Back to Journals » Patient Preference and Adherence » Volume 16
Self-Efficacy, Exercise Anticipation and Physical Activity in Elderly: Using Bayesian Networks to Elucidate Complex Relationships
Authors Chen X, Yang S, Zhao H, Li R, Luo W ![]() , Zhang X
, Zhang X
Received 4 April 2022
Accepted for publication 18 July 2022
Published 28 July 2022 Volume 2022:16 Pages 1819—1829
DOI https://doi.org/10.2147/PPA.S369380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Xiaoying Chen,1,* Shuang Yang,2,* Huiwen Zhao,3 Rui Li,1 Wen Luo,3 Xiuli Zhang3
1The 2nd Ward of Knee Trauma Department, Tianjin Hospital, Tianjin, People’s Republic of China; 2Traumatic Orthopedics Department, The 2nd Ward of Hip Joint Surgery, Tianjin Hospital, Tianjin, People’s Republic of China; 3The 2nd Ward of Joint Surgery, Tianjin Hospital, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wen Luo; Xiuli Zhang, The 2nd Ward of Joint Surgery, Tianjin Hospital, No. 406 Jiefangnan Road, Tianjin, 300211, People’s Republic of China, Tel +86 22-13116190054, Email [email protected]; [email protected]
Aim: To explore the correlation of exercise anticipation, self-efficacy and lower limb function in the elderly, and identify active predictors of exercise. The time up and go (TUG) has been used to access basic mobility skills, as well as strength, balance and agility, which is used in a range of population.
Methods: A cross-sectional survey approach was employed in this study, assessing the functional relationship of the level of exercise anticipation, modified gait efficacy scale (mGES), self-efficacy for exercise scale (SEE), perceived efficacy of patient–physician interactions (PEPPI-10), behavioral regulation in exercise questionnaire (BREQ), and the time up and go (TUG) and International Physical Activity Questionnaire (IPAQ). Consequently, we constructed the Bayesian network model utilizing Genie 2.3, in order to effectively determine clear negative and positive correlations.
Results: This investigation incorporated a total of 285 patients. The results of Spearman’s correlation analysis indicated that the TUG effectively correlated with age (r = 0.158, P < 0.01), drinking (r=− 0.362, P < 0.01), mGES (r=− 0.254, P < 0.01), PEPPI (r=− 0.329, P < 0.01), SEE (r =− 0.408, P < 0.01), BREQ (r = 0.676, P < 0.01), EA (r =− 0.688, P < 0.01) and IPAQ (r =− 0.742, P < 0.01). TUG can be used as the direct influencing factor of IPA, and five nodes in the model can be considered the primary indirect influencing factors of TUG, such as drinking, EA, age, sex and mGES in Bayesian network. The sensitivity analysis of the model confirmed that TUG (0.059), drinking (0.087), EA (0.335), age (0.080), sex (0.164), mGES (0.028) and hypertension (0.030) can become the sensitivity evaluation indicators of IPAQ in the elderly community population, in which the area under the ROC curve (AUC) was 59.6% (2207/3705), indicating a suitable prediction performance.
Conclusion: Exercise anticipation and life behavior habit can effectively predict physical activity capability in the elderly. These findings can help clinicians establish effective intervention to improve the physical activity regularly of the elderly.
Keywords: self-efficacy, physical activity, exercise anticipation, elderly
Background
The proportion of people over the age of 60 is increasing at an accelerated pace when compared to any other age group, according to the World Health Organization (WHO).1 In the US, individuals aged 65 and up will have exponential growth, estimating from 43 million to 92 million in 2060.2 Given these considerable numbers, the frequency of geriatric diseases (for example, knee osteoarthritis) is also raised accordingly.3 Despite the good health benefits of exercise, many surveys have found that over 60% of elderly do not take part in regular exercise, and only about 25% of them report regular participation in exercise.4,5
Self-efficacy relates to one’s confidence in one’s own ability to effectively execute a suitable course of action required to manage various circumstances.6 To a large extent, people frequently suffer from physical disabilities or impairments, and die prematurely as a result of avoidable health-impairing behaviors.7 Self-efficacy plays a role in the maintenance of participating exercise programme, as well as in the early stages.8 Higher self-efficacy expectations could help people maintain energy during exercise or physical activity, expand less effort during exercise or physical activity, and report more positive effects during or after physical activity and feel more relaxed.9,10 Meanwhile, the study found that effective patient–physician interaction has been confirmed to be associated with a broad range of improved outcomes of intervention, for example, functional status.11
The theory of planned behavior (TPB) is a social cognitive concept, which explains the intentional behavior.12 According to TPB, behavioral intention is the most initial aspect of individual behavior, which is influenced by attitude, behavioral control and so on. The study found that taking part in exercise or physical activity was mostly influenced by attitude among men and subjective norm among women through the application of TPB. “Not motivated to perform exercise” was a specific factor, which affected attitude toward exercise in male; meanwhile, friends and family were the important support to participate in exercise for females.13 Some elderly have the perception that exercise was not suitable for them and the physical activity that they were doing was enough.14 The misconception toward physical activity leads them to various health problems.15
With the low level of exercise in the elderly, how to promote and maintain a reasonable level of exercise or physical activity in them, has become a primary research content of psychology, behavior, medicine, and other disciplines. These theories examine and consider aspects of exercise according to different perspectives and hypotheses. Thus, this study focuses on these two key theories to explain exercise: planned behavior theory and self-efficacy theory.
