Back to Archived Journals » Integrated Blood Pressure Control » Volume 16
Self-Reported Hypertension and Associated Factors Among Adults in Butambala District, Central Uganda: A Community-Based Prevalence Study
Authors Kato AM ![]() , Kibone W
, Kibone W ![]() , Okot J
, Okot J ![]() , Baruch Baluku J
, Baruch Baluku J ![]() , Bongomin F
, Bongomin F ![]()
Received 7 August 2023
Accepted for publication 3 November 2023
Published 9 November 2023 Volume 2023:16 Pages 71—80
DOI https://doi.org/10.2147/IBPC.S434230
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Konstantinos Tziomalos
Alex Male Kato,1 Winnie Kibone,2 Jerom Okot,3 Joseph Baruch Baluku,4 Felix Bongomin3
1Department of Public Health, Gulu University, Gulu, Uganda; 2School of Medicine, College of Health Sciences, Makerere University, Kampala, Uganda; 3Department of Medical Microbiology and Immunology, Faculty of Medicine, Gulu University, Gulu, Uganda; 4Division of Pulmonology, Kiruddu National Referral Hospital, Kampala, Uganda
Correspondence: Winnie Kibone, School of Medicine, College of Health Sciences Makerere University, P O BOX 7072, Kampala, Uganda, Email [email protected]
Background: The prevalence of hypertension (HTN) differs among regions and income groups, showing a substantial increase in low- and middle-income countries. The development of hypertension is modulated by modifiable lifestyle factors, and uncontrolled hypertension poses a risk for the onset of cardiovascular diseases.
Objective: To determine the community-level point-prevalence and factors associated with self-reported HTN among adults in Butambala district, central Uganda.
Methods: A community-based cross-sectional study was conducted among adults aged ≥ 18 years in Budde subcounty, central Uganda. Data on sociodemographic characteristics and behavior were collected using a semistructured questionnaire. Self-reported HTN was assessed using a single question: “Do you have high blood pressure?” Bivariate and multivariate logistic regression analyses were performed to identify predictors of self-reported HTN.
Results: A total of 565 participants (53.5% female) with a median age of 38 years (IQR: 26– 52) were included in the study. The prevalence of self-reported hypertension was 18.9%. Factors independently associated with HTN were age 60 years or older (aOR: 2.9, 95% CI: 1.64– 5.23, p< 0.001), female sex (aOR: 3.3, 95% CI: 2.3– 6.3, p< 0.001), being widowed (aOR: 10.4, 95% CI: 1.25– 87.14, p=0.03), secondary (aOR: 0.4, 95% CI: 0.20– 0.85, p=0.016) and tertiary (aOR: 0.2, 95% CI: 0.09– 0.64, p=0.005) education, unemployment (aOR: 3.0, 95% CI: 1.11– 7.96, p=0.03), tobacco use (aOR: 2.9, 95% CI: 1.83– 4.53, p< 0.001), having had at least one blood pressure measurement during antenatal visit (aOR: 4.7, 95% CI: 1.97– 11.33, p< 0.001) or medical checkup (aOR: 10.7, 95% CI: 6.06– 18.
Conclusion: We observed a high prevalence of self-reported HTN affecting approximately one in five participants. More efforts are required to enhance routine screening, health education, and accessibility to HTN services in rural areas, with a particular emphasis on implementing HTN prevention and control strategies to effectively reduce the prevalence of HTN.
