")
Back to Journals » Infection and Drug Resistance » Volume 16
Seroprevalence and Associated Factors of Hepatitis B and Hepatitis C Viral Infections Among Prisoners in Tigrai, Northern Ethiopia
Authors Tsegay B, Gebrecherkos T, Kahsay AG , Abdulkader M
Received 18 March 2023
Accepted for publication 7 June 2023
Published 13 June 2023 Volume 2023:16 Pages 3743—3750
DOI https://doi.org/10.2147/IDR.S410017
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Belaynesh Tsegay,1 Teklay Gebrecherkos,2 Atsebaha Gebrekidan Kahsay,2 Mahmud Abdulkader2
1Ayder Comprehensive Specialized Hospital Laboratory Department, Mekelle University, Mekelle, Tigrai, Northern Ethiopia; 2Department of Medical Microbiology and Immunology, College of Health Sciences, Mekelle University, Mekelle, Tigrai, Northern Ethiopia
Correspondence: Atsebaha Gebrekidan Kahsay, Department of Medical Microbiology and Immunology, Mekelle University, P.O. Box 1871, Mekelle, Tigrai, Northern Ethiopia, Email [email protected]
Background: Hepatitis B and C viruses are important health and socioeconomic problem across the globe, with a remarkable number of diseases and deaths in sub-Saharan African countries. The burden of hepatitis is unknown in the prison settings of Tigrai. Therefore, we aimed to describe the seroprevalence and associated factors of hepatitis B and C viruses among prisoners in Tigrai, Ethiopia.
Methods: A cross-sectional study was carried out from February 2020 to May 2020 at the prison facilities of Tigrai. Demographics and associated factors were collected from 315 prisoners prospectively. Five milliliters of blood was collected and tested using rapid tests kits of HBsAg (Zhejiang orient Gene Biotech Co., Ltd., China) and HCV antibodies (Volkan Kozmetik Sanayi Ve Ticaret Ltd. STI, Turkey). Positive samples were confirmed using enzyme-linked immunosorbent assay (ELISA) (Beijing Wantai Biological Pharmacy Enterprise Co. Ltd). Data were analyzed using the Statistical Package for Social Sciences (SPSS) version 20 and p< 0.05 was considered statistically significant.
Results: The overall seroprevalence of HBV and HCV were 25 (7.9%) and 1 (0.3%), respectively. The majority of hepatitis B viral infections were identified from the age groups of 18– 25 years (10.7%) and unmarried prisoners (11.8%). Prisoners greater than 100 per cell (AOR=3.95, 95% CI=1.15– 13.6, p=0.029) and with a history of alcohol consumption (AOR=3.01, 95% CI=1.17– 7.74, p=0.022) were significantly associated with HBV infections.
Conclusion: The seroprevalence of HBV among prisoners was nearly high or borderline (7.9%) with a very low HCV prevalence (0.3%). HBV was most prevalent among young adults, those housed with a large number of prisoners per cell, and those who had a history of alcohol consumption. This study recommends that there should be prison-focused intervention, including regular health education, with the emphasis on the mode of transmission and introducing HBV screening policy for prisoners, especially when they enter the prison.
Keywords: seroprevalence, HBV, HCV, prisoners, Tigrai
Introduction
The hepatitis B and hepatitis C viruses are important health and socioeconomic problems across the world causing considerable numbers of diseases and deaths, especially in Africa and Asia.1 It is predicted that 2 billion and 170 million people have been infected by HBV and HCV, respectively, in the world. About 15–40% of patients with chronic hepatitis B virus can progress to liver cirrhosis, liver failure, and primary hepatocellular carcinoma (HCC).2,3 According to the most recent estimates of the Global Burden of Disease study, viral hepatitis is responsible for approximately 1.5 million deaths each year, which is comparable to annual deaths from HIV/AIDS, malaria, and tuberculosis (1.3, 0.9, and 1.3 million, respectively).4
In general, 80% (about 71.1 million people) of hepatitis C-infected individuals develop chronic HCV, of which 10–15% will develop liver cirrhosis.5 About 25% of global liver cancer cases are due to HCV infection.6 Chronic hepatitis B among prisoners showed varied prevalence rates globally; data reported from prison settings of the United States (US), Denmark, Belgium, Ireland, and Greece were 3.7%, 4.4%, 6.5%, 9%, and 5.8%, respectively.7,8 The majority of persons with chronic hepatitis B and hepatitis C are unaware of their infection and do not benefit from clinical care, treatment, or interventions. Thus, because of a lack of follow-up and approach to treatment, one-third of persons with chronic viral hepatitis will die because of liver disease, including cirrhosis, liver cancer, and liver failure.9
