Back to Journals » Risk Management and Healthcare Policy » Volume 15
Self-Care Mobile Application for South Korean Pregnant Women at Work: Development and Usability Study
Authors Lee Y ![]() , Choi S, Jung H
, Choi S, Jung H
Received 28 January 2022
Accepted for publication 21 April 2022
Published 11 May 2022 Volume 2022:15 Pages 997—1009
DOI https://doi.org/10.2147/RMHP.S360407
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Yaelim Lee,1,2 Soeun Choi,3 Heejae Jung4
1College of Nursing, Catholic University of Korea, Seoul, Republic of Korea; 2Redcross College of Nursing, Chung-Ang University, Seoul, Republic of Korea; 3Department of Nursing, Yeouido St. Mary’s Hospital, Seoul, Republic of Korea; 4Department of Nursing, Seoul National University Hospital, Seoul, Republic of Korea
Correspondence: Yaelim Lee, Department of Nursing, College of Nursing, The Catholic University of Korea, 222, Banpo-daero, Seocho-gu, Seoul, 06591, Republic of Korea, Tel +82-2-2258-8148, Fax +82-2-2258-8148, Email [email protected]
Background: Pregnant women at work often encounter barriers to participating in prenatal education or conducting appropriate self-care practices due to their working conditions.
Purpose: We aimed at developing a mobile-based intervention application (SPWW) for Korean pregnant women at work and testing its usability and preliminary effects to enhance their self-care practices.
Patients and Methods: The application was developed and tested with thirty-one pregnant women at work and thirteen women’s healthcare providers. The instruments used in this study were a modified Health Practices in Pregnancy Questionnaire II and a System Usability Scale. Descriptive analyses and t-tests were performed using SPSS 25.0. The participants’ open-ended answers were analyzed using ATLAS. ti 8.
Results: We developed the application focusing on four self-care topics: healthy diet, physical activity, sufficient rest, and stress management. After using the application for two weeks, participants’ levels of exercise (p = 0.006), adequate fluid intake (p = 0.002), and limiting daily caffeine intake (p = 0.048) significantly improved. In addition to good usability scores, the suggestions for improvement made by the participants included diversifying the educational materials and adding individually customizable functions to the application.
Conclusion: The application developed in this study enhanced self-care practices of pregnant women at work and showed adequate levels of usability. We expect the developmental process and details of the application provided in this study to serve as a sample guide for future studies.
Keywords: pregnancy, prenatal care, telemedicine, internet-based intervention, Asian
Introduction
Pregnancy and delivery is one of the most important experiences in women’s lives, as well as an opportunity for screening their health and reinforcing healthy behaviors.1 As pregnant women go through various physical, psychological, and social changes, their need for information and seeking behavior often increase.2 While learning about healthy pregnancy, pregnant women learn that their health practices directly affect fetal health and pregnancy results.3
Prenatal care and education are essential parts of care for maintaining maternal and fetal health during pregnancy.4 This provides an opportunity to monitor their health and deliver essential education to pregnant women and their families.4 Pregnant women who acquire adequate knowledge and coping methods have been shown to improve health practices, become confident in maternal roles, and enhance their maternal-child attachment.5 Moreover, prenatal education lowers the physical, mental, and social risks during pregnancy, helps to build healthy relationships with family and community, and reduces perinatal mortality and morbidity.6
Prenatal education in South Korea is often provided by medical centers and private agencies (eg, pharmaceutical or baby product companies).7 Many of the women, especially pregnant women at work (PWW), cannot attend to these on-site sessions due to place and time restrictions.8,9 They often rely on pregnancy-related books, acquaintances, and the internet.10 Some of this wealth of information is helpful; however, some sources offer incorrect or low-evidence information leading to concerns about what is transmitted. Considering that the working pregnant women accounted for 44.0% of total pregnant women in 2020,11 many women in South Korea may have limited access to on-site prenatal education. Several studies on Korean pregnant women have described increased adverse pregnancy outcomes in working pregnant women and have suggested that additional support is needed for these women.12,13
To address limitations of traditional prenatal education, more acceptable educational media are emerging.11 With an increase in smartphone supply, health education utilizing smartphones is increasing in the medical field.14,15 Smartphone-based education has advantages, including no temporal and spatial constraints, easy access, and convenience.16 In South Korea, the rate of smartphone usage was 94% in 2018.17 The smartphone ownership was the highest among younger adults (ie between the age of 18 and 36) compared to other age groups.17 Considering the average first-child birth age is 31.4 years in South Korea,18 the use of smartphones for prenatal education is feasible. Previous studies have used a web-based pregnancy management program that showed an increase in pregnant healthcare knowledge, self-efficacy, healthy behaviors, and better program satisfaction in the intervention group.10,19
The PWW have been reported to have many difficulties in receiving prenatal care and education. Their unmet educational and information needs often lead to anxiety and poor pregnancy management. To address these needs, this study aimed to 1) develop an smartphone application to deliver prenatal education and support self-care behavior for South Korean PWW and 2) examine preliminary effects and usability of the program.
