Back to Journals » Risk Management and Healthcare Policy » Volume 18
Midwives’ Experiences of Caring for Ukrainian War Refugees: A Qualitative Study
Authors Leoniuk K ![]() , Sobczak K
, Sobczak K ![]() , Kamińska-Skrzyńska W
, Kamińska-Skrzyńska W ![]() , Janaszczyk A
, Janaszczyk A
Received 24 February 2025
Accepted for publication 5 July 2025
Published 28 July 2025 Volume 2025:18 Pages 2505—2514
DOI https://doi.org/10.2147/RMHP.S524572
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Katarzyna Leoniuk, Krzysztof Sobczak, Weronika Kamińska-Skrzyńska, Agata Janaszczyk
Department of Sociology of Medicine and Medical Communication, Medical University of Gdansk, Gdansk, Poland
Correspondence: Krzysztof Sobczak, Department of Sociology of Medicine and Medical Communication, Medical University of Gdansk, M. Sklodowskiej-Curie 3a Street, Gdansk, Poland, Tel +48 58 349 15 50, Email [email protected]
Purpose: The outbreak of the war in Ukraine resulted in an increased number of war refugees giving birth in Polish hospitals. The aim of the study was to analyze the experiences of midwives providing perinatal care to war refugees. Additionally, the study aimed to design systemic recommendations to improve the quality of intercultural care.
Patients and Methods: The research was conducted using the qualitative method with the online Semi-Structured Interview technique. When structuring the data, the COREQ standard was chosen in accordance with EQUATOR recommendations. The analysis included interviews with 16 professionally active midwives providing perinatal care in Polish hospitals.
Results: In the study, midwives indicated four types of barriers in the care of war refugees from Ukraine. These includes: language barriers (n=16), cultural barriers (n=8), educational barriers (n=5) and psychological barriers (n=3). Fifteen respondents indicated the occurrence of differences in the care of Ukrainian women giving birth. The dissimilarities were related to the level of cultural differences (tradition; n=15), differences in accommodation (withdrawal, passivity, alienation; n=15) and in assimilation (instrumental acculturation, informational reorientation; n=11).
Conclusion: The obstetric staff notices differences in care, and identifies barriers that affect the quality of medical services provided to war refugees. The analysis of midwives’ statements contributed to the creation of a theoretical concept – a differences in care pyramid. Development of a systemic solution that minimizes the effects of the language barrier is crucial. Moreover, it is important to implement information actions that raise the level of knowledge about the functioning of the health care system in Poland, and prenatal education dedicated to war refugees.
Keywords: pregnancy, female, midwifery, refugees, Ukraine, prenatal care
Introduction
The outbreak of war in Ukraine has caused mass and forced migration, mainly of women and children. On March 3rd in 2022, the Polish parliament adopted the Act on Assistance to Ukrainian Citizens in Connection with the Armed Conflict on the Territory of that Country. It provides, among others, the right to reside, a work permit, and the possibility of using medical care under social insurance. Currently, such rights are available to 968.4 thousand people.1 EUROSTAT data indicated that Poland is the second country with the highest number of refugees from Ukraine (23.7% of all refugees in the EU).2 Ukrainian population was the largest national minority in Poland even before the war. Data obtained from the National Health Fund show that under the Act, in 2022 there were 2843 deliveries, and 2292 in 2023. Giving birth to a child can be one of the most important life events with critical significance, also in terms of social and cultural importance.3 Experiencing a threat to life, need to change place of residence, lack of stability and support from loved ones, may adversely affect the course of pregnancy and childbirth.4–6
Researchers emphasize the need for mental health screening for war-affected women during pregnancy and in the postpartum period, along with easy access to interventions. It should be remembered that language and socioeconomic barriers, as well as cultural differences in attitudes towards mental health can be significant challenges to obtaining the necessary support.7 Refugees find themselves in a situation that requires immediate adaptation to unfamiliar conditions related to medical care. The limiting experience here is the lack of knowledge of the language and customs related to care provided by midwives.8 According to the Communication Accommodation Theory (CAT), this leads to distance between the interlocutors.9 The basis for further interaction is health security, which requires the assimilation of immigrant women. The current situation forces a different approach to the assimilation process than in the classical theory of M. Gordon. First, assimilation must proceed quickly, not gradually.10 Secondly, structural assimilation is key, that is integration at the institutional level.11
