Back to Journals » Clinical Epidemiology » Volume 11
Serum 25-hydroxyvitamin D levels predict cancer survival: a prospective cohort with measurements prior to and at the time of cancer diagnosis
Authors Robsahm TE ![]() , Tretli S
, Tretli S ![]() , Torjesen PA, Babigumira R
, Torjesen PA, Babigumira R ![]() , Schwartz GG
, Schwartz GG
Received 1 March 2019
Accepted for publication 17 May 2019
Published 8 August 2019 Volume 2019:11 Pages 695—705
DOI https://doi.org/10.2147/CLEP.S207230
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor H Sorensen
Trude Eid Robsahm,1 Steinar Tretli,1 Peter Abusdal Torjesen,2 Ronnie Babigumira,1 Gary G Schwartz3
1The Cancer Registry of Norway, Institute of Population-based Cancer Research, Oslo, Norway; 2The Hormone Laboratory, Department of Endocrinology, Oslo University Hospital Health Authority, Oslo, Norway; 3Department of Population Health, University of North Dakota School of Medicine and Health Sciences, Grand Forks, ND, USA
Purpose: Circulating 25-hydroxyvitamin D (25-OHD) levels have been inversely associated with cancer death, but the nature of this relationship is unclear. We investigated this association using repeated measurements of serum 25-OHD.
Patients and methods: Pre-diagnostic serum samples were collected in population health surveys in Norway (1973–2004). Participants who subsequently developed cancer (1984–2004) provided a second serum sample at the time of cancer diagnosis. Samples were stored in the Janus Serum Bank. Repeated samples existed from 202 breast cancers, 193 lung cancers, 124 lymphomas, and 37 colon cancers. Serum 25-OHD was measured via competitive radioimmunoassay. Cox regression models assessed associations between 25-OHD and cancer-specific death (case fatality) through 2012, given as hazard ratios (HRs) with 95% confidence intervals (CIs).
Results: The median time between pre-diagnostic and diagnostic samples was 14.4 years. The median 25-OHD levels were 63.3 and 62.5 nmol/L, respectively. During follow-up, 313 cancer deaths occurred. Compared to low pre-diagnostic 25-OHD levels (<46 nmol/L), higher levels (≥46 nmol/L) had significantly lower HRs (39–54%) of case fatality. This result was also seen for the diagnostic samples. Donors who had both samples at high (≥62 nmol/L) levels had 59% lower HR of case fatality, compared to those for whom both samples were at low levels (<46 nmol/L). Furthermore, versus a decline in serum 25-OHD (median −22.4 nmol/L) from pre-diagnostic to diagnostic samples, a rise (median 22.3 nmol/L) was associated with lower case fatality (HR 0.57, 95% CI 0.43−0.75).
Conclusion: Our findings suggest a causal relationship between vitamin D and cancer case fatality.
Keywords: serum 25-OHD, repeated measurement, longitudinally, cancer case fatality
Introduction
Over the last 30 years, vitamin D metabolites have received increasing attention for their potential to prevent and/or retard cancer development. Laboratory studies have shown pleitropic anti-cancer effects of the hormonal form of vitamin D, 1,25-dihydroxycholecalciferol (1,25(OH)2D), including control of cell differentiation, proliferation, and metastasis.1 Associations between vitamin D and the natural history of cancer also have been observed in epidemiologic studies, which often preceded the laboratory studies.2 Most seroepidemiological studies have used measurements of the pro-hormonal form of vitamin D, 25-hydroxyvitamin D (25-OHD), the accepted marker of an individual’s vitamin D status.1,3 25-OHD is formed by hydroxylation of vitamin D in the liver after vitamin D is synthesized in the skin from exposure to sunlight (vitamin D3) or is obtained from the diet (vitamins D2 or D3). In addition to the “classical” endocrine synthesis of 1,25(OH)2D in the kidney, many non-renal cells convert 25-OHD intracellularly to 1,25(OH)2D in an autocrine manner (non-classical synthesis).4–8 Recognition of non-classical 1,25(OH)2D synthesis established a mechanism for vitamin D in cancer prevention.
Several studies have reported improved survival for cancer patients with higher circulating 25-OHD levels at the time of diagnosis.9,10 However, the nature of that relationship is unclear. At least two explanations are possible: (A) High circulating 25-OHD inhibits the process of the cancer disease via biological mechanisms;1 (B) The processes and/or consequences of cancer cause serum 25-OHD levels to fall (ie, reverse causality). The latter could occur through several mechanisms, including reduced sunlight exposure among cancer patients.11 One way to discriminate between these explanations is by using repeated measurements of 25-OHD obtained at different time points with respect to the time of cancer diagnosis. For example, observing a lower rate of cancer death among cases whose pre-diagnostic and diagnostic levels of 25-OHD were high would favor explanation A, as would a lower rate of cancer death among cases with increasing 25-OHD levels across the two samples. Conversely, a higher rate of cancer death among cases with continuously low 25-OHD levels as well as among cases with a temporal decline in 25-OHD levels across the two samples could be more consistent with explanation B.
We previously reported that 25-OHD levels below 50 nmol/L at the time of diagnosis were associated with elevated case fatality in individuals with cancer of the prostate,12 breast, colon, lung, and lymphoma.13 For the cases with cancer of breast, colon, lung, and lymphoma, we were now able to investigate serum levels of 25-OHD longitudinally. We examined the effects of the following conditions on cancer case fatality: low serum 25-OHD years prior to cancer diagnosis, longitudinally low serum 25-OHD, years prior to and at the time of the cancer diagnosis, and changes in serum 25-OHD levels from pre-diagnostic to diagnostic samples.
Materials and methods
The Janus Serum Bank in Norway is a population-based biobank established in 1973 that includes more than 450,000 serum samples from approximately 317,000 adult donors. Ninety-one percent (91%) of the donors were recruited from population-based health surveys for the 35−49 year age group in the period 1973−2004 (attendance rate 88%). The remainder (9%) were recruited among blood donors. A detailed description of the Janus Serum Bank cohort is published elsewhere.14 Donors who subsequently developed cancer and were admitted to the Norwegian Radium Hospital for cancer treatment donated an additional serum sample. All serum samples were stored at −25°C. In a previous study,13 we identified Janus Serum Bank donors with a diagnostic serum sample collected on average 38 days from diagnosis, prior to cancer treatment, who were alive at least 30 days after serum collection. Cases with histologically verified invasive cancer were identified via linkage with the Cancer Registry of Norway. Based on the World Health Organization’s International Classification of Diseases codes for cancer, 10th edition (ICD-10), cases with cancer of breast (C50), colon (C18), lung (C33−34), and lymphoma (C81−86, C96) were selected, giving a study cohort of 658 cancer cases. Data from the study cohort were re-linked to the Janus Serum Bank in order to identify cases with an available serum sample from the initial health surveys. Among these 658 cases, 102 had insufficient serum volume in their health survey sample for 25-OHD assessment, resulting in a study cohort of 556 cases.
National health registries
The Cancer Registry of Norway has recorded cancer diagnoses compulsorily by law since 1953. The completeness of registration is estimated to exceed 98%.15 Since 1951, all deaths of Norwegian citizens have been recorded by the national Cause of Death Registry. Linkages between these registries and the Janus Serum Bank are possible by the unique 11-digit personal identification number assigned to all Norwegian citizens. The study file provided information about the cancer diagnoses, age, sex, vital status, date, and cause of death, and date of migration, throughout 2012.
