Back to Journals » Journal of Pain Research » Volume 16
Serum 3-Hydroxybutyrate is Expected to Serve as One of the Supportive Diagnostic Markers of Persistent Idiopathic Dentoalveolar Pain (PDAP)
Authors Tamaki K, Saito N ![]() , Tomita H
, Tomita H
Received 6 October 2023
Accepted for publication 12 November 2023
Published 22 November 2023 Volume 2023:16 Pages 4005—4013
DOI https://doi.org/10.2147/JPR.S436034
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Keith
Katsuya Tamaki,1,2,* Norihiro Saito,1,* Hirofumi Tomita1,3
1Department of Clinical Laboratory Medicine Hirosaki University Graduate School of Medicine, Hirosaki City, Aomori, 036-8562, Japan; 2Tamaki Dental Clinic, Keison-Kai, Akita City, 010-0925, Japan; 3Department of Cardiology and Nephrology, Hirosaki University Graduate School of Medicine, Hirosaki City, Aomori, 036-8562, Japan
*These authors contributed equally to this work
Correspondence: Norihiro Saito, Department of Clinical Laboratory Medicine, Hirosaki University Graduate School of Medicine, 5 Zaifu-cho, Hirosaki City, Aomori, 036-8562, Japan, Tel +81-172-33-5111, Email [email protected]
Background: Persistent idiopathic dentoalveolar pain (PDAP), previously referred to as atypical odontalgia, is a chronic dental pain that occurs without signs of pathology. PDAP is considered a diagnosis of exclusion, and its definition is currently under refinement and remains ambiguous. The metabolite known as 3-hydroxybutyrate (3HB) has garnered significant interest as a potential indicator for both depression and chronic psychogenic pain. We investigated the characteristics of patients with PDAP and hypothesized that serum 3HB could support the diagnosis of PDAP.
Subjects and Methods: Forty-one patients with PDAP and 167 patients with odontogenic toothache were investigated regarding depression and anxiety scales in addition to the general dental evaluation. Blood tests including high-sensitivity CRP, HbA1c, and 3HB were performed for all patients. Associations between PDAP and patients’ varying characteristics were investigated using hierarchical multivariate logistic regression analyses.
Results: There were more females, current smokers, patients with orofacial pain (such as temporomandibular joint pain, glossalgia, and headache), and people with elevated 3HB levels among patients with PDAP than among control participants. Multivariate logistic regression analyses predicting patients with PDAP identified the female sex (odds ratio [OR]: 4.16), current smoking (OR: 14.9), glossalgia (OR: 19.8) a high CES-D score (≥ 16) (OR: 5.98), and elevated serum 3HB (≥ 80 μmol/L) (OR: 18.4) factors significantly associated with PDAP.
Conclusion: Our results demonstrated that serum 3HB levels could be elevated in patients with PDAP compared to other types of odontogenic pain, although 3HB was not specific to PDAP. Based on our findings, five factors - female sex, current smoking, depressive tendencies, chronic orofacial pains, and high serum 3HB levels - could be useful for diagnosing PDAP.
Keywords: persistent idiopathic dentoalveolar pain, atypical odontalgia, 3-hydroxybutyrate, temporomandibular disorder, orofacial pain
Introduction
Persistent idiopathic dentoalveolar pain (PDAP), classified by the International Classification of Orofacial Pain (ICOP) in 2020, was previously referred to as atypical odontalgia.1 It is characterized by pain in or around a tooth socket or extraction site, even when there is no apparent clinical or radiographic evidence of dental issues or other relevant oral hard or soft tissue problems.2–4 PDAP is surprisingly common2 and dentists often have trouble diagnosing and treating it. There are reports indicating that 680,000 teeth undergo unnecessary root canal treatment each year.5 PDAP was found in 2.1% of a population of 3000 at the University of Southern California Orofacial Pain and Oral Medicine Center.6
According to the third edition of the International Headache Classification (ICHD-3), PDAP is considered a subtype of persistent idiopathic facial pain. It is defined as persistent facial and/or oral pain, with varying presentations but recurring daily for more than 2 hours per day over more than 3 months, in the absence of a clinical neurological deficit.7 The definition of PDAP is still being refined, and it remains ambiguous.8 PDAP has been suggested to have potential psychogenic, vascular, neuropathic, or idiopathic origins.3,9 In a study by List et al, it was observed that individuals with PDAP tended to have more coexisting pain conditions and higher scores related to depression and somatization.10
Metabolomics has recently been applied to the development of new biomarkers, serving as an exploratory research tool for both physical and mental health conditions.11 As an illustration, examinations that compared metabolite levels between individuals in remission and those currently experiencing depression discovered a pattern of metabolite changes resembling those found in analyses comparing control individuals with those currently suffering from depression. One notable distinction observed in remitted patients, as opposed to those currently depressed, was an increase in the concentration of 3-hydroxybutyrate (3HB).11 Consequently, 3HB is presently gaining recognition as an indicator of depression’s degree of severity.12 The level of 3HB, a type of ketone body, can elevate in situations like diabetic ketoacidosis and periods of starvation. It serves as an indicator for conditions where lipid metabolism takes precedence over glucose metabolism, and it acts as a source of energy for the brain. Recent research has indicated a potential link between 3HB and brain inflammation, particularly in its potential contribution to epilepsy.13,14 In our findings, it was observed that the serum 3HB concentration exceeded the upper limit of the normal range (<80 μmol/L) in over 30% of individuals displaying psychogenic symptoms.15 Nonetheless, only a limited number of research studies have evaluated the clinical relevance of heightened serum 3HB levels in individuals who do not have diabetes.
