Back to Journals » Journal of Hepatocellular Carcinoma » Volume 8
Second-Line Treatment Options for Hepatocellular Carcinoma: Current Landscape and Future Direction
Received 9 July 2021
Accepted for publication 31 August 2021
Published 21 September 2021 Volume 2021:8 Pages 1147—1158
DOI https://doi.org/10.2147/JHC.S268314
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmed Kaseb
Surabhi Pathak,1 Mohamad Bassam Sonbol2
1Hematology-Oncology, King’s Daughters Medical Center, Ashland, KY, USA; 2Division of Hematology/Oncology, Department of Internal Medicine, Mayo Clinic Cancer Center, Phoenix, AZ, USA
Correspondence: Mohamad Bassam Sonbol
Department of Internal Medicine, Division of Medical Oncology, Mayo Clinic Cancer Center, 5777 East Mayo Boulevard, Phoenix, 85054, USA
, AZ Tel +1 480-342-4800
Fax +1 480-301-4675
Email [email protected]
Abstract: Hepatocellular carcinoma is a leading cause of mortality worldwide, and its incidence is rising. The last few years have witnessed a proliferation of available systemic therapeutic options, with the approval of multiple agents, including immune checkpoint inhibitors and drugs targeting vascular endothelial growth factor, such as cabozantinib, regorafenib, and ramucirumab. Most recently, the combination of atezolizumab plus bevacizumab has resulted in the longest overall survival yet known in hepatocellular carcinoma, therefore changing the preferred first-line treatment from the previous options of sorafenib and lenvatinib. The aim of this review is to summarize the available clinical data for the current second-line systemic treatment options and the future perspectives in the treatment landscape of hepatocellular carcinoma.
Keywords: hepatocellular carcinoma, atezolizumab, sorafenib, second-line
Introduction
Worldwide, hepatocellular carcinoma (HCC) remains a leading cause of mortality, with increasing incidence in the western hemisphere.1,2 It is estimated that more than 42,000 new liver cancers will be diagnosed in the USA in 2021, of which three-fourths will be HCC.3 Surgical resection is reserved for patients with preserved liver function and early-stage tumor, while ablation or transarterial therapies are options for patients with early and intermediate-stage tumors who are not surgical candidates.4,5 The majority are diagnosed at advanced stages; therefore, systemic therapy is a common treatment modality. Conventional cytotoxic chemotherapy has poor activity in HCC and is seldom utilized.6 Sorafenib, a multiple tyrosine kinase inhibitor (TKI), was the first targeted therapy to show activity in advanced HCC. The phase III placebo-controlled SHARP trial showed an improvement in overall survival (OS) and time to progression of around 3 months,7 and was granted United States Food and Drug Administration (US FDA) approval for first-line treatment of advanced HCC in 2007. Multiple other drugs were evaluated with negative results, until 2018 when, in the phase III REFLECT trial, lenvatinib, another multiple kinase inhibitor, demonstrated non-inferiority to sorafenib for OS (13.6 vs 12.7 months; HR=0.92, 95% CI 0.79–1.06).8 Since 2017, FDA has granted approvals to regorafenib, ramucirumab, and cabozantinib for advanced HCC following progression on sorafenib. The landscape of systemic therapy for advanced HCC has drastically changed since the IMbrave150 trial results in 2020.9 In this phase III multicenter trial, a combination of atezolizumab, a programmed death ligand 1 (PD-L1) inhibitor, and bevacizumab, an anti-vascular endothelial growth factor (VEGF) monoclonal antibody, was compared to sorafenib for the first-line systemic therapy of advanced HCC. At a median follow-up of 15.6 months, median OS was 19.2 months with atezolizumab plus bevacizumab compared to 13.4 months with sorafenib, which is the longest reported survival in the front-line setting.10 In this paper, we review the clinical data for the current options and offer future perspectives for the second-line treatment of advanced HCC.
Options After Sorafenib
VEGF inhibitors and immune checkpoint inhibitors (ICIs) are the two major classes of therapeutic drugs available for use following progression on sorafenib. Hepatocarcinogenesis involves aberrations in the intracellular signaling pathways containing tyrosine kinases such as MAPK and PI3K/mTOR that are involved in angiogenesis, tumor growth, and metastases, making them attractive molecular therapeutic targets.11,12 HCC has an immune-rich microenvironment, although the tumor mutational burden (TMB) is moderate to low.13 CD8+ T cells have been detected in blood samples of patients with HCC, while the tumor microenvironment is enriched with exhausted tumor-infiltrating lymphocytes,14 suggesting dampening of the antitumor immune response and potential for the efficacy of ICIs.15,16
The currently available options in the second-line setting include two TKIs, cabozantinib and regorafenib, one anti-VEGF monoclonal antibody, ramucirumab, and three ICIs, nivolumab, pembrolizumab, and ipilimumab (Table 1).
