")
Back to Journals » Drug, Healthcare and Patient Safety » Volume 15
Self-Medication and Associated Factors Among Pregnant Women in Rural Ethiopia: The Importance of Husband Education in Ensuring a Safe Pregnancy
Authors Tujuba TD, Chilo D , Abebe E, Zenu S
Received 21 October 2022
Accepted for publication 11 February 2023
Published 15 February 2023 Volume 2023:15 Pages 39—50
DOI https://doi.org/10.2147/DHPS.S394346
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Siew Siang Chua
Takele Deribu Tujuba,1 Desalegn Chilo,2 Endegena Abebe,3 Sabit Zenu1
1Department of Public Health, College of Health Science, Mattu University, Mettu, Ethiopia; 2Department of Pharmacy, College of Health Science, Mattu University, Mettu, Ethiopia; 3Department of Biomedical Sciences, College of Health Science, Mattu University, Mettu, Ethiopia
Correspondence: Sabit Zenu, Mettu, Ethiopia, Tel +251917751066, Email [email protected]
Background: Self-medication is the use of drugs without a medical prescription to treat self-identified illnesses; it is also the continued use of drugs without a physician’s order for recurring symptoms, either by sharing or purchasing them from unlicensed vendors. It entails substantial risk to pregnant women and fetuses. Magnitude of the problem and its factors among rural pregnant women is not studied in Ethiopia.
Objective: This study aimed to assess the prevalence of self-medication practice and identify its associated factors among pregnant women in rural Southwest Shewa, Ethiopia.
Methods: A cross-sectional study was conducted on 585 randomly selected pregnant women in selected rural public health institutions from May to July 2021. Data was collected by using an interviewer-administered pretested structured questionnaire. Multivariable logistic regression was used to identify factors associated with self-medication. Variables with p-value < 0.05 for the 95% confidence interval of the adjusted odds ratio were considered statistically significant.
Results: A total of 585 pregnant women participated in the study with a response rate of 92.3%. The prevalence of self-medication among pregnant women was 19.8%. Primigravidity (AOR = 2.7, 95% CI: 1.2– 6.1), lower educational status of husbands (AOR = 3.6, 95% CI: 1.02– 12.9), living close to health facilities (AOR = 0.23, 95% CI: 0.09– 0.6) and knowing one’s own gestational age (AOR = 0.5,95% CI: 0.30– 0.9) were significantly associated with self-medication practice.
Conclusion and Recommendation: One in five of the pregnant women practiced self-medication during the current pregnancy. Primigravidity and lower educational status of husbands were associated with a higher probability of self-medication. Knowing gestational age and living close to health facilities were associated with a lower likelihood of practicing self-medication. Rational drug use has to be promoted among pregnant women. Maternal and child health interventions should also target husbands. Health education has to be strengthened to help pregnant women have a safe pregnancy.
Keywords: self-medication, pregnant women, antenatal care, Southwest Shewa, Mettu University
Introduction
Pregnancy is a unique physiological condition where drug treatment presents a special concern. The drugs given to or taken by pregnant mothers for various purposes may cause serious adverse effects on mother and the foetus.1 More importantly, any effect on fetal development will not be immediately evident, and the harm that ensues may have lifelong adverse consequences.2 Thus, medication safety in pregnancy is of utmost importance.2
The World Health Organization (WHO) defines rational use of medicines as “a process that allows the prescribing of the right drug for the right patient in the proper dose, duration of therapy, and at the lowest cost to the patient and the community”. In spite of this, more than 50% of all medicines are prescribed, issued, or sold inappropriately. Self-medication is one of the most common types of irrational drug use.3 It has traditionally been defined as the taking of drugs on one’s own initiative, or on the advice of another person, without consulting a physician.4
Self-medication is influenced by several factors. The media and extensive advertising plays an important role in encouraging the practice. Inadequacies in the health-care systems, high treatment costs, and patients’ attitudes toward health-care providers are some of the key drivers of self-medication.4,5 Though practiced widely, self-medication could lead to multiple health problems ranging from minor drug reactions to severe health problems and death.6 Self-medication can impact health of communities both negatively and positively. It is generally detrimental to the health of individuals and the community especially for potentially vulnerable segments of the population like pregnant women causing range of problems both to the mother and the fetus.7
The prevalence of self-medication among pregnant women is reported to be high both in developed and developing countries. The pooled prevalence of SMP in Africa is documented as 55%.8 Considering specific countries in the continent, the prevalence of the problem among pregnant women is as high as 88% in Ghana9 and 72.4% in Nigeria.10 A multinational study in developed countries also indicated that as many as two-thirds of pregnant women practiced self-medication during their latest pregnancy.11 The prevalence of SMP among pregnant women is 50% in Italy.12 This problem is relatively low in Iran where a third of pregnant women practiced self-medication during their latest pregnancy.13 It is much lower in the Netherlands with a prevalence of 12.5%.14
In Ethiopia, the data on the prevalence of SMP among pregnant women mainly come from studies conducted in urban centers. The studies conducted in Addis Ababa, Jimma, Nekemte, Gondar, Mekelle, and Bahir Dar cities showed a concerning prevalence of SMP, reaching up to 44% in Gondar15 and 40.8% in Mekelle.16 In Addis Ababa, the prevalence was 26.6%.17 A study in a tertiary hospital in Jimma found that nearly a third of women practiced self-medication.18 A study in Nekemte hospital reported a relatively lower prevalence of SMP with 21.5%.19 In Bahir Dar, 25.1% of studied pregnant women reported self-medication during the latest pregnancy.20
As stated earlier, studies on SMP among pregnant mothers in Ethiopia were mainly conducted in major urban centres. Contrarily, large proportion of pregnant women live in rural areas where health-care coverage is low, implementation of regulations is weak and women lack basic drug safety information, opening doors for SMP and its consequences in rural areas.21 In Ethiopia, rural women are largely illiterate. According to the recent survey by the Ethiopian Central Statistical Agency (CSA), the proportion of illiterate women in rural areas was 70.2%.22 In addition, there is poor regulation of pharmacy practice where drugs are even sold in shops by individuals who have no medical training or education.7 This opens the door for the detrimental effects of self-medication among rural pregnant women. Despite this, no published study has been found to address the problem of SMP among rural pregnant women or other similar comparable settings. Assessing the prevalence of this problem and identifying its factors among rural pregnant women will help in drawing attention to and preventing the problem. This study accordingly assessed the prevalence of SMP and identified its associated factors among pregnant women in rural areas of the Southwest Shewa, Ethiopia.
