")
Back to Journals » International Journal of General Medicine » Volume 15
Serum Endocan Levels and Subclinical Atherosclerosis in Behçet’s Syndrome
Authors Nassef EM, Elabd HA, El nagger BMMA, Elzomor HM, Kotb HG, Sabry S, Zaghloul BA, Hassan AS , Mohamed EES
Received 8 May 2022
Accepted for publication 4 August 2022
Published 18 August 2022 Volume 2022:15 Pages 6653—6659
DOI https://doi.org/10.2147/IJGM.S373863
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Eman Mostafa Nassef,1 Hemmat Ahmed Elabd,2 Basma Mohamed Mohamed Ali El nagger,2 Hala Mohamed Elzomor,2 Hend Gamal Kotb,1 Seham Sabry,1 Boshra Ahmed Zaghloul,3 Asmaa S Hassan,4 Eman El Sayed Mohamed4
1Internal Medicine Department, Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt; 2Rheumatology and Rehabilitation Department, Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt; 3Radiodiagnosis Department, Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt; 4Clinical Pathology Department, Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt
Correspondence: Eman Mostafa Nassef, Internal Medicine Department, Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt, Tel +20 1098002232, Email [email protected]
Background and Aim: Behçet disease (BD) is a rare chronic relapsing-remitting inflammatory systemic vasculitis. BD patients were reported to have marked acceleration of subclinical atherosclerosis (SCA). Endocan is a soluble proteoglycan mainly secreted by the activated endothelium. The present study aimed to assess the relation between serum endocan levels and SCA in BD patients.
Subjects and Methods: The study included 40 adult BD patients in addition to twenty age- and sex-matched healthy controls. BD was diagnosed according to International Study Group criteria. Upon recruitment, all participants were subjected to careful history taking and thorough clinical examination. BD activity was assessed using Behçet Syndrome Activity Score. Measurement of serum endocan was performed using quantitative double-antibody sandwich ELISA kit. CIMT measurement was done using B-mode ultrasound.
Results: Comparison between patients and controls regarding serum endocan levels revealed significantly higher endocan levels in BD patients [median (IQR): 155.0 (69.3– 610.0) versus 73.8 (51.9– 94.6)]. Using ultrasound assessment, SCA was found in 14 BD patients (35.0%). Comparison between patients with SCA and patients without regarding the clinical and laboratory data revealed that the former group had significantly higher CRP [median (IQR): 36.5 (26.8– 43.5) versus 21.0 (11.8– 26.8) mg/dL, p < 0.001] and endocan [median (IQR): 622.0 (107.4– 974.8) versus 104.5 (64.0– 342.0) mg/dL, p = 0.004] levels. Logistic regression analysis recognized endocan [OR (95% CI): 1.0 (1.0– 1.012), p0.035] levels as significant predictor of SCA in multivariate analysis.
Conclusion: The present study identified the clinical value of serum endocan levels as a possible early marker of vascular involvement in BD patients.
Keywords: Behçet’s disease, subclinical atherosclerosis, endocan
Introduction
Behçet disease (BD) is a rare chronic relapsing-remitting inflammatory systemic vasculitis with roughly equal sex distribution. The disease is claimed to be more common in countries located along the so-called “Silk Road” passing from East Asia to the Mediterranean through the Middle East.1 The exact pathological mechanisms involved in BD remain largely unknown. However, some evidence links BD to certain environmental, genetic and immunological alterations.2
Clinically, BD is characterized by the hallmarks of oral and genital ulcers. BD associated pathology may extend to include gastrointestinal tract, cardiovascular system, bony skeleton and central nervous system with some observed gender-related differences.3,4 However, growing evidence suggests that BD presentations can be classified into distinctive phenotypes. Vascular phenotype affects ~40.0% of patients with clear male predominance. Vascular affection entails small and large vessels of the venous and arterial systems.5,6 In fact, vascular complications may be one of the earliest manifestations leading to the diagnosis of BD.7
Besides these pronounced vascular complications, BD patients were reported to have a marked acceleration of subclinical atherosclerosis (SCA) when compared with their age-matched healthy counterparts. SCA was reported in BD patients even in the absence of major atherosclerosis risk factor8 and one study identified SCA in 32.0% of BD patients in comparison to only 7.0% in healthy individuals.9
Unfortunately, mechanisms involved in the development of SCA in BD patients are not fully understood and the identification of SCA in those patients may help predict future cardiovascular events.
