Back to Journals » International Journal of Women's Health » Volume 14
Self-Reported Menstrual Alterations During the COVID-19 Syndemic in Spain: A Cross-Sectional Study
Authors Medina-Perucha L ![]() , López-Jiménez T, Holst AS, Jacques-Aviñó C, Munrós-Feliu J, Martínez-Bueno C
, López-Jiménez T, Holst AS, Jacques-Aviñó C, Munrós-Feliu J, Martínez-Bueno C ![]() , Valls-Llobet C
, Valls-Llobet C ![]() , Pinzón-Sanabria D, Vicente-Hernández MM
, Pinzón-Sanabria D, Vicente-Hernández MM ![]() , Berenguera A
, Berenguera A ![]()
Received 17 December 2021
Accepted for publication 18 March 2022
Published 13 April 2022 Volume 2022:14 Pages 529—544
DOI https://doi.org/10.2147/IJWH.S354655
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Elie Al-Chaer
Laura Medina-Perucha,1,2 Tomàs López-Jiménez,1,2 Anna Sofie Holst,1,3 Constanza Jacques-Aviñó,1,2 Jordina Munrós-Feliu,4,5 Cristina Martínez-Bueno,5,6 Carme Valls-Llobet,7 Diana Pinzón-Sanabria,8 Mª Mercedes Vicente-Hernández,5 Anna Berenguera1,2,9
1Fundació Institut Universitari per a la recerca a l’Atenció Primària de Salut Jordi Gol i Gurina (IDIAPJGol), Barcelona, Spain; 2Universitat Autònoma de Barcelona, Bellaterra (Cerdanyola del Vallès), Barcelona, Spain; 3Universitat Pompeu Fabra, Barcelona, Spain; 4Atenció a la Salut Sexual i Reproductiva (ASSIR) Muntanya/La Mina, Institut Català de la Salut, Barcelona, Spain; 5Sexual and Reproductive Health Care Research Group (GRASSIR), Barcelona, Spain; 6Servei d’Atenció a la Salut Sexual i Reproductiva (ASSIR), Direcció Assistencial d’Atenció Primària, Institut Català de la Salut, Barcelona, Spain; 7Centro de Análisis y Programas Sanitarios (CAPS), Barcelona, Spain; 8SomiArte Taller, Barcelona, Spain; 9Departament d’Infermeria, Universitat de Girona, Girona, Spain
Correspondence: Laura Medina-Perucha, Gran Via de les Corts Catalanes 587 attic, Barcelona, 08007, Spain, Tel +34 934824253, Email [email protected]
Introduction: Available evidence suggests that there might be an association between the stressors experienced during the COVID-19 syndemic and changes in menstrual patterns. The aim of this study was to assess self-reported menstrual alterations during the COVID-19 syndemic among women and people who menstruate aged 18– 55 in Spain.
Materials and Methods: A cross-sectional online survey-based study was conducted (March–July 2021). Descriptive statistics were calculated and multivariate logistic regression models were constructed. This study was conducted as part of the “Equity and Menstrual Health in Spain” research project.
Results: Among participants (N=17,455), 39.4% reported menstrual alterations since the start of the syndemic. Participants self-reporting long COVID-19 presented higher odds of menstrual alterations (aOR: 1.34, 95% CI, 1.15-1.57). In participants with no history of COVID-19, the risk for self-reported menstrual alterations was significantly higher based on employment situation, among participants experiencing financial issues (eg, financial issues always/many times < 12 months: aOR: 1.68, 95% CI, 1.48– 1.90), poorer self-perceived health (eg, poor: aOR: 2.00, 95% CI, 1.31– 3.07), and those diagnosed with polycystic ovary syndrome (aOR: 1.13, 95% CI, 1.02– 1.26). Among participants with a self-reported COVID-19 diagnosis, factors that significantly increased the odds for menstrual alterations were experiencing financial strains (eg, financial issues always/many times < 12 months: aOR: 1.53, 95% CI, 1.09– 2.14), poorer self-perceived health (eg, poor: aOR: 3.09, 95% CI, 1.01– 9.52). Overall, factors that decreased the odds of reporting menstrual alterations included age > 25, being a carer, not having a gynecological condition and using hormonal contraception.
Discussion and conclusions: Findings suggest an impact of the COVID-19 syndemic on menstrual patterns. Social inequities in reporting menstrual alterations were identified. While the risk of reporting menstrual alterations was higher among participants with long COVID-19, evidence is not conclusive. Further research on menstrual health in the context of COVID-19 is needed, also to inform policy and practice.
Keywords: menstruation, COVID-19, long COVID-19, menstrual health, menstrual inequity, women’s health
Plain Language Summary
There has been a lack of research on how the COVID-19 pandemic could have had an impact on menstrual cycles and menstruation. This study was conducted as part of a larger project on equity and menstrual health. It includes the responses of 17,455 women and people who menstruate (ie, non-binary and trans people who menstruate) to an online survey completed between March and July 2021 in Spain. We have found that 39.4% of our participants reported menstrual alterations since the start of COVID-19. The risk for indicating menstrual alterations was higher in participants with a self-reported diagnosis of long COVID-19 (COVID-19 symptoms for more than 4 weeks), aged 25 or less, full/part-time workers and students, those on benefits, houseworkers or unpaid carers. Financial strains in the 12 months, a poorer self-perceived health and a gynecological diagnosis were other risk factors. Protective factors were being older than 25, caring for someone else (eg children), not having a gynecological diagnosis and using hormonal contraception. This study offers some findings on factors associated with self-reported menstrual alterations during COVID-19 in Spain. More research is needed to understand the changes that some women and people who menstruate have noticed on their menstrual cycles and menstruations in the context of the pandemic.