Materials and Methods
Study Area, Design and Period
The study was conducted in rural areas of the Southwest Shewa Zone of Oromia Region. According to the latest census, the total population in the study area was 122,056; of which 61,578 were men and 60,478 were women. There are forty health posts, eight health centers (HC), and one primary hospital with 7023 registered pregnant women receiving Antenatal Care (ANC) follow-up in the study area in 2021. The study was conducted from May to July, 2021 by employing a cross-sectional study design.
Populations
All registered pregnant women in the rural Southwest Shewa zone in 2021 were target populations. Registered pregnant women in the selected health institutions during the study period were source populations. Registered pregnant women who fulfilled the inclusion criteria and selected through systematic random sampling were the study populations.
Inclusion and Exclusion Criteria
All pregnant women who were residents of the study area, registered as pregnant women in family folders of health posts, and available for ANC service during data collection were included in this study. Pregnant women who were professional employees of health institutions or who are married to health professionals were excluded.
Sample Size Determination
The sample size was determined using the single population proportion formula for the prevalence of SMP and the double population proportion formula for the associated factors. For the single population proportion, prevalence of self-medication of 26.6%,17 margin of error of 5% (d = 0.05) and 95% confidence interval (CI) were used. The sample size for the second objective was calculated using the double population proportion formula on Epi info-7 using the parameters stated in Table 1. After calculating the sample size for both specific objectives, the maximum sample size, which was 317, was taken. Additionally, a design effect of two (2) was used and the final sample size became 634 study participants.
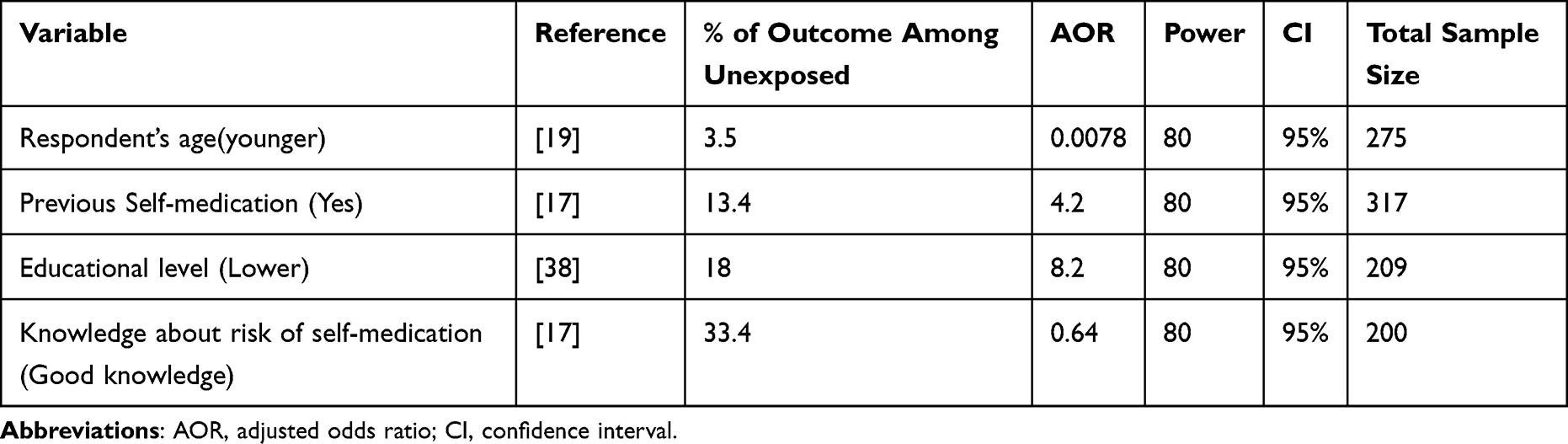 |
Table 1 Calculation of Sample Size for the Main Factors Associated with Self-Medication Practice Among Pregnant Women on Epi Info-7, 2021 |
Sampling Technique
The study area has a total of 7023 registered pregnant women. The women were registered in nine public health facilities in the study area. From the nine facilities, four HCs and one primary hospital were randomly selected. Proportional numbers of pregnant women were allocated to the selected health facilities. Participants in the specific health facilities were selected using a systematic random sampling technique from the registry. The detail of sampling procedure is presented in Figure 1.
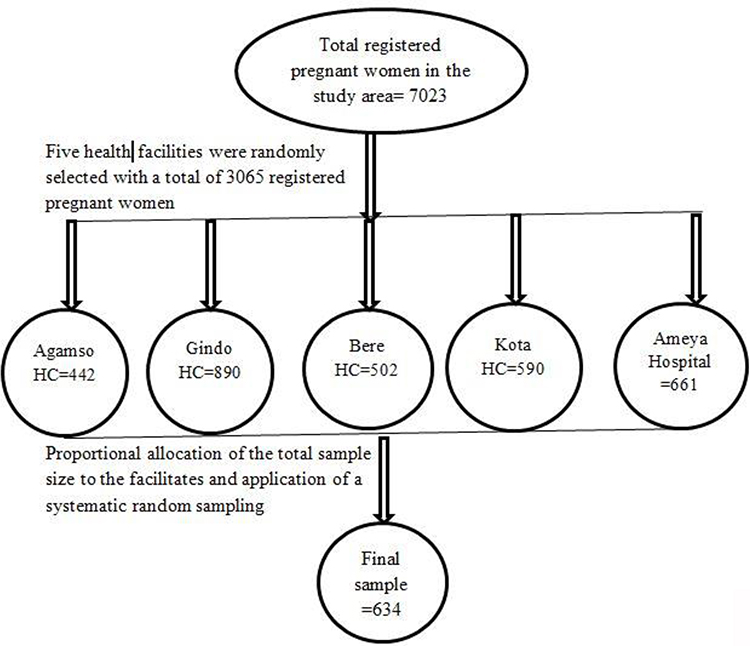 |
Figure 1 Diagrammatic presentation of the sampling procedure for the study to determine the prevalence of self-medication practice and associated factors among pregnant women in the study area. |
Data Collection Tools and Procedures
Data was collected through face-to-face interviews of pregnant women using a structured questionnaire. The questionnaire for independent variables was adopted from the Ethiopian Demographic and Health Survey (EDHS) questionnaire.23 The collected variables include socio-demographic characteristics, history of previous, history of current pregnancy, accessibility of healthcare and utilization of the services. Self-medication practice is assessed with one question asked as “Have you used a modern medication like pills, or through blood or muscles or any other routes on your own, without a prescription or guidance of a health professional during the current pregnancy?”. The mothers responded with “yes” if they made use of such drugs and “no” if they did not use one. The data collection tool was pretested on 50 pregnant women away from the study area and has a good reliability with Cronbach’s alpha value of 0.76. Data was entered into Epidata version 3.1 and exported to SPSS version 23 for analysis.
