")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Serum Levels of Tumor Necrosis Factor-α and Vascular Endothelial Growth Factor in the Subtypes of Clinical High Risk Individuals: A Prospective Cohort Study
Authors Ye J, Wei Y, Zeng J, Gao Y, Tang X, Xu L, Hu Y, Liu X, Liu H, Chen T, Li C, Zeng L, Wang J, Zhang T
Received 23 April 2023
Accepted for publication 24 July 2023
Published 31 July 2023 Volume 2023:19 Pages 1711—1723
DOI https://doi.org/10.2147/NDT.S418381
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
JiaYi Ye,1,* YanYan Wei,1,* JiaHui Zeng,1 YuQing Gao,1 XiaoChen Tang,1 LiHua Xu,1 YeGang Hu,1 XiaoHua Liu,1 HaiChun Liu,2 Tao Chen,3,4 ChunBo Li,1 LingYun Zeng,5,* JiJun Wang,1,6,7 TianHong Zhang1
1Shanghai Mental Health Center, Shanghai Jiaotong University School of Medicine, Shanghai Engineering Research Center of Intelligent Psychological Evaluation and Intervention, Shanghai Key Laboratory of Psychotic Disorders, Shanghai, 200030, People’s Republic of China; 2Department of Automation, Shanghai Jiao Tong University, Shanghai, 200240, People’s Republic of China; 3Big Data Research Lab, University of Waterloo, Ontario, Canada; 4Labor and Worklife Program, Harvard University, Cambridge, MA, USA; 5Department of Psychiatric Rehabilitation, Shenzhen Kangning Hospital, ShenZhen, GuangDong, People’s Republic of China; 6Center for Excellence in Brain Science and Intelligence Technology (CEBSIT), Chinese Academy of Science, Shanghai, People’s Republic of China; 7Institute of Psychology and Behavioral Science, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: TianHong Zhang; JiJun Wang, Shanghai Mental Health Center, Shanghai Jiaotong University School of Medicine, Shanghai Engineering Research Center of Intelligent Psychological Evaluation and Intervention, Shanghai Key Laboratory of Psychotic Disorders, Shanghai, 200030, People’s Republic of China, Email [email protected]; [email protected]
Introduction: Numerous studies have established the roles of inflammation and angioneurins in the pathogenesis of schizophrenia (SCZ). This study aimed to compare the serum levels of tumour necrosis factor (TNF)-α and vascular endothelial growth factor (VEGF) in patients at clinical high risk (CHR) for psychosis or SCZ at baseline and one year after treatment.
Methods: A total of 289 CHR participants from the Shanghai At Risk for Psychosis Extended Program (SHARP) were tracked for a year. They were divided into two and four subtypes based on symptom severity according to the Structured Interview for Prodromal Syndromes (SIPS) and received standard medical care. At baseline and one-year follow-up, TNF-α and VEGF were detected using enzyme-linked immunosorbent assay, and pathological features were assessed using the Global Assessment of Function (GAF) score.
Results: Baseline TNF-α levels did not differ significantly, while VEGF levels were lower in patients with more severe symptoms. VEGF showed a negative correlation with negative features, both overall (r = − 0.212, p = 0.010) and in the subgroup with higher positive scores (r = − 0.370, p = 0.005). TNF-α was positively correlated with negative symptoms in the subgroup with higher negative scores (r = 0.352, p = 0.002). A three-way multivariate analysis of variance demonstrated that participants in Subtype 1 of positive or negative symptoms performed better than those in Subtype 2, with significant main effects and interactions of group and both cytokines.
Discussion: TNF-α and VEGF levels are higher and lower, respectively, in CHR patients with more severe clinical symptoms, particularly negative symptoms, which point to a worsening inflammatory and vascular status in the brain.
Keywords: ultra high risk, prodromal psychosis, inflammation, TNF-α, VEGF
A Letter to the Editor has been published for this article.
A Response to Letter by Ms Lienggonegoro has been published for this article.
Despite modernisation, psychotic disorders remain among the top ten leading causes of burden worldwide. Schizophrenia (SCZ) is a debilitating, chronic mental disorder that affects 0.5–1% of the world’s population, with 80–85% heritability and complex polygenic inheritance, and is linked to significant morbidity and mortality. SCZ usually has its onset in early adulthood and is characterised by reality distortion (delusions and hallucinations), disorganisation (formal thought disorder, disorganised behaviour, and the uncommon symptom of inappropriate effect), and negative symptoms.1,2
SCZ is influenced by both genetic and environmental factors. Genome-wide association studies have identified numerous genetic loci associated with the disorder, highlighting the polygenic nature of schizophrenia. Rare copy number variants and gene-disrupting variants also contribute to the risk. Childhood trauma has been suggested as a potential environmental risk factor. The convergence of genetic and environmental factors on synaptic organization and transmission is implicated in schizophrenia pathogenesis.2
SCZ is a significant contributor to premature death and a leading cause of disability in young people globally.3 Early intervention seems to slow the disease progression and enhance the effectiveness of its treatment.4 The development of biomarkers and investigation of pathological mechanisms during the prodromal stage of SCZ will enable early disease prevention and enhance prognosis.5
Mounting evidence supports the idea that interactions between the immune system and brain dysregulation serve as key psychosis vulnerability factors.6,7 Compared to the healthy control group, the SCZ group displayed significant increases in the levels of inflammatory cytokines.8 According to a previous study, patients with SCZ had elevated levels of several cytokines.8 Another study established clinical, neurocognitive, and neuroanatomical associations with increased inflammation and demonstrated peripheral inflammatory marker alterations in psychotic disorders.9 Clinical studies on antipsychotic augmentation with nonsteroidal anti-inflammatory drugs have supported the link between inflammation and psychosis. Additionally, adjunctive anti-inflammatory drugs significantly reduced the severity of all symptoms in patients with SCZ.10 Patients with SCZ have an imbalanced proinflammatory response and antioxidant status, so these biological processes may be targets for SCZ management.11
Tumor necrosis factor (TNF)-α is secreted by T helper (h) 1 cells and promotes inflammation, as shown in earlier studies.12 Vascular endothelial growth factor (VEGF), which acts as a neurotrophic factor, can neuroprotect the central nervous system (CNS).13 To assess the degree of inflammation-angioneurins balance and the severity of the illness, we measured the serum levels of TNF-α and VEGF in clinical high risk (CHR) for psychosis who presented with the syndrome as a recent emergence or worsening of attenuated (subthreshold) positive symptoms, which typically precede a full-blown psychotic illness.
Similar standards are applied in the DSM-5’s Attenuated Psychosis Syndrome Provisional Diagnostic Category. Individuals who fit the CHR criteria are distressed and seek treatment, and even when their symptoms are not subpsychotic in intensity, they still interfere with social and occupational functioning.14,15
In this study, we classified the participants into subtypes based on positive and negative symptoms. Previous research has indicated that there may be distinct underlying pathophysiological mechanisms among different subtypes characterized by prodromal symptoms and cognitive impairment of different severities of CHR individuals for psychosis.16 By stratifying our sample, we aimed to explore potential differences in inflammatory markers and angioneurins that may be associated with each symptom profile. Emerging evidence in the field of immunology and psychiatry indicates that inflammation plays a crucial role in the development and progression of psychotic disorders.17 Therefore, we hypothesized that examining the relationship between inflammation, angioneurins, and specific symptom profiles could provide valuable insights into the complex interactions underlying the onset of psychosis. Moreover, by conducting subgroup analysis, we aimed to identify potential biomarkers that could distinguish between the subtypes, which may have important implications for early intervention and personalized treatment strategies. Understanding the inflammatory profiles associated with positive and negative symptom subtypes may help in tailoring interventions to the specific needs of each subgroup.