Keywords: self-reported hypertension, high blood pressure, blood pressure, Uganda
Introduction
Hypertension (HTN) is a critical global public health issue that significantly contributes to morbidity and mortality worldwide. HTN is a major risk factor for cardiovascular diseases such as heart disease and stroke, which are the leading causes of death worldwide.1 Moreover, the prevalence of HTN differs among regions and income groups, showing a substantial rise in low- and middle-income countries.2
According to the World Health Organization (WHO), approximately 1.28 billion adults aged 30–79 years are estimated to have hypertension, with approximately two-thirds living in low- and middle-income countries.3 The WHO African Region bears a significant burden of HTN, with an estimated prevalence of 27%, which is significantly lower than the WHO Region of the Americas, whose prevalence is estimated at approximately 18%.3 The number of adults with hypertension is expected to be over 1.5 billion by 2025, with the increase largely seen in low- and middle-income countries, including Uganda, and as observed, there is still a lack of awareness about the growing problem of noncommunicable diseases concurrently with the absence of a clear policy framework for prevention and control.4 The prevalence of HTN varies across different regions of Uganda, with the central region experiencing the highest prevalence, estimated at approximately 34.3%, as reported in a national epidemiological study published in 2019.5
The development of HTN is influenced by a multitude of factors, including both nonmodifiable and modifiable risk factors. Nonmodifiable risk factors encompass increasing age, gender (twofold risk of HTN in males than females), and genetic predisposition, while modifiable risk factors include unhealthy dietary habits, including high salt consumption (>5 g per day), high saturated fat and trans-fat diets and low intake of fruits and vegetables, physical inactivity, tobacco use, excessive alcohol consumption, obesity, and socioeconomic factors.6,7 HTN is largely asymptomatic in a majority of patients is thus referred to as a ‘silent killer’, however, uncontrolled hypertension is associated with a range of adverse health outcomes, including an increased risk of cardiovascular events such as heart attacks and strokes, as well as end-organ damage, including renal failure and retinopathy.8–10 Moreover, approximately 54% of stroke and 47% of coronary heart disease are attributable to high blood pressure.11 Furthermore, HTN imposes a substantial financial burden on individuals, families, healthcare systems, and societies as a whole.
Despite several limitations, such as low sensitivity, self-reporting is a commonly utilized method in research settings to assess the burden of conditions such as HTN.12 Self-reporting is a cost-effective method that depends on individuals willingly revealing their behaviors, beliefs, attitudes, or intentions regarding the particular condition.13 The comparability of self-reports with objective measurements of HTN has been well demonstrated by Najafi et al, where self-reported HTN had a prevalence of 16.8%, while medically confirmed HTN based on verified medical history and measurements had a prevalence of 15.7%.14 Thus, self-reported HTN exhibited a sensitivity of 75.5% and specificity of 96.4%.14 Despite several studies in Uganda investigating the prevalence of HTN, there are limited data on the prevalence of self-reported HTN in Uganda. Therefore, this study was conducted to determine the community-level prevalence and factors associated with self-reported HTN among adults in Butambala district, Uganda.
Methods
Study Design and Setting
We conducted a community-based cross-sectional study among adults from Budde Subcounty, Butambala district, central Uganda. Budde Subcounty, which is located in Butambala district in the central region of Uganda. Butambala district is approximately 68 kilometers, southwest of Kampala, Uganda’s capital and largest city. Budde Subcounty consists of four parishes and 21 villages, with a total population of approximately 13,800 people.
Study Population and Eligibility Criteria
Participants were individuals aged 18 years and above who were residents of Budde Subcounty during the data collection period and willing to participate in the study. A resident was defined as someone who had stayed within the area for at least 3 months and expected to stay for another 3 months, based on the residency rules of Uganda. Individuals with critical illness or mental retardation were excluded from the study.
Sample Size, Recruitment, and Sampling Approach
The sample size was determined using the equation obtained from the STEPS-WHO stepwise Approach to chronic disease and risk factor surveillance.15 A prevalence of 6.3% for HTN, obtained from the rural Uganda noncommunicable disease (RUNCD) Survey (2021), was used in the calculation. With a permissible error of 5% and a 95% confidence interval, the sample size was calculated to be approximately 600, considering an expected response rate of 0.9 and accounting for age-sex estimates. The target sample size was obtained through simple random sampling from the four parishes.
Data Collection
Data were collected during household visits within the community using an interviewer-administered questionnaire obtained from the WHO Stepwise Approach to Chronic Disease Risk Factors Surveillance (https://www.who.int/teams/noncommunicable-diseases/surveillance/systems-tools/steps/instrument). The questionnaire collected data on social demographic characteristics and behavior. Data on self-reported HTN were collected using a single question: “Do you have high blood pressure?” Participants who responded “YES” were considered to have self-reported hypertension, those who responded “NO” were considered to have normal blood pressure, and those who responded “I do not know” were categorized as unaware of their blood pressure status.
