Back to Journals » Infection and Drug Resistance » Volume 12
Sensitivity Pattern Of Salmonella typhi And Paratyphi A Isolates To Chloramphenicol And Other Anti-Typhoid Drugs: An In Vitro Study
Received 8 February 2019
Accepted for publication 7 June 2019
Published 14 October 2019 Volume 2019:12 Pages 3217—3225
DOI https://doi.org/10.2147/IDR.S204618
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Eric Nulens
Niranjan Patil, Prashant Mule
Microbiology and Molecular Biology Department, Metropolis Healthcare Limited, Mumbai, India
Correspondence: Niranjan Patil
Metropolis Healthcare Limited, Mumbai, India
Tel +91 8452815696
Email [email protected]
Purpose: To investigate the antimicrobial sensitivity pattern of commonly prescribed antimicrobials (chloramphenicol, cefixime, ofloxacin, azithromycin, and ceftriaxone) against Salmonella enterica isolates.
Methods: Blood culture positive isolates of S. typhi and S. paratyphi A (N = 251) received at Metropolis Healthcare Limited (Mumbai, India) from four zones of India (North, South, West, and East) between April and August 2018 were tested for antimicrobial susceptibility by E-test method. Based on the minimum inhibitory concentration (MIC), the organism was categorized as sensitive, intermediate, and resistant against the respective antibiotics as per Clinical and Laboratory Standards Institute criteria 2018.
Results: Out of 251 Salmonella isolates, 192 (76.5%) were S. typhi and 59 (23.5%) were S. paratyphi A. All 251 (100%) Salmonella isolates were sensitive to cefixime, ceftriaxone, and azithromycin; 237/251 (94.4%) isolates to chloramphenicol and only 9/251 (3.6%) isolates were sensitive to ofloxacin. Based on average MIC and MIC breakpoints, Salmonella isolates were found to be sensitive to chloramphenicol (MIC: 3.89±6.94 μg/mL), cefixime (MIC: 0.13±0.11 μg/mL), azithromycin (MIC: 3.32±2.19 μg/mL), and ceftriaxone (MIC: 0.11±0.18 μg/mL) and resistant to ofloxacin (MIC: 2.95±6.06 μg/mL). More than 20% of Salmonella isolates had MICs of chloramphenicol as 1.5 μg/mL (27.85% isolates) and 2 μg/mL (29.53% isolates).
Conclusion: Our study confirms the re‑emergence of susceptibility of Salmonella isolates to chloramphenicol. Further, the concern about fluoroquinolone-decreased susceptibility as indicated by the intermediate susceptibility or resistance was reiterated in this study. Though cefixime, azithromycin, and ceftriaxone showed susceptibility, the possibility of antibiotic resistance with the irrational use of these antibiotics cannot be deterred. This study thus emphasizes the need for continuous evaluation and judicious use of antimicrobials, considering the ever-changing landscape.
Keywords: antimicrobial susceptibility, chloramphenicol, Etest, minimum inhibitory concentration, Salmonella
Introduction
Enteric fever, a systemic infection caused by Salmonella typhi (S. typhi) and Salmonella paratyphi (S. paratyphi), is a major persistent global health problem and is predominantly reported in the developing countries.1 The most common risk factors are contaminated drinking water or food with faeces from either acutely infected persons, persistent excretors, or chronic asymptomatic carriers, poor sanitation, inadequate hygiene practices, and low socio-economic status.2 About 22 million new cases of enteric fever with 200,000 mortality cases per year have been reported worldwide.3
Enteric fever is the major public health problem in the Indian subcontinent as well.4,5 S. typhi and S. paratyphi A are the predominant organisms involved in enteric fever in India.6 Prompt and effective antimicrobial therapy is the mainstay in the management of enteric fever to preclude the cases of morbidity and mortality. The illness may last for 3–4 weeks without therapy, and the case-fatality rates may be as high as 30%, but with appropriate treatment, clinical symptoms are subsided within a few days, fever recedes within 5 days, and mortality rates are reduced to <1%.7 But the indiscriminate use and predominantly misuse of the antimicrobials have resulted in the emergence of multidrug-resistant strains.
Chloramphenicol was referred to as the gold standard of therapy since its introduction in 1948.8 However, sporadic resistance to chloramphenicol was reported in Britain in 1950, probably due to its overuse. In May 1972, an outbreak of chloramphenicol-resistant S. typhi was reported in Kerala (India) where 54% of the isolates were found to be resistant to chloramphenicol in vitro.9 In 1989, there was a rapid emergence and spread of multidrug-resistant S. typhi (resistant to ampicillin, chloramphenicol, and trimethoprim sulfamethoxazole) in several parts of India.10 In 1990, multidrug-resistant S. typhi isolates were reported from Mumbai and New Delhi.11,12 By the end of the 1990s, Salmonella enterica developed resistance simultaneously to all first-line drugs like chloramphenicol, cotrimoxazole, and ampicillin.13,14 In 1992, 40 out of 51 S. typhi isolates were multidrug-resistant, including chloramphenicol in Calcutta15 followed by Bangalore in 1995,16 Hubli in 1997,14 and Hyderabad14 and Karnataka in 1999.17
In addition to India, chloramphenicol-resistant S. typhi isolates were reported from Vietnam,18,19 South Korea,20 and Bangladesh.21 Resistance to chloramphenicol may be attributed to the acquisition of drug resistance genes on plasmids, which encodes an enzyme that inactivates or modifies the drugs. One such example of chloramphenicol-resistant gene carried on plasmids is chloramphenicol acetyltransferase type 1, which codes for an enzyme that inactivates chloramphenicol via acetylation of 2 hydroxyl groups of chloramphenicol.22 With the emergence of chloramphenicol-resistant Salmonella isolates, fluoroquinolones (eg: ciprofloxacin and ofloxacin) emerged as the drug of choice for the treatment of typhoid, owing to the oral mode of administration and cost-effectiveness.23,24 But uncontrolled use of quinolones resulted in increased resistance against them, especially ciprofloxacin, which in turn may be due to sequential mutations in genes (gyr A, gyr B, and par C, par E) encoding DNA gyrase and topoisomerase IV or enhanced active efflux mechanisms.8,10,25 Increased resistance to fluoroquinolone led to increased use of third-generation cephalosporins (eg: ceftriaxone, cefotaxime, cefixime) and azithromycin in South Asia.26 However, discontinuation/reduction of chloramphenicol use and the use of other drugs for the treatment of enteric fever resulted in roll back to sensitivity against chloramphenicol.27,28 This re-emergence of chloramphenicol-sensitivity may be possibly due to loss of plasmids encoding resistance to chloramphenicol and other first-line drugs like ampicillin, co-trimoxazole or due to the emergence of susceptible isolates in the absence of drug pressure.
