Back to Journals » Clinical Epidemiology » Volume 14
Serious Mental Illness Exacerbation Post-Bereavement: A Population-Based Study of Partners and Adult Children
Authors Tay DL ![]() , Thygesen LC
, Thygesen LC ![]() , Kozlov E, Ornstein KA
, Kozlov E, Ornstein KA
Received 30 April 2022
Accepted for publication 25 August 2022
Published 20 September 2022 Volume 2022:14 Pages 1065—1077
DOI https://doi.org/10.2147/CLEP.S372936
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor H Sorensen
Djin L Tay,1 Lau C Thygesen,2 Elissa Kozlov,3 Katherine A Ornstein4
1College of Nursing, University of Utah, Salt Lake City, UT, USA; 2National Institute of Public Health, University of Southern Denmark, Copenhagen, Denmark; 3Department of Health Behavior, Society and Policy, School of Public Health, Rutgers, The State University of New Jersey, Piscataway, NJ, USA; 4School of Nursing, Johns Hopkins University, Baltimore, MD, USA
Correspondence: Djin L Tay, College of Nursing, University of Utah, 10S 2000 E, Salt Lake City, UT, 84112, USA, Tel +1 801-882-3037, Email [email protected]
Purpose: The death of a close family member is commonly accompanied by intense grief, stress, and loss of social support. We hypothesized that recent bereavement would be associated with an increase in symptom exacerbations among adults with serious mental illness (SMI) whose partners or parents had died.
Patients and Methods: Adults whose partners and parents had died in Denmark between January 1, 2010, and June 30, 2016, were identified using linked population-based registries. History of SMI was defined as having a diagnosis of schizophrenia and schizoaffective disorders, major depression, and bipolar disorder in the five years preceding their family member’s death in the Danish Psychiatric Central Research Register using International Classification of Diseases-10 codes. The odds of SMI exacerbation (ie, attempt or completion of suicide or psychiatric hospitalization) among partners and children in the first two years after death in 3-month intervals were estimated with generalized estimating equations.
Results: 12.8% of partners and 15.0% of adult children with a history of SMI experienced any SMI exacerbation two years after bereavement. Among bereaved partners, older age (80+ years) was associated with a lower risk of experiencing an SMI exacerbation compared with partners aged 18– 49 years (ORadj=0.29, [0.18– 0.45]). Partners with a history of SMI had significantly increased odds of SMI exacerbations three months after their partners’ death compared to prior to their partners’ death (ORadj = 1.43, [1.13– 1.81]). There was no evidence that adult children with SMI experience increased SMI exacerbations after the death of their parents compared to prior to death.
Conclusion: Adults with a history of SMI whose partners had died are at increased risk for an SMI exacerbation post bereavement. Additional bereavement resources and support should be provided to those with a history of SMI, especially in the period immediately after death.
Keywords: severe mental disorders, bereavement, population register, suicide, emergency psychiatric services
Introduction
Bereavement following the death of a close family member, particularly a partner or spouse, is one of the most stressful life events for individuals.1 Partner or spousal relationships are highly interdependent emotionally, socially, and financially; as such, the loss of a partner is a devastating life event.2 Bereavement has been associated with increased use of antidepressants3 and elevated risks in mortality by natural and non-natural causes in widows4 and widowers.5 This risk is especially elevated in the early period of bereavement.6,7 Moreover, the loss of a family member has a significant impact on non-spousal family members. After the loss of a sibling, for example, young and middle-aged adult siblings are at increased risk for antidepressant, anxiolytic, and primary and inpatient mental health service use, as well as new diagnoses of mood or substance disorders.8 While the bereavement literature finds that adult children in the general population have better adjustment to the loss of a parent than partners,2,3,9,10 there is heterogeneity regarding the impact of timing on bereavement outcomes. Furthermore, the bereavement process can be complicated by unpreparedness for death, family dynamics, coping, context of death, sociodemographic differences, and the presence of mental health disorders.11–15
Notably, the presence of mental health needs prior to the death of a family member contributes to poorer bereavement outcomes such as complicated grief.16 Individuals with serious mental illnesses (SMI), characterized by mental, behavioral, or emotional disorders associated with serious impairment of daily activities and functioning,17,18 may be at greatest risk for poor bereavement outcomes. Globally, it is estimated that SMIs affect as much as 4% to 6.8% of the population.19 Individuals diagnosed with SMIs represent a highly complex patient population with a high need for psychiatric, physical health, and social support. Individuals with SMIs, such as schizophrenia, bipolar disorders, and major depression, have greater risk for alcohol and substance use disorders,20,21 poorer physical health outcomes,22–24 and increased hospitalizations and emergency department visits.25,26 The death of a close family member can affect individuals with SMI more adversely than the general population—individuals diagnosed with mental health disorders are at greater risk for post-traumatic stress disorder symptoms, self-harm, suicide, new psychiatric diagnoses, and prolonged grief after the loss of a family member or close member of their social networks.9,11,12,27,28 The intersectionality between serious mental illness and a traumatic event such as bereavement can exacerbate posttraumatic stress symptoms,28 and may be linked to poorer coping29 and maladaptive attachment12 among this population.
While a growing body of research has examined psychiatric outcomes associated with the death of a family member,3,6,8,9,16 few studies have focused on examining the risk of adverse outcomes among individuals with SMI whose family members have died. Given that SMI and close family relationships are risk factors for adverse mental health outcomes in bereavement, the purpose of this study was to determine the risk of adverse mental health outcomes among adults with SMI whose partners and parents had died. Moreover, we aimed to identify periods of time beyond the death of a family member in which adults with SMI may be more vulnerable to exacerbations during the bereavement period. Using a population dataset comprising families of all decedents in Denmark who died between 2009 and 2016, we hypothesized that (1) adults with SMI whose partners and parents had died will be at greatest risk for SMI exacerbations in the first three months after bereavement and (2) risk of SMI exacerbations will be higher for partners compared to adult children.
