Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Self-Assessed Capabilities, Attitudes, and Stress among Pediatric Nurses in Relation to Cardiopulmonary Resuscitation
Authors Hendy A ![]() , Hassani R, Ali Abouelela M, Nuwayfi Alruwaili A
, Hassani R, Ali Abouelela M, Nuwayfi Alruwaili A ![]() , Abdel Fattah HA, Abd elfattah Atia G, Reshia FAA
, Abdel Fattah HA, Abd elfattah Atia G, Reshia FAA ![]()
Received 18 December 2022
Accepted for publication 17 February 2023
Published 3 March 2023 Volume 2023:16 Pages 603—611
DOI https://doi.org/10.2147/JMDH.S401939
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Abdelaziz Hendy,1 Rym Hassani,2 Madeha Ali Abouelela,3 Abeer Nuwayfi Alruwaili,4 Hadya Abboud Abdel Fattah,5 Gehan Abd elfattah Atia,6,7 Fadia Ahmed Abdelkader Reshia8,9
1Pediatric Nursing Department, Faculty of Nursing, Ain Shams University, Cairo, Egypt; 2Medical Chemistry, University College of Darb, Jazan University, Jazan, Saudi Arabia; 3Medical-Surgical Nursing Department, Faculty of Nursing, Jazan University, Jazan, Saudi Arabia; 4Nursing Administration and Education Department, Al Jouf University, Sakākā, Jouf, Saudi Arabia; 5Nursing Department, Fatima College of Health Sciences, Al Ain, United Arab Emirates; 6Medical-Surgical Nursing Department, Faculty of Nursing, Jouf University, Sakākā, Jouf, Saudi Arabia; 7Medical-Surgical Nursing Department, Faculty of Nursing, Menoufia University, Menoufia, Egypt; 8Medical-Surgical Nursing Department, College of Nursing, Jouf University, Sakāka, Saudi Arabia; 9Critical Care and Emergency Nursing, Faculty of Nursing, Mansoura University, Mansoura, Egypt
Correspondence: Abdelaziz Hendy, Pediatric nursing department, Faculty nursing Ain Shams University, Cairo, Egypt, Email [email protected]
Background: In emergency medicine, cardiopulmonary resuscitation (CPR) is one of the most stressful scenarios for nurses who conduct both basic and advanced resuscitation methods.
Aim: This study aimed to assess nurses’ self-assessed capabilities, attitudes, and stress related to CPR.
Methods: This cross-sectional, observational study was carried out on 748 pediatric nurses at six governmental hospitals. A self–assessed ability questionnaire and a structured stress and attitude questionnaire was used for data collection.
Results: For self-assessed abilities, 45.5% of the nurses had moderate scores. Concerning stress, 48.3% had moderate scores and 63.1% negative attitudes. Also, attitude and self-assessed abilities had a high-frequency negative effect on stress scores (P< 0.05).
Conclusion: Attitude scores increased and stress scores decreased significantly with postgraduate educational level, attendance at training courses on pediatric basic life support and automated external defibrillator use, being exposed to > 10 cardiac arrest cases in the previous year, and having an advanced life-support license (P< 0.05). Positive attitudes and improving self-assessed abilities decreased the nurses’ stress levels related to CPR.
Keywords: attitudes, nurses, self-assessed capabilities, stress, pediatric life support
A Letter to the Editor has been published for this article.
Corrigendum for this paper has been published.