The literature often emphasizes the bidirectional nature of the acculturation process itself.12 It is therefore about shaping the cultural competences of the staff.8 Depending on the level of development of these competences, they may have a positive impact on the cultural differences that arise as part of communicative accommodation, leading to their blurring in the assimilation process.12 However, with poor education or lack of cultural competence, differences can turn into barriers to patient care.8
In order to better understand the nature of the problems and challenges related to perinatal care, we asked professionally active midwives about their perspective. The main aim of the study is to diagnose cultural differences noticed by midwives caring for refugee women and to create a typology of barriers in caring for refugee women from Ukraine. We assumed that understanding the perspectives of this group of healthcare workers could become the basis for developing systemic support. Intervention in this area could lead to the development of solutions resulting in improving the quality of medical services in the aspect of care for culturally different women giving birth, not only from Ukraine. Qualitative research in this area is necessary because it allows us to understand the layer of socio-emotional experiences in individual narratives, which can become fundamental for building effective solutions by healthcare providers.13
Materials and Methods
Study Design
The qualitative study with the on-line semi-structured interview technique was used to collect data. The COREQ (COnsolidated criteria for REporting Qualitative research) standard was applied to structure the data in accordance with the recommendations of Enhancing the QUAlity and Transparency of health Research (EQUATOR).
Respondents were informed about the purpose of the study, the voluntary and anonymous the possibility of withdrawing from the study during or after the interview. Moreover, they received information about the data storage including audio recordings, and interview transcripts. Before setting a date for the interview, potential respondents received the above information in writing (e-mail) along with a consent form to participate in the study. The research project and the interview questionnaire were approved by the Bioethics Committee for Scientific Research.
Participant Selection
Purposeful sampling was used in the study. The inclusion criteria used in the study included: completion of vocational education in Poland in the field of midwifery, having the right to practice the profession of a midwife, work experience in a hospital ward providing perinatal care, and expressing informed consent to participate in the study. Information about the research together with an invitation to complete the application was sent to selected hospitals and posted on the Internet on websites dedicated to midwives. Then, the researcher contacted potential respondents, informing them about the purpose of the study and explaining the details of its implementation. Respondents also received a complete set of information via email. The message again included information about the purpose of the study, as well as the methods of storing and using the collected data, as well as a consent form template for participation in the study. Once consent was obtained, interview dates were set.
The interviews were conducted synchronously using the Zoom.us platform, then the audio files with the conversations were archived. The recordings were deposited on a dedicated, protected server and transferred to a professional company with a security certificate to obtain anonymous transcripts. During the study, no sensitive or personal data (as defined by GDPR) was collected or processed, and the image of the respondents was not stored. During the interviews, information was obtained regarding: work experience, position, specialization, type of department, and reference level of the hospital in which the respondents worked. Additionally, midwives were asked to specify the frequency and character of meetings (individual/team) with patients from Ukraine.
Setting
As part of the pilot, 2 interviews were conducted with experienced midwives. Then, the first versions of the interview questionnaire were discussed with the participants. The result of the discussion and analysis of the interviews was the construction of the final version of the interview questionnaire. The research tool consisted of 5 questions about socio-professional variables (work experience, hospital reference level, ward, position, duration or form of employment) and 2 questions about relations with war refugees (frequency and specificity of contacts). The main part of the research tool contained 15 open-ended questions included four research areas:
- Barriers and differences in the care of Ukrainian women in labor (5 questions)
- Cultural stereotypes and behaviors (4 questions)
- Cultural competences of midwives (3 questions)
- Solutions and good practices in intercultural care (3 questions).
In this article, we discuss data obtained based on the first research area, the aim of which is to determine the types of barriers (communication, interpersonal, systemic) that make the care of pregnant women from Ukraine difficult. Additionally, to characterize the cultural differences perceived by midwives that influence the needs and behavior of women in labor.
