")
Back to Journals » International Journal of General Medicine » Volume 15
Selection of Laparoscopy or Laparotomy for Treating Cesarean Scar Pregnancy: A Retrospective Study
Authors Fu P, Zhou T, Cui P, Wang W, Wang S, Liu R
Received 8 April 2022
Accepted for publication 7 September 2022
Published 13 September 2022 Volume 2022:15 Pages 7229—7240
DOI https://doi.org/10.2147/IJGM.S369884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Peiying Fu, Ting Zhou, Pengfei Cui, Wenwen Wang, Shixuan Wang, Ronghua Liu
Department of Obstetrics and Gynecology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Correspondence: Ronghua Liu, Department of Obstetrics and Gynecology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, 1095 Jiefang Anv, Wuhan, Hubei, 430030, People’s Republic of China, Tel/Fax +86 27 83663078, Email [email protected]
Objective: Cesarean scar pregnancy (CSP) can have catastrophic consequences, but a standardized diagnosis and treatment for CSP are lacking. At least 10 different treatments are currently available, further confusing treatment selection. The aim of this study was to compare the outcomes of using laparotomy or laparoscopy to treat CSP.
Methods: We reviewed data from 935 patients with suspected CSP from 1 January 2013 to 31 December 2018. A total of 278 patients were included in the study, of whom 121 were treated with laparoscopy and 157 were treated with laparotomy. We compared and analyzed the characteristics of laparoscopic and open surgeries for treating CSP cases and the advantages and disadvantages of different vascular pretreatments.
Results: Intraoperative bleeding, the transfusion rate, total days of hospitalization and postoperative hospital length of stay were lower with laparoscopy than laparotomy (P < 0.05). There was no difference in the factors (beta human chorionic gonadotropin [β-HCG] decrease, reoperation rate and tissue residues) closely related to the success of the surgery in the two groups. Furthermore, we used different blood vessel pretreatments among patients. The rates of tissue residue, reoperation and intraoperative blood transfusion were lower in patients with temporary vascular occlusion than in patients with permanent vascular occlusion.
Conclusion: This study revealed that laparoscopic surgery is superior to laparotomic surgery for treating CSP. Patients in both groups benefited from temporary arterial occlusion. Thus, temporary arterial occlusion with laparoscopic surgery may be the best treatment for CSP.
Keywords: cesarean scar pregnancy, hysterotomy, laparoscopy, laparotomy, arterial occlusion
Introduction
Cesarean scar pregnancy (CSP) is a rare form of ectopic pregnancy with potentially catastrophic consequences, including massive bleeding, uterine rupture and even life-threatening events. Compared with placenta implantation alone without uterine scarring, implantation in scar tissue deficient in myometrium in CSP results in poor contractility, which may carry additional risks and further aggravate hemorrhage.1–3 CSP has also been linked with the risk of placenta accreta spectrum (PAS).4 There are several methods for classifying CSP. Vial et al classified CSP according to the degree to which the gestational sac was implanted into uterine scar tissue and the direction of gestational sac growth.5 Chinese experts have classified CSP into three types according to scar thickness and gestational sac location;6 however, data and quantitative indicators that may guide clinical treatment of CSP regarding the actual operation are lacing. Furthermore, in a wide swath of the literature, CSP is not classified into types.
A set of standardized global guidelines or consensus for treating CSP is lacking. At present, medical treatment methods for CSP include administration of potassium chloride or absolute ethanol into the embryonic sac, systemic or local (via direct injection or injection of the bilateral uterine artery) administration of methotrexate (MTX) alone or in combination with dilatation and curettage (D&C) guided by ultrasonography, and hysteroscopy or laparoscopy.7–9 Some researchers have concluded that MTX administration is an effective treatment for CSP patients with fertility requirements, as it significantly reduces beta human chorionic gonadotropin (β-hCG) levels.10,11 In contrast, others have argued the opposite. Because MTX monotherapy has low success rates and high complication rates, systemic MTX alone is not recommended.12 A reviewer suggested that MTX administration for the treatment of CSP was considered off-label use.13 In addition, high-intensity focused ultrasound followed by ultrasound-guided D&C has been used to treat CSP.14,15 Finally, transabdominal and laparoscopic approaches have been used to perform hysterotomy or even hysterectomy.16 However, conservative treatments do not alter the thin or defective muscle layers in CSP cases and instead only aggravate the condition of the muscle layer. Should these types of CSP be treated with surgery to repair and reconstruct the defective muscle layer of the lower segment of the uterus?
Many researchers have argued that hysterotomy could be used not only to remove the pregnancy but also to repair defects in the lower uterine segment. Therefore, hysterotomy may be the best treatment option for CSP.17 Laparotomy is available in almost all hospitals, and some patients had to switch to open surgery because of uncontrollable bleeding during laparoscopic surgery. On the other hand, laparoscopic surgery is safe for the removal of pregnancy tissue, requires a shorter in-hospital stay and results in little blood loss. Alternatively, many doctors have treated CSP through transvaginal hysterotomy, which is another approach for treating this condition. There are currently no studies in the literature comparing hysterotomy with laparotomy and laparoscopy in the treatment of CSP.
The goal of this study was to explore the evaluation and necessity of the surgical treatment of CSP and to compare the advantages and disadvantages of laparoscopic and laparotomic surgery.
