")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Secreted Frizzled-Related Protein 5 is Associated with Glucose and Lipid Metabolism Related Metabolic Syndrome Components Among Adolescents in Northeastern China
Authors Bai Y, Du Q, Jiang R, Zhang L, Du R , Wu N , Li P , Li L
Received 13 January 2021
Accepted for publication 4 March 2021
Published 17 June 2021 Volume 2021:14 Pages 2735—2742
DOI https://doi.org/10.2147/DMSO.S301090
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Yu Bai,1 Qiang Du,1 Ranhua Jiang,2 Le Zhang,1 Runyu Du,1 Na Wu,1 Ping Li,1 Ling Li1
1Department of Endocrinology, Shengjing Hospital of China Medical University, Shenyang, Liaoning Province, People’s Republic of China; 2Department of Endocrinology, Liaoyang Diabetes Hospital, Liaoyang, Liaoning Province, People’s Republic of China
Correspondence: Ling Li
Department of Endocrinology, Shengjing Hospital of China Medical University, No. 36, Sanhao Street, Heping District, Shenyang, Liaoning Province, 110004, People’s Republic of China
Tel +86 189 4025 1181
Fax +86 24 2594 4460
Email [email protected]
Purpose: Secreted frizzled-related protein 5 (SFRP5) is a novel anti-inflammatory adipokine that has been associated with various metabolic diseases. However, such relationship among adolescents remains unclear. The purpose of this study was to clarify the relationship between SFRP5 and the components of metabolic syndrome in Chinese adolescents.
Patients and Methods: In this cross-sectional study, we included a total of 684 adolescents aged 11– 16 years old from Liaoyang city, Liaoning province, China. The ELISA kits were implemented to measure the plasma SFRP5 and high-sensitivity C-reactive protein. Serum total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), triglycerides (TG), and high-density lipoprotein cholesterol (HDL-C), serum uric acid (UA), alanine aminotransferase (ALT), aspartate aminotransferase (AST), fasting plasma glucose (FPG), and fasting serum insulin (FINS) were also measured.
Results: The multivariate logistic regression analysis showed that low SFRP5 level were an independent risk factor of high FPG [odds ratio (OR)=5.31, 95% confidence interval (CI): 1.85– 15.22, P< 0.01] and high TC (OR=1.73, 95% CI: 1.01-2.96, P< 0.05) when adjusting for age, sex, family history of diabetes, body mass index, and high-sensitivity C-reactive protein.
Conclusion: The lower level of SFRP5 is strongly related to lipid and glucose metabolism among adolescents in Northeast China. The risk of high fasting plasma glucose and high total cholesterol increases significantly as the plasma SFRP5 level decreases.
Keywords: adolescents, secreted frizzled-related protein 5, metabolic syndrome, hyperglycemia, dyslipidemia
Introduction
Metabolic syndrome (MetS), also known as syndrome X, is a complex disorder characterized by dyslipidemia, hyperglycemia, central adiposity, and hypertension.1,2 As a combination of multiplex factors disease, MetS is associated with increased risk of cardiovascular atherosclerotic disease and type 2 diabetes mellitus.2,3 As the main determinants of MetS, obesity and overweight have demonstrated an alarming rate of increase in the incidence worldwide.4 In China, a recent study has revealed an increasing trend of the overweight and obese population.5 Between 2010–2016, the overweight incidence raised from 27.8% to 33.5%, and the obese rate increased from 5.4% to 7.0% in China. The substantial growth of the overweight and obesity population in China is accompanied by an increase in the MetS prevalence, which is estimated to be 15.5% in 2017.6 MetS among children and adolescents seeds the risk of cardiovascular disease in adulthood, the most common cause of mortality among adults.7 Due to the lack of consensus diagnostic guidelines, the prevalence of MetS in the pediatric population varied substantially when defined differently.7 Currently, the guideline developed by the International Diabetes Organization (IDF) in 2007 is widely accepted.
Adipocyte dysfunction has been suggested to play a prominent role in the pathogenesis of MetS.8 Once considered a storage organ, the adipocyte is now found to participate actively in human metabolism as an endocrine organ.9 A variety of bioactive substances are produced by the adipocytes, including hormones, growth factors, enzymes, cytokines, matrix proteins, and complement factors.9 The inclined secretion of pro-inflammatory cytokines and adipokines, such as interleukin-6 (IL-6), tumor necrosis factor α (TNF-α), angiotensin II, and monocyte chemoattractant protein-1 (MCP-1), disrupts the glucose and lipid homeostasis and induced inflammatory response, which contributes to the components of MetS, including hyperglycemia, dyslipidemia, and hypertension.2,7,10,11
Secreted Frizzled-related proteins 5 (SFRP5), an anti-inflammatory adipokine involving the Wnt signaling pathway regulation, is secreted in a substantial amount in the white adipose tissue.12 The Wnt signaling pathway partakes in the progression of cardiovascular disease and causes pleiotropic metabolic dysfunctions.13,14 Since SFRP5 inhibits the Wnt signaling pathway, protective effects of SFRP5 on metabolic abnormalities has been established.12 Previous studies have discovered a significantly reduced circulating SFRP5 level among participants diagnosed with type 2 diabetes and obesity.15,16 The protective effect of SFRP5 on MetS has been examined in vitro,17 animal,18 and adult human studies.19 However, the relationship between SFRP5 and MetS elements has not been revealed among children and adolescents in China. Therefore, this research aimed to examine the association between SFRP5 level and MetS components in Chinese adolescents.