The main transmission routes of hepatitis B virus are horizontal (blood or sexual contact) and vertical (mother to child). The routes of horizontal transmission are blood and blood derivatives, infected blood transfusion products, needle stick or blood splatter from a person infected with hepatitis B virus or an undiagnosed person, open injuries and scratches, bloody surgery, intravenous drug use, tattoos and piercings, hemodialysis, and sharing of razors and toothbrushes.10 Using sharp materials11 and having a history of multiple heterosexual partners12 are risk factors for the transmission of HBV, as reported from prison setting studies in Northern Ethiopia. Furthermore, long stays in prisons, which provide a fertile ground for infection transmission, might increase the risk of transmission of pathogenic organisms, including blood-borne viral infections such as hepatitis B and hepatitis C viruses.13,14 Limited health facilities, lack of health services, and absence of sanitary facilities in the prison settings also predispose prisoners to new infections.15 The rates of hepatitis B and hepatitis C infections among prisoners in all countries are reported to be higher than in the general population.16
The epidemiology of hepatitis B can be described in terms of the prevalence of hepatitis B surface antigen (HBsAg) in a population, broadly classified into high (>8% HBsAg prevalence), intermediate (2–7%), and low prevalence (<2%). High-HBV prevalence is common in much of the Asia Pacific and sub-Saharan African regions.17 In our regional state, Tigrai, information about hepatitis B and hepatitis C viruses in prison settings has not been addressed, however; the rates of HBV among blood donors and pregnant mothers have been reported to be 3.79%18 and 5.5%,19 respectively. The rate of HCV among blood donors was also reported as 1.3%18 from Tigrai . Hence, we found that assessing the prevalence of HBV and HCV in the prison settings is important to design further interventions for prevention and control of HBV and HCV in the Tigrai regional state of Ethiopia. Therefore, we aimed to describe the seroprevalence and associated factors among prisoners in Tigrai, Northern Ethiopia.
Methods
Study Area, Study Design, and Study Period
The study settings were the prison facilities of the Tigrai regional state, which is in the northern part of Ethiopia. We took a letter of support from Mekelle University College of Health Sciences to the office of Tigrai prison administration. Based on the letter of support, we gathered the required information and selected three prison settings; Wukro town from the Eastern zone, Mekelle city from Mekelle zone, and Michew town from the Southern zone of Tigrai using the lottery method. Mekelle, a city of Tigrai, is positioned 784 km north of Addis Ababa, the capital city of Ethiopia, and has a total of 1,800 prisoners, whereas Wukro is located 67 km northeast of Mekelle with a total of 600 prisoners. Michew, the third selected town, is the administrative town of the southern zone of Tigrai and is located 120 km to the south of Mekelle city with a total of 720 prisoners. A cross-sectional study was conducted from February 2020 to May 2020 in prison settings of Tigrai regional state of Ethiopia. Male and female individuals aged 18 and above who stayed for more than 6 months in these prison settings were included. We used a single population proportion to calculate a total of 315 study participants using a previous prevalence of 10.4%12 at a 5% margin of error and 95% level of confidence.
Sample Collection and Laboratory Analysis
Face-to-face interviews were performed to collect demographic characteristics and risk factors from study participants prospectively. These are age, sex, marital status, educational level, income status, tattooing, number of sexual partners, sharing contaminated materials, blood transfusion history, dental extraction, alcohol consumption, number of prisoners per room, and duration of imprisonment. Five milliliters of blood was aseptically obtained from each study participant using a plain tube. Plasma was separated by centrifuging blood at 1,000 revolutions per minute (rpm) for 1 minute, labeled with a participant code number, and a cold box was used to transport to Tigrai Blood Bank and −20°C was used to store the specimens upon delay. Detection of hepatitis C and hepatitis B viruses were performed using Anti-HCV antibody (Volkan Kozmetik Sanayi Ve Ticaret ltd. STI, Turkey) and Hepatitis B surface Ag (Zhejiang orient Gene Biotech Co., Ltd., China) based on standard operational procedures (SOPs), respectively. All rapid test positive results were confirmed using ELISA technique (Beijing Wantai Biological Pharmacy Enterprise Co. Ltd).
Data Management
Data was entered and analyzed using Statistical Package for Social Sciences (SPSS) version 20. Descriptive statistics, crude and adjusted odds ratio were conducted by univarate and multivariate regression model. P<0.05 was considered statistically significant.
