")
Back to Journals » International Journal of General Medicine » Volume 16
Seizure Remission and Its Predictors Among Epileptic Patients on Follow-Up at Public Hospitals in Eastern Ethiopia: A Retrospective Cohort Study
Authors Mohammed AS , Mishore KM, Tafesse TB, Jambo A , Husen AM , Alemu A
Received 23 August 2023
Accepted for publication 10 November 2023
Published 16 November 2023 Volume 2023:16 Pages 5343—5354
DOI https://doi.org/10.2147/IJGM.S436814
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ammas Siraj Mohammed,1 Kirubel Minsamo Mishore,1 Tadesse Bekele Tafesse,2 Abera Jambo,1 Ahmed Mohammed Husen,3 Addisu Alemu4
1Clinical Pharmacy Department, School of Pharmacy, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2Department of Pharmaceutical Chemistry and Pharmacognosy, School of Pharmacy, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 3Department of Pediatrics, School of Medicine, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 4Department of Reproductive Health and Nutrition, School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Kirubel Minsamo Mishore, Email [email protected]
Background: Epilepsy is one of the common chronic neurological disorders with varying therapeutic responses. Despite the high prevalence of epilepsy and the significant treatment gaps in developing nations, such as Ethiopia, there is a dearth of data on seizure remission and its predictors in Eastern Ethiopia in particular.
Objective: This study aimed to determine seizure remission and its predictors among epileptic patients on follow-up in Hiwot Fana Specialized University Hospital (HFSUH) and Dilchora Referral Hospital (DCRH), from July 2 to 31, 2021.
Methods: A retrospective cohort study was conducted among 418 newly diagnosed epilepsy patients receiving anti-seizure drugs (ASDs) between July 1, 2014, and July 31, 2019, in two public hospitals in Eastern Ethiopia. Relevant data were collected for all patients with a minimum follow-up period of two years. Data were analyzed using SPSS Version 21. Cox proportional hazards model was performed to identify predictors of seizure remission.
Results: Overall, 252 (60.3%) of the study participants have achieved seizure remission for at least one year. The mean time to achieve seizure remission was 1.9 ± 0.87 years. Regarding the seizure remission pattern, 171 (40.9%) patients achieved early remission, 81 (19.4%) achieved late remission, and 166 (39.7%) achieved no remission. Shorter pre-treatment duration (AHR = 2.36, 95% CI: 1.28– 4.37); good adherence to ASDs (AHR = 2.40, 95% CI: 1.33– 4.34); and monotherapy (AHR = 0.56, 95% CI: 0.32– 0.98) were predictors of seizure remission.
Conclusion: We observed that less than two-thirds of epileptic patients had achieved seizure remission. A shorter pre-treatment duration, good adherence to ASDs, and monotherapy were predictors of seizure remission. Therefore, we recommend the requirement of an integrated effort from different health disciplines that increases patients’ adherence to ASDs, promotes early visits to medical facilities, and improves the health-seeking behavior of epileptic patients.
Keywords: seizure, epilepsy, remission, predictors, Eastern Ethiopia
Introduction
Epilepsy is one of the common chronic neurological disorders with an enduring predisposition to generate epileptic seizures.1,2 Focal onset seizures and generalized onset seizures are common operational classification of epileptic seizures. A focal seizure is a seizure that is confined to a specific area of the brain. Automatisms, behavior arrest, hyperkinetic, autonomic, cognitive, and emotional are the new types of focal seizures. The other types of seizures, such as atonic, clonic, epileptic spasms, myoclonic, and tonic seizures, can be of either focal or generalized onset.3 A generalized onset seizure affects the entire brain at the same time. However, as the classification of seizure is not exclusive, the classification considers the predominant seizure type.4,5 Differentiating between generalized and focal epilepsies is critical because it influences treatment options, investigations, prognoses, and counseling.6
Epilepsy affects individuals of all ages and has a worldwide distribution.7 According to the World Health Organization (WHO), more than 65 million people worldwide are epileptic, of whom an estimated 10.5 million are children.8 The prevalence of epilepsy ranges from 0.5% to 1% of the population in developed countries and is higher in developing countries—nearly threefold higher than in high-income countries—and more than 80% of epileptic patients are currently living in this region.1,9 In Ethiopia, the prevalence of epilepsy ranges from 5.2 to 29.5/1000.10,11
The management of epilepsy involves pharmacologic, non-pharmacological, and surgical methods. Anti-seizure drugs (ASDs) are the cornerstone of pharmacologic epilepsy treatment medications.12 The ultimate goal of epilepsy treatment with ASDs is to achieve seizure remission with the fewest adverse effects and highest level of quality of life.13 Up to 70% of people living with epilepsy can achieve complete seizure remission with appropriate use of ASDs.8 Seizure remission is defined differently throughout the literature, however the most frequently accepted definition is provided by the ILAE and is defined as being free from all types of seizures for at least a year.14