Materials and Methods
Patients
We retrospectively reviewed patients with suspected CSP admitted to our institution between 1 January 2013 and 31 December 2018, identifying a total of 935 patients. The Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology approved the study. Among the 278 patients who were eligible for the study after application of the inclusion criteria, 121 patients underwent laparoscopy, and 157 patients underwent laparotomy (Figure 1).
 |
Figure 1 Flowchart of the study population. |
Diagnostic and Inclusion Criteria
At present, no diagnostic or classification methods for CSP are universally accepted. The standard adopted by many doctors was proposed by Vial in 2000.5 In 2016, the Chinese Journal of Obstetrics and Gynecology published an expert opinion on the diagnosis and treatment of Cesarean scar pregnancy. In this expert opinion, the following types of CSP were defined. Type I CSP was defined as the gestational sac mostly located in the intrauterine cavity and CSP with myometrial thickness >3 mm; type II CSP was defined as myometrial thickness ≤ 3 mm. In type III CSP, the gestational sac is convex in the direction of the bladder, and the myometrial thickness between the gestational sac and the bladder is obviously thin or even absent, with myometrial thickness ≤ 3 mm. The inclusion criteria for this study were as follows: (1) a history of lower uterine segment cesarean delivery; (2) positive for serum β-hCG; (3) CSP clinically diagnosed by transvaginal ultrasound, with findings of an empty cervix and uterine cavity, a gestational sac or mixed mass with or without fetal cardiac activity at the anterior wall of the uterine isthmus at the lower uterine incision scar, an absent myometrial layer between the gestational sac and the bladder, or gestational sac implantation or infiltration to the muscle layer in some cases; (4) postoperative histopathologic confirmation of tissues indicating conception; and (5) treatment with laparoscopy or laparotomy.
Preoperative Evaluation
The choice of laparoscopy or laparotomy for CSP patients was mainly based on the following factors: gestational weeks, β-hCG level, degree of extravasation of gestational sac, scar thickness and patient symptoms. Because our hospital is a referral center, many patients were referred to our hospital. Therefore, laparotomy was performed on most of these patients, although the choice of surgical method depended on the surgical skills of the individual surgeon.
Surgical Methods
Laparoscopy
First, the peritoneum was opened, the bladder was pushed aside, and the lower segment of the uterus and the protruding mass were exposed completely. Importantly, the lower boundary needed to extend past the start of the normal cervical tissue by approximately 1.5 cm to allow subsequent rapid suturing and avoid damage of the bladder, ureters and uterine arteries, even if massive bleeding were to occur. D&C of the uterus was performed by the assistant before the lower uterine scar was cut open. Next, the bulging part of the gestational ectopic mass was wedge-resected, and the scar was trimmed using scissors without electrocauterization. Finally, 1–0 absorbable sutures were employed to perform interrupted suturing of the incision in the myometrium, and the peritoneum was reapproximated.
According to the surgical technique and habits of different surgeons, different methods of vascular pretreatment have been applied when assessing the risk of massive intraoperative hemorrhage. These methods include (1) uterine artery embolism (UAE) and (2) arterial occlusion (temporary or permanent). Bilateral UAE was performed using gelatin sponge particles within 24 hours before surgery. Arterial occlusion was performed as follows: after opening the lateral peritoneum and confirming the ureter, the bilateral uterine or internal iliac arteries were exposed. Arteries were occluded by either temporary arterial occlusion with metal vascular clamps or permanent arterial occlusion with clamping or sewing. After the uterine incision was sutured, the clips were removed, and the uterine arteries were recanalized. The laparotomic procedure is similar to the laparoscopic procedure.
Laparotomy
In the more conservative treatment process, if a large amount of life-threatening bleeding that was difficult to control occurred during D&C, laparoscopic surgery (mainly for surgeons less skilled in laparoscopic vascular management) or transvaginal surgery, it was necessary to rapidly switch to open surgery to prevent serious complications such as the need to perform a hysterectomy and other catastrophic complications (even death). The laparotomic procedure was similar to the laparoscopic procedure.
Vascular pretreatment for laparotomy differed from that for laparoscopic surgery. For transabdominal surgery, temporary occlusion of the bilateral uterine arteries was performed as vascular pretreatment. Specifically, a rubber tourniquet was passed through the avascular zone on both sides of the broad ligament and temporarily tied around the uterine isthmus for temporary hemostasis after the bladder was pushed aside. After the uterine incision was sutured, the vascular band was released, and the uterine arteries were recanalized. For permanent arterial inclusion, the bilateral uterine or internal iliac arteries were exposed and then double ligated with 1–0 nonabsorbable sutures.
Analysis of Clinical Characteristics
The following variables were included: age; type of CSP; number of abortions; number of cesarean sections (CSs); interval from last CS; gestational age; gestational sac diameter; gestational sac width; gestational sac volume; thickness of the remaining myometrium; color Doppler signal; fetal heartbeat; vaginal bleeding; abdominal pain; preoperative β-hCG level; β-hCG level on the first postoperative day; preoperative hemoglobin; hemoglobin on the first postoperative day; intraoperative bleeding volume; other treatments; tissue residues; necessity of reoperation; pain; transfusion; placement time of drainage tube; postoperative length of stay; and total hospitalization days.
Follow-Up
The initial follow-up schedule was once per week from the first day after discharge until the serum β-hCG levels returned to normal. The first phase of follow-up included assessing vaginal bleeding and serum β-hCG levels, a routine blood test and ultrasonography. During the second phase, follow-up was conducted once every three months for one year. The follow-up items included menstrual status, pregnancy status, ovarian function and endocrine levels in addition to the above items.