Data Management and Analysis
Data were cleaned, coded and entered into Microsoft 2016 and exported for analysis using STATA version 16.0 analysis software. Numerical data were assessed for normality using the Shapiro‒Wilk test. Continuous variables were expressed as the mean and standard deviation for parametric variables or median and interquartile range for nonparametric variables. Categorical data are presented as frequencies and percentages. Chi-square or Fischer’s exact tests were used to compare categorical variables as appropriate, and Student’s t tests or Mann‒Whitney U-tests were used for numerical variables. Multivariable logistic regression analysis using the forward, stepwise logistic regression analysis model was used to determine factors associated with self-reported HTN, and the results are presented as adjusted odds ratios with corresponding 95% confidence intervals. A p<0.05 was considered statistically significant.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Gulu University Research Ethics Committee before data collection (Approval number GUREC-2022-233). Written informed consent was obtained from every participant. The study was conducted in accordance with the Declaration of Helsinki-2013.
Results
A total of 567 participants (response rate, were approached for the study, out of which 2 declined to provide written informed consent and were excluded. The final analysis included 565 participants, resulting in a response rate of 94.2% (565/600).
Sociodemographic Characteristics of Participants
Of the 565 participants, 302 (53.5%) were female, and the median age was 38 years, with an interquartile range (IQR) of 26–52 years. The majority (28.1%, n=159) were from Budde parish. Nearly half of the participants (48.9%, n=254) were aged 40–59 years, most (79.1%, n=446) were married and living together, and 276 (46.7%) had completed primary education. Most participants (33.5%, n=188) were employed in the private sector. Table 1
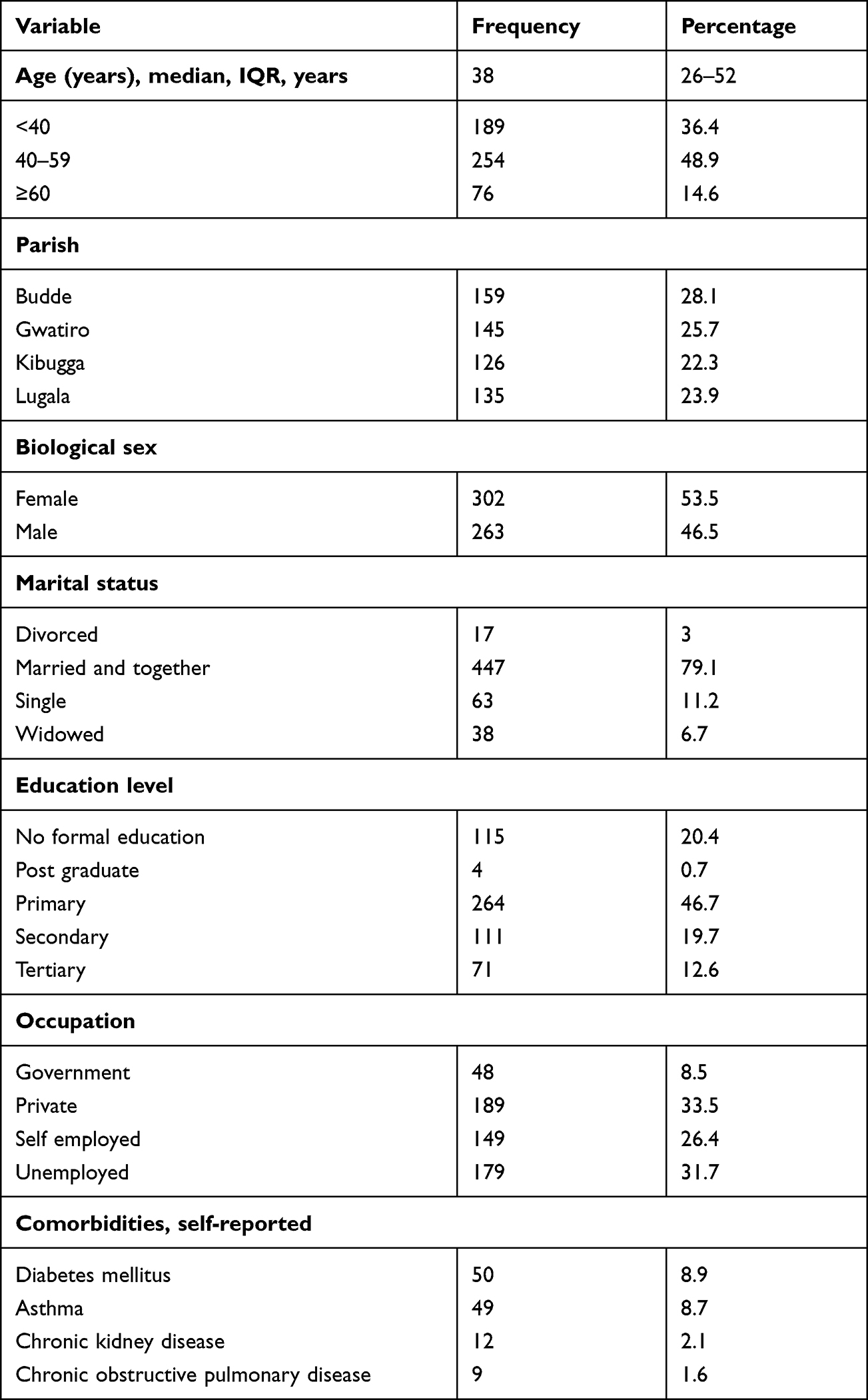 |
Table 1 Demographic Characteristics of the Study Participants (N=565) |
Frequency of Risk Factors for Hypertension