Walking is the most important way of human movement. It penetrates into daily life and sports and is needed on various occasions. Walking ability is one of the important criteria to evaluate the exercise ability of the elderly. Gait analysis is used to record, measure and explain the biomechanical process of walking. It is known as the “gold standard” for clinical evaluation of lower limb function. The time up and go (TUG) assessed basic mobility skill, as well as strength, balance and agility.16 The TUG is used in a range of populations and many conditions, for example, osteoarthritis, joint replacement, rheumatoid arthritis, and so on.17 Exercise anticipation involves not only the perceptual process of current information but also the integration of cultural background and current information, which is more complex than exercise perception. And the study showed that exercise anticipation is closely related to decision-making and judgment in sports.18
In China, the study of planned behavior theory and self-efficacy theory on exercise in the elderly is at its infancy and the Bayesian network research of rehabilitation nursing is small. To date, the exercise effects of the planned behavior theory and the self-efficacy theory have been sufficiently confirmed in teenagers.19 Accordingly, this study aims to explain and elucidate the complex relationship of self-efficacy, exercise motivation, and walking ability in the elderly, and identify influence predictors of physical activity.
Method
Design
This study is an observational research, which uses the cross-sectional survey to validate the correlation of exercise anticipation, self-efficacy and lower limb function in the elderly.
Participants
The participants in this study are the elderly, who have been fit with the inclusion criteria from five different communities. We had used the convenient sampling method.
Inclusion criteria: (1) display adequate comprehension and consciousness; (2) over 65 years; and (3) have a decent living capability as measured by the Barthel Index20 (BI) >60; and provide (4) written informed consent.
Exclusion criteria include (1) suffering from a nervous system disorder, like Alzheimer’s disease, which interferes with cognitive capacity; and (2) exhibiting symptoms like aphasia and deafness whereby the participant is unable to communicate with others.
Sample Size
The sample size of this survey is obtained by statistical formula:21

N = evaluation of the sample
P = Percentage of subjects with good exercise behavior
Q = Percentage of subjects with poor exercise behavior
Regardless of the value of P and Q, the maximum PQ should be equal to (0.5)(0.5).
Z = Value corresponding to 90% confidence interval under normal distribution curve (1.64)
d = The difference between the mean value of the accuracy sample measurement result and the actual population mean value is set as 5%
N=[(1.64)(1.64)(0.5)(0.5)]/[(0.05)(0.05)]=268.96
The sample size of this survey is 300. Considering the impact of the recovery rate, the questionnaires have been issued to ensure sufficient sample size, and the estimated recovery rate has 90%.
The Hospital Research Ethics Committee approved this study, with individuals signing consent forms with respect to their active participation. Individuals were informed about the purpose of the investigation, their rights, and the duties of the researchers before the start of this study. In order to explain the points for filling in the questionnaires, the researchers utilized standard, common advising language. Participants completed all of the surveys. Throughout the study, the individuals’ privacy was respected.
A survey was given at random to a sample of nearly 300 elderly at the community Health Center between April and July of 2021. We chose persons from the database at random.
The Tianjin Hospital Medical Ethics Committee approved this research in accordance with Chinese laws and regulations on human medical research (TJYY-2020-YLS-086).
In this study, a self-administered questionnaire was employed. Before this, the investigators explained the survey’s aim, as well as the respondents’ rights and duties, and acquired their agreement. Personal privacy was safeguarded throughout the survey, and all scales were gathered within 30 minutes. In the process of collection, the participants filled out the questionnaire independently firstly, who have been tested the expected ability of sports by computers secondly, who finally performed the time up and go test (TUG).
Assessment
Behavioral Regulation in Exercise Questionnaire (BREQ)
This questionnaire has been designed by Markland according to the planned behavior theory.22 The previous study confirmed that the Chinese version of Behavioral Regulation In Exercise Questionnaire (C-BREQ) has good internal consistency.23 The questionnaire includes 5 dimensions: non-motivation, external adjustment, internal adjustment, identity adjustment, and internal motivation. The Confirmatory factor analysis (CFA) of the C-BREQ showed that, χ2=446.283, df = 124, χ2/df=3.599, RMSEA = 0.048, CFI = 0.949 NFI = 0.930, IFI = 0.949, GFI = 0.956, which meets the model fitting standard, and thereby supporting the reliable validity of the questionnaire structure.24 Participants were asked questions relating to what they planned and motivated of exercise were measured on a five-point Likert-type scale ranging from 0 (not true for me) to 4 (very true for me).
Modified Gait Efficacy Scale (mGES)
The English version of Newell’s modified gait efficacy scale, as stated, comprises of ten indicators measuring a participant’s self-efficacy of walking safely in a range of different settings.25 These assessments are administered in various environments, and include simulated conditions such as stepping over an obstacle, walking along the roadside or stairs, and walking long-distances. Respondents chose a score in answer to the prompt “How confident are you that you would be able to safely …”. This scale used an 11-point Likert scale grading method, ranging from 0 to 100, with 100 being the highest level of gait self-efficacy. The Chinese version mGES has sufficient internal consistency, with a Cronbach’s coefficient of 0.928.26
Self-Efficacy for Exercise Scale (SEE)
The English version of self-efficacy for exercise scale (SEE) was used largely to assess exercise self-efficacy in the elderly.27 The Cronbach’s coefficient of the English version was 0.92, indicating good internal consistency. The 10-point Likert scale grading method was employed for this scale, with a high score suggesting more self-efficacy on exercise. Cronbach’s alpha for the Chinese version is 0.75, which can be used in clinical studies.28
Perceived Efficacy of Patient–Physician Interactions (PEPPI-10)
Scientists developed PEPPI-10 to examine participants’ self-efficacy in accessing medical treatment and information from a doctor or physician.29 PEPPI-10 has Cronbach’s coefficients of 0.91, demonstrating a strong theoretical foundation and sufficient clinical practicality. The Chinese version PEPPI showed high validity and reliability (Cronbach’s coefficient 0.907) in elderly. The Chinese version PEPPI is comprised of ten items.30 Each was graded on an 11-point Likert scale, with 0 represent “not at all confident” and 10 represent “extremely confident.” The score range of the Chinese version PEPPI was from 0 to 100, 100 is the highest score, indicating that the individual is the best confident on patient–physician interactions.