Therefore, we investigated the characteristics of patients with PDAP and hypothesized that serum 3HB could support the diagnosis of PDAP. Furthermore, we also investigated the characteristics of patients with dentalgia who have elevated 3HB.
Subjects and Methods
Subjects
Participants with toothache were adult patients (aged 17–82 years) recruited from Tamaki Dental Clinic from April 2022 to July 2023. All patients underwent a thorough dental assessment and imaging examinations to ascertain the underlying cause of their symptoms. Exclusion criteria involved severe concurrent conditions such as malnutrition, advanced diabetes requiring insulin treatment, cancer, coronary artery disease, heart failure, chronic respiratory failure, or undergoing dialysis. Additionally, individuals taking psychotropic medications other than benzodiazepines, such as antidepressants and atypical antipsychotics, were also excluded. Furthermore, all patients were queried about psychiatric and psychosomatic symptoms in addition to the standard interview. The level of depressive mood was assessed using the Center for Epidemiologic Studies Depression Scale (CES-D);16 The scoring system for this assessment spans from 0 (indicating the most favorable outcome) to 60 (indicating the most unfavorable outcome). Traditionally, a cutoff point of 16 has often been suggested to determine the presence of depression.17 Anxiety levels were assessed using the State-Trait Anxiety Inventory (STAI),16,18 which includes both a 20-item state scale and a 20-item trait anxiety scale. Each item is rated on a four-point Likert scale, resulting in a total score ranging from 20 to 80 for each scale, with higher scores indicating elevated anxiety levels. The Japanese version of this assessment was validated by Nakazato and Mizuguchi, and typical cutoff scores for defining potential clinical levels of anxiety are 41 (for males) or 42 (for females) for state anxiety and 44 (for males) or 45 (for females) for trait anxiety.19 Individuals with severe psychopathological conditions such as schizophrenia, delusional disorder, delirium, acute mania, or ongoing substance abuse were not included in the study. Ultimately, 41 patients diagnosed with PDAP and 167 patients experiencing odontogenic toothache consented to take part in this research.
Diagnosis of PDAP
The diagnosis of PDAP was determined to meet the following diagnostic criteria according to ICOP.1
A. Intraoral dentoalveolar pain fulfilling criteria B and C
B. Recurring daily for >2 hours/day for >3 months
C. Pain has both of the following characteristics:
1. localized to a dentoalveolar site (tooth or alveolar bone)
2. deep, dull, pressure-like quality
D. Clinical and radiographic examinations are normal, and local causes have been excluded
E. Not better accounted for by another ICOP or ICHD-3 diagnosis.
Measurement of 3HB
Serum 3HB levels were assessed through an enzymatic cycling assay that relies on a reaction involving the cofactor NAD+, which is converted to NADH. Subsequently, NADH interacts with a colorimetric probe, generating a colored compound that can be quantified at 450 nm. The intensity of this color directly correlates with the concentration of 3HB present in the sample.20
Data Analysis
Data analysis was conducted using BellCurve for Excel version 3.22, developed by Social Survey Research Information Co. in Saitama, Japan. Comparative analyses of clinical characteristics between two groups were carried out using Student’s t-test or Welch’s t-test in cases of unequal data variances for quantitative data, and the chi-square test for categorical data. Associations between PDAP and patients’ characteristics were explored through hierarchical multivariate logistic regression analysis. The goodness of fit differences between successive models was assessed by examining the changes in “-2 log-likelihood” values and degrees of freedom values. To assess potential multicollinearity, the variance inflation factor (VIF) was employed. None of the regression analyses yielded VIF values exceeding 10, signifying the absence of multicollinearity in our models. The significance level for all analyses was set at 0.05.
Results
Table 1 illustrates the contrast in clinical characteristics between the control group of patients with odontogenic toothache (n = 167) and individuals diagnosed with PDAP (n = 41). There were significantly more females and current smokers among patients with PDAP (78.0% and 24.4%, respectively) than among control participants (59.3% and 11.4%, respectively). There were no significant differences in the oral cavity’s sanitary state between control participants and patients with PDAP. There were significantly more participants with temporomandibular joint pain, glossalgia, and headache among patients with PDAP than among control patients (22.0% vs 5.4%, 22.0% vs 1.8%, and 12.2% vs 4.2%, respectively). Although there were no significant differences in psychological (CES-D, STAI-state and -trait) scores, the numbers (%) of people with scores that exceeded each cutoff score were higher among patients with PDAP than among control participants (CES-D; 34.1% vs 13.2%, STAI-state; 51.2% vs 31.7%, and STAI-trait; 51.2% vs 30.5%, respectively).
