")
Back to Journals » Integrated Blood Pressure Control » Volume 15
Serum Levels of NT-Pro BNP in Patients with Preeclampsia
Authors Nguyen TX , Nguyen VT, Nguyen-Phan HN, Hoang BB
Received 30 January 2022
Accepted for publication 25 March 2022
Published 7 April 2022 Volume 2022:15 Pages 43—51
DOI https://doi.org/10.2147/IBPC.S360584
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Turgay Celik
Thanh Xuan Nguyen,1 Van Tri Nguyen,2 Hong Ngoc Nguyen-Phan,3 Bui Bao Hoang3
1Department of Abdominal Emergency and Pediatric Surgery, Hue Central Hospital, Hue City, 530000, Vietnam; 2Department of Anesthesiology, Hue International Medical Center, Hue Central Hospital, Hue City, 530000, Vietnam; 3Department of Internal Medicine, Hue University of Medicine and Pharmacy, Hue University, Hue City, 530000, Vietnam
Correspondence: Bui Bao Hoang, Department of Internal Medicine, Hue University of Medicine and Pharmacy, Hue University, 06 Ngo Quyen Street, Hue City, Vietnam, Tel +84 905405005, Email [email protected]; [email protected]
Objective: This study aims to determine the serum levels of NT-proBNP in women with preeclampsia with and without severe signs and to evaluate the cardiovascular risks in these two groups of participants.
Methods: A descriptive cross-sectional study was conducted on 52 women with preeclampsia in the Department of Gynecology and Obstetrics – Hue Central Hospital, from August 2019 to September 2020.
Results: In preeclampsia women, the rate of hypertension in stage 3, stage 2, and stage 1 were 46.1%, 32.7%, and 21.2%, respectively. The average Sokolow-Lyon index in the preeclampsia group with and without severe signs was 22.25 ± 7.38mm, 20.16 ± 5.54mm, respectively. The average left ventricular mass index in the group of preeclampsia patients without and with severe signs was 92.27 ± 14.56g/m2 and 120.68 ± 16.47g/m2, respectively. The average ejection fraction in the group of preeclampsia patients without severe signs and with severe signs was 65.11 ± 3.45%, 56.21 ± 7.12%, correspondingly. In contrast, the difference between the two groups was statistically significant with p < 0.05. The plasma NT-proBNP level in the preeclampsia group without severe signs was 349.12 ± 93.51pg/mL, whereas the concentration in the preeclampsia group with severe signs was 725.32 ± 290.46pg/mL (p < 0.05).
Conclusion: The NT-proBNP level was statistically significantly increased in the patients with preeclampsia. Analyzing and comparing the figures and changes found in two groups of PE patients, with and without severe signs, we suggest that women diagnosed with PE with severe signs have a higher risk of developing cardiovascular problems forthwith and henceforth.
Keywords: preeclampsia, cardiovascular, NT-proBNP
Introduction
Hypertensive disorders of pregnancy constitute one of the leading causes of maternal and perinatal mortality worldwide. Preeclampsia is a pregnancy disorder associated with new-onset hypertension, which occurs most often after 20 weeks of gestation and frequently near term. Although often accompanied by new-onset proteinuria, hypertension and other signs or symptoms of preeclampsia may present in some women without proteinuria. It has been estimated that preeclampsia complicates 2–8% of pregnancies globally. According to the World Health Organization, this condition accounts for about 10–12% of the causes of maternal and perinatal mortality. In the United States, the prevalence of preeclampsia has increased by 25% over the past two decades. It has become the leading cause of maternal and fetal morbidity and mortality, with an estimated 50,000–60,000 deaths related to preeclampsia every year worldwide.1 Hypertension and preeclampsia can result in complications for the mother (left ventricular wall thickness, left-sided heart failure, coronary artery disease, stroke, acute kidney failure, acute pulmonary edema, liver failure, etc) and fetus (fetal growth retardation, preterm birth, perinatal mortality).2 In Vietnam, the prevalence of preeclampsia and eclampsia constitutes 4–5% of all pregnant women.
NT-proBNP, which stands for N-terminal pro-brain natriuretic peptide, is a non-active prohormone produced within the heart and released into the circulation in response to increased wall tension. NT-proBNP level raises in the blood in symptomatic and asymptomatic patients with left ventricular dysfunction. To ascertain the likelihood of heart failure, the FDA has recommended cut-points of 125 pg/mL for people aged <75 years and 450 pg/mL for older people.
NT-proBNP levels in women with preeclampsia, eclampsia, and hemolysis, elevated liverenzymes and Low Platelets (HELLP) syndrome are elevated, reflecting increased left ventricular filling pressure and left ventricular diastolic and/or subclinical cardiac dysfunction.3,4 NT-proBNP is also increased in participants with preterm preeclampsia and multiplies many times their risk of cardiovascular complications, but the mechanism remains unclear. The changes in the vascular system in preeclampsia are not similar to normal pregnancy, but rather an increase in vasoconstriction, thereby increasing the burden on the heart and altering the function and structure of the left ventricle. High levels of diuretic peptides reflect limited left ventricular function. NT-proBNP is considered a sensitive marker for detecting cardiac dysfunction. Recent studies have indicated that preeclampsia patients with severe signs have an increased risk of future cardiovascular disease than healthy women.3 Therefore, we carried out this study to evaluate cardiac function using transthoracic echocardiography and serum NT-proBNP level in a cohort of women with PE.
