Back to Journals » Clinical Optometry » Volume 14
Self-Reported Student Awareness and Prevalence of Computer Vision Syndrome During COVID-19 Pandemic at Al-Baha University
Authors Alatawi SK ![]() , Allinjawi K, Alzahrani K
, Allinjawi K, Alzahrani K ![]() , Hussien NK, Bashir M, Ramadan EN
, Hussien NK, Bashir M, Ramadan EN
Received 24 May 2022
Accepted for publication 6 September 2022
Published 19 September 2022 Volume 2022:14 Pages 159—172
DOI https://doi.org/10.2147/OPTO.S374837
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Mr Simon Berry
Saleha K Alatawi,1 Kareem Allinjawi,2 Khaled Alzahrani,3 Naglaa K Hussien,4 Mahadi Bashir,5 Eman N Ramadan6
1Department of Optometry, Faculty of Applied Medical Sciences, Al-Baha University, Al-Baha, Saudi Arabia; 2Department of Optometry, Faculty of Applied Medical Sciences, Jeddah University, Jeddah, Saudi Arabia; 3Ophthalmology Department, King Fahad Armed Forces Hospital, Jeddah, Saudi Arabia; 4Department of Nursing, Faculty of Applied Medical Sciences, Al-Baha University, Al-Baha, Saudi Arabia; 5Consultant of Ophthalmology, Faculty of Medicine, Al-Baha University, Al-Baha, Saudi Arabia; 6Department of Public Health, Faculty of Applied Medical Sciences, Al-Baha University, Al-Baha, Saudi Arabia
Correspondence: Saleha K Alatawi, Department of Optometry, Faculty of Applied Medical Sciences, Al-Baha University, Saudi Arabia, Email [email protected]
Background: The rapid increase increased, in using of video display terminals during the COVID-19 pandemic predisposes users to a variety of health problems restricted to visual problems and including various musculoskeletal problems, collectively known as computer vision syndrome (CVS) or computer vision syndrome.
Aim: This study aims to ascertain university students’ awareness of computer vision syndrome at Al-Baha University, including the nature, sources, accuracy, and completeness of information, as well as the attitudes towards CVS, and mitigative practices.
Methods: This study used a descriptive cross-sectional design and a convenient sample of 310 (80.0% male) students drawn from Al Baha University campuses. Data were collected using self-administered questionnaires.
Results: The mean age of the participants was 23.51 years (SD=5.42). The results show that 78.7%, 66.1%, and 11.6% received CVS information from social media, mass media, and family, respectfully. Despite 70% of respondents being aware of CVS manifestations, between 42% to 67% of those sampled had accurate and complete information about the meaning, causes, prevention, and management of the syndrome. More than a third of the participants had either a good (62.9%) or average (29%) total knowledge of CVS. Less than 15% had incorrect information. On average, 62.5% of respondents engaged in preventive or mitigative behaviours/activities as opposed to 37.5% who did not, but only 44% believed CVS was a serious health threat. 65.2% of the studied students had a satisfactory total practice score. The regression analysis showed that the coefficients of marital status and faculty were a statistically significant association with the total knowledge score.
Conclusion: CVS awareness is acceptably high, but there is a low preventive/mitigative behaviors as well as a low realization of CVS’ long-term health problems. This is why increasing CVS awareness and implementing interventions such as the 20-20-20 rule could be effective at Al Baha University.
Keywords: awareness, computer vision syndrome, COVID-19 pandemic
A Letter to the Editor has been published for this article.
Introduction
Computer Vision Syndrome
There has been a rapid increase in the use of digital devices among students in Saudi Arabia, as elsewhere in the world.1,2 It is highly likely that even with the post-pandemic return to normalcy, the utilization of some forms of virtual instruction approaches would continue, at least in the short term.3 Heightened student screen time is a risk factor for multiple eye problems, key of which is computer vision syndrome (CVS).4,5 CVS describes a complex of vision- and eye-related symptoms caused by prolonged use of high-resolution digital display terminals.6 Other than the difficulties focusing on pixels, any activities that strain near vision, often during or in conjunction with the use of digital devices (such as display quality, lighting, radiation, refresh rates, and visual ergonomics), can cause or contribute to the development of CVS.7,8 It’s estimated to affect 60 million people globally with a million new cases annually.8 About 70% of people who spend at least two hours a day (15 hours/week) using digital screens present with CVS symptoms.8,9 Its prevalence among regular computer users can reach as high as 90%.10
CVS develops due to the dissimilarity in the human eyes’ focusing mechanism for digital screens and printed text.11,12 Digital devices need to be held at a distance between distant and near vision, effectively straining the visual system, as it is designed for comfortable near and distant vision.12,13 More specifically, printed texts and texts on digital screens are different in terms of gaze angles, viewing distances, appearance, blinking rates, movement of the palpebral fissure, and accommodative demands. While digital texts comprise pixels created from electronic beams striking a phosphor-coated screen surface, the printed text comprises clearly defined and stable characters throughout its surface. As individual pixels are brighter at the center than at their periphery, human eyes cannot sustain focus on characters created by pixels. Focussing tends to lag behind computer screens because of the vertical gaze position.12
Consequently, the eyes repeatedly struggle to gain and maintain a focus of the pixels, which action of the ciliary body fatigues the eyes, causing the accommodative problems associated with CVS.12 Prolonged use of digital devices not only strains the visual system, but13,14 it also induces musculoskeletal strain and circadian disturbances.14,15 The syndrome presents with headaches itching, eye strain/asthenopia, blurred vision, dry eyes, and shoulder/neck pains. External symptoms of ache, headache, and strain are primarily associated with binocular and/or accommodative vision stress.5,11,12,16
The available evidence suggests that as little as two hours of sustained digital device usage a day is likely to develop a range of vision-related problems.4,17,18 Reddy et al, Mohan, et al and Iqbal et al estimated that CVS affected between 50% and 90% of students taking virtual classes in the Middle East.5,18,19 CVS is categorized into four strains: asthenopic CVS (manifests as eye strain, eye dryness, soreness, headache, and fatigue), ocular surface CVS (dryness, grittiness, irritation, redness, burning sensation, and heaviness often due to environmental factors, blinking rates, and use of lenses/glasses), visual CVS (double or blurred vision, presbyopia, and slow focus change), and extraocular CVS (musculoskeletal pain).7,20
Aim
To ascertain university students’ awareness of computer vision syndrome at Al-Baha University.
Objectives
- To determine the sources of information about CVS for students at Al Baha University.
- To determine the nature, accuracy, and completeness of information about CVS among students at Al Baha University.
- To determine the attitudes towards, and practices to prevent or mitigate, CVS among students at Al Baha University.