Statistical Analysis
We used SPSS 17.0 software (SPSS, Inc.) to statistically analyze the data. All data are represented as the mean ± standard deviation (SD). Categorical data are expressed as frequencies. Significant differences between the two groups were assessed with the chi-squared test and Fisher’s exact test for categorical variables. Multivariate logistic regression analysis was subsequently carried out to analyze the relationships among factors. P < 0.05 was considered statistically significant.
Results
Study Population
During the period of 2013–2018, 935 women suspected of having CSP were treated at our institution (a major tertiary referral hospital in China). Of these patients, 29 failed to meet the diagnostic criteria for CSP, and 628 underwent other types of treatments (Figure 1). Of the remaining patients, 121 (13.35%) underwent laparoscopic surgery, and 157 (17.33%) underwent laparotomic surgery. The baseline characteristics and clinical data of the two groups are presented in Table 1. The two groups were similar in most of the clinical factors, such as age, gestational age, number of abortions, number of CSs, interval from the last CS, main symptoms (vaginal bleeding and abdominal pain), type of CSP (according to the consensus of Chinese experts in 2016), characteristic features on the ultrasound scans (color Doppler signal and fetal heartbeat) and hematological indicators (hemoglobin and β-hCG levels); the two groups differed in gestational sac diameter and gestational sac volume.
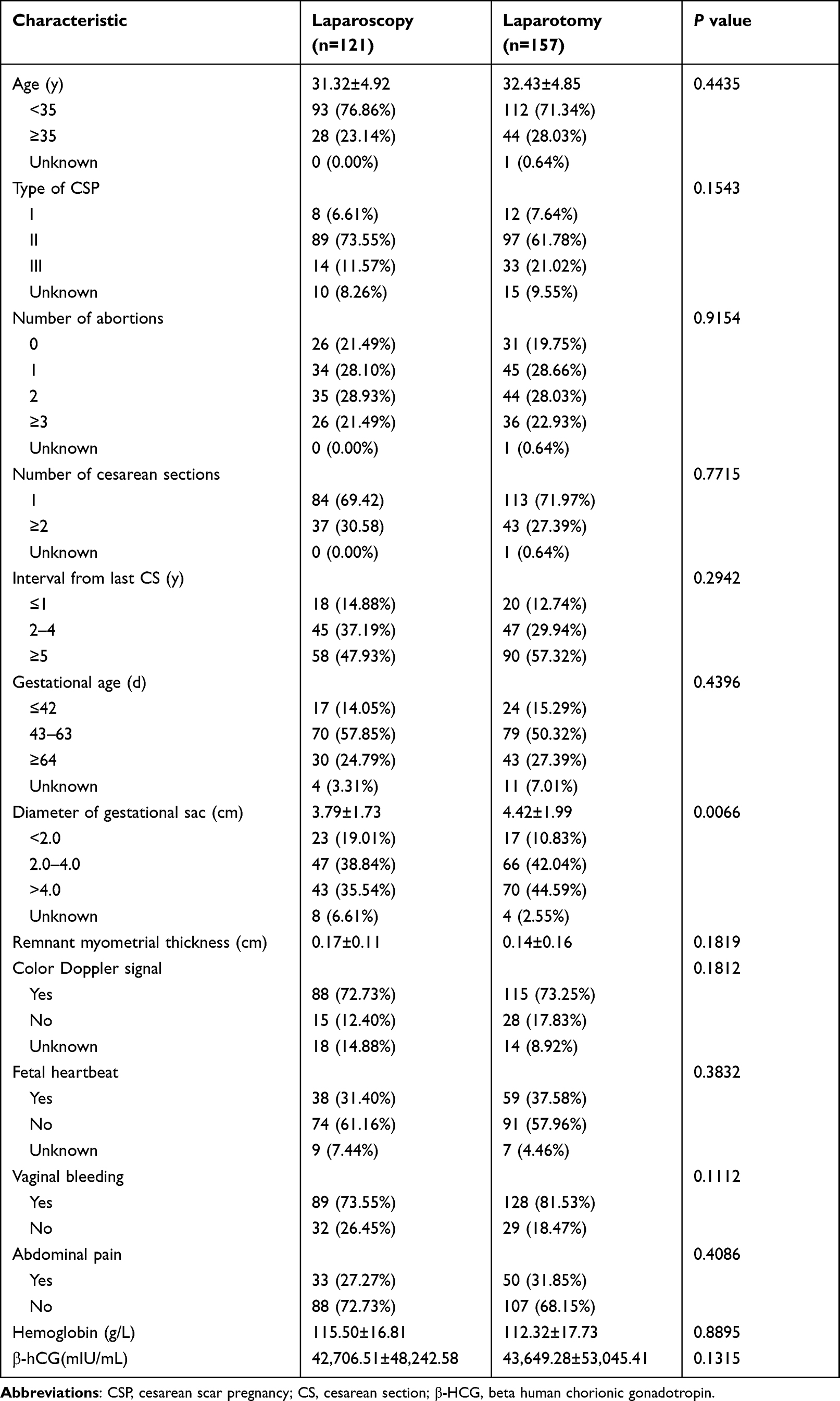 |
Table 1 Clinical Characteristics of Patients |
Laparoscopic Management of Blood Vessels in Cesarean Scar Pregnancy
We used laparoscopy to treat type III CSP. Typical type III CSP manifestations were observed under ultrasound and laparoscopy (Figure 2A and B). With laparoscopy, the uterine arteries or internal iliac arteries were fully exposed. We pretreated the bilateral uterine arteries or the internal iliac arteries before the operation. When treating the uterine arteries, we used small flexible metal vascular clips to temporarily block blood flow (Figure 2C and D). Large flexible metal vascular clips were used to temporarily occlude blood flow of the bilateral internal iliac arteries (Figure 2E and F), differing from a previous method that used silk thread to temporarily block the blood flow of the internal iliac arteries.18 Interrupted suturing of the incision was employed to close the myometrium (Figure 2G). After suturing and ensuring that there was no bleeding at the incision, the metal clamps used to occlude the blood vessels on both sides were removed (Figure 2H).
