Back to Journals » OncoTargets and Therapy » Volume 13
Serum Platelet-Derived Growth Factor Is Significantly Lower in Patients with Lung Cancer and Continued to Decrease After Platinum-Based Chemotherapy
Authors Ma R, Yang Q, Cao S, Liu S, Cao H, Xu H, Wu J, Feng J ![]()
Received 19 November 2019
Accepted for publication 13 February 2020
Published 4 March 2020 Volume 2020:13 Pages 1883—1892
DOI https://doi.org/10.2147/OTT.S239252
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leo Jen-Liang Su
Rong Ma,1,* Qing Yang,2,* Shengya Cao,2 Siwen Liu,1 Haixia Cao,1 Heng Xu,3 Jianzhong Wu,1 Jifeng Feng1
1Research Center for Clinical Oncology, Jiangsu Cancer Hospital and Jiangsu Institute of Cancer Research and Nanjing Medical University Affiliated Cancer Hospital, Nanjing, Jiangsu 210000, People’s Republic of China; 2Xuzhou Cancer Hospital, Xuzhou, Jiangsu 221000, People’s Republic of China; 3Laboratory of Pharmaceutical Chemistry, Jiangsu Province Institute of Materia Medica, Nanjing Tech University, Nanjing, Jiangsu 210000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianzhong Wu; Jifeng Feng
Research Center for Clinical Oncology, Jiangsu Cancer Hospital and Jiangsu Institute of Cancer Research and Nanjing Medical University Affiliated Cancer Hospital, No. 7 Building, 42 BaiZiTing Road, Nanjing, Jiangsu 210000, People’s Republic of China
Email [email protected]; [email protected]
Objective: This study aimed to investigate the diagnosis and prediction of serum platelet-derived growth factor (PDGF) level in patients with lung cancer (LC).
Methods: Serum concentrations of PDGF-AA and PDGF-AB/BB were determined via Luminex assay in 210 patients with non-small cell lung cancer (NSCLC), 33 patients with small cell lung cancer (SCLC), and 168 healthy controls.
Results: The serum levels of PDGF-AA and PDGF-AB/BB were lower in patients with NSCLC (P < 0.05) and SCLC (P < 0.05), compared to healthy controls. The concentration of PDGF-AA or PDGF-AB/BB continued to markedly decrease in NSCLC after therapy with platinum-based chemotherapy (P < 0.05). The median survival times were 29 and 38 months in patients with NSCLC who received PDGF-AA < 30 ng/mL and PDGF-AA ≥ 30 ng/mL (P = 0.0078), and 26 and 38 months in patients with NSCLC who received PDGF-AB/BB < 42 ng/mL and PDGF-AB/BB ≥ 42 ng/mL (P = 0.0001), respectively. At the individual protein level, PDGF-AA and PDGF-AB/BB had better diagnostic values for NSCLC (AUC = 0.905, AUC = 0.922, respectively).
Conclusion: Serum PDGF may be a potential biomarker for diagnosis of patients with NSCLC and SCLC. However, the prognostic value of serum PDGF in patients with NSCLC harboring mutations and different therapies requires additional investigation.
Keywords: PDGF-AA, PDGF-AB/BB, chemotherapy, response, lung cancer
Introduction
Lung cancer (LC) is a type of malignancy with high mortality and morbidity worldwide,1 with a low five-year survival rate (approximately 13%).2 In addition, the main cause of mortality (up to 85% of LC) is due to non-small cell LC (NSCLC). Among patients with LC who were previously treated via surgery, chemotherapy, and radiotherapy, those who underwent surgery had significant improvement in prognosis at the early stage of NSCLC.3 However, genetic and epigenetic changes to the cellular genome that led to LC progression were found, such as the epidermal growth factor receptor (EGFR) gene, which was demonstrated to activate mutations in approximately 10% to 40% of patients with NSCLC.4 Therefore, biomarkers related to efficacy and prognosis of the disease should be identified for patients with LC who may benefit from chemotherapy regimens.5,6 Considering disease evolution and treatment strategy improvements, the search for better biomarkers should be continued for the diagnosis, monitoring, and prognosis of patients with LC.
Platelet-derived growth factor is an important factor that promotes the cell proliferation and transformation of several types of cells and stimulates tumor angiogenesis through mutual interactions with other pro-angiogenic factors.7,8 Platelet-derived growth factor comprises two linked chains that can be assembled as a heterodimer or homodimer,9 known as PDGF-AA and PDGF-AB/BB according to the linked chains involved. The recruitment of stroma associated with cancer that produces angiogenic factors, and pericytes associated with microvasculature stabilization, was affected by PDGF-AA and PDGF-BB, respectively.10,11 Several studies have attempted to evaluate serum PDGF level to determine significant diagnostic or prognostic values of cancer, including breast cancer,12 ovarian cancer,13 and colorectal cancer.14 However, paradoxical results were found in the literature.15,16 Only a few studies focused on PDGF, particularly those who considered serum PDGF-AA or PDGF-AB/BB level in patients with LC.
In this study, the serum concentrations of PDGF-AA and PDGF-AB/BB were measured in a large panel of patients with LC and in healthy individuals. In addition, the relationship between PDGF-AA and PDGF-AB/BB was investigated, as well as their clinicopathological variables and curative effects on patients with NSCLC. Furthermore, the predictive values of serum PDGF-AA and PDGF-AB/BB levels were also estimated in patients with NSCLC following platinum-based chemotherapy.