Endocan is a soluble proteoglycan mainly secreted by the activated endothelium. Up-regulation of endocan is controlled by proangiogenic factors and proinflammatory cytokines and it is suggested that endocan itself may serve as a proinflammatory mediator contributing to endothelial dysfunction.10,11 In BD, endocan levels were found to be related to disease activity.12,13 Interestingly, previous reports documented an association between elevated endocan levels and SCA in many conditions, including systemic lupus erythematosus,14 type 2 diabetes mellitus15 and psoriatic disease.16
The present study aimed to assess the relation between serum endocan levels and SCA in BD patients.
Subjects and Methods
The present study was conducted at Al-Azhar University Hospitals, Cairo, Egypt in the time from January, through December, 2021. The study protocol was approved by the ethics committee of Al-Azhar Faculty of Medicine and informed consent was obtained from all participants before enrollment in line with the Declaration of Helsinki on clinical research involving human subjects.
The study included 40 adult BD patients in addition to twenty age- and sex-matched healthy controls. BD was diagnosed according to International Study Group criteria.17 Patients were excluded from the study if they had any cardiovascular or cerebrovascular diseases or possible related risk factors (eg diabetes, dyslipidemia, smoking). Other exclusions criteria were chronic conditions (eg chronic kidney disease, malignancy, autoimmune diseases). Pregnant women were also excluded.
Upon recruitment, all participants were subjected to careful history taking and thorough clinical examination. BD activity was assessed using the 10-item patient-reported Behçet Syndrome Activity Score.18 For laboratory assessment, 4 mL of peripheral venous blood was withdrawn from each individual and divided into two aliquots; 2 mL were collected in an EDTA tube for CBC. The remaining part was collected in a serum separator tube, centrifuged at 3500 rpm for 10 min and divided into two parts; the first part was used for biochemical tests and the remaining part of the serum was frozen at −20°C for analysis of endocan. Measurement of serum endocan was performed using quantitative double-antibody sandwich ELISA kit (Bioassay Technology Laboratory, China, Cat. No. E3160Hu). CIMT measurement was done using B-mode ultrasound with a high-definition L12-5 linear wideband probe (Philips HDI 5000, Bothell, Washington, USA). Patients were categorized as having SCA if their CIMT measurement was ≥0.9 mm or in the presence of carotid plaques (Figure 1).19
 |
Figure 1 (A) Longitudinal B-mode scan of the right common carotid artery at the level of atheromatous plaque showing about 50% stenosis. (B) Transverse B mode scan of the same lesion. |
Data were computerized and analyzed using IBM SPSS software package version 20.0. (IBM Corp, USA). Quantitative data were described using mean and standard deviation (SD) and were compared using t test. Qualitative data were presented in numbers and percentages and were compared using Fisher’s exact test or chi-square test as appropriate. Correlation analysis was achieved using Parsons’s correlation coefficient. P value less than 0.05 was considered statistically significant. Receiver operator characteristic (ROC) curve analysis was used to identify the diagnostic value of the investigated marker. Binary logistic regression was used to identify predictors of SCA. P value less than 0.05 was considered statistically significant.
Results
The present study included 40 adult BD patients and 20 age- and sex-matched healthy controls. Clinical and laboratory findings in the studied patients are shown in Table 1. Comparison between patients and controls regarding serum endocan levels revealed significantly higher endocan levels in BD patients [median (IQR): 155.0 (69.3–610.0) versus 73.8 (51.9–94.6), p < 0.001].