Material and Methods
This study was approved by the Danish Data Protection Agency (record number 17/9058). According to Danish law, ethical review board approval or informed consent from subjects is not required for purely register-based studies. The study was also reviewed by the Program for the Protection of Human Subjects at the Icahn School of Medicine at Mount Sinai and was considered exempt.
Population
The study included all Danish permanent residents over the age of 18 who died between January 1, 2009, and December 31, 2016. In line with our previous work and those of others focused on bereavement in populations, we limited our sample to deaths from natural causes (ie, excluding deaths from accidents, homicides, suicides, or war),3,8,9 as sudden and violent death is a well-established risk factor for poorer bereavement adjustment and mental health.5,9,13,14 We identified all adult children and partners of decedents who had five years of mental health history available within the Danish Psychiatric Central Research Register (N=737,388; 25.2% partners, 74.8% adult children). Due to the increased prevalence of adverse psychiatric outcomes and psychiatric comorbidity,19,30,31 we included the following three diagnosis groups in our definition of SMI: 1) schizophrenia and schizoaffective disorders, 2) major depression (single and recurrent episodes), and 3) bipolar disorder. The SMIs selected for this study are in line with SMI populations examined in other studies.32–35 SMIs were identified among adult children and partners using International Classification of Diseases-10 codes (1) schizophrenia (F20) and psychotic disorders (schizoaffective disorder: F25), (2) Major depression (F32-F33), and (3) bipolar disorder (F31) identified in the Danish Psychiatric Central Register in the 12 months to five years prior to the death of their family member, as individuals diagnosed earlier may have more stable conditions.
Data Sources
The data sources linked to this study are nationwide registers that have been described in the previous work8 and include the Danish Civil Registration System,36 the Danish Register of Causes of Death,37 the Danish National Patient Register,38,39 and Statistics Denmark,40,41 with diagnoses and outcomes of interest identified from the Danish Psychiatric Central Research Register.42 The Danish Psychiatric Central Research Register systematically collects clinical records from psychiatric departments and hospitals.42 Data collected includes both the times of onset and end of treatment, diagnoses, referral type, area of residence, and method of admission for the population, and are almost complete for the Danish population.42
Measures
Dependent Variable
Our primary outcome of interest was SMI symptom exacerbations.9 We defined SMI exacerbations as the following: any suicide attempt (T14.91), inpatient psychiatric hospitalization, or completed suicide (X60-X84), as used in other studies.9,33 As with our previous work and those of others, ICD-10 codes and inpatient psychiatric hospitalization events were retrieved from the Danish National Patient Register and the Danish Psychiatric Central Research Register.8,43 Because of our interest in timing of exacerbations, outcomes were assessed at 3-month intervals for the first two years of bereavement in bereaved partners or adult children with a history of SMI (ie, 1–3 months post death, 3–6 months post death, etc.). Most grief resolves naturally by 6 months,44 however we studied SMI exacerbations for 2 years after the family members’ death, as studies support that bereavement experiences are most intense in the first two years after death.3,5,8,9,45
Sociodemographic Covariates
Outcomes were adjusted for the following sociodemographic characteristics among individuals diagnosed with SMI: age (years), sex (male/female), region (Capital, Zealand, Southern, Central, and Northern Denmark regions) marital status (married, single/never married, divorced, widowed), education (primary, vocational, short theoretical, medium theoretical, and long theoretical), and income (quartiles).46–48 Decedent characteristics were not included in our analysis as previous research did not support associations between characteristics of decedents and mental health outcomes in bereavement.3,8
Mental and Physical Health Covariates
As alcohol and substance use, poorer physical health, and recent history of mental health utilization often co-occur with SMI,19,21,22,24,26,49,50 we included mental and behavioral disorders due to alcohol and psychoactive substance use (F10-F19), comorbidity (Charlson Comorbidity Index-CCI),51 and prior recent history of attempted suicide or inpatient psychiatric hospitalization in the year before the patient’s family member had died as covariates as identified through the Danish National Patient Register and the Danish Psychiatric Central Research Register.
Statistical Analysis
Counts, proportions, and descriptive statistics were produced to characterize the sample. Counts and proportions were used to describe the prevalence of SMI exacerbations among partners and adult children across time periods (1 year before death, and the first year, second year, and over the first two years after death). Logistic regression models were used to identify factors associated with SMI exacerbation among partners and adult children, and adjusted odds ratios (ORadj), 95% confidence intervals (95% CI) were produced. In order to account for non-independence of observations across time periods,52 generalized estimating equations (GEE) using a logit link function were used to examine the odds of SMI exacerbations in the period after death. The period 9 to <12 months (or 271–360 days) prior to death was used as each individual’s reference point and odds of an event occurring were calculated every 3-month interval from death up to 2 years. Analyses were run separately for partners and children, as our prior research has established that patterns of mental health utilization are different for partners and children in Denmark, with partners experiencing more change in mental health utilization patterns.3,8
Results
Between January 1, 2010, and June 30, 2016, N = 13,095 partners and adult children (partners: n = 2552, 19.5%; children n = 10,543, 80.5%) with an SMI diagnosis experienced the loss of a partner and/or parent. Table 1 describes the characteristics of the sample. The mean age of partners was 68.7 years (SD=13.6), while the mean age of children was 44.8 years (SD=10.4). The majority of partners (77.2%) and children (52.7%) were female, and greater proportions had lower levels of education (52.4% of partners and 42.0% of children had primary school educations). Children had higher median incomes (172,000 DKK) compared with partners (147,000 DKK). Almost half of partners (47%) and 20.4% of children had at least one comorbidity. The greatest proportions of partners and children resided in the Capital Region of Denmark (partners = 27.5%; children = 30.3%). The most prevalent SMI for partners and children was major depressive disorder (75.0%; 63.1%), followed by bipolar disorder for partners (17.3%) and schizophrenia for children (27.3%; Table 1).