Materials and Methods
Serum Samples
The current study collected blood samples from 210 patients with NSCLC with a mean age of 61.0 years (standard deviation, 11.3 years) and from 33 patients with SCLC with a mean age of 63.2 years (standard deviation, 9.5 years), at Jiangsu Cancer Hospital from October 2011 to December 2012. Moreover, 168 healthy controls from Yian Medical Examination Center in Nanjing were included. These patients were enrolled in a research protocol of the Research Center for Clinical Oncology, approved by the Biomedical Research Ethics Committee of Jiangsu Cancer Hospital. All participants signed written informed consent. This study was conducted in accordance with the Declaration of Helsinki. Pre-treatment (surgery and/or chemotherapy) peripheral blood samples were collected. Furthermore, blood samples from patients treated with platinum-based chemotherapy were also collected at three different intervals (ie, the first, second, and third-months post-treatment). The specimens from patients with NSCLC were divided into a training group (106 patients and 83 healthy controls for screening of diagnostic value) and a verification group (104 patients and 85 healthy controls for identification of diagnostic value) (Supplementary Table 1). Samples were collected from patients with NSCLC, centrifuged at 4°C for 10 min, and stored at –80°C until use. The selection criteria for patients with LC were consistent with the above description.17
Luminex Assays
Luminex kits for human neurodegenerative disease panel three (PDGF-AA and PDGF-AB/BB) were acquired from Millipore (cat. no. HNDG3MAG-36K) (Millipore Inc Billerica, MA, USA) and performed according to manufacturer instructions. Pre-treatment of serum samples and parameters in a FLEXMAP3D (Luminex, TX, USA) were similar to previous reports.18 Median fluorescence intensity (MFI) was determined and used to estimate serum concentration of PDGF-AA and PDGF-AB/BB. Protein concentrations were calculated according to the standard curve using a known concentration.
Statistical Analysis
The differences between the two groups were examined, and a t-test or Mann–Whitney test was used to compare the median values between the patient groups. The comparisons (≥3 groups) were performed through one-way analysis of variance followed by pair-wise comparisons using Bonferroni posthoc testing. P < 0.05 was considered statistically significant. Diagnostic power was assessed using the receiver operating characteristic (ROC), and the area under curve (AUC), sensitivity and specificity were calculated. Positive predictive value = [true positive/(true positive+false positive) * 100%] and negative predictive value = [true negative/(true negative+false negative) * 100%]. The overall survival (OS) was calculated as the interval from the time of diagnosis to death from any cause and illustrated by survival plots using GraphPad Prism v.5 software.
Results
Serum PDGF Levels in Patients with LC
Serum PDGF-AA and PDGF-AB/BB were measured in 168 healthy controls and 243 pre-treated patients with LC, including 210 NSCLC and 33 SCLC. The serum levels of PDGF-AA were 41.5, 35.1, and 53.0 ng/mL in the NSCLC, SCLC, and healthy control groups, respectively (Figure 1A). Contrastingly, the serum concentrations of PDGF-AB/BB were 97.4, 57.1, and 50.8 ng/mL in the control, NSCLC, and SCLC groups, respectively (Figure 1B).
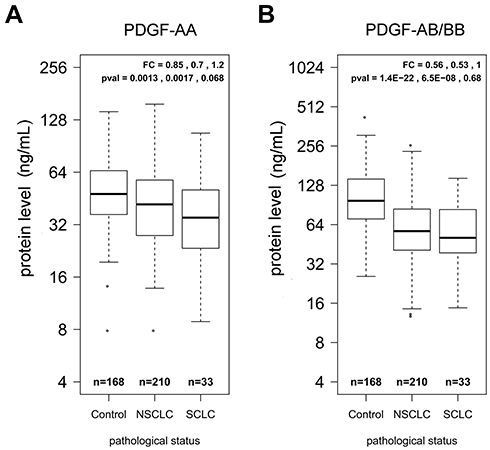 |
Figure 1 Boxplots of serum PDGF-AA and PDGF-AB/BB in healthy controls and patients. (A) The median value of PDGF-AA concentration in three different groups. (B) The median value of PDGF-AB/BB concentration in three different groups. Fold change (FC) and p-values are listed in the order of control vs SCLC, control vs NSCLC, and SCLC vs NSCLC. |
Median concentrations of serum PDGF-AA and PDGF-AB/BB were conspicuously lower in patients with NSCLC and SCLC than among those in healthy controls (P < 0.01) (Figure 1). Compared to healthy controls, the mean serum concentrations of PDGF-AB/BB decreased approximately two-fold in patients with NSCLC (P = 1.4E-22) and SCLC (P = 6.5E-8) (Figure 1B). No significant difference was observed in the serum concentration of PDGF-AA or PDGF-AB/BB between patients with NSCLC and SCLC; however, PDGF-AA or PDGF-AB/BB levels in SCLC were even lower than those in NSCLC (P > 0.05).
Logistic regressions were performed using the PDGF-AA and PDGF-AB/BB concentrations as a dependent variable, whereas sex and age were used as covariates. After adjusting by age and sex, PDGF-AA was shown to be significantly associated with NSCLC (OR = 0.987, P = 0.002677), but not with SCLC (OR = 0.980, P = 0.159) (Supplementary Table 2–1). However, PDGF-AB/BB was significantly associated with both NSCLC (OR = 0.977, P = 1.66E-14) and SCLC (OR = 0.966, P = 0.000756) (Supplementary Table 2–2)
Relation Between Serum PDGF and Clinicopathological Characteristics
In individuals with LC, a sufficient number of patients were examined for PDGF-AA and PDGF-AB/BB differences according to various clinicopathological characteristics (Table 1). Logistic regressions of joint effects for clinical events between serum PDGF and 243 patients with LC were analyzed in Table 2. As shown in Table 1, the serum concentration of PDGF-AA was lower in stage IV than in stage I to stage III patients for NSCLC (P < 0.05). However, serum PDGF-AB/BB levels were prominently lower in stages I and II than in stages III and IV patients with NSCLC (P < 0.05). There were no conspicuous differences in the PDGF-AA or PDGF-AB/BB concentration between limited and extensive patients with SCLC (P > 0.05). As shown in Table 2, the concentration of PDGF-AA and PDGF-AB/BB played important roles in joint effects between PDGF and clinical events of LC patients.
