Back to Journals » Research Reports in Clinical Cardiology » Volume 17
Serum Levels of Caspase-3 Decrease in Patients with Long-Term Arrhythmia Suppression after PVI
Authors Szuromi L ![]() , Hajas O, Nagy-Baló E, Kovács-Forgács IN, Barta J, Nagy LT, Fagyas M, Tóth A, Nagy B Jr, Kappelmayer J, Csanádi Z
, Hajas O, Nagy-Baló E, Kovács-Forgács IN, Barta J, Nagy LT, Fagyas M, Tóth A, Nagy B Jr, Kappelmayer J, Csanádi Z
Received 24 January 2026
Accepted for publication 21 April 2026
Published 20 May 2026 Volume 2026:17 598392
DOI https://doi.org/10.2147/RRCC.S598392
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Chengming Fan
Lilla Szuromi,1 Orsolya Hajas,1 Edina Nagy-Baló,1 Ildikó N Kovács-Forgács,1 Judit Barta,1 László T Nagy,1 Miklós Fagyas,1 Attila Tóth,1 Béla Nagy Jr,2 János Kappelmayer,2 Zoltán Csanádi1
1Department of Cardiology, Faculty of Medicine, University of Debrecen, Debrecen, Hungary; 2Department of Laboratory Medicine, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
Correspondence: Lilla Szuromi, Department of Cardiology, Faculty of Medicine, University of Debrecen, Debrecen, Hungary, Email [email protected]
Background: The success of pulmonary vein isolation (PVI) is limited with more advanced disease of the atrial myocardium which may develop due to aging, atrial fibrillation (AF), cardiac diseases and comorbidities leading to elevated atrial pressure. Our group has recently reported on long-term decrease in the levels of different biomarkers after PVI, potentially reflecting a reversal of the fibrotic process in the atria with arrhythmia control. Whether the presence of baseline comorbidities has a significant impact on long-term changes in the serum concentration of these substances is unknown.
Aim: Herein, we compared the levels of 4 biomarkers (CA-125, Caspase-3, Cathepsin L and Galectin-3) before and 3 years after successful PVI in patients with versus without comorbidities at baseline.
Methods: Serum concentrations of the 4 biomarkers were measured prospectively in consecutive patients undergoing PVI with any of 3 different techniques for paroxysmal/permanent AF 24 hours before and 3 years after ablation. Only patients free of AF recurrence at 3-year follow-up were included in this analysis.
Results: 28 men and 9 women (age 56.5 ± 9.2 years) were enrolled. Caspase-3 concentrations decreased significantly by the end of follow-up in patients without (from 500.9 (345.7– 719.5) to 340.5 (255.9– 387.3); p=0.016 as well as with comorbidities: from 623.8 (476.9– 751.4) to 447.7 (327.6– 636.9) p=0.039. Caspase-3 concentrations (pg/mL) were higher at 3-year follow-up in patients with versus without comorbidities: 447.7 (327.6– 636.9) vs 340.5 (255.9– 387.3); p=0.038. For Caspase-3, a significant overall time effect was observed (β=− 0.437, p=0.010), consistent with lower concentrations at 3-year follow-up after adjustment for age, sex, AF type, and ablation technique. No differences were measured with the other biomarkers.
Conclusion: Serum levels of Caspase-3 decreased in patients maintaining sinus rhythm after PVI regardless of the presence or absence of comorbidities, suggesting that it might be a sensitive biomarker indicating long-term arrhythmia suppression.
Keywords: pulmonary vein isolation, atrial fibrillation, arrhythmia recurrence, biomarkers of atrial myopathy, Caspase-3
Introduction
Major components in the pathomechanism of atrial fibrillation (AF) include small reentrant or rapidly firing foci in sleeves of atrial muscle intruding into the pulmonary veins (PVs) and multiple areas of reentry facilitated by structural and electrical abnormalities in the atrial wall. Fibrosis that develops with aging and atrial hypertrophy in response to cardiac diseases and other comorbidities are considered significant factors promoting the latter mechanism. Different catheter ablation techniques developed to isolate the PVs offer long-term symptom control for AF patients with PV triggers being the dominant mechanism in initiating or sustaining the arrhythmia, while PV isolation (PVI) alone is less successful in more advanced stages of atrial myopathy. Identifying atrial myopathy would therefore promote proper patient selection for AF ablation with a PVI only approach. Further, data support that atrial myopathy might also be related to the risk of thromboembolic complications in AF patients.1–4
In clinical practice, imaging techniques (echocardiography, Cardiac Computed Tomography (CCT) and cardiac magnetic resonance imaging (MRI) with late gadolinium enhancement are routinely used to assess the size of the atria and the presence of fibrosis in the atrial myocardium. Furthermore, the clinical value of different biomarkers sensitive to the progress of myocardial fibrosis has also been investigated. The levels of cancer antigen 125 (CA-125), Galectin-3, Caspase-3, and Cathepsin L have been studied in variable cohorts, including patients with persistent and long-standing persistent forms of AF with significant comorbidities, such as hypertension, diabetes, coronary artery disease and chronic heart failure (HF).5–13
Recently, our group reported on the potential use of these substances in predicting the long-term success of PVI with different techniques.14 Our results demonstrated that pre-ablation levels of CA-125, Caspase-3, Cathepsin L and Galectin-3 were not significant predictors of AF recurrence after PVI. However, as a novel finding of this research, Galectin-3, Caspase-3, and Cathepsin L demonstrated a significant decrease 3 years after the ablation in patients with as well as in those without arrhythmia recurrence. Additionally, Caspase-3 levels demonstrated a positive correlation with left atrial (LA) dimensions in patients with AF recurrence. These results suggest that bidirectional changes in the levels of these biomarkers may be related to the progression of atrial fibrosis. Long-term freedom from atrial arrhythmias or a significant decrease in the arrhythmia burden may halt progression or even promote the healing process in the atrial myocardium reflected by a decrease in biomarker levels. In addition to the role of atrial arrhythmias, comorbidities like hypertension, diabetes, coronary artery disease (CAD), heart failure are also associated with progressive deterioration of the myocardium structure in the left and right atrium. Whether the change in the serum levels of these substances could be used as an indicator of long-term arrhythmia suppression regardless of the presence or absence of baseline comorbidities has not been studied.
Herein, we measured the levels of CA-125, Caspase-3, Cathepsin L and Galectin-3 before and 3 years after AF ablation to study the relationship between baseline comorbidities and the long-term changes in their concentrations potentially related to the fibrotic process in the atrial myocardium.