The interviews were conducted between July 2023 and March 2024. The average duration of the interviews was 22 minutes and 46 seconds, with the shortest lasting 12 minutes and 24 seconds and the longest 32 minutes and 27 seconds. The interviews were conducted at a time convenient for the respondents, without the participation of third parties. After the interviews were completed, the interviewer made a note with comments on the course of the study and the effectiveness of the questions.
Data Analysis
Cognitive analysis (CA) was used to develop the study results within the inductive method strategy. Three members of the research team independently categorized the statements, considering the frequency of their appearance in statements as well as relevance to the analyzed topic. Then a four-person team discussed and established the final categories. Coding trees and tables with interview numbers and sample statements of the respondents were created for the four basic areas. In the analysis of differences in care, 6 categories were identified at 3 levels. Statements regarding barriers to care were divided into 4 main categories and 9 subcategories. The final report included quotes along with the identification (interview number) and frequency of occurrence of a given category.
Results
16 professionally active midwives participated in the study. This article presents the results of the analysis concerning differences and barriers in care and cultural competences of midwives. The majority of respondents had up to 5 years of experience (n=11). Half of the respondents worked in a rotational system (alternately in 2 or 3 departments) or in 2 workplaces. The largest number of respondents worked in obstetrics (n=7) and gynecology departments (n=7) and in the labor ward (n=5) in hospitals with the third reference level (n=9). The frequency of contacts with patients from Ukraine was assessed by 9 respondents as daily and 6 as repeated experience. The largest number of respondents (n=7) defined their main specificity of work as individual contact with patients (Table 1).
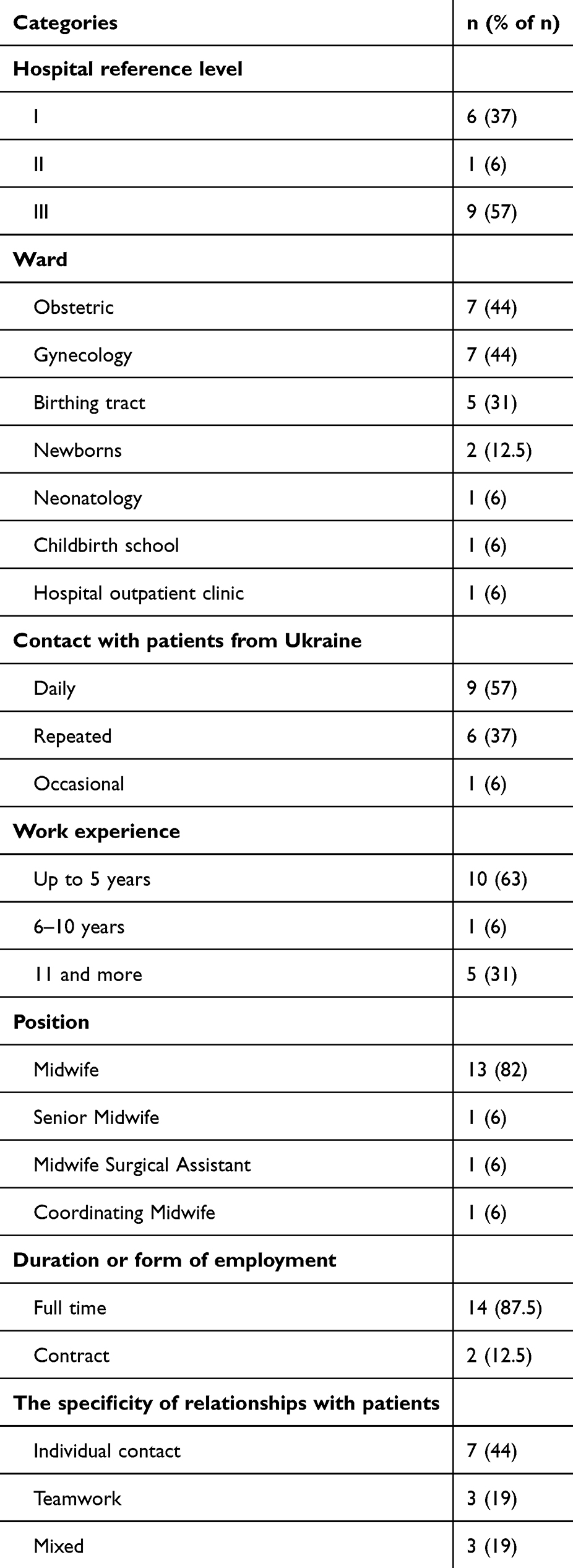 |
Table 1 Professional Variables (N = 16) |
Barriers in Care
All the respondents emphasized the language barrier as the primary difficulty in caring for pregnant women from Ukraine. Most respondents (n=14) also indicated other than language difficulties in contacts with migrants. When categorizing the statements, four groups of barriers reported by midwives were distinguished: language (n=16), cultural (n=8), educational (n=5), and psychological barriers (n=3). Figure 1 presents the distribution of categories and subcategories.