Patients and Methods
Study Design
This cross-sectional study recruited a total of 945 adolescents aged 11–16 years in Liaoyang city, Liaoning province, China, from December 2010 to January 2011 using a cluster stratified random sampling method. This study was conducted in accordance with the Declaration of Helsinki, the ethnics of which were approved by the Education Committee of Liaoyang City and the Ethics Committee of Shengjing Hospital Affiliated to China Medical University. Signed informed consent was obtained from all study participants and parents or guardians.
Of the 945 adolescents, participants with anemia, current prescription medication use, current dietary restriction, sever illness that impaired organ functioning, and missing information in sex, age, weight, height, and biochemical samples were excluded. In total, 684 participants who reported complete information were included in the analysis of this study.
Anthropometric Measurement
Participants were asked to avoid vigorous exercise for least 30 minutes before the physical examination. Height, weight, waist circumference, hip circumference, and blood pressure of the study participants were measured by trained physicians and medical school students. Weight was measured to the nearest 0.1 kg by a digital scale, while height was measured to the nearest 1 cm by a stadiometer. Participants were wearing light clothing with no shoes on during the physical examination. The body mass index (BMI) was calculated using body weight and height measures (kg/m2). The waist circumference was obtained by measuring the midpoint of the 12th rib lower edge and the sacral spine lines using a non-elastic tape. Hip circumference was determined by measuring the horizontal circumferences between the anterior superior iliac crests. Waist and hip circumference were measured to the nearest 5 mm. The waist-hip ratio was acquired by dividing hip circumference by waist circumference (waist circumference/hip circumference). After 10 minutes of rest, systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured twice using a mercury sphygmomanometer. The average of the two measurements was determined as the blood pressure of the study participant. Caffeinated beverages consumption was forbidden before measuring the blood pressure.
Biochemical Analysis
Five mL blood sample was collected from the study participant after overnight fasting for at least 10 hours. The blood sample was analyzed in the Liaoyang Diabetes Hospital Laboratory. Serum total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), triglycerides (TG), and high-density lipoprotein cholesterol (HDL-C) were examined by the enzymatic test within 1 hour after blood sample collection and centrifuging. Measurements of serum uric acid (UA), alanine aminotransferase (ALT), aspartate aminotransferase (AST), and fasting plasma glucose (FPG) were collected. Radioimmunoassay (Beijing China Institute of Atomic Energy) was used to determine the fasting serum insulin (FINS). The homeostasis model assessment of insulin resistance (HOMA-IR) index was calculated as HOMA-IR= FPG (mmol/L) × FINS (μU/L)/22.5, the normal range of which was between 2.30–3.59.20 The steady-state model to evaluate insulin secretion (HOMA-β) was calculated as HOMA-β= 20×FINS/(FPG-3.5), the reference range of which varied from 72.5 to 133.09.21–23 The SFRP5 levels and high-sensitivity C-reactive protein (hs-CRP) were measured using the ELISA kits (Wuhan Youersheng Trading Co., Ltd, Wuhan, China).
MetS Components Definition
We determined metabolic abnormalities based on the multiple criteria of children and adolescents, including guidelines provided by the National Heart, Lung, and Blood Institution, American Heart Association, International Diabetes Foundation, and Group of China Obesity Task Force.24–26 In this research, the cutoffs of abnormal MetS components were defined as: (i) Overweight (BMI ≥85th percentile) or obesity (BMI ≥95th percentile). (ii) Hyperglycemia: FPG ≥5.6 mmol/L or diagnosed type 2 diabetes. (iii) High blood pressure: SBP ≥130 mmHg or DBP ≥85 mmHg. (iv) Dyslipidemia: HDL-C <1.03 mmol/L for all participants aged 10–15 years and male ≥16 years old, HDL-C <1.29 mmol/L for female ≥16 years old; TG ≥1.70 mmol/L or receiving treatment for dyslipidemia; TC and LDL-C ≥95th percentile. (v) Abnormal liver function: ALT ≥95th percentile or AST ≥95th percentile. (vi) Hyperuricemia: UA ≥360 μmol/L or receiving treatment for hyperuricemia.
Statistical Analysis
All analyses were carried out using SPSS 16.0 (SPSS, Inc., Chicago, IL, USA). Normally distributed variables were expressed in means and standard deviations (mean ± SD), while non-normally distributed variables were displayed in medians and interquartile ranges M [Qlower, Qupper]. Categorical variables were shown as numbers and percentages (n%) and were compared by the chi-square test. Comparisons between groups were made by ANOVA or Kruskal–Wallis H-test. The multivariate logistic regression analysis was performed to investigate the correlation between SFRP5 and components of MetS. The odds ratio (OR) and the 95% confidence interval (CI) were also obtained. A P value less than 0.05 was considered statistically significant.
Results
Baseline Characteristics
Baseline characteristics of the study participants were summarized in Table 1. The average age and BMI were 13.71 ± 1.40 years and 21.50 ± 4.12 kg/m2. There were 371 males of the included individuals, corresponding to 54.24% of the population. Dyslipidemia was observed in 498 participants, demonstrating the highest incidence among all MetS components. The lowest incidence was observed in liver dysfunction, corresponding to 30 cases of the total population.