In this context of changing dynamics of resistance to antibiotics, it is imperative to have constant surveillance and antibiotic susceptibility data available to clinicians for appropriate management of the disease. The conventional method of antibiotic susceptibility testing by disc diffusion method is by far the commonest method of choice for the average laboratory for selection of appropriate antimicrobial drug. However, determination of minimum inhibitory concentration (MIC) of a suitable antibiotic either by broth dilution or E-test can be of a great help to estimate the proper therapeutic dose in drug-resistant situations. E-strip is a quantitative method for antimicrobial susceptibility testing and applies both the dilution of antibiotic and diffusion of antibiotic into the culture medium where a predefined stable antimicrobial gradient is present in a thin inert carrier strip. E-test method is considered as a fast, reliable, accurate, convenient, and a reproducible method with high specificity (33–96%), predictability (56–100%), and sensitivity (75–100%).29
The current study was undertaken to evaluate the antimicrobial susceptibility (based on MIC breakpoints) of chloramphenicol vis-à-vis other anti-typhoid drugs (cefixime, ofloxacin, azithromycin, and ceftriaxone) against Salmonella (including S. typhi and S. paratyphi A) isolates by E-test method. The data from this study would help to assess/understand if the sensitivity to chloramphenicol is still maintained among S. typhi and S. paratyphi A isolates.
Materials And Methods
Isolates
Two hundred and fifty-one isolates of S. typhi/S. paratyphi A obtained from clinically suspected cases of enteric fever across different zones (north, south, west, and east) of India between April and August 2018 at Metropolis Healthcare Limited (Mumbai, India) were evaluated for antimicrobial susceptibility testing. The institutional ethics committee (Ethics Committee of Ishwar Institute of Health Care, Aurangabad) approved the study protocol and other study-related documents. The study was conducted as per the approved study protocol.
Study Design
Four to five colonies of S. typhi/S. paratyphi A from 24-hrs-old grown culture were picked with an inoculating needle and suspended in 2 mL of 0.9% normal saline to give an opacity equivalent to 0.5 McFarland. The turbidity of the suspension was measured by McFarland Densitometer (Densimat Densitometer, Biomérieux Biotechnology). The inoculum was further diluted 1:10 times to give an adjusted concentration of 107 colony-forming units/mL. Within 15 min of adjusting the turbidity of inoculum suspension, the Mueller Hinton agar plates were swabbed by the inoculum, and the lid of a plate was left open for 5 min to allow absorption of any excess moisture before application of the E-test strips (HiMedia Laboratories Pvt Ltd, Mumbai, India). With the help of a sterile forceps, the E-test strips of chloramphenicol, ofloxacin, cefixime, ceftriaxone, and azithromycin were gently placed onto the inoculated plate, and the plates were further incubated at 35–37°C for 18–24 hrs. Following incubation, a symmetrical inhibition ellipse was produced, and the MIC was determined from the intersection of the lower part of the ellipse-shaped zone of inhibition with the value indicated on the E-test strip. Depending upon the zone of symmetrical inhibition ellipse, Salmonella isolates were categorized into three different categories – Sensitive (S), Intermediate (I), and Resistant (R) (Table 1).30
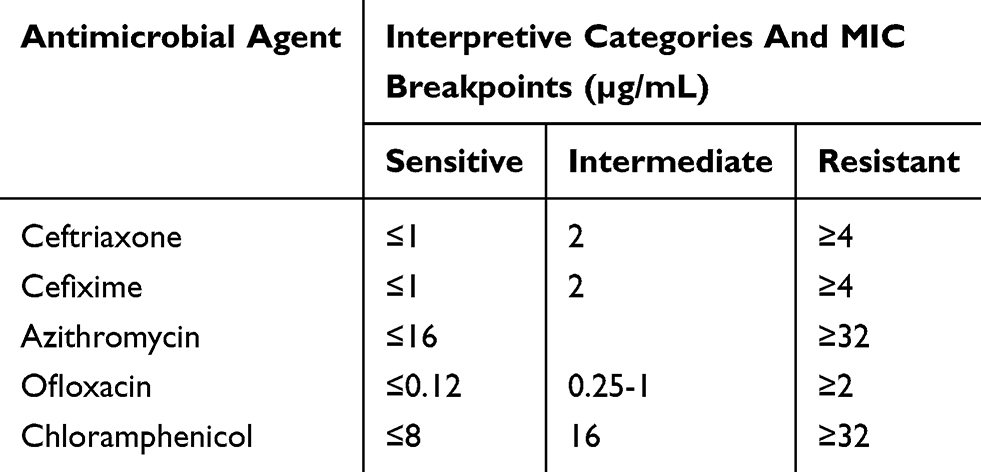 |
Table 1 Minimal Inhibitory Concentration Breakpoints For Salmonella Species (CLSI 2018) |
Study Outcomes
The primary outcome of interest was to compare the interpretive categories (S, I, and R) of Salmonella (including S. typhi and S. paratyphi A) isolates based on MIC breakpoints of chloramphenicol against other anti-typhoid drugs (cefixime, ofloxacin, azithromycin, and ceftriaxone). The secondary outcome was to evaluate the average MIC of all five anti-typhoid drugs against S. typhi and S. paratyphi A isolates.
Study Definitions
MIC: The MIC is the lowest concentration (in µg/mL) of an antibiotic that inhibits the growth of a given strain of bacteria.31,32
MIC Breakpoints: MIC breakpoint is defined as the MIC value, which is used to categorize the organism as S, I, and R.
Statistical Analyses
No formal sample size was calculated for this study. Descriptive statistics were used to analyze the study results. The Z statistic was used to test the primary hypothesis, “the proportion of sensitive isolates is same in chloramphenicol versus other antityphoid drugs” against the alternative hypothesis “not equal proportions between chloramphenicol versus other antityphoid drugs”. The statistical test was done at 5% level of significance. All the statistical analyses were performed using SAS software version 9.4.
