association of obstructive sleep apnea risk with asthma control in adults. Chest. 2010;138(3):543–550. doi:10.1378/chest.09-3066
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Real-World Experience on the Use of Mepolizumab from the Severe Asthma Registry of the German Asthma Net (MepoGAN-Study)
Korn S, Milger K, Skowasch D, Schulz C, Mohrlang C, Wernitz M, Paulsson T, Hennig M, Buhl R
Journal of Asthma and Allergy 2023, 16:541-552
Published Date: 11 May 2023
Adult Severe Asthma Registries: A Global and Growing Inventory
Cushen B, Koh MS, Tran TN, Martin N, Murray R, Uthaman T, Goh CYY, Vella R, Eleangovan N, Bulathsinhala L, Maspero JF, Peters MJ, Schleich F, Pitrez P, Christoff G, Sadatsafavi M, Torres-Duque CA, Porsbjerg C, Altraja A, Lehtimäki L, Bourdin A, Taube C, Papadopoulos NG, Zsuzsanna C, Björnsdóttir U, Salvi S, Heffler E, Iwanaga T, al-Ahmad M, Larenas-Linnemann D, van Boven JF, Aarli BB, Kuna P, Loureiro CC, Al-lehebi R, Lee JH, Marina N, Bjermer L, Sheu CC, Mahboub B, Busby J, Menzies-Gow A, Wang E, Price DB
Pragmatic and Observational Research 2023, 14:127-147
Published Date: 20 October 2023
The Path to Diagnosis of Severe Asthma-A Qualitative Exploration
Davis SR, Cvetkovski B, Katsoulotos GP, Lee JW, Rimmer J, Smallwood N, Tonga KO, Abbott P, Bosnic-Anticevich SZ
International Journal of General Medicine 2024, 17:3601-3611
Published Date: 19 August 2024
The Effect of Comorbidities on Asthma-Related Outcomes Over a Two-Year Period: A Prospective Analysis of Swiss Severe Asthma Registry (SSAR)
Jaun F, Kanagarasa M, Boesing M, Lüthi-Corridori G, Bridevaux PO, Charbonnier F, Clarenbach CF, Gianella P, Jochmann A, Kern L, Pavlov N, Rothe T, Latshang TD, Von Garnier C, Leuppi JD
Journal of Asthma and Allergy 2025, 18:1105-1118
Published Date: 15 July 2025