Anti-seizure drugs treatment should begin with a single (monotherapy) agent. Combination therapy can be considered when two attempts at monotherapy with ASDs have not been effective.6 Although, best ASD therapy is dependent on optimal seizure control and absence of unacceptable side effects,15 carbamazepine and valproate are the recommended first-line medication for partial and generalized onset seizures, respectively.16 Due to its adverse effect profile, phenobarbitone is usually considered a second- or third-line option. Newer ASDs such as lamotrigine, levetiracetam, and topiramate should be provided as add-on therapy for patients with medication resistant convulsive epilepsy. Discontinuing anti-seizure medicine can be considered after 2 years without seizures and after examining pertinent clinical, social, and personal considerations.17
Epileptic seizures significantly raise the chance of premature death by two to three times18 and overall mortality by five to seven times.19,20 They also place a heavy burden on the individual and increase the risk of disability, stigma, discrimination, and violations of human rights21 and cause physical and cognitive damage in children, especially when the seizure is not controlled.22 Moreover, the cost of treating epilepsy places a significant financial strain on both the healthcare system and patients.9
Studies carried out across Ethiopia have unequivocally revealed that adherence to ASD is associated with seizure control, making it one of the predictors of seizure control.23–25 However, the previously mentioned research presented erratic results that could differ across different regions regarding factors that determine seizure control, including caregiver relationship,23 gender,24 head injury prior to seizure occurrence and seizure attacks ≥4 episodes/week prior to AEDs initiation,25 as well as a family history of epilepsy and the existence of drug therapy problems.26
Careful identification of the type of epilepsy and its treatment outcome determinants, appropriate pharmacotherapy, and patient adherence to treatment are necessary for seizure remission.27,28 The treatment gaps are found to range from 50% to 75% in developing countries, where nearly 80% of epilepsy sufferers reside.8 This is because of the use of inconsistent treatment protocols, inaccurate epilepsy diagnoses, unsuitable healthcare providers, a lack of modern diagnostic technology, delays in seeking medical attention, and a lack of knowledge.29,30
Although epilepsy is extremely common and there are large treatment gaps in developing nations, including Ethiopia,8,10,11 data on seizure remission and predictors are scarce in these nations in general and in Eastern Ethiopia in particular. Furthermore, there are few studies that focus on seizure remission in Ethiopian children. Therefore, the aim of current study is to assess seizure remission and its predictors among epileptic patients on follow-up at public hospitals in eastern Ethiopia.
Methods
Study Area and Period
The study was conducted from July 2 to 31, 2021, among epileptic patients on follow-up at Hiwot Fana Specialized University Hospital (HFSUH) and Dilchora Referral Hospital (DCRH). HFSUH is found in Harar town, which is located 526 km east of Addis Ababa, the capital city of Ethiopia. HFSUH is one of the oldest hospitals in Ethiopia and currently serves about 5.2 million people around Harar and its surrounding regions. The hospital has 1225 registered epileptic patients for follow-up (HFSUH Statistics and Information Center, unpublished data, 2021). DCRH is located in Dire Dawa city, which is located in the eastern part of the country at 515 km from Addis Ababa. According to Ethiopia’s central statistical agency’s projections for 2013, the total population of Dire Dawa administrative city is 395,000. The hospital has 965 registered epileptic patients on follow-up (Dilchora Referral Hospital Statistics and Information Center, unpublished data, 2021). The two hospitals are organized into different inpatient and outpatient departments or clinics, one of which is the neurologic clinic where this study was conducted.
Study Design
A retrospective cohort study was conducted among epileptic patients in Hiwot Fana Specialized University Hospital (HFSUH) and Dilchora Referral Hospital (DCRH).
Study Population
All epileptic patients who had follow-up at neurologic clinic of HFSUH and DCRH were the source population, while all new patients with epilepsy who had follow-up at neurologic clinic of HFSUH and DCRH from July 1, 2014, to July 31, 2019, were the study population and the document of all patients was reviewed until July 31, 2021.
Sample Size Determination
To determine the sample size, the outcome variable and factors that were significantly associated with poor seizure remission were considered. The sample size for objectives was calculated separately by adding 10% contingency, and the one with the largest number was considered revising works of literature and the following formula:24,31–33

Finally, 418 epileptic patients with complete medical record cards were considered.