Time Up and Go Test (TUG)
Patients were asked to perform a time up and go test (TUG), which required rising from an armless chair (45 cm high), walking three meters, turning at a cone placement, returning to their seat, and resuming their seated position. They were advised to walk at a steady pace without using shoes or walking aids. When patients’ buttocks were lifted off the chair to stand, time was measured, and later stopped when their buttocks met the seat upon returning to a seated posture. After three repetitions, the average readings were used in the study. In older individuals, the TUG test is very reliable.31 This study set two Timed Up and Go test thresholds (10 and 15 s) according to previously published evidence.32,33
Exercise Anticipation (EA)
This experiment’s video material included action clips (MP4) from several athletic sports videos. There were 20-second breaks between each task, which comprised 20 cycles. (1) Judging the badminton drop point in the video, the video’s freeze-frame corresponded with the moment the upper player’s racket hits the ball. The subjects were asked to judge the landing point of badminton in the left and right half as quickly and accurately as possible. (2) Judging the penalty goal in a football match in the video: the video’s freeze-frame timing was according to the instant the player’s foot struck the ball. (3) Judging the high jumper cross the bar: the freeze-frame time of the video was the moment when the player’s hip was over the crossbar. The exam card was filled out according to the directions, and each activity underwent a three-second assessment. The blanks on the exam card were filled out with the relevant number, and each activity was judged for up to three seconds. The evaluation index for this task is the accuracy rate. The accuracy rate was higher, which represented that the participants had better exercise expectation ability.
International Physical Activity Questionnaire (IPAQ)
This is a commonly used measurement tool, which can provide researchers and practitioners with an estimate of physical activity and sedentary behaviour in different populations, across a range of socio-economic settings.34 The IPAQ (long-form) consists of 27 questions, which reflect on the previous 7 days’ activities according to domain: 1) occupational physical activity; 2) transportation physical activity; 3) housework, house maintenance and caring for family; 4) recreation, sport and leisure-time physical activity; and 5) time spent sitting.35 Evaluation criteria: 1) Low: minimum physical activity level; 2) Medium: any of the following three criteria: ①more than 3 days, vigorous activity for at least 20 minutes/day, ②at least 30 minutes/day of moderate intensity activities or walking for more than 5 days, ③any combination of walking for 5 days or more, moderate intensity or intense intensity activities to achieve 600 minutes/week; 3) High: any of the following 2 criteria:①vigorous activity for at least 3 days, accumulating at least 1500 minutes/week,②any combination of walking, at least 3000 minutes/week of moderate or severe intensity.36
Statistical Analysis
Pearson’s correlation was utilized to determine the relationship and consistency among certain elements in the exercise anticipation assessments implementing different scales and scores.37 Sunce the IPAQ used the ranking score, we cannot measure the normal distribution. And the results of TUG are the objective indicators in this research, so we selected the TUG as the target parameters in the correlation analysis of this study. Pearson’s correlation analysis was utilized if the TUG had a normal distribution; else, Spearman correlation analysis was employed. A P-value of <0.05 denotes statistical significance. In this investigation, we performed a two-tailed test to see if these characteristics were correlated.38 The correlation coefficient was calculated using the following values: weak correlation (0.20–0.39), moderate correlation (0.40–0.59), strong correlation (0.60–0.79), and very strong correlation (0.80–1.0).37,39
In this study, we constructed a Bayesian network model with TUG as the goal. In the original data, we performed data cleaning and conversion. Table 1 shows the key scores and assignments from the study. Genie 2.3 (developed by the University of Pittsburgh’s Decision Systems Laboratory) was shown to be the most effective tool for completing Bayesian network parameter learning through the maximum expected value approach in this investigation.40,41 In addition, the network parameters are iterated on a regular basis utilizing the accident data, and the circumstances for computation termination are as follows: (1) posterior probability variance for a single risk factor is less than 1%; (2) the overall variance in posterior probability across the whole network is less than 15%.