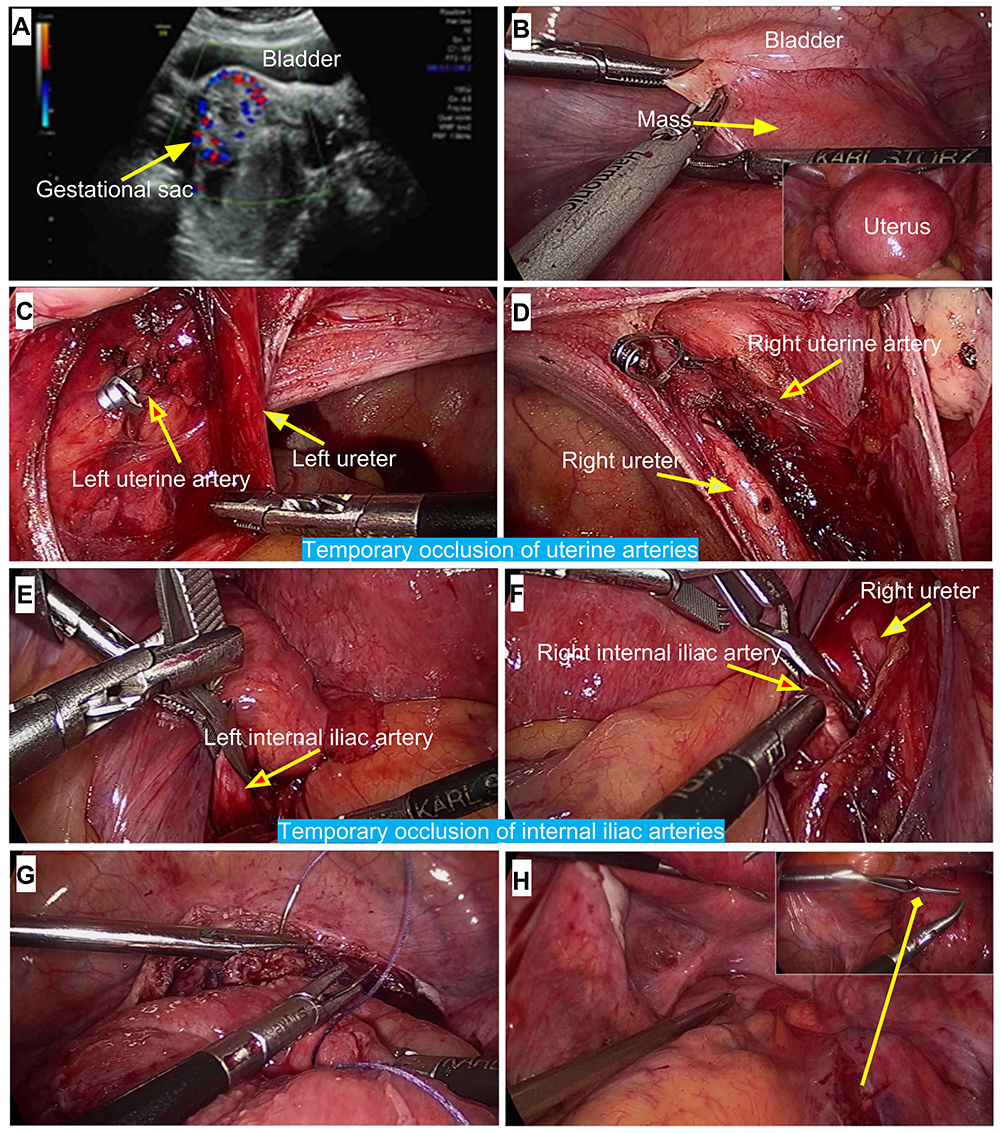 |
Figure 2 Laparoscopic management of the uterine arteries or internal iliac arteries and surgical procedures in cesarean scar pregnancy. (A) Ultrasound findings indicated implantation of the gestational sac in the scar tissue, protruding from the uterus and growing toward the bladder. (B) The uterus was markedly enlarged and full in shape, and the mass impinged on the abdominal cavity (yellow arrow). (C and D) After dissection of the pelvic sidewalls, the ureters (yellow arrows) and uterine arteries (blue arrows) were separated and identified. The bilateral uterine arteries were temporarily occluded with flexible metal clips. (E and F) The bilateral internal iliac arteries (blue arrows) were occluded with flexible metal clips. (G) Scissors were used to trim scar tissue after removal of the gestational sac. Fast interrupted suturing of the incision of the lower uterine segment was performed with 1–0 absorbable sutures. Finally, peritonealization was performed. (H) After suturing, the metal clamps on the bilateral arteries were removed. |
Comparison of Clinical Outcomes Between the Two Groups
The main outcomes of the perioperative period in the two groups are shown in Figure 3. Of the 906 patients diagnosed with CSP, 146 underwent two or more types of therapies. Because of massive vaginal bleeding during treatment, these patients were transferred to open or laparoscopic surgery. The intraoperative bleeding volume in the laparotomy group was markedly greater than that in the laparoscopy group (Figure 3A). Two indicators of surgical success (postoperative hemoglobin and β-hCG level) did not differ between the two groups (Figure 3B). The number of patients who underwent combined treatments in the laparoscopy group was greater than that in the laparotomy group (p<0.001, Figure 3C). Due to the differences between the two groups in gestational sac diameter and width (Table 1), we used multivariate logistic regression analysis to analyze the relationship between these factors and the intraoperative bleeding volume under the different surgical methods. Moreover, the two factors (ie, gestational sac diameter, and width) were collinear and thus not recommended for inclusion in the multivariate analysis. Therefore, we only included the gestational sac diameter and analyzed its relationship with the operation method. According to the analysis, the bleeding risk under laparotomy was 1.78 times higher than that under laparoscopy given the same gestational sac diameter (Table 2).