One hundred ninety-nine participants (35.2%) reported alcohol use, with the majority (89.5%, n=178) reporting current use. One hundred twenty-six participants (22.3%) reported tobacco use, with most (73%, n=94) reporting daily use. The majority of the participants (89%, n=508) reported high salt intake (added salt to already salted food). The most common comorbidities reported were diabetes mellitus (8.9%, n=50). Furthermore, 71.9% (n=406) of participants reported having a family history of high blood pressure.
Blood Pressure Status and Prevalence of Self-Reported Hypertension
Most of the participants (60.5%, n=342) had undergone at least one blood pressure measurement, with the majority reporting having it done during antenatal care services (55.9%, n=191), followed by hospital visits for ill health (36%, n=123) and medical check-ups (8.1%, n=28). The overall prevalence of self-reported HTN was 18.9% (n=107). However, 48.5% (n=274) were unaware of their blood pressure status.
Factors Associated with Self-Reported HTN
Participants with self-reported HTN were significantly older (p<0.001), predominantly female (p<0.001), widowed (p<0.001), had no formal education (p=0.002), were unemployed (p=0.006), smoked tobacco (p<0.001), and had a family history of HTN (p<0.001) compared to those without self-reported HTN (Table 2).
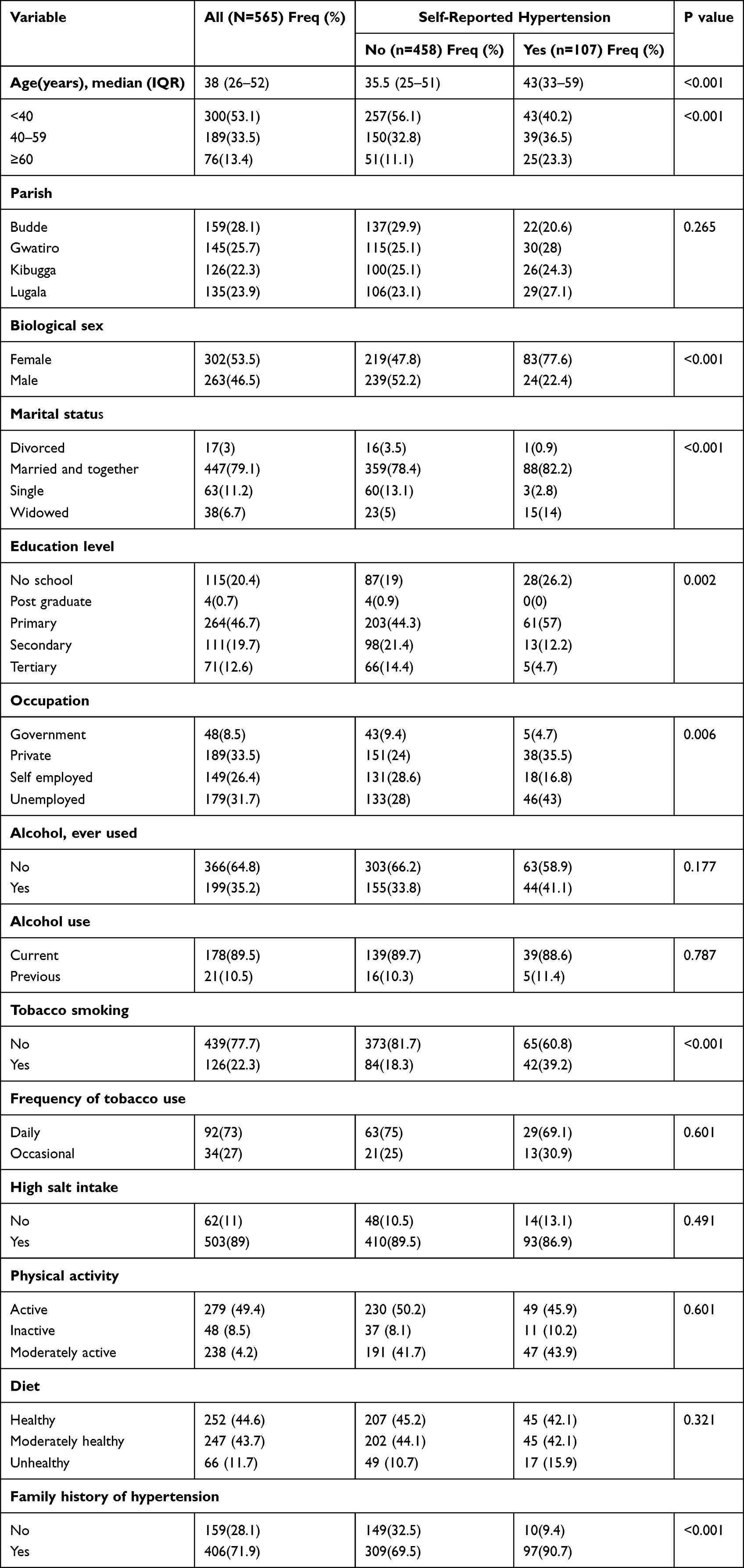 |
Table 2 Bivariate Analysis of Factors Associated with Self-Reported Hypertension (N=565) |
Factors independently associated with self-reported HTN were age 60 years or older (aOR: 2.9, 95% CI: 1.64–5.23, p<0.001), female sex (aOR: 3.3, 95% CI: 2.3–6.3, p<0.001), being widowed (aOR: 10.4, 95% CI: 1.25–87.14, p=0.03), secondary (aOR: 0.4, 95% CI: 0.20–0.85, p=0.016) and tertiary (aOR: 0.2, 95% CI: 0.09–0.64, p=0.005) education, unemployment (aOR: 3.0, 95% CI: 1.11–7.96, p=0.03), tobacco use (aOR: 2.9, 95% CI: 1.83–4.53, p<0.001), having had at least one blood pressure measurement during antenatal visit (aOR: 4.7, 95% CI: 1.97–11.33, p<0.001) or medical checkup (aOR: 10.7, 95% CI: 6. Table 3.
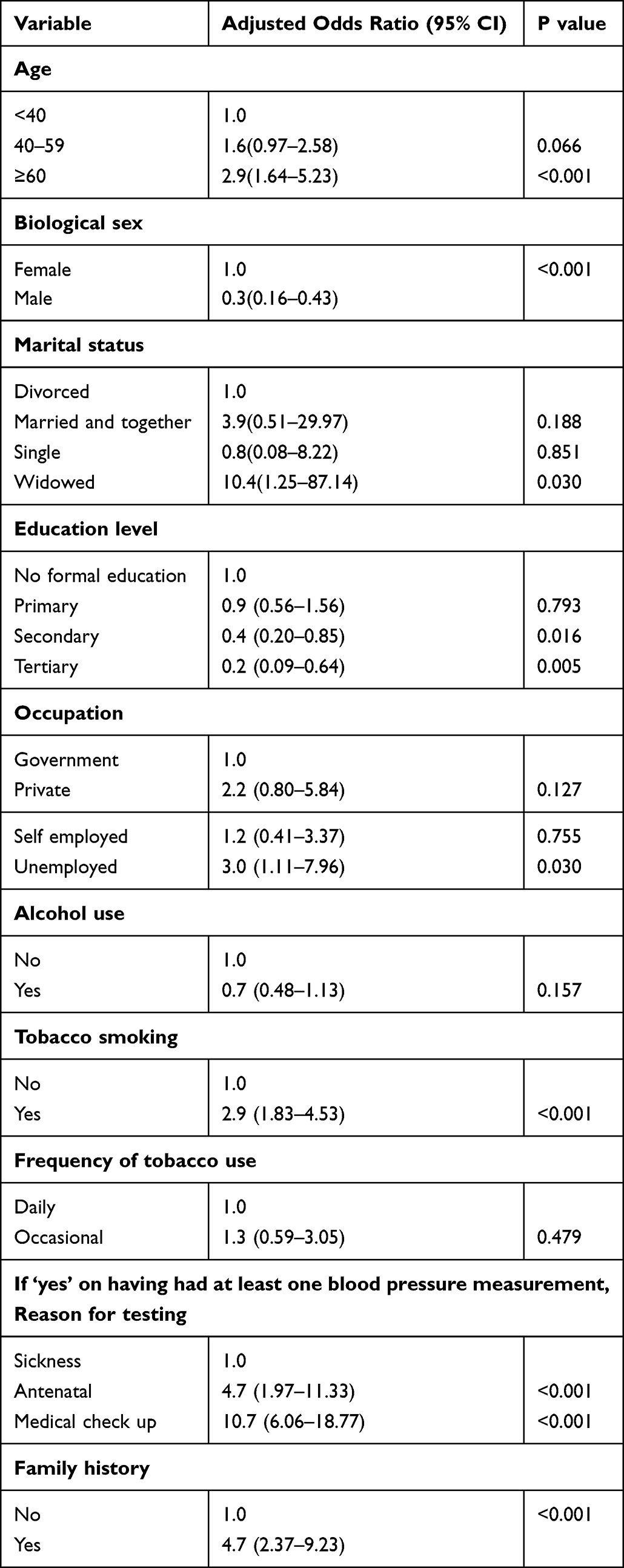 |
Table 3 Multivariable Analysis of Factors Associated with Self-Reported Hypertension (N= 565) |
Discussion