Methods
Study Design and Participants
This cross-sectional study was approved by the Institutional Review Board of Hue Central Hospital and adhered to the Guidelines for Good Clinical Practice. All participants gave written informed consent. Pregnant women with singleton pregnancies >20 weeks of gestational age were recruited from the Hue Central Hospital. Women were excluded if they had multifetal gestations, cardiac valvular disease, myocardial ischemia, atrial fibrillation, chronic hypertension, transient hypertension, brain tumor, diabetes, cerebral hemorrhage, coma, kidney failure and hypertension unresponsive to oral treatment of methyldopa and nifedipine.
We enrolled women with pre-eclampsia, which was characterized by the following criteria in Table 1.
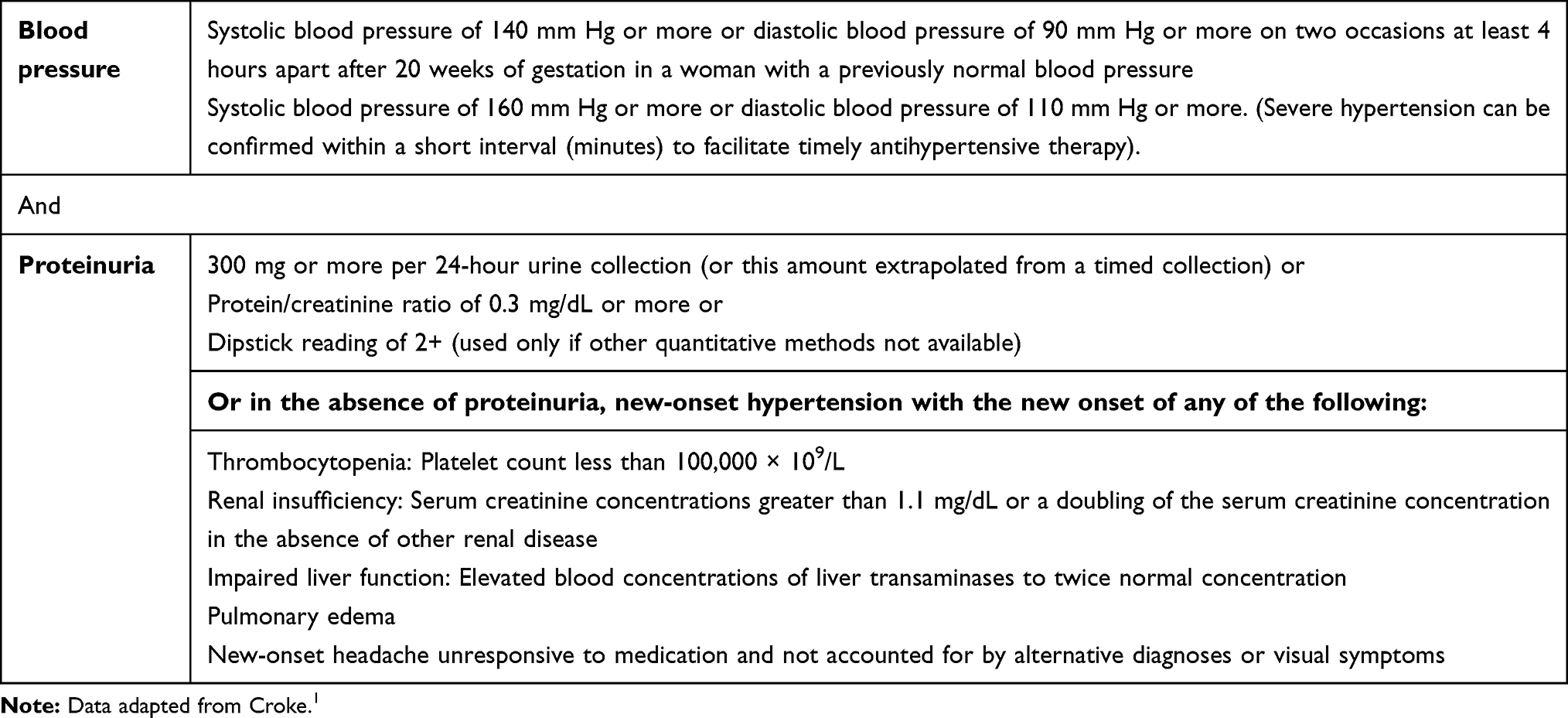 |
Table 1 Diagnostic Criteria for Preeclampsia According to American College of Obstetricians and Gynecologists (ACOG) 2019 |
Then, heart failure is another concept that needs definition provided. The European Society of Cardiology 2021 defines heart failure as not just a pathological diagnosis, but a clinical syndrome consisting of cardinal symptoms (eg, breathlessness, ankle swelling, and fatigue) that signs may accompany (eg, elevated jugular venous pressure, pulmonary crackles, and peripheral edema. It is due to structural and/or functional abnormalities of the heart that results in elevated cardiac pressures and/or inadequate cardiac output at rest and/or during exercise. Upon the measurement of left ventricular ejection fraction (LVEF), heart failure was divided into three phenotypes: heart failure with preserved ejection fraction (HFpEF – LVEF ≥ 50%), heart failure with mildly reduced ejection fraction (HFmrEF – LVEF between 41% and 49%), and lastly heart failure with reduced ejection fraction (HFrEF – LVEF ≤ 40%).5
In addition, we identified severe preeclampsia,6 which was characterized by the following criteria: (1) Systolic blood pressure of 160 mm Hg or more, or diastolic blood pressure of 110 mm Hg or more on two occasions at least 4 hours apart (unless antihypertensive therapy was initiated before this time). (2) Thrombocytopenia (platelet count less than 100,000 × 109/L. (3) Impaired liver function that is not accounted for by alternative diagnoses and as indicated by abnormally elevated blood concentrations of liver enzymes (to more than twice the upper limit normal concentrations), or by severe persistent right upper quadrant or epigastric pain unresponsive to medications. (4) Renal insufficiency (serum creatinine concentration more than 1.1 mg/dL or a doubling of the serum creatinine concentration in the absence of other renal diseases). (5) Pulmonary edema. (6) New-onset headache unresponsive to medication and not accounted for by alternative diagnoses. (7) Visual disturbances.