To exclude the confounding effect of arrhythmias, we analysed only patients who stayed free of atrial arrhythmias during follow-up, since atrial fibrosis may relate to arrhythmia burden itself. The specific question posed by this research was whether the levels of the 4 biomarkers decrease after efficient rhythm control regardless of the presence of comorbidities.
Materials and Methods
Patients
Consecutive patients undergoing PVI for documented AF at the Cardiology Department of the University of Debrecen were considered prospectively between 2018 March and 2022 December.
Patients were included in this research based on the following criteria:
- Patient underwent a single PVI procedure for paroxysmal or persistent AF with any of the following techniques: phased radiofrequency (RF) ablation with the 2nd generation pulmonary vein ablation catheter (PVAC Gold), cryoablation (CRYO) with the Arctic Front Advance catheter or point-by-point PVI with focal irrigated RF ablation using a Thermocool, Smarttouch catheter.
- Post-ablation follow-up data for at least 3 years were available including information on arrhythmia recurrence.
- Sinus rhythm (SR) was documented on all electrocardiograms (ECG) and no symptoms suggesting AF recurrence occurred throughout the entire post-ablation follow-up.
- Results of serum levels of CA-125, Caspase-3, Cathepsin L and Galectin-3 measured before the ablation as well as at the end of the 3-year follow-up were available.
- Patient signed a written informed consent to participate in the study before the ablation procedure.
Exclusion criterion:
Patients with long-standing persistent AF were excluded from this analysis.
The study design was in accordance with the guiding principles of the Declaration of Helsinki and was approved by the National Institute of Pharmacy and Nutrition (OGYÉI/12743/2018).
Baseline Cardiac Evaluation
History was taken with special attention to record previous diagnosis and treatment for comorbidities including hypertension (blood pressure>140/90 mmHg), HF, diabetes (HbA1c≥6.5%), coronary artery disease, previous stroke or Transient Ischemic Attack (TIA). The presence of any of these conditions was validated by careful review of the medical documentation of each patient and by evaluation of symptoms. Further diagnostic exams were also performed if indicated before ablation including laboratory tests, blood pressure monitoring, imaging techniques, coronary angiography and treatment of these comorbidities were optimized in line with contemporary guideline recommendations.
All patients underwent baseline evaluation, including transthoracic echocardiography (TTE) to measure left ventricular ejection fraction (LVEF) and LA diameters. Transoesophageal echocardiography was performed prior to the procedure to exclude the presence of a cardiac thrombus. Blood samples for the measurement of biomarkers were collected from a peripheral vein within 24 hours before the procedure.
Ablation Procedure
Catheter ablation protocols for PVI at our centre have been described in detail.14–17 Briefly, procedures were performed under conscious sedation using the standard technique for left atrial catheterization. PVI was then performed using any of 3 methods based on the operator’s preference: (1) Phased RF ablation with the 2nd generation PVAC-Gold catheter; (2) CRYO with the Arctic Front Advance catheter; (3) point-by-point ablation with focal irrigated RF ablation using a Thermocool, Smart-touch catheter. The procedural endpoint was the isolation of all PVs verified with pacing.
Laboratory Measurements of Biomarkers
Blood samples were collected into vacutainer tubes within 24 hours before and 3 years after the ablation. Tubes containing ethylenediamine tetra acetic acid (EDTA) anticoagulant and tubes containing clot activator (serum tubes with polymer gel separator, SST; Becton Dickinson, Franklin Lakes, NJ) were used. Within two hours, the samples were centrifuged at 1500 g for 20 minutes at room temperature. From EDTA tubes the plasma phase was pipetted, from serum separator tubes the serum phase was pipetted into aliquots and these were stored at −70°C until the analysis.
Serum CA-125 levels were determined by an electro-chemiluminescent microparticle immunoassay (Cobas® e602) (Roche Diagnostics, Mannheim, Germany). Plasma Caspase-3 concentration was measured with Human Caspase 3 enzyme-linked immunosorbent essay (ELISA) kit (Thermo Fisher, Cat. No. BMS2012INST), while plasma Galectin-3 was measured with Human Galectin-3 DuoSet ELISA kit (R&D System, Cat. No. DY1154) and plasma Cathepsin L with Human Cathepsin L DuoSet ELISA kit (R&D System, Cat. No. DY952).
Post-Ablation Follow-Up
Follow-up visits at every 6 months included 12-lead ECG and 24-hour Holter recordings. In addition, patients were asked to have an ECG recorded whenever they felt palpitation or other symptoms compatible with an AF episode. Furthermore, patients were provided with trans-telephonic monitors for up to 6 weeks to document the ECG during palpitation. Any documented episode of atrial arrhythmia lasting more than 30 seconds was considered a recurrence. LVEF and LA diameters were measured with TTE at the 3-year follow-up.
Statistical Analysis
Patients were categorized into 2 groups based on the presence or absence of significant comorbidities at baseline including hypertension, heart failure, diabetes, coronary artery disease, previous stroke or TIA. Statistical analysis was performed using GraphPad Prism version 8.0.0 for Windows (GraphPad Software, San Diego, CA, USA). Normality of data distribution was assessed with Kolmogorov–Smirnov test. Continuous variables are expressed as medians and interquartile range. Categorical data were presented as counts with percentages within brackets. Patients with missing values at the end of follow-up data were imputed by the last observation carried forward (LOCF) method. Analyses were calculated using Mann–Whitney test for continuous variables. To compare baseline and follow-up measurements, Wilcoxon test was applied. The differences between categorical variables were assessed by Fisher’s exact test or Chi-squared test. P<0.05 was considered statistically significant. Univariable regression analysis was applied to investigate independent associations between fibrosis biomarkers (dependent variables) and comorbidities (independent variables). The β standardized linear coefficients showing linear correlations between two parameters were determined. The B (+95% Cl) regression coefficient indicated independent associations between dependent and independent variables during changes. General linear model repeated measures analysis of variance (RM-ANOVA) was performed in order to determine the additional effects of comorbidities with the 3-year biomarker changes. Adjusted analyses were performed using linear mixed-effects models on log-transformed biomarker levels, with comorbidity group, time, and their interaction entered as fixed effects and patient as a random intercept. Models were adjusted for age, sex, AF type, and ablation technique.