Results
All 251 Salmonella (S. typhi: 192 [76.5%]; S. paratyphi A: 59 [23.5%]) isolates collected from different zones of the country (north: 76; south and east: 50 each; west: 75) (Figure 1) were tested for their susceptibility to five antibiotics.
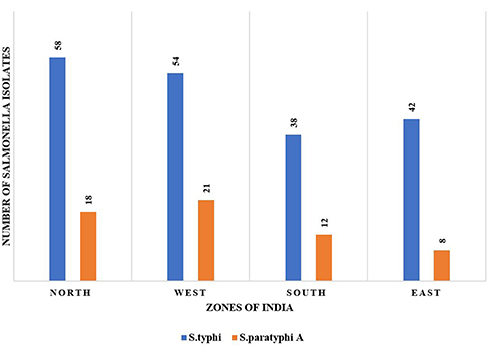 |
Figure 1 Zone-wise distribution of Salmonella isolates. |
Antimicrobial Susceptibility Testing
All (100%) Salmonella isolates were sensitive to cefixime, ceftriaxone, and azithromycin and 94.4% (237/251) of the isolates were significantly sensitive to chloramphenicol (p<0.0001; Z-test statistic). Significant reduced susceptibility to ofloxacin (3.6%; 09/251) was also observed (Table 2). The antibiotic sensitivity of Salmonella isolates was further studied by species (typhi and paratyphi A) across different zones of the country. All S. typhi and S. paratyphi A isolates were susceptible to azithromycin, cefixime, and ceftriaxone; 89.47% to 95.24% of S. typhi isolates and 100% of S. paratyphi A were susceptible to chloramphenicol. None of S. paratyphi A isolates were sensitive to ofloxacin (Table 3).
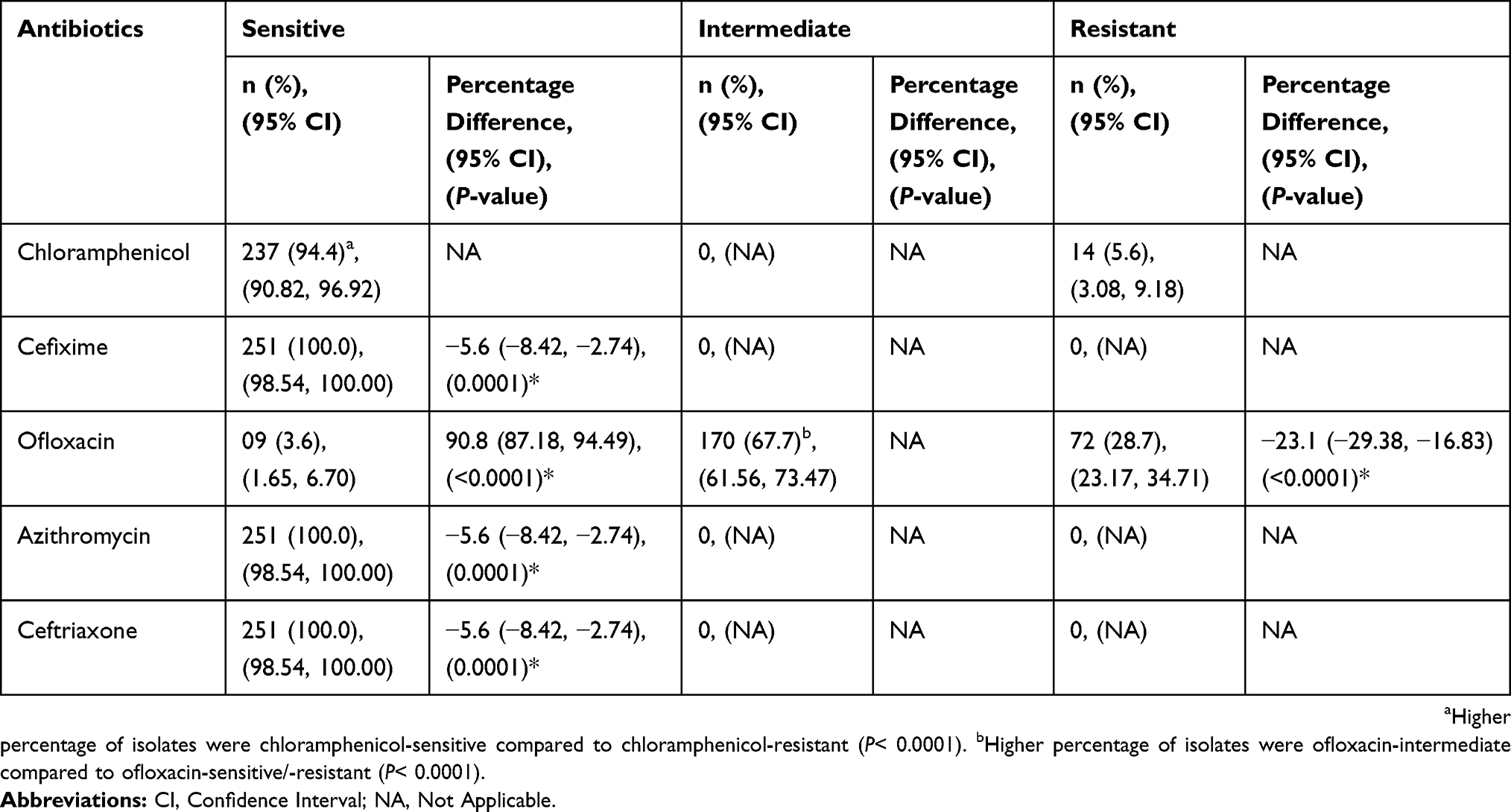 |
Table 2 Comparison Of Antibiotic Susceptibility Of Chloramphenicol Versus Other Anti-Typhoid Drugs In Salmonella Isolates |
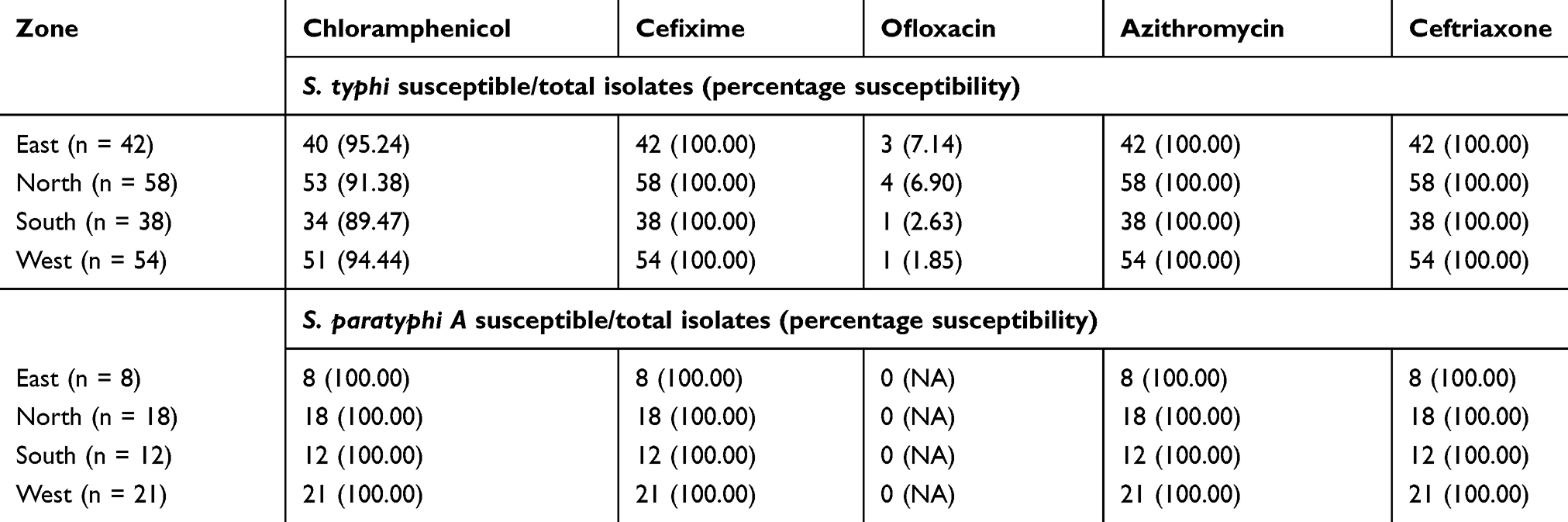 |
Table 3 Zone-Wise Susceptibility Analysis |
Minimal Inhibitory Concentration
Mean MIC of chloramphenicol (3.89±6.94 µg/mL), cefixime (0.13±0.11 µg/mL), azithromycin (3.32±2.19 µg/mL), and ceftriaxone (0.11±0.18 µg/mL) for all the isolates were in the susceptible range (as per MIC breakpoints). Mean MIC of ofloxacin (2.95±6.06 µg/mL) depicted organism resistance to ofloxacin (Table 4). More than 20% of Salmonella isolates had MICs of chloramphenicol as 1.5 µg/mL (27.85% isolates) and 2 µg/mL (29.53% isolates) (Figure 2).
 |
Table 4 Minimum Inhibitory Concentration (µg/mL) Of Anti-Typhoid Drugs |
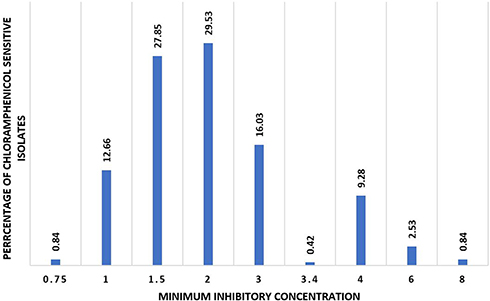 |
Figure 2 Percentage of chloramphenicol-sensitive isolates. |
Discussion
Considering changing trends of antibiotic susceptibility of S.typhi and S.paratyphi across different geographical regions in India, it is necessary to have constant surveillance and frequent re-evaluation of chloramphenicol therapy in Salmonella infection before treatment initiation, to avert further emergence of resistance.8 Hence, this study was undertaken to investigate the antimicrobial susceptibility pattern of chloramphenicol and other anti-typhoid drugs (cefixime, ofloxacin, azithromycin, and ceftriaxone) against Salmonella (including S. typhi and S.paratyphi) isolates obtained from four zones (north, south, west, and east) of India.
In the study, the proportion of S. typhi isolates was three times higher than S. paratyphi isolates (76.5% vs 23.5%) collected from blood samples throughout 4 months. Various studies had reported a higher prevalence of S. typhi over S. paratyphi isolates in blood samples collected from patients with enteric fever. In 2013, Choudhary et al reported 57.9% isolates of Salmonella to have serovar typhi and 41.6% to have serovar paratyphi A in blood isolates of Salmonella species obtained from a tertiary care hospital in south India between May 2009 and June 2011.27 In another study, 64 Salmonella isolates were isolated from 840 blood samples of suspected enteric fever where 41 (64.1%) were S. typhi, and 23 (35.9%) were S.paratyphi isolates.33 In another prospective hospital-based study, the ratio of S. typhi to S. paratyphi isolates (4:1) was found to be higher than that reported in our study.5 In 2016, Ramesh et al also reported a higher proportion of S. typhi isolates than S. paratyphi (81% vs 19%) among 200 Salmonella isolates obtained from patient blood samples.34 Other studies had also reported a higher prevalence of S. typhi against S. paratyphi with a ratio varying from 1.6:1 to 3.7:1.7,35,36 However, few studies had also reported a higher prevalence of S. paratyphi over S. typhi isolates.37–40 Though there is no specific reason for serovar variation, S. typhi infection is mainly due to waterborne transmission, and S.paratyphi is due to foodborne transmission; with the former requiring smaller inoculum, and the latter requiring a larger inoculum.41