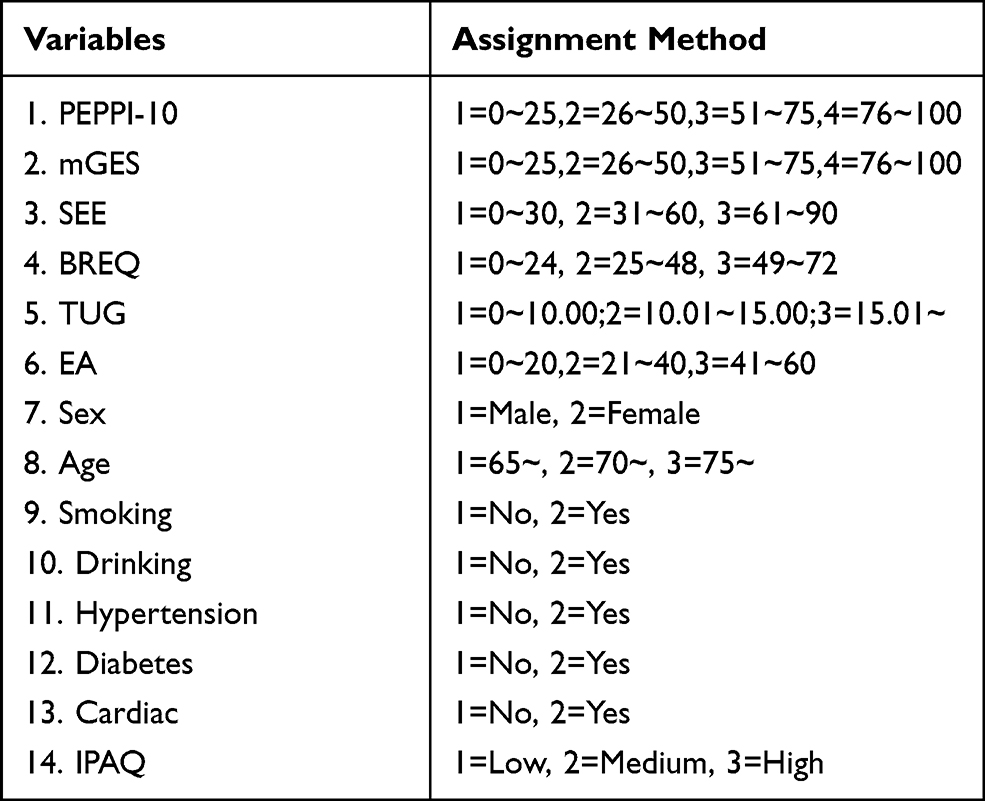 |
Table 1 The Main Variables and Assignments |
Results
Participants
Of the 296 participants recruited, eleven patients were excluded because of missing responses, leaving 285 for analysis. The clinical and demographic characteristics of the enrolled patients have been shown in Table 1. The kurtosis of TUG was −0.456 and the skewness was −0.318, which has not shown the normal distribution (Figure 1). Since the TUG was the target parameter in correlation analysis, we selected the Spearman's correlation analysis (rs) in this research.
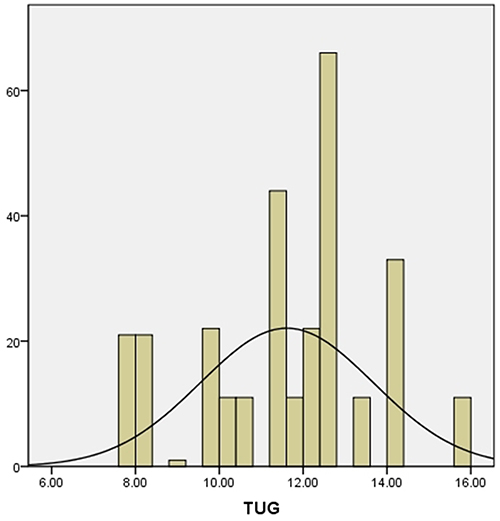 |
Figure 1 Participants’ TUG distribution. |
Correlation Analysis
The results of Spearman's correlation analysis indicated that the TUG effectively correlated with age, drinking, BREQ, mGES, SEE, PEPPI, EA and IPAQ. The results show that the TUG had weak but significant correlation with age (r = 0.158, P < 0.01), drinking (r=−0.362, P < 0.01), mGES (r=−0.254, P < 0.01) and PEPPI (r=−0.329, P < 0.01); which had moderate but significant correlation with SEE (r =−0.408, P < 0.01). What is more, that had strong and significant correlation with BREQ (r = 0.676, P < 0.01), EA (r =−0.688, P < 0.01) and IPAQ (r =−0.742, P < 0.01). Meanwhile, the results found that the TUG has no correlation with sex (r =−0.073, P > 0.05), smoking (r=−0.027, P > 0.05), hypertension (r=−0.007, P > 0.05), diabetes (r=−0.059, P>0.05), and cardiac (r =−0.019, P > 0.05) (Table 2).
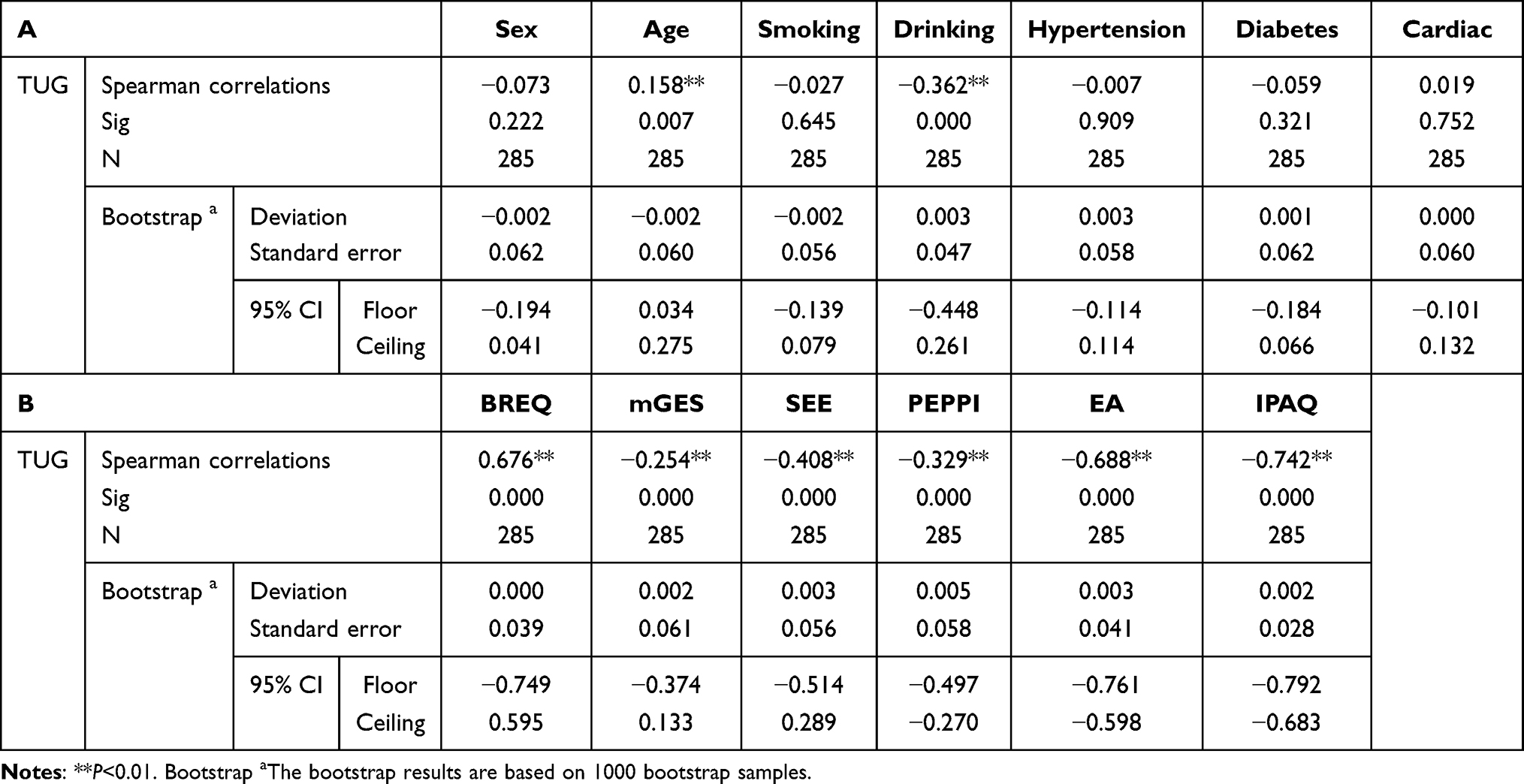 |
Table 2 Spearman Correlations Between TUG and Other Variables |
Bayesian Causal Reasoning
The learning difficulty of network topology increases with a higher number of nodes. The Bayesian model used in this study involves 14 nodes and is reported as follows: sex, age, smoking, drinking, hypertension, diabetes, cardiac, BREQ, mGES, SEE, PEPPI, TUG, EA, IPAQ.