Research Questions
- What are the sources of information about CVS for students at Al Baha University?
- What is the nature, accuracy, and completeness of information about CVS among students at Al Baha University?
- What are the attitudes towards, and practices to prevent or mitigate, CVS among students at Al Baha University?
Significance
The fact that the community prevalence of CVS is 22.3–39.8%,21 compared to 70.6–78% among students attending online classes during the COVID-19 pandemic, points to the magnitude of the problem.22 With the increasing use of digital display terminals, particularly among populations that are occupationally dependent on the same, increased CVS prevalence is a serious public health concern.4,19 CVS eats into the physical and mental well-being as well as the productivity of digital device users.5 Even so, despite the mild nature of the syndrome and the fact that most onsets are self-limited and/or managed by optometrists/general practitioners, its awareness remains relatively low.23 With millions of students intensifying the usage of digital devices in their learning as well as for entertainment purposes, CVS is likely to be a pressing public health crisis for as long as the world remains in the grip of the COVID-19 pandemic. Its prevalence varies depending on demographic, environmental, and contextual factors,5 such that Al Baha University is likely to have different prevalence rates. Without knowledge of prevalence rates and awareness of the same, targeted, effective, and efficient interventions are impossible.
Methods
Research Design
This study relies on a descriptive cross-sectional design. Al-Baha University was selected as a case organization both because it is convenient for the researcher and it is medium-sized compared to all universities in Saudi Arabia. As such, it is arguably representative of the field.
Research Strategy
This study uses a KAP survey strategy. It seeks to investigate the students’ knowledge, attitudes, and practices concerning CVS, using a standardized questionnaire.24 This strategy potentially reveals understanding and misconceptions that encourage, support or hinder instrumental preventive or mitigative behaviors. It highlights what the students know or think, and the gap between their knowledge and the behaviors that are desired to prevent or mitigate CVS.25 This way, it’s possible to measure the situation; improve knowledge, attitudes, and practices; set a baseline for future studies, particularly to measure the effectiveness of interventions; and help recommend interventions.26
Population and Context
Al-Baha University is a public university situated in Al-Baha city, Southern Region, Saudi Arabia. The University has a student population of 21,000 spread across its five campuses across four towns. The main campus hosts 16 faculties. It offers more than 40 programs (30 undergraduate and 10 postgraduate).27
Sampling Strategy
A convenience sample of students was drawn from all 16 faculties at Al-Baha University from November 2021 to February 2022. Having received the requisite permissions from gatekeepers, the researchers visited the campuses and physically approached students at random, to invite them to participate in the study by providing them with the information sheet, invitation sheets, and questionnaires. All students who were willing and able to participate in the study during the data collection period completed the questionnaires. At the end of the data collection process, 310 students had returned completed questionnaires.
Data Collection Instruments
The data was collected using a four-part structured questionnaire. The first section sought to collect demographic data, including gender, age, marital status, residence, the university faculty to which they belong, number of siblings, and year of study. The second section sought to collect data on the subjects’ knowledge of CVS, including its definition, causes, signs, symptoms, risk factors, complications, treatment, prevention, and source of information about the disease. The knowledge was scored on a Likert Scale with zero (0) denoting incorrect or no knowledge, one (1) denoting a correct and incomplete answer, and two (2) denoting a correct and complete answer.
The total knowledge scores were good if the score of the total knowledge was≥ 75%, considered average if it equals 50–75%, and considered poor if it equals or less than 50%. The third section sought to gather information on the students’ practices to prevent their vision strains at home, reduce students’ vision exposure to blue light from digital devices, manage screen time and encourage alternative physical activity. The students’ practices were scored on a binary scale of either one (1) to denote a practice that the students engaged in regularly or zero (0) to denote a practice in which the students hardly engaged. The total reported practice score was considered satisfactory if the score of the total practices ≥ 60%, while considered unsatisfactory if it is <60%.
The last section of the questionnaire measured the students’ attitude toward Computer vision syndrome at Al-Baha University during the COVID-19 pandemic. The scoring system for the student’s attitude is calculated as follows: (2) score for a positive response, (1) score for a neutral response, and (0) score for a negative response. The total attitude scores were considered positive if the score of the total attitude was≥ 75% while considered negative if it is less than 75%.
Data Analysis
The data was cleaned, coded, and entered into Microsoft Excel. It was subsequently analyzed using the Statistical Package for Social Sciences version 20.0. Both descriptive and inferential statistics were obtained and presented in suitable formats, including tables and charts. The statistical significance of relationships among categorical variables was tested using the Chi-Square test (p<0.05).
Ethical Considerations
This study’s protocols were reviewed and approved by the ethics review authorities at the Al-Baha University and conducted in line with the standards set out in the 1964 Declaration of Helsinki. Approval letters were obtained from the deans of the male and female faculties, setting out the purposes of the study, inviting cooperation from potential participants, and for the data to be collected. Key considerations included a requirement for informed consent as a prerequisite for participation in the study. The participants were given an orientation about the purposes of the study and had their concerns addressed. Further, the participants were anonymized, and all the information gathered was not only kept confidential but was only used for this study.
Results
Participants
A total of 310 valid questionnaires (mean ± SD 23.51±5.42 years and 80% males) were returned. The majority were married (83/9%), resided in rural areas (86.5%), and were in their second year of study (33.3%). The demographic characteristics of the respondents are summarised in Table 1.