Results
Baseline Patient and Procedure Characteristics
A total of 89 consecutive patients undergoing a first PVI procedure were approached to participate in the study. 77 patients out of 89 provided a written informed consent and had blood samples collected before the ablation. Follow-up data including the results of the repeat blood test were available in 63 patients. 26 out of these 63 had arrhythmia recurrence during follow-up and the 37 patients with no arrhythmia recurrence were included in this analysis. Patients with comorbidities were older (48 (42.3–60) years vs 59 (54.5–65) years; p=0.032). (Table 1). All the other parameters were comparable between the 2 groups. Acute isolation of all PVs was achieved in all patients in both groups with no complication.
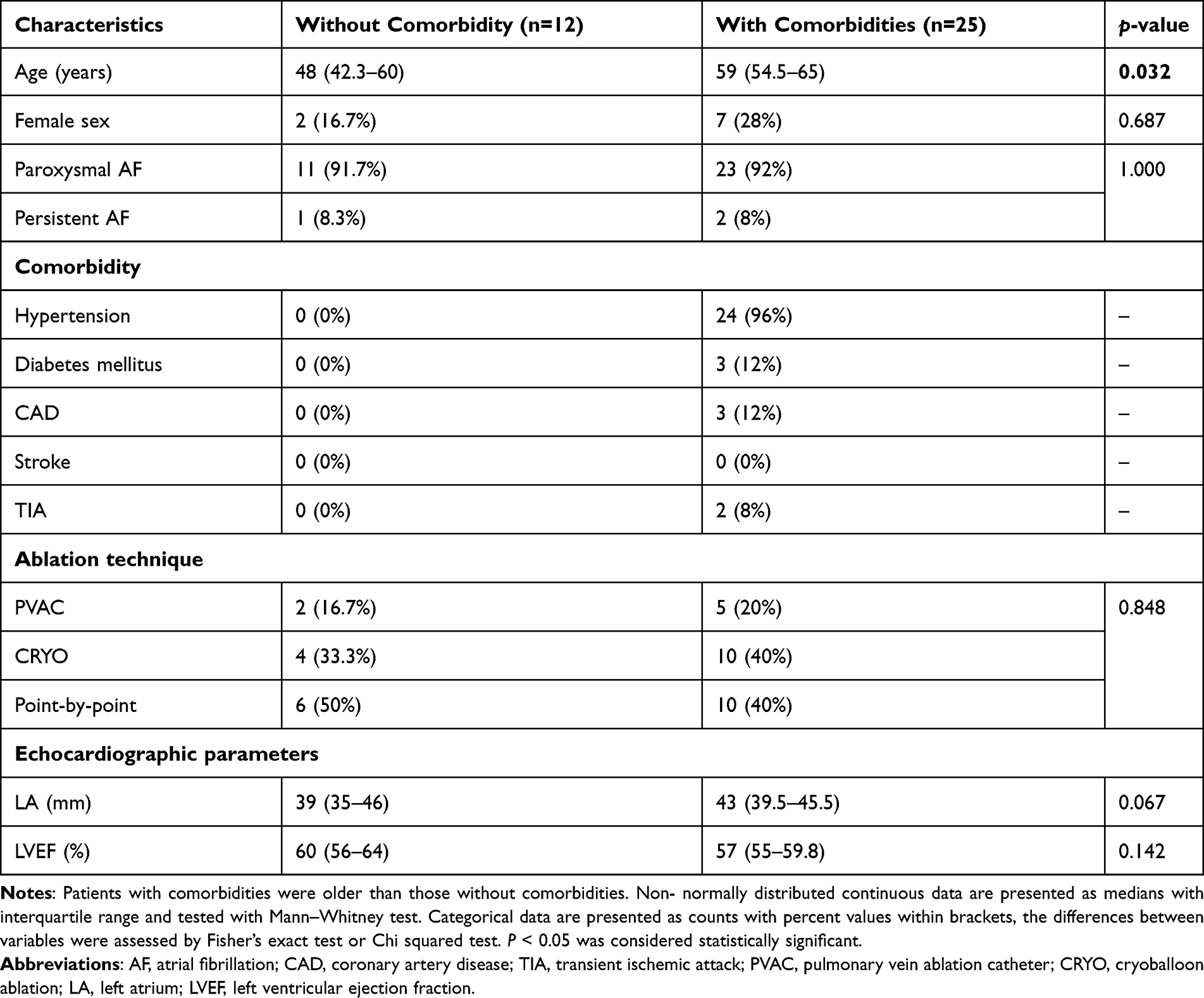 |
Table 1 Baseline Characteristics of Patients Without and with Comorbidities |
Biomarker Levels at Baseline and 3 years After the Ablation
Biomarker levels obtained before and 33.7±7.9 months after the ablation procedure were compared in patients with and without comorbidities. Where the given biomarker was below or above the cutoff value, it could not be used in the statistical analysis and it was not plotted in the figure.
Before the ablation the levels of CA-125, Galectin-3, Caspase-3 and Cathepsin L demonstrated no significant differences between the two groups. (Figure 1). At 3-year follow-up Caspase-3 levels were higher in the group with (447.7 (327.6–636.9) pg/mL) versus without (340.5 (255.9–387.3) pg/mL) comorbidities (p=0.038). (Figure 2). We performed univariable regression analysis using Caspase-3 follow-up levels as dependent, and comorbidities as independent variables. The only correlation found at 3-year follow-up was between hypertension and Caspase-3 levels (β=0.387; p=0.024; B= 181,54; 95% Cl= 25.6–337.5).
