Back to Journals » Vascular Health and Risk Management » Volume 21
Selenium and Lead Exposure are Associated with Elevated Blood Pressure in Individuals with Undiagnosed Hypertension: Findings from NHANES 2013–2020
Authors Tang L ![]() , Li X, Wang Y, He Y
, Li X, Wang Y, He Y ![]()
Received 8 July 2025
Accepted for publication 9 December 2025
Published 16 December 2025 Volume 2025:21 Pages 1093—1106
DOI https://doi.org/10.2147/VHRM.S552304
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Li Tang,1,* Xue Li,2,* Yeyuan Wang,3 Yulei He4
1Department of Healthcare, Chengdu Women’s and Children’s Central Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 2Department of Pediatric Critical Care Medicine, Chengdu Women’s and Children’s Central Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 3Chengdu Shuangliu Yixin Sub-district Community Health Service Center, Chengdu, People’s Republic of China; 4Health Management Center, Chengdu Women’s and Children’s Central Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yulei He, Health Management Center, Chengdu Women’s and Children’s Central Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, 611731, People’s Republic of China, Email [email protected]
Purpose: Prior studies on the relationship between metal exposure and blood pressure have reported inconsistent findings, potentially due to the inclusion of individuals receiving hypertension treatment. This study assessed the association between blood concentrations of selenium (Se), lead (Pb), total mercury (Hg), cadmium (Cd), and manganese (Mn) and elevated blood pressure in US adults aged 20– 60 years without a prior hypertension diagnosis. We also explored the moderating effects of age, gender and body mass index (BMI), and the mediating role of non-high-density lipoprotein cholesterol (non-HDL-C).
Methods: Data from the 2013– 2020 National Health and Nutrition Examination Survey were analyzed. Weighted logistic regression model were used to estimate odds ratios (ORs) and 95% confidence intervals (CIs), with subgroup analyses assessing effect modification. Structural equation modelling was employed to evaluated the potential mediating effects of non-HDL-C.
Results: Among 6026 participants, 1,569 had elevated blood pressure. Adjusted analyses showed significant associations between Se and Pb and increased hypertension odds. Each 1 μg/L increase in Se corresponded to a 1% rise in odds (OR: 1.01, 95% CI: 1.00, 1.01), with those in the highest Se quintiles (Q4 and Q5) having 49% (95% CI: 1.01– 2.21) and 52% (95% CI: 1.01– 2.27) greater odds, respectively. A unit increase in log-transformed Pb was associated with a 36% increase in odds (95% CI: 1.09– 1.71), with the highest Pb quintile showing nearly double the risk (OR: 1.94; 95% CI: 1.22– 3.07). BMI significantly moderated the association with Se and Pb, albeit in different ways. Non-HDL-C mediated 36.82% of Se’s and 30.80% of Pb’s total effect on elevated blood pressure (p< 0.05).
Conclusion: In US adults without diagnosed hypertension, higher blood Se and Pb concentrations were associated with elevated blood pressure, with BMI modifying and non-HDL-C potentially and partially mediating these associations. These findings highlight the need for targeted public health strategies to limit environmental metal exposure and suggest that monitoring non-HDL-C levels in conjunction with individual metabolic profiles may support early cardiovascular risk assessment and timely intervention.
Keywords: metal exposure, blood pressure, cross-sectional study, mediation analysis
Introduction
Hypertension remains one of the most pressing global public health concerns, currently affecting over 1.3 billion individuals worldwide.1 As a major modifiable risk factor, hypertension contributes substantially to the global burden of cardiovascular disease, including ischemic heart disease, stroke, heart failure, and chronic kidney disease, ultimately leading to increased premature mortality.2 With demographic shifts such as population aging and the rising prevalence of obesity, the global prevalence of hypertension is projected to escalate, potentially affecting nearly 60% of adults by 2050.3 This underscores the urgent need for improved preventive strategies and more effective management approaches to mitigate its impact on vascular health.
While traditional lifestyle-related risk factors, such as high dietary sodium intake, tobacco use, and physical inactivity, are well-established contributors to hypertension,4,5 increasing attention has turned to environmental exposures, including heavy and trace metals, as emerging yet under-recognized determinants of blood pressure regulation. Exposure to toxic metals such as lead (Pb), cadmium (Cd), and mercury (Hg) has been associated with oxidative stress, endothelial dysfunction, and vascular inflammation, mechanisms that may contribute to elevated blood pressure and impaired cardiovascular function.6,7 In contrast, essential trace elements such as selenium (Se) and manganese (Mn) are required for antioxidant defense and other physiological processes; however, their narrow safety margins mean that both deficiency and excess may have detrimental health effects, including potential links to hypertension.8–11
Environmental metal exposure arises from various sources, including industrial emissions, agricultural practices, contaminated food and water supplies, and natural deposits, resulting in widespread human exposure through inhalation, ingestion, and dermal absorption.12 Blood concentrations of metals are commonly used as biomarkers of exposure and may offer insights into potential health risks.13 However, epidemiologic studies investigating associations between blood metal concentrations and hypertension have yielded inconsistent findings. For instance, while some studies suggest a positive association between Cd exposure and elevated blood pressure,14 others find no significant relationship.15,16 Similarly, conflicting evidence surrounds the role of Se in blood pressure regulation, with some reports indicating a protective effect17 and others suggesting a potential hypertensive risk at higher concentrations.18,19
In recent years, several studies using nationally representative survey data have further examined the cardiovascular implications of heavy metal exposure. For example, analysis of NHANES 2011–2016 identified exposure patterns of seven metals and revealed that certain metal profiles were associated with higher odds of hypertension and adverse cardiovascular outcomes.20 Chen et al demonstrated positive associations between blood Pb and Cd levels and resistant hypertension using NHANES 1999–2018.21 Beyond US populations, Kim et al reported that combined exposure to Pb, Hg, and Cd in the Korean National Health and Nutrition Examination Survey (KNHANES) was associated with a higher prevalence of hypertension compared with single-metal exposure.22 However, much of the existing literature includes participants with previously diagnosed hypertension who may be receiving pharmacologic treatment or making lifestyle modification. Antihypertensive medications and treatment-related lifestyle changes can influence both circulating metal concentrations and blood pressure, potentially introducing confounding effects. Therefore, studies focusing on individuals without a prior diagnosis may provide a clearer insight into the early pathophysiological mechanisms linking metal exposure and elevated blood pressure, before clinical interventions alters these relationships.