Introduction
There is virtually no evidence on how the COVID-19 syndemic – a term used to conceptualize ill-health in complex pandemics through understanding the intersection between socio-environmental and biological factors1–4 -, COVID-19 infection and living with long-COVID-19 (or post COVID-19 condition based on a recent WHO definition)5 can have an impact on menstrual health. The prevailing neglect of menstruation and the menstrual cycle as vital health signs and important tools for health promotion has also been apparent during the COVID-19 syndemic.6,7 Menstrual inequities, partly resulting from this systemic neglect, and the actions needed to address them, are further being compromised, shadowed by the COVID-19 crisis.6–9
To our knowledge, only a handful of studies have attempted to address this knowledge gap. A single-centre retrospective study was conducted in China,10 using both clinical and laboratory data, comparing menstrual patterns among women who were mildly and severely ill, and a control group in a total sample of 177 participants. This study found that 20% of women experienced decreased menstrual bleeding after confirmed COVID-19. However, there were no significant differences either in menstrual abundance changes between mildly and severely ill women, or in menstrual length changes before and after being diagnosed with COVID-19, although severely ill patients reported longer menstrual cycles. Besides, 18% women had prolonged cycles and 3% shortened cycles, and 7% showed menstrual cycle disorders. Compared to a control group, menstrual volume and menstrual cycle changes were increased in COVID-19 patients. Changes on the menstrual cycle and menstruation, which were more likely in women with multisystem dysfunction (ie, complications in, for instance, cardiovascular or digestive systems), were thought to return to normal after one or two cycles. Furthermore, the authors found that median concentrations of sex hormones were marginally higher, but not statistically significant, in both mildly and severely ill patients, compared to the control group.10 The authors argued that the endocrine and ovarian systems were not seriously affected in women affected by COVID-19. Ovarian suppression (anovulation) was suspected given the high FSH and LH concentrations during early follicular phase.10 This is coherent with previous studies reporting anovulation occurring in various acute diseases, to ensure an adequate functioning of essential organs diseases.11 The study concluded that a direct effect of the SARS-COV-2 virus cannot be completely ruled out, given the transient alterations in hormone concentrations identified and women’s reported menstrual changes. However, findings did not support that SARS-CoV-2 caused a substantial impairment on menstrual health.10
A cross-sectional study conducted in Jordan,12 which included 200 women, indicated that menstrual problems had significantly decreased during COVID-19 curfew (10.5% vs 17.5% vs, p=0.016). Menstrual problems post-curfew did not differ from those at the pre-curfew stage. Besides, access to healthcare for menstrual problems was not statistically different between pre-curfew, during curfew and post-curfew, although telephone consultations were significantly heightened during curfew.12 With curfew in Jordan only lasting for a few consecutive days, authors argued that population stress levels might not have been high enough to result in more menstrual alterations. These findings differ from those reported in an observational study, conducted in Turkey, showing an increase in menstrual disorders during the syndemic, compared to pre-syndemic (27.6% vs 12.1%, p=0.008). However, this study included only 58 participants thus data should be interpreted carefully.13 Furthermore, in a recently published study conducted in Arizona (United States) 16% of participants with COVID-19 reported menstrual changes. Those reporting alterations were more likely to report more COVID-19 symptoms and higher self-rated illness severity scores. However, these findings should be interpreted with caution given the small sample size included.14
On the other hand, a study conducted in Turkey,15 including data from 952 female healthcare professionals, reported that depression, anxiety and stress were significantly and positively associated with irregular menstruations (changes in menstrual patterns in terms of frequency, regularity, duration or intensity and intermenstrual bleeding). In another Turkish study, researchers identified a relationship between anxiety scores, increased menstrual-related symptoms, shorter menstruations and use of menstrual pads.16 However, increased self-reported stress levels did not seem to be more significantly associated with menstrual alterations during the syndemic (compared to pre-syndemic) in a retrospective cohort study using real-world data from a mobile app, including 214,426 cycles from 18,076 app users mostly in the United Kingdom and the United States.17 In this study, the authors concluded that the COVID-19 had not significantly led to population-level changes in ovulation and menstrual patterns. Importantly, most included data were of women over 30 and with completed high education.17 In fact, irregular menstruation has been previously found to be more prevalent among women of a lower socioeconomic and educational status,18 which could be explained by a higher exposure to life stressors. Thus, socioeconomic variables should be considered when analyzing and interpreting menstrual health data.
Irregular menstrual patterns have been found to be related to a higher risk for developing cardiovascular disease, diabetes mellitus, chronic renal failure and infertility, premature menopause, breast and ovarian cancer in later life.19–22 Besides, having menstrual health problems could also greatly compromise quality of life.18,19 It is therefore urgent to conduct research on menstrual health in the context of the COVID-19 syndemic, also to address the prevailing androcentrism in science and sociopolitical structures.23–26 The aim of this study was to assess self-reported menstrual alterations during the COVID-19 syndemic (2020–2021) among women and people who menstruate (PWM) aged 18–55 in Spain. Data presented in this publication are part of the “Equity and Menstrual Health in Spain” study, a larger mixed-methods project that aimed at assessing menstrual health and menstrual inequities in Spain.
Materials and Methods
This is a cross-sectional study including women and PWM aged 18–55 living in Spain (N=22,823). Data were collected through an online survey between 24th of March and 8th of July 2021, using the Lime Survey platform (https://www.limesurvey.org). The online survey included questions on menstrual health and menstrual inequity and was developed by the research team throughout several meetings and based on previous evidence and guidelines to devise non-validated questionnaires.27 The survey was piloted and available in Spanish. Only statistical analyses referring to the COVID-19 syndemic and the perceived impacts of COVID-19 on menstrual health were included in this publication. Pregnant and breastfeeding participants who reported not menstruating at the time of data collection were excluded from the analyses. The current publication includes data from 17,455 women and PWM.
Participants and Sample Size
Main inclusion criteria were: 1) to menstruate, 3) be between 18 and 55 years old, and 3) live in Spain at the time of data collection. Having entered menopause or not menstruating for over 12 consecutive months was a main exclusion criteria. Sample size power calculations were done for the overall quantitative study for the “Equity and Menstrual Health in Spain” project. Given the lack of research on menstrual inequity, we used a menstrual hygiene management variable from previous studies as a main variable for sample size calculations. Maximum indetermination of the main variable (proportion of 50%) was assumed. These assumptions were in order to obtain a precision of 2.5% in the confidence intervals. These estimates have been calculated assuming an alfa risk of 5%. PASS software was used for the sample size calculations [PASS 15 Power Analysis and Sample Size Software (2017). NCSS, LLC. Kaysville, Utah, USA]. A minimum of 1,535 participants were required.
Sampling and Recruitment
Sampling was non-probabilistic and purposive. Participants were recruited through social media (Instagram, Twitter and WhatsApp) and relevant key persons and organizations, such as sexual and reproductive health centers, primary healthcare centers, non-governmental organizations, and other local organizations. Snowball sampling techniques were also applied. Special attention was paid to recruiting women and PWM who had limited access to social media, people living in socioeconomically deprived areas, participants from the Roma community and migrant populations. This was done through collecting data in person in a foodbank, a service for sex workers and sexual and reproductive health centers.
Data Analyses
Descriptive statistics were performed for each variable. Age was analyzed as mean (SD) and categorized. Categorical variables were described as percentages. Chi-square tests were used to assess differences between socioeconomic variables according to menstrual alterations, self-reported health, gynecological diagnosis, and use of hormonal contraception. Multivariate logistic regression models were constructed to assess the relationship between self-reported menstrual alterations (main outcome variable), and sociodemographics, self-perceived health, gynecological diagnosis, use of hormonal contraception, and diagnosed/suspected COVID-19 and long COVID-19. Models were also generated to compare odds of self-reported menstrual alterations among participants with no history of COVID-19 and participants with a self-reported diagnosis of COVID-19. We conducted a sensibility analysis, excluding participants with existing gynecological conditions (endometriosis/adenomyosis, myomas and ovary polycystic syndrome) and using hormonal contraceptives, to assess potential confounding in the relationship between menstrual alterations, sociodemographic characteristics and self-reported health. The level of statistical significance was set at 0.05 and all tests were 2-tailed. Analyses were conducted using SPSS 25.0 (SPSS Inc., Armonk, NY: IBM Corp), and Stata/MP 17.0 (StataCorp LLC, TX).