Introduction
Cardiac arrest in children has an incidence of nine per 100,000 annually, and frequently has a terrible prognosis. Children suffering cardiac arrest outside a hospital setting have a 6% overall survival rate.1 Cardiopulmonary resuscitation (CPR) and defibrillation must be started as soon as feasible. Every minute CPR is delayed, life chances reduce by 10%. Health-care staff should obtain CPR training to improve performance and patient outcomes.2 Infant cardiac arrest often begins with respiratory failure that reduces blood oxygen levels. Infant airways differ from adults. These variables make newborn CPR difficult, requiring instruction.3
Since nurses are frontline caregivers who spot collapsed inpatients, administer CPR, and call resuscitative teams, they can spend more time with patients. Nurses care for patients around the clock. In emergencies, doctors may not be nearby. In an emergency, nurses must be aware, quick to reason clinically, technically adept, and emotionally composed. Nurses require the right knowledge and abilities to conduct safe and successful resuscitation.4
All health-care personnel are required to be proficient in CPR, which is considered a core emergency skill. In underdeveloped nations versus developed nations, CPR is still a relatively recent practice.5–7 Clinical results are significantly impacted by the resuscitation’s quality. Training is necessary for the growth and maintenance of efficient resuscitation abilities.8,9 Fear of lawsuits, lack of confidence, and patient injury are all significant barriers that prevent nurses from successfully starting resuscitation and cause it to start later than it should. Increased self-assurance may assist in lessening emotions of powerlessness; therefore, educational initiatives should also address this.9
In actual CPR scenarios, tension and anxiety are prevalent emotions. All health care staff should receive regular CPR training in order to retain proficiency and reduce fear. Health-care professionals’ perspectives on CPR scenarios may influence how they act in such circumstances. It is believed that attitude is a crucial component of competence and the best indicator of one’s purpose to do CPR.10,11 The success of CPR is greatly improved by the presence of professional nurses, and the presence of someone with greater abilities and high self-efficacy can significantly improve the outcome.12
Fear of contracting a contagious infection and a lack of training, which could diminish confidence in doing CPR, are factors that have a detrimental impact on nursing staff’s attitudes regarding the delivery of CPR. Similarly, medical professionals may be hesitant to administer mouth-to-mouth ventilation in the absence of the necessary equipment because of concern that they will become ill, do harm, or that the automated external defibrillator (AED) will not function as intended.13
External defibrillator nurses, especially those with less clinical expertise in pediatric care, feel more apprehensive about pediatric emergency care than those in other groups. Anxiety associated with pediatric emergency care may be decreased by creating a pediatric medical care set and performing off-the-job training.14 In addition, overly stressed nurses feel less satisfied with their jobs and hence give lower-quality nursing care. To maintain and enhance the quality of nursing care, it is crucial to effectively control stress levels in the nursing workplace.15 With little knowledge of the underlying reasons of the disturbed physiology and frequently under pressure, dealing with resuscitation can be stressful and requires key decisions to be made.16
In Egypt, there have been many studies17,18 to measure knowledge and practices of nurses concerning CPR, but we did not find a study that measured nurses’ self-perceived abilities and their effects on levels of stress during CPR. Therefore, this study aimed to measure the self-assessed capabilities, attitudes, and stress among pediatric nurses related to CPR.
Methods
Research Questions
Q1: What are pediatric nurses’ self-assessed abilites, attitudes, and stress related to CPR?
Q2: Are there relationships between pediatric nurses’ characteristics and their attitudes and stress?
Research Hypothesis
Pediatric nurses’ self-assessed belief in their abilities and positive attitudes may lower their stress level in relation to CPR.
Research Design
This cross-sectional, observational study was conducted from May 1 to September 30, 2022. in pediatric intensive care units, neonatal intensive care units, and emergency departments at six government and university hospitals in Egypt. Convenience sampling was used. Invitations to join study were sent to 935 nurses, and 748 accepted, for a response rate of 80%.
Tools of Data Collection
Part I: The first part of the questionnaire gathered the demographic data of respondents: age, sex, marital status, educationall, years of experience, possession of a advanced life-support license, attendance at training courses on AED use and pediatric basic life support (PBLS), and exposure to cardiac arrest cases in the previous year.
Part II: Self assessed ability (independent variable): This was adopted from Koželj et al19 and contained seven questions on, eg, giving advice to the team, performing compressions, and applying the correct algorithm of current guidelines. Responses were based on a three-level Likert scale: 1 for “never”, 2 for “sometimes”, and 3 for “always.” Cronbach’s value for internal consistency reliability was good: α=0.801. Total scores ranged from 7 to 21, with higher scores indicating high self-perceived ability.
Part III: Stress level of nurses (dependent variable): This tool was adopted from Toida and Morimura,14 comprised nine questions on, eg, anxiety about choosing the appropriate size of medical device, anxiety and about choosing the appropriate medicine dose. Each item was measured by scores from 0 to 10, with 0 indicating no anxiety about pediatric care and 10 maximum anxiety. The highest possible VAS score was 90 points for all nine questions. Internal consistency reliability was acceptable: α=0.798.
