")
Back to Journals » Infection and Drug Resistance » Volume 16
Serological Evidence and Associated Factors of Hepatitis B Virus and Hepatitis C Virus Among Waste Handlers: A Cross-Sectional Study from Northeastern Ethiopia
Authors Ayele B, Weldehanna D , Demsiss W
Received 9 April 2023
Accepted for publication 15 July 2023
Published 26 July 2023 Volume 2023:16 Pages 4881—4890
DOI https://doi.org/10.2147/IDR.S416409
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Beju Ayele,1 Daniel Weldehanna,2 Wondmagegn Demsiss2
1Amhara Public Health Institute, Dessie Branch, Dessie, Ethiopia; 2Department of Medical Laboratory Sciences, College of Medicine and Health Sciences, Wollo University, Dessie, Amhara Region, 1145, Ethiopia
Correspondence: Daniel Weldehanna, Email [email protected]
Background: The World Health Organization (WHO) has identified viral hepatitis, caused by hepatitis B virus (HBV) and hepatitis C virus (HCV), as one of the main global public health issues. People who work in the collection of waste materials, from either household or medical environments, are at greatest risk.
Objective: To determine the prevalence of and factors associated with HBV and HCV among medical and domestic waste handlers in Northeast Ethiopia.
Methods: A comparative cross-sectional study was conducted from January to April 2021 at selected healthcare facilities and municipal settings in Dessie town, Northeast Ethiopia. The sample size was determined using a double population proportion formula, and a simple random sampling technique was employed to select 70 individuals in the medical waste handlers (MWHs) group and 206 in the domestic waste handlers (DWHs) group. Five milliliters of venous blood was collected from each participant and tested for HBV and HCV using an enzyme-linked immunosorbent assay. Data were analyzed using SPSS version 23; the prevalence was computed, Fisher’s exact test was used, and logistic regression was applied.
Results: A total of 276 study participants were enrolled and the overall seroprevalence of hepatitis virus was 5.1%. The seroprevalence of HBV infection among MWHs and DWHs was 8.6% and 1.9%, respectively. The overall seroprevalence of HCV infections among MWHs and DWHs was 4.3% and 0.5%, respectively. Medical waste handling, having a history of needle stick injury, and not using personal protective equipment were factors significantly associated with HBV infection.
Conclusion: The overall seroprevalence of viral hepatitis was high. The prevalence of HBV infection among MWHs was in line with the high endemicity classification of the WHO, and there was a significant difference in prevalence between DWHs and MWHs. Both groups of waste handlers should receive proper attention to protect them from HBV and HCV infection.
Keywords: waste handlers, HBV, HCV, Northeast Ethiopia
Introduction
The World Health Organization (WHO) has identified viral hepatitis, caused by hepatitis B virus (HBV) and hepatitis C virus (HCV), as one of the main global public health issues.1 The WHO announced a strategy in 2016 to end viral hepatitis as an imminent danger to public health by 2030.2 It is estimated that 354 million people are living with chronic HBV (296 million) and HCV (58 million). Viral hepatitis caused more than 1.1 million deaths in 2019, mostly due to complications of cirrhosis and hepatocellular cancer.3 Between the years 1990 and 2013, the global death rate due to viral hepatitis increased from 0.89 to 1.45 million.4 Even though the global seroprevalence of HBV and HCV decreased from 2015 to 2020, the target of elimination by 2030 may not be practical and it may prove difficult to achieve this goal.5,6 In resource-limited areas of the world in particular, the target of eliminating the two viral infections is hampered by many problems, such as diagnostic capability, population awareness, and the COVID-19 pandemic.7,8
Workers engaged primarily in the collection and transportation of waste materials face biological, chemical, and physical risks to their health when in contact with waste, and this scenario is more severe in low- and middle-income countries.9,10 People who work in the collection of waste materials from either household or medical environments are at greatest risk of developing infection owing to the presence of infectious agents such as HBV and HCV.11 The rate of HBV infection among medical waste handlers is significantly higher than that among non-medical waste handlers; this situation is even worse in developing countries.12,13 In some situations, healthcare and domestic waste exposures have been linked to comparable risks of HBV infection.14 Healthcare providers and those who manage medical waste are at risk of contracting HBV in Ethiopia, possibly as a result of prior contact with infected patients.15 Public health facilities in Ethiopia produce a sizable amount of biomedical waste, and if this is not managed appropriately, there may be a higher likelihood of such waste being a potential source of an infectious agent.16
In two successive systematic reviews conducted in Ethiopia, the pooled prevalence of HCV was 3.1%17 and 2%,18 indicating that the disease may be on the decline. However, according to systematic review and meta-analysis reports from Ethiopia, the overall prevalence of HBV remains a significant health problem in various population categories.17,19 The seroprevalence of HBV among medical and non-medical waste handlers was 6% and 1%, respectively, in another study from Ethiopia.13 According to a study carried out in Addis Ababa, Ethiopia, medical waste handlers have a significantly increased chance of contracting HBV.20 Related research conducted in public health facilities in eastern Ethiopia, where 20% of the study participants had HBV infection, provided support for this conclusion.21
Several studies have been conducted regarding the seroprevalence of HBV and HCV infection among various study groups in Ethiopia.22–24 Few studies on the prevalence of the two most common viral hepatitis types among waste handlers have been conducted in defined areas. Studies investigating the prevalence of HBV and HCV among waste handlers in health facilities and in municipal settings are rare, particularly in the northeastern part of Ethiopia. Hence, the current study was conducted to fill this gap in the literature on the prevalence of and factors associated with HBV and HCV among medical and domestic waste handlers in Northeast Ethiopia.