Data Analysis Procedures
Appropriate descriptive statistics were used to describe continuous variables depending on their distribution. Normality was checked using the Kolmogorov-Smirnov normality test. Continuous variables with a Kolmogorov-Smirnov test p-value of >0.05 were considered normally distributed. Frequencies and proportions were used to describe categorical variables. Bivariable logistic regression was performed. Variables with p<0.25 in the bivariable model were included in multivariable logistic regression. Backward stepwise multivariable logistic regression was used to identify factors that are significantly associated with SMP. Variables with a p-value <0.05 for the 95% CI of the adjusted odds ratio (AOR) were considered statistically significant.
Operational Definition
SMP is defined as the use of drugs to treat self-identified illnesses or disorders without a medical prescription; it is also a continued use of drugs without the order of physicians for recurrent symptoms either by sharing from other person or buying them from unlicensed body.4 Participants who responded ‘Yes’ to the question. “Have you used a modern medication like pills, or through blood or muscles or any other routes on your own, without a prescription or guidance of a health professional during the current pregnancy?” were regarded as practicing self-medication.
Ethics Statement
The study was conducted in line with the principles of the Declaration of Helsinki. Ethical clearance was obtained from the ethics review committee of the College of Health Science at Mattu University with reference number RPG-20-2013 issued on 03/09/2013 Ethiopian Calendar (EC) (Tuesday, May 11, 2021 of the Gregorian Calendar). Participants provided written informed consent after the provision of comprehensive information concerning the study. Confidentiality of participants was maintained at all levels.
Results
Socio Demographic and Obstetric Characteristics of Study Participants
Of the total 634 sample size, 585 pregnant women consented to participate, with a response rate of 92.3%. Three quarters (434,74.2%) of the respondents were in the age category of 21–30 years. Almost all (99.1%) of the respondents were married and 234 (40%) had completed primary education. More than half of participants were farmers (328, 56%), and half of the participants were followers of protestant religion (Table 2).
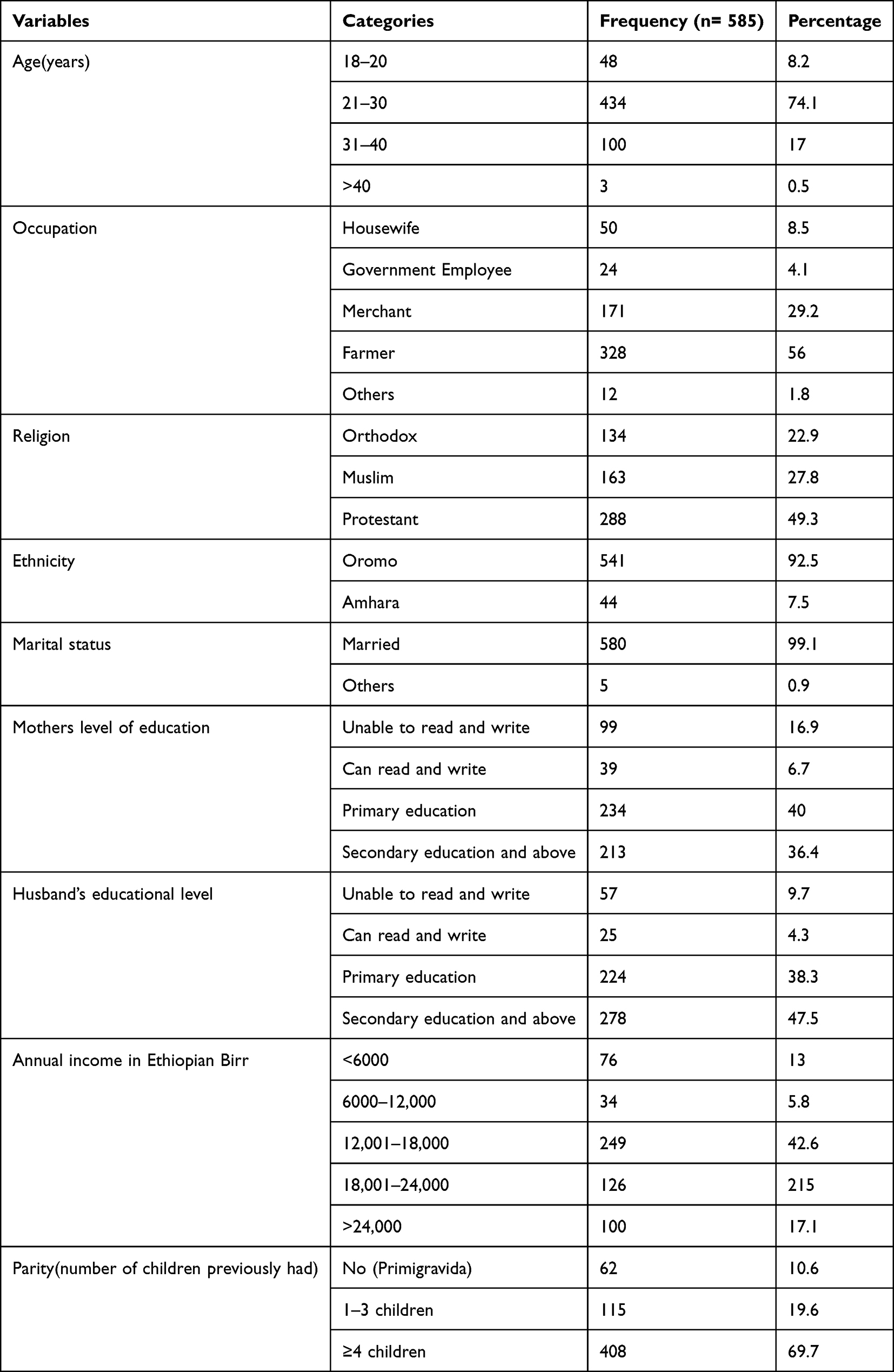 |
Table 2 Socio-Demographic Characteristics of Pregnant Women Attending Selected Public Health Institutions in Southwest Shewa, Ethiopia, 2021 |
Concerning prior history of pregnancy, two-third of the participants had four or more children, and 10.6% became pregnant for the first time. More than three quarters (459, 78.4%) of the participants knew their gestational age. Three hundred thirty three (56.9%) of the participants were in their second trimester. More than half (331,56.6%) of the participants had four or more ANC visits during the current pregnancy. Similarly, 57.4% had a planned pregnancy. Two-third of pregnant women (384,65.7%) walk for less than an hour to reach the nearest health facility (Table 3).