Part IV: Attitudes of nurses (independent variable): This was adopted from Abolfotouh et al,13 and encompassed 10 items relating to attitudes regarding CPR and AED. The reliability of this tool was good: α=0.835. A three-point Likert scale — 0 for “disagree”, 1 for “neutral”, and 2 for “agree” — was applied, and vice versa for negative statements. Total scores range from 0 to 20, with higher scores indicating positive attitudes.
Scoring Guide
Total self-assessed ability scores were categorized as high (>80%), moderate (60%–80%), and low (˂60%). Total attitude scores were categorized as positive (≥70%), and negative (<70%).20 Total stress scores were categorized as high (>70%), moderate (50%–70%), and low (˂50%).21
Ethics
Ethics approval was obtained from the institutional review board of the Faculty of Nursing ethics committee (12.03.2022). Participation in this study was voluntary, and it complied with the Declaration of Helsinki. Nurses were assured that their feedback would not affect their performance evaluations, work status, or salaries. No written consent was sought, as there were no personal identifiers on the questionnaires. The researchers did not coerce or entice anyone to complete the questionnaire. The questionnaire was filled in anonymously and the data kept confidential and used for research purposes only.
Statistical Analysis
Data were sorted and classified, and results are shown in the tables. SPSS 27 was used to analyze the data. Descriptive statistics were used to characterize participants’ demographic details. Data are presented by frequencies and percentages for categorical variables and by means and standard deviations for continuous variables. A t-test is a statistical test that is used to compare the means of two groups and ANOVA for comparing the means more than two groups. Multiple linear regression was used to identify associations between continuous dependent variable (stress) and one or both independent variables (self-rated abilities and attitude). Statistical significance was set at P<0.05.
Results
A total of 784 nurses were studied. About two-thirds were female (64.8%), 79.1% were married, and 30.6% had >5–10 years of work experience. Slightly less than half (40.6%) were aged 22–≤32 years and a minority (22.6%) aged 42–52 years, with mean age 34.99±5.12. It was revealed that 23.5% of the nurses had a nursing diploma, 41.5% had finished their education at a technical institute of nursing, 28.7% had a bachelor’s degree in nursing, and only 6.3% were postgraduates. Moreover, 51.9% had attended training courses on PBLS had 76.6% had not attended training courses on AED. The data also showed that 9.2% had not encountered a cardiac arrest case in the previous year, while slightly more than half (51.1%) had. A majority (93.4%) had no advanced life-support license, as shown in Table 1.
 |
Table 1 Demographics (n=748) |
As regards the nurses’ self-assessed abilities related to pediatric life support, about two-thirds (63.9%) of respondents never led or gave advice to the team in a cardiac arrest situation. More than a third (43.9%) reported “always” for their ability to perform compressions and ventilation (50.1%), only 22.2% for defibrillation. For applying the correct algorithm of current guidelines, 48.3% reported with “sometimes.” For assessing the responsiveness and breathing of children, 40.2% reported “always” and 40.1% “never” for knowing AED operation (Table 2).
 |
Table 2 Self-assessed abilities (n=748) |
Attitude scores increased significantly with postgraduate education, attending training courses on PBLS and AED use, being exposed to >10 cardiac arrest cases in the previous year, and having an advanced life-support license (P<0.05 for all). Stress scores increased significantly with female sex, age 22–≤32 years, experience years 1–≤5, not attending training courses on PBLS or AED, not being exposed to cardiac arrest cases in the previous year, and not having a advanced life-support license at (P<0.05 for all, Table 3). For self-assessed abilities, 45.5% had moderate scores. Regarding stress, 48.3% had moderate scores and 63.1% negative attitudes (Table 4). On multiple linear regression, F=19.555 (P=<0.05). This analysis explained 68% of the variation in stress scores (R2=0.68) and that attitudes and self-rated abilities had high-frequency negative effects on stress scores (P<0.05; Table 5).