Sampling Procedure
Medical cards of patients with epilepsy registered at neurologic clinic of HFSUH and DCRH from July 1, 2014, to July 31, 2019, were reviewed and identified from the patient registration book which was a total of 1452 cases. The sample size was proportionally allotted based on individual hospital case burden (HFSUH = 857, DCRH = 595). Then, the patient’s medical record cards were registered, coded, and entered into a computer program (Microsoft Excel). Finally, applying simple random sampling, a random of 418 medical record cards were generated and considered for data collection (Figure 1).
 |
Figure 1 Sampling procedure among epileptic patients on follow-up in HFSUH and DCRH, Eastern Ethiopia, 2021. |
Data Collection Tool, Collectors and Procedures
Data were collected from the medical records of the patients using a structured data collection format. The format was prepared by reviewing previous studies in consideration of the objective of the study.33–35 The instrument is designed to have different parts: patient demographics (sex, age, family history of epilepsy), disease characteristics (pre-treatment number of seizures, pretreatment duration of epilepsy, etiology, type of epilepsy), neurological examinations, comorbidities, ASD treatments, treatment outcome, treatment adherence, and adverse effect. Three Bachelor of Pharmacy professionals were allocated to each hospital to retrieve the data.
Study Variables
Dependent Variable
- Seizure remission.
Independent Variable
- Socio-demographic variables (Sex, age at diagnosis, family history, occupation, place of residence).
- Disease-related variables (Type of epilepsy, number of pre-treatment seizure, pre-treatment duration, etiology, neurologic examination, and comorbidities).
- Medication-related variables (Type of ASDs, presence of Adverse Drug Reaction (ADR), presence of concurrent medication, and number of medication).
Data Quality Control
The quality of the data was assured by pre-testing the data collection tool, training the data collectors, and supervising the data collection process. Prior to the study period, the instrument was pre-tested on 5% of the sample in the Federal Police Hospital, which is located in Harar City, and amendments were made accordingly. The data collectors were trained on the data collection format and appropriate data recording. Close supervision was maintained by investigators throughout the data collection process by reviewing the completed data collection tools and giving feedback to the data collectors.
Statistical Analyses
Data was checked daily for its completeness. To be edited, cleaned, and analyzed, the collected data was entered into a computer using EPI-Data version 4.2.0.0 and exported to SPSS (IBM SPSS Statistics for Windows, Version 21.0, Armonk, NY: IBM Corp) for analysis. The data was presented using the mean (with SD) and median (with IQR) for continuous variables and frequency for categorical variables. A univariable Cox proportional hazards model was performed to determine the association of each independent variable with seizure remission. Subsequently, variables with a p-value ≤0.25 in the univariate analysis were included in the multivariable Cox proportional hazards model to identify independent predictors of seizure remission. A p-value of <0.05 at 95% CI was used to declare a statistically significant association.
Ethical Considerations
This study was conducted following the Declaration of Helsinki. The study protocol was approved on June 28, 2021, by Haramaya University College of Health and Medical Sciences Institutional Health Research and Ethical Review Committee (IRERC) with the reference number IHRERC/152/2021. After securing ethical clearance, an official letter of cooperation was written to both hospitals by Haramaya University College of Health and Medical Sciences. Since our study was retrospective and based on data gathered from patients’ medical records, we obtained informed, voluntary, written, and signed consent using the Institution Information Sheet and consent form from the hospitals’ medical directors to access the patients’ medical records. The information collected was made anonymous and de-identified prior to analysis to ensure confidentiality.
Operational Definitions
Seizure remission: being free from all types of seizures for at least one year at any point during follow-up period.14 It includes early remission (achievement of remission in the first 6 months) and late remission (achievement of remission later than 6 months after treatment initiation).33
No remission means failure to achieve seizure remission during the entire follow-up period.
Pre-treatment duration: the duration between the onset of seizure and commencement of ASDs.
Adherence to ASDs: It was assessed by using the ten-item medication adherence rating scale (MARS).36 MARS consists of ten items with levelling of 1 = “Yes” and 0 = “No” for all items, and the total score was calculated from 10. Patients who scored below 7 were considered as non-adherent (Poor Adherence) to their ASDs and who score 7 and above were considered to have Good adherence.