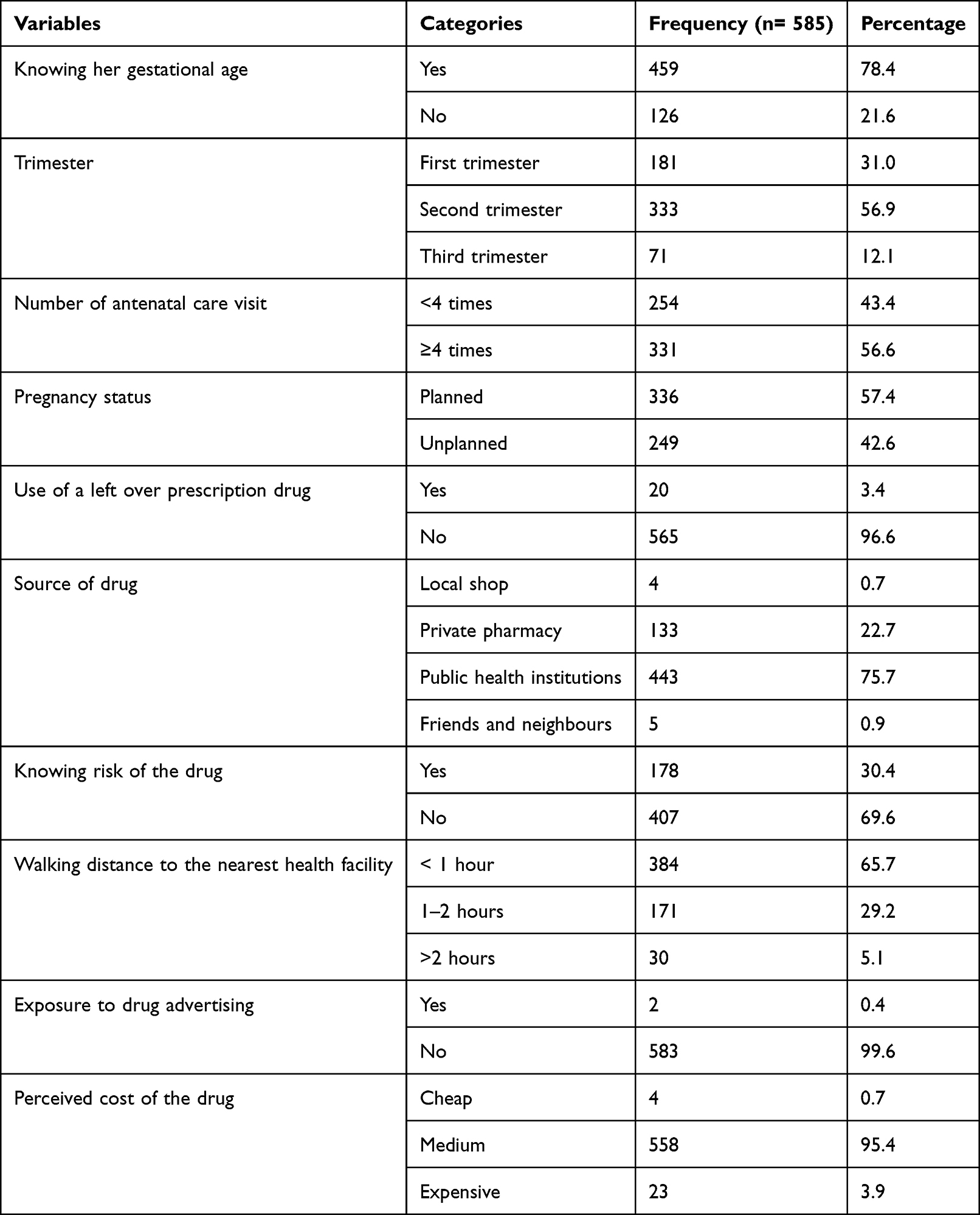 |
Table 3 Obstetric Characteristics of Pregnant Women Attending Selected Public Health Institutions of Rural Southwest Shoa, Ethiopia, 2021 |
Self-Medication Practice
Overall, 116 (19.8%, 95% CI: 16.6%, 23.2%) pregnant women practiced self-medication during the current pregnancy. Seventy-two (62%) of pregnant women who practiced self-medication were between the ages of 21 and 30 years. From respondents with SMP, eighty-nine (76.7%) had an unplanned pregnancy, and the majority (114, 98.3%) were married. A third of pregnant women who practiced self-medication had completed secondary education, and 37 (31.9%) had completed primary education. The mentioned reasons for practicing self-medication among those who self-medicated were: pregnancy-related discomforts 66 (56.9%), unwanted pregnancy 26 (22.4%), easy access to the drugs 15 (12.9%), previous experience about the drug 6 (5.2%), and family pressure 3 (2.6%). Self-medicated respondents were recommended to do so mainly by their husbands (87,75%). The majority of self-medicated respondents (98.5%) stated that they are unaware of any risks associated with the practice (Table 4).