 |
Table 3 Relationships between nurses’ characteristics, stress, and attitudes regarding CPR (n=748) |
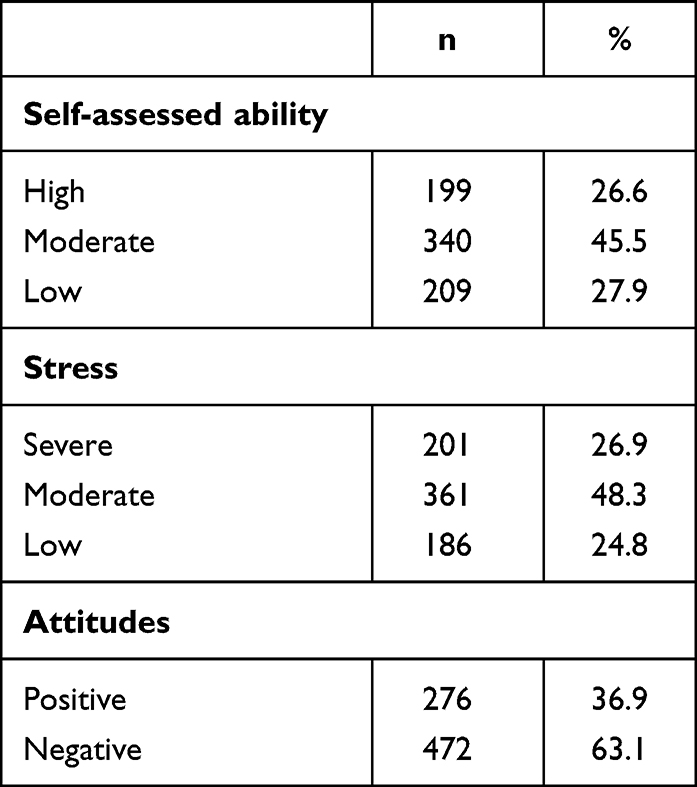 |
Table 4 Self-assessed abilities, stress, and attitudes (n=748) |
 |
Table 5 Multiple linear regression of perceived stress with attitudes and ability (n=748) |
Discussion
Pediatric ED staff have the greatest levels of emotional distress among all health-care providers. Stress impairs cognitive abilities and can improve or impede learning and memory. Attention lapses can lead to medical errors, failure to identify life-threatening symptoms, and other patient-safety issues.22,23 As regards nurses’ self-assessed abilities related to pediatric life support, the current study results revealed that about two-thirds of them had never led or given advice to the team in a cardiac arrest situation. More than a third reported “always” for their ability to perform compressions, half for ventilation, and less than a third for defibrillation. For applying the correct algorithm of current guidelines, nearly half reported “sometimes.” For assessing the responsiveness and breathing of children, more than a third reported “always” and more than a third “never” for knowing AED operation. Less than a quarter of the nurses attended training courses, and only 6.6% had an advanced life-support license.
These results support those of Chandrasekaran et al,24 who reported that awareness of pediatric life support among students, doctors, and nurses of medical, dental, homeopathy, and nursing colleges was very poor. Likewise, Silverplats et al25 reported that ability to perform defibrillation was strongly agreed to by 43%, but leadership ability only 7%. Demirtas et al26 also found that nurses’ knowledge and abilities increased due to simulation-based CPR instruction. Alaryani et al27 found that 63.8% had high self-efficacy (44.627%±58.397%). The highest domain of self-efficacy was responding and rescuing, while the lowest was debriefing and recording. We suggest encouraging pediatric nurses to undertake self-training on PBLS because that may improve self-evaluated confidence, as detected by Vestergaard et al.28
The current study showed that less than two-thirds of the studied nurses had negative attitudes about CPR. Total attitude scores increased significantly with postgraduate educational level, having attended training courses on PBLS and AED, being exposed to >10 cardiac arrest cases in the previous year, and having an advanced life-support license (P<0.05 for all). These results cohere with Ihunanya et al29 who revealed that more than half their respondents had negative attitudes about CPR. Likewise, Gebremedhn et al30 revealed that the overall attitude of nurses to performing CPR was poor; however, Majid et al31 found that a majority of nurses expressed positive attitudes toward CPR. Other contradictory finding was reported by Khatun et al,32 where among all respondents 70.62% had neutral, 15% positive, and 14.38% negative attitudes about performing CPR. Furthermore, Nasri and Bulushi4 reported that higher positive attitudes were found slightly more frequently among nurses with a diploma (63.2%) than a bachelor’s and above (46.4%) and that nurses who worked in public health-care institutions were found to have more positive attitudes (87.8%) than hospital nurses (43.8%). This study found a significant association between attitudes and validation of BLS certificate (P<0.001). Wati et al33 found a strong association between attitudes, subjective norms, and self-efficacy and intention.