Results
Socio-Demographic and Clinical Characteristics of Study Participants
A total of 418 patients who fulfilled the inclusion criteria were considered for the study. Among the participants, 276 (66%) were adults, while 182 (43.5%) of them were older than thirty years of age at the onset of seizure, more than half (56.9%) of them were males, and 246 (58.5%) of them live in urban areas. One hundred ninety-eight (47.4%) of the study participants had no family history of epilepsy. Two hundred sixty-five (63.4%) of the study participants had five or more episodes of epilepsy prior to treatment, while 178 (42.6%) visited hospitals a year after seizure onset. Regarding the type of seizure onset, the majority (64.4%) had generalized seizures, and 29 (6.9%) had focal seizures. The remaining 103 (24.6%) had an unclassified seizure onset. Regarding the use of recreational substances, 177 (42.3%) of them had never used recreational substances. When it comes to the pattern of comorbidities among epileptic patients, the most frequently occurring comorbidities were psychiatric 95 (22.8%), diabetes mellitus 41 (9.9%), and hypertension 29 (6.9%). Asthma, chronic liver disease, congestive heart failure, and HIV comprised the remaining 25 (5.9%). More than two-thirds (71.1%) of the epileptic patients who have been enrolled in the study have never had brain imaging test and only 121 (28.9) had brain imaging test, and the majority (81.8%) of participants have a normal neurologic examination and the remaining 76 (18.2%) have abnormal neurologic examination result (Table 1).
 |
Table 1 Socio-Demographic and Clinical Characteristics of Epileptic Patients on Follow-Up in HFSUH and DCRH, Eastern Ethiopia, 2021 [N = 418] |
Medication Experience of Study Participants
More than two-thirds (72.7%) of the participants were on antiseizure monotherapy. With respect to the type of ASD used during follow-up, phenobarbitone was used by more than two-thirds (73%) of the epileptic patients, with phenytoin, valproate, and carbamazepine being used by 146 (35%), 71 (16%), and 33 (8%), respectively. Almost half of the participants (45.0%) had poor adherence to their ASDs. More than half (55%) of the study participants have never experienced an adverse drug reaction during the follow-up. In terms of the distribution of adverse drug reaction types, sedation was experienced by 64 (34.0%) of the participants, followed by confusion, weakness, rash, gingival hyperplasia, and gastro-intestinal irritation by 55 (29.3%), 42 (22.3%), 14 (7.4%), 8 (4.3%), and 5 (2.7%), respectively. In terms of using additional (concurrent) medications, 236 (56.5%) did not use any, whereas 182 (43.5%) used one or more medications concurrently (Table 1).
Seizure Remission
Overall, 252 (60.3%) of the study participants have achieved seizure remission (seizure free for at least one year) at some point during the follow-up period; while the remaining 166 (39.7%) have failed to achieve seizure remission during the entire follow-up period. The mean (with standard deviation (±SD)) time to achieve remission was 1.9 + 0.87 years. Regarding the seizure remission pattern, 171 (40.9%) achieved early remission, 81 (19.4%) achieved late remission, and 166 (39.7%) achieved no remission (Figure 2). Among 276 adult participants, more than two-thirds (70%) have achieved seizure remission, whereas more than half (59%) of the recruited 142 epileptic children have never achieved remission at the end of follow-up (Figure 3).
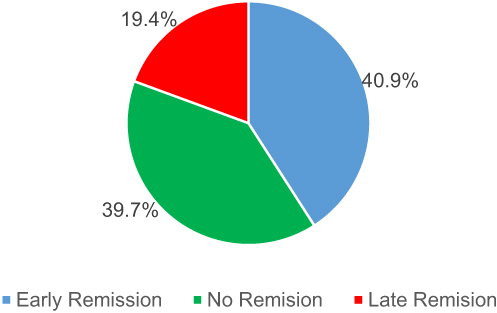 |
Figure 2 Pattern of seizure remission among epileptic patients on follow-up in HFSUH and DCRH, Eastern Ethiopia, 2021 [N = 418]. |
 |
Figure 3 Seizure remission pattern by age group among epileptic patients on follow-up in HFSUH and DCRH, Eastern Ethiopia, 2021 [N = 418]. |
Predictors of Seizure Remission Among Epileptic Patients
In multivariable Cox proportional model pre-treatment duration, adherence to ASDs and number of ASDs used were found to have a significant association with seizure remission. Those participants who had 12 months or shorter pre-treatment duration were 2.36 times more likely to achieve seizure remission than those who had greater than 12 months before commenced on ASDs (AHR = 2.36, 95% CI: 1.28–4.37). Participants who had good adherence to ASDs were 2.4 times more likely to achieve seizure remission in comparison to their counterparts who had poor adherence (AHR = 2.40, 95% CI: 1.33–4.34). The study also demonstrated that epileptic patients who were two or more ASDs were 44% less likely to achieve remission than those who were taking monotherapy (AHR = 0.56, 95% CI: 0.32–0.98) (Table 2).
 |
Table 2 Predictors of Seizure Remission Among Epileptic Patients on Follow-Up in HFSUH and DCRH, Eastern Ethiopia, 2021 [N = 418] |
Discussion
The main objective of the present study was to assess seizure remission and its predictors in epilepsy patients on follow-up at neurologic clinic of HFSUH and DCRH in Eastern Ethiopia.