In our study, the majority of S. typhi and S. paratyphi A isolates obtained across different zones of the country (94.4%) were sensitive to chloramphenicol (mean MIC: 3.89± 6.94 µg/mL). Our results support Pan India re-emergence of chloramphenicol sensitivity among Salmonella isolates. In 1999, Sood et al had reported chloramphenicol sensitivity among 71.9 (in 1994) to 91.6% (in 1998) isolates.42 Bhattacharya and Das in 2000 isolated S. typhi strains from Orissa of which 87.46% were chloramphenicol sensitive.43 Kumar et al in 2001 reported that there was an increase in chloramphenicol susceptibility from 43% (1995) to 93% (1999) among S. typhi strains in Ludhiana.44 In 2002, Gautam et al reported the re-emergence of chloramphenicol sensitivity in 90% of S. typhi isolates from Haryana by MIC determination.45 Rodrigues et al reported a decrease in the occurrence of chloramphenicol resistance in S.typhi strains (Mumbai) from 74% (1990) to 46% (2000).46 Chloramphenicol sensitivity was observed in 74.5% of S.typhi isolates (Nagpur) with MIC of 4 µg/mL.47 In 2004, Mandal et al reported a decrease in the occurrence of chloramphenicol resistance in S. typhi from 50% (1992) to 0% (2001); the strains isolated from 2002 to 2003 showed reduced susceptibility to ciprofloxacin but were sensitive to third-generation cephalosporins (ceftriaxone and cefotaxime).10 In Punjab, S. typhi showed very high (93.2%) sensitivity to chloramphenicol.25 In 2016, Ramesh et al in their study with 200 isolates of S. typhi (162 isolates) and S.paratyphi (38 isolates) obtained from patient’s blood samples between Nov 2013-Nov 2014 across 18 different regions of India also reported the re-emergence of the sensitivity of chloramphenicol.34 This re-emergence of sensitivity to chloramphenicol is of immense importance to the developing nations due to its cost-effectiveness and established clinical efficacy.24 It has found to reduce mortality due to typhoid fever from 20% to 1% and the duration of fever from 14–28 days to 3–5 days.48
In this study, out of 237 chloramphenicol-sensitive Salmonella isolates, 100% of S. paratyphi isolates and 89.47–95.24% of S. typhi isolates were susceptible to chloramphenicol. Our results were in agreement to the previous studies where 100% sensitivity to chloramphenicol was reported in S. paratyphi isolates and 96–97.4% sensitivity in S. typhi isolates.8,34,49 The MIC of chloramphenicol-sensitive isolates ranged from 0.75 to 8 µg/mL where 95.77% of our isolates had the MIC between 1 and 4 µg/mL. The results were in concordance with the earlier reports where the minimum and maximum values of MIC ranged between 1 and 4 µg/mL.45,47,49,50
In addition to chloramphenicol, S. typhi and S. paratyphi A isolates also showed excellent (100%) sensitivity against third-generation cephalosporins (ceftriaxone, cefixime) and macrolides (azithromycin). Ceftriaxone and cefixime slowly penetrate and kill intracellular bacteria, by inhibition of cell wall synthesis, and treat typhoid in 3–14 days.51–53 The resolution of symptoms is slow with fever clearance in 6–8 days, while azithromycin has a long half-life of 2 to 3 days, allowing once-daily administration. Azithromycin has an excellent penetration into most tissues with 50 to 100 times greater intracellular concentration than serum levels and has a slow release from the intracellular sites. It acts as an inhibitor of protein synthesis and results in a clinical cure rate of 90% with fever clearance time of 5–7 days in typhoid fever.54–57 Our results in terms of sensitivity to ceftriaxone, cefixime, and