Methodology
Study Settings and Population
A comparative cross-sectional study was conducted from January to April 2021 at selected health facilities and municipal settings in Dessie town, Northeast Ethiopia (Figure 1). Dessie is found at a latitude of 11°8′ N and a longitude of 39°38′ E, at an altitude of 2470–2550 m above sea level. It is located 401 km northeast of Addis Ababa and 478 km from Bahir-Dar. The town administration has five sub-cities, with eight health centers, one comprehensive specialized hospital and one general hospital under government control, and five general hospitals (private), 32 higher private clinics, one family guidance association center, and one Marie Stopes International reproductive health service clinic. According to the 2015 Amhara Regional State Statistics Bureau report, Dessie city administration has total an estimated population of 2,908,529, of whom 1,480,369 are male and 1,428,160 are female. In the town, there are a total of 350 domestic waste handlers (DWHs) and in the healthcare facilities there are also 116 medical waste handlers (MWHs). All DWHs and MWHs who volunteered to participate and gave their informed written consent were included in the study, while waste handlers who had lived in the town for less than 6 months, non-volunteers, and those who were unable to give consent owing to physical and/or mental illness were excluded from the study.
 |
Figure 1 Maps showing the study area (Dessie City). The maps were generated by the authors using ArcGIS version 10.8 software. |
Sample Size Determination and Sampling Technique
The sample size was determined using a double population proportion formula in Epi Info version 7.1, considering a 95% confidence interval, 80% power, unexposed to exposed ratio of 3, 1% of HBV in DWHs, and 6.3% of HBV in MWHs.20 As a result, the sample size was 133 MWHs and 397 DWHs. The sample size was higher than the existing total population in each group. Thus, a sample size reduction formula was used to find the minimum sample size, including a 10% non-response rate, and the final sample size was 70 MWHs and 206 DWHs, with a total sample size of 276. A simple random sampling technique was used to select the study subjects. The registered institutional identification numbers of study participants were used as a sampling frame. Then, proportional allocation was used to determine the number of study participants in the nine health institutions and the five sub-cities based on their source population.
Data Collection and Laboratory Procedures
A pretested structured questionnaire was used to collect socio-demographic, behavioral, and risky behavior characteristics. The questionnaire was administered by trained data collectors under strict supervision. After obtaining informed consent, a laboratory technologist collected 5 mL of venous blood in a labeled plain tube from each study participant. The blood sample was allowed to clot at room temperature and the serum was separated by centrifugation at 5000 rpm for 15 minutes. Serum samples were transported to the Ethiopian Red Cross Society Blood Bank, Dessie branch, in a cold box, and stored at −20°C until testing. Serum specimens were tested for HBV and HCV with the AiD™ HBsAg ELISA (Wantai Hepatitis B Virus Diagnostics, Beijing, China), with a sensitivity of 100% and specificity of 99.92%, and the AiD™ anti-HCV ELISA plus (Wantai Hepatitis C Virus Diagnostics, Beijing, China), with a sensitivity of 100% and specificity of 99.55%.
Quality Control
Quality-control checks were carried out before, during, and after data collection to generate high-quality and reliable data. The structured questionnaire was pretested on 5% of the study participants in Hayk town, which is located about 30 km away from Dessie town. Data collectors received two days’ training at each site before data collection started. Moreover, the quality of the laboratory test results was ensured using the internal quality control of the ELISA, as well as known negative and positive samples. All laboratory analyses were carried out using standard operating procedures.
Data Management and Analysis
Data were first coded and cleaned, and then entered and analyzed using SPSS version 23.0. The prevalence of HBV and HCV infections was computed. Fisher’s exact test was used to assess the differences in the proportion of hepatitis virus infections between the MWH and DWH groups. Bivariable logistic regression was computed and variables with a P-value <0.3 were entered into the multivariable logistic regression analysis; their adjusted odds ratios (AORs) were calculated and variables with a P-value <0.05 were taken as statistically significant.
Ethical Considerations
Ethical clearance was obtained from the Research and Ethics Review Committee of Wollo University, College of Medicine and Health Sciences. Then, permission was obtained from Dessie town health administration and municipality. Written informed consent was obtained from each study participant. Finally, participants who were positive for HBsAg and/or anti-HCV antibodies were referred for further management, investigation, and treatment. All aspects of this study were carried out in conformity with the ethical principles of the Declaration of Helsinki.
Results
Socio-Demographic Characteristics of Respondents
A total of 276 study participants were enrolled, with a response rate of 100%. The mean (±SD) age of the total participants was 38.53 (±9.21) years, while the mean (±SD) age of MWHs and DWHs was 37.63 (±9.17) and 38.83 (±9.23) years, respectively. About 42% of participants were above 40 years old, and around 90.9% (251/276) were female, of whom municipal participants accounted for 78.1% (196/251) (Table 1).