The women with PE underwent echocardiographic and laboratory measures within 24 hours of admission (including 24-hour proteinuria and serum creatinine) and before active labor or delivery but after initial treatment with intravenous magnesium sulfate and oral or intravenous antihypertensive agents (ie, labetalol, hydralazine, or nifedipine).
Electrocardiogram (EEG) criteria for LVH (left ventricle hypertrophy) diagnosis: Several criteria were used to diagnose LVH via electrocardiography. In this study, we are using Sokolow-Lyon index, which consists of two conditions as follows: S in V1 + R in V5 or V6 (whichever is larger) ≥35mm (≥7 large squares) and R in aVL ≥11mm.
Transthoracic Echocardiography
The transthoracic echocardiograms were performed at the cardiovascular center of our hospital by experienced cardiac sonographers using Phillips or GE ultrasound machines. Echocardiographic indices including LVDd, LVDs, IVSd, IVSs, LVPWd, LVPWs, LVM, LVMI, EF, FS were reported.
Serum NT-proBNP
Within 24 hours of echocardiographic imaging, 10-mL blood samples were obtained from the cubital vein. The blood clot was immediately separated by centrifugation and the serum was stored in 1-mL aliquots at −80°C until analysis. Serum NT-proBNP was determined with an electrochemiluminescent sandwich immunoassay with Roche immunoanalyserElecsys® 2010/Cobas e411. The between-batch coefficient of variation for the assay is 1.5–4.0% from 148 to 4423 pg/mL, with an analytical range of 5–35,000 pg/mL.
Statistical Analysis
Statistical analysis was performed using IBM SPSS version 20. Non-parametric tests, specifically Mann–Whitney U-test and Kruskal–Wallis test, were used for intergroup comparisons. Relationships with p-values <0.05 were considered significant.
Results
A total of 52 women were enrolled. The mean age was 27.4 years (range: 18–47). Baseline characteristics of the study participants are shown in Table 2. The hypertension and preeclampsia classification characteristics are demonstrated in Table 3, which was a significant difference in the classification of hypertension between the two groups of preeclampsia (P < 0.0001).