The learning outcomes of Bayesian Causal Reasoning have been depicted in Figure 2, which clearly shows the entire state of parameter and structural learning of the IPAQ prediction model for the elderly on physical activity and exercise in the community. In Figure 2 we can see that the TUG which can be used as the most direct influencing factor of IPAQ in complex relationships. Five nodes in the model can be considered the primary indirect influencing factors of TUG, respectively, drinking, EA, age, sex and mGES.
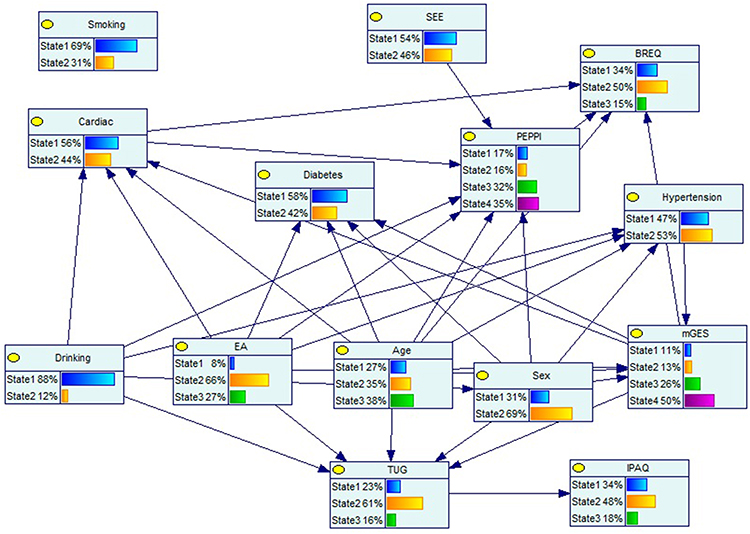 |
Figure 2 The Bayesian networks of IPAQ. |
Subsequently, we conducted a sensitivity analysis on the model of learning outcomes. The results indicated that the seven parent nodes can become the sensitivity evaluation indicators of the IPAQ in the elderly community population, and which followed TUG (0.059), drinking (0.087), EA (0.335), age (0.080), sex (0.164), mGES (0.028) and hypertension (0.030). In this study, we established the Bayesian Network Model of IPAQ in the elderly community population, which has been confirmed that the area under the ROC curve (AUC) was 59.6% (2207/3705), indicating a suitable prediction performance (Figure 3).
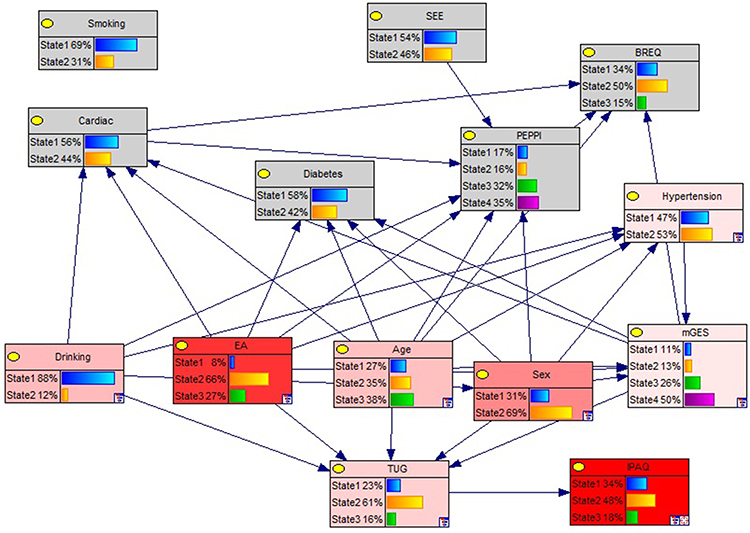 |
Figure 3 The sensitivity analysis of the Bayesian networks. |
Bayesian Predictive Reasoning
A Bayesian network can perform predictive reasoning, which is the act of determining the cause when the outcome state is known. The IPAQ is initially denoted as the state 1 according to the contents of Figure 4A, which indicates that the probability distribution of its affecting variables has altered. Compared with Figure 2, the EA value increases significantly, and the state 2 increased from 66% to 76%; the gender distribution has significantly changed, which the female population declined to 60%. And the BREQ distribution changed slightly, and the state 2 decreased to 46%.