Results
Participant Characteristics
Participants were 17,455 women and PWM between 18 and 55 years old (M=32.3, SD=8.9). Most identified their gender as women (96.6%), followed by non-binary/other (3.4%); 0.9% identified as trans. Almost all were born in Spain (93.5%) and held Spanish nationality (95.9%). Over half were working full- or part-time (62.9%) and had completed university degrees (68.2%). Carers (eg of minors) accounted for 22.4% of the sample. Almost half reported financial problems in the 12 months preceding the study (45.0%). Self-reported health was most commonly perceived as good (45.8%), followed by very good (37.5%). Besides, 29.9% reported having a diagnosis of endometriosis/adenomyosis, myoma, or polycystic ovarian syndrome (PCOS). Some participants were using hormonal contraception at the time of data collection (16.7%); 49.8% had previously used them (see Table 1).
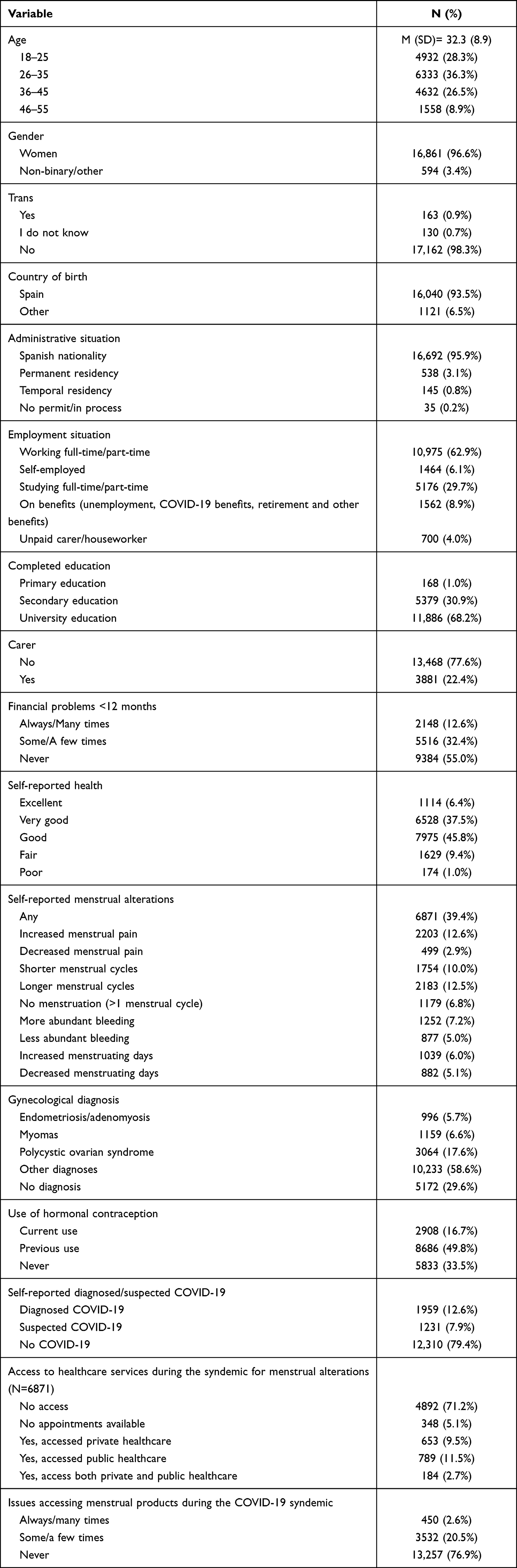 |
Table 1 Sociodemographic Characteristics, Self-Perceived Health, Menstrual Alterations, Gynecological Diagnosis, Use of Hormonal Contraception, Diagnosed/Suspected COVID-19 and Long-COVID-19 (N=17,455) |
A total of 1,959 (12.6%) participants reported having been diagnosed with COVID-19; 546 (27.9%) reported long COVID-19. Also, 1,231 (7.9%) reported having had COVID-19-compatible symptoms and, of these, 202 (16.4%) indicated a possible long COVID-19. Among participants reporting menstrual alterations, 28.8% had tried to access healthcare services to seek professional assistance; 5.1% could not access services as no appointments were available at the time of consultation. Interestingly, the use of private (9.5%) and public healthcare (11.5%) was similar. Furthermore, 23.1% participants reported having had issues accessing menstrual products during the COVID-19 syndemic (see Table 1).
Main Findings
Menstrual alterations were reported in 39.4% of participants, since the start of the COVID-19 syndemic. Changes reported were increased menstrual pain (12.6%), longer menstrual cycles (12.5%), shorter menstrual cycles (10.0%), more abundant bleeding (7.2%), missing menstruation at least in one cycle (6.8%), increased menstruating days (6.0%), decreased menstruating days (5.1%), less abundant bleeding (5.0%), and decreased menstrual pain (2.9%) (see Table 1). There were significant differences among participant groups in the reports of menstrual alterations during the COVID-19 syndemic (see Table 2).
