Back to Journals » Infection and Drug Resistance » Volume 16
Sensorineural Hearing Loss in Patients with Long-COVID-19: Objective and Behavioral Audiometric Findings
Authors Dorobisz K ![]() , Pazdro-Zastawny K, Misiak P, Kruk-Krzemień A, Zatoński T
, Pazdro-Zastawny K, Misiak P, Kruk-Krzemień A, Zatoński T ![]()
Received 7 January 2023
Accepted for publication 28 February 2023
Published 31 March 2023 Volume 2023:16 Pages 1931—1939
DOI https://doi.org/10.2147/IDR.S398126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Karolina Dorobisz, Katarzyna Pazdro-Zastawny, Paula Misiak, Anna Kruk-Krzemień, Tomasz Zatoński
Department of Otolaryngology, Head and Neck Surgery, Wroclaw Medical University, Wrocław, Poland
Correspondence: Katarzyna Pazdro-Zastawny, Email [email protected]
Introduction: The symptoms of COVID-19 are primarily respiratory system disorders. Sensorineural hearing loss can be caused by COVID-19, as other symptoms in the nervous system. Hearing loss may also be the only symptom or complication of this disease or the symptoms of long COVID-19. The study aimed to assess hearing in patients after COVID-19 infection.
Material and Methods: The study conducted ENT and full hearing assessment in COVID-19 infection. All patients underwent complete audiological diagnostics, including threshold tonal audiometry, tympanometry, otoacoustic emissions, and auditory brainstem evoked potentials (ABR) tests. The study group included 58 patients aged 23 to 75 years who were diagnosed with COVID-19 infection six months before inclusion in the present study and reported post-COVID-19 hearing impairment.
Results: There were statistically significant differences between the control and study groups. Sensorineural hearing loss was found in 65.5% of the tonal audiometry test. The stapes reflex was absent in almost 20% of post-COVID-19 patients. The analysis of ABRs demonstrated longer latencies of wave III, V, and time intervals I–III, I–V in post-COVID-19 patients.
Conclusion: COVID-19 can damage the inner ear as well as the auditory pathway. Hearing loss may be the only symptom of COVID-19 or be a late complication of the disease due to postinfectious inflammation of the nerve tissue as a symptom of long COVID-19. Prolonged conduction of the auditory pathway shows the affinity of the virus to the nervous system as a symptom of long COVID. It is advisable to perform hearing diagnostics in patients after COVID-19 and provide them with specialist care.
Keywords: hearing loss, tinnitus, long COVID-19, SARS-CoV-2
Introduction
Coronavirus 2 (SARS-CoV-2) is a virus that has caused pandemic. In September 2022, more than 610 million cases were diagnosed.1 The pathophysiology of the disease includes viral infection of the upper and lower respiratory tract and an over-response of the immune system or autoimmunity.2 The symptoms vary,3 and most patients suffer from mild inflammation. The infection may lead to severe lung damage, acute respiratory distress syndrome (ARDS), and multi-organ failure.2 Long COVID-19 occurs more than four weeks after COVID-19 or reappears after a temporary improvement.4 The damaging effect of COVID-19 on the inner ear has been confirmed, but its pathogenesis and occurrence remain unclear.5 The virus can damage the organ of Corti, stria vascularis, and spiral ganglia,6 and COVID-19 was associated with sudden sensorineural hearing loss (SSNHL), which may be the sole or one of the symptoms of COVID-19.3
Diseases of the inner ear and hearing loss rarely affect young and middle-aged patients. Sensorineural hearing loss often affects the elderly, although this problem is often overlooked by patients and doctors. Hearing loss causes a significant reduction in the quality of life, and may also be one of the first symptoms of serious neurological diseases such as cerebral ischemic disease. SSNHL is usually caused by thromboembolism and also exposure to noise, ototoxic drugs, ear or head trauma, inflammatory diseases of the ear, or viral diseases.7 Many authors point to the problem of hearing impairment after COVID-19; however, according to the meta-analysis,8 there is no study that would accurately assess the inner ear after COVID-19. Most of the research is based on pure tone audiometry or speech audiometry, without the performance of objective tests- otoacoustic emission test and auditory brainstem evoked potentials test. In addition, it was analyzed whether vaccination against COVID-19 can cause sensorineural hearing loss.9 The impact of COVID-19 on cranial nerve palsy is also being considered.10 The aim of the study was to assess the impact of COVID-19 on the inner ear, especially sensorineural hearing loss and the damage in the auditory pathway, focusing on assessing only patients reporting hearing loss after COVID-19. The study also aimed to assess which part of the hearing organ was damaged, which frequencies it concerned, and how the signal transmission in the central nervous system changed.