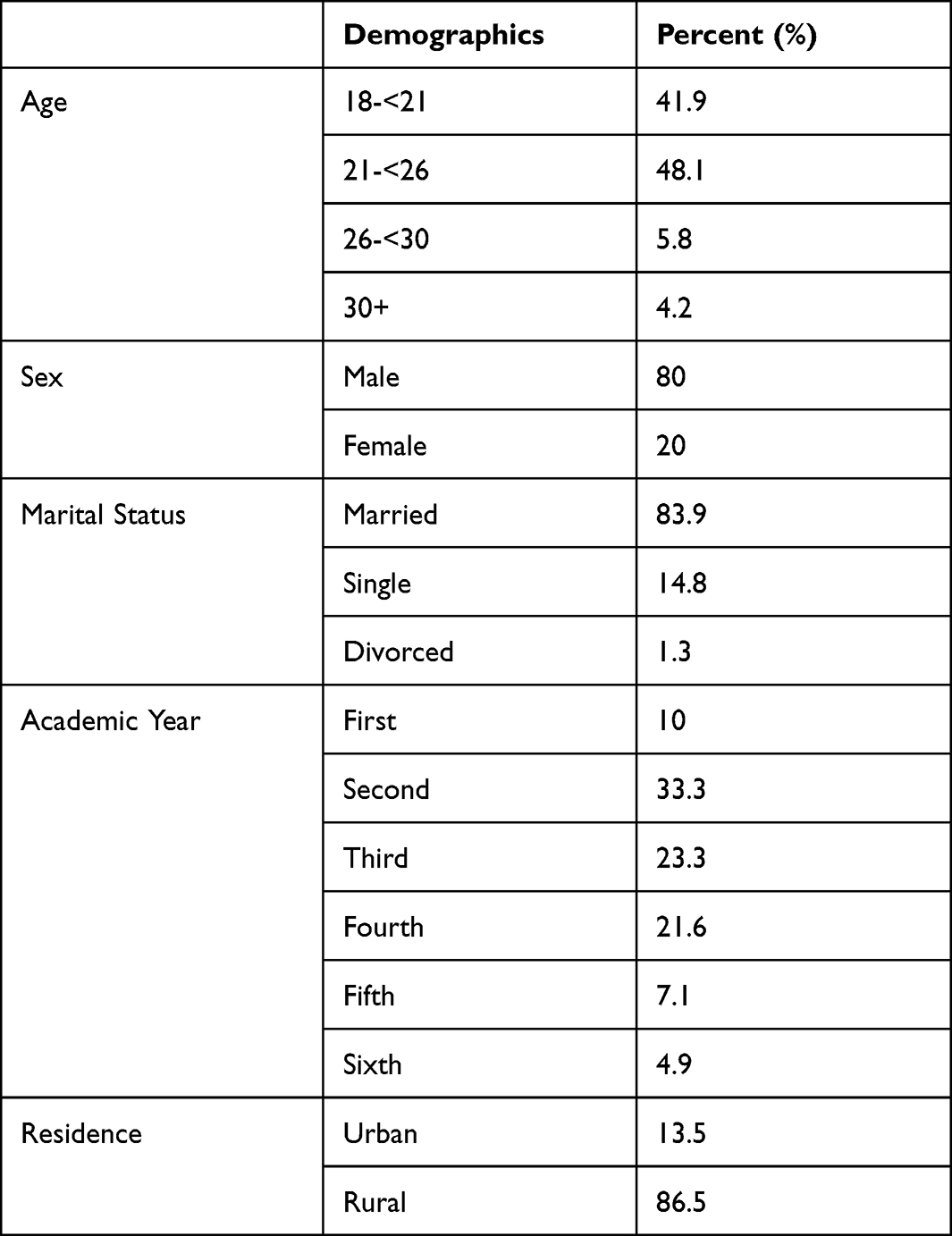 |
Table 1 The Frequency Distribution of Studied Students Regarding Their Personal Characteristics’ (n=310) |
Of the respondents, 25.8%, 12.9%, and 11.6% were drawn from the faculty of Applied Medical Science, Faculty of Arts and Humanities, and Community College, respectively. See Figure 1.
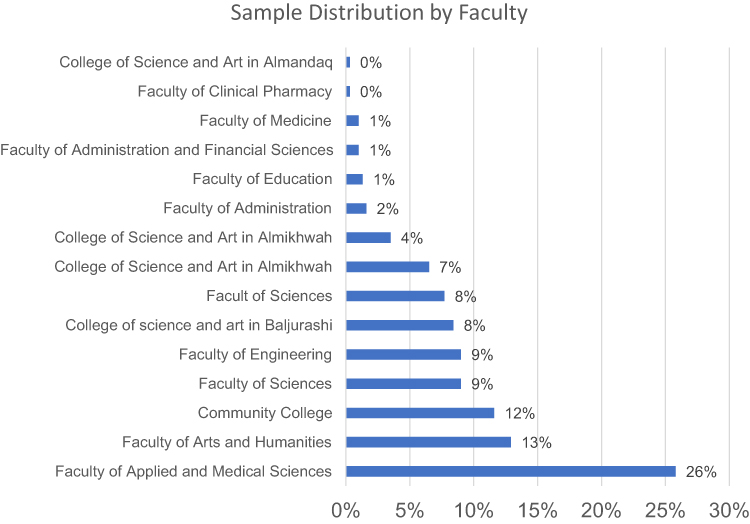 |
Figure 1 Percentage distribution of studied students regarding their faculty (n=310). |
Sources of Information on CVS
Concerning the primary sources of information, 78.7% of the respondents indicated that they primarily obtained their information from social media, while 66.1% and 11.6% said that they relied on mass media and family/friends, respectfully. See Figure 2.
 |
Figure 2 Percentage distribution of studied students regarding their source of information computer vision syndrome (n=310). |
Accuracy and Completeness of Information
The results indicated that 42.9% of the students included in the study wholly and perfectly understood the meaning of computer vision syndrome. In contrast, many students had an incomplete but correct understanding of the condition. The remaining 14.5% of the population had an incorrect understanding of computer vision syndrome. The knowledge of the causes and prevention of computer vision syndrome was comparably higher, with just 4.5% and 35.5% of those surveyed having incorrect or incomplete knowledge about causes, respectfully. Just 6.5% and 25.8% of the respondents had inaccurate or incomplete knowledge of how to prevent computer vision syndrome. Up to 70.3% of the respondents were aware of CVS symptoms, while 23.2% and 6.5% had incomplete or incorrect knowledge, respectively. See Table 2.
 |
Table 2 Frequency Distribution of Studied Students Regarding Their Knowledge About Computer Vision Syndrome (n=310) |
Total Knowledge Score
The results show that 62.9% of the students had a good total knowledge score about CVS, while 29% and 8.1% had average and poor total knowledge scores, respectively.
Total Knowledge Level
At a 5% significance level, the Chi-square test findings showed that the coefficients of the total knowledge level variation across age, residence, academic year, and gender, are not statistically significant. The variation in the coefficient of the total knowledge level is positive and statistically significant for single marital status and medical faculty. See the Table 3.