azithromycin were analogous to the previous literature where Salmonella isolates showed 100% sensitivity against ceftriaxone27 and cefixime,58 and 96.3–100% sensitivity to azithromycin.58,59 A battery of studies had also reported azithromycin to be similar or superior to chloramphenicol, fluoroquinolones, extended spectrum cephalosporins in the management of uncomplicated enteric fever with prompt resolution of clinical symptoms and poor relapse rate.60–66 In another study, a higher percentage of S. typhi and S. paratyphi A isolates were susceptible to chloramphenicol and cefixime as compared to ofloxacin (96.91% and 98.76% versus 78.39%; 100% and 100% versus 89.48%, respectively).34 Hence, oral cephalosporins and macrolides are considered as the first-line agents for empirical treatment of enteric fever cases in cases of decreased susceptibility to fluoroquinolones.67,68 However, few reports have also suggested resistance against azithromycin27,69,70 and ceftriaxone71–73 in S. typhi isolates. This may be due to production of drug-specific resistance genes, modification of target sites by enzymes (like methylases, esterases, phosphotransferases), or acquisition of an efflux pump in azithromycin-resistant cases74 and production of beta lactamases (which inactivate cephalosporins by cleaving its beta lactam ring) in cephalosporin-resistant cases. Hence, the excessive use of these antibiotics should be limited so that their efficacy against Salmonella isolates is not jeopardized.
In the study, 67.7% and 28.7% of Salmonella isolates had intermediate susceptibility and resistance to ofloxacin, respectively. Yashavanth and Vidyalakshmi (2010) and Bhatia et al (2007) reported 100% sensitivity against ofloxacin in S. typhi and S. paratyphi A isolates while Dutta et al (2014) reported ofloxacin resistance in 56% of S. paratyphi A and 18.2% of S. typhi isolates.5,8,49 Hence, high resistance against ofloxacin, which was earlier the treatment of choice for enteric fever, is a significant concern and health authorities should take appropriate measures to limit the indiscriminate use of fluoroquinolones.
Our study has a few strengths and limitations. The strengths being that the blood samples were collected from different geographical regions, covering all zones (north, south, west, and east) of India, making it a Pan India in vitro study. Secondly, the use of the culture and antimicrobial susceptibility results not only serves as an evidence-based guide to the therapeutic decisions but also may be considered as a tool to determine prevalence as well the evolution of susceptibility or resistance patterns against Salmonella isolates. Thirdly, the antimicrobial susceptibility of multiple classes of antibiotics was tested by the E-test method, which is a sensitive method to determine MIC. The MIC pattern so obtained helps to make a correct choice of the dosing regimen and route of administration of the antimicrobial agents as well. The study limitations were that no in vivo clinical responses were studied, which limited the viability of in vitro antimicrobial susceptibility results since there may be a gap between in vitro susceptibility/resistance results and the clinical outcome due to variation in achieving the peak plasma concentration due to different routes of administration.75 Hence, only an in vitro evaluation cannot be considered as robust evidence, but a judicious use with constant surveillance in clinical practice is necessarily recommended. Secondly, we did not record the medical history of illness/disease, previous medications or disease severity of the patients as these parameters may influence the current antimicrobial susceptibility profile of the organism. Thirdly, we did not genotypically characterize the organism by using any molecular typing tool; this would have helped us to determine the relatedness between the different Salmonella isolates.