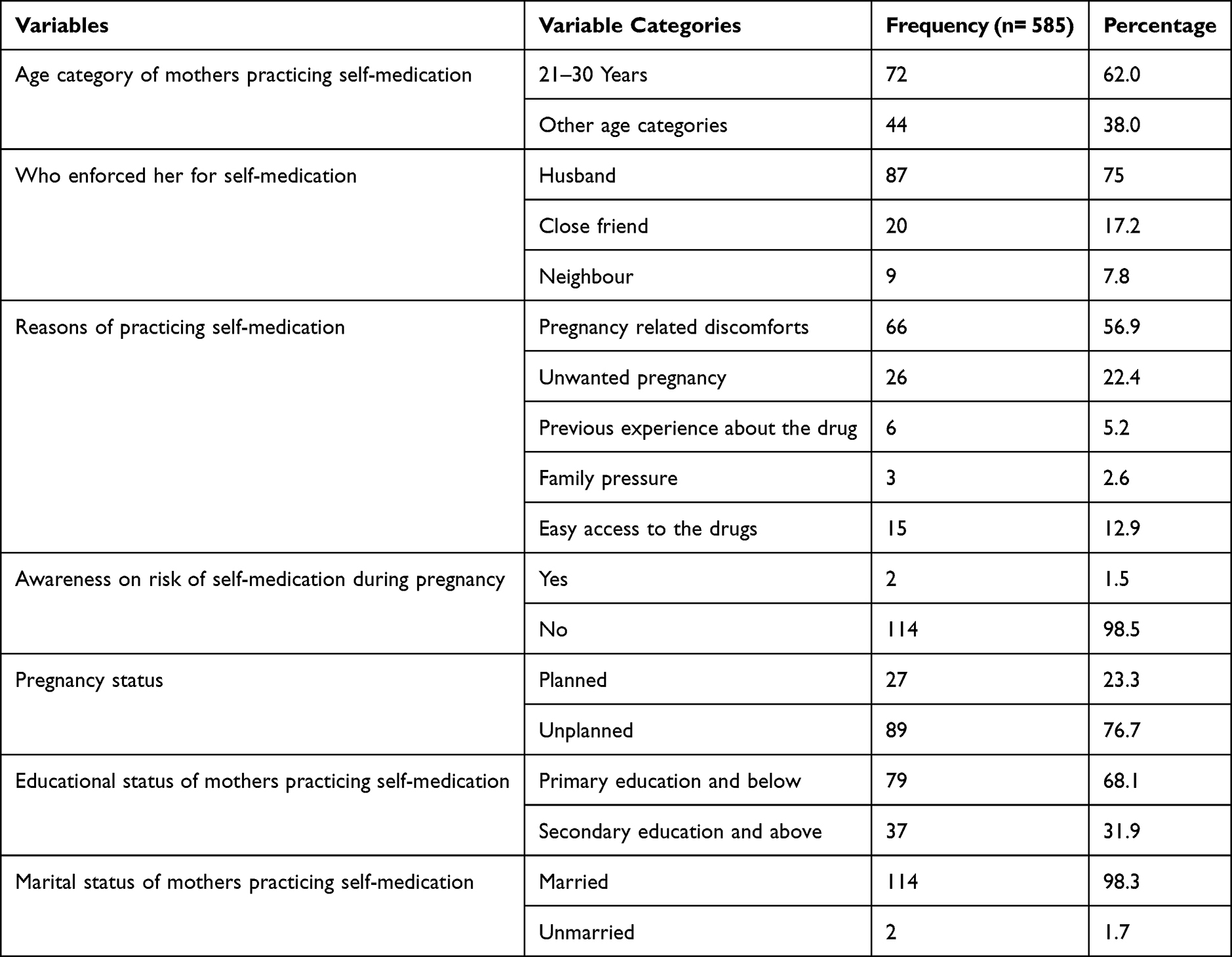 |
Table 4 Cross Tabulation of Self-Medication Practice and Associated Factors Among Rural Pregnant Women in Southwest Shewa, Ethiopia, 2021 |
Factors Associated with Self-Medication Practice
Pregnant women’s level of education, husband’s level of education, number of children, knowledge of gestational age, pregnancy planning status, knowledge about risk of self-medication, the walking distance to the nearest health facility, and cost of the drug are factors with p-value <0.25 in the bivariable logistic regression. From these factors, the husband’s level of education, number of children, knowledge of gestational age, and living close to a health facility were found to be significantly associated with SMP in the multivariate logistic regression analysis (Table 5).