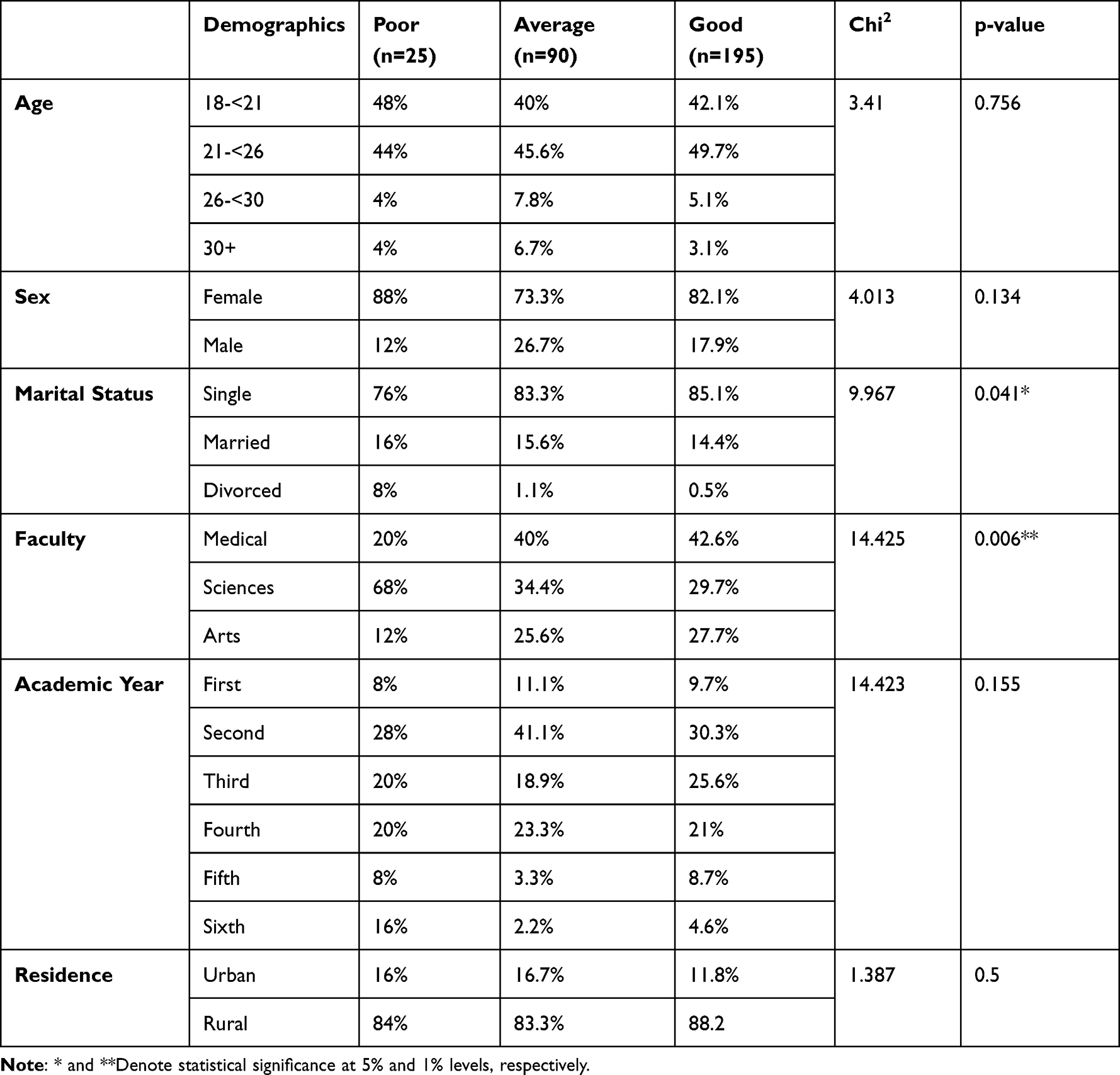 |
Table 3 Statistically Relation Between Total Knowledge Level and Personal Characteristics Among Studied Students |
Attitudes Towards, and Practices to Prevent or Mitigate, CVS
Preventive and Mitigative Practices
The results show that 76.5% of the students included in the study adjusted the lighting and often blinked to mitigate computer vision syndrome. More than 60.0% of the participants either took regular eye breaks or checked the position of their digital display, while 57.7% adjusted their seating positions. See Table 4.
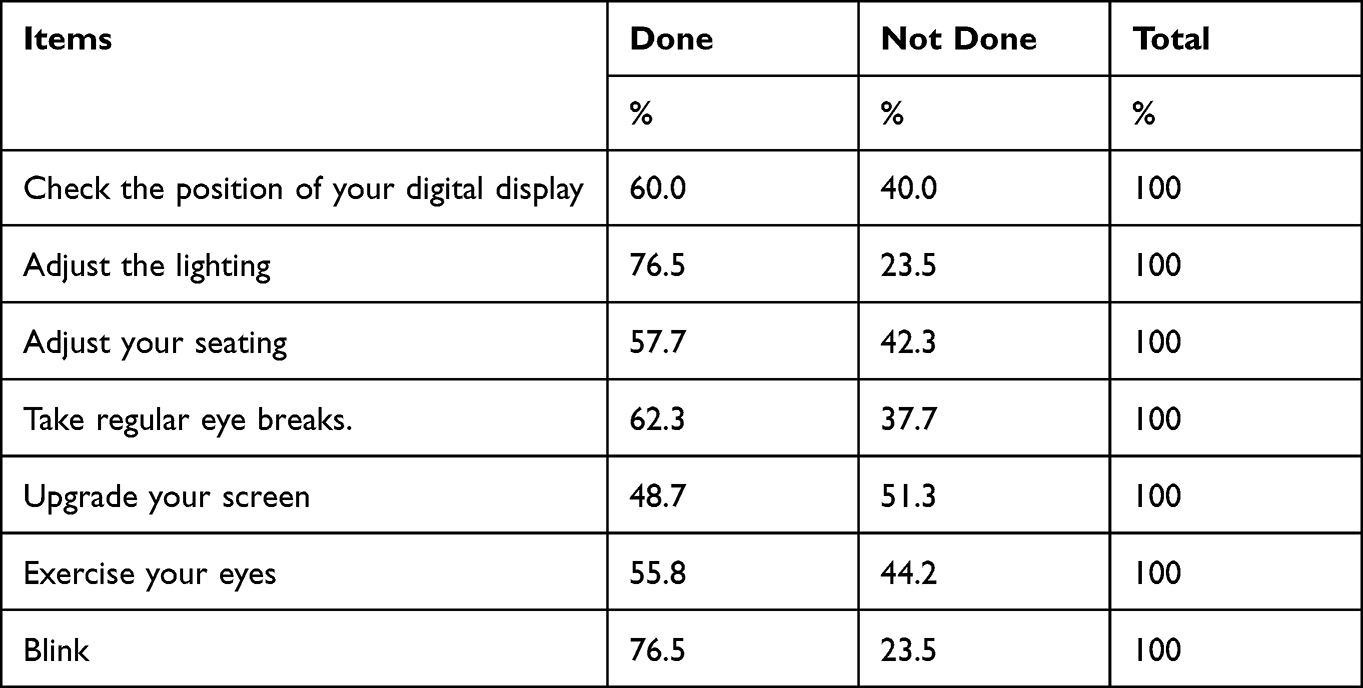 |
Table 4 Frequency Distribution of Studied Students Regarding Their Practices Toward Computer Vision Syndrome (n=310) |
Attitudes Towards CVS
The results show that 65.2% of the studied students had satisfactory total practice scores for CVS while 34.8% had unsatisfactory total practice scores for CVS. The results reveal that 67.7%, 64.5%, and 63.2% agree computer vision syndrome awareness helps one avoid developing the condition, ensures the correct use of computers can prevent one from developing CVS, and that any person is at risk of developing computer vision syndrome. See Table 5.
 |
Table 5 Frequency Distribution of Studied Students Regarding Their Attitude Toward Computer Vision Syndrome (n=310) |
Further, 53.2% of the studied students had a positive total attitude score toward computer vision syndrome while 46.8% of them had a negative total attitude score toward computer vision syndrome.