However, previous studies have investigated inflammation and angioneurins in post-onset patients with SCZ, but mostly in separate ways. Furthermore, psychosis is highly heterogeneous, and different symptoms may have different biological mechanisms. Previous studies considered psychosis as a whole, while this study hypothesises that the role of inflammation and angioneurins in different symptoms may differ. Based on positive and negative symptoms, we divided the participants into two and four subtypes for the Structured Interview for Prodromal Syndromes (SIPS). Our study tried to correlate the inflammation-angioneurins factors with clinical characteristics of different severities through subtype grouping.
We addressed the following issues in the current study: 1) Whether the level of inflammation and angioneurin factors was different in the CHR subtypes; 2) Whether there are different interactions between positive/negative symptoms and inflammation-angioneurins balance.
Methods
Trial Design
The Shanghai At Risk for Psychosis Extended Program (SHARP-Extended) was launched at the Shanghai Mental Health Center (SMHC) in 2016. A total of 400 CHR participants aged 14–35 years were included. Among these, 289 (72.3%) completed comprehensive clinical assessments at baseline and 1-year follow-up. The inclusion criteria were: (i) participants fit into one of the three prodromal syndromes—attenuated positive symptom syndrome (APSS), brief limited intermittent psychotic syndrome (BIPS), or genetic risk and deterioration syndrome (GRDS)—and underwent face-to-face interviews using the SIPS; (ii) age of 15–45 years; (iii) individuals younger than 18 years were accompanied by either a parent or legal guardian; (iv) capacity to provide informed consent or assent if under 18; and (v) must have completed at least six years of primary education. Additionally, all patients were untreated before the start of the study, and treatment only began once the study started. The exclusion criteria included severe or unstable physical illnesses, such as diseases of the nervous and endocrine systems, cardiovascular diseases, cancers, low immune function, substance abuse, and pregnancy. Patients with axis I mental disorders, such as SCZ, affective disorder, anxiety spectrum disorder, acute or chronic renal failure, cirrhosis, or active liver disease, were also excluded.18 Before blood collection, each participant was confirmed to have no recent (within two weeks) use of nonsteroidal anti-inflammatory drugs. Blood was collected in only patients who did not take nonsteroidal anti-inflammatory drugs.
Our study divided the participants into two and four subtypes based on positive and negative symptoms. The 289 samples in this study contained 181 from Subtype 1 and 108 from Subtype 2, as determined by positive symptoms. Total positive scores below ten on the SIPS indicated a moderate deficit in positive symptoms for Subtype 1, whereas total positive scores above ten indicated a potentially extensive and severe deficit in positive symptoms for Subtype 2. The 289 participants in this study included 127 in Subtype 1 and 162 in Subtype 2, as determined by negative symptoms. Total negative scores below ten in the SIPS, indicative of moderate deficits in negative symptoms, are a feature of Subtype 1; total negative scores above ten in the SIPS, which may indicate extensive and severe deficits in negative symptoms, are a feature of Subtype 2. In addition, the 289 participants were categorised into four subtypes; 67 participants from Subtype 1, 41 from Subtype 2, 95 from Subtype 3, and 86 from Subtype 4 were characterised by positive and negative symptoms. Total positive scores > 10 and total negative scores > 10 in SIPS were characteristics of Subtype 1, total positive scores > 10 and total negative scores ≤ 10 were characteristics of Subtype 2, total positive scores ≤ 10 and total negative scores > 10 were characteristics of Subtype 3, and total positive scores ≤ 10 and total negative scores ≤ 10 were characteristics of Subtype 4. Sociodemographic variables, such as age, years of education, and sex of participants, were collected at baseline. This study was approved by the Research Ethics Committee of the SMHC (2013–32C2) and was performed in accordance with the Declaration of Helsinki. Each participant signed an informed consent form, and those under the age of 18 had their guardians sign the forms (Figure 1).14–16