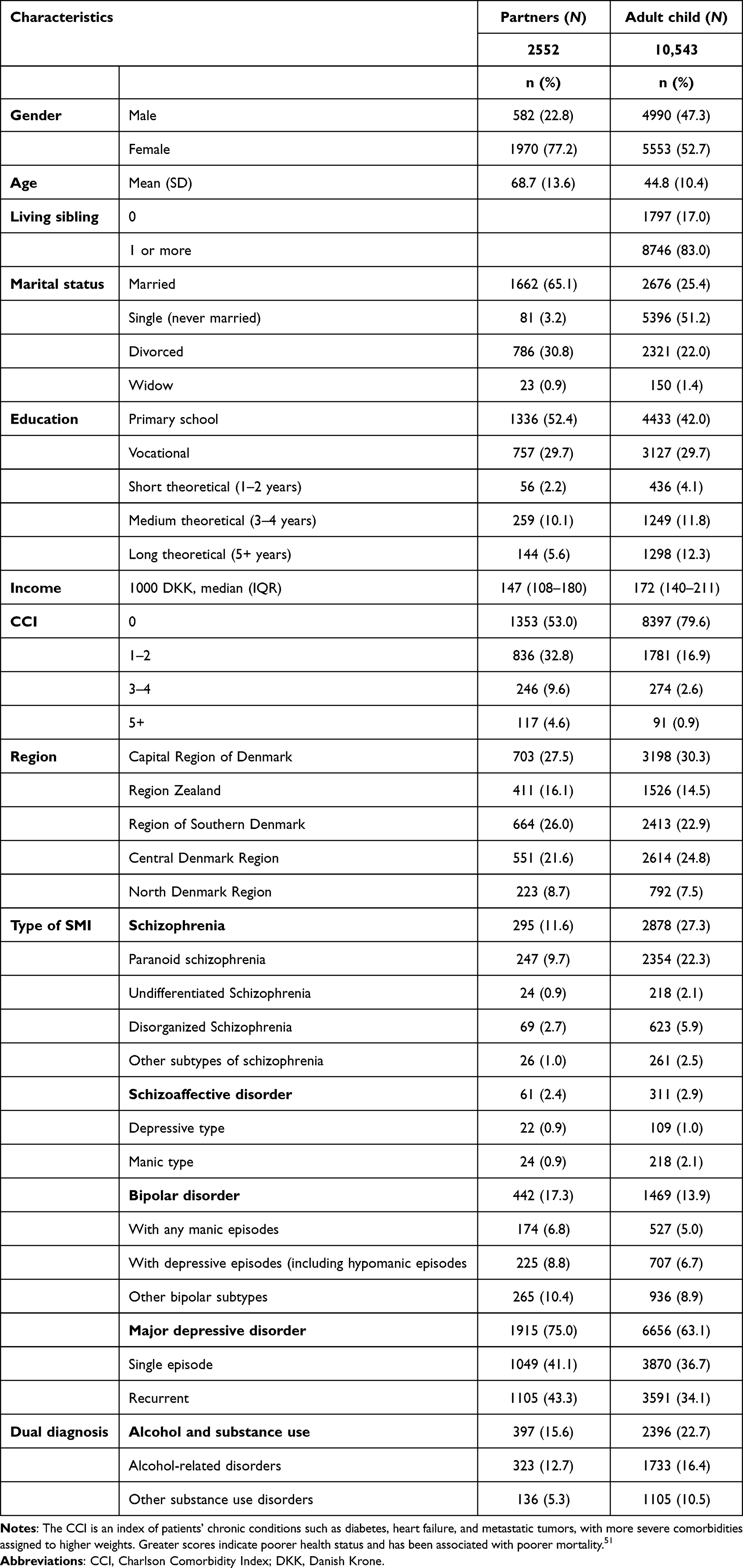 |
Table 1 Characteristics of Bereaved Partners and Children with SMI |
Table 2 describes the proportions, by year of bereavement, of psychiatric hospitalizations and attempted and completed suicide by adults with SMI before and after their partners or parents died (partners and adult children may have multiple events over the two years after the death of the family member). The proportions of SMI exacerbations increased in the first two years after the death of a partner from 26.1% to 31.5% for individuals with schizophrenia or schizoaffective disorder, from 20.1% to 26.5% for individuals with bipolar disorder, and from 9.0% to 12.7% for individuals with major depression compared to the year before the death of a partner. Among adult children with SMI, the overall proportions of an SMI exacerbation also increased slightly in the first two years after the death of a parent (schizophrenia/schizoaffective disorder: 26% to 34.9%, bipolar disorder: 18.0% to 26.3%, major depression: 9.6% to 12.9%) compared with the year before the death of their parent. Increases in psychiatric inpatient hospitalizations over the two years of bereavement were the most common SMI exacerbation for children, particularly for those diagnosed with schizophrenia or schizoaffective disorder (25.6% to 34.6%) and bipolar disorder (17.8% to 26.0%). Variations in specific SMI exacerbations for partners were not reported due to low cell counts. Lower proportions of SMI exacerbations were observed in the second year of bereavement when compared with the first year of bereavement among partners and children across all major SMI diagnoses in the second year after death. For example, there was a 6.1% and 2.7% reduction in the proportions of any SMI exacerbation for partners and children with schizophrenia and schizoaffective disorders, respectively, in the second year after the death of the family member compared to the first year.