 |
Table 2 Relationship Between the Gestational Sac Diameter and the Intraoperative Bleeding Volume Under the Two Surgical Methods According to Multivariate Logistic Regression Analysis |
 |
Figure 3 Comparison of the main intraoperative and postoperative outcomes between the two groups. (A) Perioperative hemorrhage and hemoglobin changes in the two groups. The hemoglobin on the first postoperative day and the postoperative hemoglobin decrease did not differ between the laparoscopy and laparotomy groups, but the intraoperative bleeding volume differed between the two groups (p=0.0095). (B) Serum concentration of β-hCG after the operation. The β-hCG level on the first postoperative day and the postoperative β-hCG decrease did not differ between the two groups. (C and D) Evaluation of relevant indicators of surgical and postoperative recovery. A small number of patients were treated with one or more techniques prior to laparoscopic or open surgery, with more patients in the laparoscopy group than in the laparotomy group (p<0.0001). The rate of transfusion, the total number of days of hospitalization and postoperative length of stay were lower in the laparoscopy group than in the laparotomy group (p<0.05). Rates of reoperation, residual tissue, and pain as well as drainage tube placement duration did not differ between the two groups. |
In addition, we also found that the transfusion rate in the laparotomy group was higher than that in the laparoscopy group. Finally, analysis of the postoperative data did not reveal statistically significant differences between the two groups. The total number of days of hospitalization and postoperative length of stay in the laparoscopy group were lower than those in the laparotomy group (Figure 3D).
Clinical Outcomes of Different Methods of Artery Pretreatment in the Two Groups
In both groups, we used various methods of blood vessel pretreatment before the operation. In the laparoscopy group, the incidence of residual tissue, reoperation, pain and transfusion was lower for patients who underwent temporary arterial occlusion than for patients who underwent no artery pretreatment, UAE or permanent arterial occlusion (Figure 3). Notably, the transfusion rate reached 42.86% in laparoscopic surgery following UAE treatment (Table 3). The differences in the rates of residual tissue, reoperation and transfusion between pretreatment methods were also significant in the laparotomy group (Table 4). However, the transfusion rate (41.67%) for permanent vascular occlusion was less than that for the other three arterial pretreatments (77.69%, 72.22% and 73.33%). Notably, the majority of patients who underwent laparoscopic or open surgery were categorized with type II (Vial et al) or type III (consensus of Chinese experts) CSP. Some patients had received one or more conservative treatments before surgery. The duration of drainage tube placement and postoperative length of stay were shorter in patients who received temporary arterial occlusion than in the other three arterial pretreatments.
 |
Table 3 Comparison of Clinical Outcomes Under Different Blood Vessel Pretreatments in the Laparoscopy Group |
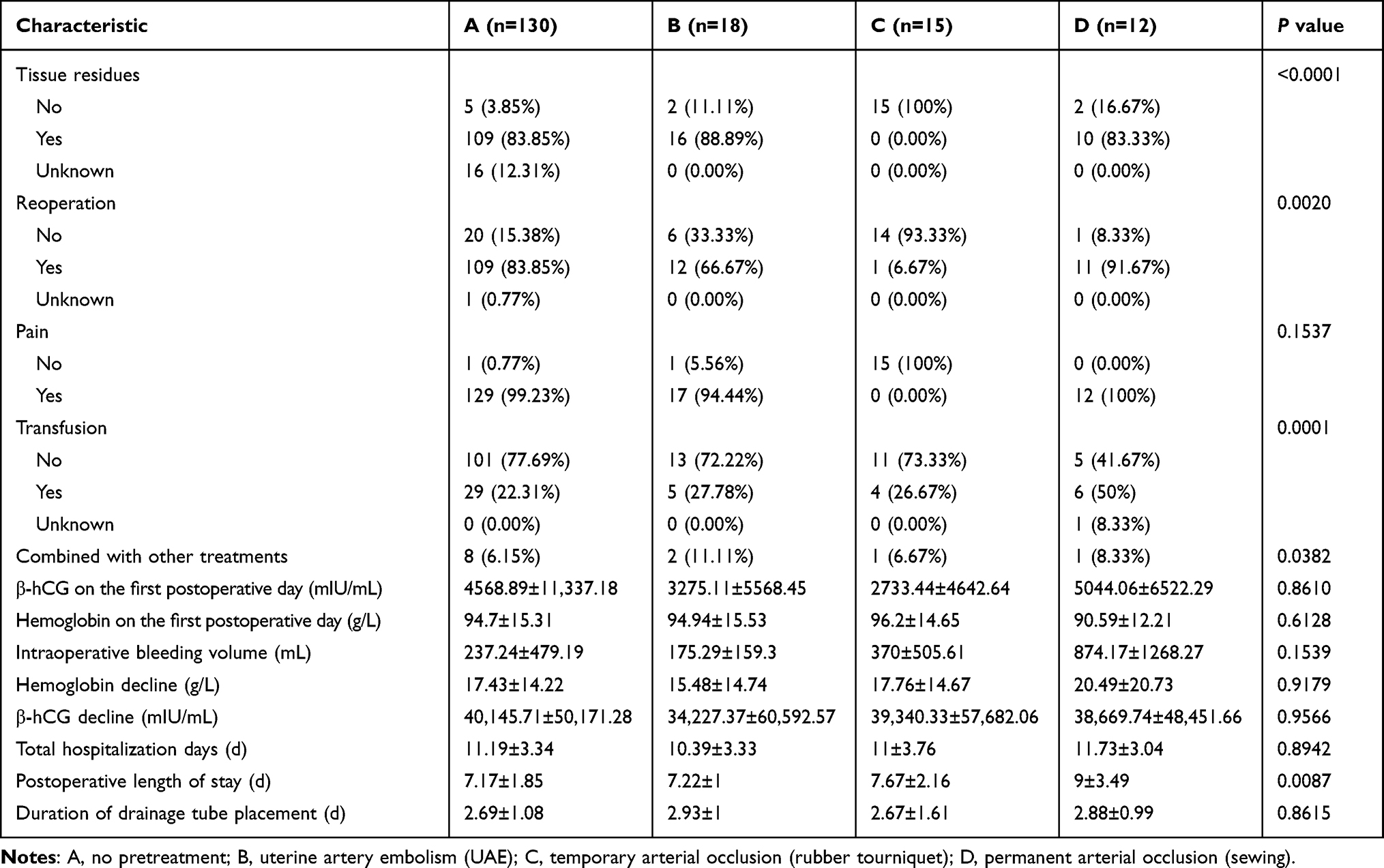 |
Table 4 Comparison of Clinical Outcomes Under Different Blood Vessel Pretreatments in the Laparotomy Group |
Discussion