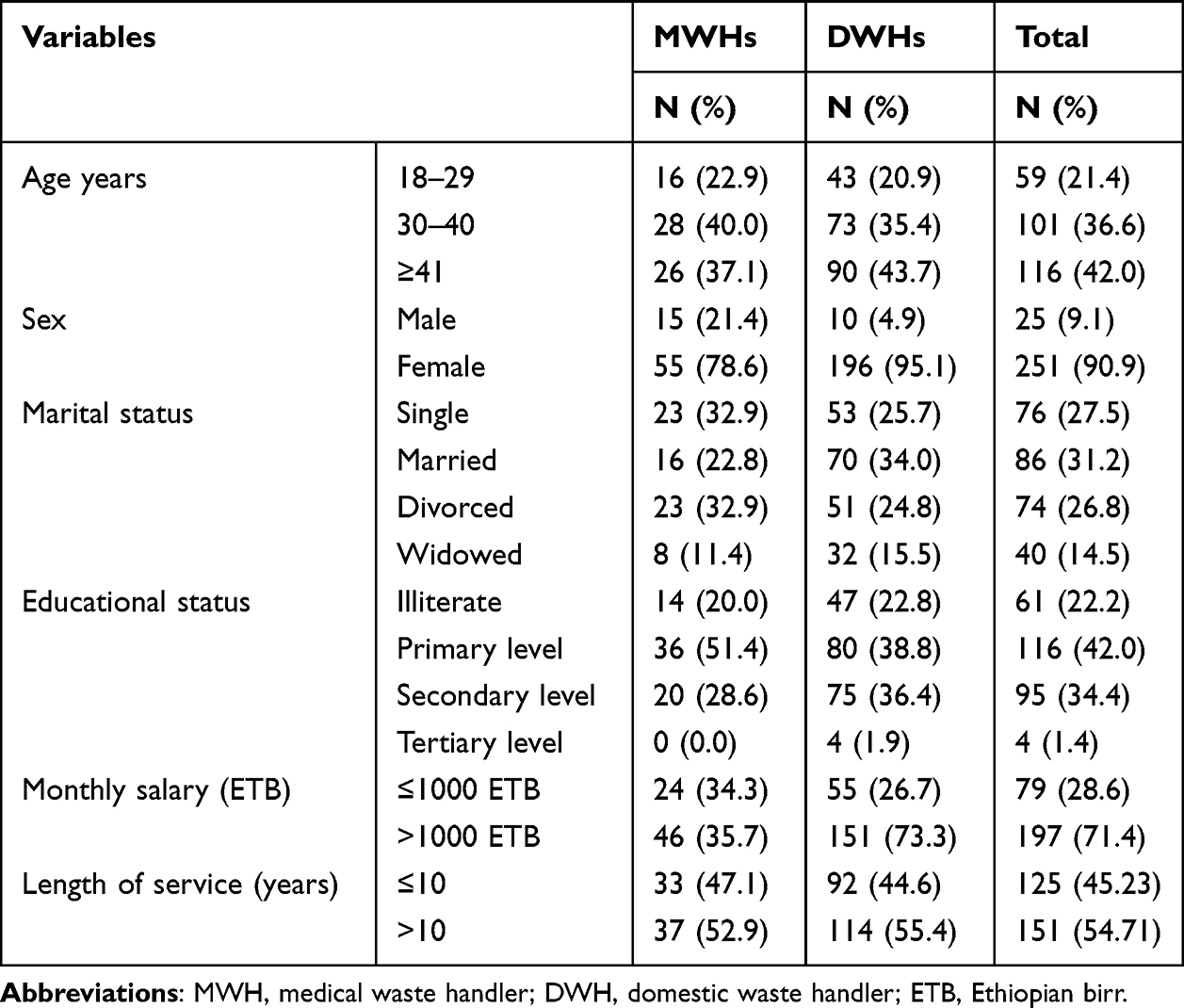 |
Table 1 Socio-Demographic Characteristics of Waste Handlers in Dessie Town, Northeast Ethiopia, 2021 |
Prevalence of HBV and HCV Infection
The overall seroprevalence of hepatitis virus in this study was 5.1% (14/276; 95% CI: 2.5–8.0). The seroprevalence of HBV infection among MWHs and DWHs was 8.6% (6/70; 95% CI: 4.1–16.0) and 1.9% (4/206; 95% CI: 0.5–4.4), respectively. The overall seroprevalence of HCV infections among MWHs and DWHs was 4.3% (3/70; 95% CI: 0.0–7.4) and 0.5 (1/206; 95% CI: 0.0–1.5), respectively. Statistically significant differences were noted in the rate of overall hepatitis virus infection (P=0.002) and HBV infection (P=0.019) between the MWH and DWH groups, as shown in Table 2.
 |
Table 2 Statistical Associations for HBV, HCV, and Overall Hepatitis Virus Infection Among Medical and Domestic Waste Handlers in Dessie Town, Northeast Ethiopia, 2021 |
A higher prevalence of HBsAg was observed among MWHs and DWHs who did not use personal protective equipment (PPE) [4/18 (22.5%) and 3/56 (5.4%), respectively] than in those who did use PPE. The differences in seroprevalence of HBV among DWHs who had a history of positive blood contact, compared to those who did not, and in males, compared to females, were significant (P<0.05). Similarly, the prevalence of HCV in males in the DWH group was 10% (1/10; P=0.0049), and this was the only variable found to be associated with anti-HCV. Thus, there was no common predictive factor for both groups (MWHs and DWHs) (Table 3).
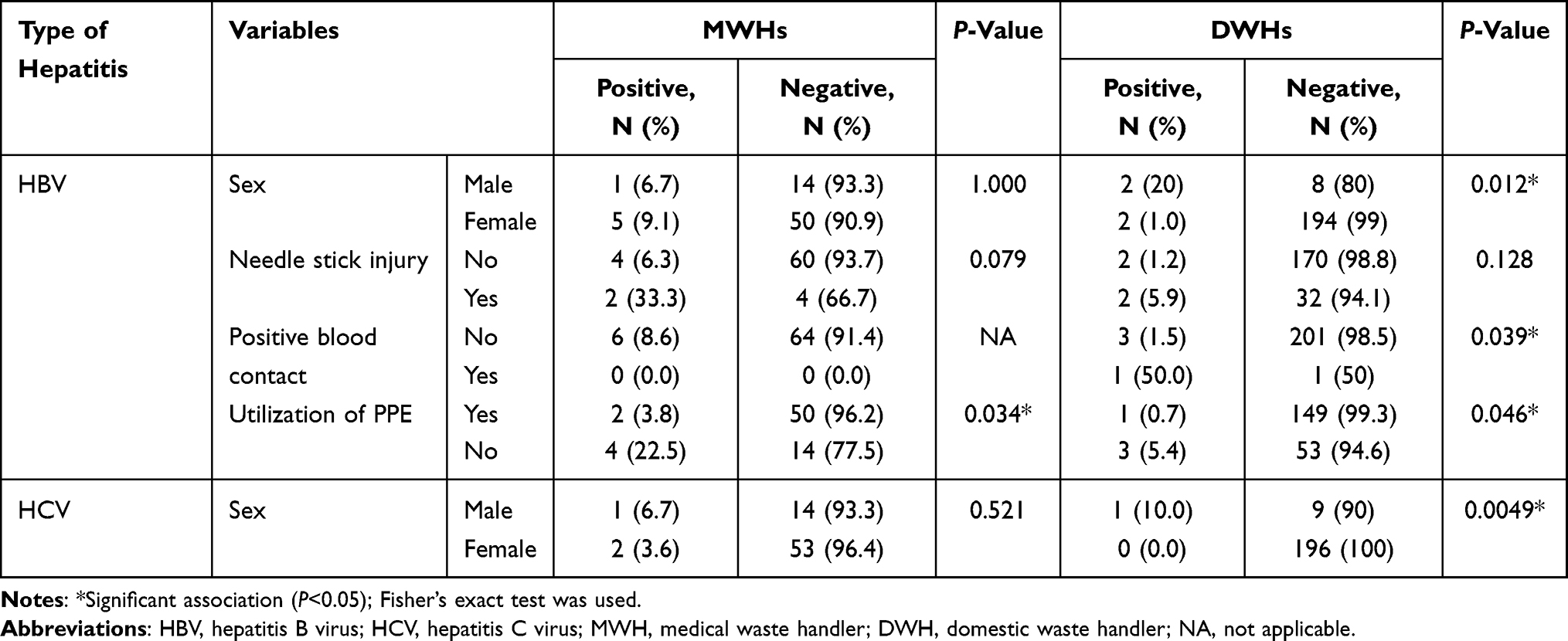 |
Table 3 Significant Distribution of HBV and HCV Infection Among MWHs and DWHs in Dessie Town, Northeast Ethiopia, 2021 |
Risk Factors Associated with HBV and HCV Infection
In multivariable analysis, working area, MWH (P=0.037), history of needle stick injury (P=0.003), and not using PPE (P=0.019) were factors significantly associated with HBV infection (Table 4).