In this study, we aimed to determine the community-level prevalence and factors associated with self-reported HTN among adults in Butambala District, Uganda. We found that the prevalence of self-reported HTN was 18.9%. The population prevalence of self-reported HTN was estimated at 7.8/1000 persons. Nearly half (48.5%) of the participants were unaware of their blood pressure status. Factors that demonstrated independent associations with self-reported HTN were age 60 years or older, female sex, being widowed, secondary and tertiary education, unemployment, tobacco use, having had at least one blood pressure measurement during antenatal visits or medical visits, and a family history of HTN.
Our findings are consistent with studies conducted in various countries, which reported relatively similar prevalence rates of self-reported HTN estimated at 13.6% in Zimbabwe,16 15.7% in China,17 16.8% in Iran,14 23.6% in South Africa18 and 24.1% in Brazil.19 However, studies in the United States and South Africa reported higher prevalence rates of 32.4% and 30.3%, respectively.13,20 Conversely, a recent study in Nakaseke District by Siddharthan et al reported a relatively low prevalence of self-reported HTN of 6.3%.21 These variations highlight the considerable differences in self-reported HTN prevalence across different populations, possibly influenced by various factors such as methodological differences, socioeconomic status, and sociocultural norms.
The high prevalence of self-reported HTN observed in our study can be attributed to several factors. Age emerged as a significant independent factor, with a higher likelihood of self-reported HTN among older individuals.19 An increase in blood pressure with age is mostly related to changes in arterial and arteriolar stiffness. Large artery stiffness is mainly due to arteriosclerotic structural alterations and calcification. The increase in life expectancy and the transition to a more sedentary lifestyle may contribute to the higher prevalence among older individuals. Furthermore, women were more likely to report being hypertensive. This could be due to higher healthcare-seeking behaviors among females compared to males, leading to better detection and reporting of HTN.22 In addition, our study showed an association between unemployment and higher self-reported HTN