Moreover, recent research suggests that the associations between metal exposure and hypertension may be influenced by complex interactions or mediating pathways. For instance, elevated Se levels have been linked to increased non–high-density lipoprotein cholesterol (non–HDL-C),23 a recognized vascular risk factor independently associated with hypertension.24,25 These findings raise the possibility that lipid metabolism may mediate or modify the effects of metal exposure on vascular health, although direct clinical evidence remains limited. Understanding these mechanisms in undiagnosed individuals may help identify early risk patterns before the onset of overt disease.
To address these knowledge gaps, the present cross-sectional study aimed to: i) investigate the associations between blood concentrations of Se, Pb, total Hg, Cd, and Mn and elevated blood pressure in adults aged 20 to 60 years with no previous diagnosis of hypertension; ii) assess potential effect modifications by key demographic and health-related factors, including age, sex, and body mass index (BMI); and iii) explore whether non-HDL-C mediates the relationship between blood metal concentrations and increased blood pressure. By focusing on a relatively young and undiagnosed adult population, this study aims to elucidate early risk patterns and inform preventive strategies for vascular health management.
Material and Methods
Study Population
This study employed data from the National Health and Nutrition Examination Survey (NHANES), a nationally representative cross-sectional survey conducted by the National Center for Health Statistics (NCHS) among the civilian, noninstitutionalized US population. Ethical approval for the original survey was granted by the NCHS Ethics Review Board, and all participants provided informed consent. As our study used publicly available, de-identified NHANES data, the Ethics Committee of Chengdu Women’s and Children’s Central Hospital confirmed that no additional ethical approval was required. In accordance with national legislation guidelines (item 1 and 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects, February 18, 2023, China), this research is exempt from ethics review.
We retrieved three consecutive cycles of publicly available data from the NHANES database: 2013–2014, 2015–2016, and 2017–2020. NHANES collects a comprehensive range of information, including demographic data, physical examinations, laboratory results, and questionnaire responses on participants’ lifestyle, diet and health. In the present study, participants aged 20–60 years with no previous diagnosis of hypertension were included in the analysis. A previous diagnosis of hypertension was defined as either a self-reported physician-diagnosed condition or the use of antihypertensive medications. Participants with missing data on whole blood metal exposures were excluded. Whole blood Se and Mn measurements were first available in the 2011–2012 cycle; however, alcohol consumption data (a covariate) from that cycle were restricted to the NCHS Research Data Center. Therefore, we initiated the analysis with data from the 2013–2014 cycle. In addition, data from 2021–2023 were not included due to the limited availability of physical activity data (a covariate), which was confined to leisure-time activities. After excluding participants with missing outcome data or those who were pregnant, the final sample size was 6,024 (Figure 1).
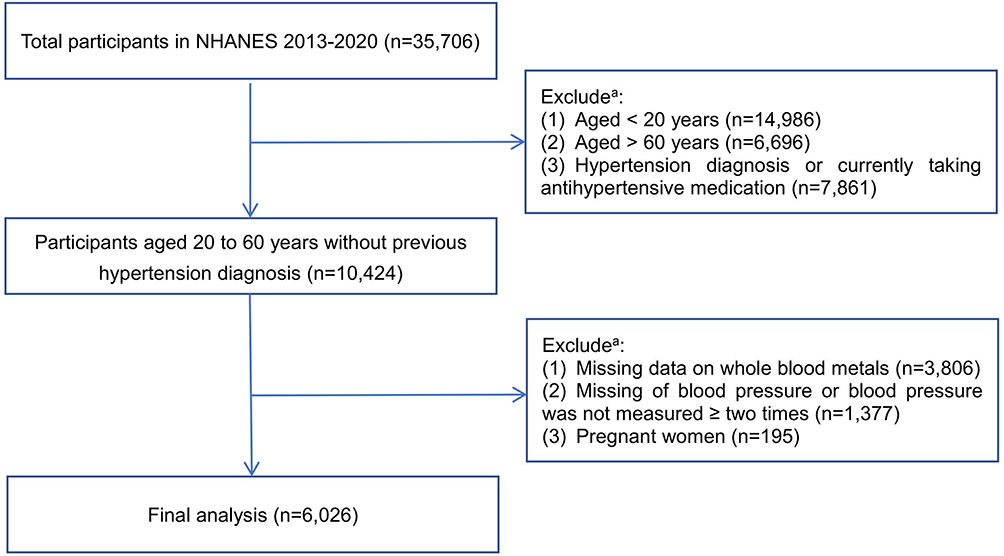 |
Figure 1 Flow chart for participant inclusion and exclusion. aThe exclusion categories are not mutually exclusive; therefore, the numbers listed under exclusions do not sum to the total excluded participants. |
Exposure
The exposure variables in this study were the levels of heavy metal in whole blood. Whole blood samples were processed, stored, and shipped to the National Center for Environmental Health for testing. Concentrations of Se, Pb, Cd, total Hg, and Mn were quantified using inductively coupled plasma mass spectrometry (ICP-MS). The lower limits of detection for Se, Pb, Cd, total Hg, and Mn were 24.48 μg/L, 0.07 μg/dL, 0.10 μg/L, 0.28 μg/L, and 0.99 μg/L, respectively. For any results below the lower limit of detection, the corresponding value was assigned as the detection limit divided by the square root of two. Further details can be found in the NHANES Laboratory Procedures Manual.26
Outcome
Blood pressure measurements were conducted in mobile examination centers (MECs) by trained physicians following a standard protocol.27 All measurements were obtained during a single examination visit. Participants were instructed to rest quietly in a seated position for five minutes before the measurements. Three consecutive brachial blood pressure readings (systolic and diastolic) were recorded, with a fourth measurement taken if any reading was incomplete or interrupted. The final blood pressure values were determined using the average of up to three valid systolic and diastolic readings. Participants with only one recorded blood pressure reading or no recorded readings were excluded from the analysis. In accordance with the 2025 American College of Cardiology/American Heart Association (ACC/AHA) Hypertension Guideline, increased blood pressure was defined as a systolic blood pressure ≥ 130 mmHg or a diastolic blood pressure ≥ 80 mmHg in adults.28
Other Variables
We also retrieved variables on sociodemographic and lifestyle data, anthropometric measurement, and laboratory results that might be associated with elevated blood pressures. Sociodemographic and lifestyle data were collected through standardized household interviews using structured questionnaires. These included age (years, 20–40, 41–60), gender (male, female), ethnicity (Hispanic, non-Hispanic White, non-Hispanic Black, other), education level (less than high school, high school or equivalent, some college or higher), smoking status (current, former, never), alcohol consumption (yes, no), dietary sodium intake (mg/day, <2300, ≥2300), and physical activity (MET-min/wk, <500, ≥500).
