Back to Journals » Clinical Ophthalmology » Volume 20
Self-Reported Vision-Related Quality of Life and Functional Impact in Portuguese Patients with Uveitis: A Cross-Sectional Study
Authors Filipa Gomes A, Oliveira AP, Roque A ![]() , Martinez-Perez C
, Martinez-Perez C ![]()
Received 21 April 2026
Accepted for publication 18 June 2026
Published 9 July 2026 Volume 2026:20 618814
DOI https://doi.org/10.2147/OPTH.S618814
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Andreia Filipa Gomes, Ana Paula Oliveira, Ana Roque, Clara Martinez-Perez
Department of Optometry, Instituto Superior de Educação e Ciências de Lisboa (ISEC Lisboa), Lisbon, Portugal
Correspondence: Clara Martinez-Perez, Email [email protected]
Purpose: To evaluate the association between uveitis and vision-related quality of life (VRQoL) in Portuguese adults and to explore self-reported relationships with daily activities, driving, and psychosocial functioning.
Methods: A cross-sectional study was conducted from January to March 2024 in Lisbon, including 92 adults (mean age: 46.0 ± 10.7 years). Participants were divided into two groups: self-reported uveitis (n=36) and without uveitis (n=56). All participants completed an online National Eye Institute Visual Function Questionnaire-25 (NEI VFQ-25) along with demographic and clinical surveys assessing perceived vision, ocular pain, activity limitations, driving status, and emotional and social reactions. Statistical analyses included group comparisons using Chi-square or Mann–Whitney U-tests and multivariable logistic regression models adjusted for age and sex.
Results: Participants with uveitis reported significantly higher levels of constant vision concern (55.6% vs. 21.4%, p< 0.001) and greater ocular pain (overall distribution, p< 0.001), with a higher proportion reporting severe pain (16.7% vs. 7.1%). They also experienced more difficulties in daily activities such as reading street signs (69.6%), cooking (63.0%), and finding objects (56.5%). Daytime driving difficulties were more frequent among uveitis participants (70.0% vs. 31.8%, p=0.0049). Emotional and social impacts, including activity restriction, staying at home, frustration, and dependence on others, were also more commonly reported (p< 0.001 in most comparisons). Multivariable analyses suggested that uveitis was associated with higher functional and psychosocial limitations; however, uveitis was not significantly associated with constant vision concern, which was primarily related to older age.
Conclusion: Uveitis was associated with poorer self-reported VRQoL, daily functioning, driving ability, and psychosocial well-being, although not all associations remained significant after adjustment. These findings should be interpreted as exploratory and hypothesis-generating. Multidisciplinary management integrating visual rehabilitation and psychosocial support may be important to improve patient-centered care.
Keywords: uveitis, quality of life, NEI VFQ-25, visual function, daily activities, driving, ocular pain, psychosocial impact, Portugal
Introduction
Uveitis is an ocular inflammatory disease that affects the uvea, the middle layer of the eye composed of the iris, ciliary body, and choroid. It is estimated to affect between 38 and 714 individuals per 100,000 inhabitants worldwide and is associated with 3% to 10% of visual disability cases in the United States and Europe.1 In low- and middle-income countries, it may account for up to a quarter of blindness cases, according to previous studies (many of them conducted nearly 30 years ago).1 More recent population-based studies suggest that the prevalence of uveitis may be higher when modern diagnostic techniques are used.2,3
The clinical manifestations of uveitis include ocular redness, pain, photophobia, blurred vision, and floaters. Timely ophthalmic evaluation is essential to determine the etiology, assess severity, and establish early treatment.4 Uveitis can be infectious (eg, associated with tuberculosis, toxoplasmosis, human immunodeficiency virus (HIV), or syphilis) or non-infectious, generally related to autoimmune diseases and systemic inflammatory processes, such as sarcoidosis or multiple sclerosis.5–10 However, in a significant percentage of cases (27% to 51%), the underlying cause remains unknown and is classified as idiopathic uveitis.6,11–13
In pediatric patients, uveitis represents approximately 5–10% of all uveitis cases and is often non-infectious, chronic, or recurrent; delayed diagnosis may increase the risk of ocular complications and long-term visual impairment, although the present study focuses exclusively on adults.14–17
Although most studies have focused on the etiology and clinical management of uveitis, there is growing interest in understanding the functional and psychosocial impact of this disease on patients. Several recent studies and reviews have highlighted that uveitis can significantly affect emotional well-being and quality of life (QoL), in both adults and children, not only due to visual impairment but also because of systemic complications and the impact of treatment.18,19 It has been reported that patients with uveitis present worse psychosocial outcomes and lower quality of life compared to the general population, with contributing factors including clinical aspects (eg, degree of visual impairment and ocular comorbidities) as well as personal characteristics (older age, female sex).18,19 To assess these aspects, various quality of life and psychosocial well-being instruments have been used, including specific questionnaires such as the National Eye Institute Visual Function Questionnaire-25 (NEI VFQ-25), the 36-Item Short Form Health Survey (SF-36), the Behçet Disease Quality of Life scale (BDQoL), and the Effect of Youngsters’ Eyesight on Quality of Life questionnaire (EYE-Q) for pediatric populations.20 In this context, although numerous previous studies have focused on the psychometric validation of patient-reported outcome measures (PROMs) and on the global description of quality of life in patients with uveitis, most have been conducted in very specific populations or without a direct control group, and updated data from the general population in Southern Europe are scarce. Furthermore, few studies have comprehensively explored the relationship between uveitis and specific functional domains such as everyday activities, driving performance, and emotional and social responses. In addition, most available evidence relies on clinical cohorts, while population-based patient-reported data remain limited.