Materials and Methods
Control Group
The control group consisted of 60 healthy patients aged 38 to 69 years. People classified in this group did not report any middle ear disease, hearing impairment, dizziness or balance disorders; otolaryngological examination showed no pathology; otoscopic examination showed normal eardrums. Patients from the control group have never had a test-confirmed COVID-19.
Study Group
The study group included 58 patients aged 23 to 75 years (mean 48) who had had COVID-19 disease up to 6 months before, as confirmed by the COVID-19 real-time polymerase reaction test- these were patients with confirmed long COVID-19. Women constituted the majority of the respondents (56.9%). These patients came to the audiology clinic or the emergency room, directed by a general practitioner. These patients contracted COVID-19 six months before and reported persistent hearing and balance disorders afterward.
The inclusion criteria were patients with hearing loss or tinnitus, at least 18 years of age, recovered from a mild to moderate COVID-19 infection confirmed by a positive polymerase chain reaction (PCR) test, and referred to an audiology clinic or acute medical emergency.
The exclusion criteria were patients with prior otological or neurological problems, hospitalized for COVID-19, presence of hearing loss or dizziness prior to COVID-19, coexisting mental, cardiovascular or circulatory diseases, those with a history of cranial trauma, meningitis, and patients taking ototoxic drugs. One patient with a history of hospitalization in the intensive care unit was excluded from the study.
The study was approved by the bioethical committee of Wroclaw Medical University, Poland, 1036/2021. The study was conducted in accordance with the Declaration of Helsinki, and all participants were informed about the purpose of the study and gave their written consent.
The medical history covered the current disease, chronic diseases and past diseases, with particular emphasis on the pathology of the middle and inner ear, as well as conditions that may affect the sense of hearing, as well as disorders of taste, smell, and vision. Hearing damage risk factors, such as exposure to noise at work and the use of ototoxic drugs, were also assessed. Each patient underwent an otolaryngological examination. A hearing was assessed by tonal threshold audiometry, tympanometry, otoacoustic emission, and auditory brainstem evoked potentials test (BERA). The severity of hearing impairment in tonal threshold audiometry was classified according to the British Society of Audiology as 20–40 dB-mild, 41–70 dB moderate, 71–95dB severe and above 95dB as profound sensorineural hearing loss.11 Only patients with type A tympanometry results were included in the study after the exclusion of conductive hearing loss. During the study stapedius reflexes were assessed, the frequencies used to trigger the reflex were 500Hz, 100Hz, 2000Hz and 4000Hz. Acoustic reflex measurements provide information about the function of the middle and inner ear, vestibulocochlear and facial nerve function, as well as brainstem function. The normal reflex threshold was considered to be 70–100 dB HL of pure tone. In the otoacoustic emission study, transient-evoked otoacoustic emission (TEOAE) and distortion product otoacoustic emission (DPOAE) were used. Otoacoustic emissions testing evaluates the response of the cochlea to a tonal pulse or click given by the probe. The test detects sensorineural hearing loss of cochlear origin. Signal-to-noise ratio (SNR) above 6dB was considered normal. The following standards were adopted in the BERA study, that norms have been standardized in the laboratory:
- wave I- <1.9 ms latency,
- V- wave latency <6.2 ms
- interval I-III- <2.6 ms,
- interval III-V- <2.4 ms,
- I–V interval- <4.6 ms,
- interaural difference in interval values - <0.2 ms,
- interaural difference in wave latency V- <0.4 ms,
Statistical Analysis
The STATISTICA v. 13.3 program (TIBCO Software Inc., Palo Alto, Ca, USA) was used to perform the statistical analysis.
The consistency of the distributions of quantitative parameters with the normal distribution was verified using the Shapiro–Wilk test. P <0.05 was adopted as the critical level of significance. Depending on the distribution, quantitative variables are presented in tables and graphs as means (M) and standard deviations (SD) or medians (Me) and lower (Q1) and upper (Q3) quartiles. The significance of differences in average values in two groups for parameters with a distribution significantly different from the normal or with heterogeneous variances was checked using the Mann–Whitney test.