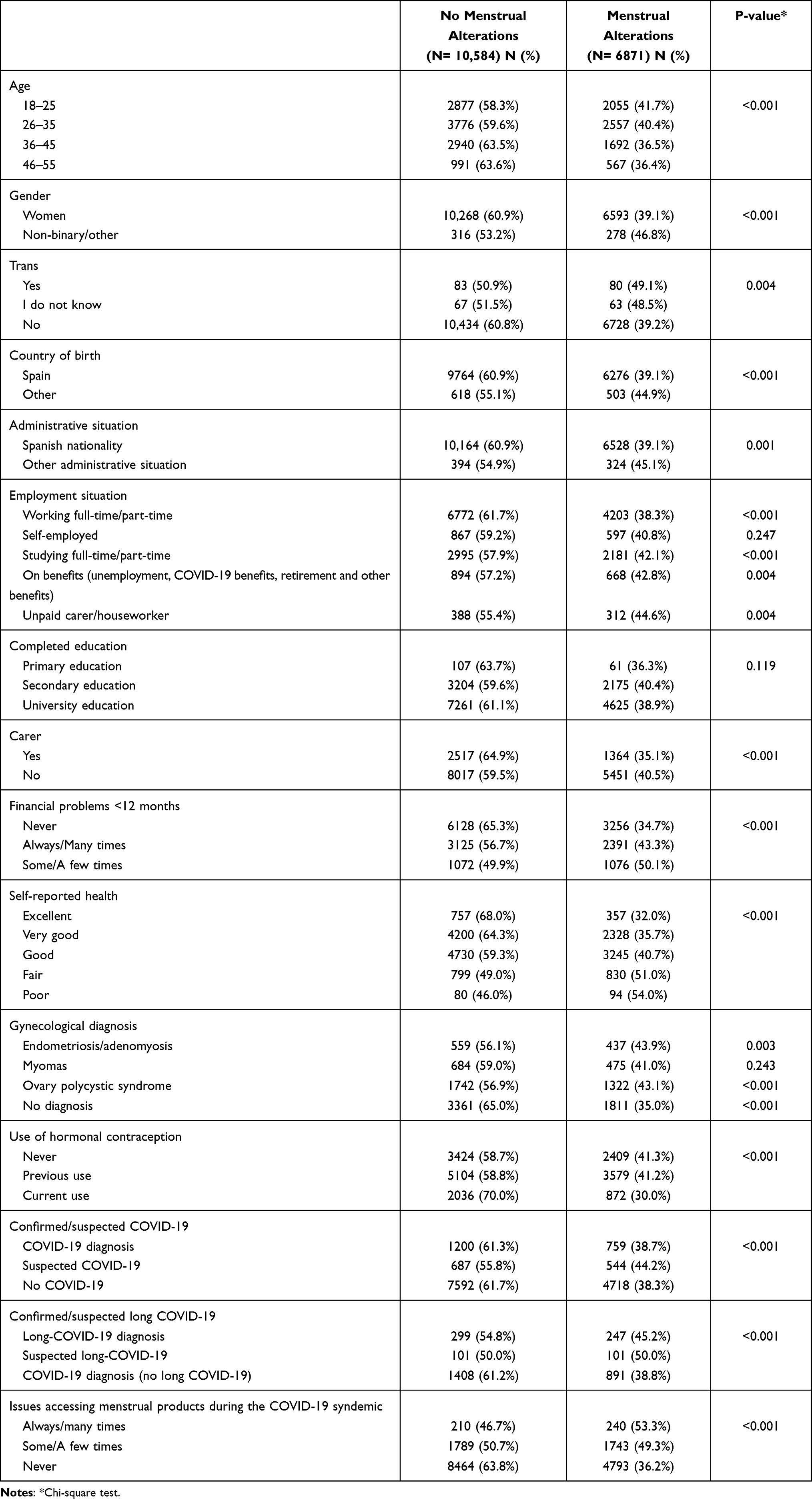 |
Table 2 Self-Reported Menstrual Alterations by Sociodemographics, Self-Reported Health, Gynecological Diagnosis, Use of Hormonal Contraception, Confirmed/Suspected COVID-19 and Long-COVID-19 and Issues Accessing Menstrual Products During the COVID-19 Syndemic (N=17,455) |
Multivariate logistic regression analyses showed associations between self-reported menstrual alterations and several variables among participants with no history of COVID-19 and participants who reported a diagnosis of COVID-19 (see Table 3). The risk of reporting menstrual alterations was significantly increased in participants with suspected COVID-19 (aOR: 1.15, 95% CI, 1.02–1.30), but it was not in participants with diagnosed COVID-19. When including long COVID-19 in the analyses, odds were only significantly increased among participants with suspected/diagnosed long-COVID-19 (aOR: 1.34, 95% CI, 1.15–1.57) (Table 3).
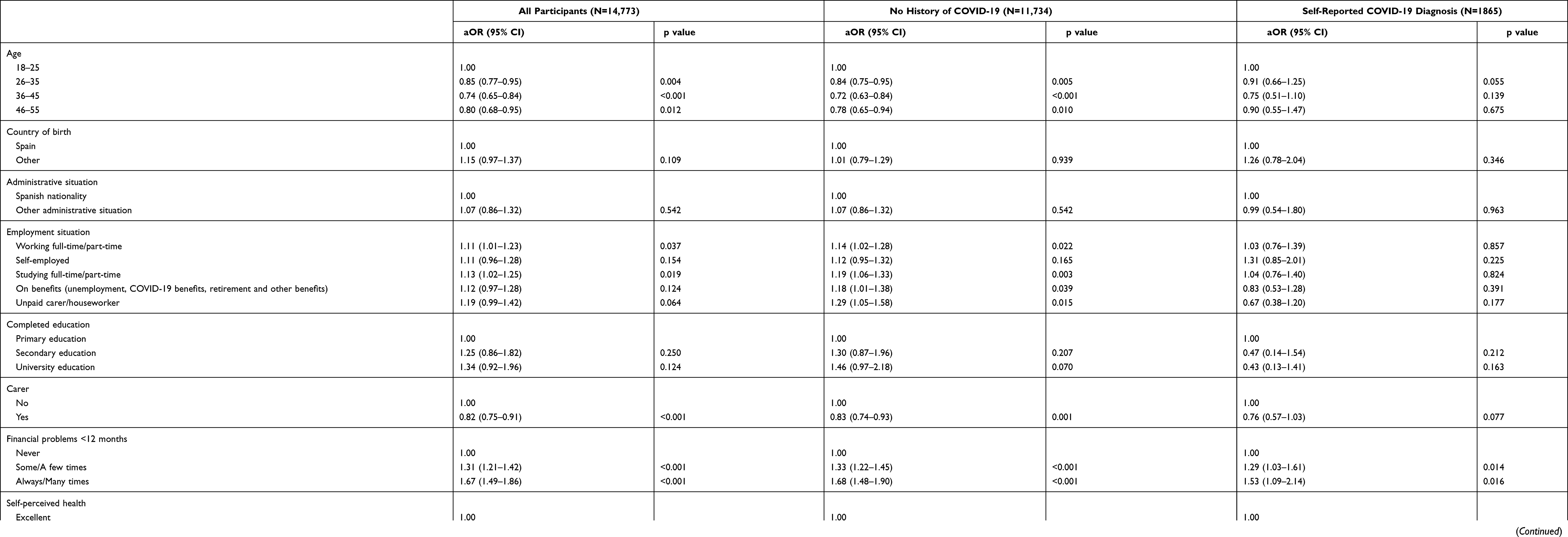 |
Table 3 Associations Between Self-Reported Menstrual Alterations and Sociodemographic Characteristics, Self-Reported Health, Gynecological Diagnosis, and Use of Hormonal Contraception, Among All Participants, Participants Reporting No History of COVID-19 and Participants Reporting a COVID-19 Diagnosis (N=14,773) |
Participants with No History of COVID-19
Among women and PWM with no history of COVID-19, some employment situations significantly heightened the odds of self-reported menstrual alterations. Risk of menstrual alterations was higher among participants working full/part-time (aOR: 1.14, 95% CI, 1.02–1.28), full and part-time students (aOR: 1.19, 95% CI, 1.06–1.33), those receiving unemployment, COVID-19 or other state benefits (aOR: 1.18, 95% CI, 1.01–1.38), and unpaid carers and houseworkers (aOR: 1.29, 95% CI, 1.05–1.58). Although not statistically significant, participants with completed university education had higher odds of reporting menstrual alterations (aOR: 1.46, 95% CI, 0.97–2.18). Having had financial problems in the 12 months preceding the study was another factor significantly associated with reporting menstrual alterations [aOR (always/many times): 1.68, 95% CI, 1.48–1.90]. Odds for self-reported menstrual alterations increased as self-perceived health worsened [aOR (poor): 2.00, 95% CI, 1.31–3.07]. Being diagnosed with myomas (aOR: 1.17, 95% CI, 1.00–1.37) or PCOS (aOR: 1.13, 95% CI, 1.02–1.26) were also associated with higher odds of menstrual alteration reports, although the relationship with myomas was only almost significant (Table 3).