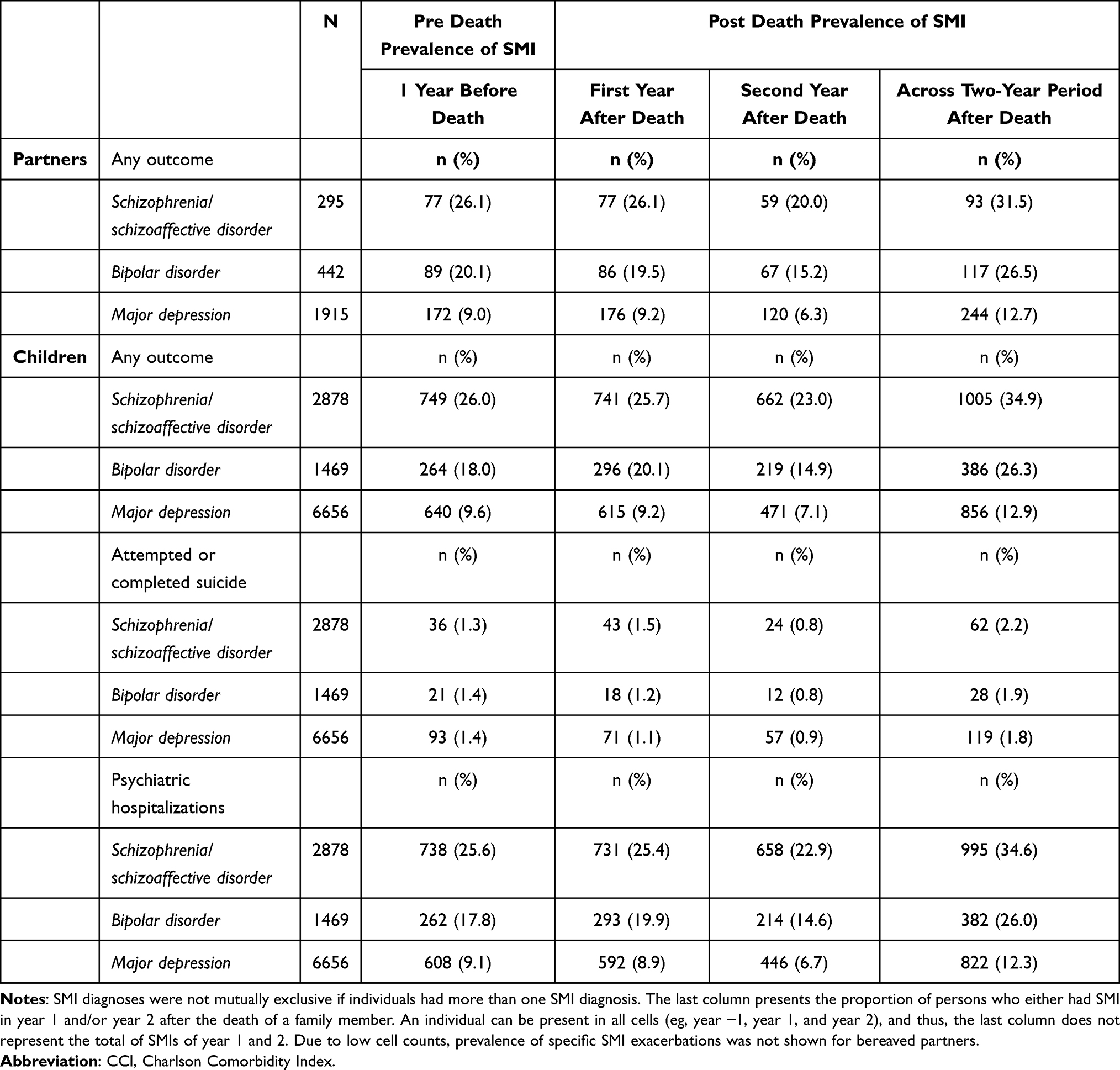 |
Table 2 Prevalence of SMI Exacerbations One Year Before and Two Years After the Death of a Partner or Parent, Among Adults Diagnosed with SMI |
Table 3 describes differences in sociodemographic characteristics among partners and adult children who experienced SMI exacerbations.
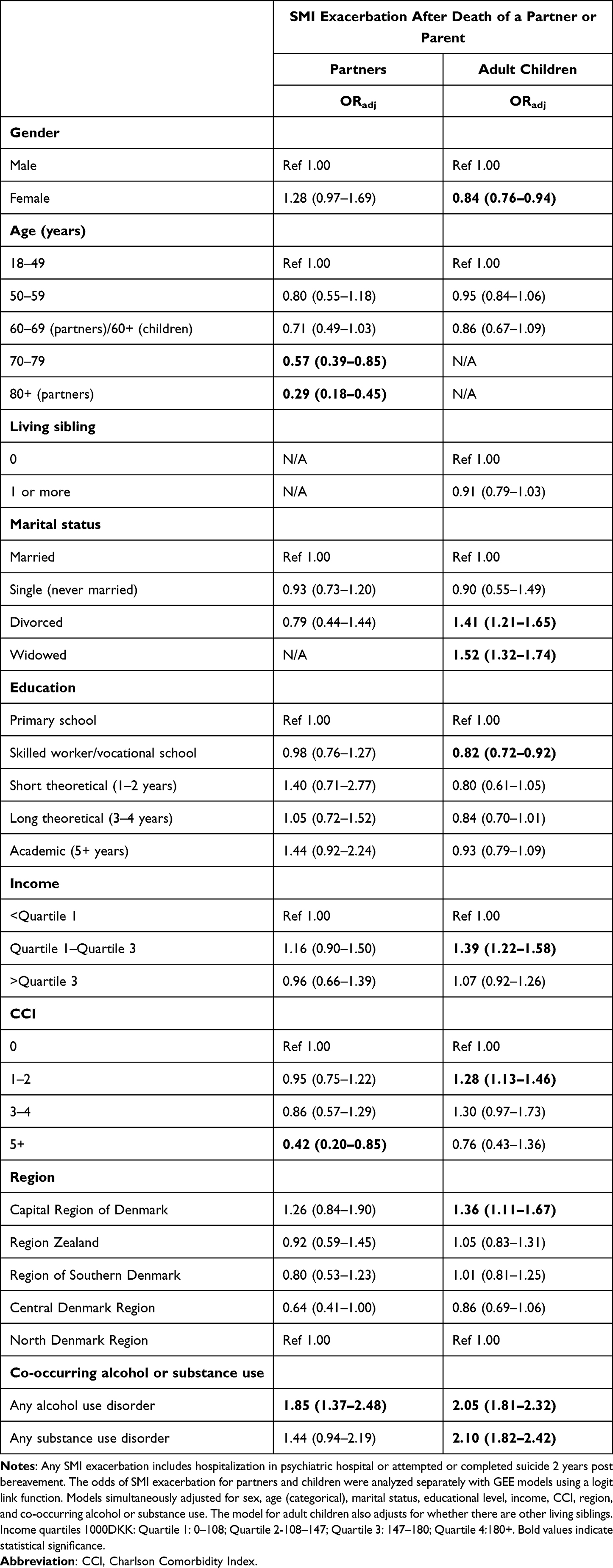 |
Table 3 Characteristics Associated with SMI Exacerbation Within 2 Years After Family Members’ Death Among Bereaved Partners and Adult Children with SMI – Results from GEE Models |
Demographic, Socioeconomic, and Geographic Factors Associated with SMI Exacerbations
Adjusting for demographic, socioeconomic, geographic, and physical and mental health characteristics, daughters with SMI were less likely than sons to experience an SMI exacerbation (ORadj=0.84, [0.76–0.94]; Table 3). In partners, being 70–79 years of age was associated with a 43% decrease (ORadj=0.57, [0.39–0.85]) and being 80 or older was associated with a 71% decrease (ORadj=0.29, [0.18–0.45]) in the odds of SMI exacerbation compared to partners under age 50. Adult children diagnosed with SMI had a higher odds of having an SMI exacerbation if they were divorced (ORadj=1.41, [1.21–1.65]) or widowed (ORadj=1.52, [1.32–1.74]) compared with married individuals or had incomes within the first and third quartiles of the population (ORadj=1.39, [1.22–1.58]) compared with those earning less than the lowest quartiles of incomes. Children with a skilled worker or vocational education (ORadj=0.82, [0.72–0.92]) had lower odds of SMI exacerbation, while children who lived in the Capital Region of Denmark (ORadj=1.36, [1.11–1.67]) had higher odds of SMI exacerbation compared with children with primary schooling and who lived in the Northern Denmark region.