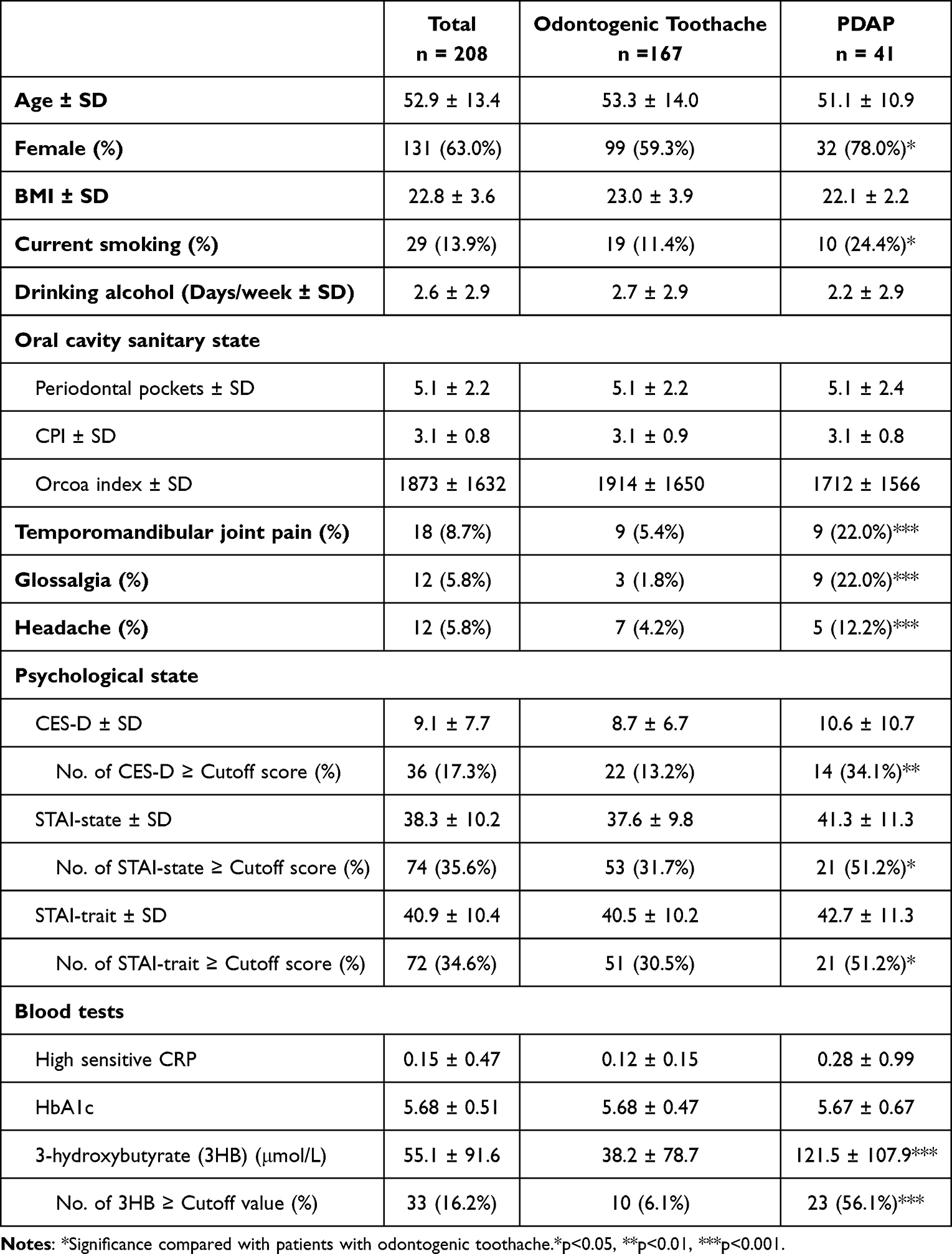 |
Table 1 Comparison of Clinical Characteristics Between Patients with PDAP and the Other Patients with Odontogenic Toothache |
Laboratory test results indicated that highly sensitive CRP and HbA1c levels did not exhibit significant differences. However, it was noteworthy that serum 3HB levels were notably higher in patients with PDAP (121.5 ± 107.9 µmol/L) compared to control patients (38.2 ± 78.7 µmol/L). Specifically, 3HB levels exceeded the upper limit of the normal range (≥80 µmol/L) in 23 out of 41 patients with PDAP (56.1%), whereas this was the case in only 9 out of 166 control patients (5.4%). To explore the relationship between elevated 3HB and PDAP, further investigation was carried out. High 3HB levels displayed a sensitivity of 56.1%. Nevertheless, its specificity was notably high at 94.6%, and the positive likelihood ratio stood at 10.4.
We conducted hierarchical multivariate logistic regression analyses to predict the presence of PDAP, with PDAP categorized as “yes = 1” and “no = 0” as the dependent variable (see Table 2). In the initial step, various factors, including those outlined in Table 1, were introduced as independent variables, except for 3HB. Subsequently, we employed multivariate logistic regression analyses using the forward-backward stepwise selection method (stepwise method) to identify significant factors from the array of independent variables (Model 1). In the subsequent step, we included the 3HB factor (3HB ≥80 μmol/L; “yes = 1, no = 0”) as an independent variable (Model 2). Regression Model 1, which did not incorporate 3HB data, revealed that current smoking, glossalgia, and a high CES-D score (≥16) exhibited significant associations with PDAP. The first regression analysis using the stepwise method did not identify the other factors, such as the oral cavity’s state, anxiety scale, and blood test items other than 3HB, predictors of PDAP. Regression Model 2, which included 3HB, showed a significant association with PDAP in females (OR: = 4.16, 95% CI: 1.15–15.1), current smokers (OR: = 14.9, 95% CI: 3.17–70.4), patients with glossalgia (OR: = 19.8, 95% CI: 2.48–157.1), patients with high CES-D scores (OR: = 5.98, 95% CI: 1.94–18.5), and patients with high 3HB levels (OR: = 18.4, 95% CI: 5.85–57.7). Regression Model 1 demonstrated a predictive accuracy of 82.7%, whereas Model 2 exhibited an accuracy of 85.7%. Notably, the p-value for the change in Δ−2 log-likelihood was less than 0.001, signifying that Model 2’s accuracy was significantly superior to that of Model 1.