In turn, factors associated with decreased odds of self-reporting menstrual alterations among participants with no history of COVID-19 were: being over 25 years old [(aOR (25–36): 0.84, 95% CI, 0.75–0.95); (aOR: 0.72, 95% CI, 0.63–0.84); (aOR: 0.78, 95% CI, 0.65–0.94)], identifying as a carer (aOR: 0.83, 95% CI, 0.74–0.93), not having a gynecological diagnosis (aOR: 0.83, 95% CI, 0.75–0.90) and currently using hormonal contraception (aOR: 0.55, 95% CI, 0.48–0.62) (Table 3).
Participants with a Self-Reported COVID-19 Diagnosis
Among participants with a reported COVID-19 diagnosis, risk for self-reported menstrual alterations was increased based on having financial problems (aOR: 1.29, 95% CI, 1.03–1.61), worse self-perceived health (aOR: 3.09, 95% CI, 1.01–9.57), and having a diagnosis of endometriosis/adenomyosis (aOR: 1.51, 95% CI, 0.98–2.32), although the latter association was not statistically significant (Table 3).
Age and employment situation variables were not significantly associated with decreased odds of menstrual alterations self-reports in participants with diagnosed COVID-19. However, age between 25–36 was an almost statistically significant risk factor (aOR: 0.91, 95% CI, 0.66–1.25). The same was found for being a carer, although a reduction in odds ratios were identified, this variable was not statistically significant (aOR: 0.76, 95% CI, 0.57–1.03). Not being diagnosed with the gynecological conditions included in the analyses (aOR: 0.63, 95% CI, 0.49–0.79) and currently using hormonal contraception (aOR: 0.40, 95% CI, 0.29–0.54) were other variables that reduced the odds of reporting menstrual alterations among participants with a COVID-19 diagnosis (Table 3).
Sensitivity analyses were conducted excluding participants with gynecological conditions and those taking hormonal contraception. Overall, there were minimal variations to odd ratios and their directionality. However, some variables ceased to be statistically significant risk (eg, employment situation) or protective (eg, age between 46 and 55 in participants with no history of COVID-19) factors in sensitivity analyses. This was due to the loss in statistical power. Therefore, there were no significant differences in the findings from the sensitivity analyses, compared to the findings reported in Table 3 (see Supplementary Table).
Discussion
Over one third of participants reported having experienced menstrual changes during the COVID-19 syndemic, a higher prevalence compared to the one reported in studies in other countries during the syndemic (10.5–12.1%).12,13 Overall, our findings suggest that experiencing menstrual alterations is associated with long COVID-19, being younger than 25, being a student or worker (full- or part-time), receiving state benefits or being an unpaid carer or houseworker, and having financial problems. Also, having a poorer self-perceived health and a gynecological diagnosis such as PCOS. On the other hand, caring for someone else and using hormonal contraception were protective factors for reporting menstrual alterations. Furthermore, 23.1% women and PWM had issues accessing menstrual products during the syndemic. Among participants experiencing menstrual alterations, 5.1% could not access healthcare services due to appointments were not available; 11.5% accessed public healthcare services and 9.5% had access to private healthcare.
In order to interpret these data, it is important to refer to the complex intersection between socio-environmental and biological factors to understand ill-health.28–30 The link between social determinants of health, social inequities and health outcomes is well-established.31–35 Recent studies have highlighted how social determinants of health have an impact on COVID-19 incidence and outcomes,36,37 as well as on other health outcomes.38–40 Besides, menstrual problems have already been found more prevalent during complex social crises (eg, wars, earthquakes),41–44 including recent evidence that identifies COVID-19 syndemic stress as a significant predictor of menstrual irregularities.15 A general plausible explanation may be related to the social and environmental context and dysregulations of the hypothalamic-pituitary-gonadal (HPA) axis.45–48
One of the findings from our research is that being aged below 25 meant a higher risk for reporting menstrual alterations. This is consistent with previous studies indicating worse mental health outcomes among younger adults in Spain38 and in other countries49 during the syndemic. Our results further support that young adults may have been more impacted by the stressors of the COVID-19 crisis, although further investigations are needed to determine the factors associated with this impact. Besides, the close relationship between mental health and menstrual patterns has also been investigated in the past,21,48,50–54 suggesting a link between emotional wellbeing and menstrual health.
Employment situation was also an important factor for reporting menstrual alterations. We can hypothesize that the relationship between employment situation and menstrual alterations is two-fold. On one hand, actively working and studying during the syndemic could have led to multiple stressors of worsening employment and studying conditions (eg, teleworking, lack of online studying resources).55 On the other hand, being on benefits (eg, unemployment or COVID-19 benefits) could explain higher self-reported menstrual alterations, based on experiencing stressors related to the loss of employment and adverse job-seeking prospects throughout the COVID-19 crisis. In fact, previous evidence already indicates that unemployment and low-quality employment have similar detrimental effects on mental wellbeing.56 In addition, women’s participation in the labor force may decrease their burden of care, which could contribute to improving their health.57 For unpaid carers and houseworkers, reporting menstrual alterations could be explained by the reduction (or disappearance) of support networks, especially during lockdown periods, and the resulting worsening of living conditions and mental health.58–61 However, we also found that being a carer was a protective factor for reporting menstrual alterations. Despite this may seem contradictory, we assume that most women and PWM who identified as carers had a source of employment or were studying. In such cases, and as we have already reported, a determining risk factor for reporting menstrual alterations might actually be employment status rather than caring itself. This could be explained by the potential good housing conditions and reduced financial strains of our sample. Apart from this, a higher socioeconomic status could mean having a more extensive care network and being able to externalize caring tasks when possible during COVID-19 (eg, hire a sitter or carer). In fact, being an informal caregiver has already been found to be a protective factor for depression among women in Spain during COVID-19.37 Besides, financial strains were systematically associated with reporting menstrual alterations in our study. In fact, experiencing financial issues has already been linked to poorer self-perceived health and psychological wellbeing among European workers.62 Southern European countries like Spain are the ones with the highest prevalence of financial strains.62 This again suggests the associations between experiencing life stressors and poorer menstrual health, as previously studies have indicated.18
On the other hand, this may be one of the first studies reporting an association between self-perceived health and menstrual patterns. We found that women and PWM who rated their health as worse were more likely to report menstrual changes in the context of COVID-19, even if we do not have data on health conditions other than some chronic gynecological conditions (ie, endometriosis/adenomyosis, myomas and PCOS). This association could not only be related to morbidity but mental health and wellbeing, given that self-perceived health is a good indicator of socioeconomic class, physical and mental health status.63 As we might expect, participants with previous gynecological conditions that commonly include menstrual changes (eg, PCOS) were more likely to report menstrual changes.64,65
Considering menstrual inequities in the context of social and health crises is also imperative.6–9 As our findings showed, more than 2 in 10 women and PWM had experienced barriers to finding menstrual products during the syndemic. We believe that this may be related to mobility restrictions during lockdown periods and in more rural areas. Besides, 5.1% of participants reporting menstrual alterations could not access healthcare assistance, likely due to the healthcare system’ saturation.66 Interestingly, participants accessed public and private healthcare similarly. This may indicate that the overload in public healthcare services led women and PWM to access private healthcare. It also means that participants could afford private healthcare, which is consistent with the high level of education and employment rates among study participants. Having private health insurance, which has become increasingly common in Spain particularly after the economic crisis in 2008, reduces the use of public services.67 However, not all women and PWM can pay for private healthcare. Therefore, public health systems need to be strengthened, not only to sustain ill-health in a syndemic but also to attend health-related consultations that might otherwise be left unattended, especially among more vulnerable populations. To attain this, we argue that social inequities and gender-based frameworks are essential for effective actions in research, policy and practice.