Concerning stress, the current study revealed that about half the nurses had moderate stress-related CPR. Moreover, stress scores were significantly higher for female nurses, age 22–≤32 years, less experience than1–≤5 years, not having attending training courses on PBLS or AED, not being exposed to cardiac arrest cases in the previous year, and not having an advanced life-support license at (P<0.05 for all. Koželj et al19 reported that nurses are exposed to a certain amount of stress during resuscitation, but most of them manage to compensate for this effectively, associations between participants’ characteristics (ie, years of service in health care, sex, area of employment, the approximate number of resuscitations with/without physician supervision) and each of the five dimensions from the Post-Code Stress Scale. Hunziker et al34 showed that higher stress/overload was associated with less hands-on time and that a brief stress-coping strategy moderately decreased perceived stress.
On regression, attitudes and self-perceived abilities had high-frequency negative effects on stress scores. These results support Citolino et al,35 who found that a majority of nurses reported that stress of any member of staff (67.3%) had a negative effect on their own efficacy. Groombridge et al16 reported that human factors contributing to decision-making during resuscitation can be mitigated by tailored stress training and cognitive aids. Silverplats et al11 reported that there was a negative effect between nurses’ attitudes and their stress level. A strength of our study is that it was conducted in different departments at different hospitals and also relied on a large sample of nurses with different levels of education and different ages. Also, this study is considered one of the first in Egypt to deal with these concepts. Therefore, we recommend conducting more studies that address health staff’s awareness of their capabilities, not just their practices. A limitation of the study was that it was of quantitative design, not a combined quantitative and qualitative design.
Conclusion
Based on our findings, it was concluded that attitude scores increased and stress scores decreased significantly with postgraduate educational level, attendance at training courses on PBLS and AED, being exposed to >10 cardiac arrest cases in the previous year, and having an advanced life-support license (P<0.05). Also, positive attitudes and higher self-assessed abilities decreased nurses’ stress levels related to CPR.
Acknowledgment
The authors thank all the nurses who participated in this study for their contribution.
Funding
The authors received no financial support for the research, authorship, or publication of this article.
Disclosure
The authors declare no potential conflicts of interest concerning the research, authorship, or publication of this article.
References
1. Binkhorst M, Coopmans M, Draaisma JM, Bot P, Hogeveen M. Retention of knowledge and skills in pediatric basic life support amongst pediatricians. Eur J Pediatr. 2018;177(7):1089–1099. doi:10.1007/s00431-018-3161-7
2. Elsayed NM, EL-Dakhakhny AM, Albanna EA. Effect of an educational training program on improvement of pediatric nurses’ practice regarding cardiopulmonary resuscitation. Zagazig Nur J. 2019;15(1):61–78.
3. van den Bos-Boon A, Hekman S, Houmes RJ, et al. Effectiveness of simulation training and assessment of PICU nurses’ resuscitation skills: a mixed methods study from the Netherlands. J Pediatr Nurs. 2021;1(59):e52–60. doi:10.1016/j.pedn.2021.01.029
4. Nasri AA, Bulushi AA. Examining nurses’ theoretical knowledge, attitude, and practice of cardio-pulmonary resuscitation in hospitals and primary health care settings in south Sharqiyah, sultanate of Oman. Am J Nurs Res. 2020;8(5):577–587. doi:10.12691/ajnr-8-5-11
5. Sturny L, Regard S, Larribau R, et al. Differences in basic life support knowledge between junior medical students and lay people: web-based questionnaire study. J Med Internet Res. 2021;23(2):e25125. doi:10.2196/25125
6. Kaihula WT, Sawe HR, Runyon MS, Murray BL. Assessment of cardiopulmonary resuscitation knowledge and skills among healthcare providers at an urban tertiary referral hospital in Tanzania. BMC Health Serv Res. 2018;18(1):1–8. doi:10.1186/s12913-018-3725-2
7. Munezero JB, Atuhaire C, Groves S, Cumber SN. Assessment of nurses knowledge and skills following cardiopulmonary resuscitation training at mbarara regional referral hospital, Uganda. Pan Afr Med J. 2018. Jun 11;30:1.