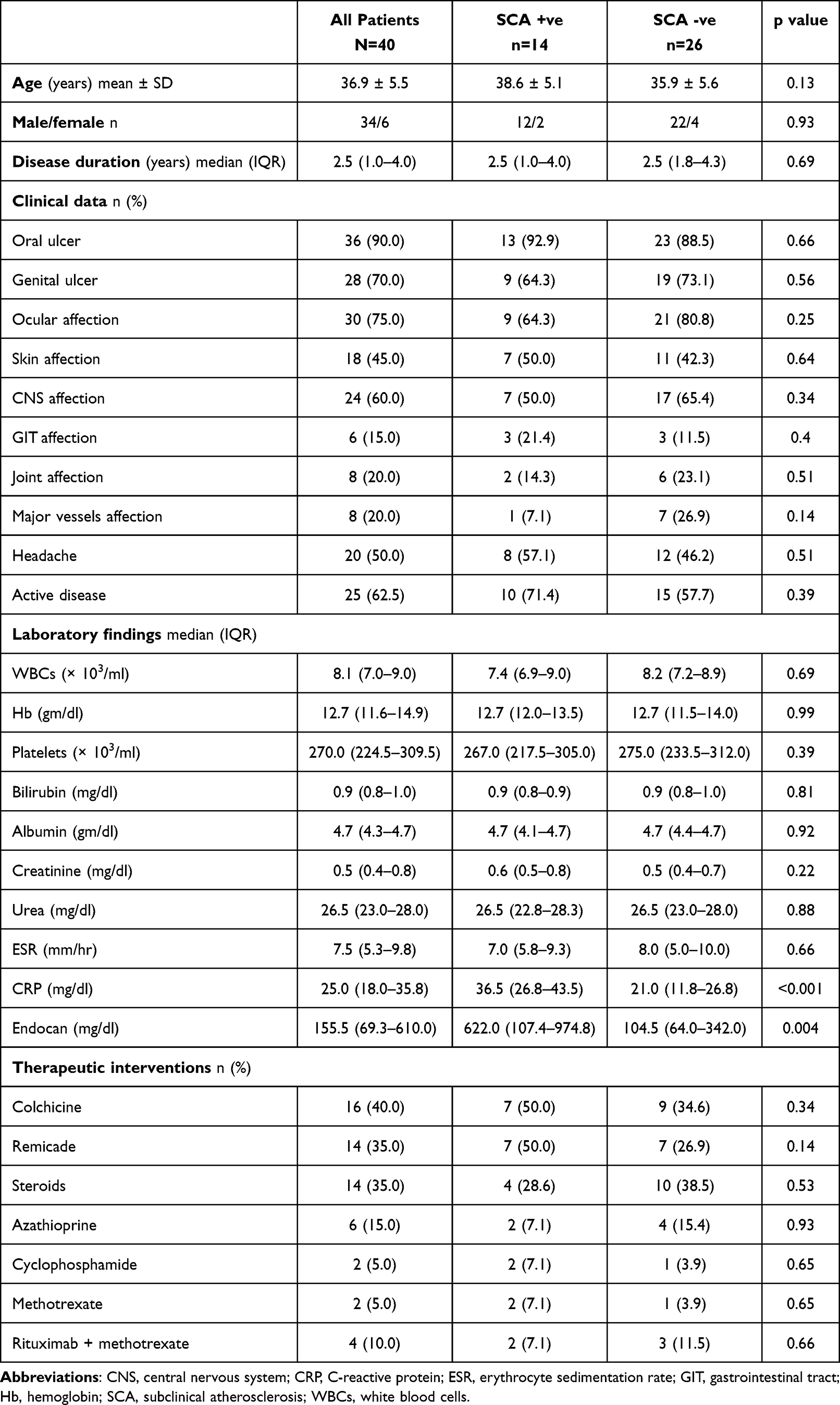 |
Table 1 Clinical and Laboratory Data in Patients with and without SCA |
Using ultrasound assessment, SCA was found in 14 BD patients (35.0%). Comparison between patients with SCA and patients without regarding the clinical and laboratory data revealed that the former group had significantly higher CRP [median (IQR): 36.5 (26.8–43.5) versus 21.0 (11.8–26.8) mg/dL, p < 0.001] and endocan [median (IQR): 622.0 (107.4–974.8) versus 104.5 (64.0–342.0) mg/dL, p = 0.004] levels (Table 1).