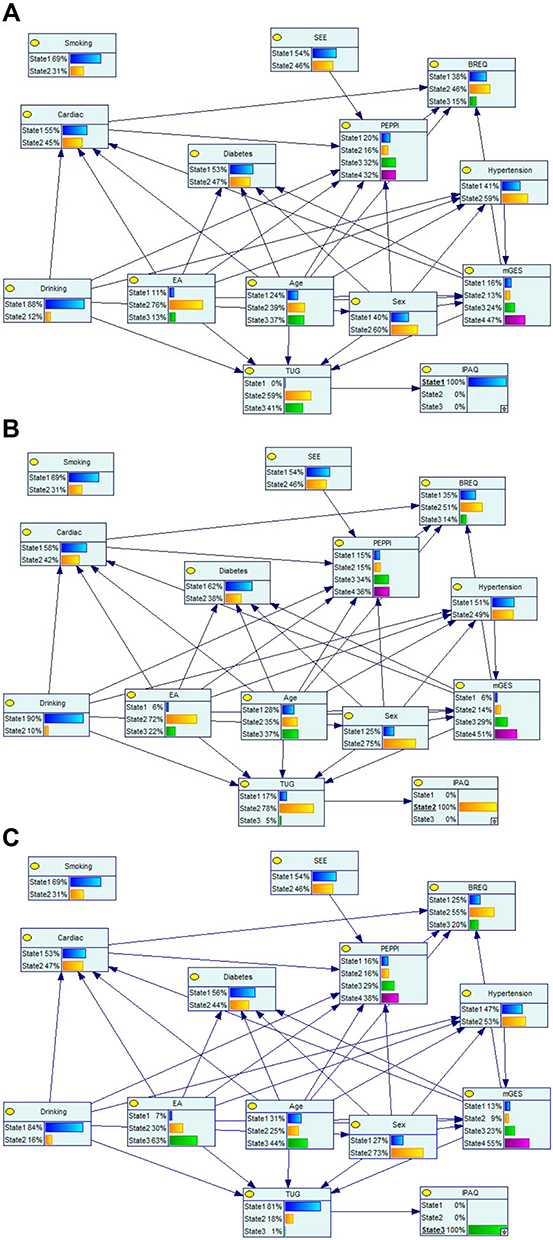 |
Figure 4 (A) The Bayesian Predictive Reasoning of IPAQ (B) the Bayesian Predictive Reasoning of IPAQ (C) the Bayesian Predictive Reasoning of IPAQ. |
According to the contents of Figure 4B, the IPAQ was initially state 2, and the probability distribution of influencing factors changes. Compared with Figure 2, the TUG changes significantly, the state 2 increases from 61% to 78%; the EA changes significantly; the state 2 increased from 66% to 72%; the gender distribution also changes significantly; and the female population increased from 69% to 75%.
According to Figure 4C: Initially, the IPAQ is state 3, and the probability distribution of the influencing factors also changed. When compared to Figure 2, the TUG changed significantly, where the state 1 increased from 23% to 81%; the EA changed significantly, where the state 3 increased from 27% to 63%; and the BREQ also changed significantly, where the state 2 increased from 50% to 55%; at the same time, the state 4 of the mGES also increased from 50% to 55%.
Discussion
The present study provided preliminary evidence for the active predictors and influences of physical activity and exercise in the elderly. The participants in this study were community-based, from three areas of Tianjin. The diversity of the participants contributes to the generalisability of the results and the findings can be used to strengthen the guideline of physical activity and exercise among the elderly for future use. In this study, the results showed that there is a strong correlation between TUG and IPAQ in elderly, which confirmed the previous hypothesis that TUG is a useful clinical index for understanding the motor characteristics of older adults.42
In the present study, we found that the TUG is also the most direct influencing factor of the IPAQ Bayesian network in elderly. Meanwhile, the results showed that drinking, EA, age, sex and mGES could influence the IPAQ indirectly. This study further confirmed that the attitude and self-efficacy of physical activity in the elderly can affect personal behaviour, in addition to demographic factors, such as age and gender. A general misconception of modern culture accepts that the old age is a time for relaxation and that physical activity and exercise are unnecessary.43 A study conducted among Iranians found that the majority of the Iranian elderly did not take part in exercise because of lazy attitude. Using Bayesian converse reasoning, we found the changing trends of TUG and EA were consistent with IPAQ in Figure 4A–C, especially when the state is at a high level. This result further illustrated the TUG and EA are the important predictors of the physical activity in the elderly.
Finally, this study confirmed that exercise anticipation is the most forecast sensitive index of the IPAQ in Bayesian network. This result showed that the ability to integrate and judge exercise information can strongly affect the level of exercise and physical activity. So improving the ability of exercise anticipation is an important method in cultivating good physical activity habits. Hence, this preliminary research would benefit from further investigation.