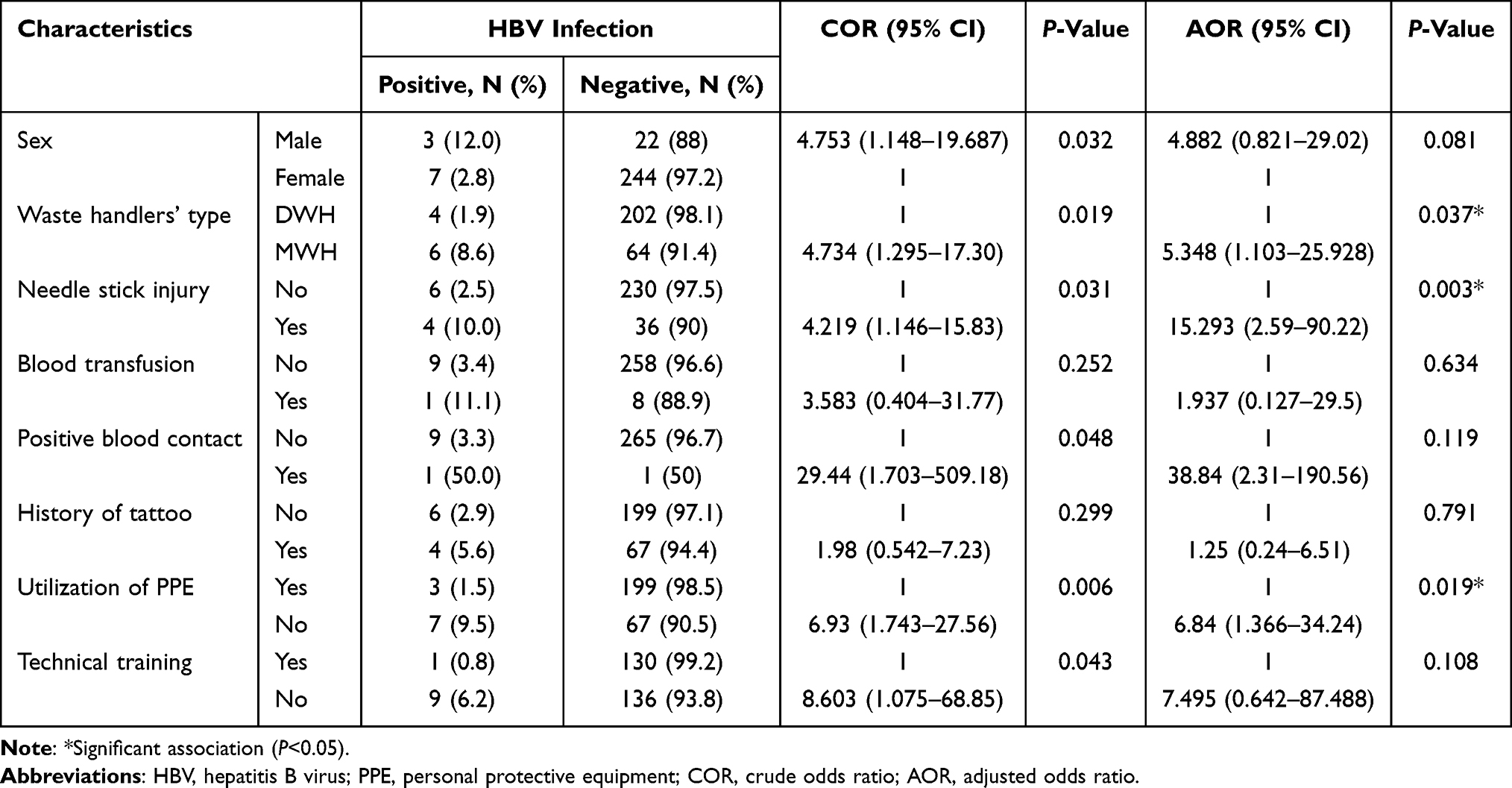 |
Table 4 Bivariable and Multivariable Logistic Regression of Factors of HBV Among Waste Handlers in Dessie Town, Northeast Ethiopia, 2021 |
The seroprevalence of HCV was significantly higher among waste handlers with a history of not using PPE (P=0.016) (Table 5).
