Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Serum Uric Acid-to-Creatinine Ratio Is Independently Associated with Sudomotor Dysfunction in Type 2 Diabetes: A Cross-Sectional Study
Authors Peng J, Liang S, Tang X, Chen X, Xu H, Liu J, Xu W, Shui X, Yang X
Received 20 August 2025
Accepted for publication 26 January 2026
Published 18 February 2026 Volume 2026:19 562091
DOI https://doi.org/10.2147/DMSO.S562091
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Jie Peng,1,* Shangyan Liang,2,* Xiaoyun Tang,1,3 Xueyan Chen,1 Huan Xu,1 Jia Liu,1,3 Wen Xu,1 Xing Shui,4,* Xubin Yang1,3
1Department of Endocrinology and Metabolism, Guangdong Provincial Key Laboratory of Diabetology, The Third Affiliated Hospital of Sun Yat-Sen University, Guangzhou, Guangdong, People’s Republic of China; 2Department of VIP Medical Service Center, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China; 3Department of Endocrinology and Metabolism, Zhaoqing Hospital, The Third Affiliated Hospital of Sun Yat-Sen University, Zhaoqing, Guangdong, People’s Republic of China; 4Department of Cardiovascular Medicine, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xubin Yang, Department of Endocrinology and Metabolism, Guangdong Provincial Key Laboratory of Diabetology, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China, Email [email protected] Wen Xu, Department of Endocrinology and Metabolism, Guangdong Provincial Key Laboratory of Diabetology, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China, Email [email protected]
Purpose: This study investigated the association between the serum uric acid-to-creatinine ratio (SUA/Cr) and sudomotor dysfunction in patients with type 2 diabetes mellitus.
Patients and Methods: This was a single-center, inpatient, cross-sectional study. A total of 781 participants were classified into three tertiles based on their SUA/Cr. The electrochemical conductivity (ESC) of sweat obtained from the hands and feet was measured using SUDOSCAN to assess sudomotor function. Mean ESC values for the hands (HESC) and feet (FESC) were computed independently. Sudomotor dysfunction was defined as HESC or FESC ≤ 60 μS. Statistical analyses were performed using SPSS 25.0, involving one-way ANOVA, Kruskal–Wallis test, chi-square test, Spearman correlation coefficient, binary/multivariable logistic regression (with three adjusted models), and subgroup analysis, with statistical significance defined as p < 0.05.
Results: The prevalence of sudomotor dysfunction in the first, second, and third tertiles of SUA/Cr was 65.0%, 57.6%, and 48.9%, respectively. Patients with lower SUA/Cr levels exhibited a markedly increased risk of sudomotor dysfunction compared to those with higher SUA/Cr levels (p < 0.001). After adjusting for potential confounders, the association between decreased SUA/Cr ratio and sudomotor dysfunction risk remained significant (OR=1.646, 95% CI: 1.088– 2.489, p = 0.018). Subgroup analyses by age, sex, glycated hemoglobin A1c, body mass index, and duration of diabetes confirmed the robustness of the relationship between SUA/Cr and the risk of diabetic peripheral neuropathy (all interactions p > 0.05).
Conclusion: The SUA/Cr ratio is independently associated with sudomotor dysfunction in patients with type 2 diabetes mellitus.
Keywords: serum uric acid-to-creatinine ratio, sudomotor dysfunction, type 2 diabetes, diabetic peripheral neuropathy
Introduction
Diabetic peripheral neuropathy (DPN) is a major complication of type 2 diabetes mellitus (T2DM), characterized by nerve dysfunction in patients with diabetes after excluding other potential causes.1 Recent studies have indicated that approximately 50% of adults with diabetes eventually develop DPN.2 This condition is a significant risk factor for diabetic foot ulceration, a leading cause of non-traumatic lower-limb amputation.3 Additionally, DPN is also associated with an increased risk of falls, painful neuropathic symptoms, and decreased quality of life.4 Early detection and effective management of DPN risk factors can mitigate its prevalence and potentially alter its progression.3 However, early detection of DPN is challenging due to the often asymptomatic nature of early-stage DPN. Previous studies have shown that small fiber nerve damage typically precedes large fiber deterioration in patients with asymptomatic DPN,5 and sudomotor function can serve as a reliable indicator of small nerve fiber function.6 Hence, the identification of sudomotor dysfunction and its risk factors can delay the progression of DPN.7 In this context, we assessed sudomotor function using electrochemical skin conductance (ESC) with SUDOSCAN, which quantifies chloride-ion conductance at the hands and feet.