25-OHD assessment and categorization
For analysis of 25-OHD, 75 μL of serum was drawn from each sample. The analysis was performed via a competitive radioimmunoassay (DiaSorin, Stillwater, MN) at the National Hormone Laboratory (at Oslo University Hospital), according to standard procedure for the laboratory. All serum samples were analyzed in August 2015.
For reproducibility, serum 25-OHD levels, both the pre-diagnostic and diagnostic samples, were categorized according to quartile limits (nmol/L) used in our previous study (<46, 46−61, 62−81, ≥82).13 In analyses by cancer site, we used cancer-specific category limits of 25-OHDas previously used (breast (≤50, 51−67, 68−86, >86), colon (≤44, 45−56, 57−77, >77), lung (≤41, 42−56, 57−76, >76), lymphoma (≤44, 45−60, 61−77, >77)).13
To account for variability in 25-OHD levels due to seasonal variation in ultraviolet radiation in Norway,16 date of blood sampling was categorized as Winter (December–February), Spring (March–May), Summer (June–August), and Fall (September–November). Moreover, to account for seasonal variability in analyses based on combinations of the repeated serum samples, the pre-diagnostic and diagnostic 25-OHD values were season-standardized using a seasonal variation factor, defined as the ratio of the 25-OHD average to the monthly 25-OHD average. Using the season-standardized 25-OHD values in both samples, we defined subgroups of all possible combinations of low (<46 nmol/L), intermediate (46–61 nmol/L), and high (>62 nmol/L) levels in the two samples. Finally, season-standardized change in serum 25-OHD was calculated and categorized by tertiles (T): T1=loss (range −84.2 to −8.6 nmol/L); T2=stable (range −8.5 to +9.5 nmol/L); T3=rise (range +10.0 to +110.9 nmol/L).
The outcome, case fatality, was defined by the main cause of death reported on the death certificate (true if death from specific cancer).
Statistical analysis
Cases were followed from the date of diagnosis until the date of death, migration, or end of follow-up (31.12.2012), whichever came first. Descriptive analyses were conducted for patient characteristics. Cox proportional hazard regression models were used to assess associations between circulating 25-OHD and case fatality. First, separate analyses, adjusted for sex, age, season of serum sampling, and serum storage time, were conducted for pre-diagnostic and diagnostic samples. Second, stratified analyses were conducted by cancer site. Third, longitudinal analysis was conducted using categories of the season-standardized 25-OHD values, from the pre-diagnostic and the diagnostic samples combined; low/low versus all possible combinations of low, intermediate, and high levels, adjusted for sex age and serum storage time. Last, analysis was conducted using tertiles of season-standardized change in 25-OHD values (between pre-diagnostic and diagnostic samples), adjusted for sex and age.
Because the processes of carcinogenesis, from initial lesion to clinical detection, typically take years,17 we reasoned that if ongoing cancer processes or its consequences cause low serum 25-OHD (explanation B), this would be most apparent for cases for whom both samples were collected close to the time of cancer diagnosis. Therefore, we stratified analysis by time between the pre-diagnostic and diagnostic samples; short (≤10 years) and long (>10 years) time.
Additional analyses were conducted, to estimate HRs of cancer case fatality according to clinical categories of 25-OHD and according to season-standardized 25-OHD levels categorized into the predefined 25-OHD categories, separately for the pre-diagnostic and the diagnostic serum samples (Supplementary materials).
Analyses employed Stata 15 (StataCorp, College Station, TX). The statistical significance level was set at 5%. Effect estimates, from crude and adjusted models, are presented as hazard ratios (HRs), with 95% confidence intervals (CI).
Results
Patient characteristics are shown in Table 1. The median age at cancer diagnosis was 57 years (range 32−82) and was lowest for breast cancer (55 years) and highest for lung cancer (59 years). The median time between the pre-diagnostic and diagnostic serum sampling was 14.4 years (range 1.1−34.4), with the shortest median time span for breast cancer (11.7 years) and longest for lung cancer (17.7 years). The median 25-OHD level in pre-diagnostic samples was 63.3 nmol/L (17.4−142.5), with only minor differences between the cancer sites. The median diagnostic level of 25-OHD was 62.5 nmol/L (13.0−185.0), lowest for lung cancer (55.0 nmol/L) and highest for breast cancer (72.0). For the season-standardized change in serum 25-OHD, from the pre-diagnostic to the diagnostic samples, the median loss for T1 was −22.4 nmol/L (range −84.2 to −8.6) and the median rise for T3 was 22.3 nmol (range 10.0−110.9), whereas for T2, the category with stable levels the median change was 0.4 nmol/L (range −8.6 to 9.4).
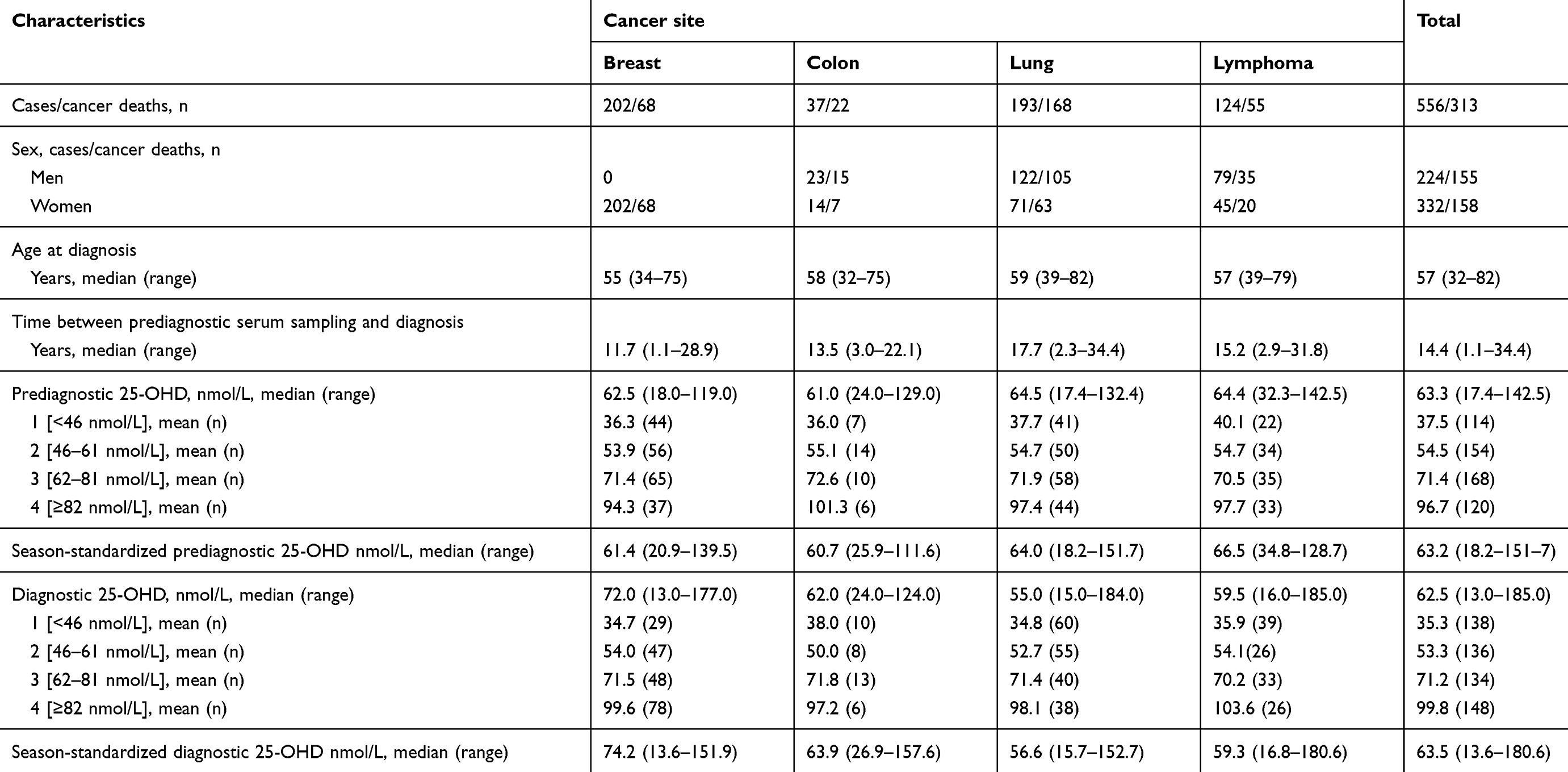 |
Table 1 Characteristics of the cancer patients; numbers (n), percentage (%), median, range, and means |
Four percent (4%) of the cases were diagnosed with cancer in the 1970s, 17% in the 1980s, 31% in the 1990s, and 48% during 2001−2012. Approximately two-thirds of the cases (n=369) died during follow-up, of which 313 (84.8%) were due to their cancer. This is consistent with the expected proportion of cancer deaths in Norway (85%) when taking cancer type, age at diagnosis, sex, and time of follow-up into account.18
Table 2 presents HRs for case fatality, all cancer sites together, by categories of pre-diagnostic and diagnostic serum 25-OHD. Results from the adjusted model show that, compared to category 1 (<46 nmol/L), cases with high serum levels, category 3 (62−81 nmol/L) and 4 (≥82 nmol/L), had significantly lower HRs of case fatality. The association was found for pre-diagnostic samples (HRs were 0.61 (95% CI 0.44−0.84) and 0.46 (95% CI 0.32−0.66), respectively) and diagnostic samples (HRs were 0.44 (95% CI 0.32−0.61) and 0.41 (95% CI 0.30−0.57), respectively). The dose–response trend was significant (ptrend ≤0.001). Similar results were found both when using clinical categories of 25-OHD (Table S1) and season-standardized 25-OHD levels categorized into the predefined 25-OHD categories (Table S2).