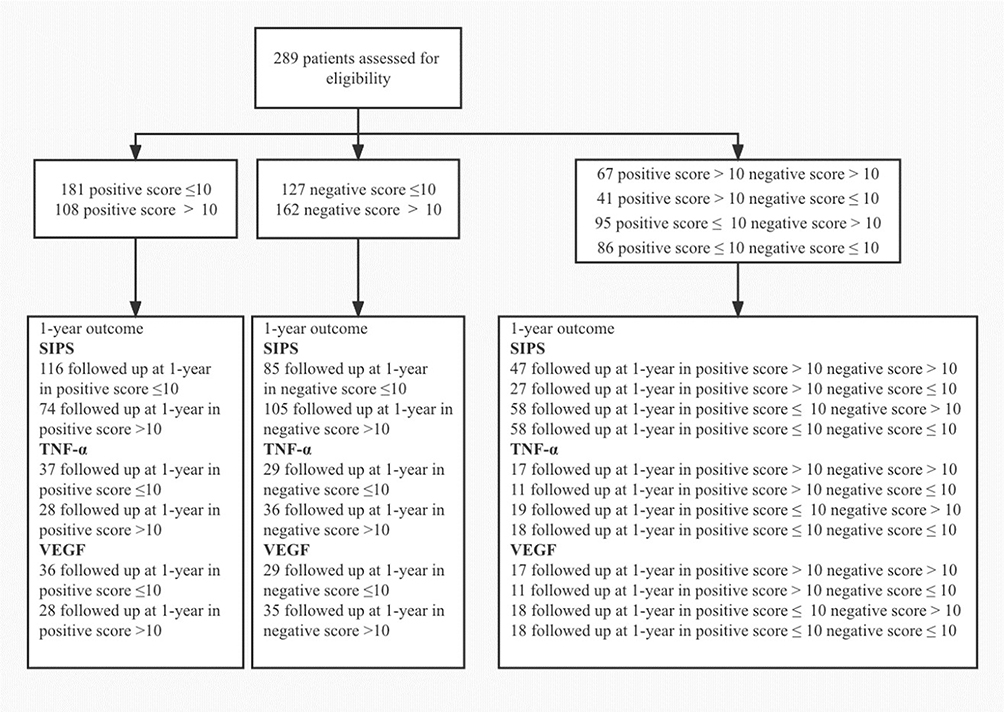 |
Figure 1 CONSORT flow diagram of participants. |
Scales and Measurements
The participants underwent face-to-face interviews using the SIPS19 at baseline and 1-year follow-up. The SIPS contains four scales for measurement (Scale of Prodromal Symptoms (SOPS), Schizotypal Personality Disorder Checklist (DSM-IV), Family History Questionnaire, and Global Assessment of Functioning scale (GAF)) and two criteria (Presence of Psychotic Syndrome (POPS), Criteria of Prodromal Syndromes (COPS)). The SOPS comprises 19 items that assess four symptom domains: positive symptoms (scales P1–P5: P1, unusual thought content; P2, suspiciousness; P3, grandiosity; P4, perceptual abnormalities; and P5, disorganised communication); negative symptoms (scales N1–N6: N1, social anhedonia; N2, avolition; N3, expression of emotion; N4, experience of emotions and self; N5, ideational richness; and N6, occupational functioning); disorganised symptoms (scales D1–D4: D1, odd behaviour or appearance; D2, bizarre thinking; D3, trouble with focus and attention; and D4, impairment in personal hygiene); and general symptoms (scales G1–G4: G1, sleep disturbance; G2, dysphoric mood; G3, motor disturbances; and G4, impaired tolerance to normal stress).19 The Schizotypal Personality Disorder Checklist was used to distinguish CHR patients from those with schizotypal personality disorders. The family history questionnaire was used to determine whether participants had first-degree relatives with SCZ. During the SIPS interview, the GAF scale was used to evaluate overall functioning levels, and the drop in GAF scores at baseline and follow-up represented functional rehabilitation or deterioration in the SIPS interview.20 The GAF, whose scores range from 1 to 100, covers the range from positive mental health to severe psychopathology; it is an overall measurement to communicate the level of impairment, indicate the need for professional help, and reflect improvement or change over time.20,21 The POPS requires one or more of the positive items from the SOPS to be scored at a psychotic level of intensity and describes psychotic symptom frequency and duration criteria. For the transition criteria of POPS, one or more of the five SOPS positive items in the psychotic range (rating of 6) should be met, and symptoms should last an average of four days per week for a month or one day if symptoms are seriously disorganising or dangerous. The CHR participants were required to meet one of the COPS criteria: (1) APSS: One or more of the five SOPS positive items scoring in the prodromal range (rating of 3 to 5), symptoms beginning within the past year or increasing by one or more points within the past year, and symptoms occurring at least once per week for the last month. (2) BIPS: One or more of the five SOPS positive items in the psychotic range (rating of 6), symptoms beginning in the past three months, and symptoms occurring currently at least several minutes per day at least once per month (less than an average of four days per week and less than three months), but not seriously disorganising or dangerous. (3) GRDS: First-degree relatives with a history of any psychotic disorder or criteria for schizotypal personality disorder in the patient and GAF drop of at least 30% over the last month vs one year ago. The SIPS was used at baseline and 1-year follow-up to determine the conversion and clinical features of the participants.19
Measurement of TNF-α and VEGF Concentrations
For CHR participants, baseline and 1-year follow-up blood samples were collected. Fasting blood samples were taken early in the morning, kept at room temperature for one hour, and then centrifuged (1710 × g, 20 min, 4°C) to separate the serum. The serum was then divided and stored at −80°C until analysis. The Luminex 200 System, Luminex 200 Validation Kit, Luminex 200 Calibration Kit, and MILLIPLEX MAP Human Complement Magnetic Bead Panel 2 were used to perform enzyme-linked immunosorbent assay (ELISA) to measure the serum levels of TNF-α and VEGF in each sample in duplicate. All samples from each subject were analysed simultaneously to minimise the impact of assay variability on measurements from specific subjects. The unit of measurement for inflammatory cytokine concentrations was picograms of protein per millilitre of serum (pg/mL). TNF-α and VEGF standard curves were used to calibrate all data. Cytokine concentrations below the detection range of the standard curves were not included in the analysis.22