Previous studies have shown that hyperuricemia is associated with an increased risk of peripheral neuropathy in diabetes.4,8,9 However, some studies have suggested that low serum uric acid (SUA) levels are associated with a higher risk of peripheral nerve dysfunction,10,11 creating controversy regarding the relationship between SUA and DPN. This discrepancy may be due to the lack of adjustment of serum uric acid levels by renal function. Owing to the influence of renal function on uric acid excretion, an increasing number of studies have used renal function-standardized uric acid as a clinical indicator to assess the severity and prognosis of T2DM. Gu et al utilized the SUA/creatinine (Cr) ratio (SUA/Cr) to calculate the standardized SUA after normalizing for renal function, indicating that SUA/Cr levels could serve as a reliable predictive marker for renal function deterioration in T2DM.12 Furthermore, SUA/Cr levels have been linked to β-cell function and metabolic-related fatty liver disease in individuals with T2DM.13,14 Nevertheless, whether the SUA/Cr ratio is related to sudomotor dysfunction remains unclear. Additionally, age, sex, obesity, diabetes duration, and glycemic control may confound the relationship between SUA/Cr and sudomotor function. We hypothesize that lower SUA/Cr is associated with an increased likelihood of sudomotor dysfunction as defined by ESC, possibly attributable to diminished antioxidant reserve15,16 and increased microvascular stress,17 which in turn lead to small-fiber damage.
This study aimed to investigate the association between standardized SUA (SUA/Cr) and early diabetic neuropathy, which presents as sudomotor dysfunction in patients with T2DM, to provide a new approach for the early screening of DPN.
Materials and Methods
Patients
This was a single-center, inpatient, cross-sectional study that included consecutive patients hospitalized at this study center between December 2020 and September 2021. All participants provided written informed consent, and the study was approved by the Ethics Committee of the Third Affiliated Hospital of Sun Yat-sen University. In accordance with the World Health Organization diagnostic guidelines established in 1999,18 1134 adult patients with T2DM aged 18–80 years were enrolled from available participants. Exclusion criteria were as follows: (1) various acute complications of diabetes, (2) use of medications that may affect UA within the past 3 months (such as allopurinol, thiazide diuretics, salicylates, and corticosteroids), (3) peripheral neuropathy caused by other reasons, (4) severe liver or kidney dysfunction, and (5) a history of peripheral vascular disease or foot amputation. Ultimately, 781 patients were included (Figure 1).
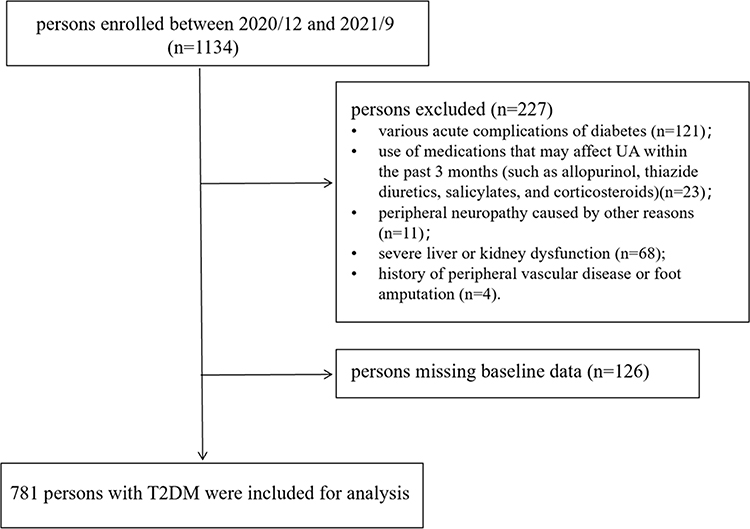 |
Figure 1 Flow chart showing the patients selection process. |
Clinical and Laboratory Data
Participants’ weight, height, resting systolic blood pressure (SBP), and diastolic blood pressure (DBP) were recorded. Experienced clinical physicians conducted detailed interviews to document the participants’ personal details, medical histories, and recent medication use. Fasting plasma samples were collected to assess levels of glycated hemoglobin A1c (HbA1c), SUA, serum Cr, estimated glomerular filtration rate (eGFR), total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and fasting plasma glucose (FPG). Each participant underwent a comprehensive evaluation of their hands and feet to check for issues such as dryness, ulcers, gangrene, or amputation, which could compromise skin integrity. Body mass index (BMI) was calculated as weight (in kilograms) divided by the square of height (in meters). The SUA/Cr was calculated as the ratio of SUA (μmol/L) to Cr (μmol/L), used to determine the standardized SUA ratio for kidney function. Based on SUA/Cr tertiles derived from sample quantiles, participants were categorized into three groups: first tertile (≤4.89), second tertile (4.90–6.61), and third tertile (>6.61).