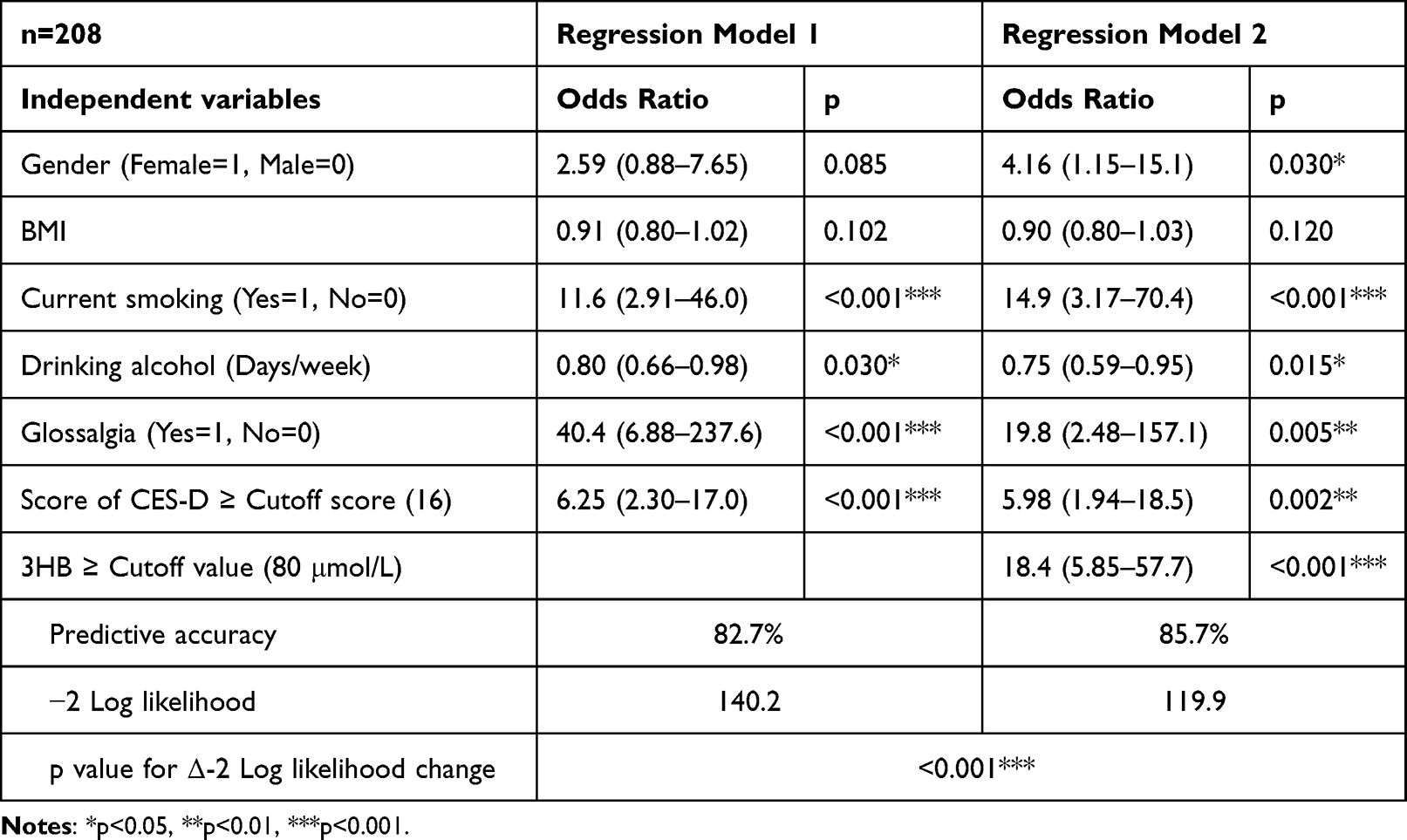 |
Table 2 Hierarchical Multivariate Logistic Regression Analysis of the Factors Associated with PDAP |
To explore the attributes of individuals with elevated 3HB levels, multivariate logistic regression analyses predicting elevated 3HB levels were performed (Table 3). These analyses showed significant associations for the presence of periodontal pockets (OR: = 1.31, 95% CI: 1.03–1.67), PDAP (OR: = 17.9, 95% CI: 5.04–63.8), temporomandibular joint pain (OR: = 7.00, 95% CI: 1.38–35.4), headache (OR: = 11.5, 95% CI: 1.98–66.1), and high CES-D scores (OR: = 4.28, 95% CI: 1.02–18.0).