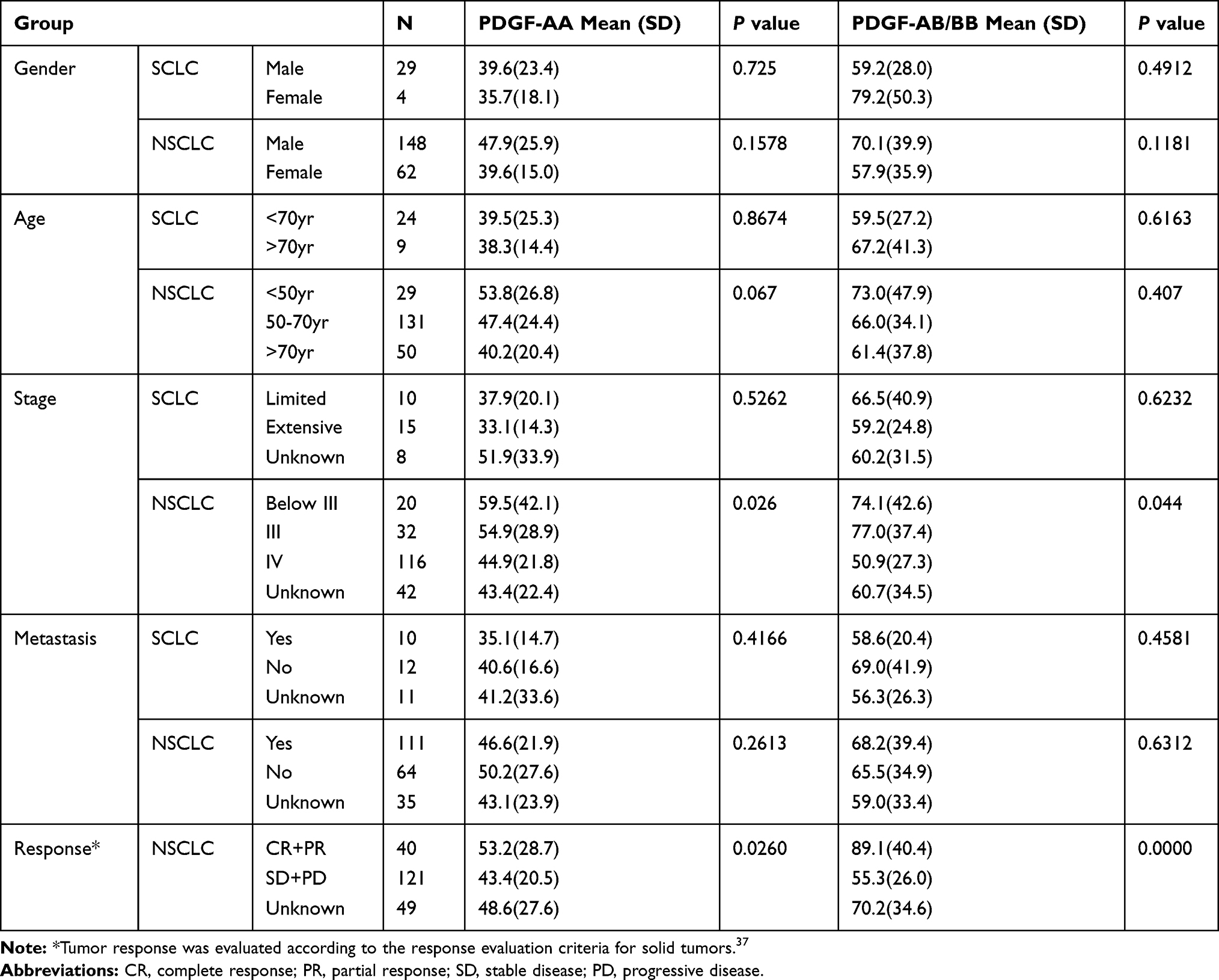 |
Table 1 Relation of Serum PDGF-AA and PDGF-AB/BB to Clinicopathological Characteristics of 243 Patients with Lung Cancer (Concentration Unit: Ng/mL) |
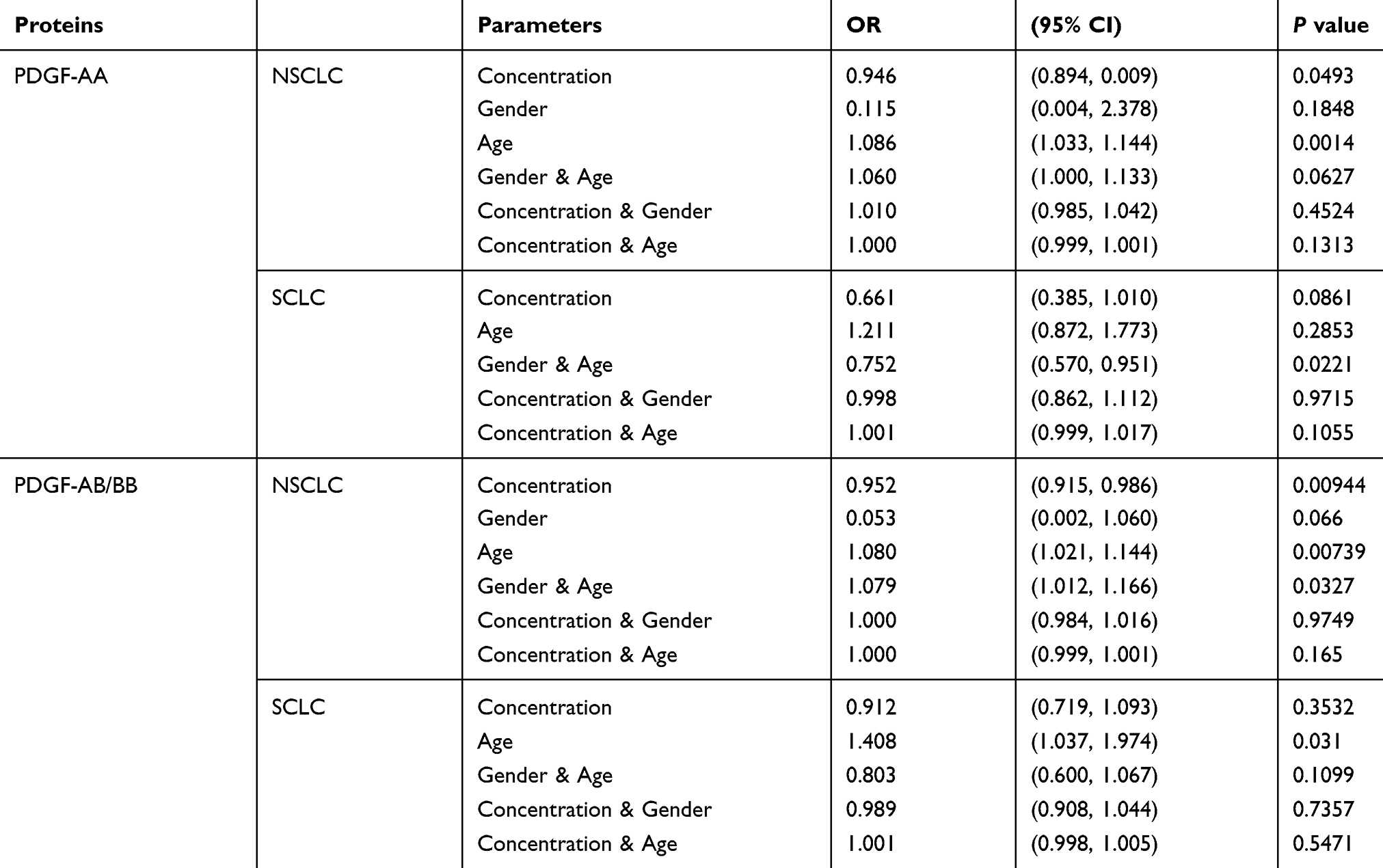 |
Table 2 Logistic Regression Analysis of Joint Effect for Clinical Events Between Serum PDGF and 243 Patients with Lung Cancer |
As demonstrated in Figure 2A, a significantly lower PDGF-AA level was observed in patients with NSCLC with metastasis (P < 0.01), whereas serum PDGF-AA level in patients with NSCLC with non-metastasis was similar to the healthy control (P > 0.05). However, the PDGF-AB/BB serum levels in NSCLC patients with non-metastasis and metastasis were significantly lower than those in the healthy control (P < 0.01) (Figure 2B).
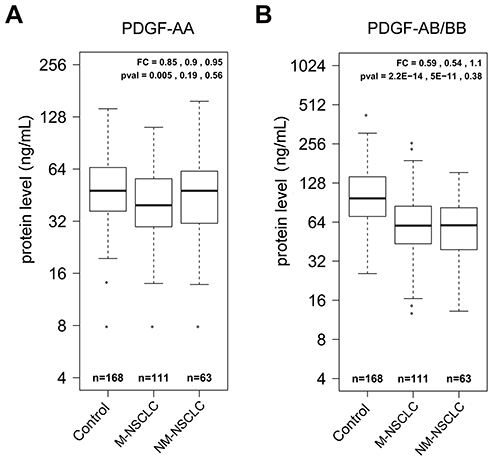 |
Figure 2 Boxplots of serum PDGF-AA and PDGF-AB/BB in healthy controls and NSCLC patients with metastasis (M-NSCLC) and non-metastasis (NM-NSCLC). (A) The median value of PDGF-AA concentration in three different groups. (B) The median value of PDGF-AB/BB concentration in three different groups. Fold change (FC) and p-values are listed in the order of control vs M-NSCLC, control vs NM-NSCLC, and M-NSCLC vs NM-NSCLC. |
PDGF Sequentially Decreased After Therapy in Patients with NSCLC
Serum samples were available from 78 patients with NSCLC treated with different chemotherapeutics at three different intervals (ie, the first, second, and third-months post-treatment), all of whom received platinum-based chemotherapies with other drugs. Compared to pre-treatment, PDGF-AA levels significantly gradually decreased (P < 0.01) in NSCLS patient sera obtained within the first, second, and third month of treatment, with 0.74, 0.57, and 0.55 post/pretreatment fold change (FC), respectively (Figure 3A). Serum PDGF-AB/BB levels also showed similar decrease in patients with NSCLC within the first, second, and third month of treatment with platinum-based chemotherapies (P < 0.01); however, there was no significant difference at the first month following treatment (P = 0.14) (Figure 4A).
 |
Figure 3 Influence of therapeutic regimens on serum PDGF-AA levels. (A) Boxplots of PDGF-AA in serum samples from pre-treatment (pre) and 1 month, 2-months and 3-months post-treatment (pos). (B) Longitudinal serum PDGF-AA in individual patients. Serum concentration of PDGF-AA is plotted on the Y-axis and sampling time after therapy is plotted on the X-axis. Each dot represents a sample and different time points for the same patient is linked by a line. All: all patients with longitudinal samples are included. PEM: patients treated with the PEM regimen are included. Taxane: patients with the