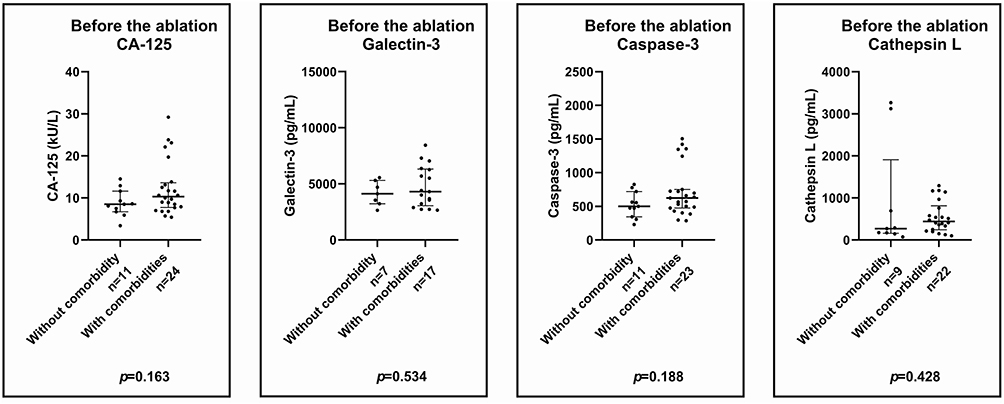 |
Figure 1 Comparison of baseline levels of CA-125, Galectin-3, Caspase-3 and Cathepsin L in patients with and without comorbidities. Before the ablation there was no significant difference in biomarker levels in comparison with patients with and without comorbidities. Data are presented as medians with interquartile range. (Mann–Whitney test). |
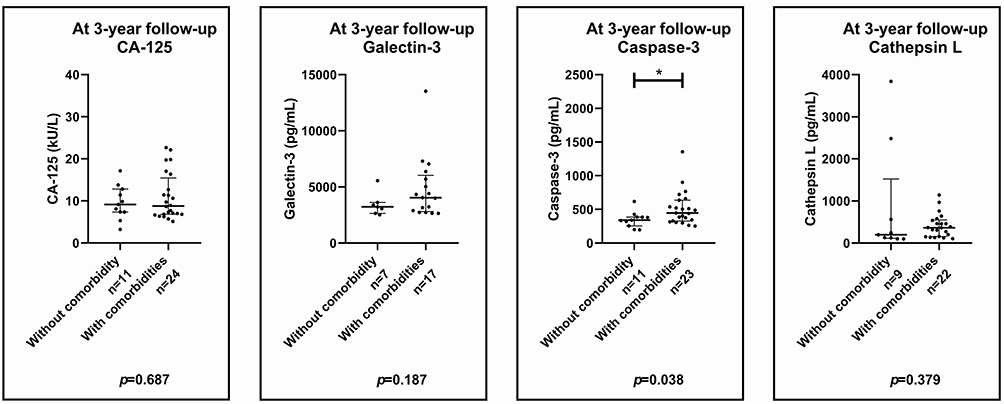 |
Figure 2 Comparison of 3-year post-ablation levels of CA-125, Galectin-3, Caspase-3 and Cathepsin L in patients with and without comorbidities. At 3-year follow-up the Caspase-3 levels were higher in patients with comorbidities. Data are presented as medians with interquartile range. p*<0.05 (Mann–Whitney test). |
Levels of the 4 biomarkers obtained at baseline were also compared to those obtained at the end of follow-up after PVI within each group. (Figure 3–4). Caspase-3 decreased significantly from the pre-ablation level by the end of follow-up in patients with (623.8 (476.9–751.4) pg/mL vs 447.7 (327.6–636.9) pg/mL, p=0.039) as well as without (500.9 (345.7–719.5) pg/mL vs 340.5 (255.9–387.3) pg/mL, p=0.016) comorbidity. No changes were demonstrated in CA-125, Galectin-3 and in Cathepsin-L levels either in patients with as well as without comorbidities. Based on RM-ANOVA tests, comorbidities had no additional effect on the 3-year biomarker changes.
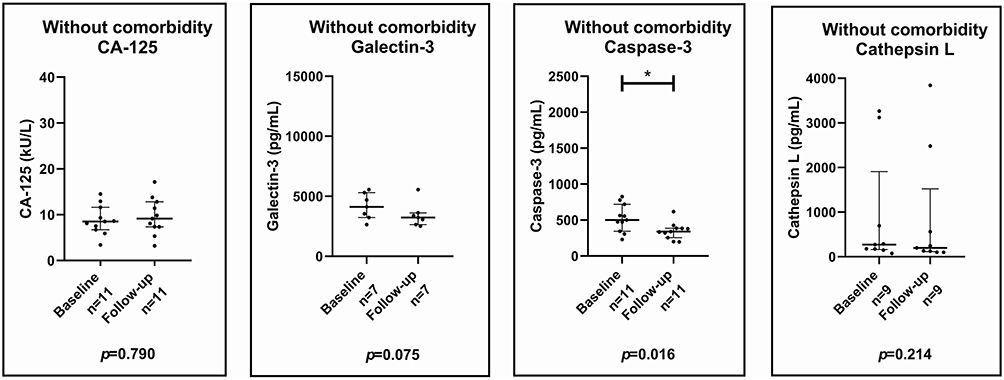 |
Figure 3 Changes in biomarker levels of CA-125, Galectin-3, Caspase-3 and Cathepsin L in patients without comorbidity from pre-ablation by the end of follow-up. Caspase-3 levels decreased significantly during the 3-year follow-up, while the other biomarker changes were not significant. Data are presented as medians with interquartile range. p*<0.05 (Wilcoxon test). |
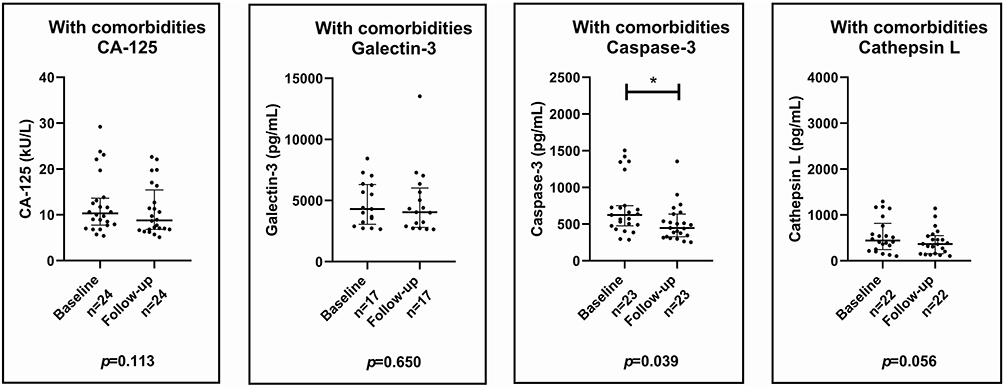 |
Figure 4 Changes in biomarker levels of CA-125, Galectin-3, Caspase-3 and Cathepsin L in patients with comorbidities from pre-ablation by the end of follow-up. The Caspase-3 levels decreased significantly during the 3-year follow-up, the other three biomarkers’ changes were not significant. Data are presented as medians with interquartile range. p*<0.05 (Wilcoxon test). |
In adjusted mixed-effects analysis, no significant comorbidity-by-time interaction was observed for CA-125 (p=0.262), Galectin-3 (p=0.273), Caspase-3 (p=0.570), or Cathepsin L (p=0.462), indicating that longitudinal biomarker changes did not differ significantly according to comorbidity status. For Caspase-3, a significant overall time effect was observed (β=−0.437, p=0.010), consistent with lower concentrations at 3-year follow-up after adjustment for age, sex, AF type, and ablation technique. (Table 2). The adjusted between-group difference in Caspase-3 at 3-year follow-up was not significant (p=0.114).