Smoking status was categorized based on responses to two questions from the smoking questionnaire: “Have you smoked at least 100 cigarettes in your entire life?” and “Do you now smoke cigarettes?” Participants who answered affirmatively to both questions were classified as current smokers. Alcohol consumption was defined as self-reported intake of alcoholic beverages on at least 12 occasions in the previous year. Dietary sodium intake was assessed through the initial 24-hour dietary recall interview, conducted by trained interviewers at the MEC. Participants were provided with a measurement guide to aid in the accurate reporting of food quantities. A daily sodium intake of 2,300 mg or more was classified as high sodium intake in this study.29 Physical activity was classified into three groups: vigorous work-related or leisure-time activities, moderate work-related or leisure-time activities, and walking or bicycling for transportation. Metabolic Equivalent of Task (MET) values were assigned based on NHANES guidelines, with MET scores set at 8.0 for vigorous activities, and 4.0 for both moderate activities and transportation-related walking or bicycling. To calculate MET-min/wk, the MET score for each activity was multiplied by the number of days per week and the daily duration for each activity (ie MET-min/wk = MET score × days × duration). Physical inactivity was defined as less than 500 MET-min/wk.30
Body mass index (BMI), an anthropometric index, was determined as weight (kg) divided by height squared (kg/m2). BMI classifications were as follows: underweight (< 18.5), normal weight (18.5–24.9), overweight (25.0–29.9) and obesity (≥ 30.0). Laboratory results, including SUA, non-HDL-C and HbA1c were also included in the analysis. Normal SUA level was defined as 3.4–7.0 mg/dL in men and 2.5–6.0 mg/dL in women.31 Non-HDL-C was calculated by subtracting HDL-C from total cholesterol, with a value of at least 155 mg/dL considered unhealthy.32 An HbA1c level of 6.5% or higher was classified as indicative of elevated blood glucose levels over the past three months.33
Statistical Analysis
Statistical analyses were conducted using Stata SE software, version 16.0 (StataCorp LLC). Continuous variables with a normal distribution were summarized as means with standard deviations (SDs), while non-normally distributed variables were presented as medians with interquartile ranges (IQRs). Categorical variables were expressed as frequencies and percentages. To compare sample characteristics and blood metal concentrations between groups with normal and elevated blood pressure, either the Student’s t-test (for normally distributed variables) or the Mann–Whitney U-test (for non-normally distributed variables) was used. Pearson’s χ2-test was applied for categorical variables. For blood metal levels that were not normally distributed, values were natural log-transformed to approximate a normal distribution.
Weighted logistic regression models were employed to explore the associations of each blood metal (both continuous and quintiles) with increased blood pressure. Model 1 was unadjusted. Model 2 was adjusted for age, gender and ethnicity. Model 3 was adjusted for age, gender, ethnicity, education level, smoking status, alcohol consumption, BMI categories, high sodium intake, physical inactivity, healthy non-HDL-C, normal SUA and elevated HbA1c. Subgroup analyses were conducted to examine whether the correlation between blood metal concentrations and increased blood pressure was modified by gender (male, female), age groups (20–40, 41–60), and BMI categories (<25 kg/m2, 25–29.9 kg/m2, ≥ 30.0 kg/m2). Parallel mediation analysis was performed using structural equation modelling (SEM) with logit function to assess the potential mediating effects of non-HDL-C in the relationship between individual blood metal concentrations (Se and natural log-transformed Pb) and increased blood pressure. The 95% confidence intervals (CIs) for the mediation estimates were based on nonparametric bias-corrected bootstrapping with 1000 resamples. All SEM models were adjusted for age, gender, ethnicity, education level, smoking status, alcohol consumption, BMI categories, high sodium intake, physical inactivity, normal SUA and elevated HbA1c. A mediation effect by the non-HDL-C level was considered statistically significant when the p value for the indirect effect was <0.05. Mediation analysis assumes that the exposure precedes or influences the mediator, the mediator influences the outcome, and there is no unmeasured confounding of the exposure-mediator or mediator-outcome associations. Although causal direction cannot be definitively established in our cross-sectional data, the analytic framework used here is supported by biological pathways linking metal exposure to lipid metabolism and subsequent blood pressure changes.34,35
Results
Characteristics of Participants
The characteristics of the study participants, stratified by blood pressure status, are summarized in Table 1. Among the 6,026 participants without a previous hypertension diagnosis, 3,273 (26.04%) exhibited elevated blood pressure. Compared to those with normal blood pressure, participants with elevated blood pressures were more likely to be older, male, and non-Hispanic Black (p<0.001). They were also more likely to be current or former smokers, obese, physical inactive, and to exhibit unhealthy non-HDL-C levels, abnormal SUA levels, and higher HbA1c levels (p<0.05). Furthermore, significant differences in blood metal concentrations of Se, Pb, and Cd were observed between the two blood pressure groups (p < 0.05).