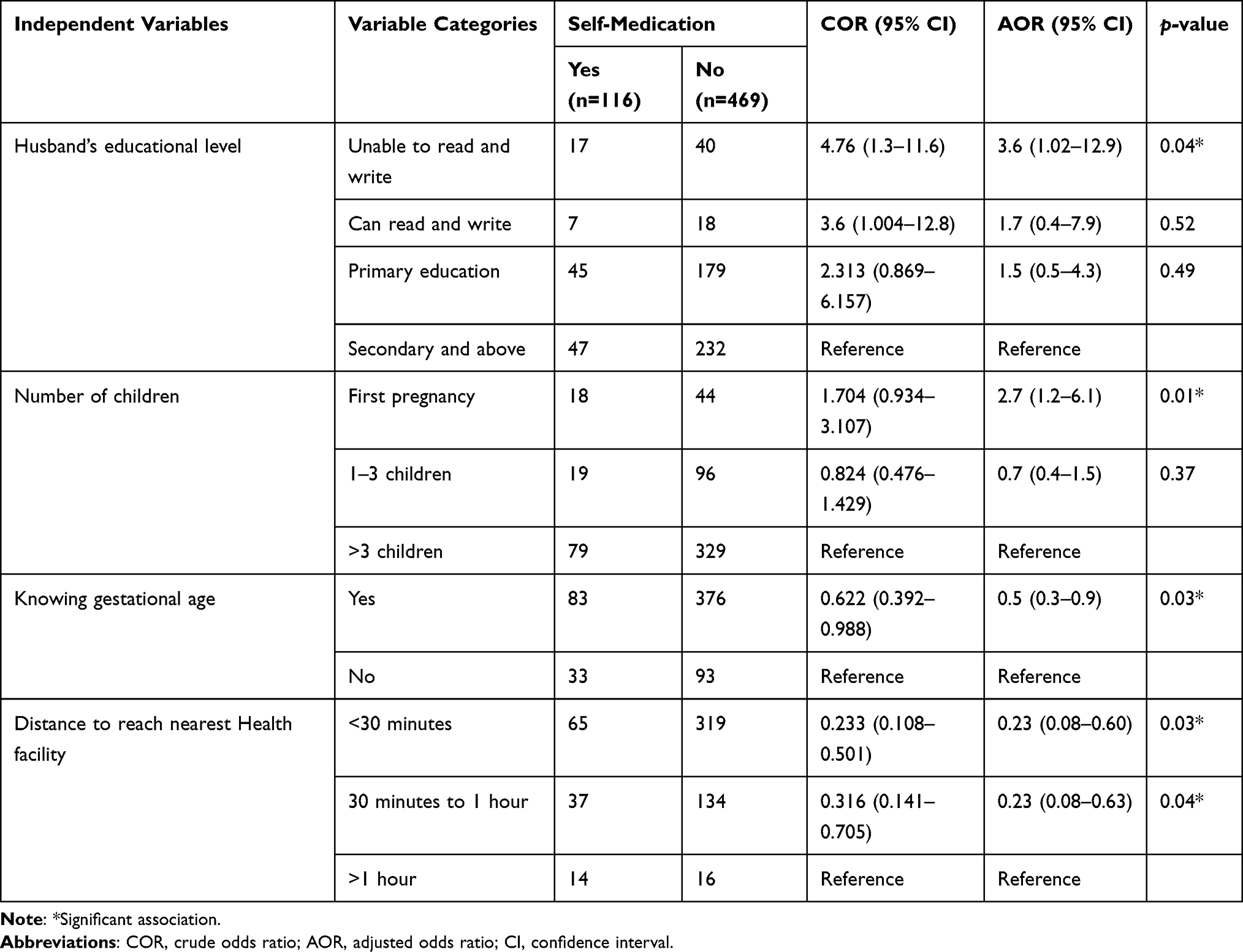 |
Table 5 Significantly Associated Variables in Multivariable Analysis of Self-Medication Among Pregnant Women in Public Health Institutions, Rural Southwest Shewa, 2021 |
Respondents who were pregnant for the first time were nearly three times more likely to practice self-medication than pregnant women who had already given birth (AOR = 2.7, 95% CI 1.2–6.1). In addition, respondents whose husbands were unable to read and write were four times more likely to practice self-medication than women whose husbands had achieved better education (AOR = 3.6, 95% CI 1.01–12.9). Contrary to this, pregnant mothers walking less than an hour to the nearest health facility were 77% less likely to practice self-medication when compared with those walking more than an hour to their nearest health facility (AOR = 0.23, 95% CI 0.08–0.6). Finally, respondents who know their gestational age were 50% less likely to practice self-medication when compared with those who do not know their gestational age (AOR = 0.5, 95% CI 0.3–0.9) (Table 5).
Discussion
This study assessed the prevalence of SMP and identified its associated factors among pregnant women attending antenatal care services in rural areas of the Southwest Shewa zone, Oromia, in 2021. One in five of the pregnant women practiced self-medication during the current pregnancy (19.8%, 95% CI: 16.6%, 23.2%). The prevalence of SMP in the study area is comparable with a report from Nekemte town hospital, where 21% of pregnant women practiced self-medication.19
The observed prevalence of SMP is surprisingly lower than the findings from major urban centres of Ethiopia like Addis Ababa (26.6%),17 Jimma (30%),18 Mekelle (40.8%),16 Gondar (44%)15 and Bahir Dar (25.1%).20 It is also lower than the national prevalence of SMP among the general population (36.8%).24 The relatively lower prevalence of SMP in our study may be due to the difference in study period, residence, and type of medications considered in the studies. Our study was conducted in 2021 as Ethiopia makes significant progress towards universal access to comprehensive maternal health care, including antenatal care for pregnant women. Since 2000, Ethiopia has progressed from total ANC coverage of 27% to 62% in 2016.23 The increased coverage of ANC and other maternal health care may have influenced the practice of mothers overtime. In addition, studies in Addis Ababa and Bahir Dar included the use of herbal drugs and home-made remedies as a SMP, while our study considered the use of modern medications only. The urban status of compared cities has also influenced the practice of pregnant women. Unlike rural residents, educated urban residents tend to practice self-medication as a means of achieving independence in dealing with their health problems.4
Despite this, the observed practice of self-medication is higher than reports from countries outside Ethiopia, like Iran, where 8.7% of pregnant women practice self-medication.25 It is also higher than a finding from Eastern India, where 6% of pregnant women practiced self-medication.26 The low prevalence of SMP in Eastern India may be due to the small sample size of the study that involved only 196 pregnant women while the current study involved 585 participants. The relatively lower level of SMP in Iran may be due to their strong drug control mechanisms.27
Concerning the factors associated with SMP, this study showed the importance of husband’s education as a major factor that is associated with pregnant women practicing self-medication. In the current study, pregnant women whose husbands cannot read and write were nearly four times more likely to practice self-medication when compared with women whose husbands had achieved secondary and above in their education. The role of husbands in maternal health is now well recognized and there are wider calls for further participation of husbands in the maternal health-care continuum.28,29 Interventions engaging men in maternal and child health care can increase care-seeking, improve home care practices, and support couple communication and decision-making for maternal and new-born health.30 In educational interventions, educating pregnant women and their male partners found to yield a greater impact on maternal health behaviors compared with educating women alone.31
Educated husbands are more likely to be engaged in the care of pregnant women. They help in making healthy decisions and intervene to prevent detrimental behaviors, one of which is taking medications against the orders of physicians.32 Corroborating this, a study that summarized demographic and health surveys of 37 countries indicated that partners’ schooling has strong effects on their spouses’ maternal health-care utilization, especially when partners have had secondary or higher levels of schooling. This study showed that women whose partners achieved a secondary or above level of education were 32% more likely to use modern contraceptives, 43% more likely to attend at least four ANC visits, and 55% more likely to deliver their most recent baby with a health professional, compared to women whose partners had no education.33
Pregnant women who had no prior history of pregnancy (primigravidas) were nearly three times more likely to practice self-medication when compared to multiparous women. This shows the susceptibility of pregnancy naive women to risky practices like SMP, and the importance of experience in preventing such practices during pregnancy. According to research, rural primigravidas have little information concerning pregnancy, maternal health care, and risks involving use of medications during pregnancy.34,35 A study in South Ethiopia also found primigravida women to be less prepared for pregnancy complications and less knowledgeable of pregnancy danger signs, indicating the gap between multigravida and primigravida mothers.36 In addition, pregnant women who know their gestational age were 50% less likely to practice self-medication. Pregnant women who know their gestational age are more likely to be alert and their pregnancy is more likely to be planned. This would cause the mothers to be more careful in taking medications during pregnancy. Further, such women are more likely to enroll in the ANC and receive the necessary information for a safer pregnancy. Finally, pregnant mothers who live close to health facilities were less likely to delve into SMP when compared with those who live far from health facilities. This could be due to the transfer of information and easy access to professional medical care whenever health problems happen to pregnant women. Studies have also shown that living close to health facilities improves mothers’ knowledge of basic maternal and new-born care and utilization of health services.37,38
Limitations
This study assessed the unauthorized use of modern medications among pregnant women in rural areas and did not include traditional medications. Furthermore, the study only included rural women and cannot be generalized to an urban setting in Ethiopia or elsewhere.