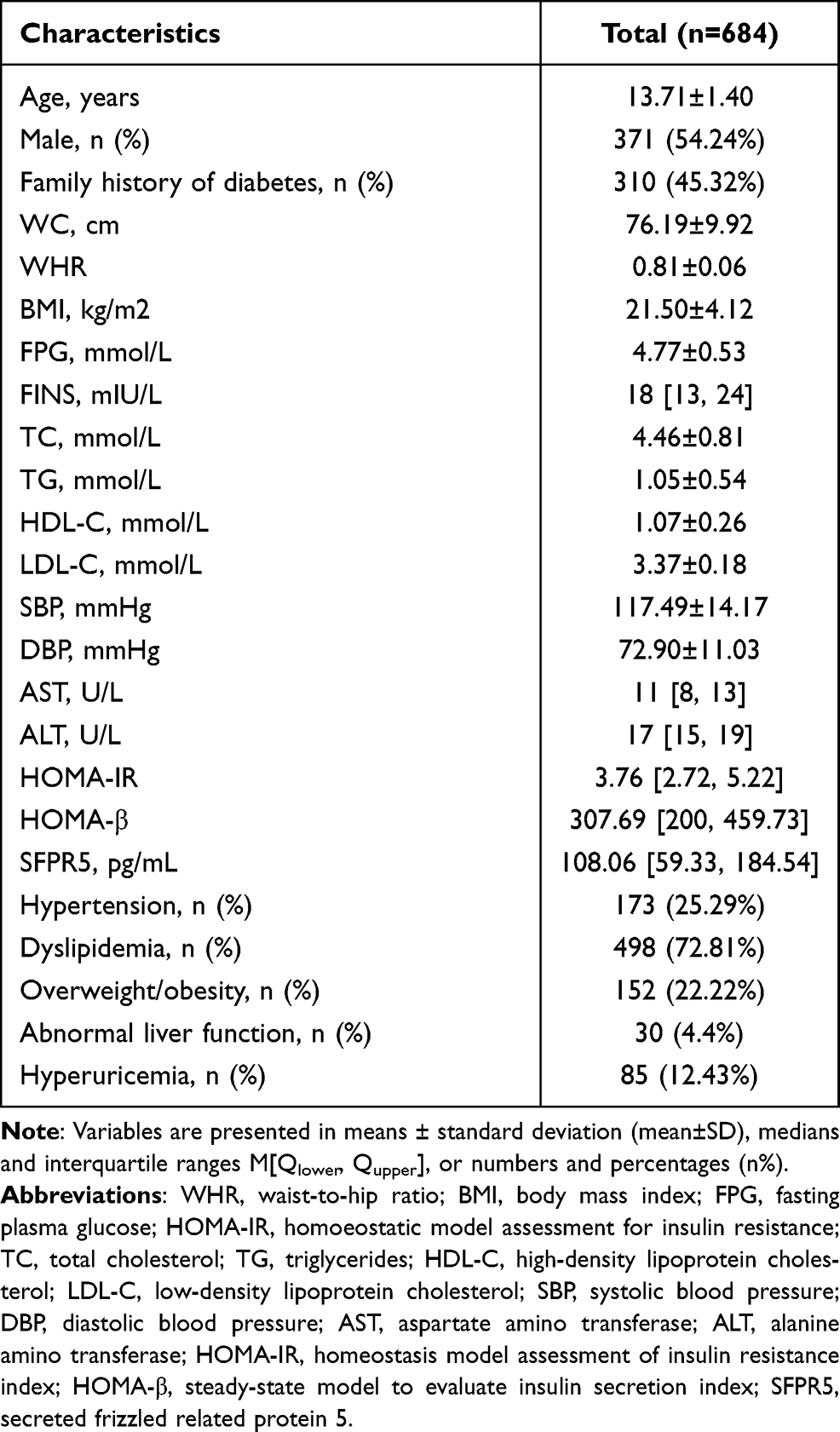 |
Table 1 Characteristics of Study Participants |
Since SFPR5 distributed non-normally, it was divided into tertiles and presented in the median and interquartile range, as shown in Table 2. In this adolescent population, the SFPR5 level ranged from 19.82 pg/mL to 625.85 pg/mL with a median at 108.06 pg/mL. The median and the interquartile range of each tertile was 265.19 (184.36–397.69) pg/mL in tertile 1 (T1), 107.71 (87.42–133.82) pg/mL in tertile 2 (T2), and 43.60 (36.66–59.83) pg/mL in tertile 3 (T3). Across all tertiles, the proportion of males was higher than the proportion of females (P<0.001). Age was significantly different among the tertiles (P=0.005), with T3 demonstrating the greatest mean age (13.95 ± 1.46 years) and T2 showing the lowest mean age (13.53 ± 1.40 years). The means of SBP (P=0.022) and DBP (P=0.022) were also different among the tertiles, with T2 indicating the highest mean while T1 showing the lowest mean. Additionally, TG was the highest in T1, 1.11 ± 0.57 mmol/L, while the lowest in T3, 0.98 ± 0.49 mmol/L, (P=0.046). The lowest FPG was observed in T3 (4.66 ± 0.47 mmol/L), and the highest FPG was found in T1 (4.84 ± 0.53 mmol/L, P=0.001).