Therefore, the objectives of this study were (i) to evaluate, for the first time in Portugal, the detailed impact of uveitis on vision-related quality of life using the NEI VFQ-25, and (ii) to explore its associations with daily activities, driving difficulties, and emotional and social functioning, in comparison with a control group without uveitis.
Methodology
The study was conducted in accordance with the ethical standards set forth in the Declaration of Helsinki and was approved by the Ethics Committee of the Higher Institute of Education and Sciences of Lisbon (ISEC Lisbon) on December 5, 2023 (approval ID: CE/2023/12/05).
Study Design and Participants
This was a cross-sectional study conducted in the Lisbon (Portugal) region between January and March 2024, and it was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines (Supplementary Material 1). A total of 92 individuals were recruited. The inclusion criteria were being 18 years or older, having the ability to understand and complete the questionnaire, and having signed informed consent. Exclusion criteria included the presence of cognitive or linguistic difficulties that prevented completing the questionnaire independently.
Participants were recruited through online platforms and social networks, including patient associations, optometry clinics, and professional groups. Duplicate responses were excluded based on Internet Protocol (IP) address and Email verification, and only complete questionnaires were retained. For participants reporting a diagnosis of uveitis, eligibility required self-report of a prior ophthalmologic diagnosis. No external clinical verification of the diagnosis was performed. Although no in-person prescreening was conducted, internal consistency checks between reported symptoms, self-reported disease duration, and diagnosis were applied to improve data reliability. This recruitment strategy may introduce selection bias and should be considered when interpreting the findings.
Control participants were recruited from the same online sources, excluding individuals with any self-reported ocular or systemic inflammatory disease.
Instrument and Data Collection
Data were collected using the National Eye Institute Visual Function Questionnaire-25 (NEI VFQ-25),21 which has been culturally and linguistically validated and adapted. This instrument assesses the subjective perception of visual function and its impact on various aspects of daily life, including general vision, ocular pain, near and distance activities, social functioning, vision-related mental health, role limitations, dependency, and color and peripheral vision. It also includes a general question on overall health status.
Responses were coded and converted to a scale from 0 to 100, where higher scores reflect better vision-related quality of life. The items of each subscale were averaged following the official NEI VFQ-25 scoring algorithm.
The questionnaire was distributed online via Google Forms® and shared through WhatsApp®, social media, professional forums, and patient groups to maximize participation and ensure accessibility. In addition to the main questionnaire, demographic and clinical variables were collected, such as age, sex, diagnosis of uveitis, perception of general health status, presence of ocular pain or discomfort, driving difficulties, and limitations in other daily activities.
Because the study relied on self-administered online questionnaires, no clinical examination or medical records were obtained to determine uveitis subtype, disease activity, or treatment status. This design allowed inclusion of a geographically diverse sample but limited clinical stratification. Future studies combining subjective and clinical measures are warranted to overcome this limitation.
Statistical Analysis
Descriptive statistics were used to summarize the study population, presenting categorical variables as frequencies and percentages and continuous variables as means with standard deviations and medians with interquartile ranges (p25–p75). Comparisons between participants with and without uveitis were performed using the Chi-square test or Fisher’s exact test for categorical variables and the Mann–Whitney U-test for continuous variables. For ordinal outcomes with more than two levels, the Kruskal–Wallis test was used to evaluate differences in age distribution.
To further explore factors associated with higher impact or difficulty, multivariable logistic regression models were fitted. For vision concern, a binary outcome was defined comparing participants who reported being concerned “All the time” versus all other levels. In the analysis of ocular pain, participants reporting “Severe” pain were contrasted with those with less severe or no pain. Regarding daily activities, a binary variable was created to indicate the presence of any difficulty across evaluated activities. For driving difficulties, separate binary variables were created for daytime and nighttime, grouping any level of reported difficulty versus no difficulty. Emotional and social reactions were also dichotomized, contrasting those who answered “Never” versus those who reported any frequency (“A few times” or more).
All models included age, sex, and uveitis status as covariates. Self-reported vision and general health were initially considered but excluded due to multicollinearity and model instability. Given the sample size, models were kept parsimonious to reduce the risk of overfitting.
Adjusted odds ratios (ORs), 95% confidence intervals (CIs), and p-values were reported. Statistical significance was set at p < 0.05. Analyses were performed using R software (version 4.4.2; R Foundation for Statistical Computing, Vienna, Austria).
No formal a priori sample size calculation was performed, as the study was exploratory and based on feasibility. Therefore, the analyses should be considered hypothesis-generating rather than confirmatory.
Results
A total of 92 participants were included in the analysis, with ages ranging from 24 to 69 years. The mean age was 46.0 ± 10.7 years (median: 45.5 years; IQR: 41–55 years). The majority of participants were female (71.7%, n=66), while 28.3% (n=26) were male. Regarding uveitis status, 39.1% (n=36) reported a diagnosis of uveitis, whereas 60.9% (n=56) did not. With respect to perceived vision, 43.5% (n=40) rated it as “good”, 37.0% (n=34) as “stable”, 8.7% (n=8) as “excellent”, 8.7% (n=8) as “poor”, and 2.2% (n=2) as “very poor”. Table 1 shows the demographic and clinical characteristics of participants with and without uveitis. Participants with uveitis were older than those without uveitis, and the sex distribution differed markedly between groups, with the control group being predominantly female (89.3%).