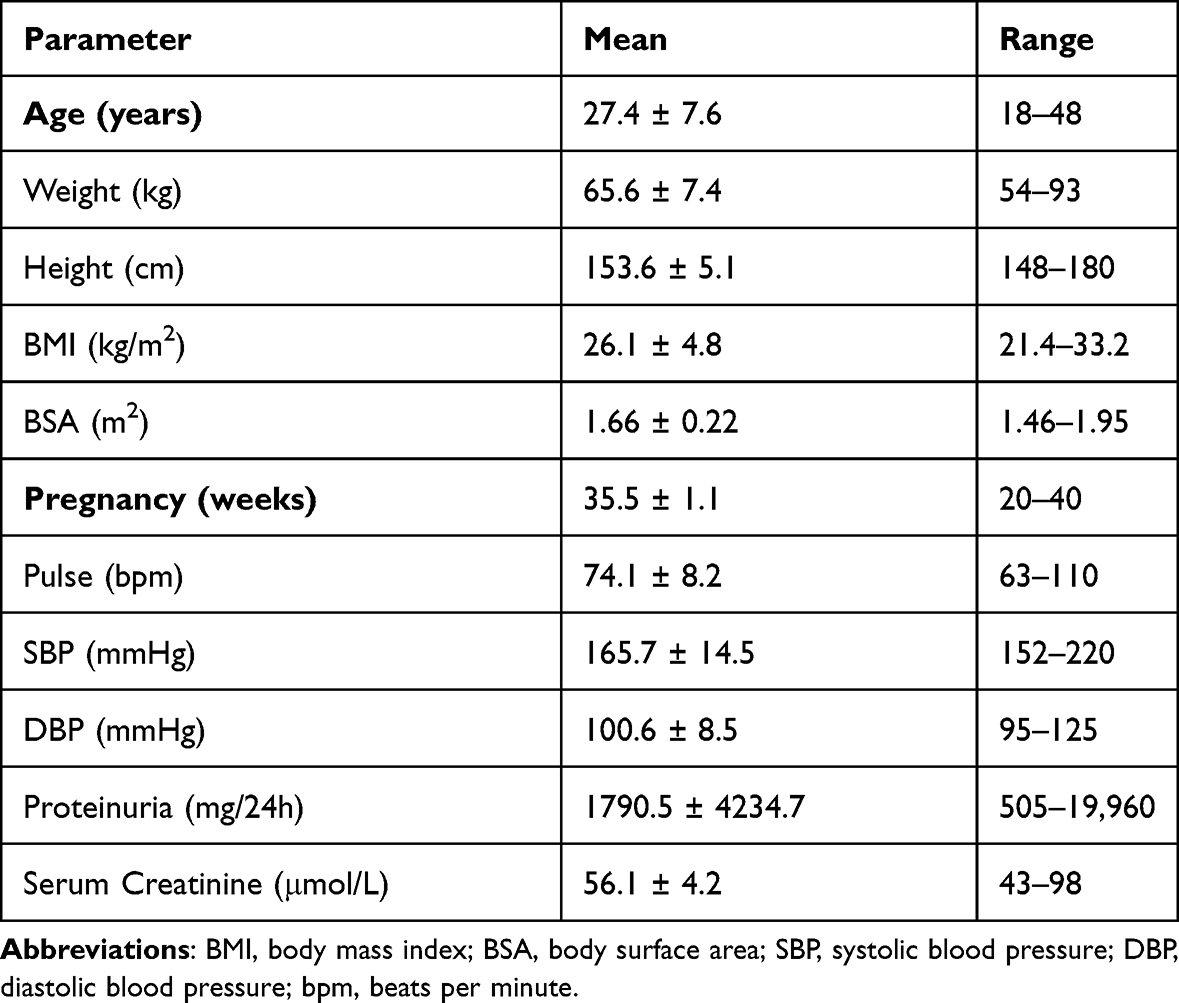 |
Table 2 Baseline Characteristics of the Studied Participants |
 |
Table 3 Classification of Hypertension and Preeclampsia |
Table 4 demonstrates the Sokolow-Lyon index on electrocardiogram (ECG) of women with PE. No difference was found in the Sokolow-Lyon index between the two groups of preeclampsia with or without severe signs. There was a significant difference between the two groups of these items: LVDs, IVSd, IVSs, LVPWd, LVM, PAPs, EF and FS (Table 5).
 |
Table 4 Sokolow-Lyon Index and Degree of Preeclampsia |
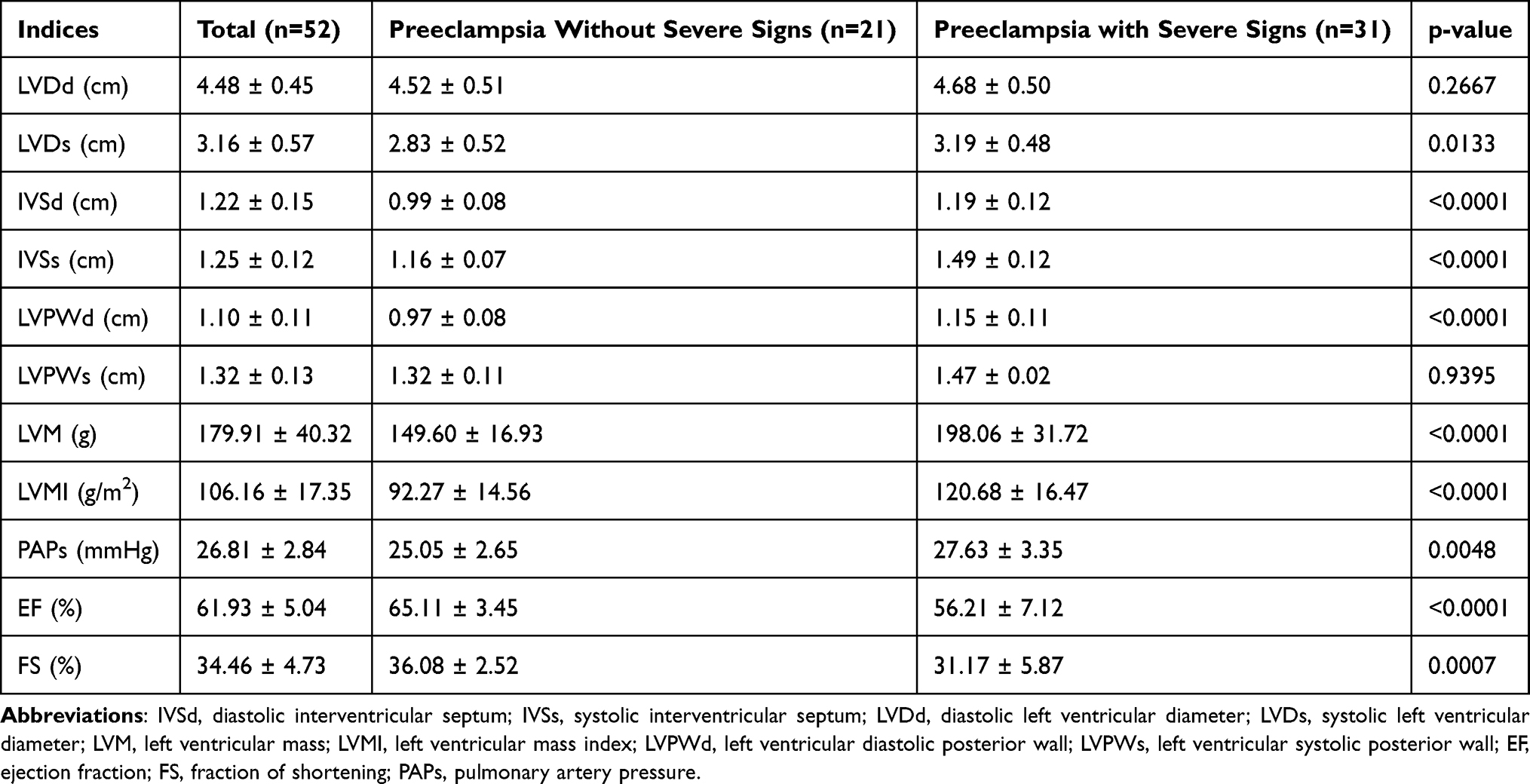 |
Table 5 Echocardiographic Indices Between Preeclampsia Groups |
The serum NT-proBNP level was significantly higher in the preeclampsia group with severe signs than in the group without severe signs (725.32 ± 290.46 pg/mL vs 349.12 ± 93.51 pg/mL, respectively) (Table 6).
 |
Table 6 Serum NT-proBNP Level by Type of Preeclampsia |