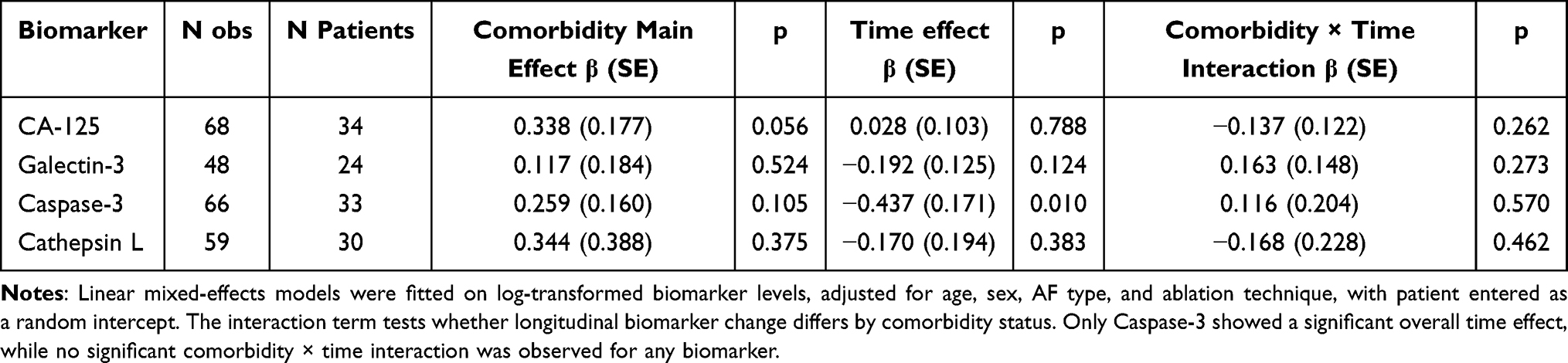 |
Table 2 Adjusted Mixed-Effects Analysis of Biomarker Changes According to Comorbidity Status |
Echocardiographic Parameters
LA diameter demonstrated no significant changes 3 years after the ablation as compared with baseline either in patients without (39 (35–46) mm vs 39 (35–41.5) mm; p=0.973) or with (43 (39.5–45.5) mm vs 42.5 (38–45) mm; p=0.177) comorbidities respectively. Similarly, no significant changes were observed in LVEF between these timepoints either in patients without (60 (56–64)% vs 58.5 (55–62)%; p=0.219) or with (57 (55–59.8)% vs 56 (54.3–59.5)%; p=0.930) comorbidities.
Discussion
Main Findings
In this study, the 4 biomarkers we tested demonstrated no difference between patients who did versus those who did not have comorbidities at the time of PVI. Caspase-3 decreased significantly from the pre-ablation level by the end of the 3-year follow-up in both patient groups, although its concentration was higher in patients with comorbidities. Serum levels of the 3 other biomarkers did not change with time in either patient group. Hypertension was the dominant baseline comorbidity which demonstrated a significant correlation with Caspase-3 levels at 3-year follow-up. Interaction analysis showed no significant interaction between comorbidities and time on the change in Caspase-3 levels (p > 0.05).
Clinical Significance of Biomarkers in Atrial Fibrillation
Atrial myopathy can be defined as any structural and electrical alterations within the atrial myocardium. The term was first introduced by Zipes in 1997 suggesting a close relationship between AF and remodeling of the atria.18 As of today, the relationship between AF and atrial myopathy is considered bidirectional: atrial myopathy may develop due to or in the absence of AF and may also contribute to the development of the arrhythmia. Although atrial myopathy has recently been considered crucial in the pathophysiology of AF, the assessment of its progress in clinical practice remains challenging. Imaging techniques (delayed gadolinium enhancement cardiac MRI, multi-detector cardiac computed tomography (MDCT), LA strain echocardiography) have been proposed to characterize the atrial wall and guide clinical decisions to select patients for AF ablation and to assess the risk of later comorbidities like stroke and HF.19 The dynamics of fibrotic alterations are a critical component of the progression of atrial myopathy thereby serial measurement of fibrosis-related substances in the human plasma might portend the course of the disease. In addition to the information provided by imaging techniques, these biomarkers may provide a simple, fast and less expensive way of assessment for the routine clinical practice even for population-based screening. For example, in the STROKESTOP II trial,20 the low level of N-terminal pro b-type natriuretic peptide (NT-pro-BNP) identified patients with negligible stroke risk not justifying anticoagulation therapy regardless of the findings of long-term ECG monitoring. Identifying other markers indicative of the extent of the fibrotic process in the atrial wall could possibly open new routes to stratify the stroke risk beyond the CHADS2-VA-score as well as to promote more specific patient selection for various methods of arrhythmia suppression and to monitor the long-term effect of these therapies.
Our Results in the Context of Published Data
Based on preclinical studies, all 4 biomarkers studied in our research have been linked to fibrosis and inflammation of the atrial myocardium. Eiras et al found positive association between epicardial cell CA-125 expression with inflammatory and fibroblast markers21 Sun et al reported that Cathepsin L regulates cardiac repair and remodeling in post-myocardial infarction mice models22 In a pig model of rapid atrial pacing knock-out of the Caspase-3 gene suppressed or delayed AF as compared with controls.23 Some preclinical studies described the role of Caspase-3 in apoptosis, myofibroblast differentiation and in cardiac remodelling.24–27 Galectin-3 increased atrial fibroblast proliferation, atrial dilatation and atrial fibrosis.13
In humans, elevated serum levels of these biomarkers were measured with different forms of AF, mostly associated with comorbidities like HF or valvular disease. (Table 3). CA-125 is known as a tumor marker, but recently it has also been related to AF.28 Yilmaz et al described an association between higher CA-125 and higher AF burden29 Cheung’s meta-analysis demonstrated elevated CA-125 levels with 1.39 times higher risk of AF. The limitation of this meta-analysis was the heterogeneity of comorbidities.5 In Dudink’s original research, levels of CA-125 and Cathepsin L were associated with a higher risk of AF in patients even without known cardiovascular disease.6 Before our work, this was the only report on Cathepsin L in the context of AF or PVI.7 The role of Caspase-3 in AF is not well described. In permanent AF increased Caspase-3 concentrations were found as compared with SR in patients with rheumatic heart disease.8 Our previous study demonstrated a correlation between Caspase-3 levels and LA dimensions.14 Elevated levels of Galectin-3 were reported in patients with HF and persistent AF. Clementy et al described the predictive value of Galectin-3 levels after PVI in patients with systolic HF12 In another research higher baseline Galectin-3 levels were predictive for AF recurrence at 1-year follow-up, in the presence of comorbidities and persistent AF at baseline.11 Although it seems reasonable to assume, that atrial myopathy is a progressive disease related to aging, comorbidities and AF burden and thereby plasma concentrations of substances related to this pathophysiological process may increase with time, none of these studies reported on the long-term changes in the levels of these biomarkers.