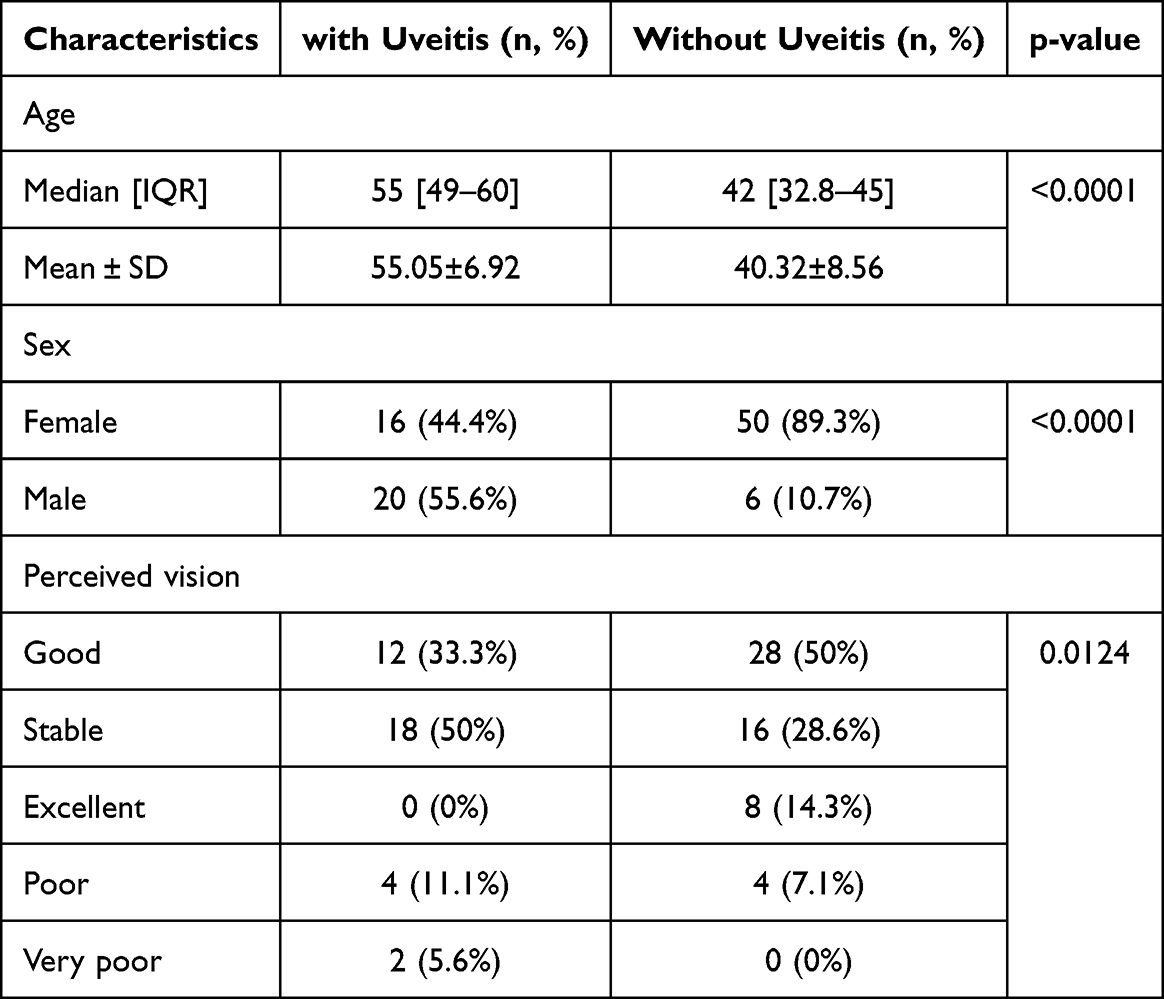 |
Table 1 Baseline Characteristics According to Uveitis Diagnosis |
Vision Concern and Ocular Pain
The overall distribution of vision concern showed that 34.8% (n=32) of participants reported being concerned “All the time”, followed by 23.9% (n=22) who reported “Most of the time”, another 23.9% (n=22) “Sometimes”, 10.9% (n=10) “A little”, and only 6.5% (n=6) indicated “Not at all”.
As shown in Figure 1A, there were significant differences in the level of concern between participants with uveitis and those without uveitis (p<0.001). Among patients with uveitis, 55.6% (n=20) reported being concerned “All the time”, whereas only 21.4% (n=12) of patients without uveitis reported being concerned “All the time”.Regarding ocular pain, in the total population, 34.8% (n=32) did not experience pain, 32.6% (n=30) reported “Mild” pain, 21.7% (n=20) “Moderate” pain, and 10.9% (n=10) “Severe” pain. As shown in Figure 1B, there were significant differences in pain levels between participants with and without uveitis (p<0.001). Among patients with uveitis, 16.7% (n=6) reported “Severe” pain, while only 7.1% (n=4) of participants without uveitis reported “Severe” pain.