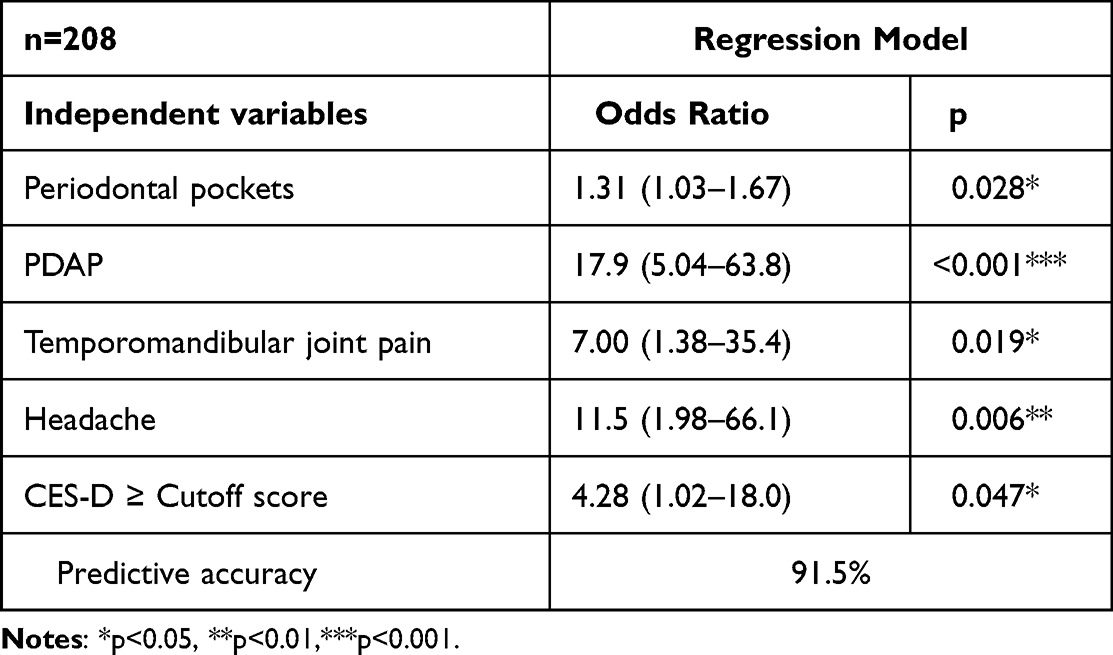 |
Table 3 Multivariate Logistic Regression Analysis of the Elevated 3HB (≥ Cutoff Value) |
Discussion
There should be some opportunities for clinical dentists to diagnose toothache of unknown origin, accompanied by temporomandibular joint pain, glossalgia, or headache, as PDAP. However, it is rare to conduct evaluations for depression or blood tests in general dental clinics, and it is often considered common practice to prescribe analgesics and observe the patient’s progress. Thus, patients with PDAP may often consult not only dentists but also otorhinologists, anesthesiologists and general practitioners. However, the diagnosis and treatment of PDAP may also be unfamiliar and challenging for such clinicians. In this study, we investigated the characteristics of patients with PDAP and examined whether the elevation of 3HB, which has recently gained attention as a marker of psychological stress and psychogenic symptoms, could be a predictive factor for PDAP.
Initially, our findings indicated a notable difference in gender distribution, with a higher proportion of females in the PDAP patient group (78.0%) compared to the control participants (59.3%). This aligns with the commonly accepted understanding that PDAP tends to manifest more frequently in females, with 80–90% of all cases being diagnosed in females.21–25 Melis et al also reported in their review of PDAP that females accounted for approximately 82% of patients with PDAP.3 Next, complications such as temporomandibular joint pain, glossalgia, and headache were more common among patients with PDAP than among control participants in this study, and glossalgia was detected as a significant factor in the regression analysis predicting PDAP. PDAP may potentially share underlying pain mechanisms with other conditions characterized by chronic orofacial pain, including atypical facial pain and temporomandibular disorder (TMD).26 In a study by Baad-Hansen et al,27 which involved 46 patients with PDAP, findings revealed that episodic tension-type headache (TTH), chronic TTH, and myofascial TMD were present in 46%, 18%, and 50% of individuals with PDAP, respectively. Other researchers have also reported a higher prevalence of TMD pain, TTH, and widespread pain among patients with PDAP compared to controls.10 Additionally, PDAP has been documented in patients with burning mouth syndrome who experience glossalgia.28,29 These orofacial pain conditions should be regarded as potential comorbid disorders in cases of PDAP.