taxane regimen are included. Other: patients treated with other regimens are plotted. PEM represents treatment with platinum plus PEM (Pemetrexed) combined with platinum (DDP, LBP, CBP or NDP); taxane represents platinum plus taxane (PTX, TAX, Abraxane, TXT, DOC) combined with platinum (DDP, LBP, CBP or NDP). (C) Mean change in the PEM, taxane and other treatment regimens relative to the pre-treatment value. The fold change (FC) between post-treatment values and pre-treatment values are calculated and the mean fold increase in each treatment group was plotted for three different time intervals (1month, 2-months and 3-months). |
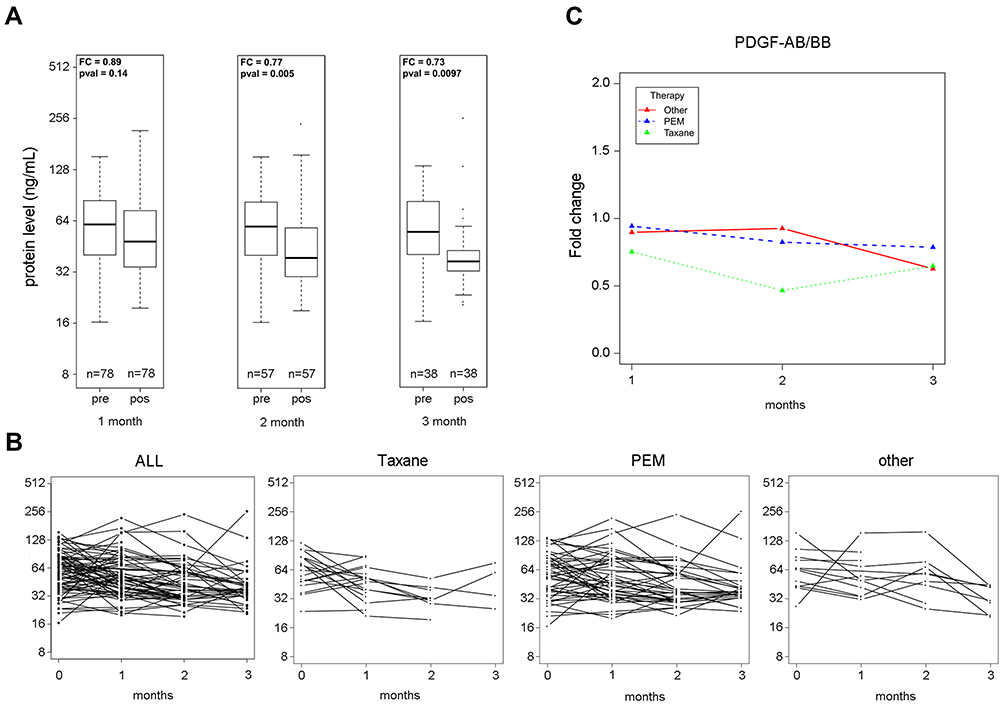 |
Figure 4 Influence of therapeutic regimens on serum PDGF-AB/BB levels. (A) Boxplots of PDGF-AB/BB in serum samples from pre-treatment (pre) and 1 month, 2-months and 3-months post-treatment (pos). (B) Longitudinal serum PDGF-AB/BB in individual patients. (C) Mean change in the PEM, taxane and other treatment regimens relative to the pre-treatment value. |
Patients with NSCLC were divided into the taxane group (platinum plus taxane), pemetrexed group (platinum plus PEM), and a third other group (platinum plus various other drugs), based on different therapy programs. The longitudinal change of serum PDGF-AA and PDGF-AB/BB for each individual is plotted in Figures 3B and Figure 4B. The data indicated that PDGF-AA and PDGF-AB/BB concentrations continuously declined in most individuals at the second and the third-months post-treatment among the three groups. The PDGF-AA or PDGF-AB/BB concentrations increased quickly within the first month for some individuals; however, PDGF-AA or PDGF-AB/BB concentrations remained relatively high in a few individuals at the third month of treatment among the three different treatment regimens. The degree of decline in PDGF-AA levels in NSCLC patients treated with the taxane regimen was more severe than for those enrolled in the PEM regimen at the first and the second-months post-treatment (P = 0.004 and P = 0.006, respectively; Figure 3C). Similarly, patients treated with the taxane regimen showed the highest degree of decline in PDGF-AB/BB levels at the first, second and third-months post-treatment among the three groups (P < 0.01; Figure 4C).
Diagnostic and Predictive Value of PDGF in Patients with NSCLC