Sudomotor Function Assessment
Sudomotor function was assessed using the SUDOSCAN device (Impeto), which measures ESC of sweat on the hands and feet. All operators conducting measurements received rigorous standardized training to ensure consistent operation. Measurements were performed in a controlled room (26°C, 45–55% relative humidity); prior to testing, participants removed hand/foot lotions, creams, or calluses, cleaned the skin with sterile water and dried it thoroughly, and abstained from caffeine (coffee, cola), strong tea, and nicotine for 24 hours to avoid confounding effects. Participants placed their hands and feet on two sets of stainless-steel electrodes simultaneously during the assessment. The electrodes were connected to a desktop computer for data processing and analysis. The test duration was approximately 2–3 minutes, during which time the sensor used reverse iontophoresis to measure the chloride ion current in the sweat. The chloride ion current was measured in microSiemens (µS). Three repeated trials were conducted per site, with average hand ESC (HESC) and foot ESC (FESC) calculated from valid trials. Failed reads (incomplete electrode contact or invalid signals) led to trial disqualification, and participants with ≥2 failed trials for hands or feet were excluded. Sudomotor dysfunction was identified by the average ESC measurement value of ≤ 60 µS on the hand or foot.19
Statistical Analyses
Statistical analyses were primarily conducted using SPSS (version 25.0). Continuous data are presented as mean ± standard deviation, non-normally distributed data as median (interquartile range), and categorical data as percentages. Group comparisons were conducted using one-way analysis of variance for continuous variables and the Kruskal–Wallis test for non-normally distributed continuous variables. The chi-square test was used for categorical data. The Bonferroni method was used to conduct pairwise comparisons among multiple samples for indicators exhibiting statistically significant differences. Spearman correlation coefficient was used to evaluate the relationship between SUA/Cr and the average ESC of the hands or feet. Binary logistic regression analysis was employed to assess the association between SUA/Cr ratio and sudomotor dysfunction. To mitigate the impact of confounding factors on sudomotor dysfunction, variables with clinical significance level of p < 0.05 in the univariate analysis were included in a multivariable logistic regression analysis. Model 1 was not adjusted for any variables; Model 2 was adjusted for age and sex; and Model 3 was adjusted for age, sex, BMI, DBP, smoking (current/former/never), TG, HDL-C, diabetes duration (years), and FPG. Odds ratios (OR) and 95% confidence intervals (CI) were calculated using logistic regression. Statistical significance was defined as p < 0.05. To address the disparities among various populations, a subgroup analysis was conducted, taking into account factors including gender, age, HbA1c, BMI, and duration of diabetes.