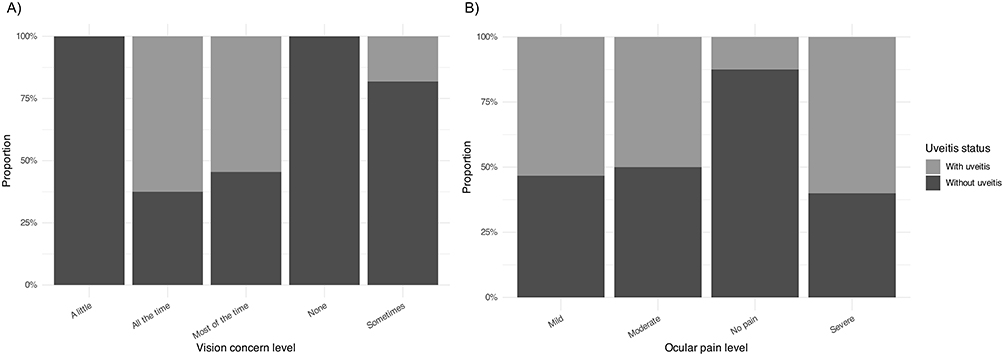 |
Figure 1 Distribution of vision concern (A) and ocular pain (B) levels by uveitis status. |
Among patients with uveitis, no significant differences were found in vision concern distribution between men and women (p>0.05). However, significant differences in ocular pain by sex were observed (p<0.001), with a higher frequency of moderate and severe pain among women (62.5%, n=10 and 12.5%, n=2, respectively), whereas mild pain was more common among men (60.0%, n=12), who also showed a higher proportion without pain (20.0%, n=4). Additionally, significant differences in age were found among different levels of vision concern (p=0.005). Patients who reported the highest level of concern (“All the time”) had a higher median age (57 years; p25: 55, p75: 60) compared to those who reported “Most of the time” (median: 50.5 years; p25: 47, p75: 57) and “Sometimes” (median: 48.5 years; p25: 48, p75: 49). Similarly, significant age differences were observed across pain levels (p=0.0078). Patients reporting “Severe” pain had the highest median age (59 years; p25: 54.5, p75: 66.5), followed by “Moderate” pain (median: 57 years; p25: 55, p75: 60), “Mild” pain (median: 52.5 years; p25: 48.8, p75: 56.2), and “No pain” (median: 47.5 years; p25: 47, p75: 48).
After adjusting for potential confounders (age, sex, vision status, and general health), older age remained significantly associated with higher odds of reporting “All the time” vision concern (OR=1.20, 95% CI: 1.08–1.35, p=0.001), whereas uveitis status was not significantly associated in the multivariable model (p>0.05).
Difficulties in Daily Activities
The overall distribution of difficulties in daily activities showed that the highest proportions of participants reporting some difficulties were found when reading street signs (69.6%, n=64), reading printed text in newspapers (67.4%, n=62), and finding objects on crowded shelves (56.5%, n=52). Additionally, 63.0% (n=58) reported difficulties with cooking, sewing, or seeing things up close; 42.2% (n=39) when choosing and matching clothes; and 43.5% (n=40) when going downstairs and noticing objects off to the side while walking alone.
On the other hand, lower percentages of difficulty were reported when seeing how people react during conversations (39.1%, n=36), visiting people in their homes, at parties, or in restaurants (37.0%, n=34), and going to movies, plays, or sports events (37.0%, n=34). As shown in Figure 2, there were significant differences in the presence of difficulties across all activities evaluated between participants with and without uveitis (p<0.001). Among participants with uveitis, no significant differences were found in the distribution of difficulties in daily activities between men and women, nor with respect to age (both p>0.05).
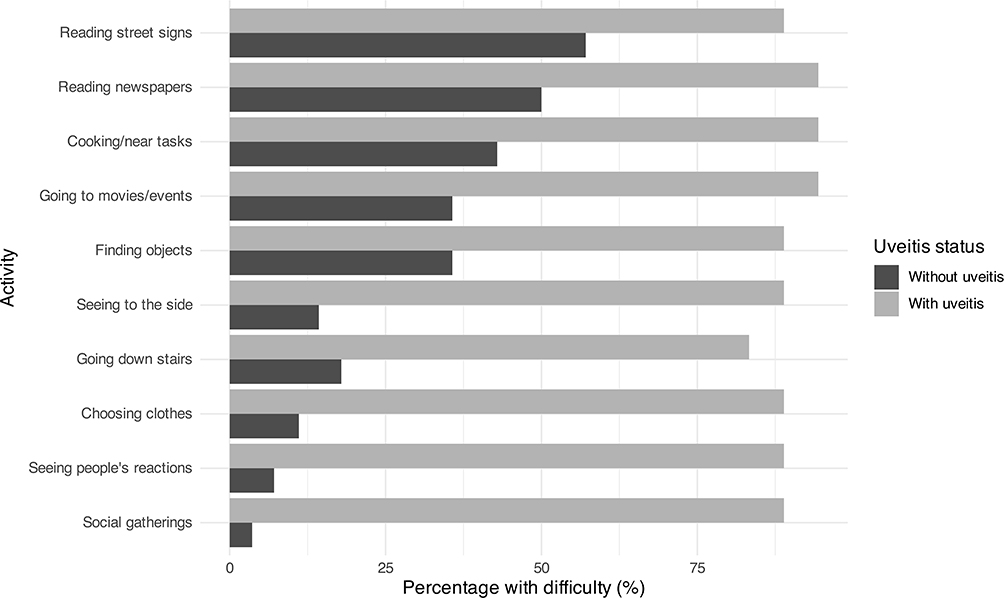 |
Figure 2 Percentage of participants with any difficulty by activity and uveitis status. |
After adjusting for age, sex, and uveitis status, male sex was significantly associated with lower odds of reporting any difficulty in daily activities (OR=0.05, 95% CI: 0.005–0.33, p=0.004). Age showed a trend toward higher odds of difficulty (OR=1.09, 95% CI: 0.99–1.22, p=0.096), while uveitis status was also suggestive of an association but did not reach statistical significance (OR=7.9, 95% CI: 0.77–114, p=0.095).