Conclusion
Our study confirms the re‑emergence of susceptibility of Salmonella strains to chloramphenicol. Further, the concern about fluoroquinolone-decreased susceptibility as indicated by the intermediate susceptibility or resistance was reiterated in this study. Though cefixime, azithromycin, and ceftriaxone showed susceptibility, the possibility of antibiotic resistance with the irrational use of these antibiotics cannot be deterred. This study thus emphasizes the need for continuous evaluation and judicious use of antimicrobials, considering the ever-changing landscape. Further prospective studies are warranted to correlate the clinical outcome of treatment based on in vitro antimicrobial susceptibility patterns of Salmonella isolates in typhoid cases.
Acknowledgments
Medical writing support for preparing this manuscript was provided by GCE Solutions Inc. Abbott Healthcare Private Limited funded this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kanungo S, Dutta S, Sur D. Epidemiology of typhoid and paratyphoid fever in India. J Infect Dev Ctries. 2008;2(6):454–460.
2. Mogasale V, Maskery B, Ochiai RL, et al. Burden of typhoid fever in low-income and middle-income countries: a systematic, literature-based update with risk-factor adjustment. Lancet Glob Health. 2014;2(10):e570–e580. doi:10.1016/S2214-109X(14)70301-8
3. Nagashetty K, Channappa ST, Gaddad SM. Antimicrobial susceptibility of Salmonella Typhi in India. J Infect Dev Ctries. 2010;4(2):70–73.
4. Ochiai RL, Acosta CJ, Danovaro-Holliday MC, et al. A study of typhoid fever in five Asian countries: disease burden and implications for controls. Bull World Health Organ. 2008;86(4):260–268. doi:10.2471/blt.06.039818
5. Dutta S, Das S, Mitra U, et al. Antimicrobial resistance, virulence profiles and molecular subtypes of Salmonella enterica serovars Typhi and Paratyphi A blood isolates from Kolkata, India during 2009‑2013. PLoS One. 2014;9(8):e101347. doi:10.1371/journal.pone.0101347
6. Jesudason MV, John TJ. Plasmid mediated multidrug resistance in Salmonella Typhi. Indian J Med Res. 1992;95:66–67.
7. Mohanty S, Renucca K, Sood S, Das BK, Kapil A. Antibiogram pattern and seasonality of salmonella serotypes in a north Indian tertiary care hospital. Epidemiol Infect. 2006;134(5):961–966. doi:10.1017/S0950268805005844
8. Bhatia JK, Mathur AD, Arora MM. Re-emergence of chloramphenicol sensitivity in enteric fever. Med J Armed Forces India. 2007;63(3):212–214. doi:10.1016/S0377-1237(07)80136-5
9. Wain J, Kidgell C. The emergence of multidrug resistance to antimicrobial agents for the treatment of typhoid fever. Trans R Soc Trop Med Hyg. 2004;98(7):423–430. doi:10.1016/j.trstmh.2003.10.015
10. Mandal S, Mandal MD, Kumar PN. Reduced minimum inhibitory concentration of chloramphenicol for salmonella enterica serovar typhi. Ind J Med Sci. 2004;58(1):16–23.
11. Sheorey HS, Kaundinya DV, Hulyalkar VS, Deshpande AK. Multidrug resistant Salmonella Typhi in Bombay. Indian J Patho Microbiol. 1993;36(1):8–12.
12. Mishra S, Patwari AK, Anand VK, et al. A clinical profile of multidrug resistant typhoid fever. Indian Pediatr. 1991;28(10):1171–1174.
13. Jog S, Soman R, Singhal T, Rodrigues C, Mehta A, Dastur FD. Enteric fever in Mumbai–clinical profile, sensitivity patterns and response to antimicrobials. J Assoc Physicians India. 2008;56:237–240.
14. Arora D, Singh R, Kaur M, Ahi RS. A changing pattern in antimicrobial susceptibility of Salmonella enterica serotype isolated in North India. Afr J Microbiol Res. 2010;4(3):197–203.
15. Halder KK, Dalal BS, Ghose E, Sanyal S. Chloramphenicol resistant Salmonella typhi: the cause of recent out-break of enteric fever in Calcutta. Indian J Pathol Microbiol. 1992;35(1):11–17.
16. Rathish KC, Chandrashekar MR, Nagesha CN. An outbreak of multidrug resistant typhoid fever in Bangalore. Ind J Pediatr. 1995;62(4):445–448. doi:10.1007/BF02755065
17. Ciraj AM, Seetha KS, Gopalakrishna BK, Shivananda PG. Drug resistance pattern and Phage types of Salmonella typhi isolates in Manipal, South Karnataka. Ind J Med Sci. 1999;53(11):486–489.
18. Butler T, Linh NN, Arnold K, Pollack M. Chloramphenicol resistant typhoid fever in Vietnam associated with R factor. Lancet. 1973;302(7836):983–985. doi:10.1016/s0140-6736(73)91086-6
19. Brown JD, Duong Hong M, Rhoades ER. Chloramphenicol resistant Salmonella Typhi in Saigon. JAMA. 1975;231(2):162–166.
20. Chun D, Seol SY, Cho DT, Tak R. Drug resistance and R plasmids in Salmonella Typhi isolated in Korea. Antimicrob Agents Chemother. 1977;11(2):209–213. doi:10.1128/aac.11.2.209
21. Rowe B, Ward LR, Threlfall EJ. Multidrug-resistant Salmonella Typhi: a worldwide epidemic. Clin Infect Dis. 1997;24(Suppl 1):S106–S109. doi:10.1093/clinids/24.supplement_1.s106
22. Zaki SA, Karande S. Multidrug-resistant typhoid fever: a review. J Infect Dev Ctries. 2011;5(5):324–337.
23. Tankhiwale SS, Agrawal G, Jalgaonkar SV. A preliminary report on current antibiogram of salmonella enterica serotype typhi in Nagpur. Indian J Med Microbiol. 2003;21(4):292.
24. Sood S, Kapil A, Das B, et al. Re-emergence of chloramphenicol-sensitive Salmonella typhi. Lancet. 1999;353(9160):1241–1242. doi:10.1016/s0140-6736(99)00637-6
25. Gupta V, Kaur J, Kaistha N. Re-emerging chloramphenicol sensitivity and emerging low level ciprofloxacin resistance among Salmonella enterica serotype Typhi isolates in North India. Trop Doct. 2009;39(1):28–30. doi:10.1258/td.2008.070452
26. Karkey A, Thwaites GE, Baker S. The evolution of antimicrobial resistance in Salmonella Typhi. Curr Opin Gastroenterol. 2018;34(1):25–30. doi:10.1097/MOG.0000000000000406
27. Choudhary A, Gopalakrishnan R, Nambi PS, Ramasubramanian V, Ghafur KA, Thirunarayan MA. Antimicrobial susceptibility of Salmonella enterica serovars in a tertiary care hospital in southern India. Indian J Med Res. 2013;137(4):800–802.