There are several limitations to this study. First, since the total sample size of study participants is small, we could not conduct more in-depth analyses, such as constructing a parameter model. Second, a scarcity of research funding meant that we were not able to complete the entire Bayesian inference. Aside from the limitations mentioned above, this study’s findings were highly supportive of the strong correlation between walking capacity and exercise in the elderly. Improving exercise anticipation and developing physical activity habits are effective strategies for successful aging.
Conclusion
This study demonstrated that the exercise anticipation and physical activity habits have a close relationship in the elderly. Exercise anticipation and life behavior habit can effectively predict physical activity capability in the elderly. These findings can help clinicians establish effective intervention to improve the physical activity regularly of the elderly.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available because the Ethical Guidelines for Epidemiological Research by the Chinese Government and prohibit researchers from providing their research data to other third-party individuals.
Ethics Approval and Consent to Participant
The current study was approved by the Institutional Ethical Review Board of Tianjin Hospital (No. TJYY-2020-YLS-086) and has been conducted in accordance with the Ethical Guidelines for Epidemiological Research by the Chinese Government and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All study participants provided written informed consent by the completion and submission of the survey.
Funding
This study was supported by the Tianjin Health Commission (THC) Grant-in-Aid for Science and Technology Project (No: ZC20220; PI: Miss Xili Zhang).
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. World Health Organization. The Charter of the World Health Organization [EB/OL]; 1946. Available from: https://www.who.int/about/who-we-are/constitution.
2. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100(2):126–131.
3. Murrell KFH, Entwisle DG. Age differences in movement pattern. Nature. 1960;185(4717):948–949. doi:10.1038/185948a0
4. Hawkins SA, Cockburn MG, Hamilton AS, et al. An estimate of physical activity prevalence in a large population-based cohort. Med Sci Sports Exerc. 2004;36(2):253–260. doi:10.1249/01.MSS.0000113485.06374.0E
5. Health Education Authority UK. Physical Activity in Later Life. London: Health Education Authority; 1999:96.
6. Bandura A. Self-Efficacy: The Exercise of Control. New York: W.H. Freeman; 1997.
7. Scherer Y, Bruce S. Knowledge, attitudes, and self-efficacy and compliance with medical regimen, number of emergency department visits, and hospitalizations in adults with asthma. Heart Lung. 2001;30(4):250–257. doi:10.1067/mhl.2001.116013
8. Aittasalo M, Miilunpalo S, Stahl T, et al. From innovation to practice: initiation, implementation and evaluation of a physician-based physical activity promotion programme in Finland. Health Promot Int. 2007;22(1):19–27. doi:10.1093/heapro/dal040
9. Bozoian S, Rejeski WJ, McAuley E. Self-efficacy influences feeling states associated with acute exercise. J Sport Exerc Psychol. 1994;16(3):326–333. doi:10.1123/jsep.16.3.326
10. Stutts WC. Physical activity determinants in adults. Perceived benefits, barriers and self-efficacy. AAOHN J. 2002;50(11):499–507.
11. Emanuel EJ, Dubler NN. Preserving the physician-patient relationship in the era of managed care. JAMA. 1995;273:323–329.
12. Ajzen I, Fishbein M. Understanding Attitudes and Predicting Social Behavior. Englewood Cliffs, NJ: Prentice-Hall; 1980.
13. Mohamad HA, Suzana S, Nur IM, et al. Applying theory of planned behavior to predict exercise maintenance in sarcopenic elderly. Clin Interv Aging. 2014;9:1551–1561. doi:10.2147/CIA.S60462
14. Grove NC, Spier BE. Motivating the well elderly to exercise. J Community Health Nurs. 1999;16(3):179–189. doi:10.1207/S15327655JCHN1603_4
15. Waters DL, Baumgartner RN, Garry PJ, et al. Advantages of dietary, exercise-related, and therapeutic interventions to prevent and treat sarcopenia in adult patients: an update. Clin Interv Aging. 2010;5:259–270. doi:10.2147/CIA.S6920
16. Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the “get-up and go” test. Arch Phys Med Rehabil. 1986;67(6):387–389.
17. Podsiadlo D, Richardson S. The timed “Up& Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi:10.1111/j.1532-5415.1991.tb01616.x
18. Norlin T, Tranaeus Fitzgerald U, Alricsson M. Barriers to and possibilities of returning to play after a severe soccer injury: a qualitative study. Eur J Physiother. 2016;18:179–184. doi:10.3109/21679169.2016.1174296
19. Wang L, Zhang Y. An extended version of the theory of planned behaviour: the role of self-efficacy and past behaviour in predicting the physical activity of Chinese adolescents. J Sports Sci. 2016;34(7):587–597. doi:10.1080/02640414.2015.1064149
20. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61–65.
21. Daniel WW. Biostatistic.
22. Markland D, Tobin V. A modification to the behavioural regulation in exercise questionnaire to include an assessment of amotivation. J Sport Exerc Psychol. 2004;26(2):191–196. doi:10.1123/jsep.26.2.191
23. Liu JD, Chung PK, Zhang CQ, et al. Chinese-translated behavioral regulation in exercise questionnaire-2: evidence from university students in the Mainland and Hong Kong of China. J Sport Health Sci. 2015;4(3):228–234. doi:10.1016/j.jshs.2014.03.017
24. Xiang MQ. The path of promotion on teenagers’ physical exercise and health-related well-being: based on self-determination theory model. Sport Sci. 2013;33(8):21–28.