8. Bush RN, Woodley L. Increasing nurses’ knowledge of and self-confidence with family presence during pediatric resuscitation. Crit Care Nurse. 2022;42(4):27–37. doi:10.4037/ccn2022898
9. van den Bos-Boon A, van Dijk M, Adema J, Gischler S, van der Starre C. Professional assessment tool for team improvement: an assessment tool for paediatric intensive care unit nurses’ technical and nontechnical skills. Aust Crit Care. 2022;35(2):159–166. doi:10.1016/j.aucc.2021.03.002
10. Magid KH, Ranney ML, Risica PM. Using the theory of planned behavior to understand intentions to perform bystander CPR among college students. J Am Coll Health. 2021;69(1):47–52. doi:10.1080/07448481.2019.1651729
11. Silverplats J, Strömsöe A, Äng B, Södersved Källestedt ML. Attitudes towards cardiopulmonary resuscitation situations and associations with potential influencing factors—A survey among in-hospital healthcare professionals. PLoS One. 2022;17(7):e0271686. doi:10.1371/journal.pone.0271686
12. Kuchaki Z, Taheri M, Esfahani H, Erfanifam T. The effect of CPR educational package on knowledge and performance of nurses working in intensive care units: a review study. J Family Med Prim Care. 2022;11(5):1677–1682. doi:10.4103/jfmpc.jfmpc_1938_21
13. Abolfotouh MA, Alnasser MA, Berhanu AN, Al-Turaif DA, Alfayez AI. Impact of basic life-support training on the attitudes of health-care workers toward cardiopulmonary resuscitation and defibrillation. BMC Health Serv Res. 2017;17(1):1. doi:10.1186/s12913-017-2621-5
14. Toida C, Morimura N. An analysis of stress concerning pediatric emergency care nurses. Cureus. 2022;14(1). doi:10.7759/cureus.21299
15. Suresh P, Matthews A, Coyne I. Stress and stressors in the clinical environment: a comparative study of fourth‐year student nurses and newly qualified general nurses in Ireland. J Clin Nurs. 2013;22(5–6):770–779. doi:10.1111/j.1365-2702.2012.04145.x
16. Groombridge CJ, Kim Y, Maini A, Fitzgerald MC, Fitzgerald MC. Stress and decision-making in resuscitation: a systematic review. Resuscitation. 2019;1(144):115–122. doi:10.1016/j.resuscitation.2019.09.023
17. Bahig Anwr AklR G, Mahmoud Saadoon M, Ahmed Sayed Z. (2021) Pediatrics basic life support simulation training: intern-ship nursing students’ performance and self-efficacy. Egypt J Health Care. 2021;12(1):383–403. doi:10.21608/ejhc.2021.141881
18. Ha Z, Sm S. Assessment of basic life support knowledge among nursing professionals. Egypt J Occup Med. 2020;44(1):455–470. doi:10.21608/ejom.2020.67630
19. Koželj A, Šikić Pogačar M, Fijan S, Strauss M, Poštuvan V, Strnad M. Exploring the Feelings of Nurses during Resuscitation—A Cross-Sectional Study. In: Healthcare. MDPI; 2021:5.