No prior studies have reported comparisons of the use of laparoscopy and laparotomy for treating CSP. Laparotomic resection has many advantages, such as completely removing pregnancy tissue implanted in the scar, repairing scar defects and reducing the risk of recurrence, but it leaves large surgical wounds.19 Laparoscopy has been widely used in gynecology, and laparoscopic surgery has many advantages for treating CSP. Moreover, few studies have focused on identifying the best treatment strategy for CSP cases, and there are no similar reports in the available literature. In the present study, hysterotomy via laparoscopy for treating CSP cases resulted in fewer complications than laparotomy.
In this study, more patients underwent laparoscopic surgery than laparotomy after other treatments failed. In addition, laparoscopy involved less bleeding and fewer blood transfusions than laparotomy. Moreover, we observed that the total number of days of hospitalization and postoperative length of stay were lower in the laparoscopy group than in the laparotomy group. In summary, we demonstrated that laparoscopic surgery is superior to laparotomic surgery for treating CSP, as it resulted in fewer complications.
To reduce the risk of bleeding during or after the operation, surgeons have utilized various blood vessel pretreatments. UAE is currently accepted as a treatment or pretreatment for CSP. However, UAE may affect the blood supply of the uterus and ovaries and cause pelvic pain, pulmonary embolism and endometrial atrophy.20 Alternatively, bilateral uterine artery (or internal iliac artery) ligation or temporary arterial occlusion has been used as a vascular pretreatment in CSP.21 In our retrospective analysis, the rates of residual tissue, reoperation and intraoperative blood transfusion were lower in patients treated with temporary vascular occlusion than in patients treated with permanent vascular occlusion. Therefore, patients benefitted more from temporary arterial occlusion in both groups.
Many doctors may underestimate the severity of CSP. Laparoscopic or open surgery was used as a remedy after other treatments were ineffective or resulted in massive bleeding. This delay in surgical approaches leads to a potential increase in risk and imposes an increased burden on patients.22–24 In a prospective study, all patients underwent MTX embolization under UAE, followed by D&C or hysteroscopy combined with laparoscopy. Laparotomy was performed as a remedial measure after D&C in 21.2% of patients and even led to hysterectomy in a patient.25 In high-risk CSP cases, D&C may not be appropriate. In other studies, CSP patients underwent laparoscopic or open surgery. However, these studies did not specify the indications for choosing these treatments and did not compare the advantages and disadvantages of laparoscopy and laparotomy.26–29 Therefore, hysterotomy should be performed as soon as possible once a definitive diagnosis of high-risk CSP is made to prevent adverse outcomes.
More importantly, we should not swing to the other extreme; instead, doctors should carefully select between medical treatment, D&C under hysteroscopy, or ultrasound monitoring for the most dangerous type of CSP. For exogenous CSP, fatal intraoperative and/or postoperative bleeding, tardive intermittent massive vaginal bleeding, residual tissue, a slow decrease or even an increase in the serum β-hCG level and intrauterine infection are likely to occur following treatment by the above methods. In addition, cesarean scar defects (CSDs) are often deep or irregular, making it difficult for the instrument to reach the deepest areas and inevitably resulting in residual tissue. Furthermore, intraoperative bleeding, perforation of the uterus, bladder injury and other serious complications may occur.30 Therefore, timely hysterotomy may avoid the above situations given a definite diagnosis.