For qualitative variables (nominal and ordinal), the counts (n) and proportions (%) were calculated and presented in the contingency tables (multi-way). The independence of the two variables was verified using the Pearson chi-square test or Fisher’s exact test. In the case of four-field tables, the values of the odds ratios and their 95% confidence intervals were additionally estimated.
Single- and multi-factor logistic regression was used to describe the relationship between the values of the explanatory variables (risk factors) and the probability of exceeding the norms of air and bone conduction and the norm of the threshold of hearing in tonal audiometry. The cut-off values for continuous variables were determined after the analysis of the ROC curves. P <0.05 was assumed as significant in all statistical tests.
Results
Medical History Analysis
Study Group
In the study group, 50% of patients reported hearing loss, while tinnitus occurred in 77% of patients, including unilateral in 43.1% of patients, and bilateral in 32.8% of patients. Smell disturbances were noticed by 10 patients (17.2%), and taste disturbances by 8 (13.8%). As many as 20 patients reported visual disturbances, which constituted 34.5% of patients.
People in the control group had no history of middle or inner ear diseases, hearing loss, tinnitus, dizziness or balance disorders. No abnormalities were found in the ENT examination. The tympanic membrane was normal in all patients in the control group.
Analysis of the results of Tonal Threshold Audiometry
In 38 patients, sensorineural hearing loss was found in the pure tone audiometry, which constitutes 65.5% of patients in the study group. For the frequency of 250Hz, mild sensorineural hearing loss was found in 15% on the left side to 17% on the right side in patients with long COVID-19. For the frequency of 500Hz, mild sensorineural hearing loss was found in 24% of patients on the right side and in 27% of patients on the left side, and moderate sensorineural hearing loss was found in 5% of patients on the right side. On the left side, for the frequency of 500Hz, in the group of patients with long COVID-19, 5% were also diagnosed with profound sensorineural hearing loss. For the frequency of 1000Hz in the study group, mild sensorineural hearing loss was found in about 20% of patients. Moderate or severe sensorineural hearing loss for this frequency was reported in 3–5% of patients. For the frequency of 2000 Hz, mild sensorineural hearing loss was found in 15–20% of patients, moderate sensorineural hearing loss in 5–8%. Severe or profound sensorineural hearing loss at 2000Hz was reported in a total of 10% of patients. Mild sensorineural hearing loss for the frequency of 4000Hz was found on the right side in 15.5% of patients from the study group and in 19% of patients on the left side. Moderate sensorineural hearing loss for 4000 Hz in the right ear was found in 10% and in the left ear in 14% of patients with long COVID-19. Severe sensorineural hearing loss at 4000 Hz was observed in 7% of patients on the right side and in 3.4% on the left side. Profound sensorineural hearing loss was found in 7% of long-term COVID-19 patients. Mild sensorineural hearing loss for 6000Hz was found in 12–13% of patients, similarly to moderate sensorineural hearing loss. Severe sensorineural hearing loss for 6000Hz occurred in 3.4% of long-COVID-19 patients. Profound sensorineural hearing loss at 6000Hz on the left side occurred in 8.5% of patients and in 1.7% of patients on the right side. However, for the highest frequency - 8000Hz, mild sensorineural hearing loss occurred in 21% of patients from the study group on the right side and in 12% on the left side. Moderate sensorineural hearing loss for 8000Hz on the right side was present in 10% of patients and in 19% of patients on the left side. Severe sensorineural hearing loss for 8000Hz concerned 5–6% of patients. Profound sensorineural hearing loss at 6000 Hz occurred in 3% of patients on the right side and in 10% on the left side. Patients from the study group were diagnosed mainly as mild or moderate sensorineural hearing loss, hearing disorders more often concerned medium and higher frequencies (Table 1). In the control group, on the other hand, one patient had mild hearing loss. The differences between the study group and the control group were statistically significant. In the multivariate logistic regression analysis, it was found that the factors influencing the increased risk of exceeding the norm in the pure tone audiometry test are COVID-19.