Correlation analysis identified a significant correlation between serum endocan levels and CIMT measurements (r = 0.47, p = 0.002) (Table 2). Logistic regression analysis recognized serum CRP [OR (95% CI): 1.27 (1.04–1.56), p = 0.019] and endocan [OR (95% CI): 1.0 (1.0–1.012), p = 0.035] levels as significant predictors of SCA in multivariate analysis (Table 3).
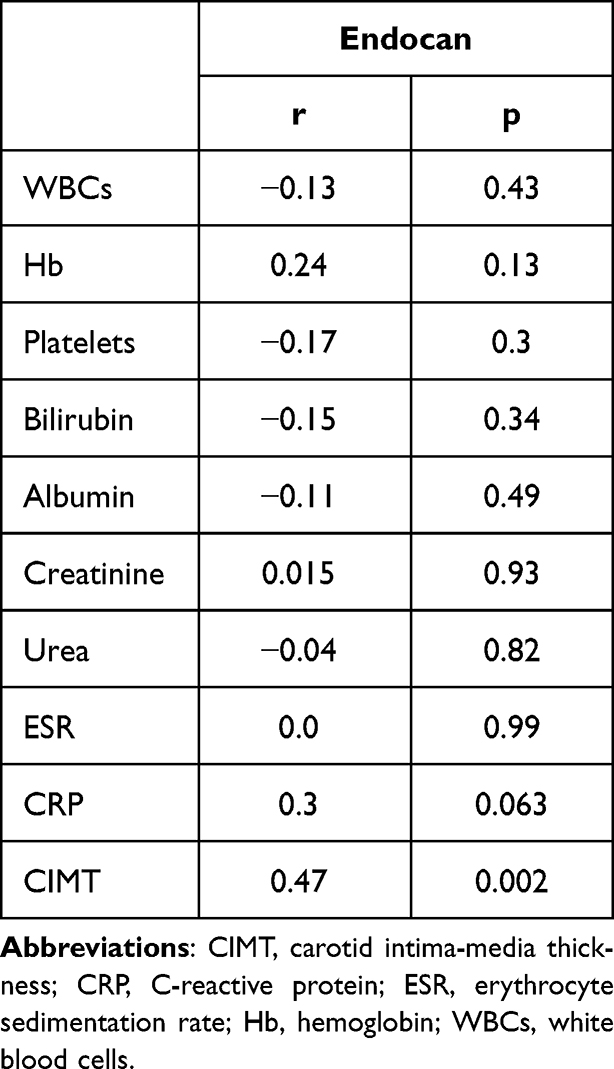 |
Table 2 Correlation Between Endocan Levels and Clinical and Laboratory Data |
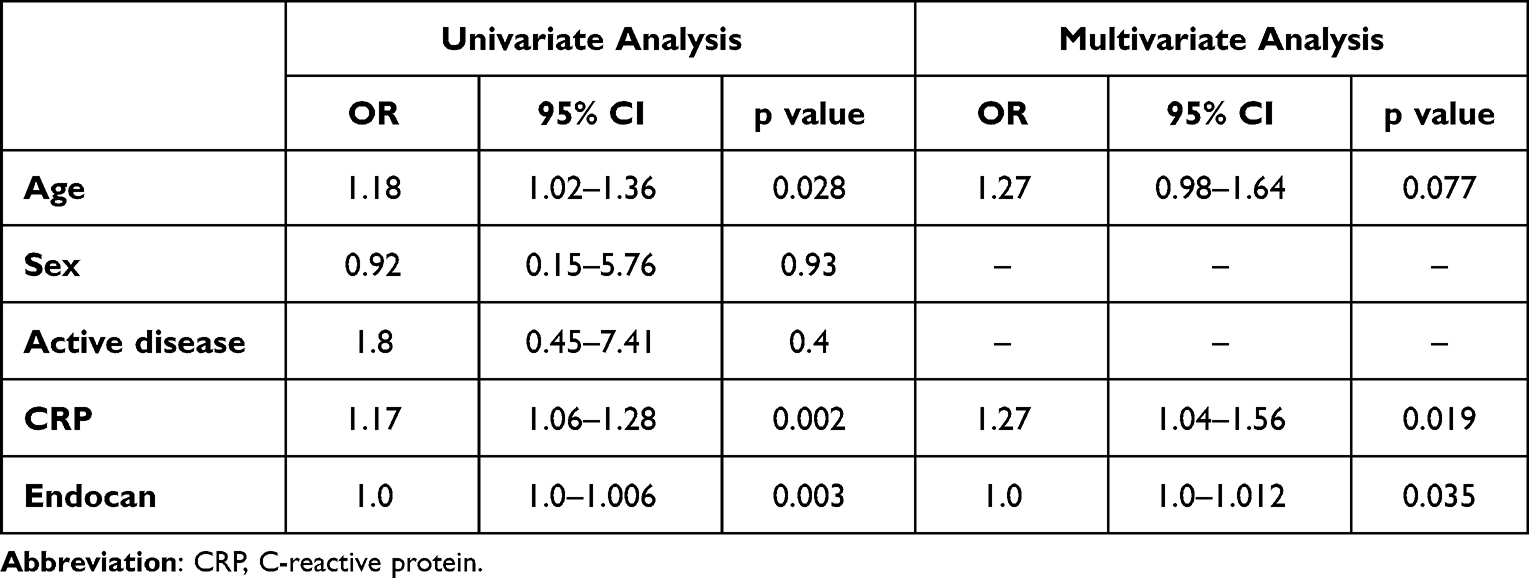 |
Table 3 Predictors of SCA in the Studied Patients |
ROC curve analysis showed good performance of serum endocan levels as a possible diagnostic marker of SCA in BD patients at a cut-off of 109.5 mg/dl: [AUC (95% CI): 0.78 (0.61–0.94), sensitivity: 78.6%, specificity: 53.8%] (Figure 2).
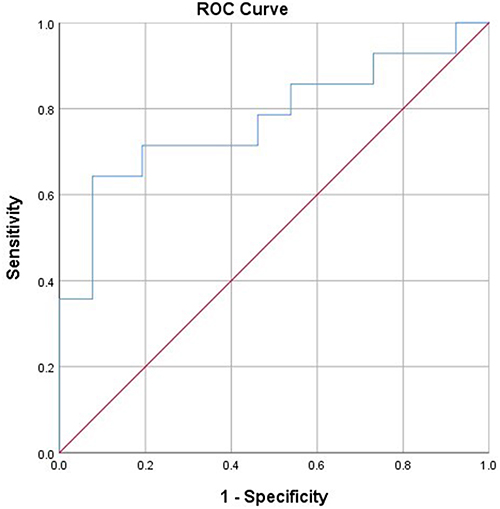 |
Figure 2 Serum endocan in diagnosis of SCA. |
Discussion
Using ultrasound assessment, the present study diagnosed SCA in 35.0% of the studied BD patients. This figure is close to that reported by the Turkish study of Uslu Yurteri et al.9 In their work, they could diagnose SCA in 32.0% of their 100 BD-patient study.
However, the present study identified no significant relation between SCA and the clinical data in the studied patients, in contrast to Uslu Yurteri et al’s9 study, which noted a significant marginal association between SCA and vascular phenotype and major organ involvement. On the other hand, our study revealed significantly higher CRP levels in BD patients with SCA as compared to their counterparts without SCA. Uslu Yurteri et al9 study failed to document such relation. In support of our conclusions, elevated CRP levels were frequently linked to SCA in many clinical conditions including rheumatoid arthritis,20 newly diagnosed diabetes21 and psoriasis.22
In our work, endocan levels were significantly elevated in BD patients as compared to healthy controls. In accordance with these findings, Balta et al12 noted significantly higher endocan levels in BD patients in comparison to controls. In addition, they found a significant relation between endocan levels and disease activity.