In the present study, 278 cases met the inclusion criteria. These patients were treated with laparoscopic surgery or laparotomic surgery. The hysterotomy rate was 30.68%, reflecting the proportion of high-risk CSP patients admitted to our center. As our hospital is one of the major tertiary referral hospitals in China, these data also indicate that doctors must give proper attention to CSP. However, we found that the CSP classifications, according to either by the Vial criteria or those proposed by Chinese experts, did not truly reflect the severity of the CSP cases observed. Hysterotomy at our hospital was performed for most type II CSP patients (according to the consensus of Chinese experts) who underwent laparoscopy or laparotomy. This pattern may lead to an overemphasis on surgical treatment, which increases patient pain, hospitalization costs and length of stay. Does this pattern hold beyond our own observations? Previous studies have shown that either laparoscopy or laparotomy is mainly performed for type II CSP (Val et al). However, the specific classification of some patients remains unknown.
Our research aimed to identify a suitable, effective and safe surgical approach for the treatment of CSP. To better guide clinical practice, a new method of classifying CSP cases is needed; a better classification method can improve the awareness and identification of CSP. We also suggest a comprehensive assessment of the probability of recurrent CSP or CSD after hysterotomy (for both laparoscopy or laparotomy). In addition, arterial occlusion, especially permanent vascular occlusion, still has shortcomings similar to those of UAE. At present, no studies have evaluated the advantages and disadvantages of temporary and permanent arterial occlusion in CSP operations. It also remains unclear whether blocking these arteries affects the function of the female reproductive system. When follow-up data become available, this topic should be evaluated.
This analysis identified 935 female patients with suspected CSP from 2013 to 2018. The main achievements of this study, including its contributions to the field, are summarized as follows. This retrospective study comprehensively assessed the feasibility, advantages and disadvantages of treating CSP cases with laparotomy or laparoscopy. Furthermore, we also compared the effects of different vascular pretreatments on surgical outcomes. The suturing technique was particularly important. As most CSs at present are performed with a transverse incision of the lower uterine segment, the uterine body prevents the needle from proceeding; this kind of incision is difficult to sew with the right hand in a laparoscopy. However, with a left-hand suture, the puncture angle is suitable (Figure 2G), and the direct visualization of the area ensures perfect suturing of the whole lower segment.
Our study also has some shortcomings. Our conclusions are limited by the retrospective design, data heterogeneity and the reliance on clinical CSP data not originally collected for research purposes. Additionally, this was a single-center study and therefore has potential selection bias, which may limit its external validity, as our results may not represent the findings of other hospitals. Another limitation of our study is the incomplete follow-up, which makes it difficult to conduct a comprehensive analysis of the follow-up parameters, such as menstruation, ovarian function and fertility.
In conclusion, our study suggests that accurate assessment of CSP severity is the most important factor in selecting appropriate treatment strategies and that temporary arterial occlusion along with laparoscopy may be the best treatment. Future work will include comprehensive follow-up data, and a multicenter clinical study of CSP is currently underway.
Ethics Approval and Consent to Participate
The Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology approved this study (No: TJ-IRB20191214). All study participants provided informed written consent, including consent to examine hospital records. The study was conducted in accordance with the ethics of the 2013 Helsinki World Medical Association Declaration.
Funding
This work was supported by the National Natural Science Foundation of China (81572563).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jurkovic D, Ben-Nagi J, Ofilli-Yebovi D, et al. Efficacy of Shirodkar cervical suture in securing hemostasis following surgical evacuation of Cesarean scar ectopic pregnancy. Ultrasound Obstet Gynecol. 2007;30(1):95–100. doi:10.1002/uog.4058
2. Chiang YC, Tu YA, Yang JH, et al. Risk factors associated with failure of treatment for cesarean scar pregnancy. Int J Gynaecol Obstet. 2017;138(1):28–36. doi:10.1002/ijgo.12157
3. Timor-Tritsch I, Buca D, Di Mascio D, et al. Outcome of cesarean scar pregnancy according to gestational age at diagnosis: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2021;258:53–59. doi:10.1016/j.ejogrb.2020.11.036
4. Cali G, Timor-Tritsch I, Forlani F, et al. Value of first‐trimester ultrasound in prediction of third‐trimester sonographic stage of placenta accreta spectrum disorder and surgical outcome. Ultrasound Obstet Gynecol. 2020;55(4):450–459. doi:10.1002/uog.21939
5. Vial Y, Petignat P, Hohlfeld P. Pregnancy in a cesarean scar. Ultrasound Obstet Gynecol. 2000;16(6):592–593.
6. Family Planning Group, Obstetrics and Gynecology Branch, Chinese Medical A ssociation. Expert consensus on diagnosis and treatment of uterine scar pregnancy after cesarean section (2016). Chin J Obstet Gynecol. 2016;51:568–572. In Chinese.