The clinical data of patients with NSCLC and the healthy group are summarized in Supplementary Table 1. Area under curve values were inspected for the ability of PDGF-AA and PDGF-AB/BB protein to distinguish patients from the healthy controls, by using these clinical data except NSCLC patients with unknown date. At the individual protein level, PDGF-AA and PDGF-AB/BB had better diagnostic value for NSCLC (AUC = 0.905, AUC = 0.922, respectively) (Figure 5A). The combination model with PDGF-AA and PDGF-AB/BB had an excellent diagnostic potential for NSCLC (AUC = 0.923). Meanwhile, the diagnostic sensitivity and specificity were verified to be 81.0% and 92.9%, respectively. Positive predictive value was 93.4% and negative predictive value was 79.8% in the verification group (Table 3).
 |
Table 3 Diagnostic Value of PDGF-AA and PDGF-AB/BB for NSCLC in Verification Group |
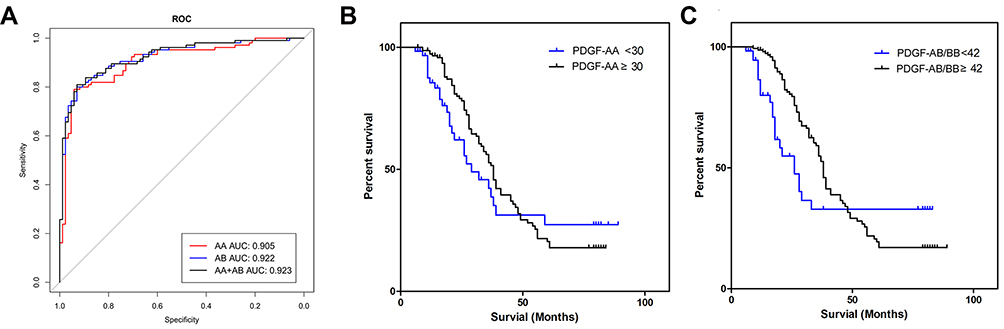 |
Figure 5 Diagnostic and predictive value of PDGF in patients with NSCLC. (A) ROC curves that evaluate the ability to distinguish LC patients from healthy controls. All: PDGF-AA and PDGF-AB/BB. (B) Overall survival with high (≥ 30 ng/mL) and low (< 30 ng/mL) treatment serum PDGF-AA levels. Hazard ratio (high vs low) =1.260 (95% CI, 0.787–2.017). (C) Overall survival with high (≥ 42 ng/mL) and low (< 42 ng/mL) treatment serum PDGF-AB/BB levels. Hazard ratio (high vs low) =1.489 (95% CI, 0.889–2.493). Abbreviation: CI, confidence interval. |
Table 1 shows 40 patients (19.0%) with complete response (CR) or partial response (PR) and 121 patients (57.6%) with stable disease (SD) or progressive disease (PD). The level of PDGF-AA was significantly lower in NSCLC patients with SD + PD than for CR + PR (P < 0.05). The PDGF-AB/BB concentration was most notably lower in NSCLC patients with SD + PD than for CR + PR (P < 0.001). As of January 2019, 22 patients with NSCLC (10.5%) had survived for 72 months. The three-year and five-year survival rates were 28.1% (59/210) and 12.4% (26/210) in patients with NSCLC, respectively. Furthermore, 13 patients with NSCLC (6.2%) underwent targeted therapy or antibody therapy, such as gefitinib, icotinib, and avastin. Following platinum-based chemotherapy, the median values of PDGF-AA and PDGF-AB/BB were approximately 30 ng/mL and 42 ng/mL in NSCLC patients, respectively. Therefore, among the variables evaluated, PDGF-AA < 30 ng/mL and PDGF-AB/BB < 42 ng/mL were determined as independent factors for OS. The median survival times were 29 and 38 months in patients with NSCLC with PDGF-AA < 30 ng/mL and PDGF-AA ≥ 30 ng/mL, respectively (P = 0.0078) (Figure 5B). Moreover, the median survival times were 26 and 38 months in patients with NSCLC with PDGF-AB/BB < 42 ng/mL and PDGF-AB/BB ≥ 42 ng/mL, respectively (P = 0.0001) (Figure 5C). Low PDGF-AA (< 30 ng/mL) or PDGF-AB/BB (< 42 ng/mL) levels tended to be associated with poor prognosis (Figure 5B and C). NSCLC patients with lower PDGF-AA (< 30 ng/mL) or PDGF-AB/BB (< 42 ng/mL) had a shorter life span by 9 to 12 months in terms of OS vs those with higher levels.