The following analyses were conducted using R software (version 4.5.1). Multicollinearity analysis was performed to assess collinearity among variables. Restricted cubic splines (RCS) analysis was applied in the multivariable-adjusted model to evaluate the non-linear association between SUA/Cr (per SD increment) and sudomotor dysfunction, with p-values calculated for both the overall and non-linear associations. Receiver operating characteristic (ROC) curve analysis was conducted to determine the predictive value of SUA/Cr for sudomotor dysfunction in patients with T2DM. The calibration of the prediction model was evaluated via calibration curves, with the Brier score, calibration intercept, and calibration slope computed to assess the consistency between the predicted and actual probabilities of sudomotor dysfunction; multi-dimensional discriminative indicators (eg, Dxy) were used to measure model performance.
Results
Baseline Characteristics
The baseline characteristics of the participants, categorized by the tertiles of the SUA/Cr ratio, are presented in Table 1. Among the 781 participants (59.0% men), the mean age was 55.09±13.22 years old, and the average SUA level was 375.43±112.00 µmol/L. Compared to those with higher SUA/Cr, the proportion of men, BMI, DBP, TG, eGFR, FPG, SUA, HESC, and FESC of patients in the lower SUA/Cr group was decreased, whereas age, smoking, HDL-C level, diabetes duration, proportion of sudomotor dysfunction, and Cr level was increased significantly (p < 0.05). The prevalence of sudomotor dysfunction in the first, second, and third tertiles of SUA/Cr was 65.0%, 57.6%, and 48.9%, respectively (p < 0.05). No significant differences were observed in other baseline features.
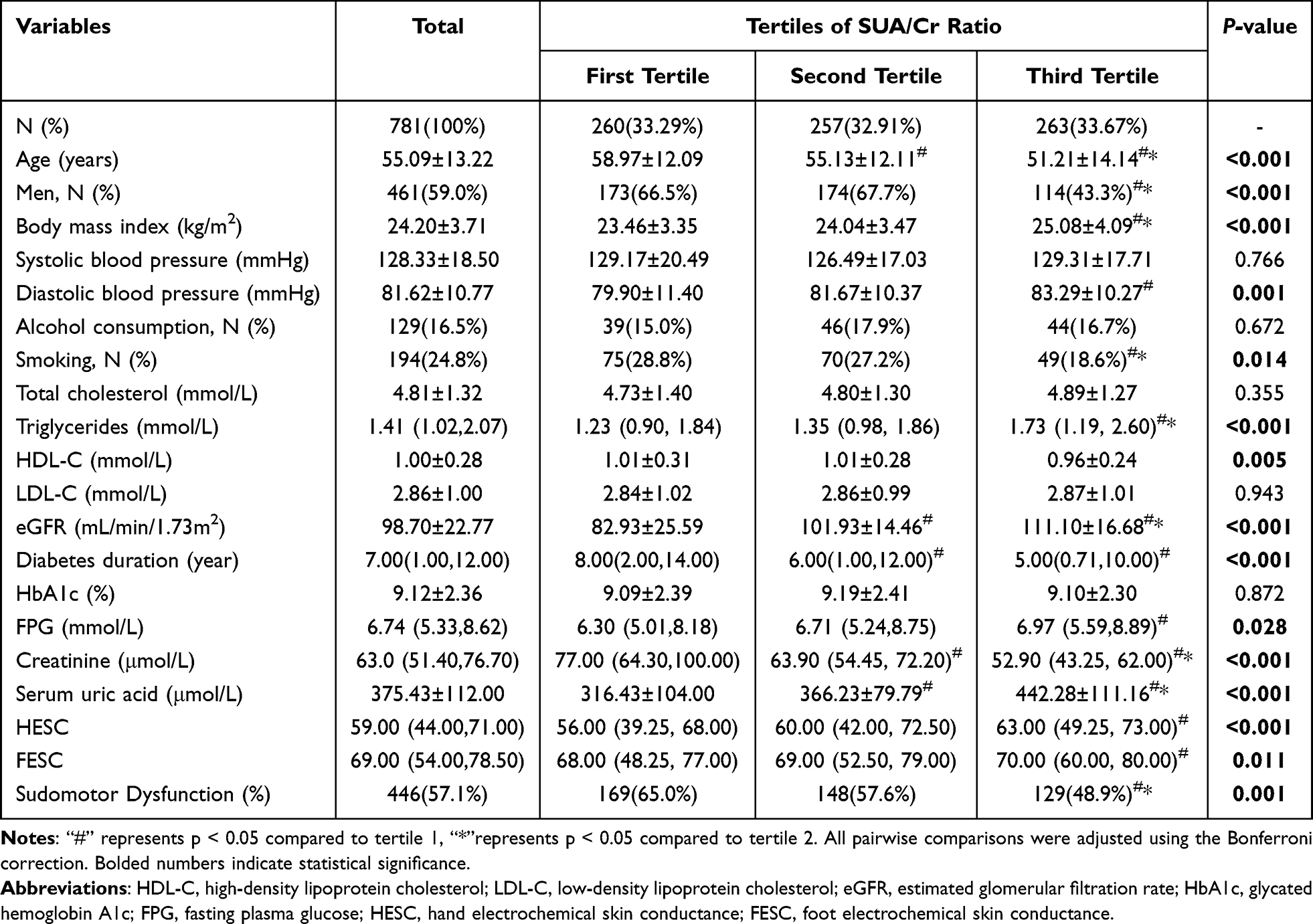 |
Table 1 Baseline Characteristics According to Tertiles of SUA/Cr Ratio |
Analysis of the Correlation Between SUA/Cr and Sudomotor Dysfunction
As shown in Figure 2a and b, Spearman correlation analysis revealed a significant correlation between the SUA/Cr ratio and both FESC and HESC. The association between SUA/Cr ratio and sudomotor dysfunction was further elucidated using binary logistic regression analysis. As indicated in Table 2, individuals with lower SUA/Cr levels were found to have a significantly increased risk of developing sudomotor dysfunction than those with higher SUA/Cr levels (OR=1.944, 95% CI: 1.368–2.761, p < 0.001) (Model 1). In Model 3, after adjusting for age, sex, BMI, DBP, smoking, TG, HDL-C, diabetes duration, and FPG, the association between decreased SUA/Cr ratio and the likelihood of experiencing sudomotor dysfunction remained significant (OR=1.646, 95% CI: 1.088–2.489, p = 0.018).
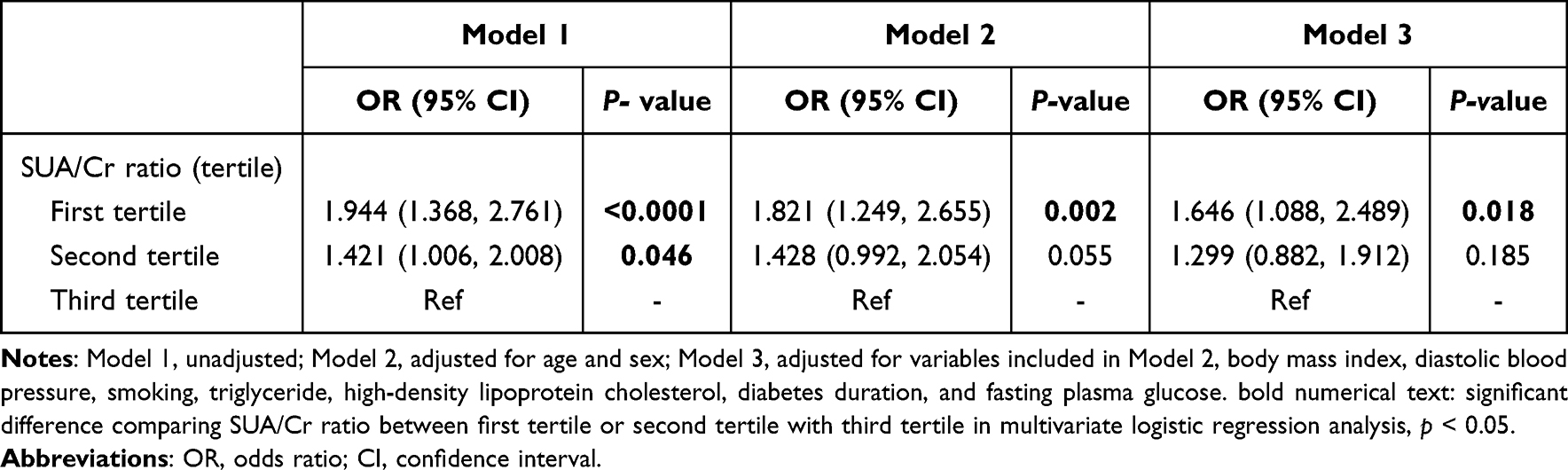 |
Table 2 Multivariate Logistic Regression Analysis of SUA/Cr and Sudomotor Dysfunction |
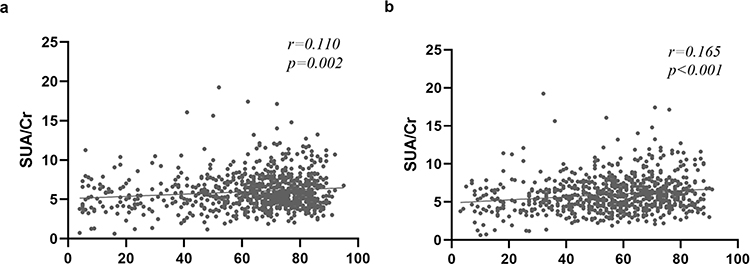 |
Figure 2 Correlation between SUA/Cr and FESC (a) or HESC (b). Abbreviations: SUA/Cr, serum uric acid-to-creatinine ratio; HESC, hand electrochemical skin conductance; FESC, foot electrochemical skin conductance. Notes: r, Spearman correlation coefficient; p < 0.05. |
Multicollinearity analysis indicated no severe multicollinearity that would distort the model estimates (Supplemental Table S1).