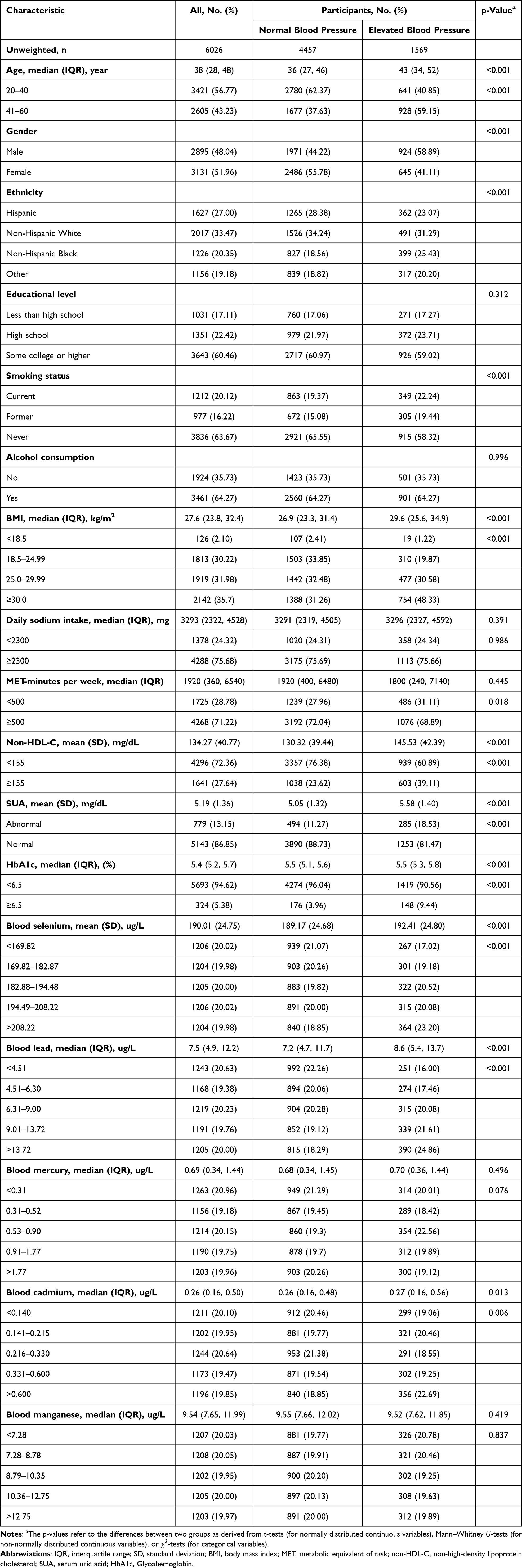 |
Table 1 Characteristics of the Study Participants by Hypertension Status |
Association Between Blood Metal Concentrations and Elevated Blood Pressure
Table 2 presents the results of three weighted logistic regression models examining the relationship between blood metal concentrations and elevated blood pressure. In the unadjusted model (Model 1), Se (both as a continuous variable and in quintiles), and Pb (both as a natural logarithm-transformed continuous variable and in quintiles) were associated with higher blood pressure. After adjusting for age, gender, and ethnicity in Model 2, Se (both continuous and quintiles) and Pb in quintiles remained statistically significant. In the fully adjusted Model 3, which accounted for age, gender, ethnicity, education level, smoking status, alcohol consumption, BMI, high sodium intake, physical inactivity, non-HDL-C, SUA, and HbA1c, Se and Pb continued to show significant associations with an increased risk of elevated blood pressure. Specifically, each 1 μg/L increase in Se concentration was associated with a 1% increase in the odds of elevated blood pressure (OR: 1.01, 95% CI: 1.00, 1.01). Compared with the lowest quintile (Q1) of Se, participants in the fourth (Q4) and fifth (Q5) quintiles had 1.49-fold (95% CI: 1.01, 2.21) and 1.52-fold (95% CI: 1.01, 2.27) higher odds of elevated blood pressure, respectively. Similarly, each one-unit increase in the natural logarithm of Pb concentration was associated with a 1.36-fold increase in the odds of elevated blood pressure (95% CI: 1.09, 1.71), with Q5 Pb levels nearly doubling the odds compared to Q1 (OR: 1.94, 95% CI: 1.22, 3.07). No significant associations were found for total Hg, Cd, or Mn (p>0.05).
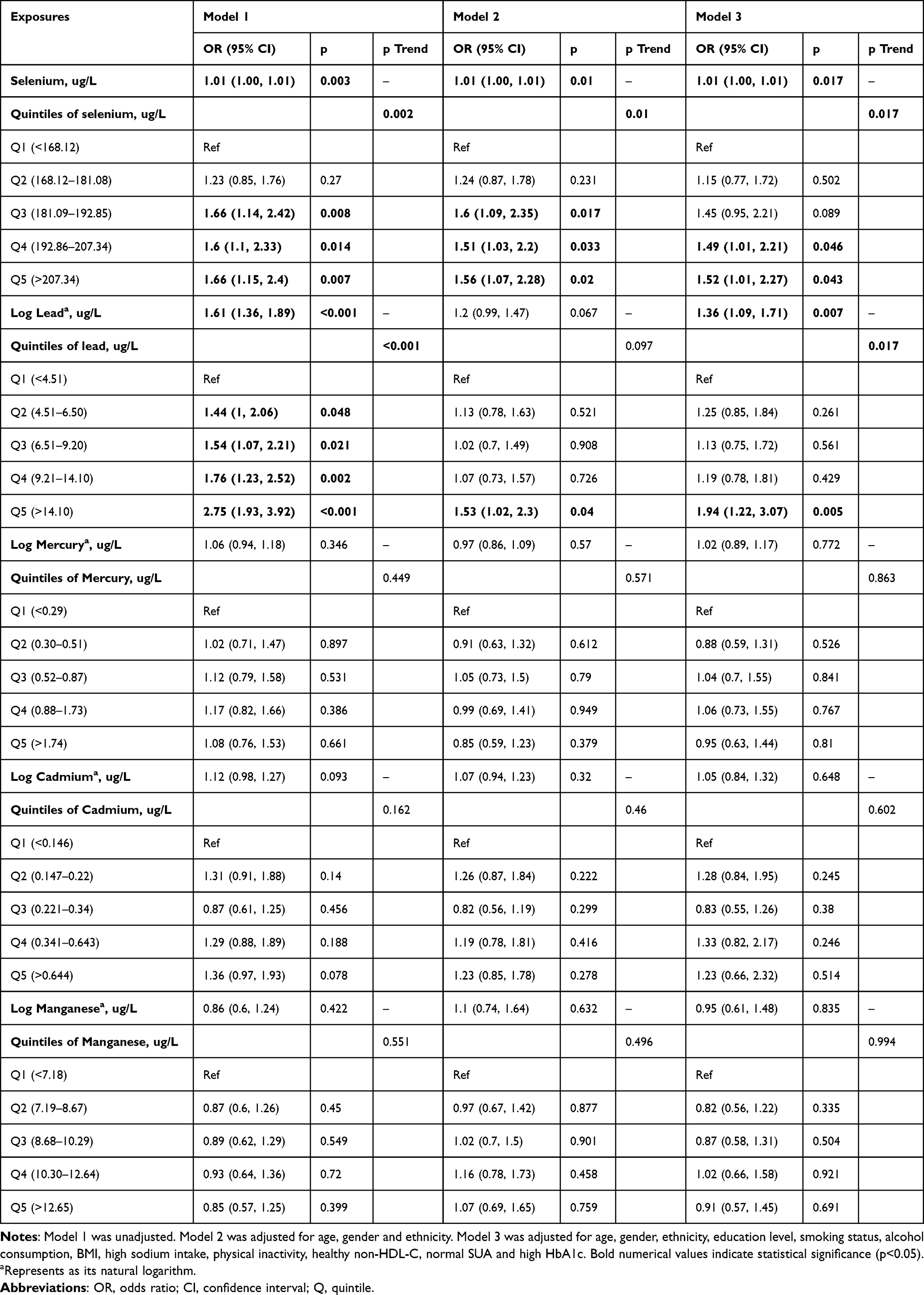 |
Table 2 The Association Between Blood Metals and Higher Blood Pressure |
Subgroup Analysis Stratified by Gender, Age and BMI