Quality Control
Positive and negative controls (HBsAg and Anti HCV) were performed in parallel to the test of interest as quality control.
Ethical Considerations
Ethical clearance was obtained from the Ethical Review Committee (ERC) of the College of Health Science, Mekelle University and the ERC number is 1499/2020. Based on the letter of support that we took from Mekelle University, the Tigrai prison administration office allowed us to proceed to the selected prison settings and we collected written informed consent from each study participant before data and blood sample collection. The confidentiality of patients’ information was safeguarded throughout the process.
Results
Demographic Characteristics of Participants
A total of 315 prisoners participated and more than 90% of them were males. The age of participants ranged between 18 and 72 years, with a mean of age of 30 (±10.5) and the majority (38%) of the prisoners were 18–25 years old. The income of more than 40% of the prisoners was low (<500 Ethiopian birr/month) and about 85% of the prisoners did not know what HBV and HCV were. About 39% of the prisoners who participated in the study had been in prison for more than 3 years (Table 1).
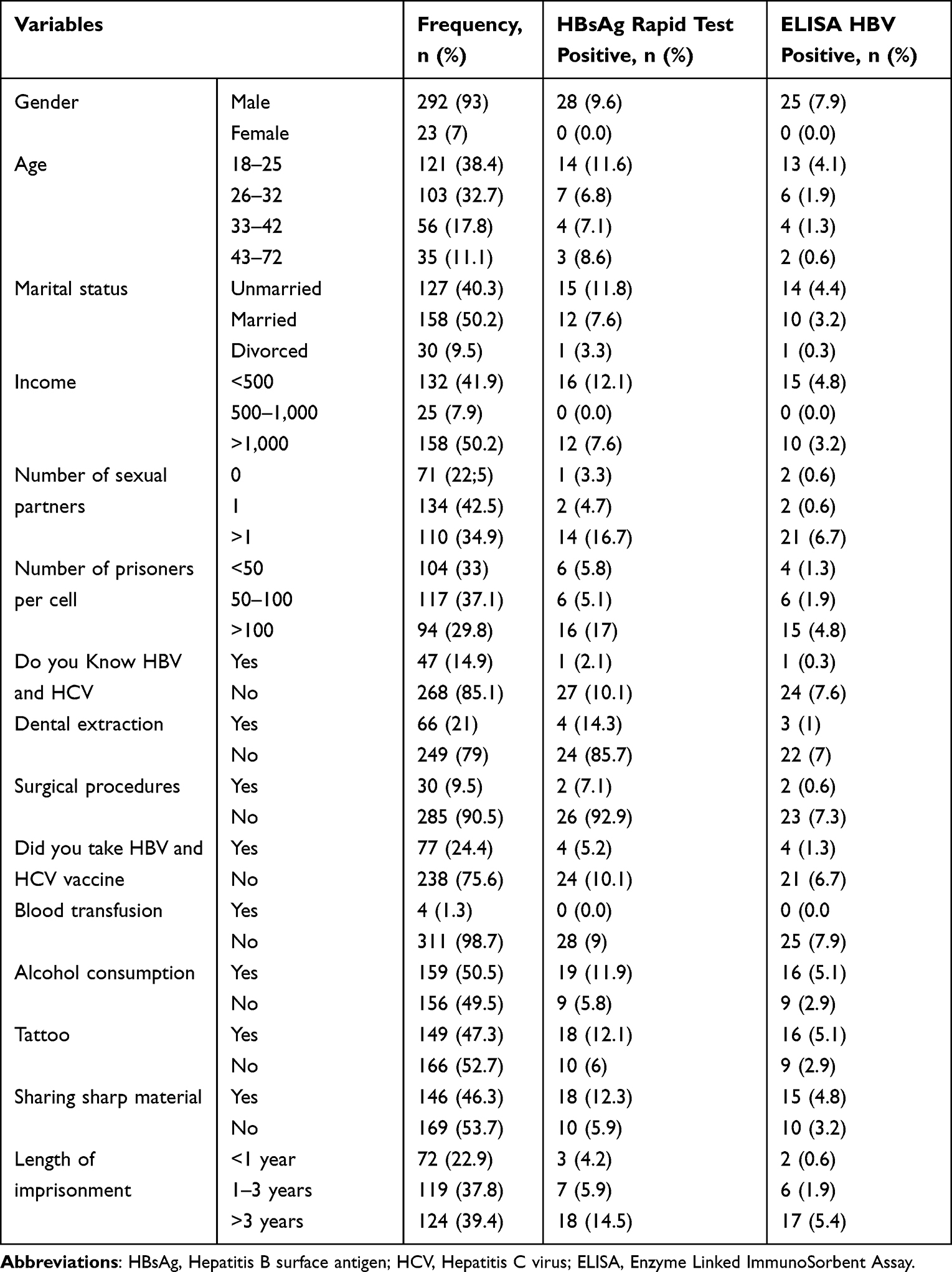 |
Table 1 Seroprevalence of HBV and HCV in Prison Settings of Tigrai, Northern Ethiopia (n=315) |
Sero-Prevalence of HBV and HCV
The overall seroprevalences of HBV and HCV were 25 (7.9%) and 1 (0.3%), respectively. Mixed infections were not identified in our study. All of the HBV and HCV were recovered from male participants. The lowest prevalence of HBV was observed in 43–72 year olds (2; 0.6%), while the highest was in the 18–25 year olds (13; 4.1%). The prevalence of HBV among unmarried was 14 (4.4%) and those with a low income (<500 Ethiopian birr/month) was 14 (4.1%) and 15 (4.8%), respectively.