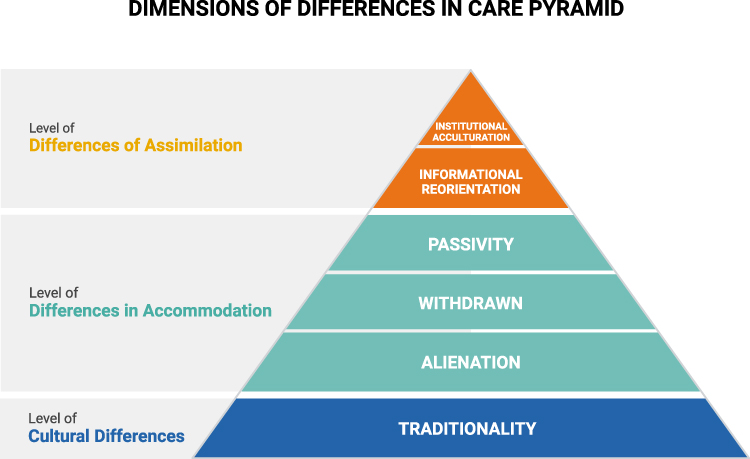 |
Figure 1 Dimensions of Differences in Care Pyramid. Notes: Created in BioRender. Anielska, A. (2025) https://BioRender.com/ smp1dw6. |
Language Barriers
Midwives indicated different levels of knowledge of Polish and English language among Ukrainian women, which had a direct impact on the possibilities of obtaining and transmitting information:
The most difficult thing is the language barrier. Although it seems that these languages are similar, it is difficult to communicate, especially with those patients who have only been there for a short time and have had no contact with the Polish language at all. (Midwife 5, 28 years of work experience)
The methods of overcoming the language barrier were varied. Most of the respondents indicated two or three methods that they used while performing their professional duties. The most frequently indicated solutions included using a translator (n=11) and assistance from medical or support staff from the Ukraine (n=10). Only half of the respondents declared that they used documents in Ukrainian while working, and four cooperated with a professional translator.
Cultural Barriers
Analyzing the respondents’ statements in the context of cultural differences, 3 subcategories were distinguished. The first one is the approach to childbirth (n=5). Midwives pointed to: a preference for natural childbirth, breastfeeding and little interest in new forms of childbirth among patients from Ukraine:
I think most of them base their experience on their parents, mothers or grandmothers… they are more focused on natural childbirth, breastfeeding, everything more physiological. (Midwife 1, 11 months of work experience)
Four midwives noticed differences in approach to newborn care, which were classified as the second subcategory of cultural barriers. The respondents drew attention to differences in child care, lack of prenatal education, reluctance to use a breast pump, and willingness to use a milk bank:
In our country, the milk bank is a very controversial topic, Poles very often disagree because they think it is disgusting, and Ukrainian parents usually agree. (Midwife 7, 12 months of work experience)
Patients from Ukraine are less likely to use, for example, antenatal education and childbirth classes. (Midwife 8, 12 months of work experience)
The third subcategory of cultural barriers is the approach to health (n=3). The respondents noted different methods of taking care of health in the postpartum period, different availability of vaccinations, screening tests and contraceptive methods between Ukraine and Poland:
A lot of tests, for example hearing tests or screening tests, vaccinations, well, not all of these patients know that we have something like that, because they don’t have it. (Midwife 6, 12 months of work experience)
Educational Barriers
Five respondents drew attention to the barrier resulting from the insufficient knowledge of Ukrainian patients regarding the functioning of the healthcare system in Poland (lack of understanding of the tasks of individual elements of the system - emergency department, clinic, hospital; lack of knowledge of patient’s rights; lack of knowledge of hospital regulations and procedures - intuitive action):
Ladies don’t know how our system works, that when nothing happens, you go to the clinic, so I kind of understand these visits to the ER. (Midwife 12, 6 years and 6 months of work experience)
Additionally, two of the respondents drew attention to insufficient health education (patients do not know what they should report to the staff, they react with surprise to standard procedures such as blood sampling or insertion of an IV catheter).