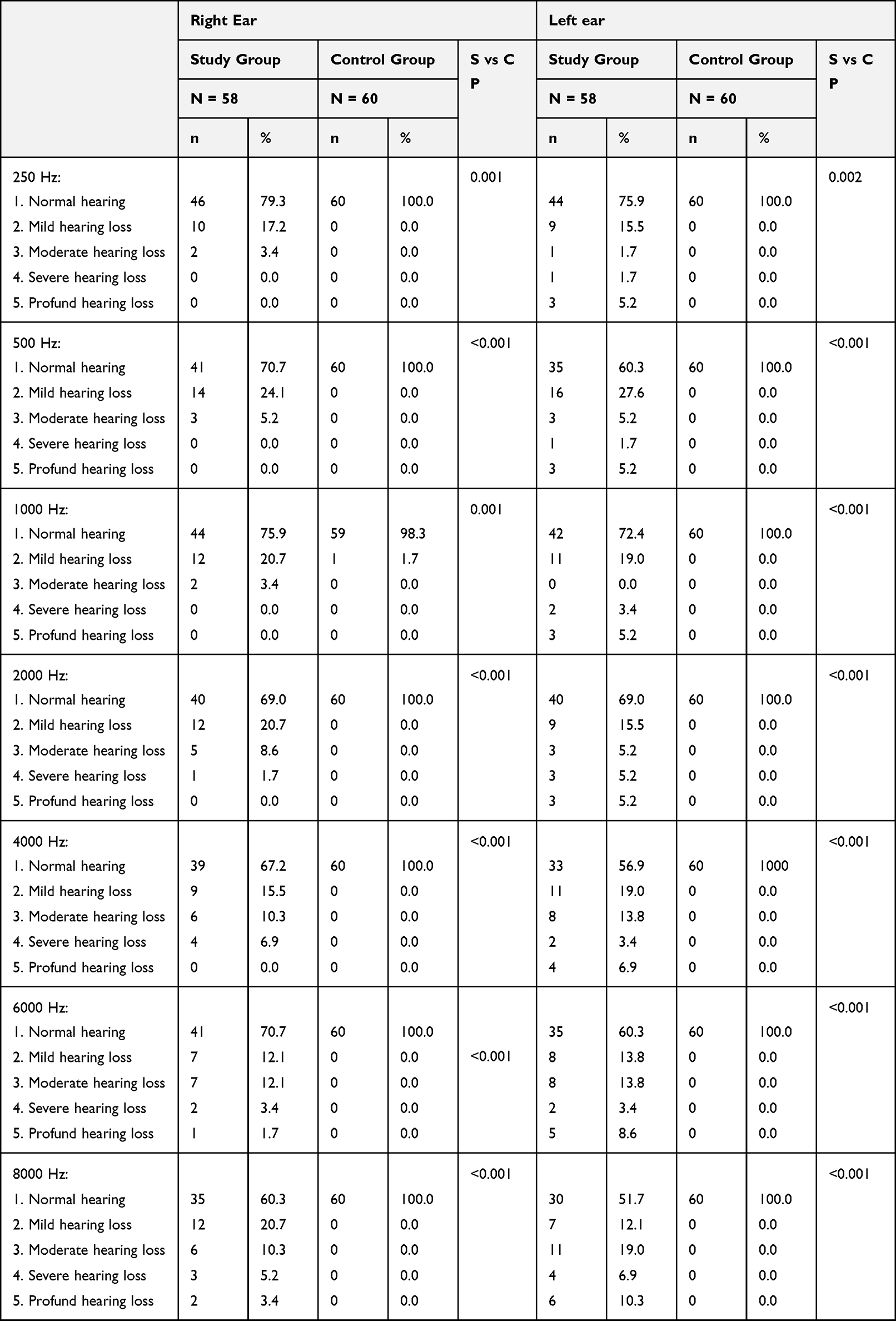 |
Table 1 Evaluation of the Pure Tone Threshold Audiometry Test |
The chance of exceeding the norm at any frequency in the pure tone audiometry test by a person who suffered from COVID-19 is over sixty times higher compared to a healthy person who did not suffer from COVID-19 (OR = 63.2).
Analysis of Tympanometry results with the Study of the Stapes Reflex
In all the patients in the study and control groups, the tympanometry curves were normal - type A. However, the group studied statistically significantly (p <0.05) more often showed the lack of stapes reflexes compared to the control group. The stapedius muscle reflex was present in 80% of the patients in the study group, compared to the control group, where the stapedius muscle reflex was recorded in all patients. These data are presented in Table 2.
 |
Table 2 Assessment of the Stapes Reflex |
Analysis of Otoacoustic Emission Test Results- TEOAE and DPOAE
The response in the otoacoustic emission study was compared between the control group and the study group. All patients from the study group obtained the correct result. In the study group, almost 40% did not receive an answer. 13% did not register responses unilaterally, while 25% - both sides. These data are presented in Table 3.