Also, the serum NT-proBNP level in the group with heart failures was higher than that without heart failures (868.85 ± 283.31 pg/mL vs 318.55 ± 193.77 pg/mL, respectively) (Table 7).
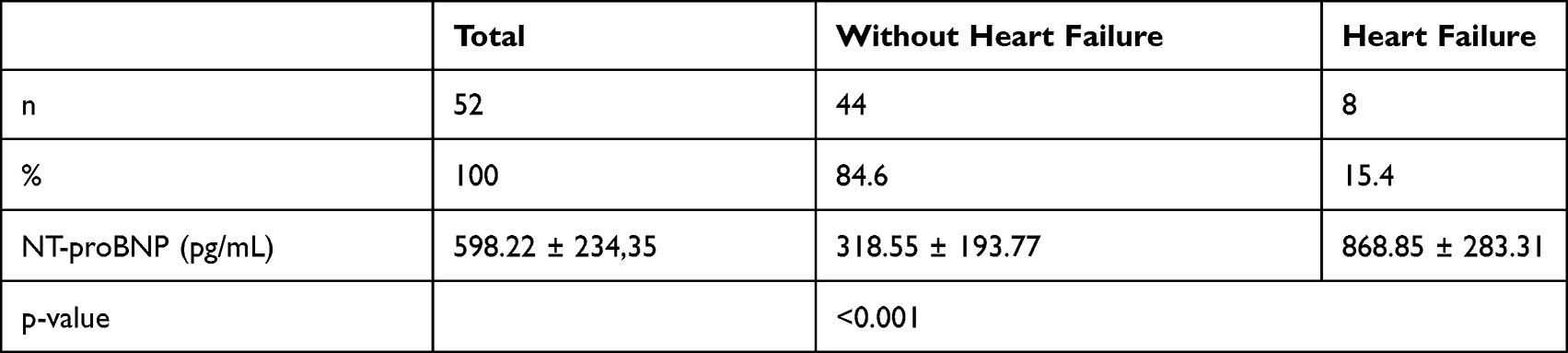 |
Table 7 Serum NT-proBNP Level by Heart Failure |
Discussion
Characteristics of Blood Pressure and Stage of Hypertension
The systolic and diastolic blood pressure in our study was 165.7 ± 14.5mmHg and 100.6 ± 8.5mmHg, respectively. According to Euliano et al, the mean SBP in the group of healthy pregnant women, hypertension and preeclampsia was 117.7 ± 1.9 mmHg, 134.8 ± 11.4 mmHg and 146.2 ± 15.0 mmHg, respectively. In the study of Kale et al, the mean SBP of preeclampsia patients was 154.5 ± 5.6 mmHg, while the DBP was 98.2 ± 3.4 mmHg.7,8 Thus, compared with the two studies, the SBP and DBP in our study were not significantly higher. Thereby, it is shown that patients with preeclampsia often have very high blood pressure, which is one of the cardiovascular risk factors.