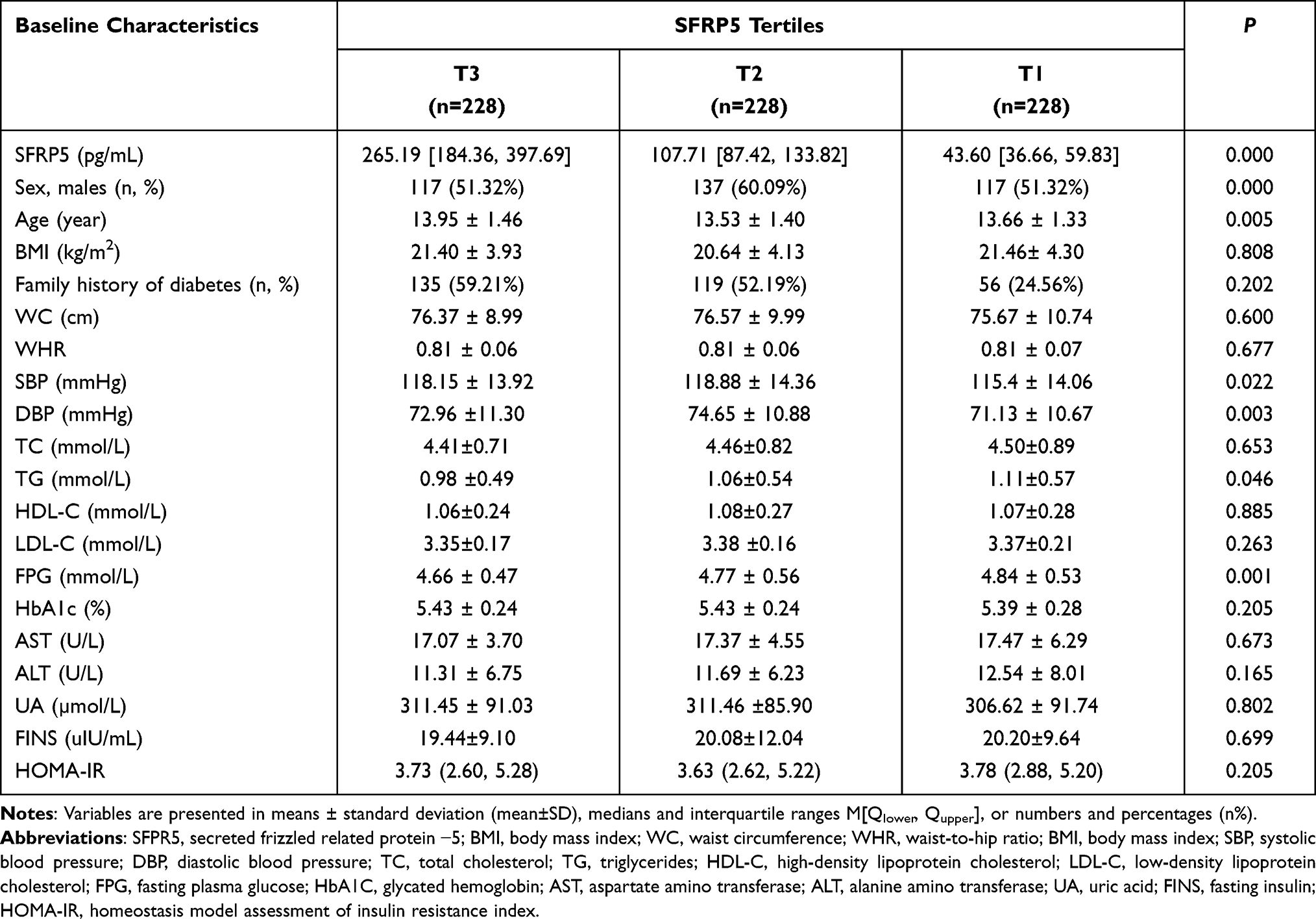 |
Table 2 Baseline Characteristics of the Study Participants by SFRP5 Tertiles |
Plasma SFPR5 and MetS Components
In the logistic regression model adjusting for age and sex (Table 3), T3 was set as the reference group of all analyses. A significantly increased risk of elevated TC was observed in T1 comparing to T3 (OR=1.98, 95% CI: 1.20–3.26, P<0.01). Moreover, the incidence of hyperglycemia raised dramatically in T1 (OR= 4.29, 95% CI: 1.58–11.63, P<0.05) and T2 (OR=5.00, 95% CI: 1.87–13.41, P<0.01) when comparing to T3. Conversely, no statistical differences were discovered in the risk of hypertension, elevated TG, elevated LDL-C, decreased HDL-C, hyperglycemia, overweight and obesity, impaired renal function, and hyperuricemia as the plasma SFRP5 level decreased.