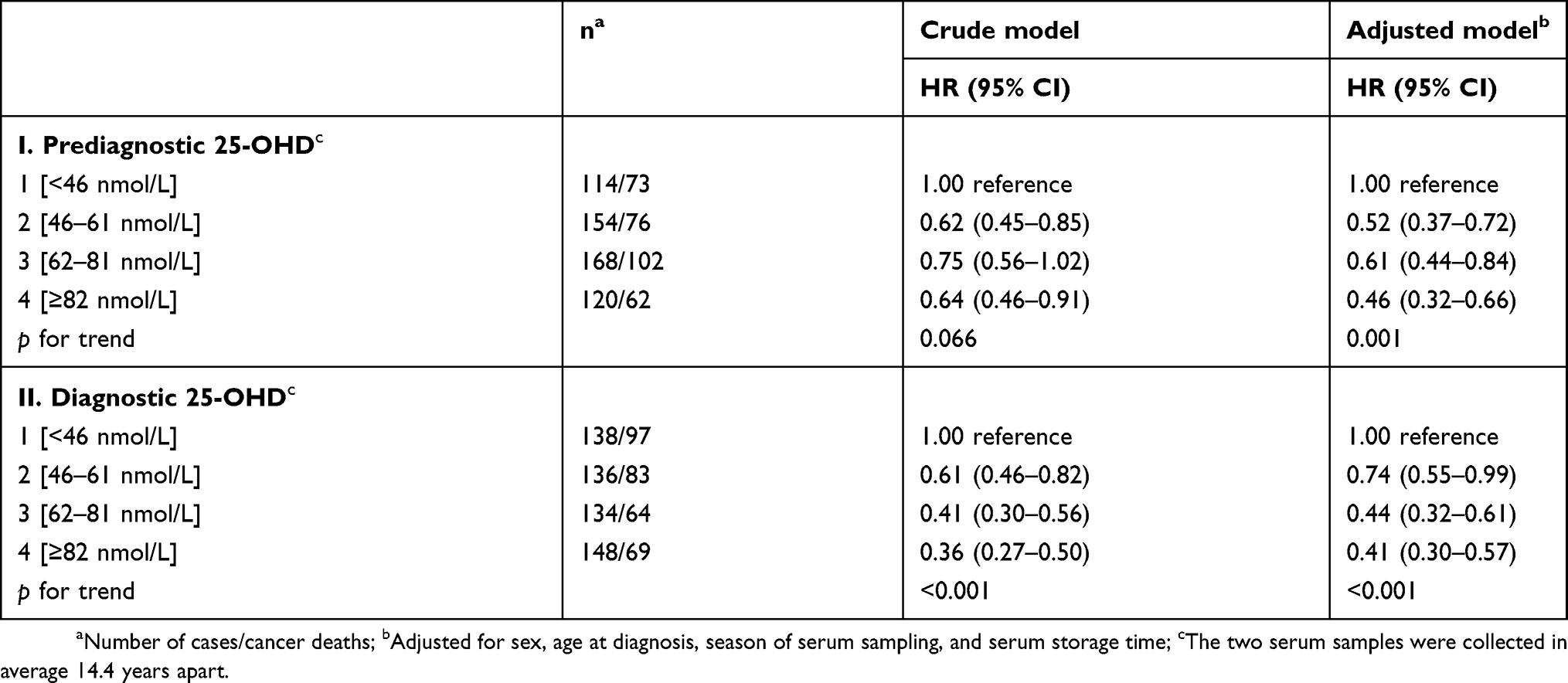 |
Table 2 Hazard ratios (HR) with 95% confidence interval (95% CI) of cancer case fatality according to predefined categories of prediagnostic (I) and diagnostic (II) 25-OHD levels, from crude and adjusted analyses |
Table 3 shows HRs for case fatality by cancer site, according to cancer-specific categories of 25-OHD (fully adjusted model) in pre-diagnostic and diagnostic samples. We found a similar pattern for all cancers, with the highest HR in cases with serum 25-OHD at the lowest category. Based on pre-diagnostic samples, however, statistically significant associations were found for lung cancer (ptrend 0.004) and lymphoma (ptrend 0.184), with HRs for the highest category of 0.55 (95% CI 0.31−0.96) and 0.29 (95% CI 0.10−0.82), respectively. Based on diagnostic samples, the association was statistically significant for all sites; breast (ptrend 0.008), colon (ptrend 0.033), lung (ptrend <0.001), and lymphoma (ptrend 0.003).