The positivity rates of HBV among prisoners who had lived with 100 individuals in a single room, stayed longer than 3 years of imprisonment, had more than one sexual partner, and had an exchange of sharp materials with another person were 15 (4.8%), 17 (5.4%). 13 (4.1%), and 15 (4.8%), respectively (Table 1).
Associated Factors of HBV
This study assessed variables such as knowledge about HBV, number of prisoners per cell, length of stay in prison, alcohol consumption, tattoos, and sharing of sharp materials whether variables have associations with HBV infection or not. Only previous alcohol consumption (AOR=3.4, 95% CI=1.17–7.74) and number of prisoners per cell (AOR=5.6, 95% CI=1.14–13.6) showed an association with HBV infection (Table 2).
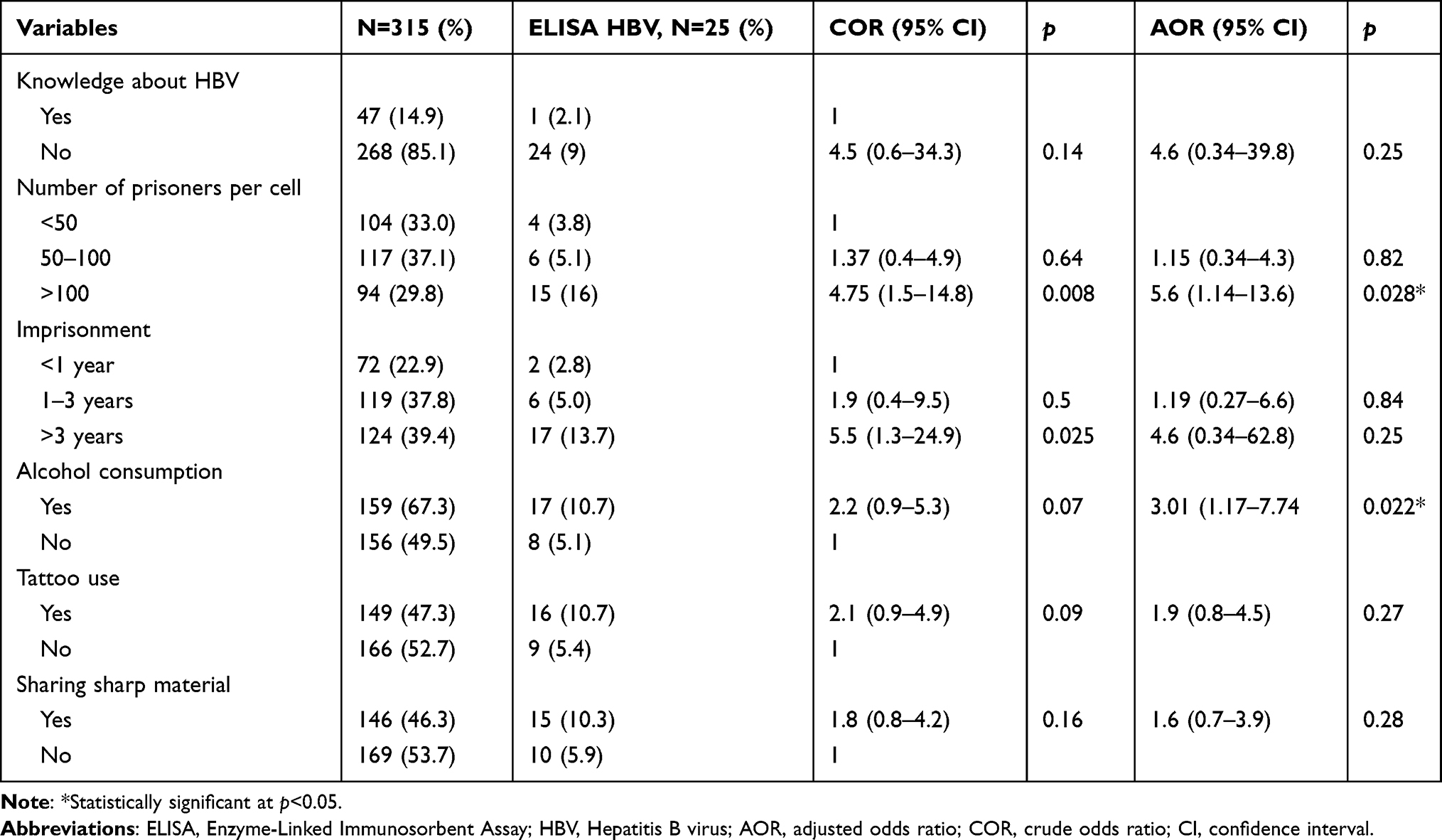 |
Table 2 Factors Associated with the Hepatitis B Viral Infection in Prison Settings of Tigrai, Northern Ethiopia (n=315) |
Discussion
The sub-Saharan Africa region is categorized as high HBV prevalence, in which the rate of HBV is greater than 8%.17 Horizontal transmission is one of the two important transmission routes of HBV and the prison setting is one example where hepatitis viruses transmission can take place.10 The prevalence of HBV and HCV in prisoners of all countries is significantly higher than those in the general population16 and prisoners contribute to the increased transmission and spread of HBV and HCV infections to the general population.20 In the study area, there was no data about the prevalence of HBV and HCV. Thus, we aimed to describe the seroprevalence of HBV, HCV, and associated factors among prisoners in Tigrai, Ethiopia.
The overall prevalence of HBV infection in the study area was 25 (7.9%). This was in line with reports from prison settings of the north east (6.5%)21 and community setting (7.2%)22 of Ethiopia, Afghanistan (6.5%),23 and Libya (6.9%).24 However, it was lower than reports from other studies in Ethiopia (10.4%)11 and abroad in Ghana (17.4%),25 Malawi (17.5%),26 Egypt (9.8%),27 and Croatia (11.3%).28 The reason why their results were high might be associated with injectable drug use (IDU) and homosexual practices,25,28 even if there was a report from Ethiopia that no homosexuality was identified from the interviewed participants.12 Our result of HBV in this study was higher than the results of studies conducted in other countries including Stockholm (1.9%),29 Switzerland (5.9%),30 Turkey (4.7%),31 Lebanon (2.4%),32 Iran (2.5%),33 Kyrgyzstan (6.2%),34 and Nigeria (5.9%).35 The reasons might be due to differences in study design, health system facilities in prisons, and prisoners’ level of awareness on HBV.31,32
The prevalence of HBV among blood donors, pregnant women, and HIV-positive individuals in Ethiopia were (3.8%,36 3.79%18), (3.7%,37 5.5%19) and (5.9%),38 respectively, which was lower than our result. The factors that were practiced in the prison settings of the study area like sharing of sharp materials might aggravate the transmission of HBV. However, a higher rate of HBV seroprevalence (10.9%) had been reported among street dwellers from Gondar-Ethiopia.39 The difference shows that street dwellers, like prison inmates, are among the high-risk populations for bloodborne infections, including HBV infections.40