Physical and Mental Health Factors Associated with SMI Exacerbations
Adjusting for demographic, socioeconomic, geographic, and physical and mental health characteristics, partners with more comorbidities (5+ comorbidity ORadj=0.42, [0.20–0.85]) had lower odds of SMI exacerbation compared with partners without any comorbidities. Additionally, adult children with one to two comorbidities had elevated odds of an SMI exacerbation (ORadj=1.28, [1.13–1.46]; Table 3). Being diagnosed with any co-occurring alcohol use disorder was associated with a higher odds of SMI exacerbation in partners (ORadj=1.85, [1.37–2.48]) and adult children (ORadj=2.05, [1.81–2.32]). In addition, being diagnosed with any substance use disorder was associated with over twice the likelihood of experiencing an SMI exacerbation in the two years after parent death (ORadj=2.10, [1.82–2.42]) in adult children.
Figure 1 shows the odds of SMI exacerbation in the two years following death by 3-month time interval, illustrating that across all time periods, partners are at greater risk for SMI exacerbations and that odds of SMI exacerbations decrease over time for bereaved partners and children. As shown in Figure 1, partners diagnosed with SMI had significantly higher odds of experiencing an SMI exacerbation in the first three months of their partners’ death compared with nine to 12 months before death (ORadj=1.43, [1.13–1.81], adjusting for sex, age, educational level, comorbidity, and region). For adult children diagnosed with SMI, odds of an SMI exacerbation dropped by 13–17% in the 2nd year after the death of a parent (12–15 months: ORadj=0.85, [0.76–0.96]; 15–18 months ORadj=0.86, [0.76–0.97]; 18–21 months: ORadj=0.83, [0.73–0.94]; 21–24 months: ORadj=0.87, [0.77–0.99] see Supplementary Table 1), adjusting for sex, age, educational level, comorbidity, region, and presence of a living sibling. Interactions for time and relationship to the decedent were statistically significant (partner: p=0.04; adult child=p=0.0003).
 |
Figure 1 Odds of experiencing SMI exacerbations among bereaved partners and children diagnosed with SMI by 3-month periods compared to before the death of the family member. |
Discussion
This study allowed us to determine the prevalence of SMI exacerbations among bereaved partners and children diagnosed with SMI within a population. Our main finding showed that bereaved partners with a history of SMI are at greatest risk for exacerbations within the first three months of bereavement.
After adjusting for covariates, bereavement was observed to have a greater negative impact on surviving partners compared to adult children with a history of SMI. The death of a partner is not only characterized by intense grief and loss but is also associated with potential losses in financial and social support, and contributes to stress and instability that may trigger additional mental health crises.18,27,28 The marital relationship is often a primary source of social support, and the protective effects of marriage on adverse outcomes for individuals with mental illness have been well documented.53,54 As such, the loss of a partner may be a destabilizing event for partners with SMI. This finding extends previous work on the bereaved population that has reported that the first months after the loss of a partner are associated with increases in new antidepressant prescriptions3,8 and incidence of self-harm, psychiatric diagnoses, and suicide compared with non-bereaved partners, especially for those with a prior diagnosis of mental illness.9 These findings highlight the importance of timely intervention for adults with SMI who lost a partner.
The odds of experiencing an SMI exacerbation was reduced for adult children in the second year after the death of a parent, which is a finding reflected in the previous work examining odds of new antidepressant use in the general population.3,8 While families are among the main sources of social support that help promote stability or intervene in SMI exacerbations,55 it is also possible that parents may be a source of stress and conflict for adult children with SMI.56 Almost one in five family members of individuals with SMI report being recipients of interpersonal violence,57,58 and it is possible that individuals with the most severe SMI may be estranged from their families,59 information that we were unable to capture using these data.
This study also observed that co-occurring alcohol and substance use disorders were associated with almost twice the odds of SMI exacerbation. Individuals diagnosed with SMI and co-occurring alcohol or substance use disorders have higher rates of self-harm and suicide,48,54 inpatient visits,26 hospital readmissions,34 and overall mortality.37,60 This finding suggests that individuals with these dual diagnoses may have more maladaptive coping in bereavement,29 which emphasizes the need for more focused bereavement support for this vulnerable population.