Out of 418 epileptic patients who took part in the study, 253 (60.3%) have achieved seizure remission (seizure free for at least one year) at some point during the follow-up period. This finding agrees with that of a retrospective cohort study conducted in Southwest Ethiopia (64.6%),33 and a prospective cohort of Scottish patients (63.7%)31 observed levels of remission that were comparable. The outcome of this study, however, was much lower than study conducted in China (80%)37 and only marginally lower than another study done by Shen et al (69.1%).38 The methodological variances such as the definitions used for remission and duration of follow-up, the types of ASDs used, the exclusion of non-adherent patients in some studies, and the potential for genetic diversity, may be the cause of the inconsistencies.33
In the current study, the rate of remission was 70% in adults and only 41% in children. The difference in the etiology of epilepsy between adult and pediatric patients, which may lead to differing seizure remission, may be the cause of this result.39 However, a previous retrospective cohort study conducted in Gondar revealed a far greater remission rate in children (93.5%).24 The prior study has used a shorter (3 month) period of follow-up, which could be the cause of the discrepancy. This is supported by earlier studies that showed controlled seizures may be more likely to occur during shorter follow-up times because over the long run, there is a higher risk of treatment resistance, comorbidity, and exposure to seizure triggers.40,41
Regarding the pattern of seizure remission, 171 (40.9%) participants had early remission, 81 (19.4%) late remission, and 166 (39.7%) achieved no remission. This finding is consistent with earlier studies done in southwest Ethiopia, where 46% of patients experienced early remission, about 18% experienced late remission and 35.4% never achieved seizure remission;33 in China, where 42.6% of patients experienced early remission and 17.5% experienced delayed remission;38 and in Italy, where 43.2% of patients experienced early remission42 during the follow-up period.
However, in earlier studies carried out in China (31%)38 and Scotland (25%),35 the proportion of patients who had never had seizure remission was a little lower than the present study. Many factors might be to account for these disparities. Initially, studies from developing nations revealed a significant prevalence of generalized seizures. For instance, in the present study, the rate of generalized seizures was 68.5%, whiles those of earlier studies from Senegal43 and Gondar, Ethiopia,44 were 72.9% and 78%, respectively. Second, non-adherence to standard treatment guidelines is a common practice in Ethiopian settings.24,45 Although the first-line ASDs for partial and generalized onset seizures, respectively, are carbamazepine and valproate,16 phenobarbitone was most frequently utilized ASD in the current and earlier studies from Ethiopia.24,45 Other explanations for variations might include the existence of high-quality healthcare in affluent nations, the presence of specialists with expertise in treating epilepsy, and the availability and utilization of recommended ASDs.
In this study pre-treatment duration, adherence to ASDs and number of ASDs showed a significant association with seizure remission. Epileptic patients who had 12 months or shorter pre-treatment duration were 2.36 times more likely to achieve remission than those who had greater than 12 months from the onset of seizure to commencing ASDs (AHR = 2.36, 95% CI: 1.28–4.37). This result might be due to the fact that a longer pre-treatment duration may correlate with patients presenting to the health facilities at a later severity of the disease, which is more likely to give a poor response to drug therapy.46 In Ethiopia, where the trend of visiting health facilities is poor among epileptic patients, traditional treatment with local herbs, holy water, and amulets was preferred until the disease reached an advanced state.11 Furthermore, the longer pre-treatment duration might lead to a high number of pre-treatment seizures, which was a predictor of poor seizure remission as reported in previous studies.33,42,47
Patients who had good adherence to anti-epileptics were 2.4 times more likely to achieve remission than those who had poor adherence (AHR = 2.40, 95% CI: 1.33–4.34). Similar finding was reported from other similar studies conducted elsewhere.33,48,49
Epileptic patients who were taking two and more ASDs are 44% less likely to achieve seizure remission than those who were taking monotherapy (AHR = 0.56, 95% CI: 0.32–0.98). This is corroborated by the earlier studies.24,50 This is best explained by the fact that patients on monotherapy are more likely to have good medication adherence due to a lower adverse drug reaction profile and lower cost, which might result in a good treatment outcome;51 additionally, patients on monotherapy are likely to have less severe epilepsy that is responsive to ASDs.38
The strength of the study is that, to the best of the investigators’ knowledge, this is the first study of its kind in Eastern Ethiopia and was conducted in two major public hospitals. Moreover, the study has addressed patients of all age groups. The limitation of the study is that the data gathered from the secondary source was susceptible to missing crucial details like family history because the study was retrospective in nature.