Discussion
In 2018, LC is still the malignant tumor with the highest morbidity (11.6%) and mortality (18.4%) worldwide.19 It is critical to identify biomarkers for early diagnosis to assist in the monitoring of treatment and to effect good prognosis for patients with LC. Early detection and therapy has been improved; however, prognosis remains poor for patients with LC.20 In the present study, the levels of PDGF-AA and PDGF-AB/BB were analyzed in a large cohort of patients with LC and healthy controls, which may be of great clinical significance for NSCLC and SCLC. Both serum PDGF-AA and PDGF-AB/BB in pre-treatment samples from patients with NSCLC or SCLC were significantly lower than that of the healthy controls (P < 0.01). In particular, the degree of decrease was severe lower in serum PDGF-AB/BB than in PDGF-AA. The combination model has the best diagnostic value for NSCLC (AUC = 0.923), while PDGF-AA and PDGF-AB/BB also possess good AUC (0.905 and 0.922, respectively), suggesting PDGF is a potential biomarker for NSCLC diagnosis.
Compared to normal or benign tumors, serum levels of PDGF-AA and/or PDGF-BB were found to be elevated in breast,12 colorectal,14 and esophageal cancer;21 however, various studies have yielded inconsistent findings.15,16 The reasons for these controversial findings remained unclear and may be multifactorial. First, PDGF concentrations may be inconsistent among different immunological assays. Considering different antigenic determinants in protein conformation, it is possible that different reagents do not measure the same determinants of PDGF-AA and/or PDGF-AA/BB protein. Second, horizontal data provided more solid evidence in the present study, based on the largest sample size for both patients and controls. Many types of LC biomarkers were evaluated using the same batch of patients and controls in the same library, including DKK1, CEA, CYFRA21.1, OPN, and SAA.17,18 Elevated serum CEA, CYFRA21.1, OPN and SAA levels, and depressed serum DKK1 levels have been found in the same library for LC. Therefore, findings in which the PDGF-AA and PDGF-AB/BB concentrations were shown to decrease in LC may be more reliable. Finally, contradictory results for PDGF-AA and PDGF-AB/BB concentrations may be related to PDGF function. The angiogenic effect of PDGF in tumor angiogenesis is increasingly emphasized.22 PDGF-AA affects the recruitment of tumor-associated stroma which produces angiogenic factors.10 PDGF-BB promotes pericyte recruitment and microvasculature stabilization,11,23 which makes it an important component in angiogenesis.
PDGF-AA and PDGF-BB belong to the PDGF family, which can combine with corresponding receptors (PDGFR) on the cell membrane to exert biological effects.24
PDGF-AB can induce vascular endothelial cells that express PDGFR-α, which will eventually express angiogenic factors (such as VEGF) through the PDGFR-α pathway and regulate the activity of microvascular endothelial cells.25 Furthermore, PDGF-AB can also combine with PDGFR-ββ to promote tumor angiogenesis.26 PDGF-AA and PDGF-BBy in the PDGF family are secreted in the form of homodimers or heterodimers. Subsequently, these substances combine with three types of PDGF receptors, which play an autocrine or paracrine role in the tumor and its vascular growth and development.27 In the present study, the results indicated that the PDGF-AA and PDGF-AB/BB concentrations decreased in both NSCLC and SCLC. It is possible that after PDGF-AA or PDGF-AB/BB combined with PDGF receptors, the PDGF and PDGFR compounds were insensitive to immunological reaction that specifically detected PDGF-AA or PDGF-AB/BB. As one of angiogenic factors, PDGF plays a critical role in tumorigenesis, tumor progression, and metastasis. PDGF released by tumor cells can induce the proliferation and migration of vascular endothelial cells, smooth muscle cells and tumor cells, and inhibit their apoptosis. In addition, PDGF can avoid the killing effect of chemotherapy drugs by increasing tissue gap pressure, preventing liquid convection of capillaries, and reducing the uptake of tumor cells against tumor drugs. Drained PDGF-AA or PDGF-AB/BB inevitably led to low PDGF-AA or PDGF-AB/BB concentrations in patients with LC. A possible reason for this was that only a few dissociative PDGF-AA or PDGF-AB/BB were detected in LC patient serum except PDGF and PDGFR conjugate. According to previous reports, PDGFR level clearly increased in breast cancer and prostate cancer.28,29
The levels of most biomarkers are generally significantly increased in NSCLC prior to treatment; however, these biomarkers markedly decreased after treatment. A small number of biomarkers significantly decreased in NSCLC before treatment; however, they were observably increased after treatment. In the present study, in contrast to the tendency of most biomarkers, the PDGF-AA and PDGF-AB/BB concentrations continued to decrease in NSCLC after therapy at month one, two, or three. However, according to longitudinal serum PDGF-AA or PDGF-AB/BB in individual patients, the PDGF-AA or PDGF-AB/BB levels among the minority of individual patients increased after treatment at month one, two, or three. Nonetheless, most patients still appeared to have received no benefit from the therapy. One possible reason for this is that treatments with platinum-based chemotherapy were not the optimal strategy for NSCLC therapy. In the past few decades, cytotoxic chemotherapy has only slightly improved the survival of patients with metastatic NSCLC. One of the important improvements in NSCLC treatment has been the discovery of specific genetic alterations that have dominated disease development.30 The activating mutation in the gene encoding EGFR has been an important factor for precision therapy, such as deletion in exon 19 and point mutation L858R in exon 21.31 In addition, the most common mutations occur in the Kirsten rat sarcoma virus (KRAS, 24% of cases), anaplastic lymphoma kinase (ALK, 3% of cases), v-raf murine sarcoma viral oncogene homolog B1 (BRAF, 2% of cases), and c-ros oncogene 1 (ROS1, 1% to 2% of cases) in patients with NSCLC.32–35