The present study recognized a possible clinical value of serum endocan levels in the identification of SCA in BD patients as shown by regression and ROC curve analysis. As previously mentioned, other studies noted similar findings in other clinical conditions.
In systemic lupus erythematosus, endocan levels were significantly correlated with CIMT measurements and showed significant association with SCA.14 Likewise, in diabetic patients, endocan levels expressed significant correlation with CIMT measurements and were a significant predictor of SCA.15 Similar findings were found in patients with moderate-severe psoriasis vulgaris patients.16
The role of endocan in the development of SCA is attributed to many factors. Overexpression of endocan is related to endothelial activation, dysfunction and neovascularization.23 Moreover, elevated endocan levels are associated with augmented oxidative stress.24 In addition, endocan is known to promote proinflammatory mediators in the context of cardiovascular diseases.25
Conclusion
In conclusion, the present study suggests serum endocan levels as a marker of subclinical atherosclerosis in BD patients. These conclusions, however, are limited by the relatively small sample size of the studied population. Further studies with larger sample size are recommended to confirm these conclusions.
Data Sharing Statement
Data from this research will be available from the corresponding author upon reasonable request.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article was submitted, gave final approval for the version to be published, and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Alpsoy E, Bozca BC, Bilgic A. Behcet disease: an update for dermatologists. Am J Clin Dermatol. 2021;22(4):477–502. doi:10.1007/s40257-021-00609-4
2. de Vargas RM, da Cruz MLN, Giarllarielli MPH, et al. Vascular involvement in Behcet’s disease: the immunopathological process. J Vasc Bras. 2021;20:e20200170. doi:10.1590/1677-5449.200170
3. Leccese P, Padula MC, Lascaro N, Padula AA, D’Angelo S. Clinical phenotypes of Behcet’s syndrome in a large cohort of Italian patients: focus on gender differences. Scand J Rheumatol. 2021;50(6):475–478. doi:10.1080/03009742.2021.1885735
4. Rodriguez-Carrio J, Nucera V, Masala IF, Atzeni F. Behcet's disease: from pathogenesis to novel therapeutic options. Pharmacol Res. 2021;167:105593. doi:10.1016/j.phrs.2021.105593
5. Tazi Mezalek Z, Khibri H, Chadli S, et al. Vascular complications of Behcet disease. Minerva Med. 2021;112(6):767–778. doi:10.23736/S0026-4806.21.07490-5
6. Yazici Y, Hatemi G, Bodaghi B, et al. Behcet syndrome. Nat Rev Dis Primers. 2021;7(1):67. doi:10.1038/s41572-021-00301-1
7. Toledo-Samaniego N, Oblitas CM, Penaloza-Martinez E, et al. Arterial and venous involvement in Behcet’s syndrome: a narrative review. J Thromb Thrombolysis. 2022;54:162–171. doi:10.1007/s11239-022-02637-1
8. Ozisler C, Kaplanoglu H. Evaluation of subclinical atherosclerosis by ultrasound radiofrequency data technology in patients with Behcet’s disease. Int J Rheum Dis. 2019;22(5):781–788. doi:10.1111/1756-185X.13579
9. Uslu Yurteri E, Ustuner E, Torgutalp M, et al. Can subclinical atherosclerosis be assessed more precisely in Behcet's syndrome patients by using a particular cutoff value for carotid intima media thickness? J Clin Rheumatol. 2022;28(1):e73–e76. doi:10.1097/RHU.0000000000001643