Conclusion and Recommendation
Less than two-thirds of the epileptic patients never achieved remission during the follow-up. A shorter pre-treatment duration, good adherence to ASDs, and monotherapy were predictors of seizure remission. Epileptic patients who are taking more than one ASD, who have more than a year of pre-treatment duration, and who are non-adherent should be addressed with due attention. In addition, health professionals should stress the importance of adherence to achieve seizure remission from ASDs during counseling sessions. Awareness-creation activities should be conducted through different routes of communication as they may improve the health-seeking behavior of epileptic patients and enable them to visit health facilities early.
Data Sharing Statement
Please contact the corresponding author for data requests.
Acknowledgment
The authors would like to thank the hospital officials, data collectors and hospital staffs for their contribution.
Author Contributions
All authors made a significant contribution to the work reported whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receiving financial support from Haramaya University for conducting this research work.
Disclosure
The authors have declared that there is no conflicts of interest in this work.
References
1. De Boer HM, Mula M, Sander JW. The global burden and stigma of epilepsy. Epilepsy Behav. 2008;12(4):540–546. doi:10.1016/j.yebeh.2007.12.019
2. Fisher RS, Boas WVE, Blume W, et al. Epileptic seizures and epilepsy: definitions proposed by the International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE). Epilepsia. 2005;46(4):470–472. doi:10.1111/j.0013-9580.2005.66104.x
3. Fisher RS, Cross JH, French JA, et al. Operational classification of seizure types by the International League Against Epilepsy: position paper of the ILAE Commission for Classification and Terminology. Epilepsia. 2017;58(4):522–530. doi:10.1111/epi.13670
4. Devinsky O, Vezzani A, O’Brien TJ, et al. Epilepsy. Nat Rev Dis Primers. 2018;4:18024. doi:10.1038/nrdp.2018.24
5. Fisher RS, Acevedo C, Arzimanoglou A, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. 2014;55(4):475–482. doi:10.1111/epi.12550
6. Epilepsy implementation task force. Provincial guidelines for the management of epilepsy in adults and children. Version 1.0. Critical Care Services Ontario; 2015.
7. Neligan A, Hauser WA, Sander JW. The epidemiology of the epilepsies. Handb Clin Neurol. 2012;107:113–133.
8. World Health Organization. Epilepsy: A Public Health Imperative. Geneva, Switzerland: World Health Organization; 2019:171.
9. Fodjo JNS, Mandro M, Wonya’rossi D, et al. Economic burden of epilepsy in rural Ituri, Democratic Republic of Congo. EClinicalMedicine. 2019;9:60–66. doi:10.1016/j.eclinm.2019.03.010
10. Tekle‐Haimanot R, Forsgren L, Ekstedt J. Incidence of epilepsy in rural central Ethiopia. Epilepsia. 1997;38(5):541–546. doi:10.1111/j.1528-1157.1997.tb01138.x
11. Worku D. Review article: epilepsy in Ethiopia. Am Acad Neurol. 2013;80(7):10–1212.
12. DiPiro JT, Wells BG, Schwinghammer TL, DiPiro CV. Pharmacotherapy Handbook.
13. Kerr M, Scheepers M, Arvio M, et al. Consensus guidelines into the management of epilepsy in adults with an intellectual disability. J Intell Disabil Res. 2009;53(8):687–694. doi:10.1111/j.1365-2788.2009.01182.x
14. Kwan P, Arzimanoglou A, Berg AT, et al. Definition of Drug Resistant Epilepsy: Consensus Proposal by the Ad Hoc Task Force of the ILAE Commission on Therapeutic Strategies. Wiley Online Library; 2010.
15. Glauser T, Ben‐Menachem E, Bourgeois B, et al. ILAE treatment guidelines: evidence‐based analysis of antiepileptic drug efficacy and effectiveness as initial monotherapy for epileptic seizures and syndromes. Epilepsia. 2006;47(7):1094–1120. doi:10.1111/j.1528-1167.2006.00585.x
16. Food Medicine Health Administration and Control Authority. Ethiopian Standard Treatment Guidelines for General Hospitals.