More importantly, PDGF-AA and PDGF-AB/BB concentrations were associated with survival in patients with NSCLC; however, these findings are controversial. While the expression of PDGF-AA has already been proven to be correlated with poor prognosis in other tumors,36 PDGF-BB level is negatively correlated with the survival ratio of patients.16 In the present study, lower concentrations of PDGF-AA (< 30 ng/mL) or PDGF-AB/BB (< 42 ng/mL) indicated shorter OS, which suggested PDGF-AA or PDGF-AB/BB to be associated with predictive values in patients with NSCLC. Although PDGF-AA and PDGF-AB/BB concentrations continued to decrease in most patients with NSCLC, 22 patients with NSCLC (10.5%) showed survival > 72 months. It is possible that some patients with NSCLC below stage Ⅲ may benefit from platinum-based chemotherapy. In addition, targeted therapy and antibody therapy, such as gefitinib, icotinib, and avastin, can potentially improve the survival time of NSCLC patients with gene mutations. The discrepancy between results in the present study and previous research regarding efficacy evaluation and survival may be partially due to differences in the determination assays, individual differences, population heterogeneity, and sample size. The limitations of the present study should also be considered, including its retrospective character. Therefore, a large-scale prospective analysis is needed to demonstrate diagnostic value of PDGF-AA or PDGF-AB/BB as a biomarker for NSCLC patients with mutations and receiving different therapies.
Conclusion
Serum PDGF may be a potential biomarker for the diagnosis of patients with NSCLC and SCLC. The combination model with PDGF-AA and PDGF-AB/BB had an excellent diagnostic potential for NSCLC (AUC = 0.923). Notably, PDGF-AA and PDGF-AB/BB were showed as useful biomarkers of response to platinum-based chemotherapy in NSCLC patients. PDGF-AA and PDGF-AB/BB concentrations continued to decrease in NSCLC patients receiving platinum-based chemotherapy. Compared to patients with PDGF-AA ≥ 30 ng/mL and PDGF-AB/BB ≥ 42 ng/mL, the median survival times were shorter among NSCLC patients with PDGF-AA < 30 ng/mL and PDGF-AB/BB < 42 ng/mL, which indicated poor prognosis in NSCLC patients. It is necessary to further investigate the prognostic value of serum PDGF-AA and PDGF-AB/BB in NSCLC patients with mutations and enrolled in different therapies.
Acknowledgments
The present study was supported by National Key Research and Development Projects-Demonstration and Application of Clinical Solutions for Cancer Prevention and Treatment (2017YFC0114303) and Six One Projects of Jiangsu Provincial Health Committee (Grant No. LGY2018046).
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ettinger DS, Wood DE, Aisner DL, et al. Non-small cell lung cancer, version 5.2017, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2017;15(4):504–535. doi:10.6004/jnccn.2017.0050
2. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009;59(4):225–249. doi:10.3322/caac.20006
3. Flehinger BJ, Kimmel M, Melamed MR. The effect of surgical treatment on survival from early lung cancer. Implications for screening. Chest. 1992;101(4):1013–1018. doi:10.1378/chest.101.4.1013
4. Shaik NA, Al-Kreathy HM, Ajabnoor GM, Verma PK, Banaganapalli B. Molecular designing, virtual screening and docking study of novel curcumin analogue as mutation (S769L and K846R) selective inhibitor for EGFR. Saudi J Biol Sci. 2019;26(3):439–448. doi:10.1016/j.sjbs.2018.05.026
5. Brown AP, Citrin DE, Camphausen KA. Clinical biomarkers of angiogenesis inhibition. Cancer Metastasis Rev. 2008;27(3):415–434.
6. Jain RK, Duda DG, Willett CG, et al. Biomarkers of response and resistance to antiangiogenic therapy. Nat Rev Clin Oncol. 2009;6(6):327–338. doi:10.1038/nrclinonc.2009.63
7. Pasanisi P, Venturelli E, Morelli D, Fontana L, Secreto G, Berrino F. Serum insulin-like growth factor-I and platelet-derived growth factor as biomarkers of breast cancer prognosis. Cancer Epidemiol Biomarkers Prev. 2008;17(7):1719–1722. doi:10.1158/1055-9965.EPI-07-0654
8. Cao R, Bråkenhielm E, Pawliuk R, et al. Angiogenic synergism, vascular stability and improvement of hind-limb ischemia by a combination of PDGF-BB and FGF-2. Nat Med. 2003;9(5):604–613. doi:10.1038/nm848
9. Li M, Jendrossek V, Belka C. The role of PDGF in radiation oncology. Radiat Oncol. 2007;2:5. doi:10.1186/1748-717X-2-5
10. Dong J, Grunstein J, Tejada M, et al. VEGF-null cells require PDGFR alpha signaling-mediated stromal fibroblast recruitment for tumorigenesis. EMBO J. 2004;23(14):2800–2810.