Figure 2 illustrates the associations between Se and Pb concentrations with elevated blood pressure in different subgroups, adjusted for all confounding variables in Model 3. Se concentrations, analyzed as a continuous variable (Figure 2A), were significantly associated with higher blood pressure in participants with a BMI ≥ 30.0 kg/m2 (p=0.022). In contrast, Pb concentrations, assessed as natural log-transformed continuous variable (Figure 2B), showed a significant association with elevated blood pressure among those with a BMI < 25.0 kg/m2 (p<0.01). When Se concentrations were categorized into quintiles, no significant association with elevated blood pressure was observed (Figure 2C). However, the quintile-based analysis of Pb concentrations (Figure 2D) revealed statistically significant associations among participants with a BMI < 30.0 kg/m2 (p=0.007). No significant interaction effect was observed for gender or age in the associations between blood metal concentrations with blood pressure.
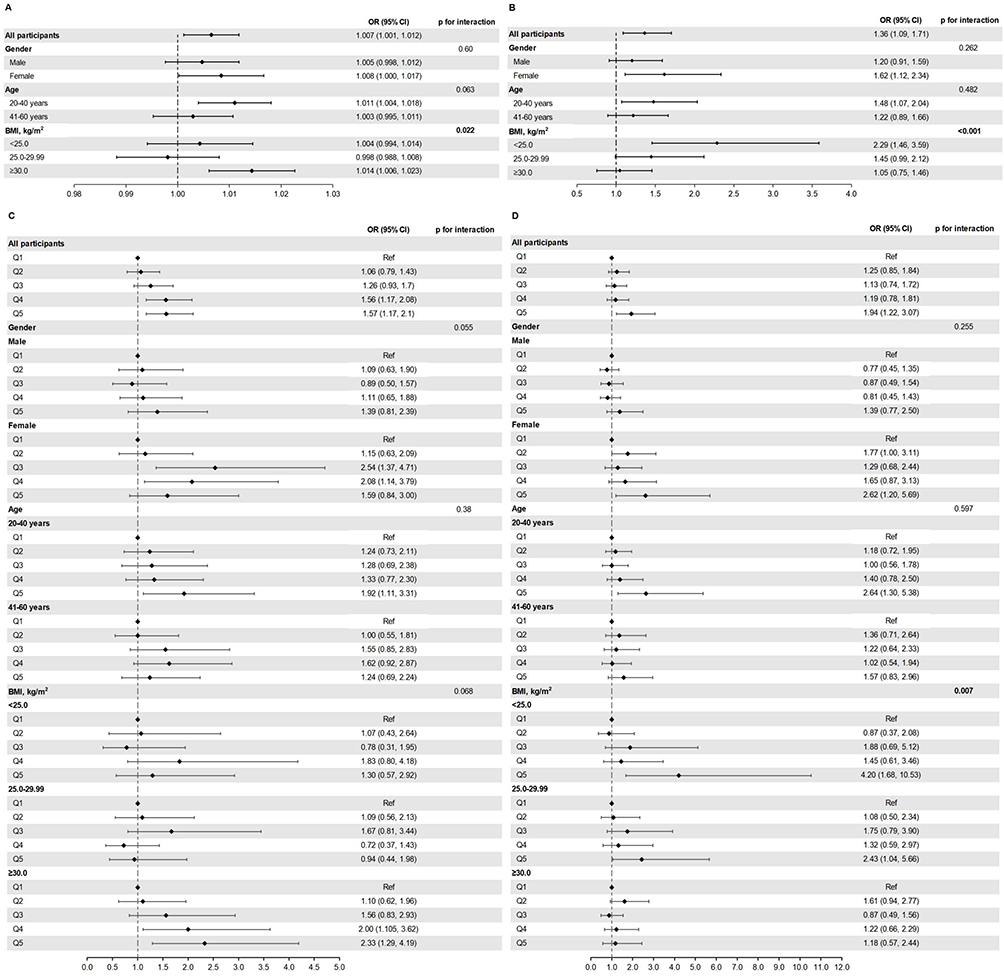 |
Figure 2 Subgroup analyses of blood Se and Pb associated with higher blood pressure stratified by gender, age and BMI. (A) Blood Se (continuous) and higher blood pressure. (B) Blood Pb (continuous in natural log-transformed) and higher blood pressure. (C) Blood Se (quintiles) and higher blood pressure. (D) Blood Pb (quintiles) and higher blood pressure. Notes: Models were adjusted for age, gender, ethnicity, education level, smoking status, alcohol consumption, BMI, high sodium intake, physical inactivity, healthy non-HDL-C, normal serum uric acid (SUA), and high HbA1c. Bold numerical values indicate statistical significance (p<0.05). |
Mediating Role of Non-HDL-C
As shown in Figure 3, non-HDL-C significantly mediated the relationship between Se and Pb concentrations and elevated blood pressure, with mediation effect accounted for 36.82% of the association for Se (Figure 3A) and 30.80% for Pb (Figure 3B) (p<0.05).