Driving Impact
The proportion of participants who reported driving was 47.8% (n=44), while 28.3% (n=26) did not drive, and 23.9% (n=22) drove occasionally. Among those who stopped driving, 8.7% (n=8) indicated that they did so mainly due to vision problems, and 6.5% (n=6) mentioned that vision was the primary reason along with other factors. Regarding difficulties during driving, 28.3% (n=26) reported “Mild difficulty” during the day, 2.2% (n=2) “Moderate difficulty”, and 39.1% (n=36) reported no difficulty. For night driving, 26.1% (n=24) reported “Mild difficulty”, 19.6% (n=18) “Moderate difficulty”, 8.7% (n=8) “Severe difficulty”, and 13.0% (n=12) reported no difficulty. As shown in Figure 3, significant differences were found in the distribution of driving status and daytime driving difficulties between participants with and without uveitis (p<0.001 and p=0.0049, respectively). In particular, 70.0% (n=21) of patients with uveitis reported difficulties driving during the day, compared to 31.8% (n=14) of participants without uveitis. For night driving, although a trend was observed, it did not reach statistical significance (p>0.05), with 90.0% (n=27) of patients with uveitis reporting difficulties versus 77.3% (n=34) of those without uveitis. Within patients with uveitis, no significant differences were observed in driving difficulties (either daytime or nighttime) by sex (p>0.05). However, significant age differences were found between patients with and without daytime driving difficulties (p=0.0079). Specifically, those reporting daytime difficulties were older (median: 60 years; p25: 51.8, p75: 65.8) compared to those reporting no difficulty (median: 48 years; p25: 45.8, p75: 53.2). Regarding night driving, although there was a trend toward older age in those reporting difficulties (median: 57 years; p25: 50, p75: 65) compared to those reporting no difficulty (median: 48 years; p25: 48, p75: 48), this difference was not statistically significant (p>0.05).
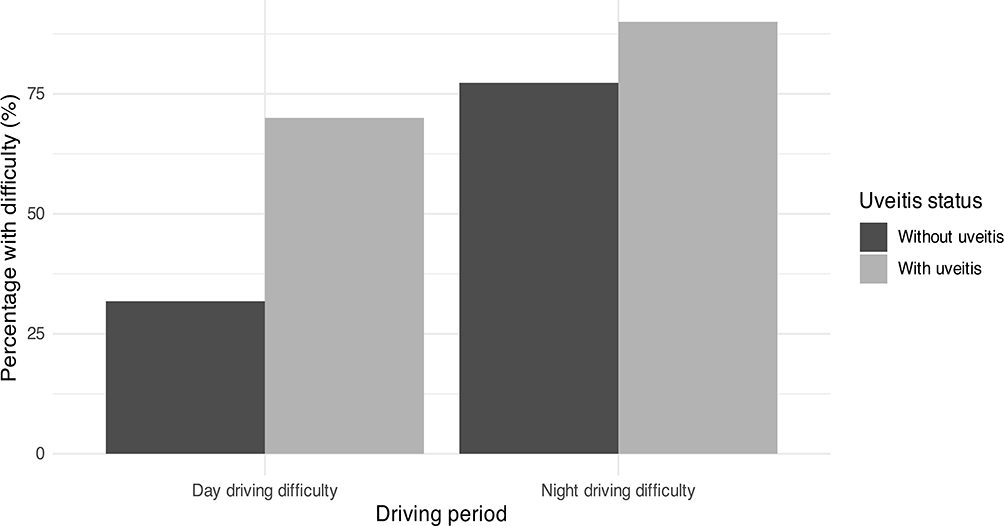 |
Figure 3 Driving difficulty by period and uveitis status. |
After adjusting for age, sex, and uveitis status, male sex was significantly associated with lower odds of reporting daytime driving difficulties (OR=0.15, 95% CI: 0.02–0.76, p=0.042). Conversely, having uveitis was strongly associated with higher odds of experiencing daytime driving difficulties (OR=29.0, 95% CI: 3.49–423, p = 0.005). Age did not show a statistically significant association in this model (p=0.235).
Emotional and Social Reactions
The proportion of participants who reported having stopped doing activities they enjoyed was 33.3% (n=26), while 66.7% (n=52) indicated “Never”. Regarding feeling limited in performing activities, 35.9% (n=28) reported some frequency (from “A few times” to “Most of the time”), and 64.1% (n=50) answered “Never”. Concerning ocular discomfort that led them to stop doing things, 34.6% (n=27) reported some frequency, whereas 65.4% (n=51) indicated “Never”. In relation to staying at home because of their vision, 31.3% (n=24) reported some frequency, while 68.7% (n=53) indicated “ Definitely false”.
Regarding feeling frustrated because of their vision, 35.9% (n=28) reported some agreement, and 64.1% (n=50) “ Definitely false”. Similarly, 33.3% (n=26) reported having less control over what they do because of their vision, while 66.7% (n=52) indicated “Definitely false”. As for depending on what others say, 28.2% (n=22) reported some agreement, while 71.8% (n=56) answered “Definitely false”. Regarding needing help from others because of their vision, 31.3% (n=24) reported some agreement, and 68.7% (n=53) “ Definitely false”. Finally, 33.3% (n=26) reported worrying about doing things that might embarrass themselves or others because of their vision, whereas 66.7% (n=52) indicated “ Definitely false”.
As shown in Figure 4, statistically significant differences were found in the distribution of all emotional and social reactions between participants with and without uveitis (p<0.001 in most comparisons). In particular, among patients with uveitis, the frequency of reporting “A few times” or more was considerably higher than in those without uveitis for almost all reactions analyzed. Within the uveitis group, no significant differences were observed in emotional and social reactions by sex (p>0.05). However, when analyzing age, significant differences were observed in several emotional and social reactions. For example, participants who reported any frequency (≥ “A few times”) of “stopping activities” had a median age of 57 years (p25: 50, p75: 60), whereas those who answered “Never” had a median age of 49 years (p25: 48, p75: 55) (p=0.0106). Similarly, differences were observed in “feeling limited” (median: 56 vs. 51.5 years, p=0.039), “ocular discomfort” (57 vs. 49 years, p=0.0106), “staying at home” (58 vs. 52 years, p=0.0183), “feeling frustrated” (56 vs. 51.5 years, p=0.039), “less control” (57 vs. 49 years, p=0.0106), “depending on others” (58 vs. 52 years, p=0.0179), “needing help” (59 vs. 49 years, p=0.0022), and “fear of feeling embarrassed” (58 vs. 52 years, p=0.0183).