Lastly, even if there were differences between participants with no history of COVID-19 and those with self-reported COVID-19 diagnosis, factors that increased the odds of reporting menstrual alterations were similar in both groups. Still, participants with a reported diagnosis of long COVID-19 seemed more likely to report menstrual alterations. This may suggest that factors potentially contributing to menstrual alterations among women and PWM with COVID-19, and particularly long COVID-19, need to be further explored for evidence to be more conclusive.10,12–17 While this article did not focus on the potential impact of COVID-19 vaccination on menstrual patterns, there are reports of women experiencing menstrual changes post-vaccine.7 However, menstrual alterations have not yet been reported and listed as plausible COVID-19 vaccine side effects, and the menstrual cycle and menstruation have not generally been considered in clinical trials for COVID-19 vaccine development and other COVID-19 research. In the meantime, women and PWM should be encouraged to share menstrual changes with their health professionals, while the latter should not dismiss these reports. Further research should urgently consider the menstrual cycle and menstruation in the context of the COVID-19 syndemic,7 to inform clinical practice and policymaking.
Limitations
Several limitations need to be acknowledged when interpreting the findings from this study. First, neither the sample included is representative of the Spanish population nor does the study design allow us to establish causality. Second, data are self-reported, including the diagnosis of COVID-19, long COVID-19 and gynecological conditions. Besides, other comorbidities including mental health were not collected and included in the analyses. Third, we do not know the time, duration and severity of the reported menstrual alterations, or whether they were also experienced before COVID-19. Fourth, we did not collect data on health habits, and use of medication other than hormonal contraception. Fifth, we used the term and definition of “long COVID-19” available at the time of data collection, although we are aware that this definition has changed over time. This may differ from current definitions and terminologies of long COVID-19. Furthermore, we do not know how long COVID-19 persisted and which were the symptoms experienced. Last, despite the team’s efforts to recruit women and PWM with lower educational attainment and a lower socioeconomic status, the sample underrepresents these groups of women and PWM. Despite all limitations, we strongly believe that this piece of research can be a valuable contribution to the scarce evidence on menstrual health and menstrual inequity in the context of COVID-19.
Conclusions
While evidence needs to be interpreted with caution, findings from this study indicate that stressors during the COVID-19 syndemic may have had an impact on menstrual patterns. Despite women and PWM with a reported diagnosis of long COVID-19 appeared to be more at risk of reporting menstrual alterations, evidence is not conclusive. Social inequities in experiencing menstrual alterations need to be considered, given the differential impact of the COVID-19 syndemic on menstrual patterns by sociodemographic characteristics. Future mixed-methods research, is required to further investigate the potential links between menstrual health and COVID-19, as well as menstrual inequities in the context of social and health crises such as the COVID-19 syndemic. Research should aim to be transformative and inform both policy and practice.
Abbreviation
PWM, people who menstruate.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available to maintain participants’ anonymity and confidentiality, but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Ethical approval was obtained from IDIAPJGol Ethical Committee on 21st November 2020, Ref 19/178-P. All activities included in the study were carried out according to existing guidance in ethics as indicated in the Universal Declaration on Bioethics and Human Rights adopted by UNESCO (19/10/2005); the Council of Europe Convention for the Protection of Human Rights and Dignity of the Human Being with regard to the Application of Biology and Medicine (1997) and its additional protocol on biomedical research (2005); the Helsinki Declaration (2013) and relevant EU laws (European Parliament and Council Directive 2001/20/EC); the Spanish Law on Biomedical Research (14/2007) and the LOPD (Spanish Law on Personal Data Protection) (3/2018). Participant information sheets were available for all participants. Written consent was requested prior to participation. All data have been stored and managed safely to ensure participants’ confidentiality and anonymity.
Acknowledgments
We would like to thank all participants, for dedicating their time and energy to take part in the study. Thank you to Carmen Revuelta, Ramona Ortiz, Rosa Turbau Valls, Mònica Isidro Albaladejo, Enara Solana Lizarza, Paula Briales Canseco, Lola Hernández for their contributions to the study. Also, to the following people and organisations for disseminating the questionnaire and contributing to the recruitment process: Institut Català de la Salut, Centre Jove d’Atenció a les Sexualitats (CJAS), Joventut Barcelona, La Caravana Roja, SomiArte Taller, Centro de Análisis y Programas Sanitarios (CAPS), La Vida en Rojo Asociación de Cultura Menstrual, CYCLO Menstruación Sostenible, DIM and DIM Protect, Aguas de Luna, Xusa Sanz, Cristina Luna, Sylvia de Bejar, Laia Casadevall, Irene Aterido, Celia Cuenca, EndoFem, Judit Pelegrí Alvárez, Blanca Albillos Mingorance, Julia Arquillos Jimenez, Gala Montenegro Nadal, Sílvia Martin Egido, Cristina Morote Muñoz, Marta Boqué Ramon, Anna Solé Valls, Anna Sánchez Benedet, Irene Blanco Alcántara, Frater Nadal, Abel Renuncio, Emilia Bailon, Tania Cedeño, Sociedad Española de Medicina Familiar y Comunitaria (semFYC), Banc Farmacèutic, La Nau and Ajuntament de Cornellà. Last but not least, to Anna Moleras Serra for her valuable technical assistance and management to devise the online questionnaire on LimeSurvey and during data collection. The authors would like to disclose that a report on the main findings included in this publication is available online in Spanish, given the public and political interest on the topic addressed in this publication: https://rediapp.org/images/Informe_alteraciones_menstruales_y_COVID19_en_Espana.pdf.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the European Society of Contraception and Reproductive Health (P-2019-A-01). It was also supported by the Spain's Ministry of Science and Innovation through the Carlos III Health Institute and European Union ERDF funds (European Regional Development Fund) through the Research Network in Preventive Activities and Health Promotion in Primary Care (redIAPP, RD16/0007/0001). The funders had no role in the design of the study, in data collection, analyses, and interpretation and in the writing of the manuscript, or in the decision to publish the results.
Disclosure
Anna Sofie Holst reports personal fees from World Health Organisation for a project-based consultancy contract working in the Digital Health Flagship in WHO/Europe, outside the commited work. The authors declare no other competing interests in this work.