prevalence, aligning with previous studies such as by Qin et al in Nanjing that have established a link between socioeconomic status and HTN risk.19,23 Unemployment poses a significant risk for developing hypertension due to multiple interconnected factors, including financial strain, psychological stress, and the adoption of unhealthy lifestyle behaviors such as sedentary habits, poor dietary choices, and substance abuse.24
Tobacco use has been shown to have detrimental effects on cardiovascular health, as it increases the risk of developing HTN among users.19,25,26 In our study, individuals who reported using tobacco had almost 3 times higher odds of hypertension than nonusers, which is comparable to findings by Solomon et al who reported a fourfold increase in the risk of developing HTN among smokers compared to their counterparts.27 Smoking causes an acute increase in blood pressure and heart rate and has been found to be associated with malignant HTN. Nicotine acts as an adrenergic agonist, mediating local and systemic catecholamine release and possibly the release of vasopressin.28 Furthermore, individuals who reported a family history of HTN had almost 5-fold higher odds of HTN than those without, which is relatively similar to findings from a study in Southwest Ethiopia where a family history of HTN was associated with an approximately threefold increase in the risk of developing HTN.27 Blood relatives tend to have many of the same genes that can predispose a person to HTN and share some habits, such as diet, exercise, and smoking, that can lead to high cholesterol, high body fat, and being more sensitive to the effects of salt on raising blood pressure.29
This study has some limitations. Self-reporting of HTN may have introduced the possibility of information bias that might have contributed to underreporting of the prevalence of HTN. Blood pressure measurements were not taken during the study to confirm the self-reported data. The cross-sectional design limits the establishment of causal relationships between the identified factors and HTN. Furthermore, the study was conducted in a specific district in Uganda, which may limit the generalizability of the findings to other regions of the country.