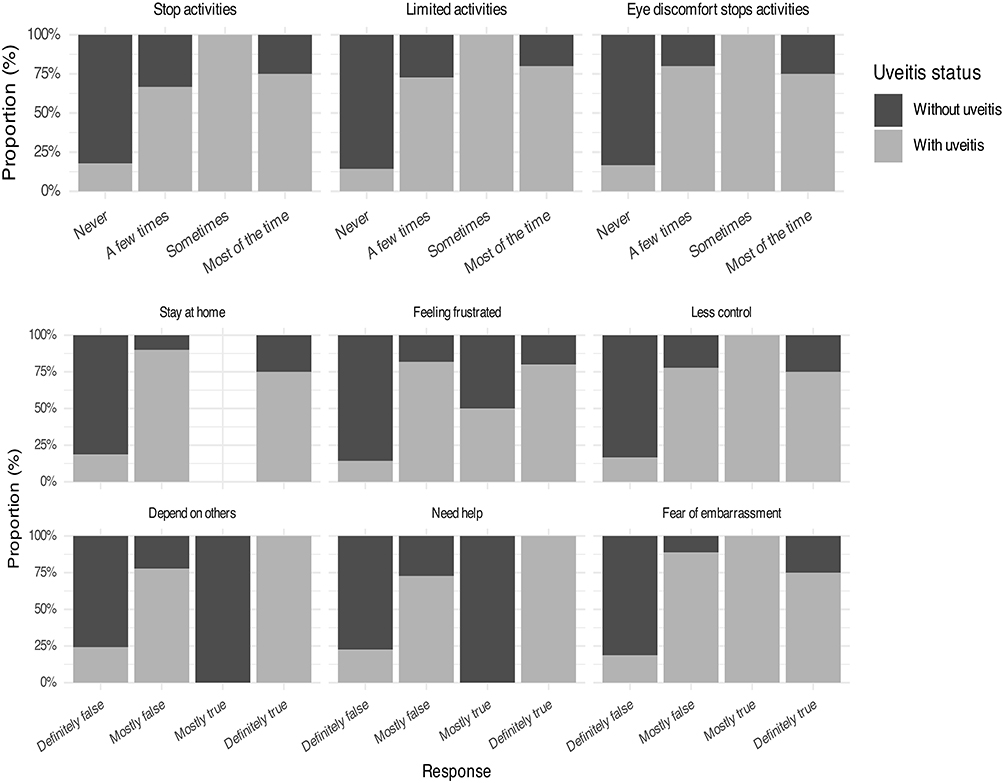 |
Figure 4 Emotional and social reactions by uveitis status. |
After adjusting for age and sex, uveitis status was significantly associated with higher odds of reporting various emotional and social difficulties. Specifically, patients with uveitis had higher odds of reporting “stopping activities” (OR=8.60, 95% CI: 1.66–67.7, p=0.018), “feeling limited” (OR=19.0, 95% CI: 3.55–162, p=0.002), and “ocular discomfort stopping activities” (OR=18.9, 95% CI: 3.50–163, p<0.001), among others. Age was also significantly associated with several reactions, while male sex generally showed a protective tendency but was not statistically significant.
Discussion
The present study is, to our knowledge, one of the first conducted in Portugal to analyze in detail the impact of uveitis on vision-related quality of life (VRQoL) and its relationship with emotional and social functioning, daily activities, and driving, using the NEI VFQ-25 and including a control group without uveitis. Overall, our findings indicate that patients with uveitis reported a higher level of impairment across emotional, social, and functional domains, including daily activities and driving. However, these findings should be interpreted with caution given the study design. As data were collected through self-administered online questionnaires, no objective clinical or functional ophthalmological measures (eg, visual acuity, optical coherence tomography (OCT), or visual field testing) were available. Therefore, the results reflect subjective perception rather than clinically verified disease severity. Although diagnoses were self-reported, internal consistency checks were applied, and recruitment through patient associations may have increased the likelihood of prior ophthalmological confirmation; nevertheless, future studies incorporating clinical verification are warranted.
In adjusted analyses, older age emerged as a significant predictor of constant vision concern and general difficulties in daily activities, whereas uveitis status did not retain statistical significance. This is consistent with the known influence of age on visual perception and functional limitations in the general population. Additionally, the modest sample size and absence of objective clinical variables may have reduced statistical power and contributed to residual confounding, with age potentially acting as a proxy for cumulative visual burden. Our findings are consistent with previous studies reporting reduced VRQoL in uveitis.22–26 Hui et al27 and Arriola-Villalobos et al28 reported worse outcomes associated with disease severity and macular involvement, while studies by Tan et al26 and Prem Senthil et al19 highlight the contribution of psychological factors, such as uncertainty and treatment burden, beyond objective visual loss.
Regarding functional impact, our results align with previous reports of limitations in daily activities in patients with uveitis, although variability exists depending on disease subtype and assessment tools.28,29 While generic instruments such as the EuroQol 5-Dimension questionnaire (EQ-5D) may lack sensitivity to detect vision-specific difficulties, our analysis of specific tasks (eg, reading signs, cooking, or finding objects) provides a more detailed perspective. A relevant contribution of this study is the inclusion of driving, a domain rarely addressed despite its importance for autonomy and social participation. Patients with uveitis reported greater driving difficulties, particularly during the day; however, the absence of objective testing prevents linking these findings to specific visual deficits. These perceptions may be related to factors such as glare sensitivity, reduced contrast sensitivity, or visual field alterations described in previous studies,22,23,28 although such mechanisms cannot be confirmed in the present study. The relatively high prevalence of night-driving difficulty among controls further supports the multifactorial nature of these perceptions.