Total Practice Level
At a 5% significance level, the Chi-square test showed that the coefficient of the first academic year is a positive and statistically significant association with the total level of practice. The same is true of the coefficient of both the 18–21 age group and the female gender. See Table 6.
 |
Table 6 Statistically Relation Between Total Practices Level and Personal Characteristics Among Studied Students |
At a 5% significance level, the Chi-square test showed that there was no statistically significant relation between the coefficient of personal characteristics of the studied sample and their total level of attitude toward CVS. See Table 7.
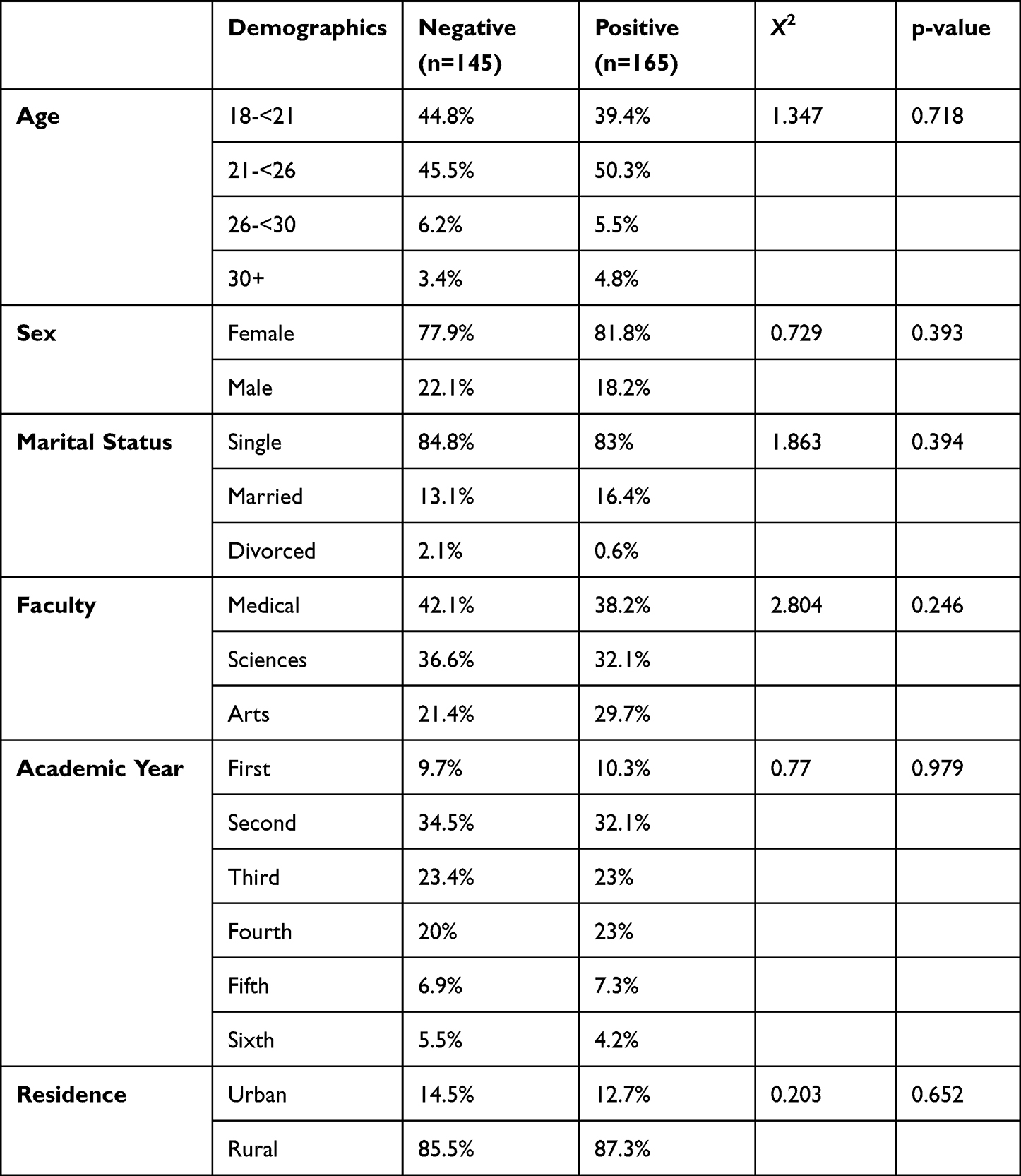 |
Table 7 Statistically Relation Between Total Attitude Level and Personal Characteristics Among Studied Students |
At a 5% significance level, the results show that there was a statistically significant correlation between total level knowledge and attitude among studied students and a statistically significant correlation between total practice and attitude. See Table 8.
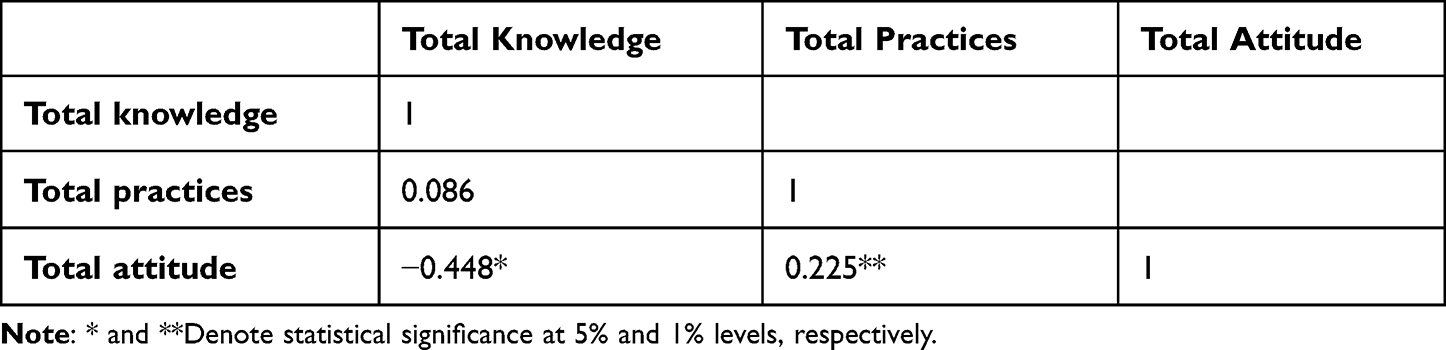 |
Table 8 Correlation Matrix Between Total Level Knowledge, Practices, and Attitude Among Studied Students |
Discussion
Sources of Information About CVS
The sources of information about CVS and other health risks are important, as they offer a pointer to the possible channels of directing public health campaigns to the students.28 The findings show that more than 78% and 65% got their information from social media and mass media, respectively, while 11.6% relied on family and friends. While this heavily depends on demographics and available communication technologies,29 the results show that there is immense potential to use social media and family/friends to create awareness about CVS. This is all the more so because it appears that the information available to the students at Al Baha University is acceptably accurate. The heavy reliance on social media and family, as against mass media, is explainable by the relatively young sample and the reach/popularity of social media among college students in Saudi Arabia.8 This is likely to change with different demographics. Even so, the results show immense potential for Al Baha University and other universities in Saudi Arabia to deploy social media resources to create CVS awareness among students.