28. Monica KH, Devi K, Devi S, Banylla S. Antibiogram of Salmonella typhi isolated from Enteric fever cases in a tertiary health care Centre in Imphal. Int J Pharmacol Ther. 2014;4:15–18.
29. Nachnani S, Scuteri A, Newman MG, Avanessian AB, Lomeli SL. E-test: a new technique for antimicrobial susceptibility testing for periodontal microorganisms. J Periodontol. 1992;63(7):576–583. doi:10.1902/jop.1992.63.7.576
30. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
31. Jorgensen J, Ferraro MJ. Antibiotic susceptibility testing: a review of general principles and contemporary practices. Clin Infect Dis. 2009;49(11):1749–1755. doi:10.1086/647952
32. Mahon C, Lehman D, Manuselis G. Textbook of Diagnostic Microbiology.
33. Adhikari D, Acharya D, Shrestha P, Amatya R. Ciprofloxacin susceptibility of Salmonella enterica serovar Typhi and Paratyphi A from blood samples of suspected enteric fever patients. Int J Infect Microbial. 2012;1(1):
34. Ramesh U, Das S, Balasubramanian A. Re-emergence of chloramphenicol-susceptible Salmonella Typhi and Paratyphi A strains in India. Indian J Med Microbiol. 2016;34(2):262–263. doi:10.4103/0255-0857.180393
35. Bhattacharya SS, Das U, Choudhury BK. Occurrence & antibiogram Salmonella typhi & S. paratyphi A isolated from Rourkela, Orissa. Ind J Med Microbiol. 2011;133:431–433.
36. World Health Organization. Indian network for surveillance of antimicrobial resistance. antibiogram of Salmonella enterica serovar typhi and Salmonella enterica serovar paratyphi A: a multi-centre study from India. WHO South-East Asia J Public Health. 2012;1:182–188. doi:10.4103/2224-3151.206930
37. Shirakawa T, Acharya B, Kinoshita S, Kumagai S, Gotoh A, Kawabata M. Decreased susceptibility to fluoroquinolones and gyrA gene mutation in the Salmonella enterica serovar typhi and paratyphi A isolated in Katmandu, Nepal, in 2003. Diagn Microbiol Infect Dis. 2006;54(4):299–303. doi:10.1016/j.diagmicrobio.2005.10.016
38. Pramod P, Binod L, Ritu A, Sharad B, Prakash P. Enteric fever caused by Salmonella enterica serovar paratyphi A: an emerging health concern in Nepal. Afr J Microbiol Res. 2016;10(42):1784–1791. doi:10.5897/AJMR
39. Verma S, Thakur S, Kanga A, Singh G, Gupta P. Emerging Salmonella Paratyphi A enteric fever and changing trends in antimicrobial resistance pattern of Salmonella in Shimla. Indian J Med Microbiol. 2010;28(1):51–53. doi:10.4103/0255-0857.58730
40. Wu W, Wang H, Lu J, Wu J. Genetic diversity of Salmonella typhi and paratyphi in Shenzhen, China from 2002 to 2007. BMC Microbiol. 2010;10:32–38. doi:10.1186/1471-2180-10-32
41. Acharya D, Bhatta DR, Malla S, Dumre SP, Adhikari N, Kandel BP. Salmonella enterica serovar Paratyphi A: an emerging cause of febrile illness in Nepal. Nepal Med Coll J. 2011;13(2):69–73.
42. Sood S, Kapil A, Dash N, et al. Paratyphoid fever in India: an emerging problem. Emerg Infect Dis. 1999;5(3):483–484. doi:10.3201/eid0503.990329
43. Bhattacharya SS, Das U. Occurrence of Salmonella typhi infection in Rourkela, Orissa. Indian J Med Res. 2000;111:75–76.
44. Kumar R, Aneja KR, Punia AK, et al. Changing pattern of biotypes, phage types and drug resistance of Salmonella typhi in Ludhiana during 1980-1999. Ind J Med Res. 2001;113:175–180.
45. Gautam V, Gupta NK, Chaudhary U, Arora DR. Sensitivity pattern of Salmonella serotypes in Northern India. Braz J Infect Dis. 2002;6(6):281–287. doi:10.1590/S1413-86702002000600003
46. Rodrigues C, Mehta A, Joshi VR. Salmonella typhi in the past decade: learning to leave with resistance. Clin Infect Dis. 2002;34(1):126. doi:10.1086/323019
47. Chande C, Shrikhande S, Kapali S, Agarwal S, Fule RP. Change in antimicrobial pattern of Salmonella Typhi in central India. Indian J Med Res. 2002;115:248–250.
48. Mirza SH, Beeching NJ, Hart CA. Multi-drug resistant typhoid: a global problem. J Med Microbiol. 1996;44(5):317–319. doi:10.1099/00222615-44-5-317
49. Yashavanth R, Vidyalakshmi K. The re-emergence of chloramphenicol sensitivity among enteric fever pathogens in Mangalore. J Clin Diagn Res. 2010;4(5):3106–3108.
50. Sania KM, Shyamasakhi PD, Pramodini KD, Sulochana KD. Evaluation of minimum inhibitory concentration of chloramphenicol for salmonella spp. Isolated from enteric fever cases in a tertiary hospital in Imphal. Int J Pharm Sci Res. 2016;7(9):3815–3819.
51. Chang HR, Vladoianu IR, Pechèe JC. Effects of ampicillin, ceftriaxone, chloramphenicol, pefloxacin and trimethoprim-sulphamethoxazole on Salmonella Typhi within human monocyte-derived macrophages. J Antimicrob Chemother. 1990;26(5):689–694. doi:10.1093/jac/26.5.689
52. Ekinci B, Coban AY, Birinci A, Durupinar B, Erturk M. In vitro effects of cefotaxime and ceftriaxone on Salmonella Typhi within human monocyte-derived macrophages. Clin Microbiol Infect. 2002;8(12):810–813.