Materials and Methods
This study included two phases. In phase one, the Self-care for Pregnant Women at Work (SPWW) mobile application was designed and developed by the research team. In phase two, usability testing of SPWW was performed by 31 PWW and 13 healthcare providers who were familiar with pregnant women’s health. The study data was collected between March and October 2019. This study complies with the Declaration of Helsinki and was performed according to the Chung-Ang University Institutional Review Board’s approval (1041078–201905-HRSB-153-01).
Phase 1. Development of SPWW
The Orem’s Self-care Deficit Nursing Theory guided the development of SPWW.20 According to the theory, human have an eager to care for oneself.21 Self-care deficit occurs when one’s self-care capacity and ability does not meet the self-care demands.21,22 This is when nursing becomes necessary.21,22 We understood from the previous studies that the PWW are experiencing self-care deficit due to various barriers from work that limit women from performing self-care.8,9 The SPWW was designed to support nursing system that addresses the deficit.
The development process and brief technical flow of the SPWW are described in Figure 1. The SPWW was developed in Google Play Console23 with Amazon Web Services backend support for storage.24 The Firebase Could Messaging was used to send messages to the users.25 The contents and constructs of the SPWW were designed based on a previously-conducted systematic review of technology-supported intervention for pregnant women.26 The health topics on which the SPWW focused on were selected based on priority health practices described in a systematic review of the technology-supported intervention for pregnant women.26 The components and functions of the SPWW were selected based on the previous study, which explored key elements of mHealth interventions.27 The most frequently used behavioral change techniques were setting behavioral goals, providing information, and promoting self-monitoring.27 The SPWW included all of these components.
 |
Figure 1 Development process and basic technical flow of Self-care for Pregnant Women at Work Mobile Application. |
The research team members consisted of a primary investigator (nursing school professor) and three registered nurses (one nurse with a Master of Science in Nursing, two with a Bachelor of Science in Nursing degrees). The technology team members constituted two software experts with various experience in developing mobile applications and one software designer. To develop an acceptable intervention program, the research team and technology team held multiple meetings to finalize the prototype between March and July 2019. Several strategies for promoting adherence to the program were discussed and embedded in the program. The application was built for the Android platform as it allows easy launch to application stores and easy updates.
Phase 2. Preliminary Effects and Usability Testing of SPWW
Participants and Settings
The usability of SPWW was tested between August and October 2019 from PWW and healthcare providers. Researchers typically recommend a sample size of a pilot study to be between 10 and 40 participants or 10% of the final study size of the pilot study.28 The sample size of the final study was calculated to be 74; however, to address possible drop-outs and calculate reliability of the study instruments, we decided to have at least 30 PWW and 10 healthcare providers for usability tests. To minimize the sampling bias only inclusion criteria of the PWW were being less than 36-week of pregnancy (considering the study period) and women who can read and type through smartphone. The healthcare providers with more than 5 years of working with this population were included in the study.
Data Collection
The PWW were recruited using a convenient sampling method. The study was advertised on three major online communities where pregnant women often exchange information and had separate posting sections for pregnant women and mothers who work. The study was delineated as a web post with a link to download the application through Google Play. After installation, the women were asked to sign informed consent, generate a nickname, answer a list of questions, and then submit. The project investigator reviewed the answers and approved their participation in the study. Upon approval, the push message was sent to the participants and asked to review step-by-step instruction for using application and answer a pre-intervention questionnaire. After completing the questionnaire, they were able to use the application freely for two weeks. On the 14th day, the participants received a push message that guides to answer a post-intervention questionnaire.
Contrarily, the healthcare providers were recruited using the snowball sampling method. It is an effective way to gather rich data based on reliable interpersonal relationships among healthcare providers.29 The project investigator explained the study to two healthcare providers who worked in the obstetrics and gynecology unit and were invited to pass on this study information to their colleagues. After signing the informed consent, the healthcare providers were able to navigate the application freely for two weeks. On the 14th day, the link to the post-intervention questionnaire designed through SurveyMonkey for the healthcare providers was sent through a multimedia messaging service. The participants from both groups received $10 mobile gift card as compensation.
Instruments
The PWW received total of 22 items on sociodemographic, pregnancy-related, and work pattern-related questions. The healthcare providers received three questions regarding their age, occupation, and years of working. The PWW received questions on health practices for healthy pregnancy and system usability. The healthcare providers only received questions on system usability. The application usage information was collected among PWW, including the amount of time spent on each application component, how they set their application alarm preferences, and performance on health logs. The primary outcomes of the study were health practices of pregnant women and application usability.
The participants’ health practices related to pregnancy were assessed using the Health Practices in Pregnancy Questionnaire-II (HPQ-II),3 a 34-item questionnaire. A higher summed score indicated a person performing more health-promoting practices in pregnancy.3 Cronbach’s alpha of the scale was 0.813 and 0.90.30 Since a Korean-language version of the scale was unavailable, the research team translated the scale into Korean using forward-and-back translation.31 During the translation process, four items from the scale were removed as they were relatively irrelevant to South Korean culture (eg, use of marijuana). A modified 30-item Korean version of the HPQ-II showed a Cronbach’s alpha of 0.86 in this study.