Similarly, in the emotional and social domains, our findings extend previous literature showing reduced well-being in patients with uveitis.22–26 Unlike studies relying on aggregate scores, our analysis provides a more detailed view of specific dimensions, including activity limitation, dependence, and concern about social situations, highlighting the psychosocial burden of the disease. The main limitations of this study include the absence of objective clinical measures, the self-reported diagnosis, the modest sample size, and the regional recruitment, which may limit generalizability, as well as the cross-sectional design, which precludes causal inference. Although self-reported uveitis duration was collected, it was not included in the multivariable models due to the modest sample size and the exploratory nature of the study. In addition, detailed information on systemic medication use, including systemic immunosuppressive therapy, was not collected. Therefore, the potential influence of disease duration and treatment status on vision-related quality of life could not be fully assessed. Nevertheless, the inclusion of a control group and the use of a validated instrument such as the NEI VFQ-25 strengthen the study. Overall, these findings support the importance of integrating patient-reported outcomes and psychosocial considerations into the clinical management of uveitis. Future longitudinal studies combining subjective and objective measures are needed to better understand determinants of VRQoL and to evaluate therapeutic and rehabilitative strategies, as well as to develop more sensitive uveitis-specific PROMs.
Conclusion
This study provides evidence of the self-reported impact of uveitis on vision-related quality of life among Portuguese patients. Our results show that individuals with uveitis report greater ocular pain and face more challenges with driving, as well as in various emotional and social domains, compared to those without the disease. These findings reflect patients’ perceived functional and psychosocial burden and should be interpreted as patient-reported outcomes rather than as indicators of objective clinical severity. In adjusted analyses, some aspects of vision concern and general daily difficulties were more strongly associated with older age than with uveitis status, underscoring the influence of age-related factors and cumulative visual burden on patient-reported outcomes.
Driving was notably affected, with a substantial proportion of patients reporting daytime difficulties, an aspect rarely addressed in the uveitis literature to date and highly relevant for personal autonomy and social independence. However, no conclusions can be drawn regarding the underlying visual or anatomical mechanisms, given the absence of objective clinical-functional assessment.
On an emotional and social level, patients with uveitis experienced higher levels of activity limitation, dependence on others, and feelings of frustration or loss of control. These findings underscore the importance of integrating psychosocial considerations and patient-reported outcomes into the clinical management of uveitis, alongside standard ophthalmological care.
Nevertheless, given the lack of objective ophthalmological data, the present results cannot be used to infer disease severity, inflammatory activity, or structural damage. Future studies integrating subjective patient-reported measures with objective clinical and functional assessments will be essential for developing more personalized and holistic interventions aimed at improving not only visual outcomes but also overall quality of life.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and its Supplementary Information.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the ethical standards set forth in the Declaration of Helsinki and was approved by the Ethics Committee of the Higher Institute of Education and Sciences of Lisbon (ISEC Lisbon) on December 5, 2023 (approval ID: CE/2023/12/05). All participants received detailed information about the study and provided written informed consent prior to their inclusion.
Author Contributions
Ana Paula Oliveira: Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, Resources, Data curation, Writing – original draft, Writing – review & editing, Visualization, Supervision, Project administration. Clara Martinez-Perez: Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, Resources, Data curation, Writing – original draft, Writing – review & editing, Visualization, Supervision, Project administration. Andreia Filipa Gomes: Conceptualization, Data curation, Investigation, Validation, Writing – review & editing. Ana Roque: Conceptualization, Data curation, Investigation, Validation, Writing – review & editing. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Miserocchi E, Fogliato G, Modorati G, Bandello F. Review on the worldwide epidemiology of uveitis. Eur J Ophthalmol. 2013;23(5):705–11. doi:10.5301/ejo.5000278
2. Kirupaharan N, Marshall RF, Spangler MD, Armbrust KR, Berkenstock MK. Incidence and prevalence of uveitis and associated ocular complications in the United States TriNetX Database. Am J Ophthalmol. 2025;276:30–39. doi:10.1016/j.ajo.2025.03.032
3. Felfeli T, Palma L, Rosella L, et al. Contrasting approaches to estimate the epidemiology of uveitis in Canadian health administrative data. Can J Ophthalmol. 2026;61(2):443–450. doi:10.1016/j.jcjo.2025.08.015
4. Dick AD, Tundia N, Sorg R, et al. Risk of ocular complications in patients with noninfectious intermediate uveitis, posterior uveitis, or panuveitis. Ophthalmology. 2016;123(3):655–662. doi:10.1016/j.ophtha.2015.11.007