 |
Figure 3 Mediation of the associations between blood Se and Pb with higher blood pressure through non-HDL-C. (A) Mediation of non-HDL-C in the association between blood Se and higher blood pressure. (B) Mediation of non-HDL-C in the association between blood Pb (natural log-transformed) and higher blood pressure. Abbreviations: IE, indirect effect estimate; DE, direct effect estimate. Notes: Models were adjusted for age, gender, ethnicity, education level, smoking status, alcohol consumption, BMI, high sodium intake, physical inactivity, normal serum uric acid (SUA), and high HbA1c. Proportion of mediation=IE/ (DE+IE). |
Discussion
In this cross-sectional study of US adults aged 20–60 years without previously diagnosed hypertension, we identified significant associations between blood concentrations of Se and Pb and elevated blood pressure, independent of key demographic, lifestyle, and metabolic variables. Moreover, non-HDL-C significantly mediated these relationships, suggesting a potential mechanistic link between metal exposure and hypertension risk. Subgroup analyses further revealed BMI-dependent variations, highlighting the complex interaction between metal exposure, metabolic health, and blood pressure regulation. Our findings are consistent with previous research demonstrating positive associations between heavy metal exposure and hypertension, including studies using NHANES and KNHANES data.20–22 Importantly, our study extends the literature by focusing on individuals without a prior hypertension diagnosis and by exploring lipid-related pathways that may underlie these associations.
Our findings are also aligned with prior research indicating that even low-level lead exposure may contribute to elevated blood pressure and increased hypertension risk.36,37 In recognition of its toxicity, the US Centers of Disease Control and Prevention (CDC) has lowered the blood lead reference value from 5 µg/dL to 3.5 µg/dL.38 In our study, the median blood Pb concentration was 7.5 µg/L, and Pb concentrations exceeding 14.1 µg/L were associated with elevated blood pressure. These levels are well below the current CDC reference threshold, reinforcing the growing consensus that no level of lead exposure is entirely safe. Given Pb’s widespread environmental persistence and ability to bioaccumulate, these findings highlight the continued importance of public health efforts aimed at minimizing exposure, even at levels previously considered to be of limited concern.
An important and novel observation of our study is the potential mediating role of non-HDL-C in the association between Pb and elevated blood pressure. Non-HDL-C includes all atherogenic lipoproteins and is a well-established marker of cardiovascular risk.39 In addition to disrupting nitric oxide production and inducing oxidative stress,40 Pb exposure has been shown to disrupt lipid metabolism,34 leading to increased levels of pro-atherogenic lipoproteins, such as very low-density lipoprotein (VLDL) and low-density lipoprotein (LDL). These pro-atherogenic lipoproteins contribute to vascular inflammation, endothelial dysfunction, and LDL oxidation, mechanisms central to the development of hypertension.35 The elevation of non-HDL-C may further potentiate these effects, serving as a pathophysiologic bridge between environmental metal exposure and vascular dysfunction. While causal pathways cannot be conclusively established in a cross-sectional design, these findings suggest that non-HDL-C may help identify individuals at heightened cardiovascular risk due to Pb exposure and could represent a potential target for future intervention studies.
Se, an essential trace element with antioxidant and thyroid-regulatory functions,9, also demonstrated a positive association with elevated blood pressure in our study. The literature on Se and hypertension remains inconclusive, with some studies reporting protective effects, while others suggest increased risk at higher Se concentrations.17–19 By focusing on individuals without prior hypertension diagnosis or treatment, our study helps clarify these inconsistencies and suggests that higher Se concentrations may contribute to elevated blood pressure in the early stages of disease. As with Pb, our mediation analysis implicates that non-HDL-C may be an intermediary in this association, pointing to disrupted lipid metabolism as a shared mechanistic pathway. Nevertheless, these potential pathways should be interpreted cautiously due to the absence of temporal information.
Our mediation analysis indicated that non-HDL-C explained 36.82% and 69.20% of the total associations between Se and Pb, respectively, and elevated blood pressure. However, given the cross-sectional nature of our data, these results should be viewed as exploratory and hypothesis-generating rather than evidence of definitive causal mediation. Interestingly, BMI appeared to modify these associations in distinct ways. The association between Se and blood pressure was more pronounced among individuals with obesity, potentially reflecting a synergistic effect of lipid dysregulation and oxidative stress in this subgroup.41 These findings suggest that weight management and balanced nutrient intake, including careful monitoring of Se supplementation, may be particularly important for reducing hypertension risk in obese individuals. In contrast, the stronger association between Pb and blood pressure among individuals with BMI <30 suggests that other mechanisms, such as endothelial dysfunction, calcium channel interference, and oxidative damage, may predominate in leaner populations.40 This finding highlights the need for universal strategies to reduce Pb exposure, regardless of body weight, as well as personalized interventions targeting population subgroups based on their metabolic profiles.
Previous studies have hypothesized that women may be more vulnerable to metal-induced cardiovascular effects due to hormonal changes, such as Pb-induced reductions in serum estradiol,42 or due to differences in body composition and fat distribution affecting metal bioaccumulation. Similarly, younger adults may face increased exposure risks from occupational or consumer product sources. Nonetheless, our findings suggest that neither gender nor age significantly modifies the associations between metal exposure and blood pressure, though future studies with larger sample sizes may be better powered to detect subtle effect modifications.