The usability of the SPWW mobile application was evaluated using the System Usability Scale (SUS),32 a 10-item scale. According to the scoring rubric, 1 was subtracted from odd-numbered items and scores of even-numbered items were subtracted from 5. The summed score was multiplied by 2.5. This final score ranged between 0 and 100. A score over 68 is considered to be a system with “good” usability.33 The Cronbach’s alpha was 0.81 in our study. In addition to the SUS, we added four open-ended questions to listen to the actual voices of the participants on suggestions to improve the application.
Data Analysis
The SPSS 25.0 statistical software package was used to analyze the quantitative data of each group. To maintain the validity of the study, participants who missed over 10% of the total questions were excluded from the study.34 The missing data from the remaining participants’ was assessed for missing at randomness and all analyses were conducted without data imputation.35 The sociodemographic data were analyzed using descriptive analysis. The preliminary effects of the SPWW on the study variables were analyzed through paired t-tests. The usability of the SPWW applications was analyzed through calculation of the SUS score and performing a content analysis of the qualitative data retrieved from four additional open-ended questions. The ATLAS.ti 8 software package was used for qualitative analysis.
Results
Phase 1. Development of SPWW
The four health practices addressed through SPWW were: (1) getting enough sleep and rest; (2) healthy eating; (3) enhancing physical activity; and (4) stress management. Each topic was addressed through the four components of SPWW (Figure 2): (1) Education Sessions; (2) the Health Log; (3) the Diary; and (4) the Discussion Board. The users could freely navigate these four components by tapping on each icon fixed at the bottom of the application.
 |
Figure 2 Four components of SPWW mobile application (English translated version). |
In the “Education Sessions,” eight educational reading materials were available from the eight different topics. The reading materials targeted a below-fifth-grade reading level and developed by the research team members. The materials’ contents were proofread and revised by two other nursing professors in women’s health. The length of each reading materials was 12 to 17 PowerPoint slides, with an estimated reading time of 15 minutes. The first four sessions were on the study’s targeted four health practices: sleep and rest, eating, physical activity, and stress management. Each session explained why this health practice is important for pregnant women and provided several specific activities that could be done in a work setting. The other four sessions were health information regarding the signs and symptoms of labor onset, tips on hospital admission for delivery, the four stages of labor, and labor pain management. To keep the participants’ adherence to the program, the first four educational materials were available from the beginning of their participation in the study, but the latter four materials were available from day 8 of participation.
The “Health Log” was designed to help participants set individualized goals to perform health practices on the study’s four targeted topics. They were asked to type in what kinds of specific activities they would like to do for each of the four topics and how often they would like to do them (eg, stretching for enhanced physical activity (topic 3) every 2 hours). The goal setting page guided the participants to refer to “Education Sessions” to help them set goals. Once they set the goal, they began receiving push alarms from the applications saying, “It is time to do health practices,” according to their alarm regularity settings. The users were free to change activities and the regularity of the alarm at any time. Also, they were able to provide their sleeping times (eg between 9 p.m. and 7 a.m.) and snooze the application’s push alarms. Upon receiving push alarms from the application, the users were guided to choose “performed” or “not performed” on each of their pre-set activities. Their performance was calculated in percentage and colors (blue for meeting over 70% of performance, yellow for meeting over 30% of performance, red for meeting less than 30% of performance). This visualization of daily performance was another strategy for the participants to enhance adherence and compliance to the study program (ie, get more green days).
The “Diary” was designed to keep a daily message for the participants’ unborn baby. On top of the diary screen, the day’s health practice performance information was shown. This guided the participants to reflect on their day and to plan better for the subsequent day.
The “Discussion Board” was divided into two. The first board was designed for participants to anonymously post their stories and write comments to each other. The second board was a one-to-one board where participants could ask questions to research team and get answers.
Phase 2. Preliminary Effects and Usability Testing of SPWW
The PWW
Among 37 PWW recruited for the study, six participants who missed over 10% of the total questions at the initial survey were excluded from the study. The sociodemographic information is summarized in Table 1. The participants’ mean length of working was 53.32 months (almost 4.44 years). They worked 8.26 hours a day and worked 4.71 days per week; thus, they worked 38.90 hours per week. Over half of the participants reported they did office jobs (67.7%), 12.9% reported they were educators, and the others said they work for the government or do service jobs.
 |
Table 1 General Characteristics of Participants (Pregnant Women at Work; N=31) |
The average number of views on each of the eight educational sessions ranged between 1.90 and 2.16 times per participant. The most viewed session topics were signs and symptoms of labor onset and tips on hospital admission for delivery. The participants set their alarm to do self-care practices every 4.03 hours on average. The most successful area of their self-care performance was taking prenatal vitamins, while the average performance of each participant was 34.13%.