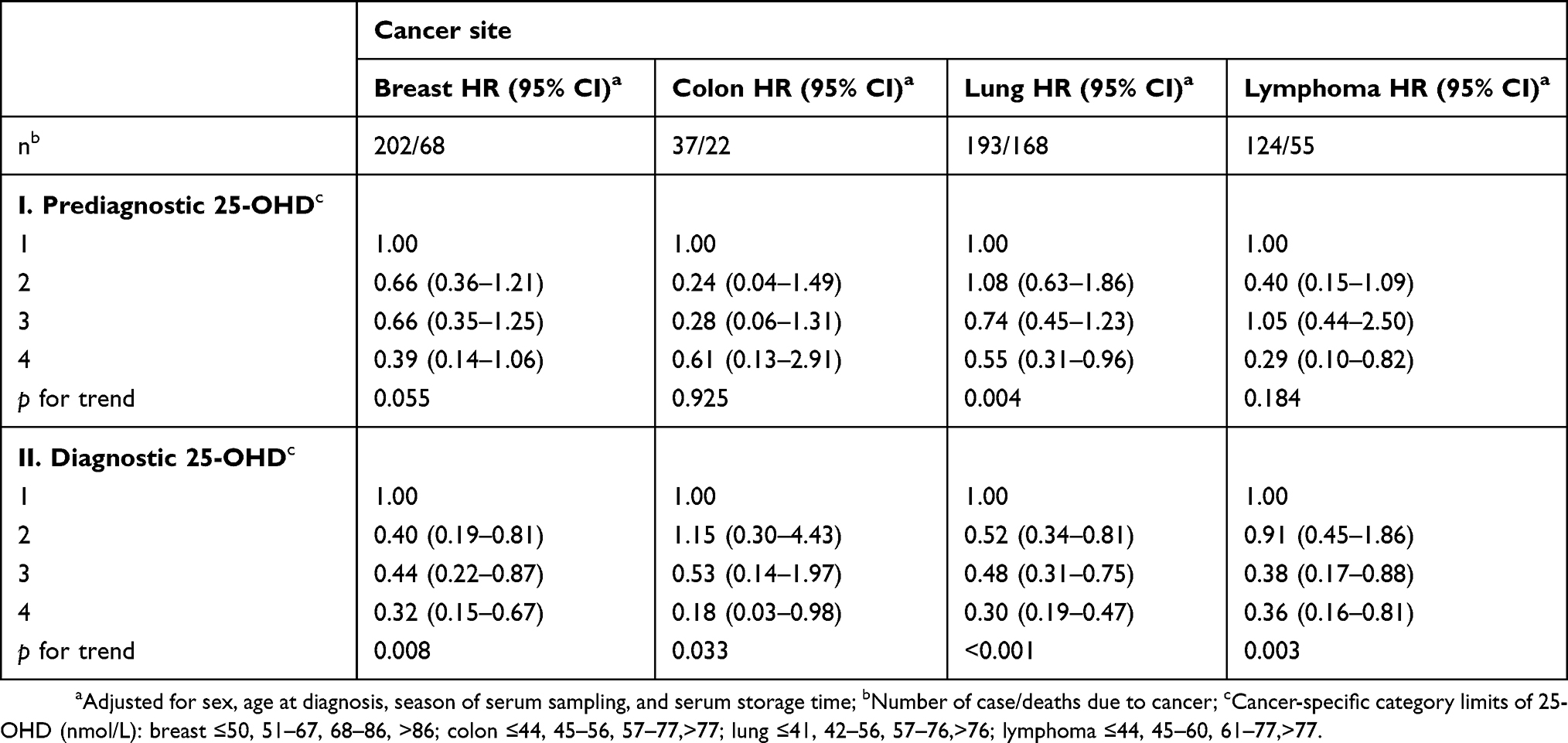 |
Table 3 Hazard ratios (HR) with 95% confidence interval (95% CI) of cancer case fatality by cancer site, according to predefined cancer-specific categories of prediagnostic (I) and diagnostic (II) 25-OHD serum levels. The two serum samples were collected in average 14.4 years apart |
Compared to donors with low 25-OHD levels (<46 nmol/L) at both time points, lower HRs of case fatality were found for all combinations, except for the combination high (≥62 nmol/L)/low, with a significant dose–response trend (ptrend ≤0.001) (Table 4). Cases with both samples at high levels or the combination of intermediate (46–61 nmol/L)/high levels had 59–57% lower HRs (HR 0.41, 95% CI 0.27−0.61 and HR 0.43 95% CI 0.26−0.73, respectively). HRs for case fatality by change in season-standardized 25-OHD, from the pre-diagnostic to the diagnostic sample, in tertiles (T), are presented in Table 5. T3 cases, with rise in serum 25-OHD (median 22.3 nmol/L), had a significantly lower risk (HR 0.57, 95% CI 0.43−0.75), compared to T1, who had loss in serum 25-OHD (median −22.4 nmol/L). Also for T2, the group with stable 25-OHD levels (median change of 0.4 nmol/L), the risk was lower (HR 0.76, 95% CI 0.58−0.99) compared to T1. When stratifying this analysis by time between the pre-diagnostic and diagnostic samples, the association was significant only for cases with more than a 10-year time span between the samples (Table 5).
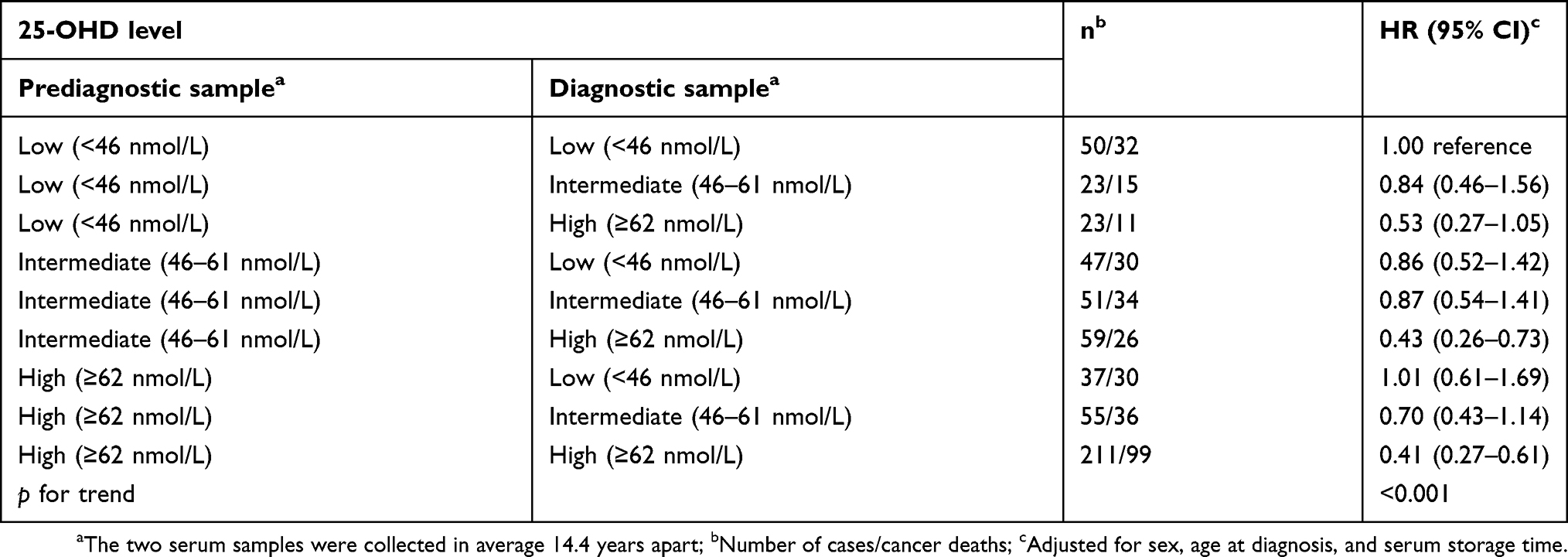 |
Table 4 Hazard ratios (HR) with 95% confidence intervals (95% CI) of cancer case fatality by all possible combinations of season-standardized 25-OHD categories in prediagnostic and diagnostic samples |
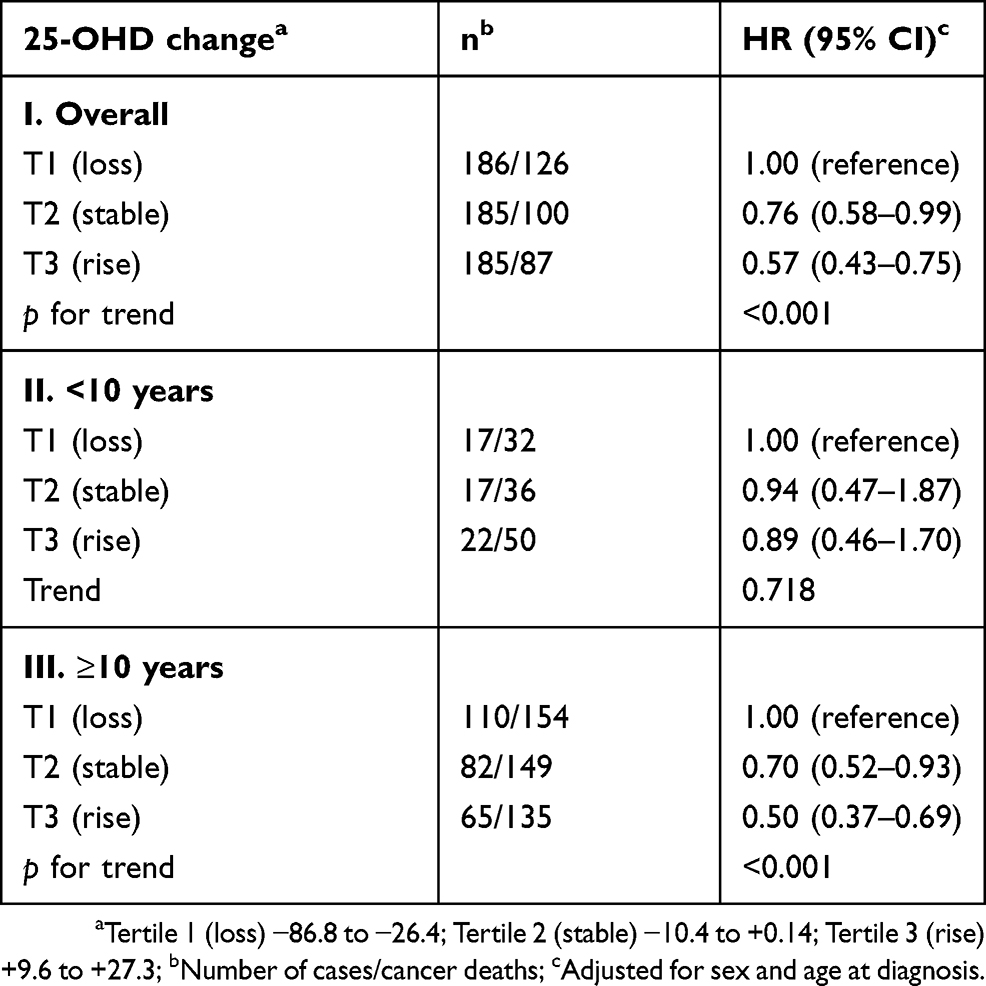 |
Table 5 Hazard ratios (HR) with 95% confidence interval (95% CI) of cancer case fatality by tertiles (T) of change in season-standardized 25-OHD between prediagnostic and diagnostic samples, overall (I), and according to time-span between collection of the samples; <10 years (II) and ≥10 years (III) |
Discussion
To our knowledge, this is the first study to use repeated measurements of the 25-OHD, obtained at different time points with respect to cancer diagnosis, to study the relationship between 25-OHD and cancer survival. We found that higher levels of 25-OHD, in both pre- and diagnostic serum samples, predict cancer survival. For the four cancer sites studied, cases with 25-OHD levels ≥46 nmol/L had lower hazards of case fatality, compared to lower 25-OHD levels. This result held for pre-diagnostic sample, collected on average 14.4 years prior to the cancer diagnosis as well as for diagnostic samples. Moreover, cases who had 25-OHD levels at ≥62 nmol/L in both samples had less than half the hazard of case fatality, compared to cases with both samples at levels <46 nmol/L. Last, we found that, compared to a decline in 25-OHD, cases with stable levels of 25-OHD and those with rising levels, from pre-diagnostic to diagnostic samples, had significantly lower hazards of case fatality.
The findings for the diagnostic samples confirm those in our previous study,13 even though the current analysis was based on a smaller number of donors (since both pre-diagnostic and diagnostic samples were required), suggesting robustness of the original findings. Further, both overall and site-specific results for the diagnostic sample are consistent with recent reports on 25-OHD and cancer survival. For example, recent meta-analyses reported improved cancer survival in cases with high 25-OHD versus cases with low 25-OHD, measured at most 1 year from diagnosis, which was significant for breast, colorectal, and hematological cancer. For lung cancer, no association was found.9,10