Conclusion
We observed a high prevalence of self-reported HTN, affecting approximately one in five adults, with a significant proportion of adults being unaware of their blood pressure status. There is an urgent need for enhanced routine screening, health education, and improved accessibility to HTN services, especially in rural areas, with a particular emphasis on implementing HTN prevention and control strategies to effectively reduce the prevalence of HTN.
Abbreviations
HTN, Hypertension; WHO, World Health Organization; RUNCD, Rural Uganda noncommunicable disease.
Data Sharing Statement
All relevant data are within the manuscript.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Gulu University Research Ethics Committee before data collection (Approval number GUREC-2022-233). Written informed consent was obtained from every participant. The study was conducted in accordance with the Declaration of Helsinki-2013.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
No external funding was received for this study.
Disclosure
All authors declare that they have no conflicts of interest for this work.
References
1. GBD 2017 Causes of Death Collaborators, Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017:A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788. doi:10.1016/S0140-6736(18)32203-7
2. Sarki AM, Nduka CU, Stranges S, Kandala NB, Uthman OA. Prevalence of hypertension in low- and middle-income countries: a systematic review and meta-analysis. Medicine. 2015;94(50):e1959. doi:10.1097/MD.0000000000001959
3. World Health Organization. Hypertension; 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/hypertension.
4. Mensah GA. 7.2 Epidemiology and global burden of hypertension. ESC Cardio Med. 2018:291–297. doi:10.1093/med/9780198784906.003.0061
5. Lunyera J, Kirenga B, Stanifer JW, et al. Geographic differences in the prevalence of hypertension in Uganda: results of a national epidemiological study. PLoS One. 2018;13(8):e0201001. doi:10.1371/journal.pone.0201001
6. Everett B, Zajacova A. Gender differences in hypertension and hypertension awareness among young adults. Biodemography Soc Biol. 2015;61(1):1–17. doi:10.1080/19485565.2014.929488
7. Uganda M. Non communicable disease risk factor baseline survey. Uganda 2014 Report; 2014:23–50.
8. Cruickshank JK, Mbanya JC, Wilks R, et al. Hypertension in four African-origin populations: current ‘Rule of Halves’, quality of blood pressure control and attributable risk of cardiovascular disease. J Hypertens. 2001;19(1):41–46. doi:10.1097/00004872-200101000-00006
9. Hoel D, Howard RB, Gifford RW. Hypertension: stalking the silent killer. Postgrad Med. 1997;101(2):116–121. doi:10.3810/pgm.1997.02.155
10. Unger T, Borghi C, Charchar F, et al. 2020 International Society of Hypertension global hypertension practice guidelines. J Hypertens. 2020;38(6):982–1004. doi:10.1097/HJH.0000000000002453
11. Wu CY, Hu HY, Chou YJ, Huang N, Chou YC, Li CP. High blood pressure and all-cause and cardiovascular disease mortalities in community-dwelling older adults. Medicine. 2015;94(47):e2160. doi:10.1097/MD.0000000000002160
12. Gonçalves VSS, Andrade KRC, Carvalho KMB, Silva MT, Pereira MG, Galvao TF. Accuracy of self-reported hypertension: a systematic review and meta-analysis. J Hypertens. 2018;36(5):970–978. doi:10.1097/HJH.0000000000001648
13. Samanic CM, Barbour KE, Liu Y, et al. Prevalence of self-reported hypertension and antihypertensive medication use among adults - United States, 2017. MMWR Morb Mortal Wkly Rep. 2020;69(14):393–398. doi:10.15585/mmwr.mm6914a1
14. Najafi F, Pasdar Y, Shakiba E, et al. Validity of Self-reported Hypertension and Factors Related to Discordance Between Self-reported and Objectively Measured Hypertension: evidence From a Cohort Study in Iran. J Prev Med Public Health. 2019;52(2):131–139. doi:10.3961/jpmph.18.257
15. World Health Organization. WHO STEPS Instrument (Core and Expanded): The WHO STEPwise Approach to Chronic Disease Risk Factor Surveillance (STEPS). Geneva; 2014.