The effects of the intervention on the PWW is summarized in Table 2. Statistically significant differences before and after the intervention were: “Exercises more than three times a week,” “Drinks adequate fluid (including water),” and “Drinks more than two caffeinated beverages a day.” The participants reported doing more exercise (t = −2.971, p = 0.006), drinking more fluid (t = −3.407, p = 0.002), and drinking less caffeinated beverages (t = 2.065, p = 0.048). The participants’ changes in overall health practices were not statistically significant; however, increased from 3.65 at pre-test to 3.76 at post-test (t = −1.196, p = 0.241).
 |
Table 2 Preliminary Effects on Health Practices (Pregnant Women at Work; N=31) |
The results of the usability assessment of the SPWW mobile application are shown in Table 3. The highest score was scored on the item: “I would imagine that most people would learn to use this system very quickly.” The lowest score was scored on the item: “I needed to learn a lot of things before I could get going with this system.” The calculated score of the scale was 67.82 ± 14.28.
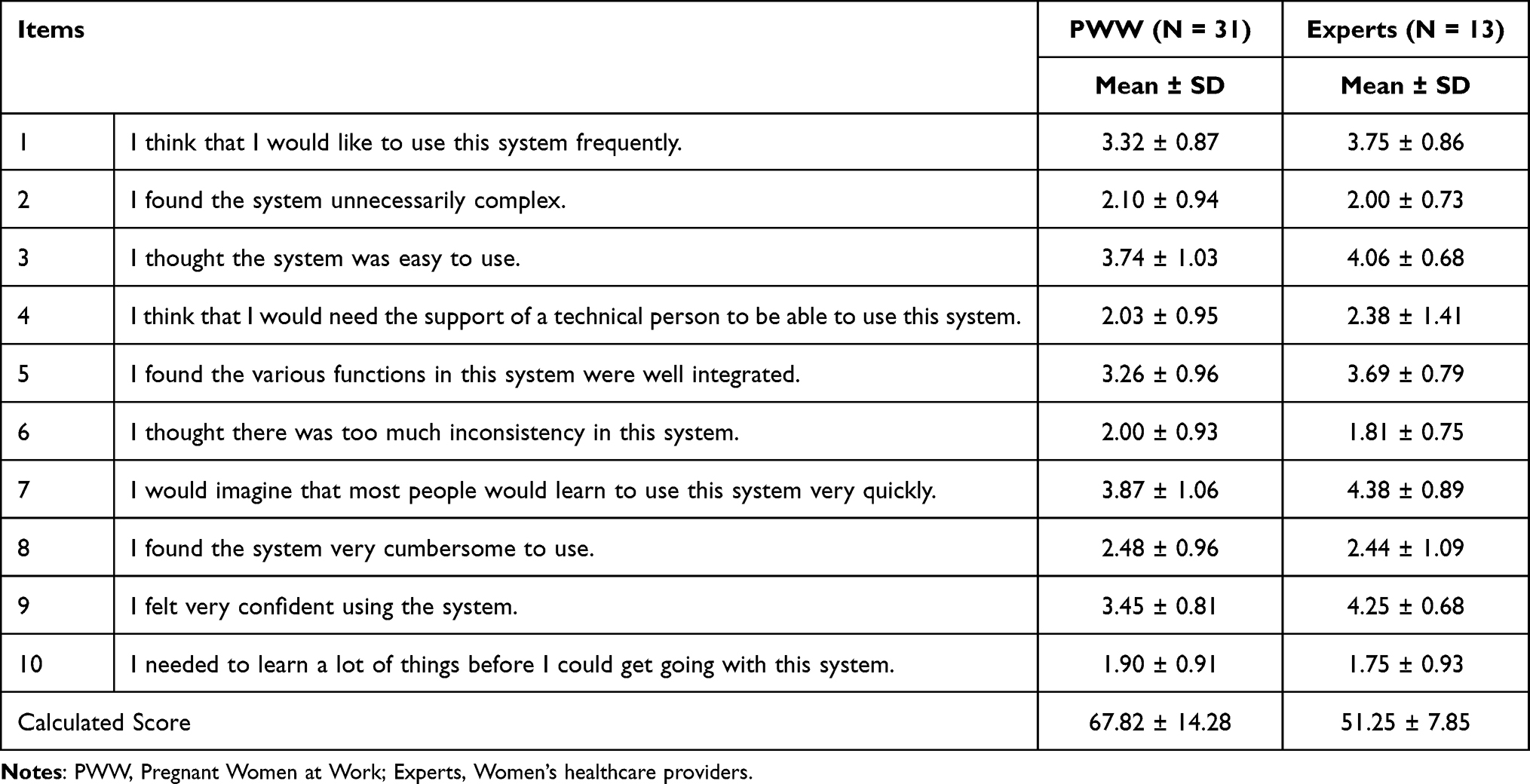 |
Table 3 Usability Assessment of the SPWW Mobile Application |
Of the participants, 64.5% provided specific answers to open-ended questions on usability, and 54.8% commented on the “Education Sessions” component. They reported using the application almost every day and thought the information was easy to understand and helpful. Some asked for a printout option for “Education Sessions” so that they could post on their desks. However, the participants suggested providing more diverse prenatal information with animation and sounds.