Statistical Analysis
The data were examined using SPSS version 26. The study groups’ baseline demographics and characteristics were described using mean and standard deviations (SD). Analysis of variance (ANOVA) and independent sample t-tests were used to compare quantitative data, including age, years of education, GAF, SIPS scores, and levels of inflammatory factors. Post-hoc comparisons were made using Bonferroni correction. To compare categorical variables such as sex, family history, prodromal syndromes, and clinical outcomes, χ2 and Fisher’s precision probability tests were used. To determine whether there was a strong correlation between TNF-α, VEGF, and the pathological symptoms indicated by baseline SIPS scores, correlation analysis and Spearman correlation coefficient were used. Additionally, correlograms were generated using GraphPad Prism 9.0. The differences between two points and subtypes and time changes for interaction were compared using a three-way multivariate analysis of variance (MANOVA) between groups divided by positive or negative symptom categories. The effect sizes of the subtypes were evaluated using partial eta squared (η2). The significance levels (p-values) used in these analyses were set at a predetermined threshold (p<0.05) to determine the statistical significance of the observed differences.
Results
Study Characteristics
For positive symptoms, 181 patients were Subtype 1 (positive score ≤ 10), and 108 were Subtype 2 (positive score > 10); for negative symptoms, 127 were Subtype 1 (negative score ≤ 10), and 162 were Subtype 2 (negative score > 10); for both positive and negative symptoms, 67 were Subtype 1 (positive score > 10 and negative score > 10), 41 were Subtype 2 (positive score > 10 and negative score ≤ 10), 95 were Subtype 3 (positive score ≤ 10 and negative score > 10), and 86 were Subtype 4 (positive score ≤ 10 and negative score ≤ 10). Of the 289 participants, 190 (65.7%) completed the 1-year interview. Subtype 2 had lower GAF_Now and higher GAF_Drop and SIPS scores than Subtype 1 in the group with positive symptoms, except for negative scores. Subtype 2 showed a higher transition rate, GAF_Drop, and SIPS scores, except for a positive score, and lower GAF_Before, GAF_Now, and VEGF scores (t = 3.474, p = 0.001) than Subtype 1. GAF scores, SIPS scores, and VEGF levels (F = 4.660, p = 0.004) differed among the four subtypes divided by positive and negative symptoms, with Subtype 1 having the highest and Subtype 4 having the lowest SIPS scores. Additionally, Subtype 1’s VEGF level was significantly lower than that of Subtype 4, and Subtype 3’s SOPS ratings were significantly higher than those of Subtype 2 (Table 1 and Table 2).
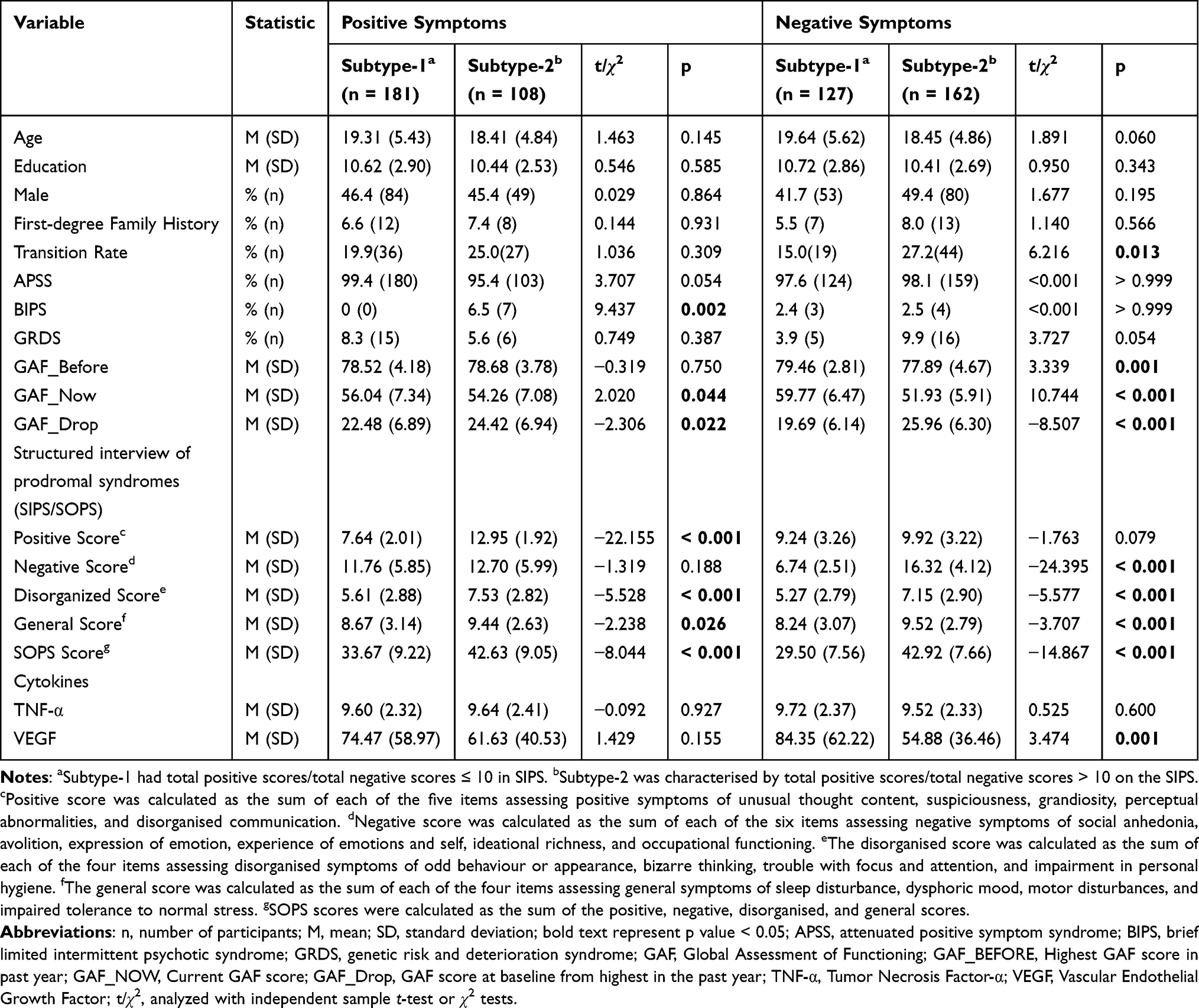 |
Table 1 Demographic and Clinical Characteristics of Different Subtypes with CHR of Positive and Negative Symptoms |
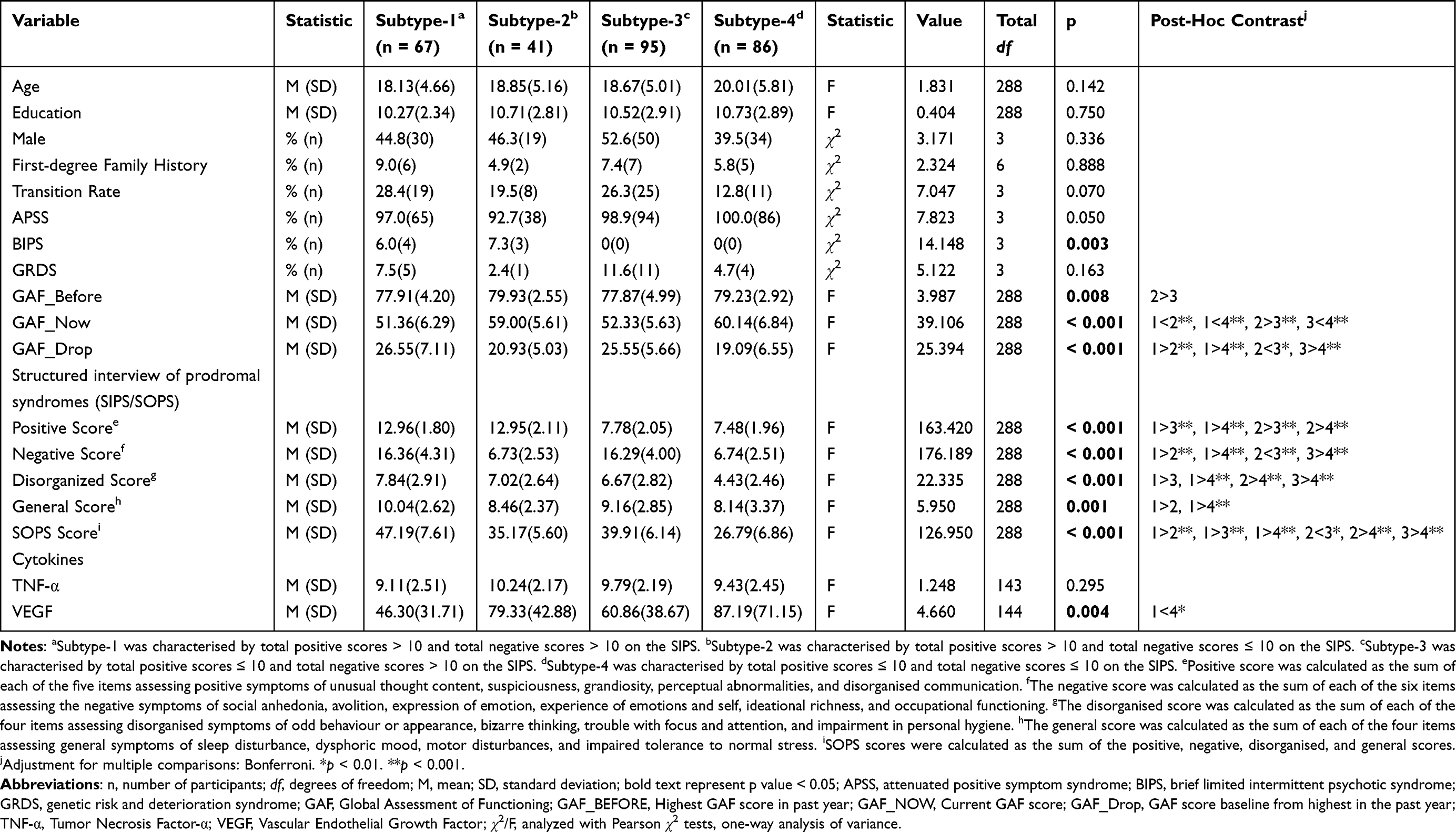 |
Table 2 Demographic and Clinical Characteristics of Different Subtypes with CHR of Both Positive and Negative Symptoms |
Group and Cytokine Differences in Positive and Negative Symptoms
The three-way MANOVA showed that groups with total scores of positive or negative symptoms less than ten performed better than groups with total scores of positive or negative symptoms greater than ten at p < 0.001, p < 0.01, and p < 0.05, respectively. There were no discernible group differences in the domain of positive symptoms and VEGF. Significant differences were found in the domains of positive symptoms and TNF-α, positive symptoms and VEGF, and negative symptoms and VEGF of cytokines at p < 0.001. For the domain of negative symptoms and TNF-α, TNF-α also showed mild significance, F (1, 61) = 4.678, p = 0.034, Pillai’s trace = 0.071, partial η2 = 0.071. A significant interaction between cytokines and groups was found for both domains of positive and negative symptoms and TNF-α (p < 0.001). For the domain of positive symptoms and VEGF, F (1, 60) = 5.879, p = 0.018, Pillai’s trace = 0.089, partial η2 = 0.089, and for the domain of negative symptoms and VEGF, F (1, 60) = 10.583, p = 0.002, Pillai’s trace = 0.150, partial η2 = 0.150 (Table 3).