In the present study, we studied serum samples collected up to three decades prior to the cancer diagnosis. We found a significant inverse association between 25-OHD levels and case fatality. Our results are consistent with the recent findings reported from the Alpha-Tocopherol, Beta-Carotene (ATBC) Cancer Prevention Study which reported a positive association between the 25-OHD levels decades prior to the cancer diagnosis and cancer survival.19 The ATBC cohort was restricted to the male smoking population and had only one 25-OHD measurement (pre-diagnostic). Strengths of the current study are that it is population-based, includes both sexes, and adds the ability to investigate the association longitudinally using repeated 25-OHD measurements. Our result is also consistent with most (but not all22) large meta-analyses on cancer mortality based on prospectively measured 25-OHD.2,20,21
Site-specific analyses based on pre-diagnostic serum samples showed lower HRs for case fatality for the highest category of 25-OHD for all four cancer sites, although was statistically significant for lymphoma and lung cancer only. A similar inverse relation between prospectively measured 25-OHD and lung cancer mortality was found in a Danish study.23 Conversely, a study from NHANES III found a positive association for men but no association for women.24 Also, the ATBC study, based on men only, found a positive association between pre-diagnostic 25-OHD and lung cancer mortality.19 Possible explanations for the discrepant results may be due to differences between the study cohorts. For example, the ATBC study included smokers only and participants were older at serum sampling than the Janus donors, both factors which are associated with lower levels of 25-OHD.25,26 Further, when comparing the median pre-diagnostic 25-OHD levels, participants in the ATBC study had lower levels (34.7 nmol/L (range 14.4–66.1) in non-survivors and 36.5 nmol/L (range 15.6–68.0) in survivors)19 than in the current study (63.3 nmol/L (range 17.4–142.5)).
For lymphoma, the ATBC study did not report separate results, but for hematological cancers as a group, no association was found.19 With regard to breast cancer, we found no comparable studies. However, the survival rate for breast cancer is high and any potential effect of the 25-OHD status years prior to diagnosis might be difficult to demonstrate. For colon cancer, the evidence is unclear. In the present study, the small number of cases is a limitation. The ATBC study found no association, but studied colorectal cancer as a group,19 whereas a large study within the European Prospective Investigation into Cancer and Nutrition cohort (EPIC) observed a significant association between high pre-diagnostic 25-OHD and improved survival for colon cancer cases.27
The present study adds several innovations to the literature on vitamin D and survival. First, we examined 25-OHD levels longitudinally and are the first to demonstrate how changes in 25-OHD over time were associated with case fatality. Cases with high season-standardized 25-OHD levels (≥62 nmol/L), in both serum samples, had less than half the HR of case fatality, compared to cases with low levels (<46 nmol/L) at both time points (Table 4). Moreover, we found that a rise in season-standardized 25-OHD (median rise 22.3 nmol/L), from the pre-diagnostic to the diagnostic serum sample, was associated with significantly lower HR (50%) of case fatality, compared to a loss (median −22.4 nmol/L). Cancer development typically spans several years,17 and a strong argument against a cause-and-effect relationship between 25-OHD and cancer prognosis is that cancer processes or consequences of the disease cause the 25-OHD level to fall. To test this, we stratified analysis by time between the serum samples. Our findings for the time interval of more than 10 years and not for the shorter time interval (Table 5) argue against the reverse causality argument. Considered together, our results are consistent with the hypothesis that high circulating 25-OHD retard cancer processes.