I liked the brief in-office stretching guide and diet suggestions. Instead of the weekly educational contents, I would like to have daily educational updates with more fun-to-read pregnancy information (PWW #15).
A majority of participants provided answers about the “Health Log” component (61.3%), with many indicating that they liked this component the most. Some participants suggested having an easy alarm-off function to use during work meetings.
I am experiencing increased forgetfulness during pregnancy. The alarm function was very easy to set and helpful. I hardly forgot about taking prenatals while using this app. However, an alarm-off function could be helpful when I am in the meeting or need to focus on my work (PWW #4).
Of the participants, 51.6% commented on the “Diary” component, stating that it was easy to use and helpful in reflecting on pregnancy self-care activities. Some suggested having individually customizable functions, such as diverse text font and color options or ways to insert images and photos.
The diary in this app was different from other diary apps as my daily self-care performance was shown in the scene so that I could reflect on my day more “health-wise.” I wished to decorate this diary page with stickers (PWW #21).
The lowest number of participants (38.7%) commented on the “Discussion Board” component. They answered that the one-to-one board that allowed them to ask questions to the research members was helpful. However, they were somewhat reluctant to use the anonymous discussion board.
There were not many postings on the anonymous discussion board. I felt that everyone using this app might be busy at her work and do not have time to chat through the app. Also the sense of “being in a study” made me feel reluctant to share my stories (PWW #26).
Women’s Healthcare Providers
The 13 healthcare providers with over five years of clinical experience and were familiar with pregnant women’s health issues were recruited from the medical institutions. The mean age of the participants was 33.62 years old. Four participants were physicians and the others were registered nurses. Their average work years were 8.84. The highest and the lowest scored items from the usability assessment of the SPWW mobile application was the same as the PWW group. However, the calculated score on the scale was 51.25 ± 7.85, which was lower than the scores from the PWW group.
All 13 participants provided answers to open-ended questions on usability. The experts’ suggestions were similar to the PWW groups’ (ie, having an alarm-off function, developing diverse educational contents, developing animated education). New suggestions from the experts were developing quiz after education sessions, providing meditation music for stress management, and having sections to keep the users’ physical traits including weights.
Discussion
To our knowledge, this was the first study that has developed a mobile application for PWW and tested its preliminary effects and usability. Our application targeted four self-care practices, sleep and rest, eating, physical activities, and stress management. Similarly, other studies that developed mobile applications for pregnant women targeted healthy eating and exercise advice.36,37 To support the mobile-based intervention, a study provided Fitbit to enhance the level of physical activity38 or dietary recipes to support their dietary choices.39 The preliminary effects and testing of usability was performed with two groups: PWW and women’s healthcare providers. Other studies pilot tested the application with research staff36 or with a targeted user population.38
The mean age of the PWW participants was 32.49 years old. Advanced age in pregnancy is related to a higher susceptibility to health problems.40 Moreover, over 80% of the women were having their first child; thus, may have relatively less knowledge and experience about pregnancy and child birth.41 Considering their mean working hours were 38.90 hours a week, we could infer that they may need to spare extra time and effort to complete their self-care practices or search for health information related to their pregnancy.
The findings of preliminary effects showed improvement in enhancing exercise, drinking adequate fluid, and limiting daily caffeine intake. The SPWW was developed to target four health practices: getting enough sleep and rest, healthy eating, enhancing physical activities, and stress management. All the improvements noted in this study were stressed in in-application education sessions and health logs. Therefore, we could infer that the application contributed to improving PWW’s self-care practices. More emphasis is needed on other health practices. The benefits of exercise in pregnant women have been stressed in multiple studies. The benefits for pregnant women include improvement in cardiovascular function, musculoskeletal discomfort, and glucose tolerance.42 In addition to these physical benefits, regular exercise is helpful in reducing depressive symptoms and improving overall health-related quality of life.43 During pregnancy, fluid needs increase to maintain circulation to the fetus, to form amniotic fluid, and to support maternal blood volume.44 However, pregnant women often experience dehydration without knowing their need for fluid increases or have awareness of their actual fluid intake.44 Drinking 8–10 glasses of water per day is recommended for healthy pregnant women.44 Caffeine consumption during pregnancy is not recommended to exceed 200 mg per day.45 Excessive caffeine intake is related to increased risks of spontaneous abortion and still birth.46
The usability of SPWW was tested using the SUS. Other studies have used different instruments and methods to test the usability, including the Mobile Application Rating Scale (MARS)47 and the alpha test.48 Although, the expert group rated more positively on the overall items than the PWW did, both groups reported that the application was acceptable and very easy to learn. Difficult to use applications often become underused, misused, or deleted from users’ phones.49 Moreover, to minimize the barriers to using mobile-based intervention, the development of detailed explanations and user-friendly applications is important.50
Both the PWW and women’s healthcare providers made several suggestions to improve the SPWW. Research team members addressed the improvements prior to the following randomized controlled study after the pilot study. The improvements made to “Education Sessions” were diversified educational contents and the inclusion of colorful images, as well as an alarm-off function for the “Health Log” component and font change functions for the “Diary” and “Discussion Board.”