11. Hellberg C, Ostman A, Heldin CH. PDGF and vessel maturation. Recent Results Cancer Res. 2010;180:103–114.
12. Rykala J, Przybylowska K, Majsterek I, et al. Angiogenesis marker quantification in breast cancer and their correlation with clinicopathological prognostic variables. Pathol Oncol Res. 2011;17(4):809–817. doi:10.1007/s12253-011-9387-6
13. Yamamoto S, Tsuda H, Takano M, et al. Expression of platelet-derived growth factors and their receptors in ovarian clear-cell carcinoma and its putative precursors. Mod Pathol. 2008;21(2):115–124. doi:10.1038/modpathol.3800984
14. Mantur M, Snarska J, Sidorska A, Ostrowska H, Kruszewska-Wnorowska K, Wojszel J. Changes in PDGF concentration in surgically treated colorectal carcinoma. Adv Med Sci. 2008;53(1):37–41. doi:10.2478/v10039-008-0030-z
15. Rahbari NN, Reissfelder C, Mühlbayer M, et al. Correlation of circulating angiogenic factors with circulating tumor cells and disease recurrence in patients undergoing curative resection for colorectal liver metastases. Ann Surg Oncol. 2011;18(8):2182–2191. doi:10.1245/s10434-011-1761-9
16. Rahbari NN, Schmidt T, Falk CS, et al. Expression and prognostic value of circulating angiogenic cytokines in pancreatic cancer. BMC Cancer. 2011;11:286. doi:10.1186/1471-2407-11-286
17. Xu H, Wu J, Chen B, et al. Serum Dickkopf-1 (DKK1) is significantly lower in patients with lung cancer but is rapidly normalized after treatment. Am J Transl Res. 2014;6(6):850–856.
18. Ma R, Xu H, Wu J, et al. Identification of serum proteins and multivariate models for diagnosis and therapeutic monitoring of lung cancer. Oncotarget. 2017;8(12):18901–18913. doi:10.18632/oncotarget.14782
19. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
20. Parkin DM. Global cancer statistics in the year 2000. Lancet Oncol. 2001;2(9):533–543. doi:10.1016/S1470-2045(01)00486-7
21. Krzystek-Korpacka M, Diakowska D, Gamian A, Matusiewicz M. Increase in serum platelet-derived growth factor (PDGF)-BB reflects lymph node involvement in esophageal cancer patients independently from platelet count. Exp Oncol. 2011;33(3):140–144.
22. Griffin RJ, Williams BW, Wild R, Cherrington JM, Park H, Song CW. Simultaneous inhibition of the receptor kinase of vascular endothelial, fibroblast and platelet-derived growth factor suppresses tumor growth and enhances tumor radiation response. Cancer Res. 2002;62(6):1702–1706.
23. Lindahl P, Johansson BR, Levéen P, Betsholtz C. Pericyte loss and microaneurysm formation in PDGF-B-deficient mice. Science. 1997;277(5323):242–245. doi:10.1126/science.277.5323.242
24. Tawfik OW, Kramer B, Shideler B, Danley M, Kimler BF, Holzbeierlein J. Prognostic significance of CD44, platelet-derived growth factor receptor alpha, and cyclooxygenase 2 expression in renal cell carcinoma. Arch Pathol Lab Med. 2007;131(2):261–267. doi:10.1043/1543-2165(2007)131[261:PSOCPG]2.0.CO;2
25. Edelberg JM, Aird WC, Wu W, et al. PDGF mediates cardiac microvascular communication. J Clin Invest. 1998;102(4):837–843. doi:10.1172/JCI3058
26. Seifert RA, Hart CE, Phillips PE, et al. Two different subunits associate to create isoform specific platelet-derived growth factor receptors. J Biol Chem. 1989;264(15):8771–8778.
27. Xu L, Tong R, Cochran DM, Jain RK. Blocking platelet-derived growth factor-D/platelet-derived growth factor receptor beta signaling inhibits human renal cell carcinoma progression in an orthotopic mouse model. Cancer Res. 2005;65(15):5711–5719. doi:10.1158/0008-5472.CAN-04-4313
28. Gehmert S, Gehmert S, Prantl L, Vykoukal J, Alt E, Song YH. Breast cancer cells attract the migration of adipose tissue-derived stem cells via the PDGF-BB/PDGFR-beta signaling pathway. Biochem Biophys Res Commun. 2010;398(3):601–605. doi:10.1016/j.bbrc.2010.06.132
29. Hägglöf C, Hammarsten P, Josefsson A, et al. Stromal PDGFRbeta expression in prostate tumors and non-malignant prostate tissue predicts prostate cancer survival. PLoS One. 2010;5(5):e10747. doi:10.1371/journal.pone.0010747
30. Lavacchi D, Mazzoni F, Giaccone G. Clinical evaluation of dacomitinib for the treatment of metastatic non-small cell lung cancer (NSCLC): current perspectives. Drug Des Devel Ther. 2019;13:3187–3198. doi:10.2147/DDDT.S194231
31. Lynch TJ, Bell DW, Sordella R, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350(21):2129–2139. doi:10.1056/NEJMoa040938
32. Shaw AT, Yeap BY, Mino-Kenudson M, et al. Clinical features and outcome of patients with non-small-cell lung cancer who harbor EML4-ALK. J Clin Oncol. 2009;27(26):4247–4253. doi:10.1200/JCO.2009.22.6993
33. Kris MG, Johnson BE, Berry LD, et al. Using multiplexed assays of oncogenic drivers in lung cancers to select targeted drugs. JAMA. 2014;311(19):1998–2006. doi:10.1001/jama.2014.3741
34. Bergethon K, Shaw AT, Ou SH, et al. ROS1 rearrangements define a unique molecular class of lung cancers. J Clin Oncol. 2012;30(8):863–870. doi:10.1200/JCO.2011.35.6345
35. Bui KT, Cooper WA, Kao S, Boyer M. Targeted molecular treatments in non-small cell lung cancer: a clinical guide for oncologists. J Clin Med. 2018;7(8):E192. doi:10.3390/jcm7080192
36. Sulzbacher I, Birner P, Trieb K, Träxler M, Lang S, Chott A. Expression of platelet-derived growth factor-AA is associated with tumor progression in osteosarcoma. Mod Pathol. 2003;16(1):66–71. doi:10.1097/01.MP.0000043522.76788.0A
37. Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92(3):205–216. doi:10.1093/jnci/92.3.205
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.