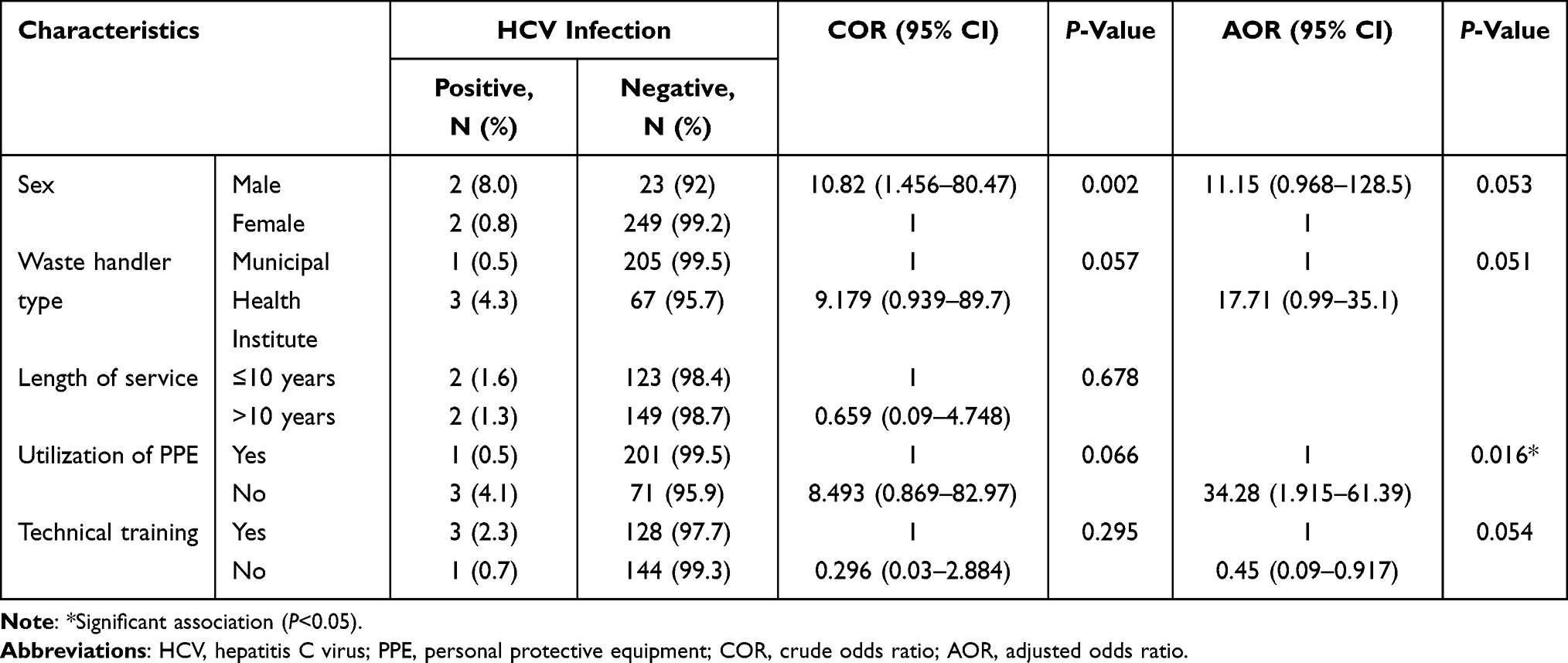 |
Table 5 Bivariable and Multivariable Logistic Regression of Factors of HCV Among Waste Handlers in Dessie Town, Northeast Ethiopia, 2021 |
Discussion
In many countries, healthcare waste management practice has not gained much attention from stakeholders in facilities25,26 and a huge amount of waste material is generated in different divisions of the healthcare services.16,26,27 Various factors are associated with biomedical waste management practice, such as educational level, training, access to bins in the working department, and attitude.28 Healthcare waste is illegally dumped along roads or in the bush in some cases, openly burned, and buried in yards. Vomit, urine, and sputum are disposed of in open areas near the homes as liquid healthcare waste.29,30 Sometimes, the household may not have sufficient sanitation facilities and the waste generated may not be disposed of in the environment in the proper manner.31 These scenarios may expose municipal and medical waste collectors to infectious diseases of various types.32 A meta-analysis that found a link between HBV infection and handling medical waste serves as proof of this hypothetical situation.12 Another review paper can be cited as evidence of the linking factor between HBV infection and exposure to either household or medical solid waste.33
The present study was carried out in a place where a high burden of HBV and HCV infection has been reported22,23,34 and a considerable number of needle stick and sharp material injuries has been demonstrated.35 In the present study, the overall seroprevalence of hepatitis virus among medical and domestic waste handlers was 5.1%. The seroprevalence of hepatitis infection (both HBV and HCV) was 12.85% among MWHs and 2.43% among DWHs. The overall prevalence of the two viral hepatitis types was lower among all study participants than in a previous study among pregnant women in Dessie town, but the infection prevalence among MWHs in the current study was consistent with the overall magnitude of viral hepatitis in different studies.23,36
HBV vaccine coverage in Africa is low, particularly among healthcare workers and waste handlers who have inadequate training and no HBV immunization history.20,37 MWHs and DWHs in this study had a frequency of HBV infection of 8.6% and 1.9%, respectively. Unlike the present study, the proportion of HBV among MWHs and DWHs was found to be comparable in a similar study, which was conducted in Tripoli, Libya.38 The seroprevalence of the virus in the current research demonstrates the high endemicity of HBV infection in our population, according to the WHO classification.39 While a lower rate of HBsAg (1.3%) was found in Southern Ethiopia,40 the seroprevalence of HBV among MWHs in Northwest Ethiopia revealed incomparable findings with the current research.15 In comparison to the current research, a study conducted in Belo Horizonte, Brazil, revealed that MWHs had a similar percentage of HBV infection but DWHs had a higher prevalence of the virus.14 This variation may be due to differences in laboratory methods, study period, demographic circumstances of the source population, and so on.
The HBV infection rate among MWHs in this study roughly corresponds to the combined prevalence of the virus in Africa’s general population and healthcare workers.41,42 It was higher than the results of a systematic research study conducted among the general public and clinical population in Germany, where a high vaccination rate was achieved.43 A study carried out in Jimma, Ethiopia, showed a significantly lower prevalence of HBV among healthcare workers compared to the present study.44 This may be due to the fact that the study participants in Jimma had a good level of knowledge and good attitudes about the standard precautionary measures. Another study, conducted in Nigeria, showed a concordant (2.6%) prevalence of HBV infection among municipal waste handlers.45 In contrast to the result of the present study, DWHs had a huge prevalence of HBV in a study conducted in Greece.46 The differences in the prevalence of HBV may be related to the laboratory method used, the study period, and variations in the population.