Conclusion and Recommendations
The prevalence of self-medication among rural pregnant women in the study is a public health problem with potential harmful consequences to the health of mothers and fetuses. Despite this, the observed prevalence of SMP is lower than the prevalence in major urban centers of Ethiopia. Lower educational achievement of husbands and primigravidity were significantly associated with a higher probability of practicing self-medication. Contrarily, residing close to health facilities and knowledge of gestational age were associated with a lower probability of SMP. This study indicated the importance of husbands to the achievement of optimal health of pregnant mothers. The efforts to achieve maternal and child health targets should also give priority to men through education. Pregnancy naive mothers should be provided with extra care as they lack experience. The strengthening of social networking and facilitation of discussion among pregnant women may help in sharing experiences to prevent unhealthy practices like self-medication. In addition, health services should be expanded to optimize the delivery of health care and education to rural communities so that families take responsibility for their health.
Abbreviations
ANC, antenatal care; AOR, adjusted odds ratio; CI, confidence interval; CSA, Central Statistical Agency; EC, Ethiopian Calendar; EDHS, Ethiopian Demographic and Health Survey; HC, health centers; SMP, self medication practice; SPSS, Statistical Package for Social Sciences; WHO, World Health Organization.
Data Sharing Statement
Data will be available upon the request from the corresponding author.
Ethics Statement
This study was conducted in line with the principles of the Declaration of Helsinki. Ethical clearance was obtained from the ethics review committee of the College of Health Science at Mattu University with reference number RPG-20-2013 issued on 03/09/2013 EC. Participants provided written informed consent after the provision of comprehensive information concerning the study. Confidentiality of participants was maintained at all levels.
Acknowledgment
We thank Mattu University college of health science for helping in the arrangement of this research work. We also thank data collectors, supervisors, and administrators of health facilities for their valuable support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Kureshee NI, Dhande PP. Awareness of mothers and doctors about drug utilization pattern for illnesses encountered during pregnancy. J Clin Diagnostic Res. 2013;7(11):2470–2474. doi:10.7860/jcdr/2013/6329.3582
2. Dathe K, Schaefer C. The use of medication in pregnancy. Dtsch Arztebl Int. 2019;116(46):783–790. doi:10.3238/arztebl.2019.0783
3. Eftimova B, Lazarova B. Drug use at clinical hospital STIP-evaluation of rational/irrational / use. Knowl. 2018;22(5):1193–1195.
4. Bennadi D. Self-medication: a current challenge. J Basic Clin Pharm. 2014;5(1):19. doi:10.4103/0976-0105.128253
5. Janatolmakan M, Abdi A, Andayeshgar B, Soroush A, Khatony A. The reasons for self-medication from the perspective of Iranian nursing students: a qualitative study. Nurs Res Pract. 2022;2022:6–9. doi:10.1155/2022/2960768
6. Ansari M. Sociobehavioral Aspects of Medicines Use in Developing Countries. In: Social and Administrative Aspects of Pharmacy in Low-and Middle-Income Countries: Present Challenges and Future Solutions. Elsevier; 2018:15–33. doi:10.1016/B978-0-12-811228-1.00002-9
7. Suleman S, Woliyi A, Woldemichael K, et al. Pharmaceutical regulatory framework in Ethiopia: a critical evaluation of its legal basis and implementation. Ethiop J Health Sci. 2016;26(3):259–276. doi:10.4314/ejhs.v26i3.9
8. Yeika EV, Ingelbeen B, Kemah BL, Wirsiy FS, Fomengia JN, van der Sande MAB. Comparative assessment of the prevalence, practices and factors associated with self-medication with antibiotics in Africa. Trop Med Int Heal. 2021;26(8):862–881. doi:10.1111/tmi.13600
9. Gbagbo FY, Nkrumah J. Implications of self-medication in pregnancy for safe motherhood and sustainable development goal-3 in selected Ghanaian communities. Public Heal Pract. 2020;1:100017. doi:10.1016/j.puhip.2020.100017
10. Abasiubong F, Bassey EA, Udobang JA, Akinbami OS, Udoh SB, Idung AU. Self-medication: potential risks and hazards among pregnant women in Uyo, Nigeria. Pan Afr Med J. 2012;13:1–8.
11. Lupattelli A, Spigset O, Twigg MJ, et al. Medication use in pregnancy: a cross-sectional, multinational web-based study. BMJ Open. 2014;4:2. doi:10.1136/bmjopen-2013-004365
12. Navaro M, Vezzosi L, Santagati G, Angelillo IF. Knowledge, attitudes, and practice regarding medication use in pregnant women in Southern Italy. PLoS One. 2018;13(6):1–14. doi:10.1371/journal.pone.0198618
13. Baghianimoghadam MH, Mojahed S, Baghianimoghadam M, Yousefi N, Zolghadr R. Attitude and practice of pregnant women regarding self-medication in Yazd, Iran. Arch Iran Med. 2013;16(10):580–583.