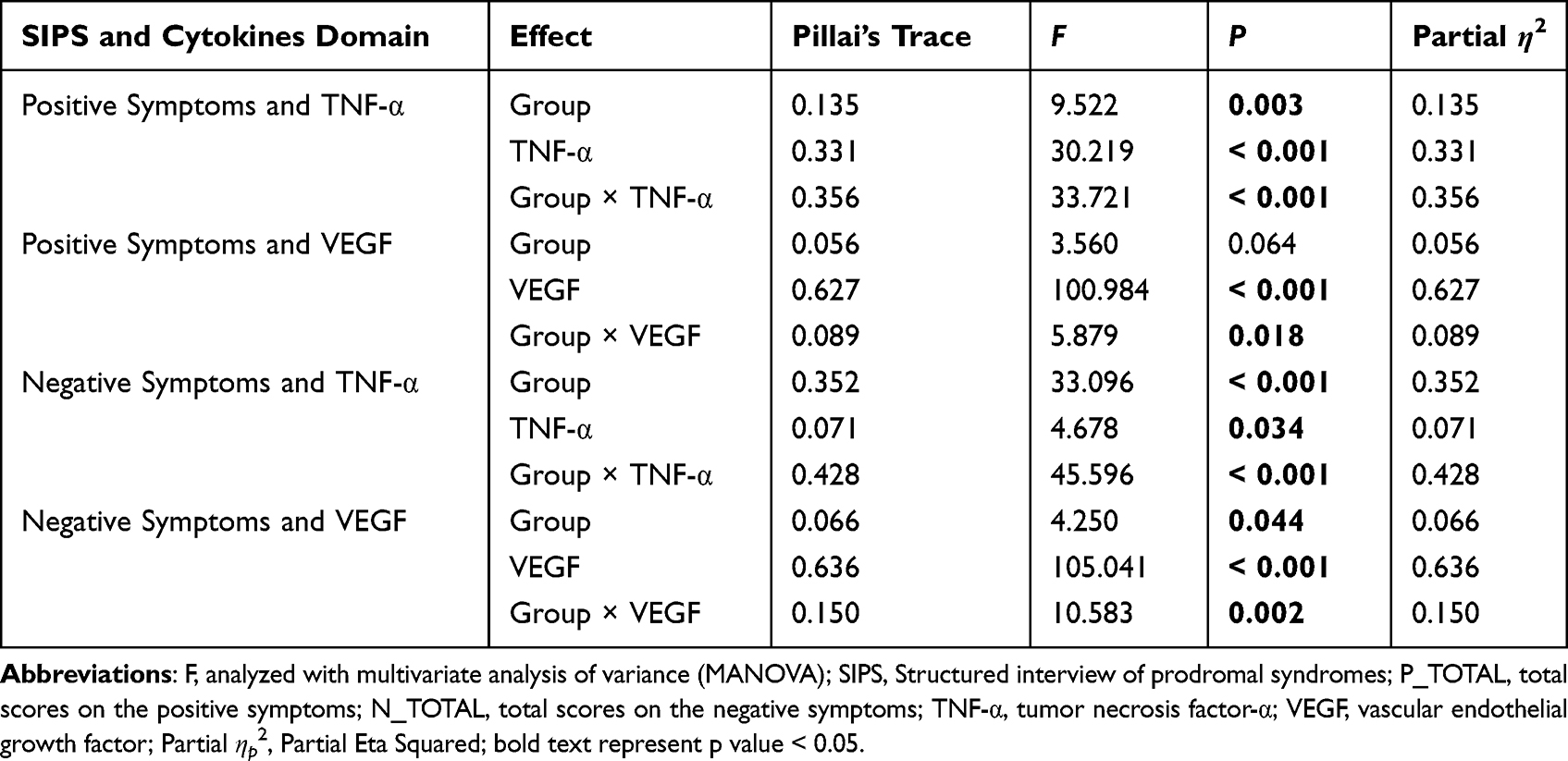 |
Table 3 MANOVA Results for Each SIPS and Cytokines Domain Including Main and Interaction Effects |
Correlation Analysis
VEGF was negatively correlated to negative scores when not grouping (r = −0.212, p = 0.010) and in the group with total positive scores > 10 (r = −0.370, p = 0.005). In the group with total negative scores >10, TNF-α was positively correlated with negative symptoms (r = 0.352, p = 0.002) (Figure 2).
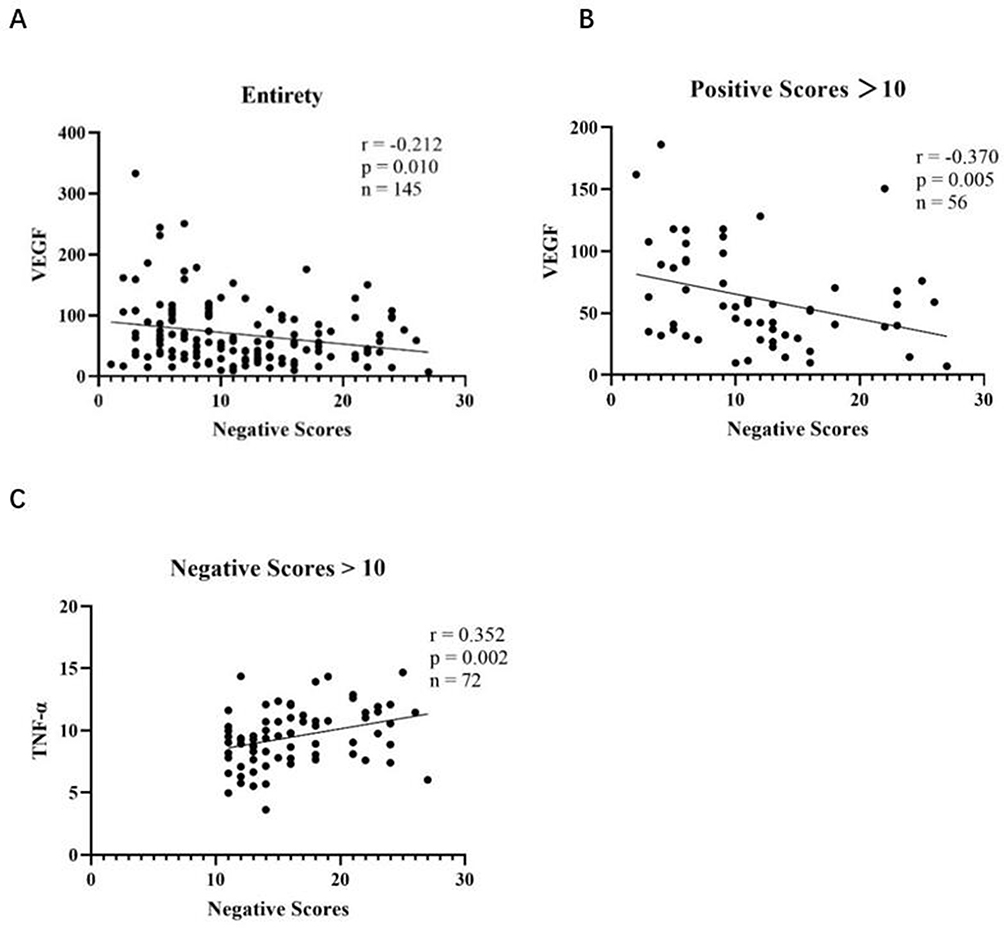 |
Figure 2 Correlations between cytokines and clinical symptoms. (A) Levels of VEGF were negatively correlated with negative scores when not grouping, (B) and the group which positive scores > 10. (C) Levels of TNF-α were positively correlated with negative scores in the group which negative scores > 10. Spearman correlation coefficients were calculated. |
Discussion
Key Findings
In this study, we have found that people with severe clinical symptoms would show a terrible inflammatory and vascular condition in the brain, especially the individuals with severer negative symptoms, were more likely to have the imbalance of inflammation and angioneurins and converse to the first-episode SCZ. As most recent literature focused on the pro-/anti-inflammation and angioneurins between post-/first-onset or chronic patients with SCZ or general paychosis and healthy controls,23–25 and the inflammation in CHR group and different subtypes has seldom been descript; recent literature investigated the CHR with inflammatory mechanism divided the individuals into convertors and non-convertors, but did not show other heterogeneity in CHR.26,27 Our study demonstrated the inflammation and angioneurins in the CHR, and further grouped CHR and explored the subtypes of CHR, which supplement an extensive insight into the pathogenesis of SCZ. By the combination of categorization of CHR and pro-/anti-inflammatory factors, we illustrated the heterogeneity of the SCZ and related different symptoms with different biological mechanisms.
The results of our study demonstrated that lower VEGF levels were associated with more severe symptoms, particularly negative symptoms. Additionally, when not grouping and in the subtype with positive scores > 10, VEGF levels were negatively associated with negative symptoms, whereas TNF-α levels were positively associated with negative symptoms in the subtype with negative scores > 10. Meanwhile, CHR individuals with higher negative scores were more likely to develop first-episode SCZ. Additionally, according to the three-way MANOVA, certain main effects and interactions of group, TNF-α, and VEGF were demonstrated, with mild positive or negative symptoms outperforming the severe ones, and negative symptoms tending to have higher partial η2 of effects of groups, cytokines, and interactions than positive symptoms, suggesting that negative symptoms represented more severe inflammation and vascular damage in the brain.