In this study, we found that current smoking is significantly more common among patients with PDAP. Pain and heightened sensitivity are notably more prevalent among individuals who smoke compared to those who do not smoke, as indicated by previous research.30–32 Meta-analyses involving six studies have further underscored this observation by revealing that orofacial pain is significantly more severe in smokers (odds ratio: 3.55, 95% confidence interval: 1.92–6.58) in contrast to non-smokers. Subgroup analyses have indicated that the likelihood of experiencing orofacial pain is three times higher among smokers (odds ratio: 3.13, 95% confidence interval: 1.16–8.46). While existing evidence suggests a bidirectional relationship between smoking and general body ache, further investigation is required to better understand the specific connection between smoking and orofacial pain. Additionally, numerous studies have reported associations between smoking and conditions like depression or anxiety.33
There is widespread agreement regarding the role of psychological issues, whether as primary or secondary factors, in the development of PDAP.26 In this study, to avoid extreme data variance and the potential influence of psychotropic therapy, we excluded cases in which individuals had a pre-existing diagnosis of mental illness and were currently receiving treatment with antidepressants or atypical antipsychotics. Nevertheless, 34.1% of patients with PDAP exceeded the cutoff value of CES-D, and our regression analyses showed that abnormally high scores on CES-D were identified as significant predictors of PDAP (OR: 5.98, p = 0.002). Reports indicate that patients with PDAP often have a history of depression (66%) or experience depressive symptoms (41%).23,34 Notably, List et al conducted an examination of 46 PDAP patients, revealing significantly higher depression and somatization scores within the PDAP group compared to control patients without orofacial pain.10 Similarly, Baad-Hansen et al found moderate-to-high mean scores for depression and somatization in their study involving 46 PDAP patients, further highlighting the strong connection between PDAP and psychological conditions.27
There has not been a prospective study assessing the utility of assaying 3HB, except in cases of diabetic ketoacidosis.35–37 However, Setoyama et al reported an association between 3HB and suicidal ideation, suggesting that 3HB might regulate emotional systems in the brain through its involvement in energy metabolite processes. As an endogenous ketone body, 3HB plays a crucial role in supporting mammalian cell metabolism during energy-deficient states, such as fasting or exercise.38,39 In recent years, multiple studies have indicated that 3HB could potentially have antidepressant effects,40,41 likely through its ability to inhibit the activation of the nucleotide-binding domain, leucine-rich repeat and pyrin domain-containing 3 (NLRP3) inflammasome.14
Therefore, we hypothesized that serum 3HB could support the diagnosis of PDAP. In this study, 56.1% of the 41 PDAP patients exhibited elevated serum 3HB levels, indicating a sensitivity of 56.1%. However, the specificity was 94.6%, and the positive likelihood ratio stood at 10.4. In other words, even if 3HB is negative, it cannot rule out PDAP, but elevated 3HB levels in patients with unexplained toothache are considered a useful factor for suspecting PDAP. Additionally, the positive likelihood ratio is also greater than 10, indicating its value in clinical diagnostics. Incidentally, the sensitivity of CES-D≥cut-off for PDAP was 34.1%, the specificity was 86.8%, and the positive likelihood ratio was 2.6. To confirm the significance of 3HB in the diagnosis of PDAP, we further conducted a comparative analysis between two regression models using hierarchical logistic regression analysis. Model 1 excluded 3HB as a variable, while the other Model 2 included it. The outcome revealed that Model 2 demonstrated significantly higher accuracy than Model 1 (p < 0.001), with an odds ratio (OR) of 18.4 (p < 0.001) for elevated 3HB. These findings underscore the importance of incorporating 3HB measurements in the assessment, independent of CES-D, and suggest that elevated 3HB levels in patients with toothache may serve as predictive factors for PDAP patients.
However, high 3HB levels are not specific to PDAP but seem to be observed in patients with psychogenic chronic pain in general, as seen in our previous report on psychosomatic chronic somatic symptoms.15 The analysis predicting elevated 3HB in this study showed that not only PDAP but temporomandibular joint pain, headache, and high scores on the depression scale were identified as factors significantly associated with high 3HB levels. One of several multifactorial diseases, temporomandibular dysfunction (TMD) has mostly been linked to five etiological factors: occlusion, trauma, severe pain stimuli, parafunctional activities, and psychological elements, including stress, anxiety, and depression.42 TMDs can also cause headaches, neck pain and ringing in the ears.43 Orofacial pains, including PDAP, are considered to have a psychogenic component in a certain proportion, and this psychogenic chronic pain is more likely to be associated with elevated 3HB.
Study Limitation
To further enhance the accuracy of this study, a larger sample size with subsets of various groups based on CES-D and STAI scores, along with an analysis of their correlation with 3HB levels, is necessary. For example, further investigation is needed for cases with high CES-D and low 3HB levels, as well as the reverse cases.
In the context of this study, we did not delve into the specifics of PDAP treatment. Nonetheless, previous pharmacological approaches to address PDAP have primarily centered around the administration of tricyclic antidepressants as the preferred initial treatment.3,4 Over the past few years, there have been instances reported where antidepressants like selective serotonin reuptake inhibitors (SSRIs) and serotonin-noradrenaline reuptake inhibitors (SNRIs) have been utilized.44 Previously, we reported that a high proportion of patients with chronic idiopathic complaints who had elevated 3HB levels showed noticeable effectiveness of SSRIs and SNRIs in this group.15 Taking these findings into consideration, it is anticipated that SSRIs/SNRIs may be effective for cases with elevated 3HB levels among patients with PDAP or orofacial pains.
Conclusion
Our results demonstrated that serum 3HB levels could be elevated in patients with PDAP compared to other types of odontogenic pain, although 3HB was not specific to PDAP. Based on our findings, five factors - female sex, current smoking, depressive tendencies, chronic orofacial pains, and high serum 3HB levels - could be useful for diagnosing PDAP.