Limitations of the Study
The study poses several limitations. First, the study was limited to using online recruitment. Sampling bias often exists in web-based studies.51 However, considering the participants were relatively young adults and the ubiquity of the internet and smartphones in South Korea, we expect the sampling bias to be minimal. Moreover, authenticity of the participants can be another limitation to web-based studies.52 Therefore, careful consideration is necessary when interpreting the study’s findings. Second, the study holds a limitation of response shift bias.53 The PWW group’s pre-test and post-test responses were collected two weeks apart. The participants’ post-test response could have changed due to the changes in their internal standards of questionnaires or efforts to meet the target goals addressed in the study intervention. To minimize this risk, their pre-test answers were hidden by the application before initiating the actual use of the mobile application.
Conclusion
Pregnant women who work often find it difficult to participate in regular prenatal care or perform daily self-care related to their pregnancy because of inflexible working conditions. This study developed a mobile-based intervention program for South Korean PWW to enhance their self-care practices, which can contribute to a healthy pregnancy. The SPWW was effective in enhancing exercise, drinking adequate fluid, and limiting daily caffeine intake. For the use of the application, both PWW and expert groups reported good usability of the mobile application. The results from this study suggest that SPWW can be an acceptable, engaging, manageable, and effective intervention for PWW. Still, there is a need for future research to test the long-term effects of this application on larger sample sizes. Nevertheless, the application developed in this study is promising, in that it can help PWW enhance their self-care practices and maintain healthy lives during their pregnancy in a user-friendly way. Additionally, developmental process and the details of the application are explained in this manuscript. We expect this manuscript to provide a guide for researchers who plan to develop user-friendly mobile applications involving the target population and utilize it in the intervention study.
Acknowledgments
We would like to thank the two healthcare providers from the obstetrics and gynecology unit for their assistance in recruiting women’s healthcare providers for the study.
Disclosure
This research was funded by the National Research Foundation of Korea in 2019-2020 (2017R1C1B5075221). The funding body plays no role in the design of the study, data collection, analysis, interpretation, and writing the manuscript. The authors report no conflicts of interest in this work. The data of this study is available from the project investigator upon reasonable requests.
References
1. Van der Gucht N, Lewis K. Women’s experiences of coping with pain during childbirth: a critical review of qualitative research. Midwifery. 2015;31(3):349–358. doi:10.1016/j.midw.2014.12.005
2. Javanmardi M, Noroozi M, Mostafavi F, Ashrafi-Rizi H. Internet Usage among Pregnant Women for Seeking Health Information: a Review Article. Iran J Nurs Midwifery Res. 2018;23(2):79–86. doi:10.4103/ijnmr.IJNMR_82_17
3. Lindgren K. Testing the Health Practices in Pregnancy Questionnaire–II. J Obstetric Gynecol Neonatal Nursing. 2005;34(4):465–472. doi:10.1177/0884217505276308
4. Amanak K, Sevil U, Karacam Z. The impact of prenatal education based on the Roy adaptation model on gestational hypertension, adaptation to pregnancy and pregnancy outcomes. J Pak Med Assoc. 2019;69(1):11–17.
5. Serçekuş P, Başkale H. Effects of antenatal education on fear of childbirth, maternal self-efficacy and parental attachment. Midwifery. 2016;34:166–172. doi:10.1016/j.midw.2015.11.016
6. Cantone D, Lombardi A, Assunto DA, et al. A standardized antenatal class reduces the rate of cesarean section in southern Italy: a retrospective cohort study. Medicine. 2018;97(16):e0456. doi:10.1097/md.0000000000010456
7. Wang HJ, Park HS, Kim IO. Comparison of Prenatal Health Management State and Educational Needs for Pregnant Women with Advanced Maternal Age and Under the Age of 35. Comparison of Prenatal Health Management State and Educational Needs for Pregnant Women with Advanced Maternal Age and Under the Age of 35. Korean J of Women Health Nursing. 2013;19(4):230–241.
8. Karkowsky CE, Morris L. Pregnant at work: time for prenatal care providers to act. Am J Obstet Gynecol. 2016;215(3):
9. Sanguanklin N, McFarlin BL, Finnegan L, et al. Job strain and psychological distress among employed pregnant Thai women: role of social support and coping strategies. Arch Womens Ment Health. 2014;17(4):317–326. doi:10.1007/s00737-013-0410-7
10. van den Heuvel JF, Groenhof TK, Veerbeek JH, et al. eHealth as the Next-Generation Perinatal Care: an Overview of the Literature. J Med Internet Res. 2018;20(6):e202. doi:10.2196/jmir.9262
11. Korea Statistical Information Service (KOSIS). Work ratio of women before and after pregnancy. Available from: https://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_CC2020F001&vw_cd=MT_ZTITLE&list_id=D_002_004&seqNo=&lang_mode=ko&language=kor&obj_var_id=&itm_id=&conn_path=MT_ZTITLE.