Negative symptoms were recently demonstrated to be essential characteristics of SCZ and linked to poor functioning, poor prognosis, higher conversion rate, and refractoriness.28,29 According to previous studies, conversion was more likely when CHR-negative symptoms were more severe and persistent, which increased the risk of developing psychosis.30
The association between inflammatory markers and CHR suggests the importance of early intervention. Detecting and monitoring inflammatory markers, such as TNF-α and VEGF, in individuals at CHR can help identify individuals who may be at greater risk for developing psychosis. This enables timely interventions aimed at reducing inflammation, managing symptoms, and potentially preventing or delaying the onset of full-blown psychosis. The early identification and intervention based on inflammatory profiles may improve long-term outcomes and reduce the burden of illness in this population.
TNF-α is a multifunctional proinflammatory cytokine with modulatory effects on nerve cell growth, differentiation, apoptosis, and synaptic function.12,31 It is primarily expressed by macrophages and produced by neurons and glial cells in the CNS.12,32 TNF-α plays a crucial role in the coordination of both peripheral and central immune processes,12 influencing transforming growth factor (TGF)-β, which is altered in patients with SCZ33 and is related to dissociative pathology.34 Among the proinflammatory cytokines, multiple studies have focused on the elevation of serum TNF-α levels which can cause inflammation, oxidative stress, vascular permeability increasing and apoptotic cell death by stimulating macrophages.12,35 Findings provided evidence that the negative effects of TNF-α on the brain-derived neurotrophic factor (BDNF) may confer susceptibility to SCZ and cognitive dysfunction.31 Several studies have shown significantly increased serum TNF-α levels in SCZ compared to those in healthy controls which are related to the negative symptoms,8 indicating that TNF-α and disturbance of oxidative stress status, as well as their interaction, may be involved in the pathophysiology of SCZ.12 Studies have found that TNF-α decreases the nodes and total dendritic length and inhibits cortical neuron dendrite development, contributing to the impairment of neuronal survival and development.36 Activation of microglia increases the production of proinflammatory cytokines and oxygen species and disturbs the development and function of neuronal circuits in the brain, leading to excessive synaptic pruning; loss of cortical gray matter in stress-sensitive regions, such as the prefrontal cortex, dentate gyrus, and hippocampus; and disinhibition of subcortical dopamine, resulting in deficits in neural connectivity, changes in the balance between the excitatory and inhibitory signals of neurons, which triggers immune dysfunction in the cerebral cortex and affects neurotransmitters, especially glutamate and aminobutyric acid, thereby causing psychotic symptoms.5,11,12,35,37–41 Research has demonstrated that the breakdown of connectivity between the cerebellum and right dorsolateral prefrontal cortex and gray matter reductions of certain frontal lobe components, such as inferior and superior frontal gyri, medial and dorsolateral prefrontal cortices, orbitofrontal cortex, and anterior cingulate cortex, were associated with negative symptom severity.42,43 Our results indicated that the subtype of positive scores > 10 and negative scores ≤ 10 performed better than the subtype of positive scores ≤ 10 and negative scores > 10 in GAF_Before, GAF_Now, and GAF_Drop, and implied greater significance in negative symptoms of GAF_Drop compared to the positive symptoms. In addition, we found that the VEGF levels of the subtype with positive scores > 10 and negative scores >10 were much lower than those of the subtype with positive scores ≤ 10 and negative scores ≤ 10. Although no significant TNF-α was shown at baseline, the obvious synergy of TNF-α along with time and clinical symptoms was exhibited by MANOVA. The findings of more severe negative symptoms leading to worse clinical outcomes were aligned with previous studies. Thus, we assumed that VEGF is a protective factor in the CNS to balance the proinflammatory and destructive effects of TNF-α. When patients suffer from stressors, the rising levels of TNF-α may cause apoptosis, raise the levels of other proinflammatory cytokines, reduce BDNF, increase oxidative stress in the brain, and damage nerve tissues, leading to a decrease in cortical volumes and impaired brain function connectivity which may result in severe negative symptoms and a high transition rate. The corpus callosum, thalamus, hippocampal formation, subiculum, parahippocampal gyrus, superior temporal gyrus, prefrontal and orbitofrontal cortices, and amygdala-hippocampal complex have been shown to have decreased volumes in SCZ by imaging studies.33
Furthermore, a large body of research points to a link between blood flow, regional cellular energy metabolism, and micro- and macrovascular abnormalities in the brain in patients with SCZ.44–46 The pathogenesis of neuropsychiatric diseases is influenced by VEGF.46 Its production can be stimulated in various cells, including endothelial cells, monocytes, astroglial cells, and T-cells, and ultimately produced in hypoxic cells.13,44 As one of the vascular endothelial biomarkers, it is a signal protein and neurotrophic factor involved in angiogenesis, poised at the nexus of inflammatory response and vascular risk.47,48 VEGF promotes neurogenesis, neuronal plasticity, genesis, differentiation, regeneration or degeneration, growth, and axon outgrowth13,46 and induces vascular endothelial cell proliferation, migration, and vasopermeability in various tissues49 suggesting its neuroprotection of the CNS. VEGF has been shown to protect the brain from cell loss, blood–brain barrier (BBB) dysfunction, dendritic spine loss, spatial memory impairment, and cognitive decline in response to injuries in both animal and human studies,50 and antipsychotics have been shown to increase cyclic adenosine monophosphate (cAMP) response element-binding protein phosphorylation in the hippocampus and enhance VEGF expression.49
Additionally, the fact that VEGF is a crucial regulator of glutamatergic synaptic function suggests that it plays a role in the pathophysiology of psychiatric disorders; genetic studies have revealed that VEGF-related polymorphisms are linked to SCZ,51 and decreased mRNA levels of VEGF genes have been demonstrated in patients with SCZ.33 According to previous studies,46,49 VEGF levels in pre-treatment patients were significantly lower than those in healthy controls and increased in post-treatment patients; VEGF levels gradually decreased with the severity of cognitive impairment in psychosis.50 A previous study shows a statistically significant positive correlation between VEGF levels and the Positive and Negative Syndrome Scale (PANSS) negative subscale.46 Lower baseline VEGF levels predicted resistance to drug therapy in acute-stage SCZ, according to a study that found a significant positive correlation between baseline serum VEGF levels and antipsychotic efficacy.48 In postmortem studies, the dorsolateral prefrontal cortex and thalamus showed reduced VEGF expression.13,44
These stressors can induce inflammation that causes hypoxia in the brain tissue, ultrastructural damage to capillaries, and endothelial maladaptation and dysfunction.44,48 These effects may have been triggered by TNF-α/soluble TNF receptor 1 signalling and transduced through AP-1/c-FOS signalling to modify VEGF-C-VEGF receptor 3 and the VEGF promoter.52,53 A lack of VEGF may cause alterations in cellular energy metabolism, including decreased glucose metabolism and blood flow,44,50 which raises vascular permeability and changes the BBB, encourages the infiltration of inflammatory cells and cytokines into the CNS,48 and further impairs BBB integrity.9
Our findings have significant clinical implications in the context of CHR. By identifying different subtypes based on positive and negative symptoms, and their associated inflammatory profiles, we gain valuable insights into the underlying mechanisms and potential treatment targets. These findings offer opportunities for personalized treatment approaches and early intervention strategies in CHR individuals.
Limitations
This study has some limitations that should be considered. First, the study’s participants were all Chinese and were chosen from a single centre, and the sample size was quite small; hence, it is unlikely that the traits identified in these participants would apply to other populations. Second, the high missing rate might have impacted the complete and final results. Third, there is insufficient information when only two cytokines are considered. It has been noted that SCZ has high VEGF levels.9 However, this might have been brought on by the retaliatory rise in stress and will eventually wane upon exhaustion. Fourth, the absence of healthy controls contributes to unknown differences between participants with mild clinical deficits and healthy individuals. Finally, the current CHR individuals received natural treatments, such as various medications with different dosages, types, durations, and compliance rates, which may have confounded the changes in cytokines and conversion outcomes.