7. Naeh A, Shrim A, Shalom-Paz E, et al. Cesarean scar pregnancy managed with local and systemic methotrexate: a single center case series. Eur J Obstet Gynecol Reprod Biol. 2019;238:138–142. doi:10.1016/j.ejogrb.2019.05.014
8. Lu F, Liu Y, Tang W, et al. Successful treatment of cesarean scar pregnancy with transvaginal injection of absolute ethanol around the gestation sac via ultrasound. BMC Pregnancy Childbirth. 2019;19(1):312. doi:10.1186/s12884-019-2468-3
9. Gulino FA, Pappalardo E, Ettore C, et al. Caesarean scar pregnancy: descriptive paper of three different types of management on a series of clinical cases. Prz Menopauzalny. 2020;19(2):61–65. doi:10.5114/pm.2020.97836
10. Gulino FA, Ettore C, Ettore G. A review on management of caesarean scar pregnancy. Curr Opin Obstet Gynecol. 2021;33(5):400–404. doi:10.1097/GCO.0000000000000734
11. Tanaka K, Coghill E, Ballard E, et al. Management of caesarean scar pregnancy with high dose intravenous methotrexate infusion therapy: 10-year experience at a single tertiary centre. Eur J Obstet Gynecol Reprod Biol. 2019;237:28–32. doi:10.1016/j.ejogrb.2019.04.008
12. Birch Petersen K, Hoffmann E, Rifbjerg Larsen C, et al. Cesarean scar pregnancy: a systematic review of treatment studies. Fertil Steril. 2016;105(4):958–967. doi:10.1016/j.fertnstert.2015.12.130
13. Liu L, Ross WT, Chu AL, et al. An updated guide to the diagnosis and management of cesarean scar pregnancies. Curr Opin Obstet Gynecol. 2020;32(4):255–262. doi:10.1097/GCO.0000000000000644
14. Zhang C, Zhang Y, He J, et al. Outcomes of subsequent pregnancies in patients following treatment of cesarean scar pregnancy with high intensity focused ultrasound followed by ultrasound–guided dilation and curettage. Int J Hyperthermia. 2019;36(1):926–931. doi:10.1080/02656736.2019.1654619
15. Liu CN, Tang L, Sun Y, et al. Clinical outcome of high-intensity focused ultrasound as the preoperative management of cesarean scar pregnancy. Taiwan J Obstet Gynecol. 2020;59(3):387–391. doi:10.1016/j.tjog.2020.03.009
16. Gao L, Huang Z, Gao J, et al. Uterine artery embolization followed by dilation and curettage within 24 hours compared with systemic methotrexate for cesarean scar pregnancy. Int J Gynaecol Obstet. 2014;127(2):147–151. doi:10.1016/j.ijgo.2014.05.005
17. Fylstra DL. Ectopic pregnancy within a cesarean scar: a review. Obstet Gynecol Surv. 2002;57(8):537–543. doi:10.1097/00006254-200208000-00024
18. Su X, Yang M, Na Z, et al. Application of laparoscopic internal iliac artery temporary occlusion and uterine repair combined with hysteroscopic aspiration in type III cesarean scar pregnancy. Am J Transl Res. 2022;14(3):1737–1741.
19. Wang G, Liu X, Bi F, et al. Evaluation of the efficacy of laparoscopic resection for the management of exogenous cesarean scar pregnancy. Fertil Steril. 2014;101(5):1501–1507. doi:10.1016/j.fertnstert.2014.01.045
20. Holub Z, Mara M, Kuzel D, et al. outcomes after uterine artery occlusion: prospective multicentric study. Fertil Steril. 2008;90(5):1886–1891. doi:10.1016/j.fertnstert.2007.08.033
21. Dior UP, Palma-Dias R, Reidy KL, et al. Cesarean scar pregnancies: incidence and factors associated with conversion to surgery from medical management. J Minim Invasive Gynecol. 2019;26(5):919–927. doi:10.1016/j.jmig.2018.09.771
22. Fang Q, Sun L, Tang Y, et al. Quantitative risk assessment to guide the treatment of cesarean scar pregnancy. Int J Gynaecol Obstet. 2017;139(1):78–83. doi:10.1002/ijgo.12240
23. Jiao LZ, Zhao J, Wan XR, et al. Diagnosis and treatment of cesarean scar pregnancy. Chin Med Sci J. 2008;23(1):10–15. doi:10.1016/S1001-9294(09)60002-X
24. Le A, Li M, Xu Y, et al. Different surgical approaches to 313 cesarean scar pregnancies. J Minim Invasive Gynecol. 2019;26(1):148–152. doi:10.1016/j.jmig.2018.03.035
25. Wu X, Xue X, Wu X, et al. Combined laparoscopy and hysteroscopy vs. uterine curettage in the uterine artery embolization-based management of cesarean scar pregnancy: a cohort study. Int J Clin Exp Med. 2014;7(9):2793–2803.
26. Özcan HÇ, Uğur MG, Balat Ö, et al. Is ultrasound–guided suction curettage a reliable option for treatment of cesarean scar pregnancy? A cross–sectional retrospective study. J Matern Fetal Neonatal Med. 2018;31(22):2953–2958. doi:10.1080/14767058.2017.1359827
27. Sun YY, Xi XW, Yan Q, et al. Management of type II unruptured cesarean scar pregnancy: comparison of gestational mass excision and uterine artery embolization combined with methotrexate. Taiwan J Obstet Gynecol. 2015;54(5):489–492. doi:10.1016/j.tjog.2015.08.002
28. Wang YL, Weng SS, Huang WC, et al. Laparoscopic management of ectopic pregnancies in unusual locations. Taiwan J Obstet Gynecol. 2014;53(4):466–470. doi:10.1016/j.tjog.2014.01.004
29. Giampaolino P, De Rosa N, Morra I, et al. Management of cesarean scar pregnancy: a single-institution retrospective review. Biomed Res Int. 2018;2018:6486407. doi:10.1155/2018/6486407
30. Wang L, Sun L, Wang L, et al. Laparoscopic temporary bilateral uterine artery occlusion with silicone tubing to prevent hemorrhage during vacuum aspiration of cesarean scar pregnancies. J Obstet Gynaecol Res. 2015;41(11):1762–1768. doi:10.1111/jog.12784
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.