This study has several strengths, including the use of a large, nationally representative sample and the novel focus on individuals with undiagnosed and untreated hypertension, a group less likely to be affected by confounding from medication or behavior change. In addition, we performed comprehensive statistical adjustments and explored both mediation and interaction effects. However, several limitations should be acknowledged. First, the cross-sectional design precludes causal inference, and longitudinal studies are needed to establish temporality. Second, blood metal concentrations, while useful biomarkers of exposure, may not fully capture long-term or cumulative exposure. Third, potential residual confounding cannot be ruled out, as unmeasured factors such as genetic susceptibility, dietary patterns, and environmental co-exposures may influence the observed associations. Finally, while non-HDL-C was identified as a mediator, other potential pathways, such as oxidative stress, warrant further investigation.
Conclusion
Our findings demonstrate that, among adults with undiagnosed hypertension, elevated blood concentrations of Se and Pb were independently associated with an increased risk of hypertension, with non-HDL-C suggesting a potential mediating pathway. However, no significant associations were observed for total Hg, Cd, or Mn. Subgroup analyses revealed that these associations varied by BMI. Higher Se concentrations were significantly associated with elevated blood pressure among individuals with obesity (BMI ≥30.0 kg/m2), whereas increased Pb concentrations were more strongly linked to blood pressure elevation in individuals with BMI <30.0 kg/m2. These findings underscore the importance of considering individual metabolic profiles when evaluating cardiovascular risks related to metal exposure. Targeted public health strategies aimed at reducing environmental metal exposure, particularly in high-risk subgroups, may offer opportunities for early intervention in the prevention of hypertension. However, given the cross-sectional design, causal interpretations cannot be confirmed, and the mediation findings should be considered exploratory. Longitudinal studies and mechanistic investigations are warranted to further clarify these associations and identify potential interventions to reduce metal-induced cardiovascular harm.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Mills KT, Bundy JD, Kelly TN, et al. Global Disparities of Hypertension Prevalence and Control: a Systematic Analysis of Population-Based Studies From 90 Countries. Circulation. 2016;134(6):441–450. doi:10.1161/CIRCULATIONAHA.115.018912
2. G Danaei, Y Lu, GM Singh, et al. Cardiovascular disease, chronic kidney disease, and diabetes mortality burden of cardiometabolic risk factors from 1980 to 2010: a comparative risk assessment. Lancet Diabetes Endocrinol. 2014;2(8):634–647. doi:10.1016/S2213-8587(14)70102-0
3. Joynt Maddox KE, Elkind MSV, Aparicio HJ, et al. Forecasting the Burden of Cardiovascular Disease and Stroke in the United States Through 2050-Prevalence of Risk Factors and Disease: a Presidential Advisory From the American Heart Association. Circulation. 2024;150(4):e65–e88. doi:10.1161/CIR.0000000000001256
4. Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16(4):223–237. doi:10.1038/s41581-019-0244-2
5. Moiz A, Zolotarova T, Eisenberg MJ. Outpatient management of essential hypertension: a review based on the latest clinical guidelines. Ann Med. 2024;56(1):2338242. doi:10.1080/07853890.2024.2338242
6. Patra RC, Rautray AK, Swarup D. Oxidative stress in lead and cadmium toxicity and its amelioration. Vet Med Int. 2011;2011:457327. doi:10.4061/2011/457327
7. Takahashi T, Shimohata T. Vascular Dysfunction Induced by Mercury Exposure. Int J Mol Sci. 2019;20(10):2435. doi:10.3390/ijms20102435
8. Li L, Yang X. The Essential Element Manganese, Oxidative Stress, and Metabolic Diseases: links and Interactions. Oxid Med Cell Longev. 2018;2018:7580707. doi:10.1155/2018/7580707
9. National Institutes of Health Office of Dietary Supplements. Selenium Fact Sheet for Health Professionals. Available from: https://ods.od.nih.gov/factsheets/Selenium-HealthProfessional/.
10. Rayman MP. Selenium and human health. Lancet. 2012;379(9822):1256–1268. doi:10.1016/S0140-6736(11)61452-9
11. National Institutes of Health Office of Dietary Supplements. Manganese Fact Sheet for Health Professionals. Available from: https://ods.od.nih.gov/factsheets/Manganese-HealthProfessional/.
12. Tchounwou PB, Yedjou CG, Patlolla AK, Sutton DJ. Heavy metal toxicity and the environment. Exp Suppl. 2012;101:133–164. doi:10.1007/978-3-7643-8340-4_6
13. Martinez-Morata I, Sobel M, Tellez-Plaza M, Navas-Acien A, Howe CG, Sanchez TR. A State-of-the-Science Review on Metal Biomarkers. Curr Environ Health Rep. 2023;10(3):215–249.