References
1. Rod MH, Hulvej Rod N. Towards a syndemic public health response to COVID-19. Scand J Public Health. 2021;49(1):14–16. doi:10.1177/1403494820982862
2. Singer M, Bulled N, Ostrach B, Mendenhall E. Syndemics and the biosocial conception of health. Lancet. 2017;389(10072):941–950. doi:10.1016/S0140-6736(17)30003-X
3. Harish V. The syndemics of emergency: how COVID-19 demands a holistic view of public health promotion and preparedness. Am J Public Health. 2021;111(3):353–354. doi:10.2105/AJPH.2020.306116
4. Caron RM, Adegboye ARA. COVID-19: a syndemic requiring an integrated approach for marginalized populations. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.675280
5. World Health Organization. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus; 2021.
6. Jahan N. Bleeding during the pandemic: the politics of menstruation. Sex Reprod Health Matters. 2020;28(1):1801001. doi:10.1080/26410397.2020.1801001
7. Male V. Menstrual changes after covid-19 vaccination. BMJ. 2021;15:n2211. doi:10.1136/bmj.n2211
8. Ashraf S, Kuang J, Das U, Bicchieri C. Sanitation practices during early phases of COVID-19 lockdown in Peri-Urban Communities in Tamil Nadu, India. Am J Trop Med Hyg. 2020;103(5):2012–2018. doi:10.4269/ajtmh.20-0830
9. Sommer M, Gruer C, Smith RC, Maroko A, Kim H. Menstruation and homelessness: challenges faced living in shelters and on the street in New York City. Health Place. 2020;66:102431. doi:10.1016/j.healthplace.2020.102431
10. Li K, Chen G, Hou H, et al. Analysis of sex hormones and menstruation in COVID-19 women of child-bearing age. Reprod Biomed Online. 2021;42(1):260–267. doi:10.1016/j.rbmo.2020.09.020
11. Karagiannis A, Harsoulis F. Gonadal dysfunction in systemic diseases. Eur J Endocrinol. 2005;152(4):501–513. doi:10.1530/eje.1.01886
12. Aolymat I, Cross-Sectional A. Study of the impact of COVID-19 on domestic violence, menstruation, genital tract health, and contraception use among women in Jordan. Am J Trop Med Hyg. 2021;104(2):519–525. doi:10.4269/ajtmh.20-1269
13. Yuksel B, Ozgor F. Effect of the COVID‐19 pandemic on female sexual behavior. Int J Gynecol Obstet. 2020;150(1):98–102. doi:10.1002/ijgo.13193
14. Khan SM, Shilen A, Heslin KM, et al. SARS-CoV-2 infection and subsequent changes in the menstrual cycle among participants in the Arizona CoVHORT study. Am J Obstet Gynecol. 2022;226(2):270–273. doi:10.1016/j.ajog.2021.09.016
15. Takmaz T, Gundogmus I, Okten SB, Gunduz A. The impact of COVID‐19‐related mental health issues on menstrual cycle characteristics of female healthcare providers. J Obstet Gynaecol Res. 2021;47(9):3241–3249. doi:10.1111/jog.14900
16. Demir O, Sal H, Comba C. Triangle of COVID, anxiety and menstrual cycle. J Obstet Gynaecol. 2021;41(8):1257–1261. doi:10.1080/01443615.2021.1907562
17. Nguyen BT, Pang RD, Nelson AL, et al. Detecting variations in ovulation and menstruation during the COVID-19 pandemic, using real-world mobile app data. PLoS One. 2021;16(10):e0258314. doi:10.1371/journal.pone.0258314
18. Kwak Y, Kim Y, Baek KA, Erbil N. Prevalence of irregular menstruation according to socioeconomic status: a population-based nationwide cross-sectional study. PLoS One. 2019;14(3):e0214071. doi:10.1371/journal.pone.0214071
19. Cirillo PM, Wang ET, Cedars MI, Chen L, Cohn BA. Irregular menses predicts ovarian cancer: prospective evidence from the child health and development studies. Int J Cancer. 2016;139(5):1009–1017. doi:10.1002/ijc.30144
20. Terry KL, Willett WC, Rich-Edwards JW, Hunter DJ, Michels KB. Menstrual cycle characteristics and incidence of premenopausal breast cancer. Cancer Epidemiol Biomark Prev. 2005;14(6):1509–1513. doi:10.1158/1055-9965.EPI-05-0051
21. Fraser I, Critchley H, Broder M, Munro M. The FIGO recommendations on terminologies and definitions for normal and abnormal uterine bleeding. Semin Reprod Med. 2011;29(5):383–390. doi:10.1055/s-0031-1287662
22. Nillni Y, Wesselink A, Hatch E, et al. Mental health, psychotropic medication use, and menstrual cycle characteristics. Clin Epidemiol. 2018;10:1073–1082. doi:10.2147/CLEP.S152131
23. Bailey AH, LaFrance M, Dovidio JF. Is man the measure of all things? a social cognitive account of androcentrism. Pers Soc Psychol Rev. 2019;23(4):307–331. doi:10.1177/1088868318782848
24. Valls-Llobet C. Mujeres, Salud y Poder. Madrid: Cátedra. Feminismos; 2009.
25. Valls-Llobet C. Mujeres invisibles para la medicina. Madrid: Capitán Swing; 2020.
26. Criado Perez C. Invisible Women: Exposing Data Bias in a World Designed for Men. Vintage; 2020.
27. Boynton PM, Greenhalgh T. Selecting, designing, and developing your questionnaire. BMJ. 2004;328(7451):1312–1315. doi:10.1136/bmj.328.7451.1312
28. Singer M. Dose of drugs, a touch of violence, a case of AIDS: conceptualizing the SAVA syndemic. Free Inq Creat Sociol. 1996;24(2):99–110.
29. Singer M, Clair S. Syndemics and public health: reconceptualizing disease in bio-social context. Med Anthropol Q. 2003;17(4):423–441. doi:10.1525/maq.2003.17.4.423
30. Singer M, Bulled N, Ostrach B. Whither syndemics?: trends in syndemics research, a review 2015–2019. Glob Public Health. 2020;15(7):943–955. doi:10.1080/17441692.2020.1724317
31. Rose G. Sick individuals and sick populations. Int J Epidemiol. 2001;30(3):427–432. doi:10.1093/ije/30.3.427
32. Solar O, Irwin A. A conceptual framework for action on the social determinants of health; 2010. Available from: https://www.who.int/sdhconference/resources/ConceptualframeworkforactiononSDH_eng.pdfv.