Abbreviations
PDAP, persistent idiopathic dentoalveolar pain; ICOP, International Classification of Orofacial Pain; ICHD-3, Third edition of the International Headache Classification; 3HB, 3-hydroxybutyrate; CES-D, Center for Epidemiologic Studies Depression Scale; STAI, State-Trait Anxiety Inventory; VIF, The variance inflation factor; TMD, Temporomandibular disorder; TTH, Tension-type headache; SSRI, Selective serotonin reuptake inhibitors; SNRI, Serotonin noradrenaline reuptake Inhibitors; IRB, Institutional Review Board.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Hirosaki University Graduate School of Medicine (approval number 2022-205). This study protocol was approved by the Institutional Review Board (IRB). The hospital patient data we used in the study were anonymized per the recommendations of the governance of Hirosaki University Graduate School of Medicine. As the study comprised solely of data collected retrospectively by Tamaki Dental Clinic, the IRB waived informed consent. Caretakers, legal guardians, and relatives of the patients included in this study were given the opportunity to opt out of the study at any time.
Acknowledgments
We thank Dr. Tamaki M for contributing to the work done in Tamaki Dental Clinic.
Funding
The authors received no specific funding for this work.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Orofacial T. International classification of orofacial pain, 1st edition (ICOP). Cephalalgia. 2020;40(2):129–221. doi:10.1177/0333102419893823
2. Woda A, Tubert-Jeannin S, Bouhassira D, et al. Toward a new taxonomy of idiopathic orofacial pain. Pain. 2005;116:396–406. doi:10.1016/j.pain.2005.05.009
3. Melis M, Lobo SL, Ceneviz C, et al. Atypical odontalgia: a review of the literature. Headache. 2003;43:1060–1074. doi:10.1046/j.1526-4610.2003.03207.x
4. Baad-Hansen L. Atypical odontalgia–pathophysiology and clinical management. J Oral Rehabil. 2008;35:1–11. doi:10.1111/j.1365-2842.2007.01813.x
5. Benjamin P. Pain after routine endodontic therapy may not have originated from the treated tooth. J Am Dent Assoc. 2011;142:1383–1384. doi:10.14219/jada.archive.2011.0140
6. Ram S, Teruel A, Kumar SK, et al. Clinical characteristics and diagnosis of atypical odontalgia: implications for dentists. J Am Dent Assoc. 2009;140:223–228. doi:10.14219/jada.archive.2009.0136
7. Headache Classification Subcommittee of the International Headache Society (IHS). The international classification of headache disorders. 3rd ed. Cephalalgia. 2013;33:629–808. doi:10.1177/0333102413485658
8. Benoliel R. Atypical odontalgia: quo vadis? Quintessence Int. 2013;44(6):383. doi:10.3290/j.qi.a29632
9. Ahlawat J, Malhotra A, Sharma A, Talwar S. Atypical odontalgia: a non-odontogenic toothache of neuropathic origin. Int J Res Ayurveda Pharm. 2016;7:98–101. doi:10.7897/2277-4343.07137
10. List T, Leijon G, Helkimo M, et al. Clinical findings and psychosocial factors in patients with atypical odontalgia: a case-control study. J Orofac Pain. 2007;21:89–98.
11. Kaddurah-Daouk R, Krishnan KR. Metabolomics: a global biochemical approach to the study of central nervous system diseases. Neuropsychopharmacology. 2009;34:173–186. doi:10.1038/npp.2008.174
12. Setoyama D, Kato TA, Hashimoto R, et al. Plasma metabolites predict severity of depression and suicidal ideation in psychiatric patients-a multicenter pilot analysis. PLoS One. 2016;11:e0165267.
13. Sada N, Lee S, Katsu T, Otsuki T, Inoue T. Epilepsy treatment. Targeting LDH enzymes with a stiripentol analog to treat epilepsy. Science. 2015;347:1362–1367. doi:10.1126/science.aaa1299
14. Youm YH, Nguyen KY, Grant RW, et al. The ketone metabolite beta-hydroxybutyrate blocks NLRP3 inflammasome-mediated inflammatory disease. Nat Med. 2015;21:263–269. doi:10.1038/nm.3804
15. Saito N, Itoga M, Minakawa S, Kayaba H. Serum 3-hydroxybutyrate in patients with psychogenic somatoform symptoms may be a predictor of the effectiveness of sertraline and venlafaxine. Int J Gen Med. 2021;14:1785–1795. doi:10.2147/IJGM.S300517
16. Okun A, Stein RE, Bauman LJ, Silver EJ. Content validity of the psychiatric symptom index, CES-depression scale, and state-trait anxiety inventory from the perspective of DSM-IV. Psychol Rep. 1996;79:1059–1069. doi:10.2466/pr0.1996.79.3.1059
17. Weissman MM, Sholomskas D, Pottenger M, Prusoff BZ, Locke BZ. Assessing depressive symptoms in five psychiatric populations: a validation study. Am J Epidemiol. 1977;106:203–214. doi:10.1093/oxfordjournals.aje.a112455
18. Spielberger CD, Gorsuch RL, Lushene RE. Manual for the State-Trait Anxiety. Palo Alto, CA: Consulting Psychologist Press; 1970.
19. Nakazato K, Mizuguchi K. Studies on psychometric characteristics of depression in the field of internal medicine. Shinshin-Igaku. 1982;22:107–112.
20. 3-Hydroxybutyrate REAGENT KIT. KAINOS Co., Ltd. Tokyo, Japan. Available from: http://www.kainos.co.jp/jp/products/pdf/TKA5520.pdf.