The rate of HCV was only 1 (0.32%), which was much lower than previous reports in Ethiopia (2.6%,12 1.9%,22 1.3%18), Ghana (19.2%),25 Egypt (15.8%),27 Iran (9.5%),33 and Nigeria (13.7%)35 but almost similar with a study done in Turkey (0.5%).31
The age group of 18–25 years was identified by World Health Organizations and the United Nations as key vulnerable subgroup prisoner populations for HIV and viral hepatitis.41–43 Risk behaviors of HBV and HCV were observed more prevalently among young and male prisoners.44,45 This might be realized by sexually active groups and illegalization of substance use globally.46
In our study, 10.7% of study participants who had tattoos were positive for HBV infection. This was supported by previous studies conducted in Brazil (14%)47 and Ghana (12%),25 while 10.3% of HBV-positive individuals had shared risk materials.11,12 Prisoners who stayed longer than 3 years in prison were 3-times more likely to be infected by HBV infection than those who reported a period of imprisonment less than 1-year, but not statistically significant, which is supported by a previous study conducted in Egypt.27
A multivariate analyses result showed that individuals living in prison rooms consisting of more than 100 prisoners were 4-times (AOR=3.95, 95% CI=1.14–13.6, p=0.028) more infected with HBV than as compared with their counterparts living in prison rooms with less than 50 individuals. The cells might to be overcrowded and individuals in these cells might be in cloth contact with each other. Prisoners who had an alcohol consumption history were 3-fold (AOR=3.1 95% CI=1.17–7.74, p=0.022) more infected with HBV as compared with those without an alcohol consumption history. This was comparable with a previous study conducted in Nigeria.27,35
The association between HCV infection and different factors were not done because of the low (1; 0.31%) prevalence rate. However, HCV infection in association with tobacco, alcohol consumption, period of imprisonment, and intravenous drug use were reported in the previous studies.30,48
Conclusions
The prevalence of HBV among prisoners in the selected prisons of Tigrai was nearly high or borderline with a very low prevalence of HCV. The most HBV positive prisoners were the young adults, large number of prisoners per cell, and those who had a previous history of alcohol consumption. The overall outcome of the present study recommends that there should be prison-focused intervention activities such as conducting regular health education, more enhanced prevention, and control activities with more emphasis on the mode of transmission. There should be an HBV screening policy introduced, especially when prisoners enter the prison facility.