Future Directions
More attention should be paid to the inflammatory marks examinations and combined use of anti-inflammatory agents may also be taken into account in clinical practice. Nevertheless, the department concerned may draft relevant policies to allow CHR or SCZ individuals to enjoy a free physical examination about the pro-/anti-inflammatory cytokines per year to better evaluate their condition. Moreover, for future research, more CHR, healthy controls, cytokines, and the transition rate of the individuals who use anti-inflammatory agents in combination compared with those do not use or use placebo in combination should be included and investigated. In addition, understanding the interplay between genetic susceptibility and environmental factors, facilitating the translation of research findings into evidence-based guidelines and clinical practice are critical for elucidating the complex etiology of psychotic disorders, and long-term follow-up studies should also be warranted. By addressing these specific research directions, future studies can build upon the foundation laid by this research and contribute to a more comprehensive understanding of the immunological mechanisms underlying CHR individuals for psychosis. Additionally, the implementation may lead to advancements in early detection, intervention, and personalized treatments, ultimately improving patient outcomes and the overall management of psychotic disorders.
Conclusion
Higher TNF-α and lower VEGF levels are found in people with more severe clinical symptoms, especially negative symptoms, which points to a terrible inflammatory and vascular condition in the brain. The pathogenic potential of the cytokines and the subtypes we discovered suggests that novel clinical diagnosis and therapeutic targeting may be a promising strategy for halting the debilitating disease in its prodromal stage.
Acknowledgments
This study was supported by National Key R&D Program of the Ministry of Science and Technology of China (2016YFC1306800), National Natural Science Foundation of China (82151314, 81901832, 81871050, 82171497, and 82101623), Shanghai Clinical Research Center for Mental Health (19MC1911100), Shenzhen Science and Technology R&D Fund Project (JCYJ20180306171033310), The Clinical Research Center at Shanghai Mental Health Center (CRC2018ZD01, CRC2018ZD04 and CRC2018YB01), and Clinical Research Plan of SHDC (SHDC2022CRD026, SHDC2020CR4066). JiaYi Ye, YanYan Wei and LingYun Zeng are co-first authors for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors confirm that there are no competing interests to disclose in this work.
References
1. GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry. 2022;9(2):137–150. doi:10.1016/S2215-0366(21)00395-3
2. Jauhar S, Johnstone M, McKenna PJ. Schizophrenia. Lancet. 2022;399(10323):473–486. doi:10.1016/S0140-6736(21)01730-X
3. Agarwal SM, Stogios N, Ahsan ZA, et al. Pharmacological interventions for prevention of weight gain in people with schizophrenia. Cochrane Database Syst Rev. 2022;10(10):CD013337. doi:10.1002/14651858.CD013337.pub2
4. Kim SW, Nelson B, Yang YK, Chung YC. Editorial: early intervention in psychotic disorders. Front Psychiatry. 2020;11:574532. doi:10.3389/fpsyt.2020.574532
5. Shnayder NA, Khasanova AK, Strelnik AI, et al. Cytokine imbalance as a biomarker of treatment-resistant schizophrenia. Int J Mol Sci. 2022;23(19). doi:10.3390/ijms231911324
6. Campeau A, Mills RH, Stevens T, et al. Multi-omics of human plasma reveals molecular features of dysregulated inflammation and accelerated aging in schizophrenia. Mol Psychiatry. 2022;27(2):1217–1225. doi:10.1038/s41380-021-01339-z
7. De Picker LJ, Victoriano GM, Richards R, et al. Immune environment of the brain in schizophrenia and during the psychotic episode: a human post-mortem study. Brain Behav Immun. 2021;97:319–327. doi:10.1016/j.bbi.2021.07.017
8. Dunleavy C, Elsworthy RJ, Upthegrove R, Wood SJ, Aldred S. Inflammation in first-episode psychosis: the contribution of inflammatory biomarkers to the emergence of negative symptoms, a systematic review and meta-analysis. Acta Psychiatr Scand. 2022;146(1):6–20. doi:10.1111/acps.13416
9. Lizano P, Lutz O, Xu Y, et al. Multivariate relationships between peripheral inflammatory marker subtypes and cognitive and brain structural measures in psychosis. Mol Psychiatry. 2021;26(7):3430–3443. doi:10.1038/s41380-020-00914-0
10. Jeppesen R, Christensen RHB, Pedersen EMJ, et al. Efficacy and safety of anti-inflammatory agents in treatment of psychotic disorders - a comprehensive systematic review and meta-analysis. Brain Behav Immun. 2020;90:364–380. doi:10.1016/j.bbi.2020.08.028
11. Fraguas D, Díaz-Caneja CM, Ayora M, et al. Oxidative stress and inflammation in first-episode psychosis: a systematic review and meta-analysis. Schizophr Bull. 2019;45(4):742–751. doi:10.1093/schbul/sby125
12. Zhu S, Zhao L, Fan Y, et al. Interaction between TNF-α and oxidative stress status in first-episode drug-naïve schizophrenia. Psychoneuroendocrinology. 2020;114:104595. doi:10.1016/j.psyneuen.2020.104595
13. Misiak B, Stramecki F, Stańczykiewicz B, Frydecka D, Lubeiro A. Vascular endothelial growth factor in patients with schizophrenia: a systematic review and meta-analysis. Prog Neuropsychopharmacol Biol Psychiatry. 2018;86:24–29. doi:10.1016/j.pnpbp.2018.05.005
14. Cannon TD. The current state of the clinical high risk for psychosis research paradigm. Biol Psychiatry. 2020;88(4):284–286. doi:10.1016/j.biopsych.2020.06.008
15. Ciarleglio AJ, Brucato G, Masucci MD, et al. A predictive model for conversion to psychosis in clinical high-risk patients. Psychol Med. 2019;49(7):1128–1137. doi:10.1017/s003329171800171x
16. Zhang T, Wang J, Xu L, et al. Subtypes of clinical high risk for psychosis that predict antipsychotic effectiveness in long-term remission. Pharmacopsychiatry. 2021;54(1):23–30. doi:10.1055/a-1252-2942
17. Khandaker GM, Cousins L, Deakin J, Lennox BR, Yolken R, Jones PB. Inflammation and immunity in schizophrenia: implications for pathophysiology and treatment. Lancet Psychiatry. 2015;2(3):258–270. doi:10.1016/S2215-0366(14)00122-9
18. Zhang T, Tang X, Li H, et al. Clinical subtypes that predict conversion to psychosis: a canonical correlation analysis study from the ShangHai at risk for psychosis program. Aust N Z J Psychiatry. 2020;54(5):482–495. doi:10.1177/0004867419872248
19. Miller TJ, McGlashan TH, Rosen JL, et al. Prodromal assessment with the structured interview for prodromal syndromes and the scale of prodromal symptoms: predictive validity, interrater reliability, and training to reliability. Schizophr Bull. 2003;29(4):703–715. doi:10.1093/oxfordjournals.schbul.a007040
20. Aas IH. Global Assessment of Functioning (GAF): properties and frontier of current knowledge. Ann Gen Psychiatry. 2010;9:20. doi:10.1186/1744-859x-9-20