Individuals diagnosed with SMIs often face inadequate social support which can pose substantial barriers to recovery.61,62 In this study, we found that divorced and widowed children had greater odds of experiencing an SMI exacerbation compared to married children. Additionally, our findings that older age and presence of comorbidities were associated with lower risk for SMI exacerbations in partners with SMI are supported in the literature.33,63 This is unsurprising, as research demonstrates that biological aging is protective for schizophrenia64 and bipolar disorder65 symptom severity, and that individuals with SMI also have poorer health and higher medical utilization than the general population.26,34 Apart from these sociodemographic and health factors, this study also finds that the highest proportions of SMI exacerbations occurred among individuals diagnosed with schizophrenia, schizoaffective, and bipolar disorders in the first two years of bereavement, hence highlighting populations that can be targeted for intervention.
In addition to these findings, we observed factors associated with SMI exacerbations that were unexpected and should be further studied. For example, children living in the Capital Region of Denmark were at higher risk of SMI exacerbations compared with adult children living in the North Denmark region. This is in contrast to other studies which find that living in more urban regions may be protective regarding mental health recovery.49 It is unclear why there are increased odds of SMI exacerbation associated with income and region in this study, although individuals with SMI face increased social marginalization,66 economic challenges such as unstable housing and employment,49,66 and financial struggles,67 which may be affected by income and region of residence. It is also possible that smaller towns have tighter knit social support systems that may better support the bereaved.
Limitations
This study focuses on the impact of bereavement on partners and adult children only. Research on the impact of bereavement on other relationship types (family and otherwise) should also be explored in the context of SMI exacerbation. These data fail to capture whether families were estranged, or if other caregiving roles were involved. Thus, we are unable to assess the quality of relationships between partners and adult children with the deceased, which is a key predictor of complicated grief.18 While the analyses were adjusted for pre-existing chronic disease conditions, the data do not allow for the assessment of other confounders such as social engagement, coping skills, and other family and/or community support. Additionally, while this population sample was large, Denmark is a relatively small and culturally homogeneous country with a nationalized healthcare system, making the generalizability of these results limited beyond the Nordic countries. Due to the nationalized healthcare system, access to mental health services is greater compared to other health systems such as in the US; as such, this study may have greater representation of the SMI population, which is a strength of the present study. Furthermore, data collected for these analyses do not rely on participant report and thus are more objective.
Conclusion
Individuals diagnosed with SMI are a vulnerable population at risk of adverse mental health outcomes. This study is the first to characterize the likelihood of an SMI exacerbation in a population among adults with SMI whose partners and parents had died. Findings from this study provide insight into groups that may benefit from additional support and highlight that the first three months after the death of a partner is a crucial time for intervention.
Acknowledgments
Research reported in this publication was supported by the National Palliative Care Research Center of the National Institutes of Health and the National Institute on Aging under the award number K01AG047923. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. We thank Nathan Caines, BS, for assistance in the literature search for this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stroebe M, Schut H, Stroebe W. Health outcomes of bereavement. Lancet. 2007;370(9603):1960–1973. doi:10.1016/S0140-6736(07)61816-9
2. Osterweis M, Solomon F, Green M. Reactions to particular types of bereavement. In: Bereavement: Reactions, Consequences, and Care. National Academies Press (US); 1984.
3. Ornstein KA, Aldridge M, Gillezeau C, et al. New antidepressant utilization pre- and post-bereavement: a population-based study of partners and adult children. Soc Psychiatry Psychiatry Epidemiol. 2020;55(10):1261–1271. doi:10.1007/s00127-020-01857-1
4. Lichtenstein P, Gatz M, Berg S. A twin study of mortality after spousal bereavement. Psychol Med. 1998;28(3):635–643. doi:10.1017/S0033291798006692
5. Erlangsen A, Jeune B, Bille-Brahe U, Vaupel JW. Loss of partner and suicide risks among oldest old: a population-based register study. Age Ageing. 2004;33(4):378–383. doi:10.1093/ageing/afh128
6. Prior A, Fenger-Grøn M, Davydow DS, et al. Bereavement, multimorbidity and mortality: a population-based study using bereavement as an indicator of mental stress. Psychol Med. 2018;48(9):1437–1443. doi:10.1017/S0033291717002380
7. Martikainen P, Valkonen T. Mortality after death of spouse in relation to duration of bereavement in Finland. J Epidemiol Community Health. 1996;50(3):264–268. doi:10.1136/jech.50.3.264
8. Gazibara T, Ornstein KA, Gillezeau C, et al. Bereavement among adult siblings: an examination of health services utilization and mental health outcomes. Am J Epidemiol. 2021;190(12):2571–2581. doi:10.1093/aje/kwab212
9. Guldin MB, Ina Siegismund Kjaersgaard M, Fenger-Gron M, et al. Risk of suicide, deliberate self-harm and psychiatric illness after the loss of a close relative: a nationwide cohort study. World Psychiatry. 2017;16(2):193–199. doi:10.1002/wps.20422
10. Aoyama M, Miyashita M, Masukawa K, et al. Predicting models of depression or complicated grief among bereaved family members of patients with cancer. Psycho-Oncology. 2021;30(7):1151–1159. doi:10.1002/pon.5630
11. Macias C, Jones D, Harvey J, Barreira P, Harding C, Rodican C. Bereavement in the context of serious mental illness. Psychiatr Serv. 2004;55(4):421–426. doi:10.1176/appi.ps.55.4.421
12. Mason TM, Tofthagen CS, Buck HG. Complicated grief: risk factors, protective factors, and interventions. J Soc Work End Life Palliat Care. 2020;16(2):151–174. doi:10.1080/15524256.2020.1745726
13. Groot MH, Keijser J, Neeleman J. Grief shortly after suicide and natural death: a comparative study among spouses and first-degree relatives. Suicide Life Threat Behav. 2006;36(4):418–431. doi:10.1521/suli.2006.36.4.418
14. Kristensen P, Weisæth L, Heir T. Bereavement and mental health after sudden and violent losses: a review. Psychiatry. 2012;75(1):76–97. doi:10.1521/psyc.2012.75.1.76
15. Stroebe MS, Folkman S, Hansson RO, Schut H. The prediction of bereavement outcome: development of an integrative risk factor framework. Soc Sci Med. 2006;63(9):2440–2451. doi:10.1016/j.socscimed.2006.06.012
16. Nielsen MK, Neergaard MA, Jensen AB, Vedsted P, Bro F, Guldin MB. Predictors of complicated grief and depression in bereaved caregivers: a nationwide prospective cohort study. J Pain Symptom Manage. 2017;53(3):540–550. doi:10.1016/j.jpainsymman.2016.09.013
17. National Institute of Mental Health. Mental illness: statistics; 2022. Available from: https://www.nimh.nih.gov/health/statistics/mental-illness.