There may be several mechanisms whereby 25-OHD exerts anti-cancer effects. It was previously believed that the hormonal form of vitamin D, 1,25(OH)2D, was the only vitamin D metabolite that acted to retard cancer and that its autocrine synthesis depended upon the level of its substrate, 25-OHD. However, evidence from several cancers, including prostate and lung cancer, indicates that 25-OHD can activate the receptor for 1,25(OH)2D and exert genomic responses.5,28 Low 25-OHD levels are also shown to be associated with higher serum levels of inflammatory cytokines and poor immune function that are biomarkers of adverse prognosis in several cancers.29,30 In this regard, vitamin D supplementation may support immune responses of cancer patients and contribute thereby to improved survival.30 It is noteworthy that a recent review of studies of vitamin D supplementation reported supplementation to play an important role in disease-free survival in a number of cancers.31
Alternative explanations for the inverse association found between 25-OHD status and case fatality in cancer patients include chance, selection bias, and confounding. We believe that chance is an unlikely explanation as our results were consistent across cancer sites and were consistent for both pre-diagnostic and diagnostic samples. Significant selection and/or survival bias is unlikely since the Janus cohort is population-based and there was no loss to follow-up.32 Long storage time of serum, before 25-OHD assessment, could have influenced our results, but long-term storage of serum has been shown to have little effect on serum levels of 25-OHD.33 Additionally, the associations persisted after storage time was taken into account. However, effects of personal characteristics and potential confounding factors cannot be excluded. The 25-OHD level is influenced by sun exposure and thus varies with season and place of residence. Although we accounted for season of sampling, we did not have information about individual differences in sun exposure or lifestyle factors, such as physical activity and body mass index (BMI) that are associated with both 25-OHD level and cancer death. However, in studies taking such factors into account, these factors did not change the results significantly.2,9,10
Furthermore, genetic and epigenetic factors can account for variability in serum 25-OHD and alterations in its function.8 Secular changes in treatment could influence cancer survival if newer treatments were significantly better than older treatments and if the 25-OHD status increased over time. Our analysis indicates, however, that 25-OHD levels actually decreased slightly by calendar year of collection (ie, changed in a conservative direction).
Conclusion
Our study demonstrates that 25-OHD levels <46 nmol/L, both several years prior to and at the time of cancer diagnosis, were associated with higher case fatality. We found lower hazards of case fatality in cases with rise in serum 25-OHD toward diagnosis, when the pre-diagnostic sample was collected ≥10 years prior to the diagnosis. These data are consistent with explanation A; a causal relationship between higher vitamin D and reduced cancer case fatality.
Ethical approval
The study was approved by the National Committee for Research Ethics, South-East Health Authority and by the Janus Serum Bank board. All procedures performed in the study were in accordance with ethical standards of the institution and national research committee.
Abbreviations list
25-OHD, 25-Hydroxyvitamin D; HR, hazard ratio; CI, confidence interval; n, number; ICD-10, the World Health Organization’s International Classification of Diseases codes for cancer 10th edition; T, tertile; ptrend, p-value for trend; BMI, body mass index.
Acknowledgments
We address sincere thanks to Janus Serum Bank, which made this study possible. The Norwegian Cancer Society is gratefully acknowledged for grant support, and we also address our thanks to the Hormone Laboratory at Aker, Oslo University Hospital, for the 25-OHD assessment.
Author contributions
All authors contributed towards data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Bikle D Nonclassic actions of vitamin D. J Clin Endocrinol Metab. 2009;94:26–34. doi:10.1210/jc.2008-1454
2. Yin L, Ordonez-Mena JM, Chen T, Schöttker B, Arndt V, Brenner H Circulating 25-hydroxyvitamin D serum concentration and total cancer incidence and mortality: A systematic review and meta-analysis. Prev Med. 2013;57:753−64. doi:10.1016/j.ypmed.2013.08.026
3. Cashman KD, van den Heuvel EGHM, Schoemaker RJW, Preveraud DP, Macdonald HM, Arcot J 25-hydroxyvitamin D as a biomarker of vitamin D status and its modeling to inform strategies for prevention of vitamin D deficiency within the population. Sdv Nutr. 2017;8:947−57.
4. Schwartz GG, Whitlatch LW, Chen TC, Lokeshwar BL, Holick MF Human prostate cells synthesize 1,25-dihydroxyvitamin D3 from 25-hydroxyvitamin D3. Cancer Epidemiol Biomarkers Prev. 1998;7(5):391–395.
5. Barreto A, Schwartz GG, Woodruff R, Cramer SD 25-hydroxyvitamin D3, the prohormonal form of 1,25-Dihydroxyvitamin D3, inhibits the proliferation of primary prostatic epithelial cells. Cancer Epidemiol Biomarkers Prev. 2000;9:265−270.
6. Chen TC, Schwartz GG, Burnstein KL, Lokeshwar BL, Holick MF The in vitro evaluation of 25-hydroxyvitamin D3 and 19-nor-1,25-dihydroxyvitamin D2 as therapeutic agents for prostate cancer. Clin Cancer Res. 2000;6:901−8.
7. Swami S, Krishnan AV, Wang JY, et al. Dietary vitamin D3 and 1,25-dihydroxyvitamin D3 (calcitriol) exhibit equivalent anticancer activity in mouse xenograft models of breast and prostate cancer. Endocrinolology. 2012;153:2576−87. doi:10.1210/en.2011-1600
8. Merchan BB, Morcillo S, Martin-Nunez G, Tinahones FJ, Marcias-Gonzalez M The role of vitamin D and VDR in carcinogenesis: through epidemiology and basic science. J Steroid Biochem Mol Biol. 2017;167:203−18.
9. Li M, Chen P, Li J, Chu R, Xie D, Wang H Review: the impact of circulating 25-hydroxyvitamin D levels on cancer patient outcomes: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2014;99:2327−36. doi:10.1210/jc.2013-4320
10. Vaughan-Shaw PG, O’Sullivan F, Farrington SM, et al. The impact of vitamin D pathway genetic variation and circulating 25-hydroxyvitamin D on cancer outcome: systematic review and meta-analysis. Brit J Cancer. 2017;116:1092−1110. doi:10.1038/bjc.2017.44
11. Robsahm TE, Schwartz GG, Tretli S The inverse relationship between 25-hydroxyvitamin D and cancer survival: discussion of causation. Cancers (Basel). 2013;5(4):1439−55. doi:10.3390/cancers5041439
12. Tretli S, Hernes E, Berg JP, Hestvik UE, Robsahm TE Association between serum 25(OH)D and death from prostate cancer. Brit J Cancer. 2009;100:450−54. doi:10.1038/sj.bjc.6604865
13. Tretli S, Schwartz GG, Torjesen PA, Robsahm TE Serum levels of 25-hydroxyvitamin D and survival in Norwegian patients with cancer of breast, colon, lung, and lymphoma: a population-based study. Cancer Causes Control. 2012;23:363−70. doi:10.1007/s10552-011-9885-6
14. Langseth H, Gislefoss RE, Martinsen JI, Dillner J, Ursin G Cohort profile: the janus serum bank cohort in Norway. Int J Epidemiol. 2017;46(2):403−404g. doi:10.1093/ije/dyw317
15. Larsen IK, Smastuen M, Johannesen TB, et al. Data quality at the cancer registry of Norway: an overview of comparability, completeness, validity and timeliness. Eur J Cancer. 2009;45(7):1218−31. doi:10.1016/j.ejca.2008.10.037
16. Aalerud TN, Johnsen BJ The Norwegian UV monitoring network. Period 1995/96 to 2004. Report 2006: 4. Østerås: Norwegian Radiation Protection Authority; 2006.