17. World Health Organization. Anti-Epileptic Medicines for Medication Resistant Convulsive Epilepsy. Swiztherland, Geneva: World Health Organization; 2015.
18. Neligan A, Bell GS, Johnson AL, Goodridge DM, Shorvon SD, Sander JW. The long-term risk of premature mortality in people with epilepsy. Brain. 2011;134(2):388–395. doi:10.1093/brain/awq378
19. Bruno E, Nimaga K, Foba I, et al. Results of an action-research on epilepsy in rural Mali. PLoS One. 2012;7(8):e44469. doi:10.1371/journal.pone.0044469
20. Sperling MR. The consequences of uncontrolled epilepsy. CNS Spectr. 2004;9(2):98–109. doi:10.1017/S1092852900008464
21. Golyala A, Kwan P. Drug development for refractory epilepsy: the past 25 years and beyond. Seizure. 2017;44:147–156. doi:10.1016/j.seizure.2016.11.022
22. Laxer KD, Trinka E, Hirsch LJ, et al. The consequences of refractory epilepsy and its treatment. Epilepsy Behav. 2014;37:59–70. doi:10.1016/j.yebeh.2014.05.031
23. Abiy H, Shiferaw Z, Tafere Y. Clinical outcome and its associated factors among children with meningitis admitted in Debre Markos Comprehensive Specialized Hospital, Northwest Ethiopia, 2019. Int J Nurs Care Res. 2023;1(1):1–6.
24. Beyene A, Ayalew AF, Mulat G, Simachew Kassa A, Birhan T, Russo E. The treatment outcomes of epilepsy and its root causes in children attending at the University of Gondar teaching hospital: a retrospective cohort study, 2018. PLoS One. 2020;15(3):e0230187. doi:10.1371/journal.pone.0230187
25. Zewudie A, Mamo Y, Feyissa D, Yimam M, Mekonen G, Abdela A. Epilepsy treatment outcome and its predictors among ambulatory patients with epilepsy at Mizan-Tepi University Teaching Hospital, southwest Ethiopia. Neurol Res Int. 2020;2020:1–8. doi:10.1155/2020/8109858
26. Bekele F, Gezimu W. Treatment outcome and associated factors among epileptic patients at ambulatory clinic of Mettu Karl Comprehensive Specialized Hospital: a cross-sectional study. SAGE Open Med. 2022;10:20503121221125149. doi:10.1177/20503121221125149
27. Krumholz A, Wiebe S, Gronseth GS, et al. Evidence-based guideline: management of an unprovoked first seizure in adults: report of the guideline development subcommittee of the American Academy of Neurology and the American Epilepsy Society: evidence-based guideline. Epilepsy Curr. 2015;15(3):144–152. doi:10.5698/1535-7597-15.3.144
28. Radhakrishnan K. Challenges in the management of epilepsy in resource-poor countries. Nat Rev Neurol. 2009;5(6):323–330. doi:10.1038/nrneurol.2009.53
29. Desjarlais RR. World Mental Health: Problems and Priorities in Low-Income Countries. USA: Oxford University Press; 1995.
30. Panahi S, Aram Z, Jafari S, Ma J, Sprott JC. Modeling of epilepsy based on chaotic artificial neural network. Chaos Solitons Fractals. 2017;105:150–156. doi:10.1016/j.chaos.2017.10.028
31. Chen Z, Brodie MJ, Liew D, Kwan P. Treatment outcomes in patients with newly diagnosed epilepsy treated with established and new antiepileptic drugs: a 30-year longitudinal cohort study. JAMA Neurol. 2018;75(3):279–286. doi:10.1001/jamaneurol.2017.3949
32. Ethiopia CSA. Population Projection of Ethiopia for All Regions at Wereda Level from 2014–2017. Addis Ababa: Agency CS; 2013.