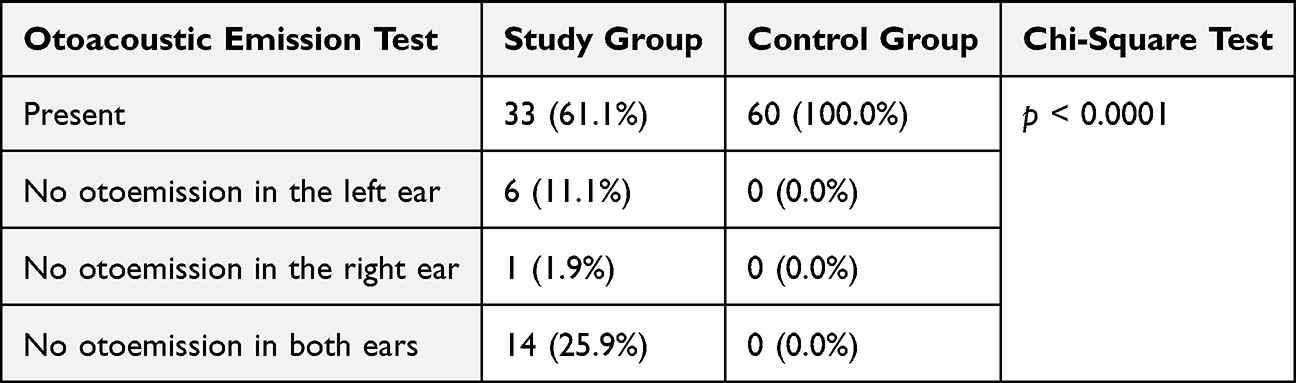 |
Table 3 Results of Otoacoustic Emission Test |
Analysis of Auditory Brainstem Evoked Potential Results
BERA scores were compared between the test group and the control group. The latency of wave III, V and time intervals I–III, I–V was statistically significantly longer in patients after COVID 9 (Table 4). An analysis was then performed to compare the number of normal and abnormal results in the test group versus the control group. Patients after COVID-19 disease obtained abnormal results significantly more often, especially wave I, I–III and I–V latencies were significantly (p <0.05) abnormal more often compared to the results of patients in the control group (Table 5 and Table 6).
 |
Table 4 Results of the Examination of Auditory Brainstem Evoked Potentials in the Test (S) and Control (C) Groups and the Results of the Mann–Whitney Significance Tests |
 |
Table 5 Results of the Auditory Brainstem Evoked Potentials. |
 |
Table 6 Results of the Auditory Brainstem Evoked Potentials- comparison of the left and right sides. |
Discussion
The patients in the study were 6 months after COVID-19, even if they had conductive hearing loss during the course of the disease. It is noteworthy that despite frequent complaints of the Eustachian tube problems in the course of COVID-19, the tympanometry results were normal in all patients, which confirms the absence of conductive hearing loss components in the discussed patients, and confirms the significant effect of the virus on the nervous system and the inner ear.
Many authors have shown that COVID-19 can lead to ENT disorders. ENT symptoms are known in COVID-19, but little information is available about damage to the hearing organ. Osman Kilic et al12 indicated in their publication the relationship between hearing loss and COVID-19. SSNHL after COVID-19 is mainly reported in the form of case reports. Fance et al13 confirmed hearing loss in 40.5% of patients after COVID-19, diagnosing one-sided or bilateral sensorineural hearing loss. In the discussed publication, sensorineural hearing loss was confirmed in 65.5%, also confirming unilateral or bilateral hearing loss. However, one-sided changes were more frequent, as in other publications.12,14–16 Bilateral hearing loss may be caused by the harmful effects of COVID-19 on the outer hair cells of the cochlea.17 On the other hand, in another study evaluating hearing in long COVID-19 patients, air conduction thresholds showed a typical threshold for the average age of the subjects.18 This study shows that tinnitus and vertigo are significantly more common than hearing loss in long COVID-19.18
In addition, it was analyzed whether vaccination against COVID-19 can cause sensorineural hearing loss.9 The impact of COVID-19 on cranial nerve palsy is also being considered.10
The evaluation of the otoacoustic emissions after COVID-19 infection shows that the absence of symptoms does not guarantee the proper function of the cochlea.17 The reduced amplitude of the Transient evoked otoacoustic emissions (TEOAEs) shows the significant effect of the virus on the outer hair cells.17 In our work, we also confirmed the damage to the cochlea in the otoacoustic emission test. Other authors have also confirmed cochlea damage as a possible complication of COVID-19.19 On the other hand, the work of Mostafa et al20 showed that COVID-19 most likely has no effect on the hearing of a newborn baby whose mother underwent COVID-19 while pregnant.