12. Lee B-E, Ha M, Park H, et al. Psychosocial work stress during pregnancy and birthweight. Paediatr Perinat Epidemiol. 2011;25(3):246–254. doi:10.1111/j.1365-3016.2010.01177.x
13. Park C, Kang M-Y, Kim D, Park J, Eom H, Kim E-A. Prevalence of abortion and adverse pregnancy outcomes among working women in Korea: a cross-sectional study. PLoS One. 2017;12(8):e0182341. doi:10.1371/journal.pone.0182341
14. Ledford CJW, Canzona MR, Cafferty LA, Hodge JA. Mobile application as a prenatal education and engagement tool: a randomized controlled pilot. Patient Educ Couns. 2016;99(4):578–582. doi:10.1016/j.pec.2015.11.006
15. Valle J, Godby T, Paul DP 3rd, Smith H, Coustasse A. Use of Smartphones for Clinical and Medical Education. Health Care Manag (Frederick). 2017;36(3):293–300. doi:10.1097/hcm.0000000000000176
16. Rathbone AL, Prescott J. The Use of Mobile Apps and SMS Messaging as Physical and Mental Health Interventions: systematic Review. J Med Internet Res. 2017;19(8):e295. doi:10.2196/jmir.7740
17. Winskel H, Kim TH, Kardash L, Belic I. Smartphone use and study behavior: a Korean and Australian comparison. Heliyon. 2019;5(7):e02158. doi:10.1016/j.heliyon.2019.e02158
18. Kim JH, Oh SS, Bae SW, Park EC, Jang SI. Gender Discrimination in the Workplace: effects on Pregnancy Planning and Childbirth among South Korean Women. Int J Environ Res Public Health. 2019;16:15. doi:10.3390/ijerph16152672
19. Lee Y, Moon M. Utilization and Content Evaluation of Mobile Applications for Pregnancy, Birth, and Child Care. Healthc Inform Res. 2016;22(2):73–80. doi:10.4258/hir.2016.22.2.73
20. Hartweg D. Dorothea Orem: Self-Care Deficit Theory. Notes on Nursing Theories. SAGE Publications; 1991.
21. Kumar CP. Application of Orem’s self-care deficit theory and standardized nursing languages in a case study of a woman with diabetes. Int j Nursing Terminol Classifications. 2007;18(3):103–110. doi:10.1111/j.1744-618X.2007.00058.x
22. Hart MA. Orem’s Self-Care Deficit Theory: research with Pregnant Women. Nurs Sci Q. 1995;8(3):120–126. doi:10.1177/089431849500800307
23. Google LCC. Google Play Console Dashboard. Available from: https://play.google.com/console/u/0/developers/7172877606434246916/app-list.
24. Amazon Web Services I. AWS Management Console. Available from: https://ap-northeast-2.console.aws.amazon.com/console/home?region=ap-northeast–2#.
25. Google Developers. Firebase Cloud Messaging. Available from: https://firebase.google.com/docs/cloud-messaging.
26. Lee Y, Cho S. Technology-Supported Interventions for Pregnant Women: a Systematic. CIN. 2019;37(10):501–512. doi:10.1097/CIN.0000000000000535
27. Eckerstorfer LV, Tanzer NK, Vogrincic-Haselbacher C, et al. Key Elements of mHealth Interventions to Successfully Increase Physical Activity: meta-Regression. JMIR mHealth and uHealth. 2018;6(11):e10076–e10076. doi:10.2196/10076
28. Hertzog MA. Considerations in determining sample size for pilot studies. Res Nurs Health. 2008;31(2):180–191. doi:10.1002/nur.20247
29. Sheu SJ, Wei IL, Chen CH, Yu S, Tang FI. Using snowball sampling method with nurses to understand medication administration errors. J Clin Nurs. 2009;18(4):559–569. doi:10.1111/j.1365-2702.2007.02048.x
30. Alhusen JL, Ayres L, DePriest K. Effects of Maternal Mental Health on Engagement in Favorable Health Practices During Pregnancy. J Midwifery Womens Health. 2016;61(2):210–216. doi:10.1111/jmwh.12407
31. Squires A, Aiken LH, van den Heede K, et al. A systematic survey instrument translation process for multi-country, comparative health workforce studies. Int J Nurs Stud. 2013;50(2):264–273. doi:10.1016/j.ijnurstu.2012.02.015
32. Brooke J. SUS: A ‘Quick and Dirty’ Usability Scale. Usability evaluation in industry. Taylor & Francis; 1996.
33. Mohamad Marzuki MF, Yaacob NA, Yaacob NM. Translation, Cross-Cultural Adaptation, and Validation of the Malay Version of the System Usability Scale Questionnaire for the Assessment of Mobile Apps. JMIR Hum Factors. 2018;5(2):e10308. doi:10.2196/10308
34. Dong Y, Peng CYJ. Principled missing data methods for researchers. SpringerPlus. 2013;2(1):1–17.
35. Enders CK, Bandalos DL. The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Structural Equation Modeling. 2001;8(3):430–457.