21. Aas IHM, Sonesson O, Torp S. A qualitative study of clinicians experience with rating of the Global Assessment of Functioning (GAF) scale. Community Ment Health J. 2018;54(1):107–116. doi:10.1007/s10597-016-0067-6
22. Zhang T, Zeng J, Wei Y, et al. Changes in inflammatory balance correlates with conversion to psychosis among individuals at clinical high-risk: a prospective cohort study. Psychiatry Res. 2022;318:114938. doi:10.1016/j.psychres.2022.114938
23. Baek SH, Kim H, Kim JW, et al. Association between peripheral inflammatory cytokines and cognitive function in patients with first-episode schizophrenia. J Pers Med. 2022;12(7). doi:10.3390/jpm12071137
24. Mednova IA, Boiko AS, Kornetova EG, Semke AV, Bokhan NA, Ivanova SA. Cytokines as potential biomarkers of clinical characteristics of schizophrenia. Life. 2022;12(12). doi:10.3390/life12121972
25. Morales-Munoz I, Palmer ER, Marwaha S, Mallikarjun PK, Upthegrove R. Persistent childhood and adolescent anxiety and risk for psychosis: a longitudinal birth cohort study. Biol Psychiatry. 2022;92(4):275–282. doi:10.1016/j.biopsych.2021.12.003
26. Ouyang L, Li D, Li Z, et al. IL-17 and TNF-beta: predictive biomarkers for transition to psychosis in ultra-high risk individuals. Front Psychiatry. 2022;13:1072380. doi:10.3389/fpsyt.2022.1072380
27. Zhang T, Zeng J, Wei Y, et al. Changes in inflammatory markers in clinical high risk of developing psychosis. Neuropsychobiology. 2023;1–13. doi:10.1159/000528770
28. Mahmood Z, Van Patten R, Keller AV, et al. Reducing negative symptoms in schizophrenia: feasibility and acceptability of a combined cognitive-behavioral social skills training and compensatory cognitive training intervention. Psychiatry Res. 2021;295:113620. doi:10.1016/j.psychres.2020.113620
29. Tam MHW, Ling-Ling W, Cheng KM, et al. Latent structure of self-report negative symptoms in patients with schizophrenia: a preliminary study. Asian J Psychiatr. 2021;61:102680. doi:10.1016/j.ajp.2021.102680
30. Fusar-Poli P, Salazar de Pablo G, Correll CU, et al. Prevention of psychosis: advances in detection, prognosis, and intervention. JAMA Psychiatry. 2020;77(7):755–765. doi:10.1001/jamapsychiatry.2019.4779
31. Zhang Y, Fang X, Fan W, et al. Interaction between BDNF and TNF-α genes in schizophrenia. Psychoneuroendocrinology. 2018;89:1–6. doi:10.1016/j.psyneuen.2017.12.024
32. Suchanek-Raif R, Raif P, Kowalczyk M, et al. Promoter polymorphisms of TNF-α gene as a risk factor for schizophrenia. Arch Med Res. 2018;49(4):248–254. doi:10.1016/j.arcmed.2018.09.007
33. Mohammadi A, Rashidi E, Amooeian VG. Brain, blood, cerebrospinal fluid, and serum biomarkers in schizophrenia. Psychiatry Res. 2018;265:25–38. doi:10.1016/j.psychres.2018.04.036
34. Roydeva MI, Reinders A. Biomarkers of pathological dissociation: a systematic review. Neurosci Biobehav Rev. 2021;123:120–202. doi:10.1016/j.neubiorev.2020.11.019
35. Lin C, Chen K, Yu J, et al. Relationship between TNF-α levels and psychiatric symptoms in first-episode drug-naïve patients with schizophrenia before and after risperidone treatment and in chronic patients. BMC Psychiatry. 2021;21(1):561. doi:10.1186/s12888-021-03569-5
36. Zhu M, Liu Z, Guo Y, et al. Sex difference in the interrelationship between TNF-α and oxidative stress status in first-episode drug-naïve schizophrenia. J Neuroinflammation. 2021;18(1):202. doi:10.1186/s12974-021-02261-5
37. Monji A, Mizoguchi Y. Neuroinflammation in late-onset schizophrenia: viewing from the standpoint of the microglia hypothesis. Neuropsychobiology. 2022;81(2):98–103. doi:10.1159/000517861
38. Nakahara S, Turner JA, Calhoun VD, et al. Dentate gyrus volume deficit in schizophrenia. Psychol Med. 2020;50(8):1267–1277. doi:10.1017/S0033291719001144
39. Pollak TA, Drndarski S, Stone JM, David AS, McGuire P, Abbott NJ. The blood-brain barrier in psychosis. Lancet Psychiatry. 2018;5(1):79–92. doi:10.1016/s2215-0366(17)30293-6
40. Radhakrishnan R, Kaser M, Guloksuz S. The link between the immune system, environment, and psychosis. Schizophr Bull. 2017;43(4):693–697. doi:10.1093/schbul/sbx057
41. Strzelecki D, Urban-Kowalczyk M, Wysokiński A. Serum levels of TNF-alpha in patients with chronic schizophrenia during treatment augmentation with sarcosine (results of the PULSAR study). Psychiatry Res. 2018;268:447–453. doi:10.1016/j.psychres.2018.08.002
42. Brady RO, Gonsalvez I, Lee I, et al. Cerebellar-prefrontal network connectivity and negative symptoms in schizophrenia. Am J Psychiatry. 2019;176(7):512–520. doi:10.1176/appi.ajp.2018.18040429
43. Ince E, Ucok A. Relationship between persistent negative symptoms and findings of neurocognition and neuroimaging in schizophrenia. Clin EEG Neurosci. 2018;49(1):27–35. doi:10.1177/1550059417746213
44. Lizano PL, Keshavan MS, Tandon N, et al. Angiogenic and immune signatures in plasma of young relatives at familial high-risk for psychosis and first-episode patients: a preliminary study. Schizophr Res. 2016;170(1):115–122. doi:10.1016/j.schres.2015.12.001
45. Pillai A, Howell KR, Ahmed AO, et al. Association of serum VEGF levels with prefrontal cortex volume in schizophrenia. Mol Psychiatry. 2016;21(5):686–692. doi:10.1038/mp.2015.96
46. Ye F, Zhan Q, Xiao W, et al. Altered serum levels of vascular endothelial growth factor in first-episode drug-naïve and chronic medicated schizophrenia. Psychiatry Res. 2018;264:361–365. doi:10.1016/j.psychres.2018.04.027
47. Nguyen TT, Dev SI, Chen G, et al. Abnormal levels of vascular endothelial biomarkers in schizophrenia. Eur Arch Psychiatry Clin Neurosci. 2018;268(8):849–860. doi:10.1007/s00406-017-0842-6
48. Rampino A, Annese T, Torretta S, Tamma R, Falcone RM, Ribatti D. Involvement of vascular endothelial growth factor in schizophrenia. Neurosci Lett. 2021;760:136093. doi:10.1016/j.neulet.2021.136093
49. Lee BH, Hong JP, Hwang JA, et al. Alterations in plasma vascular endothelial growth factor levels in patients with schizophrenia before and after treatment. Psychiatry Res. 2015;228(1):95–99. doi:10.1016/j.psychres.2015.04.020
50. Zhao Y, Xiao W, Chen K, et al. Neurocognition and social cognition in remitted first-episode schizophrenia: correlation with VEGF serum levels. BMC Psychiatry. 2019;19(1):403. doi:10.1186/s12888-019-2397-8
51. Pu J, Liu Y, Gui S, et al. Vascular endothelial growth factor in major depressive disorder, schizophrenia, and bipolar disorder: a network meta-analysis. Psychiatry Res. 2020;292:113319. doi:10.1016/j.psychres.2020.113319
52. Cao R, Ji H, Yang Y, Cao Y. Collaborative effects between the TNFα-TNFR1-macrophage axis and the VEGF-C-VEGFR3 signaling in lymphangiogenesis and metastasis. Oncoimmunology. 2015;4(3):e989777. doi:10.4161/2162402x.2014.989777
53. Catar R, Moll G, Kamhieh-Milz J, et al. Expanded hemodialysis therapy ameliorates uremia-induced systemic microinflammation and endothelial dysfunction by modulating VEGF, TNF-α and AP-1 signaling. Front Immunol. 2021;12:774052. doi:10.3389/fimmu.2021.774052
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.