The cochlea is usually damaged secondary to viral infection,21 but it should be remembered that it may involve the auditory pathway,22 which was confirmed in the discussed study. Some authors noticed a statistically significant difference in hearing high frequencies between the study and control groups.17 Hearing loss in the discussed study concerned high frequencies more often and to a greater extent, but low and medium frequency hearing loss was also diagnosed, similar relationships were noticed by other researchers.17 On the other hand, other authors noticed significant differences only for the 1000 Hz frequency in patients after the COVID-19 group, compared to the control group.23 Mustafa et al17 showed a significant worsening of TEAOAE in patients with asymptomatic COVID-19. In the discussed study, the patients also had an asymptomatic course of COVID-19, which indicates a high risk of neurotrophic complications after the infection.
Many authors emphasize the important role of endothelium dysfunction and microthrombosis in the pathogenesis of hearing loss.24 COVID-19 can damage various organs by binding to the ACE 2 receptor, including the cochlea, the auditory nerve and the central nervous system.25 It has been proven that the process of deoxygenation of erythrocytes by COVID-19 leads to hypoxia and further damage to the inner ear. However, according to Delgado-Roche et al26 during COVID-19, the immune system is activated, which causes the destruction of cells and tissues. Cashman et al27 consider that the main cause of hearing loss caused by viral infection is inflammation of the auditory nerve and perineural tissue. An important role in the inflammatory process is played by oxidative stress causing the production of ROS-reactive oxygen species in cells and tissues, which can damage cells. ROS stimulate inflammatory processes, stimulating the secretion of IL-6, IL-1beta and TNF-alpha. Both of these processes have been described in the course of COVID-19.
It has also been confirmed that ROS and pro-inflammatory cytokines are involved in the course of SSHL and tinnitus. There is also a cytokine storm in COVID-19 that can affect postinfectious inflammation of neuronal tissue.
The BAEP test may show the effect of COVID-19 on brainstem. In our study, the extension of auditory conduction time of brainstem evoked potentials confirms the thesis about postinfectious nerve damage. In the study by Gedik et all,28 no significant differences were noticed in this test, but the latencies of waves I, III and V were prolonged in the study group. Ozturk et all noted a similar relationship.29
The fact that there are abnormal stapedius reflex also supports this hypothesis.
Umesawa et al30 indicate that idiopathic SSNHL is more common in smokers. On the other hand, Nasser et al31 indicate that smoking is not related to COVID-19 and its ENT complications. In the discussed study, most of the patients were non-smokers, which shows that smoking was not really affected, and confirmed that the virus had a strong influence on hearing.
The risk of hearing impairment after vaccination against COVID-19 has also been shown, as well as after other vaccinations, such as against the flu virus or diphtheria virus.32 This hypothesis may support the supposition that COVID-19 damages the hearing organ.
Ototoxicity used in the treatment of remdesivir, ribavir, chloroquine and hydroxychloroquine plays an important role in the pathogenesis of hearing loss after COVID-19, but patients were not subjected to this treatment in this study.
Limitations
The study did not examine patients prior to COVID-19 infection, it was based only on the history of the normal function of the inner ear. The study included patients who had COVID-19 asymptomatically, it is worth comparing this group with patients who had symptoms. The lack of long-term follow-up of our patients does not allow us to assess the further course of the disease.
Conclusions
COVID-19 can damage to the inner ear as well as the auditory pathway. Hearing loss may be the only symptom of COVID-19 or be a late complication of the disease due to postinfectious inflammation of the nerve tissue as a symptom of long COVID-19. Prolonged conduction of the auditory pathway shows the affinity of the virus to the nervous system as a symptom of long COVID-19. It is advisable to perform hearing diagnostics in patients after COVID-19 and provide them with specialist care.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World Health Organization. COVID-19 pandemic. Available from: https://www.who.int.