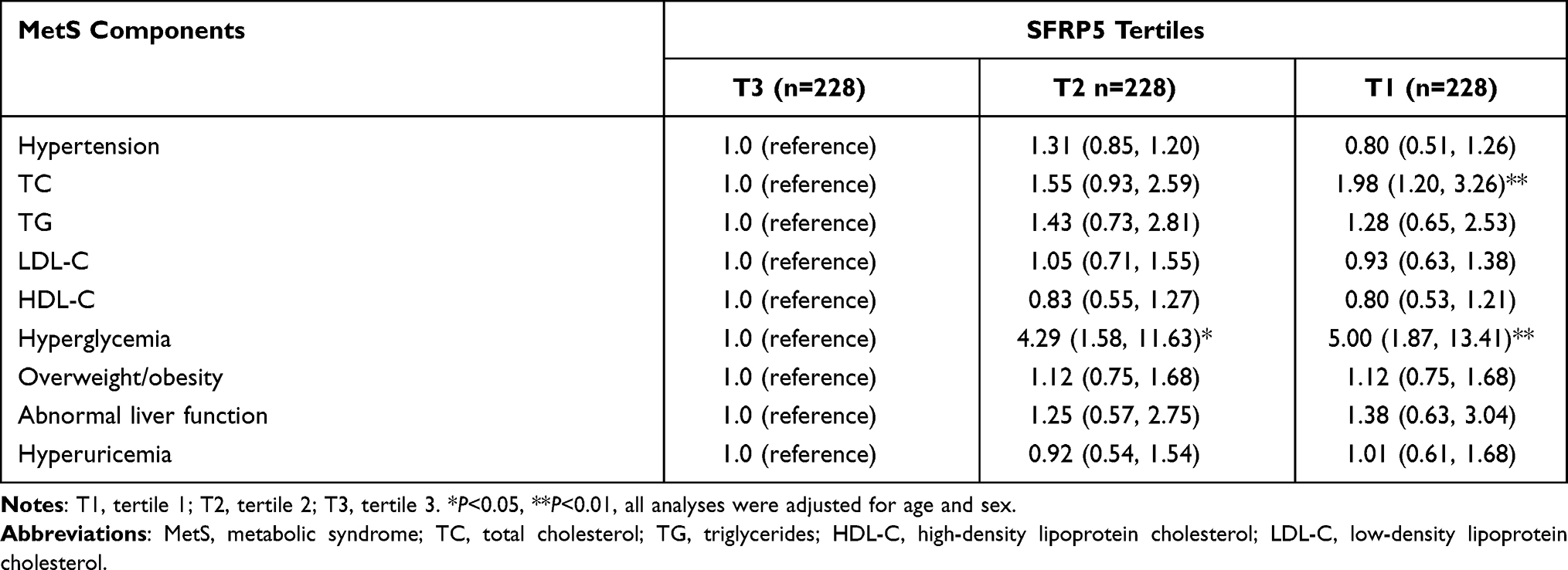 |
Table 3 The Association Between the SFRP5 Level and Components of MetS |
A further examination of the influence of SFRP5 on FPG and TC was conducted using multivariate logistic regression models (Table 4). Five different models were implemented, adjusting potential covariates incrementally from model 1 to model 4 and 5. Model 1 only adjusted for age and sex, and model 2 added the family history of diabetes. Model 3 included all potential covariates in model 2 with additional consideration of BMI. Model 4 controlled for age, sex, family history of diabetes, BMI, and HOMA-IR, while model 5 adjusted for age, sex, family history of diabetes, BMI, and hs-CRP.
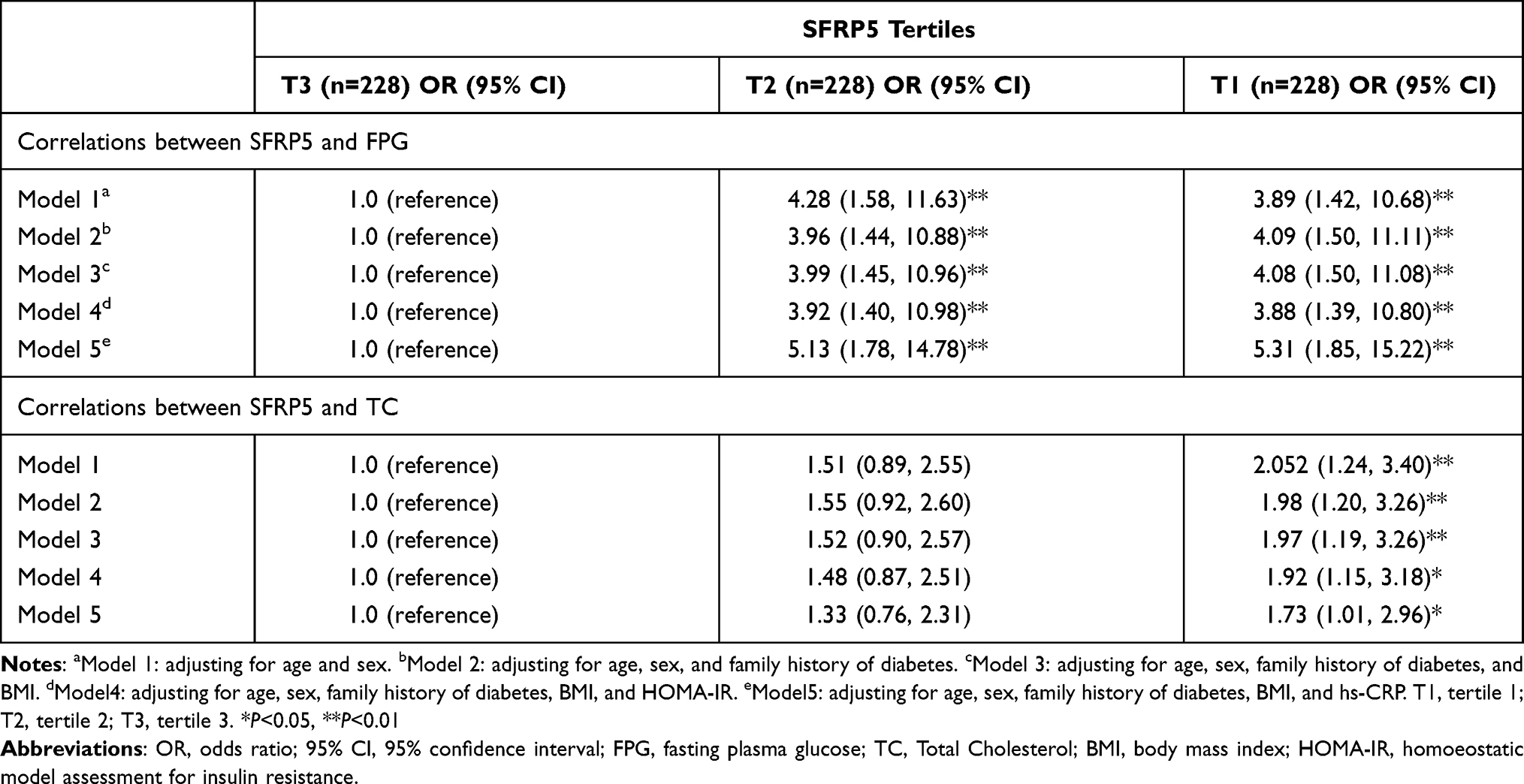 |
Table 4 The Multivariate Logistic Regression Models of FPG and TC Analyses |
When comparing to the reference T3, the risk of elevated FPG was significantly higher in T1 and T2 in all five models. Model 5 displayed the greatest increase in the risk of elevated FPG in T1 (OR=5.31, 95% CI:1.85–15.22, P<0.01) and T2 (OR=5.13, 95% CI: 1.78–14.78, P<0.01) among the five models. For T2, the risks of high FPG in model 1 was (OR=4.28, 95% CI: 1.58-11.63, P<0.01), model 2 was (OR=3.96, 95% CI: 1.44-10.88, P<0.01), model 3 was (OR=3.99, 95% CI: 1.45-10.96, P<0.01), and model 4 was (OR=3.92, 95% CI: 1.40-10.98, P<0.01). For T3, the ORs from model 1 to model 4 were 3.89, 4.09, 4.08, and 3.88, respectively.
In the TC analysis, the increased risk of high TC was observed in T3 but not in T2 across all five models. The OR decreased as more potential covariates being controlled, with model 1 demonstrating the highest OR of high TC (OR= 2.052, 95% CI: 1.24–3.40, P<0.01) and model 5 displaying the lowest OR (OR=1.73, 95% CI: 1.01-2.96, P<0.05). High TC risk was also significantly higher in model 2 (OR=1.98, 95% CI: 1.20-3.26, P<0.01), model 3 (OR=1.97, 95% CI: 1.19-3.26, P<0.01), and model 4 (OR=1.92, 95% CI: 1.15-3.18, P<0.05).
Discussion
Our research examined the association between SFRP5 level and components of MetS, overweight, hyperglycemia, high blood pressure, dyslipidemia, abnormal liver function, hyperuricemia, in Chinese adolescents for the first time. The findings of the current study suggest a significant influence of plasma SFRP5 level on lipid metabolism, as well as glucose metabolism among Chinese adolescents. The low plasma SFRP5 group demonstrated significantly higher odds of elevated TC than the high plasma SFRP5 group, the risk of which increased approximately 2 folds. A more significant relationship was observed between the plasma SFRP5 level and hyperglycemia incidence. The risk of hyperglycemia increased 4.29 times in T2 as compared to T3 and raised to 5 folds in T1. Our