20. Hassanein SM, Tantawi HR, Sadek BN, Hendy A, Awad HA. Impact of structured simulation-based and on-job training program on nurses’ competency in pediatric peripheral intravenous cannulation: children’s hospital experience. Nurse Educ Today. 2021;98:104776. doi:10.1016/j.nedt.2021.104776
21. Hendy A, Abozeid A, Sallam G, Abboud Abdel Fattah H, Ahmed Abdelkader Reshia F. Predictive factors affecting stress among nurses providing care at COVID‐19 isolation hospitals at Egypt. Nursing Open. 2021;8(1):498–505. doi:10.1002/nop2.652
22. Bragard I, Seghaye MC, Farhat N, et al. Implementation of a 2-day simulation-based course to prepare medical graduates on their first year of residency. Pediatr Emerg Care. 2018;34(12):857–861. doi:10.1097/PEC.0000000000000930
23. Łoś K, Chmielewski J, Cebula G, Bielecki T, Torres K, Łuczyński W. Relationship between mindfulness, stress, and performance in medical students in pediatric emergency simulations. GMS J Medical Educ. 2021;38:4.
24. Chandrasekaran S, Kumar S, Bhat SA, Shabbir PM, Chandrasekaran VP, Chandrasekaran VP. Awareness of basic life support among medical, dental, nursing students and doctors. Indian J Anaesth. 2010;54(2):121. doi:10.4103/0019-5049.63650
25. Silverplats J, Källestedt ML, Wagner P, Ravn-Fischer A, Äng B, Strömsöe A. Theoretical knowledge and self-assessed ability to perform cardiopulmonary resuscitation: a survey among 3044 healthcare professionals in Sweden. Eur J Emerg Med. 2020;27(5):368. doi:10.1097/MEJ.0000000000000692
26. Demirtas A, Guvenc G, Aslan Ö, Unver V, Basak T, Kaya C. Effectiveness of simulation-based cardiopulmonary resuscitation training programs on fourth-year nursing students. Australas Emerg Care. 2021;24(1):4–10. doi:10.1016/j.auec.2020.08.005
27. Alaryani ZD, Alhofaian A, Elhady M. The relationship between knowledge and self-efficacy of nurses regarding early initiation of cardiopulmonary resuscitation and automated defibrillation in Saudi Arabia. Belitung Nurs J. 2021;7(5):387–394.
28. Vestergaard LD, Løfgren B, Jessen CL, et al. A comparison of pediatric basic life support self-led and instructor-led training among nurses. Eur J Emerg Med. 2017;24(1):60–66. doi:10.1097/MEJ.0000000000000294
29. Ihunanya OM, Oke Michael RN, Babcock BN, Amere LT, Rphn B. Knowledge, attitude and practice of cardiopulmonary resuscitation among nurses in Babcock university teaching hospital in Ilishan-Remo, Ogun State, Nigeria. Int J Caring Sci. 2020;13(3):1773–1782.
30. Gebremedhn EG, Gebregergs GB, Anderson BB, Nagaratnam V. Attitude and skill levels of graduate health professionals in performing cardiopulmonary resuscitation. Adv Med Educ Pract. 2017;8:43. doi:10.2147/AMEP.S114726
31. Majid S, Foo S, Luyt B, et al. Adopting evidence-based practice in clinical decision making: nurses’ perceptions, knowledge, and barriers. J Med Libr Assoc. 2011;99(3):229. doi:10.3163/1536-5050.99.3.010
32. Khatun R, Chowdhury S, Goni O. Knowledge and attitudes towards cardiopulmonary resuscitation: a cross sectional survey on health care providers in clinical practice. Health Sci Q. 2021;1(3):87–93. doi:10.26900/hsq.1.3.01
33. Wati SG, Wihastuti TA, Nasution TH. Application of the theory of planned behavior to identify nursing student’s intention to be a bystander cardiopulmonary resuscitation. Nurs J. 2021;6(1):23–30. doi:10.19184/nlj.v6i1.19228
34. Hunziker S, Pagani S, Fasler K, Tschan F, Semmer NK, Marsch S. Impact of a stress coping strategy on perceived stress levels and performance during a simulated cardiopulmonary resuscitation: a randomized controlled trial. BMC Emerg Med. 2013;13(1):1–9. doi:10.1186/1471-227X-13-8
35. CitolinoCM, Santos ES, Silva RD, Nogueira LD. Factors affecting the quality of cardiopulmonary resuscitation in inpatient units: perception of nurses. Rev Esc Enferm USP. 2015;49:907–913. doi:10.1590/S0080-623420150000600005
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.