During pregnancy, high blood pressure gives rise to various complications for mother and fetus as the cause of preeclampsia, poor fetal growth, stillbirth, bleeding disorders, and future cardiovascular risks of pregnant women. Periodic antenatal check-ups allow timely screening and treatment of preeclampsia, reducing complications and mortality rates for the mother and fetus.2
In our study, the rate of hypertension in stage 3, stage 2 and stage 1 accounted for 46.1%, 32.7% and 21.2%, respectively. There was a difference in hypertension classification between the two groups of preeclampsia – with and without severe signs – and this difference was statistically significant. According to ACOG 2019 and National Institute for Health and Care Excellence (NICE) 2011, preeclampsia has severe signs in the presence of severe hypertension.1,9 Thus, our study is consistent with ACOG and NICE, which means that preeclampsia with severe signs frequently falls into hypertension stage 2 and stage 3. Therefore, blood pressure treatment is crucially necessary for each patient with preeclampsia to reduce the degree of hypertension, which is the expectation of obstetricians and cardiologists.
Cardiovascular Features
Through the study of 52 participants with preeclampsia, we recorded that the average Sokolow-Lyon index was 21.73 ± 4.52mm. There was no statistically significant difference between the preeclampsia group without severe signs and preeclampsia with severe signs. In the study of Zangeneh et al on 123 people, 48 patients with preeclampsia without severe signs, and the 33 with severe signs, 42 healthy pregnant women recorded no difference in Sokolow-Lyon index between groups. Another study of Paget et al on 684 patients with hypertension without symptoms or history of cardiovascular disease from 1998 to 2008 recorded an average value of Sokolow-Lyon index at 23 mm, without signs of left ventricular hypertrophy on ECG, while the NT-proBNP level was elevated and there were implications of left ventricular hypertrophy on echocardiography. As a result, NT-proBNP is an independent biomarker to detect left ventricular hypertrophy when not seen on ECG.10,11 Because the presence of left ventricle hypertrophy will change the workflow of caring after birth, and echocardiography is not a routinely applied exam during pregnancy, including women with preeclampsia, we recommend performing an echocardiography in chronic hypertension women at the beginning of prenatal care, or at least an ECG.
Many studies have documented that circulation volumes are 9–21% lower in pre-eclamptic hypertension patients than in pregnant women without hypertension. The systolic and diastolic blood pressure in hypertension patients with preeclampsia is higher than in healthy pregnant women. Left ventricular hypertrophy is not detected early on ECG but only on echocardiography and several biomarkers. The early detection of cardiac structural changes in expectant women with preeclamptic hypertension contributes to diagnosis and treatment, a reduction in long-term cardiovascular risk, and a reduction in maternal and fetal mortality.12
In our study, LVMI in patients with preeclampsia without severe signs was 92.27 ± 14.56 and LVMI in those with severe signs was 120.68 ± 16.47g/m2. Research of Reddy et al, left ventricular mass index in the expectants with preeclampsia increased by 4.25 g/m2, while there was a rise of only 0.03 g/m2 of the index in healthy pregnant women. Dennis’ study on left ventricular mass index (LMVI) between the group of non-pregnant women, healthy pregnant women and the group of preeclampsia was 97.0 ± 24.7g, 130.8 ± 21.0g and 189.1 ± 40.1g, respectively, the difference between the three groups was statistically significant with p < 0.01. Therefore, the indexes on echocardiography in women with preeclampsia are higher than in healthy pregnant women. This suggests that the heart of patients with preeclampsia must rapidly adapt to acute pressure overload by increasing wall thickness.13,14
According to Yuan et al, the LVMI in healthy pregnant women and pregnant women with preeclampsia with severe signs were 96.3 ± 17.8g/m2 and 110.9 ± 29g/m2, respectively. The difference was statistically significant with p < 0.01.15 Left ventricular hypertrophy is an independent cardiovascular risk factor in all patients with preeclampsia, and its early detection plays an important role in prompt hypertension control. ECG is recommended for the evaluation of hypertensive complications; however, due to its low sensitivity and specificity, echocardiography has higher sensitivity and specificity in diagnosing left ventricular hypertrophy, but it is not routinely applied in all hypertension patients. Some authors recently studied NT-proBNP in the diagnosis and early detection of left ventricular hypertrophy and left ventricular diastolic dysfunction in women with preeclampsia.10,16,17
In our study, there were three cases of EF less than 45%, accounting for 5.8%, with 2 cases of class 2 heart failure and 1 case of class 3 heart failure, similar to the study of Yuan et al. Mass overload often leads to an increase in ventricular volume, pressure overload will lead to an increase in left ventricular muscle mass, which alter ventricular shape, cardiac morphology and structure.15 In healthy pregnant women, there is a change in the morphology of the mother’s heart structure. Still, it is only physiological, whereas in patients with preeclampsia, this change, if not controlled, will be closely related to future cardiovascular diseases such as hypertension, myocardial ischemia, diastolic heart failure, myocardial damage and even death.4,10