18. Lobb EA, Kristjanson LJ, Aoun SM, Monterosso L, Halkett GK, Davies A. Predictors of complicated grief: a systematic review of empirical studies. Death Stud. 2010;34(8):673–698. doi:10.1080/07481187.2010.496686
19. Kessler RC, Aguilar-Gaxiola S, Alonso J, et al. The global burden of mental disorders: an update from the WHO World Mental Health (WMH) surveys. Epidemiol Psychiatr Soc. 2009;18(1):23–33. doi:10.1017/S1121189X00001421
20. Rehm J, Shield KD. Global burden of disease and the impact of mental and addictive disorders. Curr Psychiatry Rep. 2019;21(2):1–7. doi:10.1007/s11920-019-0997-0
21. Choi NG, DiNitto DM. Alcohol use disorder and treatment receipt among individuals aged 50 years and older: other substance use and psychiatric correlates. J Subst Abuse Treat. 2021;131:108445. doi:10.1016/j.jsat.2021.108445
22. Correll CU, Solmi M, Veronese N, et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: a large‐scale meta‐analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry. 2017;16(2):163–180. doi:10.1002/wps.20420
23. Gronholm PC, Chowdhary N, Barbui C, et al. Prevention and management of physical health conditions in adults with severe mental disorders: WHO recommendations. Int J Mental Health Sys. 2021;15(1):1–10.
24. Vancampfort D, Correll CU, Galling B, et al. Diabetes mellitus in people with schizophrenia, bipolar disorder and major depressive disorder: a systematic review and large scale meta-analysis. World Psychiatry. 2016;15(2):166–174. doi:10.1002/wps.20309
25. Azar KMJ, Petersen JP, Shen Z, et al. Serious mental illness and health-related factors associated with regional emergency department utilization. Popul Health Manag. 2020;23(6):430–437. doi:10.1089/pop.2019.0161
26. Fouayzi H, Ash AS. High-frequency hospital users: the tail that wags the readmissions dog. Health Serv Res; 2021;57(3):579–586.
27. O’Hare T, Sherrer M. Subjective distress associated with sudden loss in clients with severe mental illness. Community Ment Health J. 2011;47(6):646–653. doi:10.1007/s10597-011-9382-0
28. O’Hare T, Sherrer MV, Shen C. Sudden losses and negative appraisal in people with severe mental illness. Am J Orthopsychiatry. 2014;84(6):664–673. doi:10.1037/ort0000014
29. Caparrós B, Masferrer L. Coping strategies and complicated grief in a substance use disorder sample. Front Psychol. 2020;11:624065. doi:10.3389/fpsyg.2020.624065
30. Cai H, Jin Y, Liu S, et al. Prevalence of suicidal ideation and planning in patients with major depressive disorder: a meta-analysis of observation studies. J Affect Dis. 2021;293:148–158. doi:10.1016/j.jad.2021.05.115
31. Carmassi C, Bertelloni CA, Dell’Oste V, et al. Post-traumatic stress burden in a sample of hospitalized patients with bipolar disorder: which impact on clinical correlates and suicidal risk? J Affect Disord. 2020;262:267–272. doi:10.1016/j.jad.2019.10.044
32. Chwastiak LA, Davydow DS, McKibbin CL, et al. The effect of serious mental illness on the risk of rehospitalization among patients with diabetes. Psychosomatics. 2014;55(2):134–143. doi:10.1016/j.psym.2013.08.012
33. Edgcomb JB, Shaddox T, Hellemann G, Brooks JO
34. Germack HD, Noor-E-Alam M, Wang X, Hanrahan N. Association of comorbid serious mental illness diagnosis with 30-Day medical and surgical readmissions. JAMA Psychiatry. 2019;76(1):96–98. doi:10.1001/jamapsychiatry.2018.3091
35. Ribe AR, Laursen TM, Sandbaek A, Charles M, Nordentoft M, Vestergaard M. Long-term mortality of persons with severe mental illness and diabetes: a population-based cohort study in Denmark. Psychol Med. 2014;44(14):3097–3107. doi:10.1017/S0033291714000634
36. Schmidt M, Pedersen L, Sørensen HT. The Danish civil registration system as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
37. Helweg-Larsen K. The Danish register of causes of death. Scand J Public Health. 2011;39(7 Suppl):26–29. doi:10.1177/1403494811399958
38. Andersen JS, Olivarius Nde F, Krasnik A. The Danish National Health Service Register. Scand J Public Health. 2011;39(7 Suppl):34–37. doi:10.1177/1403494810394718
39. Lynge E, Sandegaard JL, Rebolj M. The Danish national patient register. Scand J Public Health. 2011;39(7 Suppl):30–33. doi:10.1177/1403494811401482
40. Baadsgaard M, Quitzau J. Danish registers on personal income and transfer payments. Scand J Public Health. 2011;39(7 Suppl):103–105. doi:10.1177/1403494811405098
41. Jensen VM, Rasmussen AW. Danish education registers. Scand J Public Health. 2011;39(7 Suppl):91–94. doi:10.1177/1403494810394715
42. Mors O, Perto GP, Mortensen PB. The Danish psychiatric central research register. Scand J Public Health. 2011;39(7 Suppl):54–57. doi:10.1177/1403494810395825
43. Christiansen E, Larsen KJ, Agerbo E, Bilenberg N, Stenager E. Incidence and risk factors for suicide attempts in a general population of young people: a Danish register-based study. Aust N Z J Psychiatry. 2013;47(3):259–270. doi:10.1177/0004867412463737
44. Lundorff M, Holmgren H, Zachariae R, Farver-Vestergaard I, O’Connor M. Prevalence of prolonged grief disorder in adult bereavement: a systematic review and meta-analysis. J Affect Dis. 2017;212:138–149. doi:10.1016/j.jad.2017.01.030