Psychological Barriers
Three of the respondents emphasized psychological barriers, which included: difficult access to psychological support in crisis situations (intensive neonatal care), burden of war experiences and the absence of loved ones during childbirth:
There was one woman who ended up in the maternity ward after 12 hours on the train, who had escaped from Ukraine and came to us straight to the maternity ward because she had simply started bleeding on the train. (Midwife 2, 11 months of work experience)
Care Differences
The second research area concerned differences in care. Only one respondent did not indicate their occurrence. Based on the analysis and categorization of the meanings of the respondents’ statements (n = 15), a pyramid of differences was created, consisting of 6 categories arranged on 3 levels (Figure 2).
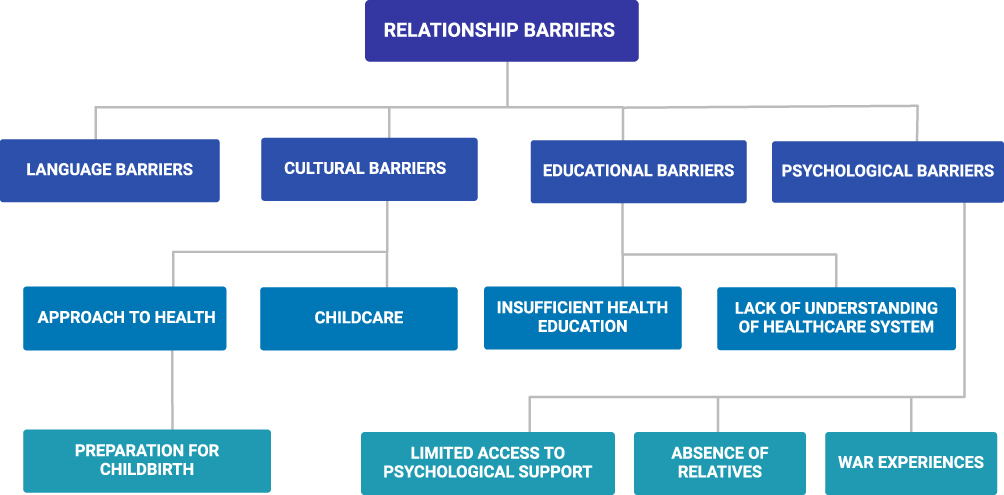 |
Figure 2 Relationship Barriers. Notes: Created in BioRender. Anielska, A. (2025) https://BioRender.com/ rwzm6ap. |
The Level of Cultural Differences
The base of the pyramid is the level of cultural differences containing references to fundamental values and beliefs about childbirth and infant care passed on to women culturally (traditionality, n=14). This area was the most frequently noticed difference indicated by fourteen midwives. The respondents noticed among the emigrants a greater attachment to traditional knowledge and experiences passed on intergenerationally in the family, a preference for physiological childbirth and breastfeeding, and less interest in proposals related to improving comfort during childbirth and the postpartum period.
Polish women come really from the first slight abdominal tension, and here the ladies come at the end. I have never had anyone be induced. (Midwife 14, 7 months of work experience)
Level of Accommodation Differences
The second level of the pyramid is differences in accommodation, which refer to the psychological and social consequences of forced migration. Midwives noted the alienation (n = 15), withdrawal (n = 9) and passivity (n = 9) of Ukrainian women. Alienation is mainly evidenced by statements referring to communication problems, including taciturnity, not asking questions, lack of effusiveness, less articulation of needs, or pretending to understand instructions:
Patients are not very talkative, they rather answer questions, they themselves do not seem to want to talk about anything else. (Midwife 1, 12 months of work experience)
The midwives also noted behaviors indicating the withdrawal of the refugees, describing them as: quiet, modest, closed, calm, reserved, stressed, subdued, uncertain, worried, shy, polite, fearful, less expressing emotions, not wanting to cause problems.