33. Gidey K, Chelkeba L, Gemechu TD, Daba FB. Treatment response and predictors in patients with newly diagnosed epilepsy in Ethiopia: a retrospective cohort study. Sci Rep. 2019;9(1):1–7. doi:10.1038/s41598-019-52574-y
34. Ashmawi A, Hosny H, Abdelalim A, Bianchi E, Beghi E. The long-term prognosis of newly diagnosed epilepsy in Egypt: a retrospective cohort study from an epilepsy center in Greater Cairo. Seizure. 2016;41:86–95. doi:10.1016/j.seizure.2016.07.016
35. Brodie MJ, Barry SJE, Bamagous GA, Norrie JD, Kwan P. Patterns of treatment response in newly diagnosed epilepsy. Neurology. 2012;78(20):1548–1554. doi:10.1212/WNL.0b013e3182563b19
36. Thompson K, Kulkarni J, Sergejew AA. Reliability and validity of a new Medication Adherence Rating Scale (Mars) for the psychoses. Schizophr Res. 2000;42(3):241–247. doi:10.1016/S0920-9964(99)00130-9
37. Zhang Y, Yu N, Su L, Di Q. A prospective cohort study of prognosis for newly diagnosed epilepsy in east China. BMC Neurol. 2013;13(1):1–8. doi:10.1186/1471-2377-13-116
38. Shen C, Du Y, Lu R, et al. Factors predictive of late remission in a cohort of Chinese patients with newly diagnosed epilepsy. Seizure. 2016;37:20–24. doi:10.1016/j.seizure.2016.02.007
39. Yazie TS, Kefale B, Molla M, Biagini G. Treatment outcome of epileptic patients receiving antiepileptic drugs in Ethiopia: a systematic review and meta-analysis. Behav Neurol. 2021;2021:1–11. doi:10.1155/2021/5586041
40. Niriayo YL, Mamo A, Kassa TD, et al. Treatment outcome and associated factors among patients with epilepsy. Sci Rep. 2018;8(1):1–9. doi:10.1038/s41598-018-35906-2
41. Tigistu M, Azale T, Kebebe H, Yihunie T. Frequency of seizure attack and associated factors among patients with epilepsy at University of Gondar Referral Hospital: a cross-sectional study, Gondar, North West Ethiopia, 2017. BMC Res Notes. 2018;11(1):1–6. doi:10.1186/s13104-018-3761-3
42. Del Felice A, Beghi E, Boero G, et al. Early versus late remission in a cohort of patients with newly diagnosed epilepsy. Epilepsia. 2010;51(1):37–42. doi:10.1111/j.1528-1167.2009.02141.x
43. Ndoye NF, Sow AD, Diop AG, et al. Prevalence of epilepsy its treatment gap and knowledge, attitude and practice of its population in sub-urban Senegal an ILAE/IBE/WHO study. Seizure. 2005;14(2):106–111. doi:10.1016/j.seizure.2004.11.003
44. Birru EM, Shafi M, Geta M. Drug therapy of epileptic seizures among adult epileptic outpatients of University of Gondar Referral and Teaching Hospital, Gondar, North West Ethiopia. Neuropsychiatr Dis Treat. 2016;12:3213–3219. doi:10.2147/NDT.S119030
45. Gurshaw M, Agalu A, Chanie T. Anti-epileptic drug utilization and treatment outcome among epileptic patients on follow-up in a resource poor setting. J Young Pharm. 2014;6(3):47. doi:10.5530/jyp.2014.3.8
46. Rogawski MA, Johnson MR. Intrinsic severity as a determinant of antiepileptic drug refractoriness. Epilepsy Curr. 2008;8(5):127–130. doi:10.1111/j.1535-7511.2008.00272.x
47. Gilad R, Lampl Y, Gabbay U, Eshel Y, Sarova-Pinhas I. Early treatment of a single generalized tonic-clonic seizure to prevent recurrence. Arch Neurol. 1996;53(11):1149–1152. doi:10.1001/archneur.1996.00550110089017
48. Gabr WM, Shams MEE. Adherence to medication among outpatient adolescents with epilepsy. Saudi Pharm J. 2015;23(1):33–40. doi:10.1016/j.jsps.2014.05.003
49. Hovinga CA, Asato MR, Manjunath R, et al. Association of non-adherence to antiepileptic drugs and seizures, quality of life, and productivity: survey of patients with epilepsy and physicians. Epilepsy Behav. 2008;13(2):316–322. doi:10.1016/j.yebeh.2008.03.009
50. Nasir BB, Yifru YM, Engidawork E, Gebrewold MA, Woldu MA, Berha AB. Antiepileptic drug treatment outcomes and seizure-related injuries among adult patients with epilepsy in a tertiary care hospital in Ethiopia. Patient Relat Outcome Meas. 2020;11:119–127. doi:10.2147/PROM.S243867
51. Nevitt S, Sudell M, Weston J, Tudur Smith C, Marson AG. Antiepileptic drug monotherapy for epilepsy: a network meta-analysis of individual participant data. Cochrane Database Syst Rev. 2017. doi:10.1002/14651858.CD011412.pub2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.