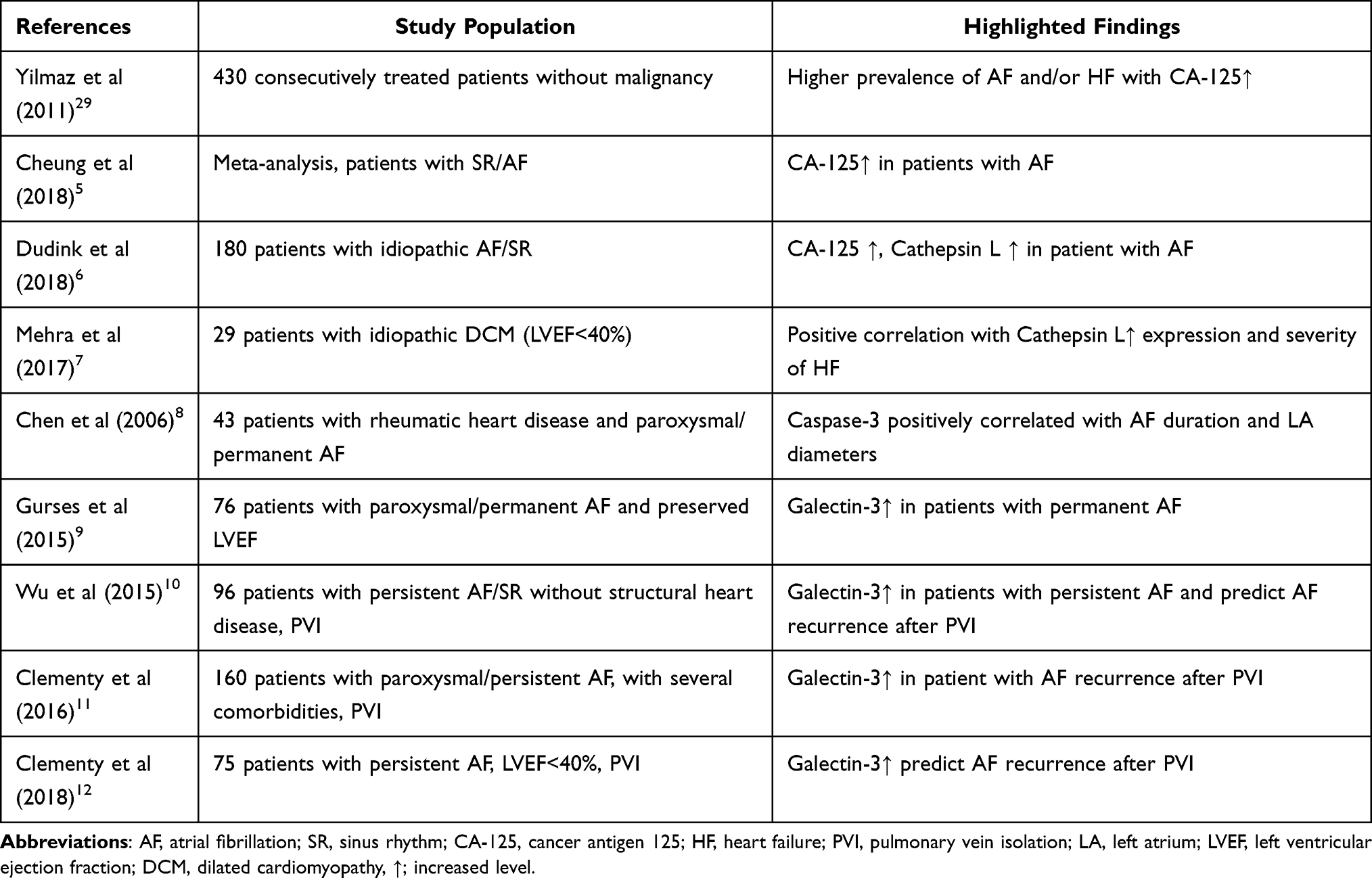 |
Table 3 Biomarkers with Elevated Levels in Atrial Fibrillation in Human Studies |
The only available data on the long-term changes in serum concentrations of these substances was published by our group14 In a cohort of 63 patients who underwent PVI a significant decrease was demonstrated by the end of a 3-year follow-up with Galectin-3, Cathepsin-L and Caspase-3 Importantly, these changes were uniformly observed in patients who did and in those who did not have arrhythmia recurrence As a novel finding, these results suggest that the longitudinal changes in biomarker concentrations are not necessarily unidirectional, and serum levels may also decrease in case of successful arrhythmia control achieved either with catheter-based techniques like in our patients or with medication A possible explanation we proposed was that the ongoing fibrosis in the atrial wall was halted or even reversed after the elimination (in the no recurrence group) or at least significant reduction (in the recurrence group) of AF episodes after PVI Favourable post ablation changes in LA dimensions supporting this concept have been demonstrated in several trials using cardiac MRI30–32 or 3-dimensional echocardiography.33
Importantly, in our previous study, patients with or without comorbidities were not analysed separately, although the influence of age, gender, cardiac and non-cardiac pathologies on biomarkers has been demonstrated.34 Therefore, the specific question posed in the current research was whether the presence or the absence of comorbidities at baseline had an impact on the long-term changes of these biomarkers in patients who had no recurrence after AF ablation, thereby the potential influence of atrial arrhythmias was less likely We found Caspase-3 to be the only biomarker which demonstrated significant decrease in the serum levels 3 years post-ablation regardless of the presence or the absence of comorbidities at the time of ablation.