Restricted cubic splines (RCS) analysis was employed to assess non-linear associations between SUA/Cr per SD and sudomotor dysfunction in multivariable-adjusted model. The results indicated a significant overall association (p for overall = 0.004) but no evidence of non-linearity (p for nonlinear = 0.430), suggesting that the relationship between SUA/Cr and sudomotor dysfunction was linear (Supplemental Figure S1). Specifically, each SD increase in SUA/Cr was associated with a gradual decrease in the risk of sudomotor dysfunction.
Subgroup Analyses
In subgroup analysis, individuals with lower SUA/Cr levels were more likely to develop sudomotor dysfunction than those with higher SUA/Cr levels, regardless of sex, age, poor blood sugar control, obesity, or diabetes duration (all interactions, p > 0.05) (Figure 3).
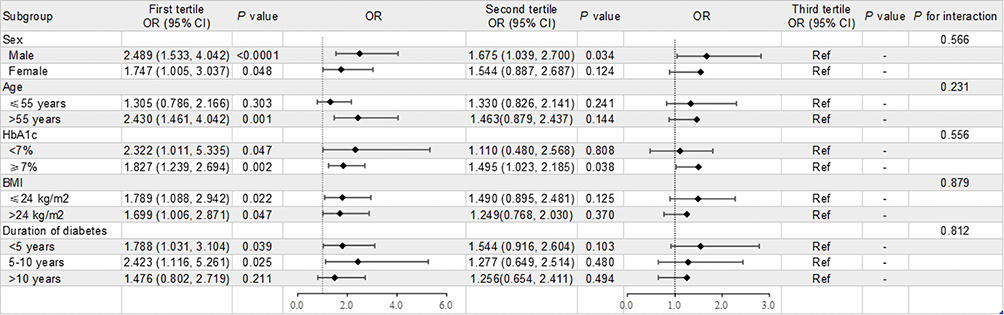 |
Figure 3 Subgroup analysis of the impact of SUA/Cr on sudomotor dysfunction. Abbreviations: HbA1c, glycated hemoglobin A1c; BMI, body mass index; OR, odds ratio; CI, confidence interval. Notes: p < 0.05. |
ROC Curve Analysis and Calibration Slope
ROC curve analysis was conducted to confirm the predictive values of SUA/Cr in detecting sudomotor dysfunction in patients with T2DM. The Youden’s Index, sensitivity, and specificity were 0.591, 0.686 and 0.549, respectively. The area under the curve (AUC) and its 95% confidence interval were 0.652 and 0.612–0.693, respectively (p < 0.001), as shown in Supplementary Figure S2. Systematic evaluation of the prediction model (calibration curves and multi-dimensional indicators) showed moderate discriminative ability (AUC = 0.652; Dxy = 0.310) and excellent calibration. The calibration curve approximated the ideal line (y=x), with a Brier score of 0.227, and ideal-calibrated intercept (0.000) and slope (1.000), reflecting high consistency between predicted and actual probabilities, as shown in Supplementary Figure S3.
Discussion
Diabetic peripheral neuropathy (DPN) is a severe complication of diabetes that significantly impacts patients’ quality of life, contributing to increased mortality rates, lower limb amputations, and painful neuropathic symptoms.3,20 Therefore, the early identification of DPN and its risk factors is crucial for slowing its progression. Sudomotor dysfunction, a reliable indicator for damage of small nerve fiber, is recognized as an early manifestation of DPN. Our current cross-sectional study found that the prevalence of sudomotor dysfunction in participants in the lowest tertiles of SUA/Cr levels was significantly higher than that in those in the highest tertiles. After adjusting for age, sex, BMI, and other potential confounders, the lowest tertile of SUA/Cr was independently associated with an increased risk of sudomotor dysfunction (adjusted OR=1.646, 95% CI: 1.088–2.489, p = 0.018).