Institutions could use own mass media (university radios/TV stations) or locally-tailored ads on mainstream media,30 even though Jamieson argues that mass media is inefficient for micro-targeting. While the word of mouth (eg, teachers/lecturers) is easily one of the most effective in producing functional changes,31 particularly the already high awareness of CVS, the low reliance on it points to dubious effectiveness.29 According to Brownson et al, Heldman et al and Gatewood et al, social media could be very effective and efficient as it has tools for micro-targeting users depending on their attributes, including their screen time and website cookies.31–33 The potential for misinformation, astroturfing, and lower premium on social media information is such that there are still substantial uncertainties on the best ways to utilize in disseminating evidence-based research to ensure effective implementation.31
It is critical to note that delivering information alone is not adequate. There is often a gap between information acquisition of public health information and its actual application in practice on one hand and policy development on the other.29,31 This is because of ineffective information dissemination, which is, in turn, a function of the failure to take into account the messaging, sources, audiences, and channels.31
Nature, Accuracy, and Completeness of Information About CVS
The results show that the awareness of CVS and its symptoms is acceptably good, but also that there is immense potential for improvement. This is particularly so in respect to the meaning of CVS, causes, prevention, and management, in which respect, incomplete or inaccurate information is unacceptably high. Increasing good total knowledge scores above 62% should be helpful. This study similarly reveals important demographic variables that could be targeted for increased effectiveness in creating awareness about CVS.
Generally, CVS prevalence is associated with people who do not observe the 20-20-20 rule and those with pre-existing eye conditions, poor ergonomics, and higher screen time. In addition to the use of more than one device, older age, employment status, sedentary lifestyles, usage of re-wetting drops, gender, and optical correction.8,17,22,34–36 It’s notable, however, that self-reported awareness/complaints may be misleading in the absence of clinical assessments, particularly given leading responses in the questionnaire. Iqbal et al’s study of 4030 medical students drawn from five universities in Egypt, for example, found that while self-reported awareness of CVS was 84.8%, ophthalmic assessments of the same respondents showed only 56% prevalence. This is all the more so because this study involved medical students, whose awareness scores should be closer to clinically assessed scores.17
Total Knowledge Level and Demographic Characteristics
The total knowledge level is above average across all demographic attributes. This study found no statistically significant variation across all tested demographic attributes except the medical faculty and marital status. The study’s findings show that the total knowledge level is likely to be higher among medical students is partly explainable by the likelihood of higher medical and public health knowledge/awareness.37,38 Students who are married or are drawn from the Medical faculty, are likely to have better knowledge of CVS. Accordingly, awareness campaigns should be more targeted using variables that were not statistically significant, including age, gender, year of study, and area of residence.
This is, however, contrary to the finding by both Kumar et al and Garg et al, that only 20% and 39.9%, respectively, of medical students, were aware of CVS.18,39 It’s similarly difficult to explain the apparent higher knowledge level among married students, but it’s impossible to exclude the potential of sampling errors given the fact that only 14.8% and 20% of the sample were single and female, respectfully, which are not reflective of the population parameters and susceptible to the effect of outliers.21,40 In Mohan Kumar et al, Das and Dubey Kumar et al and Garg et al, female student participants were 50%, 47%, 23.3%, and 37.38%, respectfully.5,18,39,41
Attitudes Towards, and Practices to Prevent or Mitigate, CVS
Instrumental Behaviors
This study’s findings show that the knowledge of the causes, risk factors, symptoms/signs, and prevention of CVS, including the accuracy and completeness of information about CVS is acceptably high, and the same appears to be matched by instrumental behaviors to either prevent or treat the syndrome. The awareness level in this study is considerably higher than was the case in studies such as Garg et al and Kumar et al.5,39
The findings show that about the same proportion of students as those with accurate and complete knowledge about CVS engaged in behaviors consistent with mitigating CVS, including adjusting display settings, seating positions, taking frequent breaks, blinking, and exercising eyes. A proportionate number of participants believe at such knowledge is essential in preventing CVS is a further pointer to the necessity of bolstering such knowledge among high-risk populations such as students undertaking virtual classes during lockdowns.23,35 Effectively, this study’s shows at creating awareness is likely to enhance preventive and mitigative behaviours, thereby reducing CVS prevalence among students.