45. O’Connor M, Nickerson A, Aderka IM, Bryant RA. The temporal relationship between change in symptoms of prolonged grief and posttraumatic stress following old age spousal bereavement. Depress Anxiety. 2015;32(5):335–340. doi:10.1002/da.22349
46. Erlangsen A, Mortensen PB, Vach W, Jeune B. Psychiatric hospitalisation and suicide among the very old in Denmark: population-based register study. Br J Psychiatry. 2005;187(1):43–48. doi:10.1192/bjp.187.1.43
47. Mortensen PB, Pedersen MG, Pedersen CB. Psychiatric family history and schizophrenia risk in Denmark: which mental disorders are relevant? Psychol Med. 2010;40(2):201–210. doi:10.1017/S0033291709990419
48. Qin P, Agerbo E, Mortensen PB. Suicide risk in relation to socioeconomic, demographic, psychiatric, and familial factors: a national register-based study of all suicides in Denmark, 1981–1997. Am J Psychiatry. 2003;160(4):765–772. doi:10.1176/appi.ajp.160.4.765
49. McHugo GJ, Drake RE, Xie H, Bond GR. A 10-year study of steady employment and non-vocational outcomes among people with serious mental illness and co-occurring substance use disorders. Schizophr Res. 2012;138(2–3):233–239. doi:10.1016/j.schres.2012.04.007
50. Walter F, Carr MJ, Mok PL, et al. Multiple adverse outcomes following first discharge from inpatient psychiatric care: a national cohort study. Lancet Psychiatry. 2019;6(7):582–589. doi:10.1016/S2215-0366(19)30180-4
51. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
52. Hanley JA, Negassa A, Edwardes MD, Forrester JE. Statistical analysis of correlated data using generalized estimating equations: an orientation. Am J Epidemiol. 2003;157(4):364–375. doi:10.1093/aje/kwf215
53. Feder KA, Heatherington L, Mojtabai R, Eaton WW. Perceived marital support and incident mental illness: evidence from the National Comorbidity Survey. J Marital Fam Ther. 2019;45(4):668–683. doi:10.1111/jmft.12343
54. Wang AG, Stórá T. Core features of suicide. Gender, age, alcohol and other putative risk factors in a low-incidence population. Nord J Psychiatry. 2009;63(2):154–159. doi:10.1080/08039480802429458
55. Chronister J, Fitzgerald S, Chou -C-C. The meaning of social support for persons with serious mental illness: a family member perspective. Rehab Psychol. 2021;66(1):87. doi:10.1037/rep0000369
56. Hanson JG. Families of people with a severe mental illness: role conflicts, ambiguity and family burden. J Sociol Soc Welfare. 1993;20:105.
57. Labrum T, Solomon P. Serious mental illness and incidents between adult children and parents responded to by police. Psychol Med. 2020;1–10. doi:10.1017/S0033291720001762
58. Labrum T, Zingman MA, Nossel I, Dixon L. Violence by persons with serious mental illness toward family caregivers and other relatives: a review. Harv Rev Psychiatry. 2021;29(1):10–19. doi:10.1097/HRP.0000000000000263
59. Fairman N, Irwin SA. A retrospective case series of suicide attempts leading to hospice admission. Palliat Support Care. 2013;11(3):273–276. doi:10.1017/S1478951513000096
60. Saha S, Chant D, McGrath J. A systematic review of mortality in schizophrenia: is the differential mortality gap worsening over time? Arch Gen Psychiatry. 2007;64(10):1123–1131. doi:10.1001/archpsyc.64.10.1123
61. Cullen BA, Mojtabai R, Bordbar E, Everett A, Nugent KL, Eaton WW. Social network, recovery attitudes and internal stigma among those with serious mental illness. Int J Soc Psychiatry. 2017;63(5):448–458. doi:10.1177/0020764017712302
62. Kilbourne AM, McCarthy JF, Post EP, Welsh D, Blow FC. Social support among veterans with serious mental illness. Soc Psychiatry Psychiatr Epidemiol. 2007;42(8):639–646. doi:10.1007/s00127-007-0212-1
63. Ganesh Kudva K, Abdin E, Vaingankar JA, et al. The relationship between suicidality and socio-demographic variables, physical disorders, and psychiatric disorders: results from the Singapore mental health study 2016. Int J Environ Res Public Health. 2021;18(8):4365. doi:10.3390/ijerph18084365
64. Merritt K, McGuire PK, Egerton A, et al. Association of age, antipsychotic medication, and symptom severity in schizophrenia With proton magnetic resonance spectroscopy brain glutamate level: a mega-analysis of individual participant-level data. JAMA Psychiatry. 2021;78(6):667–681. doi:10.1001/jamapsychiatry.2021.0380
65. Smilowitz S, Aftab A, Aebi M, Levin J, Tatsuoka C, Sajatovic M. Age-Related differences in medication adherence, symptoms, and stigma in poorly adherent adults with bipolar disorder. J Geriatr Psychiatry Neurol. 2020;33(5):250–255. doi:10.1177/0891988719874116
66. Parpouchi M, Moniruzzaman A, Buxton JA, Somers JM. Multivariable modelling of factors associated with criminal convictions among people experiencing homelessness and serious mental illness: a multi-year study. Sci Rep. 2021;11(1):16610. doi:10.1038/s41598-021-96186-x
67. Spivak S, Cullen B, Eaton WW, Rodriguez K, Mojtabai R. Financial hardship among individuals with serious mental illness. Psychiatry Res. 2019;282:112632. doi:10.1016/j.psychres.2019.112632
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.