Serum NT-proBNP Level
The average concentration of NT-proBNP in our study was 598.22 ± 234.35 pg/dL. The concentration of NT-proBNP between the two groups of preeclampsia patients without severe signs and those with severe signs had a statistically significant difference with p < 0.05. According to the study of Fustaret et al, the average concentration of NT-proBNP in the group of participants with pre-existing hypertension, HELLP syndrome and chronic hypertension was 936 pg/mL, 1909 pg/mL and 107 pg/mL, respectively, the highest level of serum NT-proBNP was 12,386 pg/mL. The concentration of NT-proBNP in the groups was statistically significant with p < 0.01.18
A study of Fleming et al on 24 pregnant hypertensive women and 42 healthy pregnant women showed that NT-proBNP concentration in the hypertension group and multiple pregnancies were higher than that in healthy pregnant women and their offspring. The difference was statistically significant with p < 0.01.19 Cardiac overload increases the secretion of cardiomyocyte diuretic peptides such as ANP, BNP and NT-proBNP. In which NT-proBNP is a substance with a long half-life and persistent in the blood. When excessively elevated, it reflects abnormalities in left ventricular diastolic function, systolic function and cardiac structure, especially in women with chronic heart failure. The changes in the vascular system in preeclampsia are not similar to those of normal pregnancy, but rather an increase in vasoconstriction, thereby increasing the burden on the heart and altering the function and structure of the left ventricle. In other words, high NT-proBNP concentrations in preeclampsia reflect the heart strain caused by increased afterload.20 On further research, Balenceanu, Tihtonen and Hamad all agree that in women with PE, NT-proBNP level and cardiovascular risk level have a strong positive correlation.17,20,21 For that reason, Balceanu and his team suggest carefully supervising pregnant women with high NT-proBNP concentration, both clinical and imaging.21 Recent studies have indicated that preeclampsia patients with severe signs have an increased risk of future cardiovascular disease than healthy women. In this study, we found out that in the group of women with preeclampsia, those with severe signs have a higher risk of developing cardiovascular problems than the participants who do not have severe signs. In addition, according to a study by Mogbeli et al, the NT-proBNP biomarker may help discriminating between women with and without hypertensive disorders of pregnancy.16
Despite many advances in the diagnosis and treatment of heart failure, the morbidity and mortality rates have only decreased in men, but still increased in women. That difference has been unknown, while risk factors such as smoking and obesity are the same. It is thought that factors such as estrogen, pregnancy, menopause and so on increase the risk of cardiovascular disease in women.2,4 In our study, the rate of participants without heart failure constituted 84.6%, whereas those with heart failure occupied 15.4%. There was a statistically significant difference in the concentration of NT-proBNP between the two groups. According to Moghbeli, research showed that poor fetal growth and preeclampsia were two causes of long-term cardiovascular risk for the mother. Left ventricular diastolic dysfunction was found in healthy women, pregnant women with poor fetal growth and preeclampsia at the proportion of 4%, 28%, and 52%, respectively. Systolic dysfunction in healthy pregnant women, pregnant women with poor fetal growth and preeclampsia was at 0%, 4%, and 28%, distributively.16 Thus, patients with preeclampsia and eclampsia have a higher cardiovascular risk than healthy pregnant women. Tanous’s study on 78 hospitalized pregnant women showed there were 66 pregnant women with heart disease and 12 healthy pregnant women. According to NYHA grade I, grade II and grade III or higher, the rate of heart failure made up 82%, 15% and 3%, respectively.22 Another study of Roos-Hesselink on 1321 pregnant women with heart disease, over 60 hospitals in 28 countries from 2007 to 2011 recorded 72% of women with grade I heart failure, of which, 66% with congenital heart disease, 25% with valvular disease, 7% with cardiomyopathy, 2% with ischemic heart disease. Thus, the rate of cardiovascular disease in women with preeclampsia is quite high, it is very necessary to find a biomarker like NT-ProBNP to screen for cardiovascular disease in pregnant women.23
Conclusion
Through the study of 52 women with preeclampsia, we found that the rate of high-stage hypertension in these participants was very high, with hypertension stage 2 and stage 3 accounting for 78.8%. The rate of heart failure amounted to 15.4%, the Sokolow-Lyon index was not an early sign of left ventricular hypertrophy, while the increase of the left ventricular muscle mass index between the two groups of preeclampsia was statistically significant. The concentration of NT-proBNP was increased in the preeclampsia group with severe signs and in pregnant women with heart failure. Therefore, women with preeclampsia with severe signs have a higher risk of developing cardiovascular problems compared to those with preeclampsia without severe signs.