33. Dover DC, Belon AP. The health equity measurement framework: a comprehensive model to measure social inequities in health. Int J Equity Health. 2019;18(1):36. doi:10.1186/s12939-019-0935-0
34. Kawachi I. A glossary for health inequalities. J Epidemiol Community Health. 2002;56(9):647–652. doi:10.1136/jech.56.9.647
35. Marmot M. The health gap: the challenge of an unequal world: the argument. Int J Epidemiol. 2017;46(4):1312–1318. doi:10.1093/ije/dyx163
36. Upshaw TL, Brown C, Smith R, Perri M, Ziegler C, Pinto AD. Social determinants of COVID-19 incidence and outcomes: a rapid review. PLoS One. 2021;16(3):e0248336. doi:10.1371/journal.pone.0248336
37. Vásquez-Vera H, León-Gómez BB, Borrell C, et al. Inequities in the distribution of COVID-19: an adaptation of WHO’s conceptual framework. Gaceta Sanitaria. 2021. doi:10.1016/j.gaceta.2021.10.004
38. Jacques-Aviñó C, López-Jiménez T, Medina-Perucha L, et al. Gender-based approach on the social impact and mental health in Spain during COVID-19 lockdown: a cross-sectional study. BMJ Open. 2020;10(11):e044617. doi:10.1136/bmjopen-2020-044617
39. Fisher J, Languilaire J-C, Lawthom R, et al. Community, work, and family in times of COVID-19. Community Work Fam. 2020;23(3):247–252. doi:10.1080/13668803.2020.1756568
40. The Lancet Global Health. Mental health matters. Lancet Global Health. 2020;8(11):e1352. doi:10.1016/S2214-109X(20)30432-0
41. Hannoun AB, Nassar AH, Usta IM, Zreik TG, Abu Musa AA. Effect of war on the menstrual cycle. Obstet Gynecol. 2007;109(4):929–932. doi:10.1097/01.AOG.0000257170.83920.de
42. Liu X, Yang Y, Yuan P, et al. A study of the relationship between mental health and menstrual abnormalities in female middle school students from postearthquake Wenchuan. Biosci Trends. 2010;4(1):4–8.
43. Pasternak A, Brooks PG. The long-term effects of the holocaust on the reproductive function of female survivors. J Minim Invasive Gynecol. 2007;14(2):211–217. doi:10.1016/j.jmig.2006.10.026
44. Whitacre FE. War Amenorrhea. J Am Med Assoc. 1944;124(7):399. doi:10.1001/jama.1944.02850070001001
45. Young EA, Korszun A. The hypothalamic–pituitary–gonadal axis in mood disorders. Endocrinol Metab Clin North Am. 2002;31(1):63–78. doi:10.1016/S0889-8529(01)00002-0
46. Johnson EO, Kamilaris TC, Chrousos GP, Gold PW. Mechanisms of stress: a dynamic overview of hormonal and behavioral homeostasis. Neurosci Biobehav Rev. 1992;16(2):115–130. doi:10.1016/S0149-7634(05)80175-7
47. Nicoletti I, Filipponi P, Sfrappini M, et al. Catecholamines and pituitary function. Horm Res. 1984;19(3):158–170. doi:10.1159/000179883
48. Schliep KC, Mumford SL, Vladutiu CJ, et al. Perceived stress, reproductive hormones, and ovulatory function. Epidemiology. 2015;26(2):177–184. doi:10.1097/EDE.0000000000000238
49. Gloster AT, Lamnisos D, Lubenko J, et al. Impact of COVID-19 pandemic on mental health: an international study. PLoS One. 2020;15(12):e0244809. doi:10.1371/journal.pone.0244809
50. Jung E-K, Kim S-W, Ock S-M, Jung K-I, Song C-H. Prevalence and related factors of irregular menstrual cycles in Korean women: the 5th Korean National Health and Nutrition Examination Survey (KNHANES-V, 2010–2012). J Psychosom Obstet Gynecol. 2018;39(3):196–202. doi:10.1080/0167482X.2017.1321631
51. Fenster L, Waller K, Chen J, et al. Psychological stress in the workplace and menstrual function. Am J Epidemiol. 1999;149(2):127–134. doi:10.1093/oxfordjournals.aje.a009777
52. Palm-Fischbacher S, Ehlert U. Dispositional resilience as a moderator of the relationship between chronic stress and irregular menstrual cycle. J Psychosom Obstet Gynecol. 2014;35(2):42–50. doi:10.3109/0167482X.2014.912209
53. Lin HT, Lin LC, Shiao JS. The impact of self-perceived job stress on menstrual patterns among Taiwanese Nurses. Ind Health. 2007;45(5):709–714. doi:10.2486/indhealth.45.709
54. Nagma S, Kapoor G, Bharti R, et al. To evaluate the effect of perceived stress on menstrual function. J Clin Diagn Res. 2015;9(3):QC01–3. doi:10.7860/JCDR/2015/6906.5611
55. Kniffin KM, Narayanan J, Anseel F, et al. COVID-19 and the workplace: implications, issues, and insights for future research and action. Am Psychol. 2021;76(1):63–77. doi:10.1037/amp0000716
56. Cortès-Franch I, Puig-Barrachina V, Vargas-Leguás H, Arcas MM, Artazcoz L. Is being employed always better for mental wellbeing than being unemployed? exploring the role of gender and welfare state regimes during the economic crisis. Int J Environ Res Public Health. 2019;16(23):4799. doi:10.3390/ijerph16234799
57. Palència L, de Moortel D, Artazcoz L, et al. Gender policies and gender inequalities in health in Europe. Int J Health Serv. 2017;47(1):61–82. doi:10.1177/0020731416662611
58. Bergmann M, Wagner M. The Impact of COVID-19 on informal caregiving and care receiving across Europe during the first phase of the pandemic. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.673874
59. Gérain P, Zech E. Informal caregiver burnout? development of a theoretical framework to understand the impact of caregiving. Front Psychol. 2019;10. doi:10.3389/fpsyg.2019.01748
60. Chatzidakis A, Hakim J, Littler J, Rottenberg C, Segal L. From carewashing to radical care: the discursive explosions of care during Covid-19. Fem Media Stud. 2020;20(6):889–895. doi:10.1080/14680777.2020.1781435
61. Malherbe N. Community psychology and the crisis of care. J Community Psychol. 2020;48(7):2131–2137. doi:10.1002/jcop.22427
62. Artazcoz L, Cortès-Franch I, Escribà-Agüir V, Benavides FG. Financial strain and health status among European workers: gender and welfare state inequalities. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.616191
63. Wu S, Wang R, Zhao Y, et al. The relationship between self-rated health and objective health status: a population-based study. BMC Public Health. 2013;13(1):320. doi:10.1186/1471-2458-13-320
64. Agarwal SK, Chapron C, Giudice LC, et al. Clinical diagnosis of endometriosis: a call to action. Am J Obstet Gynecol. 2019;220(4):
65. Dunselman GAJ, Vermeulen N, Becker C, et al. ESHRE guideline: management of women with endometriosis. Hum Reprod. 2014;29(3):400–412. doi:10.1093/humrep/det457
66. Legido-Quigley H, Mateos-García JT, Campos VR, Gea-Sánchez M, Muntaner C, McKee M. The resilience of the Spanish health system against the COVID-19 pandemic. Lancet Public Health. 2020;5:e251–2. doi:10.1016/S2468-2667(20)30060-8
67. Cantarero-Prieto D, Pascual-Sáez M, Gonzalez-Prieto N. Effect of having private health insurance on the use of health care services: the case of Spain. BMC Health Serv Res. 2017;17(1):716. doi:10.1186/s12913-017-2667-4
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.