To explain why only one out of the four substances demonstrated these changes, one may speculate that Caspase-3 might be a more sensitive marker of atrial myopathy related to AF than the others and could thereby be used in clinical practice as an indicator of effective arrhythmia control in patients with variable degree of fibrosis in the atrial wall in the absence or presence of comorbid conditions As of today, instant Caspase-3 ELISA tests are available although at a possibly high expense for routine use in clinical practice. However, we consider our observation only as hypothesis generating, awaiting confirmation by larger scale studies.
Limitations
This was a single center study on a limited number of patients decreasing the statistical power of our findings. Patients were categorized as no recurrence based on the absence of a symptomatic episode or an incidental detection of AF in the absence of continuous monitoring during follow-up. In a recent paper.35 Patients reporting on the results of continuous monitoring (implantable loop recorder) after CRYO ablation for paroxysmal/persistent AF only half of the patients with documented arrhythmia recurrence were symptomatic. However, the AF burden might be a more significant factor as far as atrial remodeling is concerned as opposed to shorter duration episodes which indeed are partially missed with routine, not continuous monitoring during-follow-up. Importantly, although patients with AF recurrence were excluded from this analysis, cohorts with versus without recurrence had similar baseline comorbidities, age and echocardiographic parameters as published earlier.14
Biomarker levels were measured before the ablation and only at 3-year follow-up providing no data on the time-course of changes in between. Although 3 different ablation technologies were applied in our patients, the potential effect of these methods on biomarker levels was not analyzed. However, while the acute myocardium injury caused by different energy sources may differ, this impact is unlikely to be reflected in the levels of sub-stances measured 3 years after the procedure. Of note, successful isolation of all PVs was achieved in all patients regardless of the ablation technique, thereby long-term changes in the measured biomarkers likely reflect pathological processes throughout the 3-year post-ablation period. Further, potential confounders such as differences in comorbidity management during post-ablation follow-up might have influenced our results.
Conclusion
In our study, serum levels of Caspase-3 decreased significantly in patients who demonstrated no recurrence after PVI regardless of the presence or absence of comorbidities, although at 3-year the Caspase-3 levels were higher in patients with comorbidities. If confirmed by further research, a decrease in Caspase-3 can serve as a dynamic monitoring indicator of therapeutic efficacy at the atrial myocardial level.
Abbreviations
AF, atrial fibrillation; CA-125, cancer antigen 125; CAD, coronary artery disease; CCT, Cardiac Computed Tomography; CRYO, cryoablation; ECG, electrocardiograms; EDTA, ethylenediamine tetra acetic acid; ELISA, enzyme-linked immunosorbent essay; HF, heart failure; LA, left atrial; LOCF, last observation carried forward; LVEF, left ventricular ejection fraction; MDCT, multi-detector cardiac computed tomography; MRI, magnetic resonance imaging; NT-pro-BNP, N-terminal pro b-type natriuretic peptide; PVAC, pulmonary vein ablation catheter; PVI, pulmonary vein isolation; PVs, pulmonary veins; RF, radiofrequency; RM-ANOVA, repeated measures analysis of variance; SR, sinus rhythm; TIA, Transient Ischemic Attack; TTE, transthoracic echocardiography.
Declaration of AI and AI Assisted Technologies in the Writing Process
During the preparation of this work the authors did not use AI Technologies.
Data Sharing Statement
The data sets generated and analysed in the current study are not publicly available due to institutional policies but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study design was in accordance with the guiding principles of the Declaration of Helsinki and was approved by the National Institute of Pharmacy and Nutrition (OGYÉI/12743/2018). Patients signed a written informed consent to participate in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Project no. TKP2021-EGA-18 has been implemented with the support of the National Research Development and Innovation Fund of Hungary, financed under the TKP2021-EGA funding scheme. Foundation to support cardiac catheterization, Debrecen, Hungary.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Haïssaguerre M, Jaïs P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339(10):659–12. doi:10.1056/NEJM199809033391003
2. Van Gelder IC, Rienstra M, Bunting KV, et al. ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2024;45(36):3314–3414. doi:10.1093/eurheartj/ehae176
3. Oakes RS, Badger TJ, Kholmovski EG, et al. Detection and quantification of left atrial structural remodeling with delayed-enhancement magnetic resonance imaging in patients with atrial fibrillation. Circulation. 2009;119(13):1758–1767. doi:10.1161/CIRCULATIONAHA.108.811877
4. Marrouche NF, Wilber D, Hindricks G, et al. Association of atrial tissue fibrosis identified by delayed enhancement MRI and atrial fibrillation catheter ablation: the DECAAF study. JAMA. 2014;311(5):498–506. doi:10.1001/jama.2014.3
5. Cheung A, Gong M, Bellanti R, et al. Cancer antigen-125 and risk of atrial fibrillation: a systematic review and meta-analysis. Heart Asia. 2018;10(1):e010970. doi:10.1136/heartasia-2017-010970
6. Dudink EA, Weijs B, Tull S, et al. The biomarkers NT-proBNP and CA-125 are elevated in patients with idiopathic atrial fibrillation. J Atr Fibrillation. 2018;11(4):2058. doi:10.4022/jafib.2058
7. Mehra S, Kumar M, Manchanda M, et al. Clinical significance of cathepsin L and cathepsin B in dilated cardiomyopathy. Mol Cell Biochem. 2017;428(1–2):139–147. doi:10.1007/s11010-016-2924-6
8. Chen YQ, Wang L, Su X, et al. Calpain-I, calpastatin, caspase-3 and apoptosis in the human left atrium in rheumatic atrial fibrillation. Zhonghua Xin Xue Guan Bing Za Zhi. 2006;34(4):303–307.