This is contrary to Garg et al and Mohan et al, which found awareness levels of 40% and only instrumental behaviors among 10% of the sample. Notably, this finding is not based on a causal relationship between knowledge of CVS and instrumental behavior to prevent/mitigate the same.18,42 As such, it is not possible to deduce infer whether the instrumental behaviors observed among the participants are related to CVS or are caused by other factors.40 The available literature on the blink rate, blink amplitude, and tear volume during digital device usage is inconclusive.10,23 Clearly, more research along the lines of Loh and Redd on the precise causal mechanisms/processes for CVS (eg, extraocular, accommodative, and ocular surface mechanisms’ adaptations to digital devices’ visual effects) could help develop and improve awareness, prevention, and treatment.4,10,19
Despite the majority of the participants knowing that anyone could develop CVS and have a positive total attitude score, the findings show that less than a third considered CVS a serious health risk. In addition, more than half only cared about CVS once they developed serious symptoms. The majority of respondents are alive to the fact that the correct use of computers can prevent/mitigate CVS. Patient education is critical to ensuring proper ergonomics, computer usage, and other behavioral changes necessary to prevent or mitigate CVS.19
Total Practice Level
The sampling bias could yet account for the statistically significant, positive coefficient of the total knowledge area for female participants included in the sample.42 It is curious, however, that the coefficients for first-year students and the 18–21 age group are positive and statistically significant, while those of the subsequent age groups and schooling year, even though the sample representation is, on face value, comparable to other clusters. Without further research, it is difficult to rule out sampling bias.40,43 It is notable, however, that the total knowledge area is matched by the total practice level, except for the medical faculty, implying that increasing the total knowledge level is likely to increase instrumental behavior to prevent or mitigate CVS. Just like Garg et al and Mohan et al, which did not undertake inferential statistics, the findings show that instrumental behaviors are positively associated with awareness.18,42
Total Attitude Level and Demographics
This study’s findings show that the total attitude level is not related to any of the tested demographic attributes. This is consistent with the 53.2% positive and 46/8% negative total attitude score toward CVS. It’s arguable at attitudes can be tailored towards those that can foster instrumental behaviors to prevent or mitigate CVS, with increased awareness.15 This finding is consistent with Amirul et al, which found a statistically significant relationship between attitudes, knowledge, and practice of CVS.44 This is consistent with the findings that the correlation between total level knowledge and attitude among studied students and a highly significant correlation between total practice and attitude.18,44
Conclusion
Increased reliance on virtual learning at Al Baha University and other universities in Saudi Arabia is likely to increase screen times for students and lecturers,2,17,18 with implications for CVS prevalence.10 This study shows that the awareness of CVS among students at Al Baha University is acceptably high, but could be improved, particularly by narrowing the gap between awareness and practice. Demographic variables that did not have a statistically significant association with either knowledge or practice could be targeted in order to enhance effectiveness. Based on the findings of the present study, the following recommendations were suggested:
- Educational strategy to raise awareness among all Al-Baha University students in all facilities, all departments, and all levels toward computer vision syndrome.
Further Research
- Virtual teaching resources and teachers should incorporate information and reminders to students to engage in desired behavior to prevent/mitigate CVS, such as suggestions to adjust seating, display settings, and take breaks.23,35 Targeted ads and social media content can similarly be used to achieve similar ends.29,31
- Well-regarded and fact-based blogs as well as other social media handles/pages/channels can establish authority and enhance social media influence. These must be tailored to the community’s uniqueness and messages must be grounded in the conversations that occur in those very communities.29,31
- With or without awareness, early visual assessments of students who face a heightened risk of CVS, eg, due to mandated virtual learning, could help attain earlier/proper diagnosis and trigger effective management.6 Institutions could facilitate these checks and/or directly recommend them to their students.
- Mandated breaks and reduced hours of online lessons, of 10 minutes per hour, should be introduced for online learning sessions.35,42
- Public service campaigns should be introduced at the institutional and other higher levels to encourage reducing screen time and increasing physical activity, abiding by the 20-20-20 rule, utilizing rewetting solutions, proper ergonomics, and other evidence-based interventions to mitigate the symptoms.21,22
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organisation. Numbers at a glance; 2021. Avaiable from: https://www.who.int/emergencies/diseases/novel-coronavirus–2019.
2. Viner RM, Russell SJ, Croker H, et al. School closure and management practices during coronavirus outbreaks including COVID-19: a rapid systematic review. Lancet Child Adolesc Health. 2020;4(5):397–404. doi:10.1016/S2352-4642(20)30095-X
3. UNESCO. COVID-19 impact on education; 2021. Avaiable from: vhttps://en.unesco.org/covid19/educationresponse#schoolclosures.
4. Reddy SC, Low C, Lim Y, Low L, Mardina F, Nursaleha M. Computer vision syndrome: a study of knowledge and practices in university students. Nepal J Ophthalmol. 2013;5(2):161–168. doi:10.3126/nepjoph.v5i2.8707
5. Mohan A, Sen P, Shah C, Jain E, Jain S. Prevalence and risk factor assessment of digital eye strain among children using online e-learning during the COVID-19 pandemic: digital eye strain among kids (DESK study-1). Indian J Ophthalmol. 2021;69(1):140. doi:10.4103/ijo.IJO_2535_20
6. Zalat MM, Amer SM, Wassif GA, El Tarhouny SA, Mansour TM. Computer vision syndrome, visual ergonomics and amelioration among staff members in a Saudi medical college. Int J Occupat Safety Ergonom. 2022;28(2):1033–1041. doi:10.1080/10803548.2021.1877928
7. Basnet A, Basnet P, Karki P, Shrestha S. Computer vision syndrome prevalence and associated factors among the medical student in Kist Medical College. Nepal Med J. 2018;1(1):29–31. doi:10.3126/nmj.v1i1.20396
8. Adane F, Alamneh YM, Desta M. Computer vision syndrome and predictors among computer users in Ethiopia: a systematic review and meta-analysis. Trop Med Health. 2022;50(1):26. doi:10.1186/s41182-022-00418-3
9. Charpe NA, Kaushik V. Computer Vision Syndrome (CVS): recognition and control in software professionals. J Human Ecol. 2009;28(1):67–69. doi:10.1080/09709274.2009.11906219
10. Blehm C, Vishnu S, Khattak A, Mitra S, Yee RW. Computer vision syndrome: a review. Surv Ophthalmol. 2005;50(3):253–262. doi:10.1016/j.survophthal.2005.02.008
11. Sheppard AL, Wolffsohn JS. Digital eye strain: prevalence, measurement and amelioration. BMJ Open Ophthalmol. 2018;3(1):e000146. doi:10.1136/bmjophth-2018-000146
12. Alemayehu AM. Pathophysiologic mechanisms of computer vision syndrome and its prevention: review. World J Ophthalmol Vision Res. 2019;2(5). doi:10.33552/WJOVR.2019.02.000547
13. Portello JK, Rosenfield M, Bababekova Y, Estrada JM, Leon A. Computer-related visual symptoms in office workers. Ophthal Physiol Optics. 2012;32(5):375–382. doi:10.1111/j.1475-1313.2012.00925.x
14. Mowatt L, Gordon C, Santosh ABR, Jones T. Computer vision syndrome and ergonomic practices among undergraduate university students. Int J Clin Pract. 2018;72(1):e13035. doi:10.1111/ijcp.13035
15. Boadi-Kusi SB, Adueming POW, Hammond FA, Antiri EO. Computer vision syndrome and its associated ergonomic factors among bank workers. Int J Occupat Safety Ergonom. 2022;28(2):1219–1226. doi:10.1080/10803548.2021.1897260
16. Assefa NL, Weldemichael D, Alemu H, Anbesse DH. Prevalence and associated factors of computer vision syndrome among bank workers in Gondar City, northwest Ethiopia, 2015. Clin Optomet. 2017;9:67–76. doi:10.2147/OPTO.S126366
17. Iqbal M, Elzembely H, Elmassry A, et al. Computer vision syndrome prevalence and ocular sequelae among medical students: a university-wide study on a marginalized visual security issue. Open Ophthalmol J. 2021;15(1):156–170. doi:10.2174/1874364102115010156
18. Mohan Kumar B, Thiruvalluvan G, Arjunan M. Effectiveness on knowledge about computer vision syndrome among medical coding trainee in medical coding training institute in urban Chennai, Tamil Nadu – a cross- sectional study. J Fam Med Prim Care. 2021;10(1):228. doi:10.4103/jfmpc.jfmpc_1151_20