53. Cao XT, Kneen R, Nguyen TA, Truong DL, White NJ, Parry CM. A comparative study of ofloxacin and cefixime for treatment of typhoid fever in children. The Dong Nai Pediatric Center Typhoid Study Group. Pediatr Infect Dis J. 1999;18(3):245–248. doi:10.1097/00006454-199903000-00007
54. Panteix G, Guillaumond B, Harf R, et al. In vitro concentration of azithromycin in human phagocytic cells. J Antimicrob Chemother. 1993;31(SupplE):1–4. doi:10.1093/jac/31.suppl_e.1
55. Rakita RM, Jacques-Palaz K, Murray BE. Intracellular activity of azithromycin against bacterial enteric pathogens. Antimicrob Agents Chemother. 1994;38(9):1915–1921. doi:10.1128/aac.38.9.1915
56. Gladue RP, Bright GM, Isaacson RE, Newborg MF. In-vitro and in-vivo uptake of azithromycin (CP-62,993) by phagocytic cells: possible mechanisms of delivery and release at sites of infection. Antimicrob Agents Chemother. 1989;33(3):277–282. doi:10.1128/aac.33.3.277
57. Bhan MK, Bahl R, Bhatnagar S. Typhoid and paratyphoid fever. Lancet. 2005;366(9487):749–762. doi:10.1016/S0140-6736(05)67181-4
58. Bhetwal A, Maharjan A, Khanal PR, et al. Enteric fever caused by salmonella enterica serovars with reduced susceptibility of Fluoroquinolones at a community based teaching hospital of Nepal. Int J Microbiol. 2017;2017:2869458. doi:10.1155/2017/2869458
59. Chayani N, Tiwari S, Sarangi G, et al. Role of azithromycin against clinical isolates of family enterobacteriaceae: a comparison of its minimum inhibitory concentration by three different methods. Indian J Med Microbiol. 2009;27(2):107–110. doi:10.4103/0255-0857.45361
60. Butler T, Sridhar CB, Daga MK, et al. Treatment of typhoid fever with azithromycin versus chloramphenicol in a randomized multicenter trial in India. J Antimicrob Chemother. 1999;44:243–250. doi:10.1093/jac/44.2.243
61. Frenck RW, Nakhla IA, Sultan Y, et al. Azithromycin versus ceftriaxone for the treatment of uncomplicated typhoid fever in children. Clin Infect Dis. 2000;31:1134–1138. doi:10.1086/317450
62. Frenck RW, Mansour A, Nakhla I, et al. Short-course azithromycin for the treatment of uncomplicated typhoid fever in children and adolescents. Clin Infect Dis. 2004;38:951–957. doi:10.1086/382359
63. Chinh NT, Parry CM, Ly NT, et al. A randomized controlled comparison of azithromycin and ofloxacin for treatment of multidrug-resistant or nalidixic acid-resistant enteric fever. Antimicrob Agents Chemother. 2000;44:1855–1859. doi:10.1128/aac.44.4.1029-1034.2000
64. Parry CM, Ho VA, Phuong LT, et al. Randomized controlled comparison of ofloxacin, azithromycin, and an ofloxacin-azithromycin combination for treatment of multidrug-resistant and nalidixic acid-resistant typhoid fever. Antimicrob Agents Chemother. 2007;46:819–825. doi:10.1128/AAC.00447-06
65. Dolecek C, Tran TP, Nguyen NR, et al. A multi-center randomised controlled trial of gatifloxacin versus azithromycin for the treatment of uncomplicated typhoid fever in children and adults in Vietnam. PLoS One. 2008;3:e2188. doi:10.1371/journal.pone.0002188
66. Effa EE, Bukirwa H. Azithromycin for treating uncomplicated typhoid and paratyphoid fever (enteric fever). Cochrane Database Syst Rev. 2011;10:CD006083.
67. Crump JA, Sj¨olund-Karlsson M, Gordon MA, Parry CM. Epidemiology, clinical presentation, laboratory diagnosis, antimicrobial resistance, and antimicrobial management of invasive Salmonella infections. Clin Microbiol Rev. 2015;28(4):901–937. doi:10.1128/CMR.00064-15
68. Kariuki S, Gordon MA, Feasey N, Parry CM. Antimicrobial resistance and management of invasive Salmonella disease. Vaccine. 2015;33(3):C21–C29. doi:10.1016/j.vaccine.2015.03.102
69. Rai S, Jain S, Prasad KN, Ghoshal U, Dhole TN. Rationale of azithromycin prescribing practices for enteric fever in India. Indian J Med Microbiol. 2012;30(1):30–33. doi:10.4103/0255-0857.93017
70. Patel SR, Bharti S, Pratap CB, Nath G. Drug resistance pattern in the recent isolates of Salmonella typhi with special reference to cephalosporins and azithromycin in the gangetic plain. J Clin Diagn Res. 2017;11(6):DM01–DM03.
71. Gonza´ Lez-Lo´ Pez JJ, Piedra-Carrasco N, Salvador F, et al. ESBL-producing Salmonella enterica Serovar typhi in traveler returning from Guatemala to Spain. Emerg Infect Dis. 2014;20(11):1918–1920. doi:10.3201/eid2011.140525
72. Harrois D, Breurec S, Seck A, et al. Prevalence and characterization of extended-spectrum b-lactamase-producing clinical Salmonella enterica isolates in Dakar, Senegal, from 1999 to 2009. Clin Microbiol Infect. 2014;20(2):O109–O116. doi:10.1111/1469-0691.12339
73. Ahmed D, Hoque A, Mazumder R, et al. Salmonella enterica serovar typhi strain producing extended-spectrum -lactamases in Dhaka, Bangladesh. J Med Microbiol. 2012;61(Pt 7):1032–1033. doi:10.1099/jmm.0.044065-0
74. Braoudaki M, Hilton AC. Mechanisms of resistance in Salmonella enterica adapted to erythromycin, benzalkonium chloride and triclosan. Int J Antimicrob Agents. 2005;25:31–37. doi:10.1016/j.ijantimicag.2004.08.020
75. Acharya GP, Davis TM, Ho M, et al. Factors affecting the pharmacokinetics of parenteral chloramphenicol in enteric fever. J Antimicrob Chemother. 1997;40(1):91–98. doi:10.1093/jac/40.1.91
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.