9. Gurses KM, Yalcin MU, Kocyigit D, et al. Effects of persistent atrial fibrillation on serum galectin-3 levels. Am J Cardiol. 2015;115(5):647–651. doi:10.1016/j.amjcard.2014.12.021
10. Wu XY, Li SN, Wen SN, et al. Plasma galectin-3 predicts clinical outcomes after catheter ablation in persistent atrial fibrillation patients without structural heart disease. Europace. 2015;17(10):1541–1547. doi:10.1093/europace/euv045
11. Clementy N, Benhenda N, Piver E, et al. Serum galectin-3 levels predict recurrences after ablation of atrial fibrillation. Sci Rep. 2016;6:34357. doi:10.1038/srep34357
12. Clementy N, Garcia B, André C, et al. Galectin-3 level predicts response to ablation and outcomes in patients with persistent atrial fibrillation and systolic heart failure. PLoS One. 2018;13(8):e0201517. doi:10.1371/journal.pone.0201517
13. Takemoto Y, Ramirez RJ, Yokokawa M, et al. Galectin-3 regulates atrial fibrillation remodeling and predicts catheter ablation outcomes. JACC Basic Transl Sci. 2016;1(3):143–154. doi:10.1016/j.jacbts.2016.03.003
14. Szuromi L, Hajas O, Nagy-Baló E, et al. Long-term changes in the biomarkers of left atrial fibrosis after pulmonary vein isolation for paroxysmal and persistent atrial fibrillation. Rev Cardiovasc Med. 2023;24(6):171. doi:10.31083/j.rcm2406171
15. Hajas O, Bagoly Z, Tóth NK, et al. Intracardiac fibrinolysis and endothelium activation related to atrial fibrillation ablation with different techniques. Cardiol Res Pract. 2020;2020:1570483. doi:10.1155/2020/1570483
16. Nagy-Baló E, Tint D, Clemens M, et al. Transcranial measurement of cerebral microembolic signals during pulmonary vein isolation: a comparison of two ablation techniques. Circ Arrhythm Electrophysiol. 2013;6(3):473–480. doi:10.1161/CIRCEP.112.971747
17. Kiss A, Nagy-Baló E, Sándorfi G, Edes I, Csanádi Z. Cerebral microembolization during atrial fibrillation ablation: comparison of different single-shot ablation techniques. Int J Cardiol. 2014;174(2):276–281. doi:10.1016/j.ijcard.2014.03.175
18. Zipes DP. Atrial fibrillation. A tachycardia-induced atrial cardiomyopathy. Circulation. 1997;95(3):562–564. doi:10.1161/01.CIR.95.3.562
19. De Sensi F, Penela D, Soto-Iglesias D, Berruezo A, Limbruno U. Imaging techniques for the study of fibrosis in atrial fibrillation ablation: from molecular mechanisms to therapeutical perspectives. J Clin Med. 2021;10(11):2277. doi:10.3390/jcm10112277
20. Katrin KG. STROKESTOP II trial (presented at European Society of Cardiology Congress, London, United Kingdom, (1 September 2024).
21. Eiras S, de la Espriella R, Fu X, et al. Carbohydrate antigen 125 on epicardial fat and its association with local inflammation and fibrosis-related markers. J Transl Med. 2024;22(1):619. doi:10.1186/s12967-024-05351-z
22. Sun M, Chen M, Liu Y, et al. Cathepsin-L contributes to cardiac repair and remodelling post-infarction. Cardiovasc Res. 2011;89(2):374–383. doi:10.1093/cvr/cvq328
23. Trappe K, Thomas D, Bikou O, et al. Suppression of persistent atrial fibrillation by genetic knockdown of caspase 3: a pre-clinical pilot study. Eur Heart J. 2013;34(2):147–157. doi:10.1093/eurheartj/ehr269
24. Porter AG, Jänicke RU. Emerging roles of caspase-3 in apoptosis. Cell Death Differ. 1999;6(2):99–104. doi:10.1038/sj.cdd.4400476
25. Laplante P, Sirois I, Raymond MA, et al. Caspase-3-mediated secretion of connective tissue growth factor by apoptotic endothelial cells promotes fibrosis. Cell Death Differ. 2010;17(2):291–303. doi:10.1038/cdd.2009.124
26. Yang B, Ye D, Wang Y. Caspase-3 as a therapeutic target for heart failure. Expert Opin Ther Targets. 2013;17(3):255–263. doi:10.1517/14728222.2013.745513
27. Philipp S, Pagel I, Höhnel K, et al. Regulation of caspase 3 and Fas in pressure overload-induced left ventricular dysfunction. Eur J Heart Fail. 2004;6(7):845–851. doi:10.1016/j.ejheart.2004.01.014
28. Zhang R, Jin W, Han M, Hou Y. Carbohydrate antigen 125 in atrial fibrillation. Clin Chim Acta. 2023;549:117550. doi:10.1016/j.cca.2023.117550
29. Yilmaz MB, Zorlu A, Tandogan I. Plasma CA-125 level is related to both sides of the heart: a retrospective analysis. Int J Cardiol. 2011;149(1):80–82. doi:10.1016/j.ijcard.2009.12.003
30. Assaf AY, Noujaim C, Mekhael M, et al. Early remodeling of the left atrium following catheter ablation of atrial fibrillation: insights from DECAAFII. JACC Clin Electrophysiol. 2023;9(11):2253–2262. doi:10.1016/j.jacep.2023.07.025
31. Jahnke C, Fischer J, Gerds-Li JH, et al. Serial monitoring of reverse left-atrial remodeling after pulmonary vein isolation in patients with atrial fibrillation: a magnetic resonance imaging study. Int J Cardiol. 2011;153(1):42–46. doi:10.1016/j.ijcard.2010.08.034
32. Hof IE, Velthuis BK, Chaldoupi SM, et al. Pulmonary vein antrum isolation leads to a significant decrease of left atrial size. Europace. 2011;13(3):371–375. doi:10.1093/europace/euq464
33. Müller H, Noble S, Keller PF, et al. Biatrial anatomical reverse remodelling after radiofrequency catheter ablation for atrial fibrillation: evidence from real-time three-dimensional echocardiography. Europace. 2008;10(9):1073–1078. doi:10.1093/europace/eun187
34. Nishimura M, Brann A, Chang KW, Maisel AS. The confounding effects of non-cardiac pathologies on the interpretation of cardiac biomarkers. Curr Heart Fail Rep. 2018;15(4):239–249. doi:10.1007/s11897-018-0398-4
35. Foti R, Di Silvestro M, Campisi G, et al. Continuous monitoring with implantable loop recorders after cryoballoon ablation: impact on atrial fibrillation recurrence and therapeutic management in era of artificial intelligence. J Clin Med. 2025;14(9):2932. doi:10.3390/jcm14092932
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Safety and Efficacy of Cryoballoon Pulmonary Vein Isolation and Left Atrial Appendage Closure Combined Procedure and Half-Dose Rivaroxaban After Operation in Elderly Patients with Atrial Fibrillation
Zhang X, Xing Z, Fang C, Yang M, Luo J, Ning Z
Journal of Multidisciplinary Healthcare 2023, 16:2603-2611
Published Date: 5 September 2023