14. Martins AC, Almeida Lopes ACB, Urbano MR, et al. An updated systematic review on the association between Cd exposure, blood pressure and hypertension. Ecotoxicol Environ Saf. 2021;208:111636. doi:10.1016/j.ecoenv.2020.111636
15. Ahn J, Kim NS, Lee BK, Park J, Kim Y. Association of Blood Pressure with Blood Lead and Cadmium Levels in Korean Adolescents: analysis of Data from the 2010–2016 Korean National Health and Nutrition Examination Survey. J Korean Med Sci. 2018;33(44):e278. doi:10.3346/jkms.2018.33.e278
16. Park SK, Zhao Z, Mukherjee B. Construction of environmental risk score beyond standard linear models using machine learning methods: application to metal mixtures, oxidative stress and cardiovascular disease in NHANES. Environ Health. 2017;16(1):102. doi:10.1186/s12940-017-0310-9
17. Nawrot TS, Staessen JA, Roels HA, et al. Blood pressure and blood selenium: a cross-sectional and longitudinal population study. Eur Heart J. 2007;28(5):628–633. doi:10.1093/eurheartj/ehl479
18. Laclaustra M, Navas-Acien A, Stranges S, Ordovas JM, Guallar E. Serum selenium concentrations and hypertension in the US Population. Circ Cardiovasc Qual Outcomes. 2009;2(4):369–376. doi:10.1161/CIRCOUTCOMES.108.831552
19. Bastola MM, Locatis C, Maisiak R, Fontelo P. Selenium, copper, zinc and hypertension: an analysis of the National Health and Nutrition Examination Survey. BMC Cardiovascular Disorders. 2020;20(1):45. doi:10.1186/s12872-020-01355-x
20. Wang X, Han X, Guo S, Ma Y, Zhang Y. Associations between patterns of blood heavy metal exposure and health outcomes: insights from NHANES 2011–2016. BMC Public Health. 2024;24(1):558. doi:10.1186/s12889-024-17754-0
21. Chen H, Zou Y, Leng X, et al. Associations of blood lead, cadmium, and mercury with resistant hypertension among adults in NHANES, 1999–2018. Environ Health Prev Med. 2023;28:66. doi:10.1265/ehpm.23-00151
22. Kim DH, Lee S, Jang M, Kim K. Effect of combined exposure to lead, mercury, and cadmium on hypertension: the 2008–2013 Korean National Health and Nutrition Examination Surveys. Int J Occup Med Environ Health. 2025;38(3):264–279. doi:10.13075/ijomeh.1896.02524
23. Stranges S, Laclaustra M, Ji C, et al. Higher selenium status is associated with adverse blood lipid profile in British adults. J Nutr. 2010;140(1):81–87. doi:10.3945/jn.109.111252
24. Otsuka T, Takada H, Nishiyama Y, et al. Dyslipidemia and the Risk of Developing Hypertension in a Working-Age Male Population. J Am Heart Assoc. 2016;5(3):e003053. doi:10.1161/JAHA.115.003053
25. He D, Fan F, Jia J, et al. Lipid profiles and the risk of new-onset hypertension in a Chinese community-based cohort. Nutr, Metab Cardiovasc Dis. 2021;31(3):911–920. doi:10.1016/j.numecd.2020.11.026
26. Centers for Disease Control and Prevention. National health and nutrition examination survey (NHANES): MEC laboratory procedures manual. Hyattsville: National Center for Health Statistics. 2016.
27. Centers for Disease Control and Prevention. National health and nutrition examination survey (NHANES): physician examination procedures manual. Hyattsville: National Center for Health Statistics. 2020.
28. Jones DW, Ferdinand KC, Taler SJ, et al. AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults: a Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Hypertension. 2025;82(10):e212–e316. doi:10.1161/HYP.0000000000000249
29. Heart. How much sodium should I eat per day? Written by American Heart Association editorial staff and reviewed by science and medicine advisors. 2021. Available from: https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/sodium/how-much-sodium-should-i-eat-per-day.
30. Singh R, Pattisapu A, Emery MS. US Physical Activity Guidelines: current state, impact and future directions. Trend Cardiovasc Med. 2020;30(7):407–412. doi:10.1016/j.tcm.2019.10.002
31. Jain BP, Goswami SK, Pandey S. Chapter 9 - Clinical Biochemistry. In: Jain BP, Goswami SK, Pandey S, editors. Protocols in Biochemistry and Clinical Biochemistry. Academic Press; 2021:101–118.
32. NHS. Cholesterol levels: high cholesterol. https://www.nhs.uk/conditions/high-cholesterol/cholesterol-levels/. Available from:
33. Eyth E, Naik R. Hemoglobin A1C. In: StatPearls. Treasure Island (FL): StatPearls Publishing LLC.; 2025.
34. Hu M, Zhang J, Wu J, Su P. Lead exposure induced lipid metabolism disorders by regulating the lipophagy process in microglia. Environ Sci Pollut Res Int. 2023;30(60):125991–126008. doi:10.1007/s11356-023-31086-3
35. Harrison DG, Coffman TM, Wilcox CS. Pathophysiology of Hypertension. Circulation Research. 2021;128(7):847–863. doi:10.1161/CIRCRESAHA.121.318082
36. Gambelunghe A, Sallsten G, Borné Y, et al. Low-level exposure to lead, blood pressure, and hypertension in a population-based cohort. Environ Res. 2016;149:157–163. doi:10.1016/j.envres.2016.05.015
37. Kim MG, Kim MG, Ahn Y-S. Does low lead exposure affect blood pressure and hypertension? J Occupational Health. 2020;62(1):e12107. doi:10.1002/1348-9585.12107
38. CDC. CDC Updates Blood Lead Reference Value. 2024. Available from: https://www.cdc.gov/lead-prevention/php/news-features/updates-blood-lead-reference-value.html.
39. Raja V, Aguiar C, Alsayed N, et al. Non-HDL-cholesterol in dyslipidemia: review of the state-of-the-art literature and outlook. Atherosclerosis. 2023;383:117312. doi:10.1016/j.atherosclerosis.2023.117312
40. Vaziri ND. Mechanisms of lead-induced hypertension and cardiovascular disease. Am J Physiol Heart Circ Physiol. 2008;295(2):H454–465. doi:10.1152/ajpheart.00158.2008
41. Li B, Chen J, Ma H, Yu Y, He S, Yang L. Serum selenium accelerates the development of metabolic disorders in a metabolically healthy obese U.S. population: a retrospective cross-sectional analysis of a population-based study from the NHANES (2011–2018). Front Immunol. 2024;15:1398299. doi:10.3389/fimmu.2024.1398299
42. Wang X, Ding N, Harlow SD, et al. Exposure to heavy metals and hormone levels in midlife women: the Study of Women’s Health Across the Nation (SWAN). Environ Pollut. 2023;317:120740. doi:10.1016/j.envpol.2022.120740
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Visceral Fat, Blood Pressure and Arterial Stiffness in Patients with HFpEF: A Mediation Analysis
Sun M, Gao L, Bai H, Hu W, Zhang X, Xiao J, Deng X, Tao H, Ge P, Qin Y, Zhang D
Diabetes, Metabolic Syndrome and Obesity 2023, 16:653-662
Published Date: 8 March 2023
Perseverative Cognition as a Mediator Between Personality Traits and Blood Pressure
Arroyave-Atehortua D, Cordoba-Sanchez V, Zambrano-Cruz R
Vascular Health and Risk Management 2023, 19:363-370
Published Date: 29 June 2023