These patients are more subdued. They don’t show their emotions as much as Polish patients. (Midwife 6, 12 months of work experience)
The last subcategory at the level of differences in accommodation is passivity. The respondents indicated less articulation of needs, lack of inquisitiveness, low requirements, a waiting attitude and greater submissiveness towards midwives:
When it comes to parents from Ukraine, they are usually so calm, modest and simply cannot communicate in Polish that they just give up and leave. (Midwife 7, 12 months of work experience)
Level of Differences in Assimilation
The third level of the pyramid consists of differences in the level of assimilation. Two categories were distinguished at this level, the first is informational reorientation (n = 11) understood as the need to function in a new cultural space without having the appropriate information and experience, as evidenced by statements of midwives regarding: differences in knowledge of perinatal care, lack of knowledge of patient rights, less frequent preparation in childbirth classes, lack of a birth plan, information on vaccinations and screening tests mandatory in Poland, required tests or medical documentation:
Patients from Ukraine are less likely to use, for example, antenatal education or childbirth classes, but this may be due to the fact that most of them are conducted in Polish, they have less access to such places, so if they want to learn, they rather do it on their own, from their closest relatives or simply from other people. (Midwife 8, 7 months of work experience)
The second category is instrumental acculturation (n=10) which included: patients’ expressions of surprise at the complementarity of care, encouragement to ask questions, positive assessment of the database and the level of services, openness of medical staff and gratitude related to positive experiences:
The patients are satisfied, for example, sometimes they are surprised that we help them so much, that we want to explain and help them. (Midwife 4, 29 years of work experience)
Discussion
In the study we asked 16 professionally active Polish midwives to share their experiences of perinatal care for women giving birth from Ukraine. Analysis of the statements revealed that the experience of difficulties in relation to cultural and social differences and personal experiences of patients significantly affects the nature of care. Language, cultural, educational and psychological barriers are key aspects of interactions that affect the quality of care and, in some areas, also the safety of patients.
One of the key categories was the language barrier. There are many reports indicating the common occurrence of this type of limitation.3,14,15 As Barrio-Ruiz et al pointed out, the language barrier determines the limitation of the ability to navigate the health care system. In our study, all midwives indicated the language barrier as a significant obstacle in providing perinatal services to women from Ukraine. As many as 11 respondents indicated language skills and an active search for methods to overcome the language barrier as important intercultural competences in midwives.
Ukrainian mothers gave great importance to breastfeeding and were skeptical about the existing solutions in child care, such as: methods of newborn care or vaccinations. It seems to us that this area is particularly sensitive.3 On the one hand, women who give birth have the right to act in accordance with their own beliefs, traditions and preferences.16 On the other hand, these expectations may not be possible to meet in a different healthcare system.17 One of the areas that clearly illustrates this type of tension is the differently constructed neonatal vaccination program in Ukraine than in Poland.
Other issue was that migrants did not know their patient rights and the rules and procedures in force in healthcare facilities well enough. This situation may increase the medical risk of pregnant women and result in their medical isolation.18 It also reinforces the structural asymmetry between healthcare workers and patients, which, according to reports, poses a potential risk of abuse and fosters distrust.19,20
The differences in care pyramid that we proposed (Figure 1) highlights the complexity of the perception of migrant patients by midwives. The basis of the pyramid is cultural differences expressed in the expectations, attitudes and behaviors of patients during labor and in child care. The level of differences in accommodation refers to the uncertainty and fears that accompany the need to quickly adapt to a new, unfamiliar institutional space. The passivity and withdrawal noticed by midwives may result from both traumatic experiences related to war and/or migration, as well as from the language barrier that prevents free communication with staff. The level of differences in assimilation indicates adaptation to the new reality, acceptance of standards and penetration into new treatment and care structures. Assimilation and accommodation are therefore understood as a process of cognitive changes aimed at adaptation and development.10 The higher the level of the pyramid, the easier it seems to change the elements identified as differences in care, mainly through disseminating knowledge about the operation of the healthcare system, health education, including prenatal education, or introducing systemic solutions that improve the functioning and communication in medical institutions.