results uncovered that lower level of SFRP5 was an independent risk factor of hyperglycemia and high TC, the mechanism of which might be related to the Wnt signaling pathway.27 SFRP5 has been found to bind to Wnt5a as an inhibitor, down-regulating the Wnt/JNK signaling pathway, suppressing the production of TNF-α, MCP-1, and IL-6, reducing chronic inflammation, and improving insulin sensitivity.28 Additionally, SFRP5 downregulates Peroxisome Proliferator-activated Receptor Gamma (PPAR-γ) and Ccaat-Enhancer-Binding-Protein Alpha (CEBPα) expression, two genes that are essential for lipid production. Mori et al clarified that SFRP5/Wnt signaling promoted adipocyte growth and lipid accumulation by inhibiting mitochondrial oxidative metabolism.29
Variables, including BMI, family history of diabetes, HOMA-IR, and hs-CRP, were strongly associate with the predictive variable or the outcome variables.15,30–32 Therefore, we created several multivariate logistic regression models adjusting for these variables to minimize the influence of potential covariates. We implemented all five models to further examine the effect of SFRP5 on TC and FPG. Similar to the model that controlled for age and sex, the odds of high TC and high FPG increased significantly in the low plasma SFRP5 group. Moreover, the incidence of elevated FPG increased in both T2 and T1, while high TC odds only increased in T1 when compared to T3, demonstrating a similar pattern to the previous age-sex-adjusted model. Interestingly, the occurrence of high TC displayed a decremental change as more potential covariates being controlled, while the incidence of high TC remained significantly higher in the low plasma SFRP5 group than the reference group after adjusting for multiple covariates, implying that the SFRP5 level was an independent predictor of the risk of high TC and the potential covariates impacted the association to some degree.
Although the relationship between the serum SFRP5 level and MetS components has barely been studied in children and adolescents, the connection has been established in multiple previous adult studies. A previous study recruited 284 middle-aged adults in China to examine the relationship between the plasma SFRP5 level and the determinants of MetS.19 The fasting plasma SFRP5 concentration was significantly lower among participants with MetS than the controls in their study, ascertaining the role SFRP5 played in the pathogenesis of MetS. In terms of the MetS components, Lu et al found that the SFRP5 level was higher in patients diagnosed with type 2 diabetes than that in the control group. The SFRP5 level was positively correlated with fasting hyperglycemia in diabetic patients,33 which was allied with findings in our study.