10. Balta S, Balta I, Mikhailidis DP. Endocan: a new marker of endothelial function. Curr Opin Cardiol. 2021;36(4):462–468. doi:10.1097/HCO.0000000000000867
11. Bessa J, Albino-Teixeira A, Reina-Couto M, Sousa T. Endocan: a novel biomarker for risk stratification, prognosis and therapeutic monitoring in human cardiovascular and renal diseases. Clin Chim Acta. 2020;509:310–335. doi:10.1016/j.cca.2020.07.041
12. Balta I, Balta S, Koryurek OM, et al. Serum endocan levels as a marker of disease activity in patients with Behcet disease. J Am Acad Dermatol. 2014;70(2):291–296. doi:10.1016/j.jaad.2013.09.013
13. Kul A, Ates O, Alkan Melikoglu M, et al. Endocan measurement for active behcet disease. Arch Rheumatol. 2017;32(3):197–202. doi:10.5606/ArchRheumatol.2017.6072
14. Icli A, Cure E, Cure MC, et al. Endocan levels and subclinical atherosclerosis in patients with systemic lupus erythematosus. Angiology. 2016;67(8):749–755. doi:10.1177/0003319715616240
15. Lv Y, Zhang Y, Shi W, et al. The association between endocan levels and subclinical atherosclerosis in patients with Type 2 diabetes mellitus. Am J Med Sci. 2017;353(5):433–438. doi:10.1016/j.amjms.2017.02.004
16. Elkamshoushi AM, Omar SS, El Abd AM, Hassan SZ, Sultan EA, Abd Elkawy E. Subclinical atherosclerosis in psoriatic disease: relation to endocan, TNF-alpha, age of onset, and body fat. Int J Dermatol. 2019;58(4):456–464. doi:10.1111/ijd.14290
17. Criteria for diagnosis of Behcet’s disease. International study group for Behcet’s disease. Lancet. 1990;335(8697):1078–1080.
18. Yilmaz S, Simsek I, Cinar M, et al. Patient-driven assessment of disease activity in Behcet’s syndrome: cross-cultural adaptation, reliability and validity of the Turkish version of the Behcet’s syndrome activity score. Clin Exp Rheumatol. 2013;31(3 Suppl 77):77–83.
19. Touboul PJ, Hennerici MG, Meairs S, et al. Mannheim intima-media thickness consensus. Cerebrovasc Dis. 2004;18(4):346–349. doi:10.1159/000081812
20. Mena-Vazquez N, Redondo-Rodriguez R, Rioja J, et al. Postprandial hyperlipidemia: association with inflammation and subclinical atherosclerosis in patients with rheumatoid arthritis. Biomedicines. 2022;10(1):133. doi:10.3390/biomedicines10010133
21. Zhou Z, Chen H, Sun M, Jin H, Ju H. Fetuin-A to adiponectin ratio is an independent indicator of subclinical atherosclerosis in patients with newly diagnosed type 2 diabetes mellitus. J Diabetes Complications. 2022;36(1):108102. doi:10.1016/j.jdiacomp.2021.108102
22. Niknezhad N, Haghighatkhah HR, Zargari O, et al. High-sensitivity C-reactive protein as a biomarker in detecting subclinical atherosclerosis in psoriasis. Dermatol Ther. 2020;33(4):e13628. doi:10.1111/dth.13628
23. Kali A, Shetty KS. Endocan: a novel circulating proteoglycan. Indian J Pharmacol. 2014;46(6):579–583. PMID: 25538326; PMCID: PMC4264070. doi:10.4103/0253-7613.144891
24. Kumar SK, Mani KP. Endocan alters nitric oxide production in endothelial cells by targeting AKT/eNOS and NFkB/iNOS signaling. Nitric Oxide. 2021;117:26–33. PMID: 34592471. doi:10.1016/j.niox.2021.09.006
25. Balta S, Mikhailidis DP, Demirkol S, Ozturk C, Celik T, Iyisoy A. Endocan: a novel inflammatory indicator in cardiovascular disease? Atherosclerosis. 2015;243(1):339–343. PMID: 26448266. doi:10.1016/j.atherosclerosis.2015.09.030
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.