17. Yachida S, Jones S, Bozic I, et al. Distant metastasis occurs late during the genetic evolution of pancreatic cancer. Nature. 2010;467:1114−17. doi:10.1038/nature09515
18. Cancer Registry of Norway. Cancer in Norway 2017 – Cancer Incidence, Mortality, Survival and Prevalence in Norway. Oslo: Cancer Registry of Norway, 2018.
19. Weinstein SJ, Mondul AM, Yu K, et al. Circulating 25-hydroxyvitamin D up to 3 decades prior to diagnosis in relation to overall and organ-specific cancer survival. Eur J Epidemiol. 2018 [Epub ahead of print]. doi:10.1007/s10654-018-0428-2
20. Chowdhury R, Kunutsor S, Vitezova A, et al. Vitamin D and risk of cause specific death: systematic review and meta-analysis of observational cohort and randomised intervention studies. BMJ. 2014;348:g1903. doi:10.1136/bmj.g1903
21. Schöttker B, Jorde R, Peasey A, et al. Consortium on health and ageing: network of cohorts in Europe and the United States. Vitamin D and mortality: meta-analysis of individual participant data from a large consortium of cohort studies from Europe and the United States. BMJ. 2014;348:g3656. doi:10.1136/bmj.g3656
22. Gaksch M, Jorde R, Grimnes G, et al. Vitamin D and mortality: individual participant data meta-analysis of standardized 25-hydroxyvitamin D in 26916 individuals from a European consortium. PLoS One. 2017;12(2):e0170791. doi:10.1371/journal.pone.0170791
23. Afzal S, Brøndum-Jacobsen P, Bojesen SE, Nordestgaard BG Genetically low vitamin D concentrations and increased mortality: mendelian randomisation analysis in three large cohorts. BMJ. 2014;349:g6330. doi:10.1136/bmj.g6330
24. Freedman DM, Looker AC, Abnet CC, Linet MS, Graubard BI Serum 25-hydroxyvitamin D and cancer mortality in the NHANES III study (1988–2006). Cancer Res. 2010;70:8587−97. doi:10.1158/0008-5472.CAN-10-1420
25. Mousavi SE, Amini H, Heydarpour P, Chermahini FA, Godderis L Air pollution, environmental chemicals, and smoking may trigger vitamin D deficiency: evidence and potential mechanisms. Environ Int. 2018;122:67−90. pii: S0160-4120(18)32126-3.
26. Schöttker B, Hagen L, Zhang Y, et al. Serum 25-hydroxyvitamin D levels as an ageing marker. Strong associations with age and all-cause mortality independent from telomere length, epigenetic age acceleration and 8-isoprostane levels. J Gerontol A Biol Sci Med Sci. 2018;74(1):121−128.
27. Fedirko V, Riboli E, Tjønneland A, et al. Pre-diagnostic 25-hydroxyvitamin D, VDR and CASR polymorphisms, and survival in patients with colorectal cancer in Western European populations. Cancer Epidemiol Biomarkers Prev. 2012;21(4):582−9. doi:10.1158/1055-9965.EPI-11-1065
28. Verone-Boyle AR, Shoemaker S, Attwood K, et al. Diet-derived 25-hydroxyvitamin D3 activates vitamin D receptor target gene expression and suppresses EGFR mutant non-small cell lung cancer growth in vitro and in vivo. Oncotarget. 2016;7(1):995–1013. doi:10.18632/oncotarget.6493
29. Kim SJ, Shu C, Ryu KJ, et al. Vitamin D deficiency is associated with inferior survival of patients with extranodal natural killer/T-cell lymphoma. Cancer Sci. 2018. [Epub ahead of print]. doi:10.1111/cas.13844
30. Bochen F, Balensiefer B, Körner S, et al. Vitamin D deficiency in head and neck cancer patients - prevalence, prognostic value and impact on immune function. Oncoimmunology. 2018;7(9):e1476817. doi:10.1080/2162402X.2018.1490854
31. Griffin N, Dowling M Vitamin D supplementation and clinical outcomes in cancer surviovorship. Br J Nurs. 2018;27(19):1121–1128. doi:10.12968/bjon.2018.27.19.1121
32. Hjerkind KV, Gislefoss RE, Tretli S, et al. Cohort profile update: the janus serum bank cohort in Norway. Int J Epidemiol. 2017;46(4):1101−1102f. doi:10.1093/ije/dyw317
33. Agborsangaya C, Toriola AT, Grankvist K, et al. The effects of storage time and sampling season on the stability of serum 25-hydroxy vitamin D and androstenedione. Nutr Cancer. 2010;62(1):51−7.
Supplementary materials
Additional analyses were conducted to estimate hazard ratios (HR) of cancer case fatality according to clinical categories of 25-OHD, both for pre-diagnostic and diagnostic samples. The established limits for vitamin D levels are defined with respect to bone health, with cut-off at ≥50 nmol/L for sufficiency.1 Laboratories use categories of vitamin D levels as follows: deficient <25 nmol/L, insufficient <50 nmol/L, sufficient 50–75 nmol/L and optimal >75 nmol/L.2 Due to low numbers (only 9 in deficient), we collapsed the deficient and insufficient categories. Results from the adjusted model (Table S1) show that, compared to insufficient levels (<50 nmol/L), cases with sufficient (50–75 nmol/L) and optimal levels (>75 nmol/L) have significantly lower HRs of case fatality. The association was found for the pre-diagnostic and the diagnostic samples. The dose–response trend was significant (ptrend ≤0.001).