Ethics Approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by The Ethics Committee of Hue Central Hospital. A written consent form was obtained from all participants after explaining the aims of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest regarding the contents of this article nor this work.
References
1. Croke L. Gestational Hypertension and Preeclampsia: a Practice Bulletin from ACOG. Am Fam Physician. 2019;100(10):649–650.
2. Leon LJ, McCarthy FP, Direk K, et al. Preeclampsia and cardiovascular disease in a large UK pregnancy cohort of linked electronic health records: a CALIBER study. Circulation. 2019;140(13):1050–1060.
3. Kumari S, Gupta M, Vardhan H, Saini V, Gupta S, Research D. NT-PROBNP: a Biochemical Marker of Maternal Complications in Pre-eclampsia. J Clin Diagnostic Res. 2017;11(11):34.
4. Seong WJ, Kim SC, Hong DG, Koo TB, Park I. Amino-terminal pro-brain natriuretic peptide levels in hypertensive disorders complicating pregnancy. Hypertension Pregnancy. 2011;30(3):287–294.
5. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726.
6. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013;122(5):1122–1131.
7. Euliano TY, Michalopoulos K, Singh S, et al. Photoplethysmography and Heart Rate Variability for the Diagnosis of Preeclampsia. Anesth Analg. 2018;126(3):913–919.
8. Kale A, Kale E, Yalinkaya A, Akdeniz N, Canoruc N. The comparison of amino-terminal probrain natriuretic peptide levels in preeclampsia and normotensive pregnancy. J Perinat Med. 2005;33(2):121–124.
9. Webster K, Fishburn S, Maresh M, Findlay SC, Chappell LC, Guideline C. Diagnosis and management of hypertension in pregnancy: summary of updated NICE guidance. BMJ. 2019;366:l5119.
10. Paget V, Legedz L, Gaudebout N, et al. N-terminal pro-brain natriuretic peptide: a powerful predictor of mortality in hypertension. Hypertension. 2011;57(4):702–709.
11. Zangeneh M, Veisi F, Malekkhosravi S, et al. Electrocardiographic changes in healthy and preeclamptic pregnant women. J Kermanshah Univ Med Sci. 2012;16(4):e78789.
12. Ferrazzi E, Stampalija T, Monasta L, Di Martino D, Vonck S, Gyselaers W. Maternal hemodynamics: a method to classify hypertensive disorders of pregnancy. Am J Obstet Gynecol. 2018;218(1):124e121–124 e111.
13. Therese DA. Cardiac function in women with preeclampsia. University of Melbourne, Parkville, Australia. 2010;1:115–182.
14. Reddy M, Wright L, Rolnik DL, et al. Evaluation of Cardiac Function in Women With a History of Preeclampsia: a Systematic Review and Meta-Analysis. J Am Heart Assoc. 2019;8(22):e013545.
15. Yuan L-J, Duan -Y-Y, Xue D, Cao T-S, Zhou NJB. Ultrasound study of carotid and cardiac remodeling and cardiac-arterial coupling in normal pregnancy and preeclampsia: a case control study. BMC Pregnancy Childbirth. 2014;14(1):1–8.
16. Moghbeli N, Srinivas SK, Bastek J, et al. N-terminal pro-brain natriuretic peptide as a biomarker for hypertensive disorders of pregnancy. Am J Perinatol. 2010;27(04):313–319.
17. Rafik Hamad R, Larsson A, Pernow J, Bremme K, Eriksson MJ. Assessment of left ventricular structure and function in preeclampsia by echocardiography and cardiovascular biomarkers. J Hypertens. 2009;27(11):2257–2264.
18. Fustaret MC, Escobar A, Illia R, et al. PP113. NT-Pro-BNP: a predictor of adverse maternal outcomes in hypertensive gestational syndromes? Pregnancy Hypertension. 2012;2(3):301.
19. Fleming SM, O’Byrne L, Grimes H, Daly KM, Morrison JJ, Morrison J. Amino-terminal pro-brain natriuretic peptide in normal and hypertensive pregnancy. Pregnancy Hypertension. 2001;20(2):169–175.
20. Tihtonen KM, Koobi T, Vuolteenaho O, Huhtala HS, Uotila JT. Natriuretic peptides and hemodynamics in preeclampsia. Am J Obstet Gynecol. 2007;196(4):328 e321–327.
21. Balaceanu A. B-type natriuretic peptides in pregnant women with normal heart or cardiac disorders. Med Hypotheses. 2018;121:149–151.
22. Tanous D, Siu SC, Mason J, et al. B-type natriuretic peptide in pregnant women with heart disease. J Am Coll Cardiol. 2010;56(15):1247–1253.
23. Roos-Hesselink JW, Ruys TP, Stein JI, et al. Outcome of pregnancy in patients with structural or ischaemic heart disease: results of a registry of the European Society of Cardiology. Eur Heart J. 2013;34(9):657–665.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.