19. Loh KY, Redd SC. Understanding and preventing computer vision syndrome. Malays Fam Physician. 2008;3(3):128–130.
20. Alhasan AS, Aalam WA. Magnitude and determinants of computer vision syndrome among radiologists in Saudi Arabia: a national survey. Acad Radiol. 2021. doi:10.1016/j.acra.2021.10.023
21. Bhattacharya S, Saleem S, Singh A. Digital eye strain in the era of COVID-19 pandemic: an emerging public health threat. Indian J Ophthalmol. 2020;68(8):1709. doi:10.4103/ijo.IJO_1782_20
22. Alabdulkader B. Effect of digital device use during COVID-19 on digital eye strain. Clin Exp Optomet. 2021;104(6):698–704. doi:10.1080/08164622.2021.1878843
23. Jaiswal S, Asper L, Long J, Lee A, Harrison K, Golebiowski B. Ocular and visual discomfort associated with smartphones, tablets and computers: what we do and do not know. Clin Exp Optomet. 2019;102(5):463–477. doi:10.1111/cxo.12851
24. Saunders M, Lewis P, Thornhill A. Research Methods for Business Students. Pearson Education; 2018.
25. Wang R, Yang Y, Chen R, et al. Knowledge, Attitudes, and Practices (KAP) of the relationship between air pollution and children’s respiratory health in Shanghai, China. Int J Environ Res Public Health. 2015;12(2):1834–1848. doi:10.3390/ijerph120201834
26. USAID. The KAP survey model (knowledge, attitudes, & practices); 2012. Available from: https://www.spring-nutrition.org/sites/default/files/publications/annotation/spring_kap_survey_model_0.pdf.
27. Al Baha University. Albaha University from https://bu.edu.sa/ar/home. Accessed September 14, 2022.
28. Thackeray R, Neiger BL, Smith AK, van Wagenen SB. Adoption and use of social media among public health departments. BMC Public Health. 2012;12(1):242. doi:10.1186/1471-2458-12-242
29. Bernhardt JM, Mays D, Kreuter MW. Dissemination 2.0: closing the gap between knowledge and practice with new media and marketing. J Health Commun. 2011;16(sup1):32–44. doi:10.1080/10810730.2011.593608
30. Bayer J. Double harm to voters: data-driven micro-targeting and democratic public discourse. Internet Policy Rev. 2020;9(1). doi:10.14763/2020.1.1460
31. Gatewood J, Monks SL, Singletary CR, Vidrascu E, Moore JB. Social media in public health: strategies to distill, package, and disseminate public health research. J Public Health Manage Pract. 2020;26(5):489–492. doi:10.1097/PHH.0000000000001096
32. Heldman AB, Schindelar J, Weaver JB. Social media engagement and public health communication: implications for public health organizations being truly “social”. Public Health Rev. 2013;35(1):13. doi:10.1007/BF03391698
33. Brownson RC, Eyler AA, Harris JK, Moore JB, Tabak RG. Getting the word out: new approaches for disseminating public health science. J Public Health Manage Pract. 2018;24(2):102–111. doi:10.1097/PHH.0000000000000673
34. Li R, Ying B, Qian Y, et al. Prevalence of self-reported symptoms of computer vision syndrome and associated risk factors among school students in China during the COVID-19 pandemic. Ophthalmic Epidemiol. 2021;1–11. doi:10.1080/09286586.2021.1963786
35. Ganne P, Najeeb S, Chaitanya G, Sharma A, Krishnappa NC. Digital eye strain epidemic amid COVID-19 pandemic – a cross-sectional survey. Ophthalmic Epidemiol. 2021;28(4):285–292. doi:10.1080/09286586.2020.1862243
36. Ranasinghe P, Wathurapatha WS, Perera YS, et al. Computer vision syndrome among computer office workers in a developing country: an evaluation of prevalence and risk factors. BMC Res Notes. 2016;9(1):150. doi:10.1186/s13104-016-1962-1
37. Densen P. Challenges and opportunities facing medical education. Trans Am Clin Climatol Assoc. 2011;122(1):48–58.
38. Gurpinar E, Musal B, Aksakoglu G, Ucku R. Comparison of knowledge scores of medical students in problem-based learning and traditional curriculum on public health topics. BMC Med Educ. 2005;5(1):7. doi:10.1186/1472-6920-5-7
39. Gargouri S, Khochtali S, Zina S, et al. Ocular involvement associated with varicella in adults. J Ophthalmic Inflamm Infect. 2016;6(1):47. doi:10.1186/s12348-016-0117-9
40. Greene WH. Econometric Analysis. Prentice Hall; 2013.
41. Das S, Dubey RS. Computer vision syndrome among medical undergraduates at MRIMS, Hyderabad, Telangana. Ophthalrrol Alliecl Sci. 2018;4:15.
42. Garg S, Mallik D, Kumar A, Chunder R, Bhagoliwal A. Awareness and prevalence on computer vision syndrome among medical students: a cross-sectional study. Asian J Med Sci. 2021;12(9):44–48. doi:10.3126/ajms.v12i9.37247
43. Galindo-Romero C, Ruiz-Porras A, García-Ayuso D, Di Pierdomenico J, Sobrado-Calvo P, Valiente-Soriano FJ. Computer vision syndrome in the Spanish population during the COVID-19 lockdown. Optomet Vision Sci. 2021;98(11):1255–1262. doi:10.1097/OPX.0000000000001794
44. Amirul FZ, Aqilah R, Lee ML, Ariffin A. Knowledge, attitude and practice of computer vision syndrome among staff that use video display terminal in a faculty of a Malaysian Public University. Int J Public Health Clin Sci. 2018;2(1):137–147.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cross-Sectional Analyses of Factors Related to Digital Eye Strain Symptoms Among Children Using Online Learning Devices During the COVID-19 Pandemic in Thailand
Chattinnakorn S, Chaicharoenpong K, Pongpirul K
Clinical Ophthalmology 2023, 17:1769-1776
Published Date: 21 June 2023