14. Verstappen GM, Smolders EJ, Munster JM, Aarnoudse JG, Hak E. Prevalence and predictors of over-the-counter medication use among pregnant women: a cross-sectional study in the Netherlands. BMC Public Health. 2013;13:1. doi:10.1186/1471-2458-13-185
15. Sema FD, Addis DG, Melese EA, Nassa DD, Kifle ZD. Prevalence and associated factors of self-medication among pregnant women on antenatal care follow-up at university of Gondar comprehensive specialized hospital in Gondar, Northwest Ethiopia: a cross-sectional study. Int J Reprod Med. 2020;46(1):1–12. doi:10.1155/2020/2936862
16. Niriayo YL, Mohammed K, Asgedom AW, Demoz GT, Wahdey SGK. Self-medication practice and contributing factors among pregnant women. PLoS One. 2021;(5):1–10. doi:10.1371/journal.pone.0251725
17. Beyene KGM, Beza SW. Self-medication practice and associated factors among pregnant women in Addis Ababa, Ethiopia. Trop Med Health. 2018;46(1):1–14. doi:10.1186/s41182-018-0091-z
18. Ahmed SM, Sundby J, Aragaw YA, Abebe F. Self-medication and safety profile of medicines used among pregnant women in a tertiary teaching hospital in Jimma, Ethiopia: a cross-sectional study. Int J Environ Res Public Health. 2020;17:11. doi:10.3390/ijerph17113993
19. Wakjira GB, Boru BG, Labata BG. Prevalence of self-medication and its associated factors among pregnant women attending antenatal care at nekemte referral hospital, Oromia regional state. J Bioanal Biomed. 2019;11(1):160–165. doi:10.4172/1948-593X.1000228
20. Abeje G, Admasie C, Wasie B. Factors associated with self medication practice among pregnant mothers attending antenatal care at governmental health centers in Bahir Dar city administration, Northwest Ethiopia, a cross sectional study. Pan Afr Med J. 2015;20:276. doi:10.11604/pamj.2015.20.276.4243
21. Central Statstical Agency. The Federal Democratic Republic of Ethiopia, Central Statistical Agency: Key Findings on the 2012 Urban Unemployment Survey.
22. Central Statistical Agency. Ethiopian Welfare Monitoring Survey 2011:Summary Report. CSA; 2011.
23. Central Statstical Agency. Ethiopian Demographic and Health Survey, 2016; Final Report. CSA; 2016.
24. Ayalew MB. Self-medication practice in Ethiopia: a systematic review. Patient Prefer Adherence. 2017;11:401–413. doi:10.2147/PPA.S131496
25. Pakseresht S, Khalili Sherehjini A, Rezaei S. Self-medication and its related factors in pregnant women: a cross-sectional study. J Midwifery Reprod Heal. 2020;8(3):2359–2367. doi:10.22038/jmrh.2020.44982.1542
26. Gupta M, Dalai CK, Ahmed SN, Sarkar D, Ur RR, Nirala SK. Prevalence and risk factors of self-medication in pregnancy: a cross-sectional study from a tertiary care hospital in Eastern India. Asian J Med Sci. 2021;12(12):68–72. doi:10.3126/ajms.v12i12.39217
27. Zaboli P, Hashemi-Meshkini A, Varmaghani M, et al. Pharmaceutical laws and regulations in Iran: an overview. J Res Pharm Pract. 2016;5(3):155–161. doi:10.4103/2279-042x.185709
28. Yargawa J, Leonardi-bee J. Male involvement and maternal health outcomes: systematic review and meta-analysis. J Epidemiol Community Heal. 2015;69:604–612. doi:10.1136/jech-2014-204784
29. Rahman AE, Perkins J, Islam S, et al. Knowledge and involvement of husbands in maternal and newborn health in rural Bangladesh. BMC Pregnancy Childbirth. 2018;18(1):1–12. doi:10.1186/s12884-018-1882-2
30. Tokhi M, Comrie-Thomson L, Davis J, Portela A, Chersich M, Luchters S. Involving men to improve maternal and newborn health: a systematic review of the effectiveness of interventions. PLoS One. 2018;13(1):1–16. doi:10.1371/journal.pone.0191620
31. Mullany BC, Becker S, Hindin MJ. The impact of including husbands in antenatal health education services on maternal health practices in urban Nepal: results from a randomized controlled trial. Health Educ Res. 2007;22(2):166–176. doi:10.1093/her/cyl060
32. Laksono AD, Wulandari RD, Matahari R. Does a husband’s education matter in antenatal care visits involvement?: study on the poor in Indonesia. ResearchSquare. 2020;1–14. doi:10.21203/rs.3.rs-76095
33. Adjiwanou V, Bougma M, LeGrand T. The effect of partners’ education on women’s reproductive and maternal health in developing countries. Soc Sci Med. 2018;197:104–115. doi:10.1016/j.socscimed.2017.11.054
34. Jaiswal S, Shankar R, Jaiswal SK. Antenatal care awareness among rural pregnant women of Uttar Pradesh, India: a community-based study. Int J Reprod Contraception. 2022;11(7):1877. doi:10.18203/2320-1770.ijrcog20221662
35. Kebede AA, Taye BT, Wondie KY. Factors associated with comprehensive knowledge of antenatal care and attitude towards its uptake among women delivered at home in rural Sehala Seyemit district, northern Ethiopia: a community-based cross- sectional study. PLoS One. 2022;17(10):1–18. doi:10.1371/journal.pone.0276125
36. Bolanko A, Namo H, Minsamo K, Addisu N, Gebre M. Knowledge of obstetric danger signs and associated factors among pregnant women in Wolaita Sodo town, South Ethiopia: a community-based cross-sectional study. SAGE Open Med. 2021;9:205031212110011. doi:10.1177/20503121211001161
37. Singh DR, Harvey CM, Bohara P, et al. Factors associated with newborn care knowledge and practices in the upper Himalayas. PLoS One. 2019;14(9):1–18. doi:10.1371/journal.pone.0222582
38. Rosário EVN, Gomes MC, Brito M, Costa D. Determinants of maternal health care and birth outcome in the dande health and demographic surveillance system area, Angola. PLoS One. 2019;14(8):1–19. doi:10.1371/journal.pone.0221280
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.