The KORA F4 study in Germany characterized the relationship between serum SFRP5 level and cardiometabolic risk factors, as well as identified the effect of serum SFRP level on the odds of hyperglycemia and obesity.34 The researchers found an inverse association between SFRP5 levels and the risk of cardiovascular risk factors. Independently from BMI, a high level of SFRP was also associated with a low incidence of prediabetes and type 2 diabetes.
Yin et al examined the plasma SFRP5 level in relation to blood pressure among obese adolescents.30 Their cross-sectional study observed significantly lower mean plasma SFRP5 levels in obese adolescents with hypertension than obese adolescents without hypertension. As an inflammatory marker, the SFRP5 level was negatively associated with SBP and DBP values. However, the correlation was not detected in our research.
Despite the differences in sample size and study population, the cross-sectional design may also contribute to the discrepancies between our results and previous findings, which is one limitation of our research. Researchers have proposed that the SFRP5 expression increases transiently to alleviate metabolic abnormalities at the early stage of the disease, while the SFRP5 is downregulated in response to serious obesity-related metabolic dysfunctions, implying a potential fluctuation in the SFRP5 level during metabolic disease progression.35 Therefore, a future longitudinal study is required to investigate the possible variation of the SFRP5 level among patients at different disease stages. Another limitation of this research is the study population. We recruited Chinese adolescents in Northeastern China, the population of which consists of Asians exclusively. Thus, the results need a comprehensive interpretation when generalizing to other ethnic groups.
Conclusion
Our study discovers that the plasma SFRP5 level is associated with high fasting plasma glucose and total cholesterol. The lower level of SFRP5 is strongly related to lipid and glucose metabolism among Chinese adolescents. As the plasma SFRP5 level decreases, the risk of hyperglycemia and high total cholesterol increases approximately 5 folds and 2 folds, respectively. Future longitudinal researches on children and adolescents are needed to address potential variations of SFRP5 level during MetS progression and to consider the possible physiological changes during human development.
Funding
This study was supported by the 345-talent project plan of Shengjing Hospital of China Medical University and the Department of Education Foundation of Liaoning Province [grant numbers L2015568].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Saklayen MG. The global epidemic of the metabolic syndrome. Curr Hypertens Rep. 2018;20(2):1–8. doi:10.1007/s11906-018-0812-z
2. Kassi E, Pervanidou P, Kaltsas G, Chrousos G. Metabolic syndrome: definitions and controversies. BMC Med. 2011;9(1):48. doi:10.1186/1741-7015-9-48
3. Sherling DH, Perumareddi P, Hennekens CH. Metabolic syndrome. J Cardiovasc Pharmacol Ther. 2017;22(4):365–367. doi:10.1177/1074248416686187
4. Chooi YC, Ding C, Magkos F. The epidemiology of obesity. Metabolism. 2019;92:6–10. doi:10.1016/j.metabol.2018.09.005
5. Wang Yiru WC. Study on the trend and influencing factors of overweight and obesity in Chinese adults under interactions of individual and environment. Prog Geogr. 2020;39(1):100–110. doi:10.18306/dlkxjz.2020.01.010
6. Wang Y, Mi J, Shan X-Y, Wang QJ, Ge K-Y. Is China facing an obesity epidemic and the consequences? The trends in obesity and chronic disease in China. Int J Obes. 2007;31(1):177–188.
7. Wittcopp C, Conroy R. Metabolic syndrome in children and adolescents. Pediatr Rev. 2016;37(5):193–202. doi:10.1542/pir.2014-0095
8. Kadowaki T, Yamauchi T, Kubota N, Hara K, Ueki K, Tobe K. Adiponectin and adiponectin receptors in insulin resistance, diabetes, and the metabolic syndrome. J Clin Invest. 2006;116(7):1784–1792. doi:10.1172/JCI29126
9. Coelho M, Oliveira T, Fernandes R. Biochemistry of adipose tissue: an endocrine organ. Arch Med Sci. 2013;9(2):191–200. doi:10.5114/aoms.2013.33181
10. Weihe P, Weihrauch-Blüher S. Metabolic syndrome in children and adolescents: diagnostic criteria, therapeutic options and perspectives. Curr Obes Rep. 2019;8(4):472–479. doi:10.1007/s13679-019-00357-x
11. Jung UJ, Choi M-S. Obesity and its metabolic complications: the role of adipokines and the relationship between obesity, inflammation, insulin resistance, dyslipidemia and nonalcoholic fatty liver disease. Int J Mol Sci. 2014;15(4):6184–6223.