Abbreviations
Anti-HCV, Anti-Hepatitis C Virus; ELISA, Enzyme-Linked Immunosorbent Assay; HBsAg, Hepatitis B Surface Antigen; HBV, Hepatitis B Virus; HCV, Hepatitis C Virus; HIV, Human Immunodeficiency Virus; SPSS, Statistical Package for Social Sciences; WHO, World Health Organizations; UN, United Nations.
Acknowledgment
We would like to thank the study participants for their collaboration to participate in the study. We would also like to thank the Department of Medical Microbiology and Immunology, College of Health Sciences, Mekelle University for their support and Mekelle University NORAD project for providing the funds to finalize this study. Our sincere thanks also go to the administration offices and staff of the respective prisons.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Hutin YJF, Bulterys M, Hirnschall GO. How far are we from viral hepatitis elimination service coverage targets? J Intel AIDS Soc. 2018;21:25050.
2. Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ. Estimations of the worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet. 2015;386(10003):1546–1555. doi:10.1016/S0140-6736(15)61412-X
3. World Health Organization. Department of communicable diseases surveillance and response. Hepatitis B, 2002. Available from: http://www.who.int/csr/disease/hepatitis.
4. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
5. Robaeys G, Arain A, Stover H. Hepatitis C viral infection in prisons. In: Emerging Issues in Prison Health. Dordrecht: Springer; 2017:169–181.
6. Baillargeon J, Wu H, Kelley MJ, Grady J, Linthicum L, Dunn K. Hepatitis C seroprevalence among newly incarcerated inmates in the Texas correctional system. Public Health. 2003;117(1):43–48. doi:10.1016/S0033-3506(02)00009-4
7. Wilcox RD. Hepatocellular carcinoma and HIV: is there an association? HIV Clin. 2009;21(4):11–12.
8. Kassaian N, Adibi P, Kafashaian A, et al. Hepatitis C virus and associated risk factors among prison inmates with a history of drug injection in Isfahan, Iran. Int J Prev Med. 2012;3(l1):156.
9. World Health Organization. Hepatitis: Improving the Health of Patients with Viral Hepatitis. One Hundred Thirty-Fourth Session of the Executive Board. Geneva: World Health Organization; 2014:20–24.
10. Drazilova S, Kristian P, Janick M, et al. What is the role of the horizontal transmission of hepatitis B virus infection in young adult and middle-aged Roma population living in the settlements in East Slovakia? Int J Environ Res Public Health. 2020;17:3293. doi:10.3390/ijerph17093293
11. Berhe H, Yismaw G, Addis Z, Haileslassie H, Anagaw B, Unakal C. Seroprevalence and associated risk factors of human immunodeficiency virus and hepatitis B virus infections among prison inmates. J Pharm Biomed Sci. 2013;30(23):1035–1045.