25. Newell AM, Van Swearingen JM, Hile E, et al. The modified gait efficacy scale: establishing the psychometric properties in older adults. Phys Ther. 2012;92(2):318–328. doi:10.2522/ptj.20110053
26. An X, Zhang XL, Liu Y, et al. Validation of the Chinese version of the modified Gait Efficacy scale for patients removing Ilizarov external fixation device for over one year. Patient Perfer Adher. 2020;14:1307–1315.
27. Resnick B, Palmer MH, Jenkins LS, et al. Path analysis of efficacy expectations and exercise behavior in older adults. J Adv Nurs. 2000;31(6):1309–1315. doi:10.1046/j.1365-2648.2000.01463.x
28. Lee LL, Perng SJ, Ho CC, et al. A preliminary reliability and validity study of the Chinese version of the self-efficacy for exercise scale for older adults. Int J Nurs Stud. 2009;46(2):230–238. doi:10.1016/j.ijnurstu.2008.09.003
29. Maly RC, Frank JC, Marsball GN, et al. Perceived efficacy in patient-physician interactions (PEPPI): validation of an instrument in older persons. J Am Geriatr Soc. 1998;46(7):889–894. doi:10.1111/j.1532-5415.1998.tb02725.x
30. Zhao HW, Luo W, Maly RC, et al. Validation of the Chinese version 10-item perceived efficacy in patient–physician interactions scale in patients with osteoarthritis. Patient Prefer Adher. 2016;67:2189–2195. doi:10.2147/PPA.S110883
31. Lee SH, Han JH, Jin YY, et al. Poor physical fitness is independently associated with mild cognitive impairment in elderly Koreans. Biol Sport. 2016;33(1):57–62. doi:10.5604/20831862.1185889
32. Son KY, Shin DW, Lee JE, et al. Association of timed up and go test outcomes with future incidence of cardiovascular disease and mortality in adults aged 66 years: Korean national representative longitudinal study over 5.7 years. BMC Geriatr. 2020;20(1):111. doi:10.1186/s12877-020-01509-8
33. Viccaro LJ, Perera S, Studenski SA. Is timed up and go better than gait speed in predicting health, function, and falls in older adults? J Am Geriatr Soc. 2011;59(5):887–892. doi:10.1111/j.1532-5415.2011.03336.x
34. Cerin E, Barnett A, Cheung MC, et al. Reliability and validity of the IPAQ-L in a sample of Hong Kong urban older adults: does neighborhood of residence matter? J Aging Phys Act. 2012;20(4):402–420. doi:10.1123/japa.20.4.402
35. IPAQ. Guidelines for data processing and analysis of the International Physical Activity Questionnaire (IPAQ) [Online] The International Physical Activity Questionnaire; 2005.
36. Hagstromer M, Oja P, Sjostrom M. The international physical activity questionnaire (IPAQ): a study of concurrent and construct validity. Public Health Nutr. 2006;9(6):755–762. doi:10.1079/PHN2005898
37. Browne MW, Cudeck R. Alternative Ways of Assessing Model Fit: Testing Structural Equation Models. Newbury Park: Sage Publications; 1993:136–162.
38. Terwee CB, Bot SD, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34–42. doi:10.1016/j.jclinepi.2006.03.012
39. Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the global burden of disease study. Lancet. 2013;380(9859):2224–2260. doi:10.1016/S0140-6736(12)61766-8
40. Eggers KM, Ellenius J, Dellborg M, et al. Artificial neural network algorithms for early diagnosis of acute myocardial infarction and prediction of infarct size in chest pain patients. Int J Cardiol. 2007;114(3):366–374. doi:10.1016/j.ijcard.2005.12.019
41. Kurosawa C, Shimadu N, Yamamoto S. Where do healthy older adults take more time during the timed up and go test? J Phys Ther Sci. 2020;32(10):663–668. doi:10.1589/jpts.32.663
42. Buttery AK, Martin FC. Knowledge, attitudes and intentions about participation in physical activity of older post-acute hospital inpatients. Physiotherapy. 2009;95(3):192–198. doi:10.1016/j.physio.2009.03.002
43. Mortazavi SS, Mohammad K, Ardebili HE, et al. Mental disorder prevention and physical activity in Iranian elderly. Int J Prev Med. 2012;3(Suppl 1):S64–S72.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Impact of Smartphone Addiction on Chinese University Students’ Physical Activity: Exploring the Role of Motivation and Self-Efficacy
Lin B, Teo EW, Yan T
Psychology Research and Behavior Management 2022, 15:2273-2290
Published Date: 23 August 2022
Delay Discounting and BMI in Hypertensives: Serial Mediations of Self-Efficacy, Physical Activity and Sedentary Behavior
Wang Y, Hu Z, Ding Y, Sun Y, Meng R, He Y
Journal of Multidisciplinary Healthcare 2024, 17:4319-4334
Published Date: 4 September 2024
Physical Activity Self-Efficacy Among Pregnant Women at High Risk for Gestational Diabetes Mellitus in China: A Cross-Sectional Study
Yang X, Song Y, Zhang J, Wang Y, Huang H, Zhang J, Gao L
Journal of Multidisciplinary Healthcare 2024, 17:5725-5736
Published Date: 3 December 2024
Current Status and Determinants of Fatigue in Chinese Older Adults Receiving Maintenance Hemodialysis: A Multicentre Cross-Sectional Study
Zhang N, Jiang P, Fan S, Wang W, Liu F
Clinical Interventions in Aging 2025, 20:1847-1860
Published Date: 4 November 2025
Physical Activity and Its Predictors Among Women of Advanced Maternal Age in the First Trimester: A Cross-Sectional Study
Zeng L, Han R, Chen X, Zeng D, Yuan H, Meng L, Gao L
International Journal of Women's Health 2026, 18:574662
Published Date: 6 February 2026