2. Dorobisz K, Dorobisz T, Janczak D, Zatoński T. Doxycycline in the coronavirus disease 2019 therapy. Ther Clin Risk Manag. 2021;17:1023–1026. doi:10.2147/TCRM.S314923
3. Yaseen NK, Al-Ani RM, Ali Rashid R. COVID-19-related sudden sensorineural hearing loss. Qatar Med J. 2021;2021(3):58. PMID: 34745911. doi:10.5339/qmj.2021.58
4. Alwan NA, Johnson L. Defining long COVID: going back to the start. Med. 2021;2:501–504. doi:10.1016/j.medj.2021.03.003
5. Chirakkal P, Al Hail AN, Zada N, Vijayakumar DS. COVID-19 and Tinnitus. Ear Nose Throat J. 2021;100(2_suppl):160S–162S. PMID: 33275033. doi:10.1177/0145561320974849
6. Abramovich S, Prasher DK. Electrocochleography and brainstem potentials in Ramsay hunt syndrome. Arch Otolaryngol Head Neck Surg. 1986;112(9):925–928. doi:10.1001/archotol.1986.03780090021002
7. Gerstacker K, Speck I, Riemann S, Aschendorff A, Knopf A, Arndt S. Deafness after COVID-19? HNO. 2021;69:1–4. doi:10.1007/s00106-021-01041-0
8. Jafari Z, Kolb BE, Mohajerani MH. Hearing loss, tinnitus, and dizziness in COVID-19: a systematic review and meta-analysis. Can J Neurol Sci. 2022;49(2):184–195. doi:10.1017/cjn.2021.63
9. Tsetsos N, Poutoglidis A, Vlachtsis K, Kilmpasanis A, Gougousis S. Sudden sensorineural hearing loss following the second dose of COVID-19 vaccine. Cureus. 2021;13(8):e17435. doi:10.7759/cureus.17435
10. Poutoglidis A, Tsetsos N, Karamitsou P, et al. Bilateral vocal fold palsy following COVID-19 infection. Ear Nose Throat J. 2022;2022:01455613221080987.
11. Audiology BS of. Descriptors for pure-tone audiograms. Br J Audiol. 1988;22:2.
12. Kilic O, Kalcioglu MT, Cag Y, et al. Could sudden sensorineural hearing loss be the sole manifestation of COVID-19? An investigation into SARS-COV-2 in the etiology of sudden sensorineural hearing loss. Int J Infect Dis. 2020;97:208–211. doi:10.1016/j.ijid.2020.06.023
13. Dusan M, Milan S, Nikola D. COVID-19 caused hearing loss. Eur Arch Otorhinolaryngol. 2022;279(5):2363–2372. PMID: 34235578; PMCID: PMC8263317. doi:10.1007/s00405-021-06951-x
14. Koumpa FS, Forde CT, Manjaly JG. Sudden irreversible hearing loss post COVID-19. BMJ Case Reports CP. 2020;13(11):e238419. doi:10.1136/bcr-2020-238419
15. Karimi-Galougahi M, Naeini AS, Raad N, Mikaniki N, Ghorbani J. Vertigo and hearing loss during the COVID19 pandemic–is there an association? Acta Otorhinolaryngol Ital. 2020;40(6):463. doi:10.14639/0392-100X-N0820
16. Swain SK, Das S, Lenka S. Sudden Sensorineural hearing loss among covid-19 patients-our experiences at an Indian teaching hospital. Siriraj Med J. 2021;73(2):77–83. doi:10.33192/Smj.2021.11
17. Mustafa MWM. Audiological profile of asymptomatic Covid-19 PCR-positive cases. Am J Otolaryngol. 2020;41(3):102483. doi:10.1016/j.amjoto.2020.102483
18. Degen CV, Mikuteit M, Niewolik J, et al. Audiological profile of adult Long COVID patients. Am J Otolaryngol. 2022;43(5):103579. doi:10.1016/j.amjoto.2022.103579
19. Fancello V, Fancello G, Hatzopoulos S, et al. Sensorineural hearing loss post-COVID-19 infection: an update. Audiol Res. 2022;12:307–315. doi:10.3390/audiolres12030032
20. Mostafa BE, Mostafa A, Fiky LME, et al. Maternal COVID-19 and neonatal hearing loss: a multicentric survey. Eur Arch Otorhinolaryngol. 2022;279:3435–3438. doi:10.1007/s00405-021-07098-5
21. Cohen BE, Durstenfeld A, Roehm PC. Viral causes of hearing loss: a review for hearing health professionals. Trends Hear. 2014;18:1–17.