Uric acid, a by-product purine metabolism, is primarily synthesized in the liver. Approximately 70% of uric acid is excreted by the kidneys, and the remaining 30% is excreted through the intestines.21 Because renal function significantly influences uric acid levels, it is a crucial factor to consider when investigating the association between SUA levels and peripheral neuropathy in patients with T2DM. Currently, the relationship between SUA and DPN remains controversial, with conflicting study results potentially attributable to variations in renal function among participants. However, the exact mechanism linking SUA and DPN is not fully understood.
Research has demonstrated that elevated SUA, which functions as a bioactive pro-inflammatory agent, may trigger a cascade of oxidative stress responses, ultimately contributing to the initiation and progression of inflammatory processes.15,16 Moreover, high SUA levels may decrease NO production, subsequently impairing endothelial cell function. This impairment results in local vascular contraction and reduced tissue perfusion, further exacerbating the occurrence and development of DPN.17 A nationwide multicenter cross-sectional study in Thailand involving 7511 adult patients with T2DM revealed that elevated serum uric acid levels were independently associated with DPN occurrence. Multivariable logistic regression analysis in their study revealed that patients with serum uric acid levels exceeding 7.3 mg/dL had a 1.54-fold higher risk of developing DPN compared to those with levels below 4.4 mg/dL (OR, 1.54; 95% CI, 1.02–2.32).22 However, the baseline characteristics of the participants indicated variations in the eGFR among patients with different serum uric acid levels. A limitation of this study was the exclusion of eGFR from the multiple regression model, which did not account for the potential influence of renal function as a confounding factor on the study’s conclusions. A case-control study conducted in Guilan, northern Iran, involving 280 patients with T2DM, revealed a significant increase in SUA levels among patients with DPN compared with the control group. Additionally, the baseline characteristics of the population indicated a notable elevation in creatinine levels among patients with DPN compared with the control group.23
Conversely, uric acid may also have a significant antioxidant function by inhibiting the formation of reactive oxygen species and peroxynitrite, thereby preventing the activation of inflammatory cells in the blood.11 Zhang et al reported that relatively low SUA levels might affect peripheral nerve function and serve as a risk factor for the development of DPN in patients with T2DM.24 However, their multiple linear regression analysis was adjusted only for glycated hemoglobin levels and did not account for the influence of renal function on SUA levels. A prospective study involving 525 patients with T2DM demonstrated a significant association between low SUA levels and DPN, even after adjusting for eGFR and other potentially confounding variables in a multivariate model.11 However, the association between SUA levels and DPN warrants further investigation. A cross-sectional study found no direct correlation between hyperuricemia and diabetic peripheral neuropathy.25
The variations in results from these studies may be attributed to the lack of adjustment for serum uric acid levels by renal function. To address this, our study introduced the standardization of renal function for uric acid to explore the correlation between standardized UA and DPN and revealed that SUA/Cr was independently associated with sudomotor dysfunction. This study provides a novel perspective on uric acid metabolism and diabetic neuropathy. Furthermore, we validated the consistency of the relationship between SUA/Cr and the risk of DPN across various subgroups categorized by age, sex, glycemic control, body mass index, and duration of diabetes through a comprehensive subgroup analysis. These results indicate that the association between SUA/Cr and sudomotor dysfunction does not vary by age, sex, glycemic control, body mass index, and duration of diabetes. Various studies have investigated the association between the SUA/Cr ratio and diabetic microvascular and macrovascular complications, but not diabetic neuropathy. To the best of our knowledge, this is the first study to explore the relationship between SUA/Cr ratio and sudomotor dysfunction. In this study, we evaluated diabetic neuropathy with sudomotor dysfunction, which represents damage to small nerve fiber function. The SUDOSCAN served as the primary method for detecting sudomotor dysfunction. This device assesses ESC by analyzing the chloride concentration in sweat from the hands and feet, providing a precise evaluation of potential impairment in sweat gland function.26 Its diagnostic performance is comparable to that of gold-standard skin biopsies.27 Detecting very early damage to diabetic neuropathy and identifying its risk factors, SUA/Cr, could eventually delay the progression of DPN and improve the prognosis of patients with DPN.
Despite its strengths, the current study has some limitations. First, as a cross-sectional study, it cannot establish causality, and further prospective studies are necessary to validate these conclusions. Second, our study was a single-center study involving only patients with type 2 diabetes who were hospitalized at this research center; therefore, caution should be exercised when generalizing these results to other populations. Third, we did not collect relevant data on the use of antidiabetic medications, and some studies suggested that metformin and sodium-glucose cotransporter-2 may affect SUA levels, potentially serving as confounding factors that could impact our results.28,29 Fourth, our primary assessment tool for sudomotor function, is designed to evaluate small fiber integrity and thus cannot fully capture large fiber neuropathy, which may restrict our ability to comprehensively assess peripheral nerve involvement. Finally, the absence of albuminuria data in our dataset limits our capacity to disentangle the potential role of early renal injury in the relationship between SUA/Cr and sudomotor dysfunction. Future studies incorporating comprehensive kidney function assessments—including albuminuria—are therefore warranted to further validate our findings.