5. Hermann L, Falcão-Reis F, Figueira L. Epidemiology of uveitis in a tertiary care centre in Portugal. Semin Ophthalmol. 2021;36(1–2):51–57. doi:10.1080/08820538.2020.1803255
6. Bertrand PJ, Jamilloux Y, Ecochard R, et al. Uveitis: autoimmunity… and beyond. Autoimmunity Rev. 2019;18(9):102351. doi:10.1016/j.autrev.2019.102351
7. Bro T, Tallstedt L. Epidemiology of uveitis in a region of southern Sweden. Acta Ophthalmologica. 2020;98(1):32–35. doi:10.1111/aos.14165
8. Bajwa A, Osmanzada D, Osmanzada S, et al. Epidemiology of uveitis in the mid-Atlantic United States. Clin Ophthalmol. 2015;9:889–901. doi:10.2147/OPTH.S81737
9. Tsirouki T, Dastiridou A, Symeonidis C, et al. A focus on the epidemiology of uveitis. Ocul Immunol Inflammation. 2018;26(1):2–16. doi:10.1080/09273948.2016.1196713
10. Tyagi M, Das AV, Kaza H, et al. LV Prasad Eye Institute EyeSmart electronic medical record-based analytics of big data: LEAD-Uveitis Report 1: demographics and clinical features of uveitis in a multi-tier hospital-based network in Southern India. Indian J Ophthalmol. 2022;70(4):1260–1267. doi:10.4103/ijo.IJO_1594_21
11. Chang JHM, Wakefield D. Uveitis: a global perspective. Ocul Immunol Inflammation. 2002;10(4):263–279. doi:10.1076/ocii.10.4.263.15564
12. Jabs DA, Busingye J. Approach to the diagnosis of the uveitides. Am J Ophthalmol. 2013;156(2):228–236. doi:10.1016/j.ajo.2013.03.023
13. Barisani-Asenbauer T, MacA SM, Mejdoubi L, Emminger W, MacHold K, Auer H. Uveitis – a rare disease often associated with systemic diseases and infections: a systematic review of 2619 patients. Orphanet J Rare Dis. 2012;7:57. doi:10.1186/1750-1172-7-57
14. Päivönsalo-Hietanen T, Tuominen J, Saari KM. Uveitis in children: population-based study in Finland. Acta Ophthalmologica Scandinavica. 2000;78(1):84–88. doi:10.1034/j.1600-0420.2000.078001084.x
15. Rosenberg KD, Feuer WJ, Davis JL. Ocular complications of pediatric uveitis. Ophthalmology. 2004;111(12):2299–2306. doi:10.1016/j.ophtha.2004.06.018
16. Maleki A, Anesi SD, Look-Why S, Manhapra A, Foster CS. Pediatric uveitis: a comprehensive review. Surv Ophthalmol. 2022;67(2):217–238. doi:10.1016/j.survophthal.2021.06.008
17. Chan NSW, Choi J, Cheung CMG. Pediatric uveitis. Asia-Pac J Ophthalmol. 2018;7(3):192–199. doi:10.22608/APO.2018145
18. Zhang Z, Griva K, Rojas-Carabali W, et al. Psychosocial well-being and quality of life in uveitis: a review. Ocul Immunol Inflammation. 2024;32(7):1380–1397. doi:10.1080/09273948.2023.2289248
19. Prem Senthil M, Lim L, Braithwaite T, et al. The impact of adult uveitis on quality of life: an exploratory study. Ophthal Epidemiol. 2021;28(5):444–452. doi:10.1080/09286586.2020.1838608
20. Senthil MP, Simon S, Constable PA. A review of patient-reported outcome measures used in uveitis. Surv Ophthalmol. 2023;68(2):225–240. doi:10.1016/j.survophthal.2022.06.006
21. Mangione CM, Lee PP, Gutierrez PR, et al. Development of the 25-item National Eye Institute Visual Function Questionnaire. Archives of Ophthalmology. 2001;119(7):1050–1058. doi:10.1001/archopht.119.7.1050
22. De-La-Torre A, González-López G, Montoya-Gutiérrez JM, Marín-Arango V, Gómez-Marín JE. Quality of life assessment in ocular toxoplasmosis in a Colombian population. Ocul Immunol Inflammation. 2011;19(4):262–266. doi:10.3109/09273948.2011.578583
23. Fabiani C, Vitale A, Orlando I, et al. Impact of uveitis on quality of life: a prospective study from a tertiary referral rheumatology-ophthalmology collaborative uveitis center in Italy. Israel Medical Assoc J. 2017;19(8):478–483.
24. Leske DA, Hatt SR, Wernimont SM, et al. Quality of life and functional vision across pediatric eye conditions assessed using the PedEyeQ. J AAPOS. 2021;25(1):23.e1–23.e6. doi:10.1016/j.jaapos.2020.08.002
25. Maca SM, Wagner J, Weingessel B, Vécsei-Marlovits P. Acute anterior uveitis is associated with depression and reduction of general health. Br J Ophthalmol. 2013;97(3):333–337. doi:10.1136/bjophthalmol-2012-302190
26. Tan P, Koh YT, Wong PY, Teoh SC. Evaluation of the impact of uveitis on visual-related quality of life. Ocul Immunol Inflammation. 2012;20(6):453–459. doi:10.3109/09273948.2012.723114
27. Hui MM, Wakefield D, Patel I, Cvejic E, McCluskey PJ, Chang JH. Visual functioning and health-related quality of life are compromised in patients with uveitis. Ocul Immunol Inflammation. 2017;25(4):486–491. doi:10.3109/09273948.2016.1149579
28. Arriola-Villalobos P, Abásolo L, García-Feijoo J, et al. Vision-related quality of life in patients with non-infectious uveitis: a cross-sectional study. Ocul Immunol Inflammation. 2018;26(5):717–725. doi:10.1080/09273948.2017.1363968
29. Frick KD, Drye LT, Kempen JH, et al. Associations among visual acuity and vision- and health-related quality of life among patients in the multicenter uveitis steroid treatment trial. Invest Ophthalmol Visual Sci. 2012;53(3):1169–1176. doi:10.1167/iovs.11-8507
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Living Through Sweat: A Qualitative Study of the Pre-Surgical Decision-Making Trajectory in Patients with Palmar Hyperhidrosis
Yan M, Chao S, Yu L, Liu C, Li Z, Gong L, Bao B, You S, Zhang G, Ren Y, Du G
Patient Preference and Adherence 2026, 20:589191
Published Date: 4 May 2026
Quality of Life Following Rhegmatogenous Retinal Detachment: A Systematic Review and Meta-Analysis
Sriranganathan A, Abdul-Hay MJ, Diaz Martinez JP, Felfeli T
Clinical Ophthalmology 2026, 20:590040
Published Date: 27 May 2026