22. Jereb M, Lainscak M, Marin J, Popovic M. Herpes simplex virus infection limited to the brainstem. Wien Klin Wochenschr. 2005;117:495–499. doi:10.1007/s00508-005-0324-0
23. Kokten N, Celik S, Mutlu A, Pektas E, Icten S, Tayyar Kalcioglu M. Does COVID-19 have an impact on hearing? Acta Otolaryngol. 2022;142(1):48–51. doi:10.1080/00016489.2021.2020897
24. McFadyen JD, Stevens H, Peter K. The emerging threat of (micro)thrombosis in COVID-19 and Its therapeutic implications. Circ Res. 2020;127(4):571–587. doi:10.1161/CIRCRESAHA.120.317447
25. Harenberg J, Jonas JB, Trecca EMC. A liaison between sudden sensorineural hearing loss and SARS-CoV-2 infection. Thromb Haemost. 2020;120(9):1237–1239. doi:10.1055/s-0040-1714370
26. Delgado-Roche L, Mesta F. Oxidative stress as key player in severe acute respiratory syndrome coronavirus (SARS-CoV) infection. Arch Med Res. 2020;51(5):384–387. doi:10.1016/j.arcmed.2020.04.019
27. Cashman KA, Wilkinson ER, Zeng X, et al. Immune-mediated systemic vasculitis as the proposed cause of sudden onset sensorineural hearing loss following Lassa virus exposure in cynomolgus macaques. MBio. 2018;9(5):e01896–18. doi:10.1128/mBio.01896-18
28. Gedik O, Hüsam H, Bas¸oz M, Tas N, Aksoy F. The effect of coronavirus disease 2019 on the hearing system. J Laryngol Otol. 2021;135:810–814. doi:10.1017/S0022215121001961
29. Öztürk B, Kavruk H, Aykul A. Audiological findings in individuals diagnosed with COVID-19. Am J Otolaryngol. 2022;May-Jun;43(3):103428. doi:10.1016/j.amjoto.2022.103428
30. Umesawa M, Kobashi G, Kitoh R, et al. Relationships among drinking and smoking habits, history of diseases, body mass index and idiopathic sudden sensorineural hearing loss in Japanese patients. Acta Otolaryngol. 2017;137(sup565):S17–23. doi:10.1080/00016489.2017.1297898
31. Nasser AMA, Geng Y, Al-Wesabi SA. The prevalence of smoking (cigarette and waterpipe) among university students in some Arab countries: a systematic review. Asian Pacific J Cancer Prev APJCP. 2020;21(3):583. doi:10.31557/APJCP.2020.21.3.583
32. Jeong J, Choi HS. Sudden sensorineural hearing loss after COVID-19 vaccination. Int J Infect Dis. 2021;113:341–343. doi:10.1016/j.ijid.2021.10.025
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
Comparison of the Diagnostic Performance of a Rapid Antigen Test with Real-Time Polymerase Chain Reaction for Detection of SARS-CoV-2 Among Patients Diagnosed with COVID-19 at Selected Hospitals in Addis Ababa, Ethiopia
Desalegn Z, Sebre S, Yohannes M, Seman A, Shiferaw W, Ademe M, Biazin H, Firdawoke E, Asemamaw Y, Teka B, Teshome S, Amogne W, Addissie A, Gebrehiwot Y, Kantelhardt E, Abebe T
Infection and Drug Resistance 2022, 15:4299-4305
Published Date: 6 August 2022
A Pilot Study of 0.4% Povidone-Iodine Nasal Spray to Eradicate SARS-CoV-2 in the Nasopharynx
Sirijatuphat R, Leelarasamee A, Puangpet T, Thitithanyanont A
Infection and Drug Resistance 2022, 15:7529-7536
Published Date: 21 December 2022
Distinct Features of Vascular Diseases in COVID-19
Ceasovschih A, Sorodoc V, Shor A, Haliga RE, Roth L, Lionte C, Onofrei Aursulesei V, Sirbu O, Culis N, Shapieva A, Tahir Khokhar MA, Statescu C, Sascau RA, Coman AE, Stoica A, Grigorescu ED, Banach M, Thomopoulos C, Sorodoc L
Journal of Inflammation Research 2023, 16:2783-2800
Published Date: 6 July 2023
Re-Emerging COVID-19: Controversy of Its Zoonotic Origin, Risks of Severity of Reinfection and Management
Chala B, Tilaye T, Waktole G
International Journal of General Medicine 2023, 16:4307-4319
Published Date: 20 September 2023