12. Kebede W, Abdissa A, Seid Y, Mekonnen Z. Seroprevalence and risk factors of hepatitis B, hepatitis C, and HIV infections among prisoners in Jimma Town, Southwest Ethiopia. Asian Pac J Trop Dis. 2017;7(5):270–275. doi:10.12980/apjtd.7.2017D6-422
13. Joseph AB. Infection control in jails and prisons. Clin Infect Dis. 2007;45(8):1047–1055. doi:10.1086/521910
14. Massoglia M. Incarceration as exposure: the prison, infectious disease, and other stress- related illnesses. J Health Soc Behav. 2008;49:56–71. doi:10.1177/002214650804900105
15. Busi S, Oltaye Z. Assessment of the magnitude of sexually transmitted infections, and sexual reproductive health status among prisoners aged between 18–49 years in tabor prison, Hawassa, Ethiopia. Momona Ethiop J Sci. 2016;8(1):89–97. doi:10.4314/mejs.v8i1.8
16. European Monitoring center for Drug and Drug Addiction. HIV in prison: situation and needs assessment tool kit. Vienna, United Nations Office on Drug and Crime; 2010. Available from: http://www.unodc.org/documents/hivaids/publication/HIVinprisonsituationandneedassessmentdocument.pdf.
17. MacLauchlan JH, Cowie BC. Hepatitis B virus epidemiology. Cold Spring Harb Perspect Med. 2015;5:a02141.
18. Degefa B, Gebreeyesus T, Gebremedhin Z. Prevalence of hepatitis B virus, hepatitis C virus, and human immunodeficiency virus among blood donors of Mekelle blood bank, Northern Ethiopia: a three‐year retrospective study. J Med Virol. 2018;90:
19. Mezgebo TA, Niguse S, Kahsay AG, et al. Hepatitis B virus infection and associated risk factors among pregnant women attending antenatal care in health facilities of Tigray, Northern Ethiopia. J Med Virol. 2017;89:1–7. doi:10.1002/jmv.24696
20. Salari N, Darvishi N, Hemmati M, et al. Global prevalence of hepatitis C in prisoners: a comprehensive systematic review and meta-analysis. Arch Virol. 2022;167:1025–1039. doi:10.1007/s00705-022-05382-1
21. Kassa Y, Million Y, Biset S, Moges F. Hepatitis B and hepatitis C viral infections and associated factors among prisoners in Northeastern Ethiopia. J Blood Med. 2021;12:561–570. doi:10.2147/JBM.S314556
22. Woldegiorgis AE, Erku W, Medhin G, Berhe N, Legesse M. Community-based sero-prevalence of hepatitis B and C infections in South Omo Zone, Southern Ethiopia. PLoS One. 2019;14(12):e0226890. doi:10.1371/journal.pone.022689
23. Todd CS, Abed AM, Strathdee SA, et al. HIV, hepatitis C, and hepatitis B infections and associated risk behavior in injection drug users, Kabul, Afghanistan. Emerg Infect Dis. 2007;13(9):1327. doi:10.3201/eid1309.070036
24. Ziglam H, Zorgani AA, Balouz A, Abudher AH, Elahmer O. Prevalence of antibodies to human immunodeficiency virus, hepatitis B, and hepatitis C in prisoners in Libya. Libyan J Med. 2012;7. doi:10.3402/ljm.v7i0.19713
25. Adjei AA, Armah HB, Gbagbo F, et al. Prevalence of human immunodeficiency virus, hepatitis B virus, hepatitis C virus, and syphilis among prison inmates and officers at Nsawam and Accra, Ghana. J Med Microbiol. 2006;55(5):593–597. doi:10.1099/jmm.0.46414-0
26. Nyirenda M, Beadsworth MB, Stephany P, et al. Prevalence of infection with hepatitis B and C viruses and co-infection with HIV in medical inpatients in Malawi. J Infect. 2008;57(1):72–77. doi:10.1016/j.jinf.2008.05.004
27. Mohamed HI, Saad ZM, Abd-Elreheem EM, et al. Hepatitis C, hepatitis B, and HIV infection among Egyptian prisoners: seroprevalence, risk factors, and related chronic liver diseases. J Infect Public Health. 2013;6(3):186–195. doi:10.1016/j.jiph.2012.12.003
28. Burek V, Horvat J, Butorac K, Mikulić R. Viral hepatitis B, C, and HIV infection in Croatian prisons. Epidemol Infect. 2010;138(11):1610–1620. doi:10.1017/S0950268810000476
29. Gahrton C, Westman G, Lindahl K, et al. Prevalence of Viremic hepatitis C, hepatitis B, HIV infection and vaccination status among prisoners in Stockholm County. BMC Infect Dis. 2019;19(1):955. doi:10.1186/s12879-019-4581-3