The discussion of the presented results indicates the need not only to adapt the healthcare system, but also to conduct educational activities supporting the development of cultural competences of medical personnel. There are many tools that have already been developed to improve the quality of medical care for war refugees. In our further research, we would like to focus on developing systemic solutions, consisting of:
- Developing and implementing communication cards that, using pictograms, would help in quick communication, collecting key medical information, and informing about medical interventions and obtaining informed consent from the patient,
- Creating a training program to develop intercultural competences for midwives and implementing it in cooperation with the Chamber of Nurses and Midwives,
- Cooperating with non-governmental organizations and patient foundations in order to draw attention to the need to activate local community leaders (assimilated significant others in migrant communities), who may prove to be an important social resource in finding the right path to the health care system.
We are aware that our study also has objective limitations. The first one concerns the reference of the obtained results to other contexts occurring in studies on war refugees giving birth. We acknowledge that caution should be exercised when comparing results across studies referring to different healthcare systems and different migration spaces. Sociocultural conditions and solutions within health care systems seem to function in a very wide spectrum of cultural sensitivity, which is conditioned by macro and micro social factors. However, the threads appearing in our studies and the studies of other authors, seem to focus on a common area of problems and challenges. The second significant limitation, is the situation of migrants in relation to the quality standard within the organization of health care in a given country. Baranowska et al noticed that among Polish women a sense of discrimination and stigmatization was revealed by 8.8% of the respondents, a lack of respect from the medical personnel by 16.3%, not providing all the necessary information by 35.3% and providing information in an incomprehensible way by 17.1%.21 It can therefore be assumed that conditions related to the sociocultural situation of refugee women seem to expose problems and beliefs in providing high-quality.
We are also aware that the results obtained may be influenced by the length of service of the midwives surveyed, which is related to their level of professional experience, and may also be influenced by the choice of solutions used.
Conclusion
Understanding the values, beliefs and customs of Ukrainian women giving birth can significantly contribute to improving the quality of their experiences of childbirth and motherhood. These activities also help to avoid misunderstandings, build an atmosphere of safety and respect for different value systems. Every woman, regardless of her social or migration status, should be provided with health care adapted to current standards and taking into account their social and cultural perspective.16,17 The obstetric staff requires organizational support, including preparation of information for patients in Ukrainian language (information on the organization of the health system and the operation of individual hospital departments), bilingual obstetric interview questionnaires and a birth plan. Access to a medical translator, especially in crisis situations and when obtaining intimate information. In order to improve the cultural competence of midwives, it is necessary to provide systemic training in cultural differences and overcoming barriers.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Ethics Approval and Consent to Participate
Our research is in accordance with the Helsinki Declaration. The proprietary research tool was approved by the Independent Bioethics Committee of the Medical University of Gdansk (decision no.100/2022). All methods were carried out in accordance with relevant guidelines and regulations. All participants gave informed consent to participate in the study. The participants informed consent included publication of anonymized responses and direct quotes.
Disclosure
The authors report no conflicts of interest in this work. We declare that we have not used or cooperated with Chat Generative Pre-trained Transformer (ChatGPT) technology or other Artificial Intelligence (AI) models in conducting the study, analyzing the data and preparing the manuscript. The figures were prepared using BioRender.
References
1. Otwarte Dane. Poland’s data portal. Available from: https://dane.gov.pl/en/dataset?categories%5Bid%5D%5Bterms%5D=152.
2. Eurostat. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Ukrainian_citizens_in_the_EU#Population_of_Ukraine.
3. Carolan M, Cassar L, Dip G. Antenatal care perceptions of pregnant African women attending maternity services in Melbourne, Australia. Midwifery. 2010;26(2):189–201. doi:10.1016/j.midw.2008.03.005
4. Arnetz B, Drutchas A, Sokol R, Kruger M, Jamil H. 1991 Gulf War exposures and adverse birth outcomes. US Army Med Dep J. 2013:58–65.