21. Bates RE
22. Jacobs R, Wu CH, Goossens K, et al. A case-control study on the psychophysical and psychological characteristics of the phantom tooth phenomenon. Clin Oral Investig. 2002;6:58–64. doi:10.1007/s00784-001-0149-9
23. Rees RT, Harris M. Atypical odontalgia. Br J Oral Surg. 1979;16:212–218. doi:10.1016/0007-117X(79)90027-1
24. Reik L
25. Schnurr RF, Brooke R. Atypical odontalgia: update and comment on long-term follow-up. Oral Surg Oral Med Oral Pathol. 1992;73:445–448. doi:10.1016/0030-4220(92)90322-H
26. Abiko Y, Matsuoka H, Chiba I, Toyofuku A. Current evidence on atypical odontalgia: diagnosis and clinical management. Int J Dent. 2012;2012:518548. doi:10.1155/2012/518548
27. Baad-Hansen L, Leijon G, Svensson P, List T. Comparison of clinical findings and psychosocial factors in patients with atypical odontalgia and temporomandibular disorders. J Orofac Pain. 2008;22:7–14.
28. Woda A, Pionchon P. A unified concept of idiopathic orofacial pain: pathophysiologic features. J Orofac Pain. 1999;13:172–184.
29. Grushka M, Epstein JB, Gorsky M. Burning mouth syndrome and other oral sensory disorders: a unifying hypothesis. Pain Res Manag. 2003;8:133–135. doi:10.1155/2003/654735
30. Ditre JW, Brandon TH, Zale EL, Meagher MM. Pain, nicotine, and smoking: research findings and mechanistic considerations. Psychol Bull. 2011;137:1065–1093. doi:10.1037/a0025544
31. Unell L, Söderfeldt B, Halling A, Birkhed D. Explanatory models for clinically determined and symptom-reported caries indicators in an adult population. Acta Odontol Scand. 1999;57:132–138. doi:10.1080/000163599428850
32. Al-Wahadni A, Linden GJ. Dentine hypersensitivity in Jordanian dental attenders. A case control study. J Clin Periodontol. 2002;29:688–693. doi:10.1034/j.1600-051X.2002.290804.x
33. Fluharty M, Taylor AE, Grabski M, Munafò MR. The association of cigarette smoking with depression and anxiety: a systematic review. Nicotine Tob Res. 2017;19:3–13. doi:10.1093/ntr/ntw140
34. Brooke RI, Schnurr RF. Diagnosing and treating atypical odontalgia. J Mass Dent Soc. 1995;44:30–32.
35. Arora S, Henderson SO, Long T, Menchine M. Diagnostic accuracy of point of care testing for diabetic ketoacidosis at emergency department triage: beta hydroxybutyrate versus the urine dipstick. Diabetes Care. 2011;34:852–854. doi:10.2337/dc10-1844
36. Noyes KJ, Crofton P, Bath LE, et al. Hydroxybutyrate near patient testing to evaluate a new end point for intravenous insulin therapy in the treatment of diabetic ketoacidosis in children. Pediatr Diabetes. 2007;8:150–156. doi:10.1111/j.1399-5448.2007.00240.x
37. Laffel LM, Wentzell K, Loughlin C, et al. Sick day management using blood 3-hydroxybutyrate (3-OHB) compared with urine ketone monitoring reduces hospital visits in young people with T1DM: a randomized clinical trial. Diabet Med. 2006;23:278–284. doi:10.1111/j.1464-5491.2005.01771.x
38. Newman JC, Verdin E. Ketone bodies as signaling metabolites. Trends Endocrinol Metab. 2014;25:42–52. doi:10.1016/j.tem.2013.09.002
39. Cotter DG, Schugar RC, Crawford PA. Ketone body metabolism and cardiovascular disease. Am J Physiol Heart Circ Physiol. 2013;304:H1060–H1076. doi:10.1152/ajpheart.00646.2012
40. Chen L, Miao Z, Xu X. Beta-hydroxybutyrate alleviates depressive behaviors in mice possibly by increasing the histone3-lysine9-beta- hydroxybutyrylation. Biochem Biophys Res Commun. 2017;490:117–122. doi:10.1016/j.bbrc.2017.05.184
41. Yamanashi T, Iwata M, Kamiya N, et al. Beta-hydroxybutyrate, an endogenic NLRP3 inflammasome inhibitor, attenuates stress-induced behavioral and inflammatory responses. Sci Rep. 2017;7:7677. doi:10.1038/s41598-017-08055-1
42. Minervini G, Franco R, Maddalena M, et al. Correlation between Temporomandibular Disorders (TMD) and Posture Evaluated trough the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD): a systematic review with meta-analysis. J Clin Med. 2023;12:2652. doi:10.3390/jcm12072652
43. Minervini G, Franco R, Maddalena M, et al. Prevalence of temporomandibular disorders in subjects affected by Parkinson disease: a systematic review and metanalysis. J Oral Rehabil. 2023;50:877–885. doi:10.1111/joor.13496
44. Ito M, Kimura H, Yoshida K, et al. Effectiveness of milnacipran for the treatment of chronic pain in the orofacial region. Clin Neuropharmacol. 2010;33:79–83. doi:10.1097/WNF.0b013e3181cb5793
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.