12. Ouchi N, Higuchi A, Ohashi K, et al. Sfrp5 is an anti-inflammatory adipokine that modulates metabolic dysfunction in obesity. Science. 2010;329(5990):454–457. doi:10.1126/science.1188280
13. Abou Ziki MD, Mani A. The interplay of canonical and non-canonical Wnt signaling in metabolic syndrome. Nutr Res. 2019;70:18–25. doi:10.1016/j.nutres.2018.06.009
14. Gay A, Towler DA. Wnt signaling in cardiovascular disease: opportunities and challenges. Curr Opin Lipidol. 2017;28(5):387–396. doi:10.1097/MOL.0000000000000445
15. Hu Z, Deng H, Qu H. Plasma SFRP5 levels are decreased in Chinese subjects with obesity and type 2 diabetes and negatively correlated with parameters of insulin resistance. Diabetes Res Clin Pract. 2013;99(3):391–395. doi:10.1016/j.diabres.2012.11.026
16. Cheng L, Zhang D, Chen B. Declined plasma sfrp5 concentration in patients with type 2 diabetes and latent autoimmune diabetes in adults. Pak J Med Sci. 2015;31(3):602–605. doi:10.12669/pjms.313.6964
17. Carstensen M, Wiza C, Röhrig K, et al. Effect of Sfrp5 on cytokine release and insulin action in primary human adipocytes and skeletal muscle cells. PLoS One. 2014;9(1):e85906. doi:10.1371/journal.pone.0085906
18. Carstensen-Kirberg M, Röhrig K, Niersmann C, et al. Sfrp5 increases glucose-stimulated insulin secretion in the rat pancreatic beta cell line INS-1E. PLoS One. 2019;14(3):e0213650. doi:10.1371/journal.pone.0213650
19. Xu Q, Wang H, Li Y, et al. Plasma Sfrp5 levels correlate with determinants of the metabolic syndrome in Chinese adults. Diabetes Metab Res Rev. 2017;33(6):e2896. doi:10.1002/dmrr.2896
20. Arellano-Ruiz P, García-Hermoso A, Cavero-Redondo I, Pozuelo-Carrascosa D, Martínez-Vizcaíno V, Solera-Martinez M. Homeostasis model assessment cut-off points related to metabolic syndrome in children and adolescents: a systematic review and meta-analysis. Eur J Pediatr. 2019;178(12):1813–1822. doi:10.1007/s00431-019-03464-y
21. Sung K-C, Reaven GM, Kim SH. Utility of homeostasis model assessment of beta-cell function in predicting diabetes in 12,924 healthy Koreans. Diabetes Care. 2010;33(1):200–202. doi:10.2337/dc09-1070
22. Ghasemi A, Tohidi M, Derakhshan A, Hasheminia M, Azizi F, Hadaegh F. Cut-off points of homeostasis model assessment of insulin resistance, beta-cell function, and fasting serum insulin to identify future type 2 diabetes: Tehran Lipid and Glucose Study. Acta Diabetol. 2015;52(5):905–915. doi:10.1007/s00592-015-0730-3
23. Yoon H, Jeon DJ, Park CE, You HS, Moon AE. Relationship between homeostasis model assessment of insulin resistance and beta cell function and serum 25-hydroxyvitamin D in non-diabetic Korean adults. J Clin Biochem Nutr. 2016;59(2):139–144. doi:10.3164/jcbn.15-143
24. Zimmet P, Alberti KGM, Kaufman F, et al. The metabolic syndrome in children and adolescents – an IDF consensus report. Pediatr Diabetes. 2007;8(5):299–306. doi:10.1111/j.1399-5448.2007.00271.x
25. Group of China Obesity Task Force. Body mass index reference norm for screening overweight and obesity in Chinese children and adolescents. Zhonghua Liu Xing Bing Xue Za Zhi. 2004;25(2):97–102.
26. Alberti KGMM, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640–1645. doi:10.1161/CIRCULATIONAHA.109.192644
27. Ehrlund A, Mejhert N, Lorente-Cebrián S, et al. Characterization of the Wnt inhibitors Secreted Frizzled-Related Proteins (SFRPs) in human adipose tissue. J Clin Endocrinol Metab. 2013;98(3):E503–E508. doi:10.1210/jc.2012-3416
28. Liu L-B, Chen X-D, Zhou X-Y, Zhu Q. The Wnt antagonist and secreted frizzled-related protein 5: implications on lipid metabolism, inflammation, and type 2 diabetes mellitus. Biosci Rep. 2018;38(4). doi:10.1042/BSR20180011
29. Mori H, Prestwich TC, Reid MA, et al. Secreted frizzled-related protein 5 suppresses adipocyte mitochondrial metabolism through WNT inhibition. J Clin Invest. 2012;122(7):2405–2416. doi:10.1172/JCI63604
30. Yin C, Chu H, Li H, Xiao Y. Plasma Sfrp5 and adiponectin levels in relation to blood pressure among obese children. J Hum Hypertens. 2017;31(4):284–291. doi:10.1038/jhh.2016.76
31. Anthanont P, Ramos P, Jensen MD, Hames KC. Family history of type 2 diabetes, abdominal adipocyte size and markers of the metabolic syndrome. Int J Obes. 2017;41(11):1621–1626. doi:10.1038/ijo.2017.171
32. Hu X, Yu W, Yang L, et al. The association between first-degree family history of diabetes and metabolic syndrome. Endocr Pract. 2019;25(7):678–683.
33. Lu Y-C, Wang C-P, Hsu -C-C, et al. Circulating secreted frizzled-related protein 5 (Sfrp5) and wingless-type MMTV integration site family member 5a (Wnt5a) levels in patients with type 2 diabetes mellitus. Diabetes Metab Res Rev. 2013;29(7):551–556. doi:10.1002/dmrr.2426
34. Carstensen-Kirberg M, Kannenberg JM, Huth C, et al. Inverse associations between serum levels of secreted frizzled-related protein-5 (SFRP5) and multiple cardiometabolic risk factors: KORA F4 study. Cardiovasc Diabetol. 2017;16:1–10. doi:10.1186/s12933-017-0591-x
35. Tong S, Ji Q, Du Y, Zhu X, Zhu C, Zhou Y. Sfrp5/Wnt pathway: a protective regulatory system in atherosclerotic cardiovascular disease. J Interferon Cytokine Res. 2019;39(8):472–482. doi:10.1089/jir.2018.0154
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.