5. Keasley J, Blickwedel J, Quenby S. Adverse effects of exposure to armed conflict on pregnancy: a systematic review. BMJ Global Health. 2017;2:e000377. doi:10.1136/bmjgh-2017-000377
6. Fellmeth G, Plugge E, Nosten S, et al. Living with severe perinatal depression: a qualitative study of the experiences of labour migrant and refugee women on the Thai-Myanmar border. BMC Psychiatry. 2018;18:229. doi:10.1186/s12888-018-1815-7
7. Rodríguez-Muñoz MF, Chrzan-Dętkoś M. Refugee women and perinatal mental health: the experience of war. Arch Womens Ment Health. 2025;28:197–199. doi:10.1007/s00737-025-01576-z
8. Nenko I, Baranowska B, Szlendak B, Sahraoui N, Węgrzanowska M. We were left to our own devices”: Midwives’ experiences of providing maternity care to Ukrainian women in Poland after the outbreak of the full-scale war in Ukraine. Women Birth. 2024;37:101629. doi:10.1016/j.wombi.2024.101629
9. Hoffman WB, Zhang YB. Explaining communication adjustment: accommodation theory and its utility in intercultural communication. J Intercult Commun Interact Res. 2022;1:75–100. doi:10.3726/jicir.2022.1.0005
10. Hanfstingl B, Arzesek A, Apschner J, Golly KI. Assimilation and accommodation: a systematic review of the last two decades. Eur Psychol. 2021;27:1708. doi:10.1027/1016-9040/a000463
11. Rumbaut RG. Assimilation of Immigrants. Int Encycl Soc Behav Sci. 2015;2:81–87.
12. Elhami A, Roshan A. The history of acculturation: a review article. SHE J. 2024;5(1):180–196. doi:10.25273/she.v5i1.19330
13. Liamputtong P. Qualitative Research Methods.
14. Converso D, Hinddrichs I, Bruno A, Dell’Aversana G, Viotti S. Born in translation: midwifery practice with pregnant migrants — between stereotypes and empathy. Test Psychom Methodol Appl Psychol. 2021;28:19–35. doi:10.4473/TPM28.1.2
15. Barrio-Ruiz C, Ruiz de Vinaspre-Hernandez R, Colaceci S, et al. Language and cultural barriers and facilitators of sexual and reproductive health care for migrant woman in high-income European countries: an integrative review. J Midwifery Womens Health. 2023;69(1):71–90. doi:10.1111/jmwh.13545
16. Pottie K, Greenaway C, Ferightner J, et al. Evidence – based clinical guidelines for immigrants and refugees. CMAJ. 2011;183(12):824–925. doi:10.1503/cmaj.090313
17. Benza S, Liamputtong P. Pregnancy, childbirth and motherhood: a meta-synthesis of the lived experiences of immigrant woman. Midwifery. 2014;30(6):575–584. doi:10.1016/j.midw.2014.03.005
18. Fair F, Raben L, Watson H. Migrant women’s experiences of pregnancy, childbirth and maternity care in European countries: a systematic review. PLoS One. 2020;15(2):0228378. doi:10.1371/journal.pone.0228378
19. Almeida LM, Caldas JP. Migration and maternal health: experiences of Brazilian women in Portugal. Revista Brasileira de Saude Materno Infantil. 2013;13(4):309–316. doi:10.1590/S1519-38292013000400003
20. Phillimore J. Migrant maternity in an era of superdiversity: new migrant’s access to, and experience of, antenatal care in the West Midlands, UK. Soc Sci Med. 2016;148:152–159. doi:10.1016/j.socscimed.2015.11.030
21. Baranowska B, Kubicka-Kraszyńska U, Pietruszewicz J, et al. Is there respectful maternity care in Poland? Women’s view about care during labor and birth. BMC Pregnancy Childbirth. 2019;19:520. doi:10.1186/s12884-019-2675-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Self-Care Mobile Application for South Korean Pregnant Women at Work: Development and Usability Study
Lee Y, Choi S, Jung H
Risk Management and Healthcare Policy 2022, 15:997-1009
Published Date: 11 May 2022