30. Getaz L, Casillas A, Siegrist CA, et al. Hepatitis B prevalence, risk factors, infection awareness, and disease knowledge among inmates: a cross-sectional study in Switzerland’s largest pre-trial prison. J Global Health. 2018;8(2):020407. doi:10.7189/jogh.08.020407
31. Kose S, Adar P, Gozaydin A, Kuzucu L, Akkoclu G. Hepatitis B, and Hepatitis C in prisons: a prevalence study. Int J Prison Health. 2019. doi:10.1108/IJPH-01-2018-0004
32. Mahfoud Z, Kassak K, Kreidieh K, Shamra S, Ramia S. Prevalence of antibodies to human immunodeficiency virus (HIV), hepatitis B and hepatitis C and risk factors in prisoners in Lebanon. J Infect Dev Ctries. 2010;4(03):144–149. doi:10.3855/jidc.517
33. Moradi G, Gouya MM, Azimizan Zavareh F, et al. Prevalence and risk factors for HBV and HCV in prisoners in Iran: a national bio-behavioral surveillance survey in 2015. Trop Med Int Health. 2018;23(6):641–649. doi:10.1111/tmi.13065
34. Azbel L, Polonsky M, Wegman M, et al. Intersecting epidemics of HIV, HCV, and syphilis among soon-to-be-released prisoners in Kyrgyzstan: implications for prevention and treatment Int. J Drug Policy. 2016;37:9–20. doi:10.1016/j.drugpo.2016.06.007
35. Dan-Nwafor C, Adeoye I, Aderemi K, et al. Knowledge, serological markers and risk factors associated with hepatitis B and C Virus infection among kuje prison inmates, federal capital territory, Nigeria. Int J Infect Dis. 2018;73:374. doi:10.1016/j.ijid.2018.04.4260
36. Tessema B, Yismaw G, Kassu A, et al. Seroprevalence of HIV, HBV, HCV and syphilis infections among blood donors at Gondar University Teaching Hospital, Northwest Ethiopia: declining trends over five years. BMC Infect Dis. 2010;10:111. doi:10.1186/1471-2334-10-111
37. Awole M, Gebre-Selassie S. Seroprevalence of HBsAg and its risk factors among pregnant women in Jimma, Southwest Ethiopia. Ethiop J Health Dev. 2005;19(1):45–50. doi:10.4314/ejhd.v19i1.9970
38. Weldemhret L, Asmelash T, Belodu R, Gebreegziabiher D. Seroprevalence of HBV and associated risk factors among HIV positive individuals attending ART clinic at Mekelle hospital, Tigray, Ethiopia. AIDS Res Ther BioMed Centr. 2016;13:6. doi:10.1186/s12981-016-0090-2
39. Moges F, Kebede Y, Kassu A, et al. Seroprevalence of HIV, hepatitis B infections and syphilis among street dwellers in Gondar city, Northwest Ethiopia. Ethiop J Health Dev. 2006;20:160–165.
40. Roy E, Haley N, Lemire N, Boivin JF, Leclerc P, Vincelette J. Hepatitis B virus infection among street youths in Montreal. Can Med Assoc J. 1999;161:689.
41. Van Dooren K, Kinner SA, Forsyth S. Risk of death for young ex‐prisoners in the year following release from adult prison. Aust N Z J. 2013;4:377–382.
42. World Health Organization. WHO Consolidated Guidelines on HIV Prevention, Diagnosis, Treatment, and Care for Key Populations. Geneva: World Health Organization; 2014.
43. McCall-Smith K. United Nations’ standard minimum rules for the treatment of prisoners (Nelson Mandela rules). Int Leg Mat. 2016;55(6):1546–1555. doi:10.1017/S0020782900030898
44. Kinner SA, Jenkinson R, Gouillou M, Milloy MJ. High-risk drug-use practices among a large sample of Australian prisoners. Int J Drug Pol. 2012;126(1–2):156–160.
45. Australian Institute of Health and Welfare. AIHW Canberra. The Health of Australia’s Prisoners. National Criminal Justice Reference Service NCJRS; 2015.
46. Csete J, Kamarulzaman A, Kazatchkine M, et al. Public health and international drug policy. Lancet. 2016;387(10026):1427–1480. doi:10.1016/S0140-6736(16)00619-X
47. La Torre G, Miele L, Chiaradia G, et al. Socio-demographic determinants of coinfections by HIV, hepatitis B and hepatitis C viruses in central Italian prisoners. BMC Infect Dis. 2007;7(1):100. doi:10.1186/1471-2334-7-100
48. World Health Organization. Good Governance for Prison Health in the 21st Century: A Policy Brief on the Organization of Prison Health. WHO Regional Office for the fund the Europe; IRIS (Institutional Repository for Information Sharing); 2013.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.