Moreover, the prevalence of HCV infection among MWHs in the present study was 4.3%, whereas its prevalence among DWHs was 0.5%. This result was found to be comparable with a study conducted in Brazil.14 A lower prevalence of HCV among MWHs and DWHs was reported in a study conducted in Gondor town, Ethiopia,13 and another similar study also reported a lower prevalence of HCV among MWHs.47 The rate of HCV among MWHs was found to be lower than a pooled prevalence of HCV among healthcare workers in Africa, but it was higher than the rate in East African healthcare workers and in Jimma town.41,44 In the present study, HBV and HCV coinfection was not detected in either the MWH or the DWH group. Most of the studies on similar topics also found no coinfection of HBV and HCV.13,21,40
In the present study, MWHs were shown to have 5.35 times higher likelihood of acquiring HBV infection compared to DWHs. Similar results were found in studies conducted in Gondar and Addis Ababa, Ethiopia, which indicated the strong association between HBV infection and medical waste handling work type.13,20 A meta-analysis on the association between HBV and medical waste handling demonstrated a strong statistical correlation between HBV infection and MWHs relative to DWHs. This study also showed that the association was particularly strong in African reports.12 This may be the result of accepted medical waste management practices being disregarded and a lack of planning for work-related safety precautions.48 Besides, various occupational risks and injuries that can occur in the medical setting can predispose MWHs to this problem.35
Waste workers are more susceptible to infectious agents as a result of sharp material injuries, inappropriate PPE use, and a lack of HBV vaccination.49 A history of needle stick injury had a substantial association (AOR=15.293; 95% CI=2.59–90.22; P=0.003) with HBV infection. In Greece, waste collectors who reported occupational injuries with needle sticks were found to be at a higher risk of HBV infection.46 In contrast, similar research indicated that needle stick injury did not demonstrate any statistical association with HBV infection.15 Owing to insufficient instruction on its use, technical issues, and the tolerability of PPE in the workplace, adhering to appropriate PPE use is challenging.50 Study participants who did not utilize PPE had nearly seven times greater odds of developing HBV and 34 times higher likelihood of acquiring HCV infection in comparison with those who used it properly.
In this study, nearly half of the study participants revealed they had received technical training about infectious waste management. Having or not having received technical training did not show any statistical association with HBV or HCV infections. This is consistent with the results of studies conducted in Gondar13 and Bahir Dar, Ethiopia,15 and in Kenya.51 A history of tattooing and blood transfusion demonstrated statistical associations in different research conducted in Ethiopia and elsewhere,21,40,45,52 whereas these variables did not show any association with the infection rates of HBV and HCV among our study participants or in other similar research.53
Limitations of the Study
In contrast to straightforward cross-sectional research, the comparative nature of the study was a crucial factor in enhancing its quality. To ensure the quality of the data, the study was also conducted under strict supervision and with regular follow-up. Despite these advantages, there are also some drawbacks to the study, such as the absence of quantitative real-time polymerase chain reaction (qRT-PCR). As a result, it was not possible to rule out occult HBV infection, which may have underestimated the prevalence of hepatitis virus infection in general and HBV infection specifically. The low percentage of MWHs may be another drawback of this research. Therefore, it is important to take these limitations into account when interpreting the results of this research.
Conclusion
The overall seroprevalence of viral hepatitis in the current study was high. The prevalence of HBV infection among MWHs is in line with the high endemicity classification of the WHO, and there was a significant difference in the prevalence of HBV between DWHs and MWHs. The burden of HCV in the present study was in agreement with other similar studies in various study populations including waste handlers. The results of the current study did not indicate coinfection with HBV and HCV. A number of variables, such as working area, history of needle stick injury, and not using PPE, showed statistically significant associations with HBV infection. The seroprevalence of HCV was significantly higher among waste handlers with a history of not using PPE. Both groups of waste handlers should receive proper attention to protect them from any infectious agents, including HBV and HCV, that they can acquire during working hours. Healthcare administrators, municipal officers, and other stakeholders should work together to minimize the chances of infection due to viral hepatitis by ensuring access to PPE, arranging practical training, supplying informative guidelines, and providing free HBV vaccination schemes.
Abbreviations
HBV, hepatitis B virus; HCV, hepatitis C virus; DWH, domestic waste handler; MWH, medical waste handler; ELISA, enzyme-linked immunosorbent assay.
Data Sharing Statement
The original data used for this study are available from the corresponding author upon reasonable request.
Acknowledgment
We would like to acknowledge the Research and Ethics Review Committee of Wollo University, College of Medicine and Health Sciences, who gave us permission to conduct this study. We are also grateful to our data collectors, and to the study participants who provided blood specimens for screening purposes and information about their socio-demographic and clinical characteristics.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global Hepatitis Report 2017. World Health Organization; 2017.
2. World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021. Towards Ending Viral Hepatitis. World Health Organization; 2016.
3. World Health Organization. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021: Accountability for the Global Health Sector Strategies 2016–2021: Actions for Impact. World Health Organization; 2021.
4. Stanaway JD, Flaxman AD, Naghavi M, et al. The global burden of viral hepatitis from 1990 to 2013: findings from the Global Burden of Disease Study 2013. Lancet. 2016;388(10049):1081–1088. doi:10.1016/S0140-6736(16)30579-7
5. Blach S, Terrault NA, Tacke F, et al. Global change in hepatitis C virus prevalence and cascade of care between 2015 and 2020: a modelling study. Lancet Gastroenterol Hepatol. 2022;7(5):396–415. doi:10.1016/S2468-1253(21)00472-6
6. Le LV, Blach S, Rewari B, et al. Progress towards achieving viral hepatitis B and C elimination in the Asia and Pacific region: results from modelling and global reporting. Liver Int. 2022;42(9):1930–1934. doi:10.1111/liv.15131
7. Said ZNA, El-Sayed MH. Challenge of managing hepatitis B virus and hepatitis C virus infections in resource-limited settings. World J Hepatol. 2022;14(7):1333–1343. doi:10.4254/wjh.v14.i7.1333
8. Do Carmo RF, de Souza CDF. Impact of the COVID-19 pandemic on hepatitis C diagnosis in Brazil: is the global hepatitis C elimination strategy at risk? J Hepatol. 2022;76(2):470–472. doi:10.1016/j.jhep.2021.08.005
9. Abd El-Wahab EW, Eassa SM, Lotfi SE, El Masry SA, Shatat HZ, Kotkat AM. Adverse health problems among municipality workers in Alexandria (Egypt). Int J Prev Med. 2014;5(5):545.