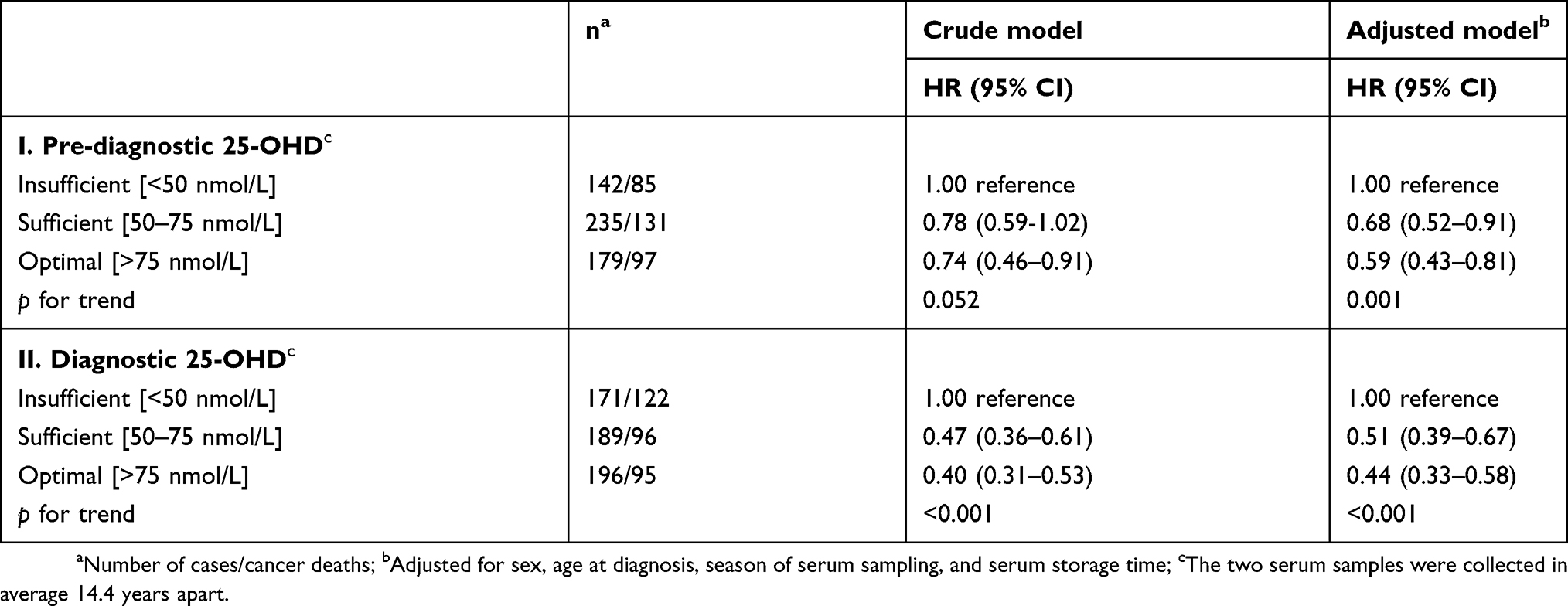 |
Table S1 Hazard ratios (HR) with 95% confidence interval (95% CI) of cancer case fatality according to clinically categories of pre-diagnostic (I) and diagnostic (II) 25-OHD levels |
The 25-OHD levels in the Norwegian population vary by season due to seasonal variation in ultraviolet radiation. To account for this variability, the date of blood sampling was categorized as Winter (December–February), Spring (March–May), Summer (June–August), and Fall (September–November), which variable was included in the analysis model (Tables 2 and 3, adjusted model). In analyses based on combinations of the repeated serum samples, we used another approach to account for seasonal variation. The 25-OHD levels were season-standardized, using a seasonal variation factor that was defined as the ratio of the 25-OHD average to the monthly 25-OHD average. This ratio, which is similar to the ratio in the moving average method of de-trending time-series data,3 was used to smooth out the fluctuations in levels of 25-OHD that are due to season. Table S2 shows HRs of cancer case fatality by season-standardized 25-OHD levels categorized into the predefined 25-OHD categories, separately for the pre-diagnostic and the diagnostic serum samples. Results from the adjusted model show significantly lower HRs of case fatality for cases with serum levels in category 3 (62−81 nmol/L) and 4 (≥82 nmol/L), compared to cases in category 1 (<46 nmol/L). The association was found for pre-diagnostic and diagnostic samples, with a significant dose–response trend (ptrend 0.007 and <0.001, respectively).
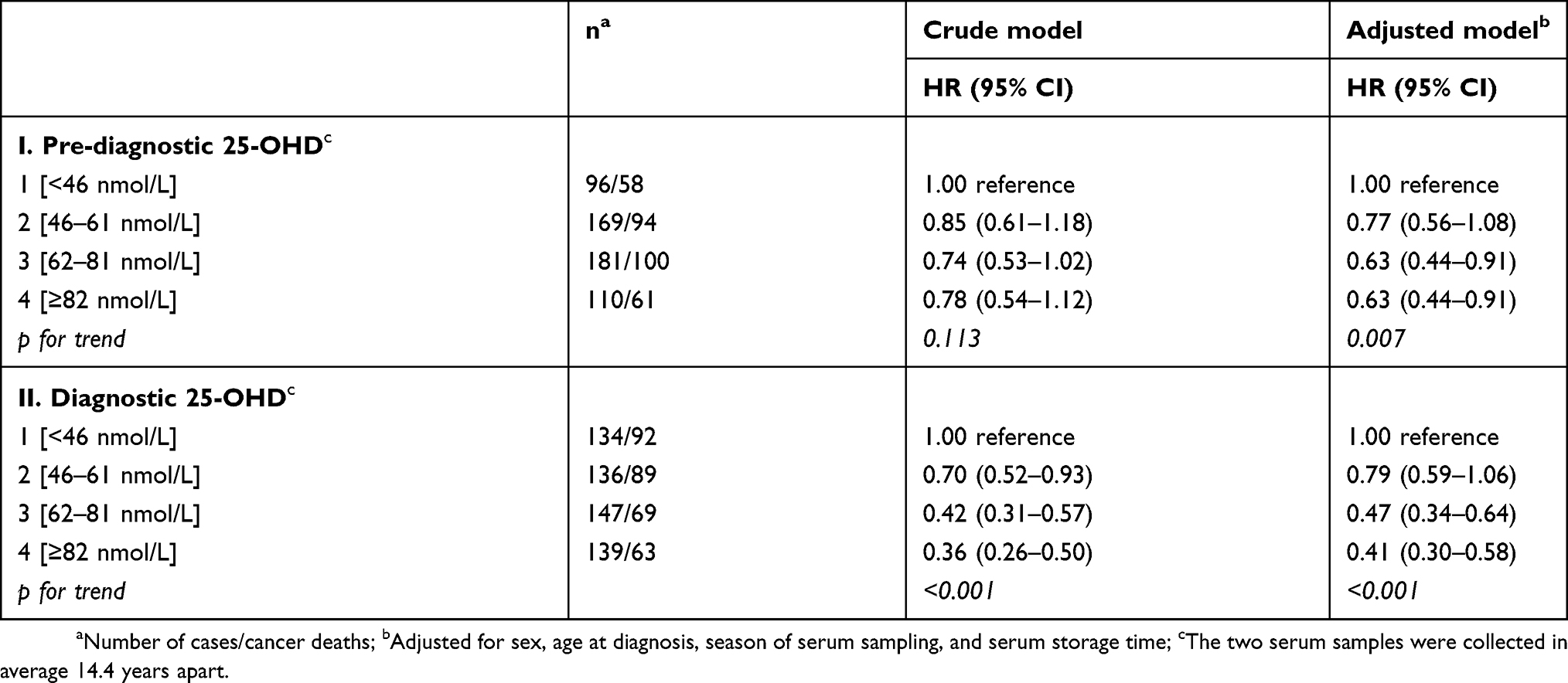 |
Table S2 Hazard ratios (HR) with 95% confidence interval (95% CI) of cancer case fatality according to season-standardized 25-OHD levels in predefined categories of pre-diagnostic (I) and diagnostic (II) 25-OHD levels |
References
1. The National Advice Board for Nutrition. [Vitamin D in Norway]. Helsedirektoratet, IS 2772, Oslo, Norway: Helsedirektoratet; 2018. Available from: https://www.helsedirektoratet.no/search?searchquery=vitamin+D+i+befolkningen&type=helsedirektoratet%3Arapport.Norwegian. Norwegian.
2. Fürst medical laboratory. Available from: http://www.furst.no/analyse-og-klinikk/analyser/vitamin-d/. Accessed May 6, 2019. Norwegian.
3. Carlberg C. Moving averages and centered moving averages. In: More Predictive Analytics: Microsoft Excel, Que; Upper Saddle River: Que (Pearson Education Informit); 2015. Available from: http://www.informit.com/articles/article.aspx?p=2433607&seqNum=2.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.