36. Dodd JM, Louise J, Cramp C, Grivell RM, Moran LJ, Deussen AR. Evaluation of a smartphone nutrition and physical activity application to provide lifestyle advice to pregnant women: the SNAPP randomised trial. Matern Child Nutr. 2018;14:1. doi:10.1111/mcn.12502
37. Redman LM, Gilmore LA, Breaux J, et al. Effectiveness of SmartMoms, a Novel eHealth Intervention for Management of Gestational Weight Gain: randomized Controlled Pilot Trial. JMIR Mhealth Uhealth. 2017;5(9):e133. doi:10.2196/mhealth.8228
38. Choi J, Lee JH, Vittinghoff E, Fukuoka Y. mHealth Physical Activity Intervention: a Randomized Pilot Study in Physically Inactive Pregnant Women. Matern Child Health J. 2016;20(5):1091–1101. doi:10.1007/s10995-015-1895-7
39. Kennelly MA, Ainscough K, Lindsay K, Gibney E, Mc Carthy M, McAuliffe FM. Pregnancy, exercise and nutrition research study with smart phone app support (Pears): study protocol of a randomized controlled trial. Contemp Clin Trials. 2016;46:92–99. doi:10.1016/j.cct.2015.11.018
40. Jolly M, Sebire N, Harris J, Robinson S, Regan L. The risks associated with pregnancy in women aged 35 years or older. Hum Reprod. 2000;15(11):2433–2437. doi:10.1093/humrep/15.11.2433
41. Jokić-Begić N, Zigić L, Nakić Radoš S. Anxiety and anxiety sensitivity as predictors of fear of childbirth: different patterns for nulliparous and parous women. J Psychosom Obstet Gynaecol. 2014;35(1):22–28. doi:10.3109/0167482x.2013.866647
42. Melzer K, Schutz Y, Boulvain M, Kayser B. Physical activity and pregnancy: cardiovascular adaptations, recommendations and pregnancy outcomes. Sports Med. 2010;40(6):493–507. doi:10.2165/11532290-000000000-00000
43. Montoya Arizabaleta AV, Orozco Buitrago L. Aerobic exercise during pregnancy improves health-related quality of life: a randomised trial. J Physiother. 2010;56(4):253–258. doi:10.1016/s1836-9553(10)70008-4
44. Montgomery KS. Nutrition Column An Update on Water Needs during Pregnancy and Beyond. J Perinat Educ. 2002;11(3):40–42. doi:10.1624/105812402x88830
45. Wierzejska R, Jarosz M, Wojda B. Caffeine Intake During Pregnancy and Neonatal Anthropometric Parameters. Nutrients. 2019;11:4. doi:10.3390/nu11040806
46. Li J, Zhao H, Song JM, Zhang J, Tang YL, Xin CM. A meta-analysis of risk of pregnancy loss and caffeine and coffee consumption during pregnancy. Int J Gynaecol Obstet. 2015;130(2):116–122. doi:10.1016/j.ijgo.2015.03.033
47. Rodríguez S, Sanz AM, Llano G, et al. Acceptability and usability of a mobile application for management and surveillance of vector-borne diseases in Colombia: an implementation study. PLoS One. 2020;15(5):e0233269. doi:10.1371/journal.pone.0233269
48. Madhani Z, Aslani A, Kasraeian M. Development and Pilot Testing of a Mobile Based Patient Decision Aid for Childbirth Decision Making. Stud Health Technol Inform. 2019;261:223–229.
49. Maguire M. Methods to support human-centred design. Int J Hum Comput Stud. 2001;55(4):587–634. doi:10.1006/ijhc.2001.0503
50. Schnall R, Rojas M, Bakken S, et al. A user-centered model for designing consumer mobile health (mHealth) applications (apps). J Biomed Inform. 2016;60:243–251. doi:10.1016/j.jbi.2016.02.002
51. Lee Y, Im EO. Stress and premenstrual symptoms among Korean women studying in the U.S. and South Korea: a longitudinal web-based study. Women Health. 2017;57(6):665–684. doi:10.1080/03630242.2016.1181139
52. Im EO, Chee W. Issues in Internet research. Nurs Outlook. 2003;51(1):6–12. doi:10.1067/mno.2002.29
53. Tugwell P, Knottnerus JA. Does response shift bias invalidate asking patients if they are better or worse? J Clin Epidemiol. 2014;67(5):485–486. doi:10.1016/j.jclinepi.2014.02.007
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Midwives’ Experiences of Caring for Ukrainian War Refugees: A Qualitative Study
Leoniuk K, Sobczak K, Kamińska-Skrzyńska W, Janaszczyk A
Risk Management and Healthcare Policy 2025, 18:2505-2514
Published Date: 28 July 2025
Digital Health in Pediatric Oncology and Hematooncology: A Quasi-Systematic Review of Telehealth, mHealth and Precision Medicine
Ziętara KJ, Pawłowski P, Zaj N, Banasik M, Samardakiewicz M
Cancer Management and Research 2026, 18:570990
Published Date: 17 April 2026