10. Gutberlet J, Uddin SMN. Household waste and health risks affecting waste pickers and the environment in low-and middle-income countries. Int J Occup Environ Health. 2017;23(4):299–310. doi:10.1080/10773525.2018.1484996
11. Mol MPG, Greco DB, Cairncross S, Heller L. Hepatitis B and C in household and health services solid waste workers. Cad Saude Publica. 2015;31:295–300. doi:10.1590/0102-311X00083814
12. Arafa A, Eshak ES. Medical waste handling and hepatitis B virus infection: a meta-analysis. Am J Infect Control. 2020;48(3):316–319. doi:10.1016/j.ajic.2019.08.011
13. Anagaw B, Shiferaw Y, Anagaw B, et al. Seroprevalence of hepatitis B and C viruses among medical waste handlers at Gondar town Health institutions, Northwest Ethiopia. BMC Res Notes. 2012;5(1):1–10. doi:10.1186/1756-0500-5-55
14. Mol MP, Gonçalves JP, Silva EA, et al. Seroprevalence of hepatitis B and C among domestic and healthcare waste handlers in Belo Horizonte, Brazil. Waste Manage Res. 2016;34(9):875–883. doi:10.1177/0734242X16649686
15. Yizengaw E, Getahun T, Geta M, et al. Sero-prevalence of hepatitis B virus infection and associated factors among health care workers and medical waste handlers in primary hospitals of North-west Ethiopia. BMC Res Notes. 2018;11(1):1–6. doi:10.1186/s13104-018-3538-8
16. Endris S, Tamir Z, Sisay A. Medical laboratory waste generation rate, management practices and associated factors in Addis Ababa, Ethiopia. PLoS One. 2022;17(4):e0266888. doi:10.1371/journal.pone.0266888
17. Belyhun Y, Maier M, Mulu A, Diro E, Liebert UG. Hepatitis viruses in Ethiopia: a systematic review and meta-analysis. BMC Infect Dis. 2016;16:1–14. doi:10.1186/s12879-016-2090-1
18. Deress T, Million Y, Belachew T, Jemal M, Girma M. Seroprevalence of hepatitis C viral infection in Ethiopia: a systematic review and meta-analysis. Sci World J. 2021;2021. doi:10.1155/2021/8873389
19. Yazie TD, Tebeje MG. An updated systematic review and meta-analysis of the prevalence of hepatitis B virus in Ethiopia. BMC Infect Dis. 2019;19:1–13. doi:10.1186/s12879-019-4486-1
20. Shiferaw Y, Abebe T, Mihret A. Hepatitis B virus infection among medical waste handlers in Addis Ababa, Ethiopia. BMC Res Notes. 2011;4:1–7. doi:10.1186/1756-0500-4-479
21. Mengiste DA, Dirbsa AT, Ayele BH, Hailegiyorgis TT. Hepatitis B virus infection and its associated factors among medical waste collectors at public health facilities in eastern Ethiopia: a facility-based cross-sectional study. BMC Infect Dis. 2021;21(1):1–8. doi:10.1186/s12879-021-05918-x
22. Kebede E, Getnet G, Enyew G, Gebretsadik D. Transfusion transmissible infections among voluntary blood donors at Dessie Blood Bank, Northeast Ethiopia: cross-sectional study. Infect Drug Resist. 2020;Volume 13:4569–4576. doi:10.2147/IDR.S287224
23. Gebretsadik D, Assefa M, Fenta GM, Daba C, Ali A, Tekele SG. High seroprevalence of hepatitis B and C virus infections among pregnant women attending antenatal clinic in Borumeda General Hospital, Northeast Ethiopia. Biomed Res Int. 2022;2022:1–11. doi:10.1155/2022/1395238
24. Metaferia Y, Ali A, Eshetu S, Gebretsadik D. Seroprevalence and associated factors of human immunodeficiency virus, Treponema pallidum, hepatitis B virus, and hepatitis C virus among female sex workers in Dessie City, Northeast Ethiopia. Biomed Res Int. 2021;2021:1–13. doi:10.1155/2021/6650333
25. Hossain MR, Islam MA, Hasan M. Assessment of medical waste management practices: a case study in Gopalganj Sadar, Bangladesh. Eur J Med Health Sci. 2021;3(3):62–71.
26. Adu RO, Gyasi SF, Essumang DK, Otabil KB. Medical waste-sorting and management practices in five hospitals in Ghana. J Environ Public Health. 2020;2020:1–14. doi:10.1155/2020/2934296
27. Shalini S, Harsh M, Mathur B. Evaluation of bio-medical waste management practices in a government medical college and hospital. Natl J Commun Med. 2012;3(01):80–84.
28. Mitiku G, Admasie A, Birara A, Yalew W. Biomedical waste management practices and associated factors among health care workers in the era of the covid-19 pandemic at metropolitan city private hospitals, Amhara region, Ethiopia, 2020. PLoS One. 2022;17(4):e0266037. doi:10.1371/journal.pone.0266037
29. Hangulu L, Akintola O. Health care waste management in community-based care: experiences of community health workers in low resource communities in South Africa. BMC Public Health. 2017;17:1–10. doi:10.1186/s12889-017-4378-5
30. Shahzadi A, Hussain M, Afzal M, Gilani SA. Determination the level of knowledge, attitude, and practices regarding household waste disposal among people in rural community of Lahore. Int J Soc Sci Manage. 2018;5(3):219–224. doi:10.3126/ijssm.v5i3.20614
31. Zikhathile T, Atagana H. Challenges facing home-based caregivers in the management of health care risk waste. Int J Environ Res Public Health. 2018;15(12):2700. doi:10.3390/ijerph15122700
32. Selvan Christyraj JRS, Selvan Christyraj JD, Adhimoorthy P, Rajagopalan K, Nimita Jebaranjitham J. Impact of biomedical waste management system on infection control in the midst of COVID-19 pandemic. In: The Impact of the COVID-19 Pandemic on Green Societies: Environmental Sustainability. Springer; 2021:235–262.