Conclusion
In summary, our findings indicate that the SUA/Cr ratio is independently associated with sudomotor dysfunction, while standardized SUA levels are independently associated with DPN. Nevertheless, the relationship between the SUA/Cr ratio and sudomotor dysfunction requires confirmation via additional longitudinal studies. As hypothesis-generating findings, they also delineate key requirements for validation: employing prospective cohorts to establish temporality, adjusting for kidney function and urate-modifying medications, validating alternative ESC thresholds, and assessing generalizability beyond the single-center inpatient sample.
Abbreviations
DPN, Diabetic Peripheral Neuropathy; T2DM, Type 2 Diabetes Mellitus; ESC, Electrochemical Skin Conductance; HESC, Hand Electrochemical Skin Conductance; FESC, Foot Electrochemical Skin Conductance; SUA, Serum Uric Acid; Cr, Creatinine; SBP, Systolic Blood Pressure; DBP, Diastolic Blood Pressure; HbA1c, Glycated Hemoglobin A1c; eGFR, Estimated Glomerular Filtration rate; TC, Total cholesterol; TG, Triglycerides; HDL-C, High-density Lipoprotein Cholesterol; LDL-C, Low-density Lipoprotein Cholesterol; FPG, Fasting Plasma Glucose; BMI, Body Mass Index; OR, Odds Ratios; CI, Confidence Intervals.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Xubin Yang, upon reasonable request.
Ethics Approval
This study complied with the ethical principles of the Declaration of Helsinki for medical research involving human participants. The study was approved by the Ethics Committee of the Third Affiliated Hospital of Sun Yat-sen University ([2020]02-020-01).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Acknowledgments
We sincerely thank all of the participants involved in this study. We also thank the support of all the colleagues in the Department of Endocrine and Metabolic Diseases at the Third Affiliated Hospital of Sun Yat-sen University.
Author Contributions
Jie Peng: Writing - original draft, Software, Validation. Shangyan Liang: Writing - original draft, Methodology, Validation. Xiaoyun Tang: Writing – review & editing, Validation. XueYan Chen: Writing – review & editing, data curation. Huan Xu: Writing – review & editing, Formal analysis. Jia Liu: Writing – review & editing, Investigation. Wen Xu: Writing –review & editing, data curation, Project administration. Xing Shui: Writing – review & editing, Methodology, data curation, Supervision. Xubin Yang: Writing – review & editing, Conceptualization, Funding acquisition. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Natural Science Foundation of Guangdong Province[2018A030313915]; Medical Scientific Research Foundation of Guangdong Province of China[A20182867].
Disclosure
The authors declare that there is no conflict of interest.
References
1. Yang K, Wang Y, Li Y-W, et al. Progress in the treatment of diabetic peripheral neuropathy. Biomed Pharmacother. 2022:148. doi:10.1016/j.biopha.2022.112717
2. Hicks CW, Selvin E. Epidemiology of peripheral neuropathy and lower extremity disease in diabetes. Curr Diab Rep. 2019;19(10). doi:10.1007/s11892-019-1212-8
3. Selvarajah D, Kar D, Khunti K, et al. Diabetic peripheral neuropathy: advances in diagnosis and strategies for screening and early intervention. Lancet Diabetes Endocrinol. 2019;7(12):938–10. doi:10.1016/s2213-8587(19)30081-6
4. Zhang W, Chen L, Lou M. Association of elevated serum uric acid with nerve conduction function and peripheral neuropathy stratified by gender and age in type 2 diabetes patients. Brain Sciences. 2022;12(12):1704. doi:10.3390/brainsci12121704
5. Akbar M, Wandy A, Soraya GV, Goysal Y, Lotisna M, Basri MI. Sudomotor dysfunction in diabetic peripheral neuropathy (DPN) and its testing modalities: a literature review. Heliyon. 2023;9(7):e18184. doi:10.1016/j.heliyon.2023.e18184
6. Lacomis D. Small‐fiber neuropathy. Muscle Nerve. 2002;26(2):173–188. doi:10.1002/mus.10181
7. Russell JW, Zilliox LA. Diabetic neuropathies. Am Acad Neurol. 2014;20(5):1226–1240.
8. Kiani J, A. Habibi, Habibi Z, et al. Association between serum uric acid level and diabetic peripheral neuropathy (A case control study). Caspian J Intern Med. 2014;5(1):17–21.