16. Davis K, Moorhouse L, Maswera R, et al. Associations between HIV status and self-reported hypertension in a high HIV prevalence sub-Saharan African population: a cross-sectional study. BMJ open. 2023;13(1):e067327. doi:10.1136/bmjopen-2022-067327
17. Su M, Si Y, Zhou Z, et al. Comparing the income-related inequity of tested prevalence and self-reported prevalence of hypertension in China. Int J Equity Health. 2018; 17:1. doi:10.1186/s12939-017-0710-z
18. Ntenda PAM, El-Meidany WMR, Tiruneh FN, et al. Determinants of self-reported hypertension among women in South Africa: evidence from the population-based survey. Clinical Hypertension. 2022;28(1):39. doi:10.1186/s40885-022-00222-5
19. Malta DC, Bernal RTI, Andrade S, Silva M, Velasquez-Melendez G. Prevalence of and factors associated with self-reported high blood pressure in Brazilian adults. Rev Saude Publica. 2017;51(suppl 1):11 s. doi:10.1590/s1518-8787.2017051000006
20. Phaswana-Mafuya N, Phaswana-Mafuya N. Self-reported prevalence of chronic noncommunicable diseases and associated factors among older adults in South Africa. Glob Health Action. 2013;1-8:6. doi:10.3402/gha.v6i0.18871
21. Siddharthan T, Gautier L, Radermacher R, Srivastava S, Meshack M, De Allegri M. The rural Uganda noncommunicable disease (RUNCD) study: prevalence and risk factors for self-reported NCDs from a cross sectional survey. BMC Public Health. 2021;21(1):1–8. doi:10.1186/s12889-020-10013-y
22. Ilinca S, Di Giorgio L, Salari P, Chuma J. Socioeconomic inequality and inequity in use of health care services in Kenya: evidence from the fourth Kenya household health expenditure and utilization survey. Int J Equity Health. 2019;18(1):1–13. doi:10.1186/s12939-019-1106-z
23. Qin Z, Li C, Qi S, et al. Association of socioeconomic status with hypertension prevalence and control in Nanjing: a cross-sectional study. BMC Public Health. 2022;22(1):423. doi:10.1186/s12889-022-12799-5
24. Nygren K, Gong W, Hammarström A. Is hypertension in adult age related to unemployment at a young age? Results from the Northern Swedish Cohort. Scand J Public Health. 2015;43(1):52–58. doi:10.1177/1403494814560845
25. Virdis A, Giannarelli C, Neves MF, Taddei S, Ghiadoni L. Cigarette smoking and hypertension. Curr Pharm Des. 2010;16(23):2518–2525. doi:10.2174/138161210792062920
26. Gao N, Liu T, Wang Y, et al. Assessing the association between smoking and hypertension: smoking status, type of tobacco products, and interaction with alcohol consumption. Front cardiovasc Med. 2023;10:1027988. doi:10.3389/fcvm.2023.1027988
27. Solomon M, Shiferaw BZ, Tarekegn TT, et al. Prevalence and Associated Factors of hyprtension among adults in Gurage zone, Southwest Ethiopia. SAGE Open Nurs. 2023;9:23779608231153473.
28. Primatesta P, Falaschetti E, Gupta S, Marmot MG, Poulter NR. Association between smoking and blood pressure: evidence from the health survey for England. Hypertension. 2001;37:187–193.
29. CDC. Know Your Risk for High Blood Pressure. Center for Disease Control and Prevention; 2020:1–4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.