33. Mol MPG, Cairncross S, Greco DB, Heller L. Is waste collection associated with hepatitis B infection? A meta-analysis. Rev Soc Bras Med Trop. 2017;50:756–763. doi:10.1590/0037-8682-0010-2017
34. Gedefie A, Adamu A, Alemayehu E, Kassa Y, Belete MA. Hepatitis C virus infection among HIV-infected patients attending Dessie Referral Hospital, Northeastern Ethiopia. Int J Microbiol. 2021;2021:1–7. doi:10.1155/2021/6675851
35. Assen S, Wubshet M, Kifle M, Wubayehu T, Aregawi BG. Magnitude and associated factors of needle stick and sharps injuries among health care workers in Dessie City Hospitals, north east Ethiopia. BMC Nurs. 2020;19:1–8. doi:10.1186/s12912-020-00422-0
36. Kassa Y, Million Y, Biset S, Moges F. Hepatitis B and hepatitis C viral infections and associated factors among prisoners in northeast Ethiopia. J Blood Med. 2021;Volume 12:561–570. doi:10.2147/JBM.S314556
37. Auta A, Adewuyi EO, Kureh GT, Onoviran N, Adeloye D. Hepatitis B vaccination coverage among health-care workers in Africa: a systematic review and meta-analysis. Vaccine. 2018;36(32):4851–4860. doi:10.1016/j.vaccine.2018.06.043
38. Franka E, El-Zoka A, Hussein A, Elbakosh M, Arafa A, Ghenghesh K. Hepatitis B virus and hepatitis C virus in medical waste handlers in Tripoli, Libya. J Hosp Infect. 2009;72(3):258–261. doi:10.1016/j.jhin.2009.03.019
39. Nelson NP, Easterbrook PJ, McMahon BJ. Epidemiology of hepatitis B virus infection and impact of vaccination on disease. Clin Liver Dis. 2016;20(4):607–628. doi:10.1016/j.cld.2016.06.006
40. Anteneh A, Mesfin W, Endale T, Techalew S. The exposure rate to hepatitis B and C viruses among medical waste handlers in three government hospitals, southern Ethiopia. Epidemiol Health. 2016;38:245.
41. Atlaw D, Sahiledengle B, Tariku Z. Hepatitis B and C virus infection among healthcare workers in Africa: a systematic review and meta-analysis. Environ Health Prev Med. 2021;26(1):1–14. doi:10.1186/s12199-021-00983-9
42. Spearman CW, Afihene M, Ally R, et al. Hepatitis B in sub-Saharan Africa: strategies to achieve the 2030 elimination targets. Lancet Gastroenterol Hepatol. 2017;2(12):900–909. doi:10.1016/S2468-1253(17)30295-9
43. Sperle I, Steffen G, Leendertz SA, et al. Prevalence of hepatitis B, C, and D in Germany: results from a scoping review. Front Public Health. 2020;8:424. doi:10.3389/fpubh.2020.00424
44. Hebo HJ, Gemeda DH, Abdusemed KA. Hepatitis B and C viral infection: prevalence, knowledge, attitude, practice, and occupational exposure among healthcare workers of Jimma University Medical Center, Southwest Ethiopia. Sci World J. 2019;2019:1–11. doi:10.1155/2019/9482607
45. Sawyerr HO, Yusuf RO, Adeolu AT. Risk factors and rates of hepatitis B virus infection among municipal waste management workers and scavengers in Ilorin, Kwara State, Nigeria. J Health Pollut. 2016;6(12):1–6. doi:10.5696/2156-9614-6.12.1
46. Rachiotis G, Papagiannis D, Markas D, Thanasias E, Dounias G, Hadjichristodoulou C. Hepatitis B virus infection and waste collection: prevalence, risk factors, and infection pathway. Am J Ind Med. 2012;55(7):650–655. doi:10.1002/ajim.22057
47. Uddin MS, Islam MN, Khan MEU, Yeasmin S, Ahmed F, Amiruzzaman M. Frequency of hepatitis B and C viral infection among the medical waste handlers. Bangla J Infect Dis. 2017;4(1):3–9. doi:10.3329/bjid.v4i1.37673
48. Anozie OB, Lawani LO, Eze JN, et al. Knowledge, attitude and practice of healthcare managers to medical waste management and occupational safety practices: findings from Southeast Nigeria. J Clin Diagn Res. 2017;11(3):IC01. doi:10.7860/JCDR/2017/24230.9527
49. Shiferaw Y, Abebe T, Mihret A. Sharps injuries and exposure to blood and bloodstained body fluids involving medical waste handlers. Waste Manage Res. 2012;30(12):1299–1305. doi:10.1177/0734242X12459550
50. Honda H, Iwata K. Personal protective equipment and improving compliance among healthcare workers in high-risk settings. Curr Opin Infect Dis. 2016;29(4):400–406. doi:10.1097/QCO.0000000000000280
51. Kangethe JM, Komu JG, Muturi DN, et al. Hepatitis B virus infections and associated risk factors among medical waste handlers at the Kenyatta National Hospital, Nairobi Kenya. JMSCR. 2019;7(03):499–506.
52. Haley RW, Fischer RP. Commercial tattooing as a potentially important source of hepatitis C infection: clinical epidemiology of 626 consecutive patients unaware of their hepatitis C serologic status. Medicine. 2001;80(2):134–151. doi:10.1097/00005792-200103000-00006
53. Ansari-Moghaddam A, Ansari H, Khosravi S, et al. The prevalence of hepatitis B virus among municipal solid waste workers: necessity for immunization of at-risk groups. Hepat Mon. 2016;16(3). doi:10.5812/hepatmon.30887
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.