9. Papanas N, Katsiki N, Papatheodorou K, et al. Peripheral neuropathy is associated with increased serum levels of uric acid in type 2 diabetes mellitus. Angiology. 2011;62(4):291–295. doi:10.1177/0003319710394164
10. Jiang T-N, Li Y-F, Huo L-L, et al. Association between serum uric acid and large-nerve fiber dysfunction in type 2 diabetes. Chin Med J. 2019;132(9):1015–1022. doi:10.1097/cm9.0000000000000223
11. Zhuang Y, Huang H, Hu X, Zhang J, Cai Q. Serum uric acid and diabetic peripheral neuropathy: a double-edged sword. Acta Neurologica Belgica. 2022;123(3):857–863. doi:10.1007/s13760-022-01978-1
12. Gu L, Huang L, Wu H, Lou Q, Bian R. Serum uric acid to creatinine ratio: a predictor of incident chronic kidney disease in type 2 diabetes mellitus patients with preserved kidney function. Diab Vasc Dis Res. 2017;14(3):221–225. doi:10.1177/1479164116680318
13. Li M, Gu L, Yang J, Lou Q. Serum uric acid to creatinine ratio correlates with β‐cell function in type 2 diabetes. Diabetes Metab Res Rev. 2018;34(5). doi:10.1002/dmrr.3001
14. Xing Y, Chen J, Liu J, Song G, Ma H. Relationship between serum uric acid-to-creatinine ratio and the risk of metabolic-associated fatty liver disease in patients with type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2022;15:257–267. doi:10.2147/dmso.S350468
15. Liu L, Jiang S, Liu X. Inflammatory response and oxidative stress as mechanism of reducing hyperuricemia of Gardenia jasminoides - Poria cocos with network pharmacology. Oxid Med Cell Longev. 2021;2021. doi:10.1155/2021/8031319
16. Sautin YY, Johnson RJ. Uric acid: the oxidant-antioxidant paradox. Nucleosides Nucleotides Nucleic Acids. 2008;27(6–7):608–619. doi:10.1080/15257770802138558
17. Zhang Y, Tang Z, Tong L, Wang Y, Li L. Serum uric acid and risk of diabetic neuropathy: a genetic correlation and mendelian randomization study. Front Endocrinol. 2023;14. doi:10.3389/fendo.2023.1277984
18. Alberti KGMM, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15:539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
19. Casellini CM, Parson HK, Richardson MS, Nevoret ML, Vinik AI. Sudoscan, a noninvasive tool for detecting diabetic small fiber neuropathy and autonomic dysfunction. Diabet Technol Ther. 2013;15(11):948–953. doi:10.1089/dia.2013.0129
20. Sloan G, Selvarajah D, Tesfaye S. Pathogenesis, diagnosis and clinical management of diabetic sensorimotor peripheral neuropathy. Nat Rev Endocrinol. 2021;17(7):400–420. doi:10.1038/s41574-021-00496-z
21. Yanai H, Adachi H, Hakoshima M, Katsuyama H. Molecular biological and clinical understanding of the pathophysiology and treatments of hyperuricemia and its association with metabolic syndrome, cardiovascular diseases and chronic kidney disease. Int J Mol Sci. 2021;22(17):9221. doi:10.3390/ijms22179221
22. Kaewput W, Thongprayoon C, Rangsin R, et al. The association between serum uric acid and peripheral neuropathy in patients with type 2 diabetes mellitus: a multicenter nationwide crosssectional study. Korean J Fam Med. 2020;41(3):189–194. doi:10.4082/kjfm.18.0205
23. Fayazi HS, Yaseri M, Mortazavi SS, Sharifhassan Z, Assadinia A-S. The relation between serum uric acid levels and diabetic peripheral neuropathy in type 2 diabetes in Guilan, north of Iran. BMC Endocr Disord. 2022;22(1). doi:10.1186/s12902-022-00952-5
24. Zhang H, Vladmir C, Zhang Z, et al. Serum uric acid levels are related to diabetic peripheral neuropathy, especially for motor conduction velocity of tibial nerve in type 2 diabetes mellitus patients. J Diabetes Res. 2023;2023:1–7. doi:10.1155/2023/3060013
25. Gaita L, Timar R, Lupascu N, et al. The impact of hyperuricemia on cardiometabolic risk factors in patients with diabetes mellitus: a cross-sectional study. Diabetes Metab Syndr Obes. 2019;12:2003–2010. doi:10.2147/dmso.S222570
26. Mayaudon H, Miloche PO, Bauduceau B. A new simple method for assessing sudomotor function: relevance in type 2 diabetes. Diabet Metabol. 2010;36(6):450–454. doi:10.1016/j.diabet.2010.05.004
27. Gordon Smith A, Lessard M, Reyna S, Doudova M, Singleton JR. The diagnostic utility of Sudoscan for distal symmetric peripheral neuropathy. J Diabetes Complications. 2014;28(4):511–516. doi:10.1016/j.jdiacomp.2014.02.013
28. Hussain A, Latiwesh OB, Ali F, Younis MYG, Alammari JA. Effects of body mass index, glycemic control, and hypoglycemic drugs on serum uric acid levels in type 2 diabetic patients. Cureus. 2018. doi:10.7759/cureus.3158
29. Hussain M, Elahi A, Hussain A, et al. Sodium-glucose cotransporter-2 (SGLT-2) attenuates serum uric acid (SUA) level in patients with type 2 diabetes. J Diabetes Res. 2021;2021:1–5. doi:10.1155/2021/9973862
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relationship Between Fasting C-Peptide to Diabetes Duration Ratio (FCP/DD) and Diabetic Peripheral Neuropathy
Fu Y, Xing Y, Yang L, Liu J, Ma H
Diabetes, Metabolic Syndrome and Obesity 2024, 17:4469-4477
Published Date: 26 November 2024