 |
Table 1 Pivotal Clinical Trials of the Currently Approved Systemic Therapy Options for Second-Line Treatment in Hepatocellular Carcinoma |
Regorafenib
Regorafenib was the first TKI approved for use after progression on sorafenib in HCC. It is a multikinase inhibitor with antiangiogenic, antitumor, and immune activities through inhibition of the receptors for VEGF, platelet-derived growth factor (PDGF), and fibroblast growth factor (FGF), and oncogenic kinases KIT, RET, and B-RAF.17 In a phase II study of patients with Barcelona Clinic Liver Cancer (BCLC) stage B or C HCC and Child–Pugh A liver function, regorafenib demonstrated clinical activity18 with acceptable tolerability. This led to the RESORCE study, a randomized double-blind, phase III trial which assessed the efficacy of regorafenib compared to placebo in patients with HCC after progression on sorafenib.19 Inclusion criteria were BCLC stage B or C HCC and Child–Pugh A liver function. Patients who did not previously tolerate sorafenib were excluded. Patients were stratified based on geographic location (Asia vs rest of world), alpha-fetoprotein (AFP) concentration (<400 or ≥400 ng/mL), macrovascular invasion, and extrahepatic disease. The primary endpoint was OS and the secondary endpoints included progression-free survival (PFS), time to progression, objective response rate (ORR), and disease control rate (DCR). The regorafenib arm had significantly better median OS compared to placebo, with median OS of 10.6 vs 7.8 months, respectively (HR=0.61, 95% CI 0.50–0.75).20 Median PFS was 3.4 months for regorafenib and 1.5 months in the placebo arm (HR=0.43, 95% CI 0.35–0.52). The DCR was also better in the regorafenib arm (65% vs 36%; p<0.0001). Benefit was observed across all stratified groups. Exploratory analysis of the RESORCE trial for the sequential treatment of sorafenib followed by regorafenib showed a median OS from the time of sorafenib initiation of 26 months for the regorafenib arm and 19.2 months for the placebo arm (HR=0.62, 95% CI 0.50–0.78).21 Based on these data, regorafenib was approved by the US FDA in April 2017 for patients with advanced HCC who progressed on prior sorafenib.22
The most common grade 3/4 adverse events of regorafenib were palmar–plantar erythrodysesthesia (13%), hypertension (13%), fatigue (5%), and diarrhea (3%). Dose-escalation strategies to minimize the risk of serious toxicities that lead to drug discontinuation have been studied in metastatic colon cancer and may be extrapolated to the treatment of HCC.23 For example, the ReDOS study of weekly dose escalation of regorafenib versus standard daily dose in metastatic colorectal cancer showed a higher rate of treatment continuation in the weekly escalation arm, while maintaining clinical efficacy.24
Cabozantinib
Cabozantinib is an inhibitor of multiple tyrosine kinases with activities against VEGF-1, 2, and 3, MET, RET, KIT, and AXL receptors.25,26 In preclinical models, cabozantinib inhibited tumor angiogenesis, cell growth, and metastases.27 Sorafenib-induced antiangiogenesis and tissue hypoxia is associated with upregulation of MET signaling, potentially decreasing its efficacy.28,29 Given its activity against VEGF and MET signaling pathways, cabozantinib was evaluated in the second-line treatment of advanced HCC after progression on sorafenib. In a phase II study, cabozantinib demonstrated clinical activity in HCC with a DCR of 66% and an AFP response of more than 50%.30 A subsequent phase III randomized, double-blind trial, CELESTIAL, compared cabozantinib to placebo in the second- or third-line setting in patients with HCC who were previously treated with sorafenib.26,31 All 707 participants had preserved liver function with Child–Pugh A, except for nine patients who had Child–Pugh B. Stratification was based on disease etiology, geographic region, and extrahepatic tumor spread. The primary endpoint of median OS was significantly longer in the cabozantinib arm compared to placebo (10.2 vs 8 months; HR=0.76, 95% CI 0.63–0.92; p=0.005). The secondary endpoints of PFS (5.2 vs 1.9 months; HR=0.44, 95% CI 0.36–0.52; p<0.001) ORR (4% vs <1%; p=0.009), and DCR (64% vs 33%) were also better in the cabozantinib arm compared to placebo. Similarly, cabozantinib showed efficacy in PFS and OS across all prespecified subgroups of race, geographic region, AFP level, age, etiology of the disease, extrahepatic tumor spread, and macrovascular invasion. Grade 3 or 4 adverse events were reported in 68% of the participants in the cabozantinib arm and 36% in the placebo arm. Treatment discontinuation due to adverse events was reported in 16% in the cabozantinib arm and 3% in the placebo arm. The most common grade 3 or 4 adverse events causing dose reductions were palmar–plantar erythrodysesthesia, hypertension, elevated hepatic enzymes, and diarrhea. Cabozantinib was approved by the US FDA in January 2019 for advanced HCC in patients who have been previously treated with sorafenib.
In a post-hoc analysis of the CELESTIAL trial, those who received at least one transarterial chemoembolization (TACE) treatment had a median OS of 11.4 months with cabozantinib versus 8.6 months with placebo.32 The efficacy of cabozantinib persisted irrespective of the duration of sorafenib use, although better survival was observed following a longer period of sorafenib use. Those with more than 6 months’ treatment duration with sorafenib had a median OS of 29.9 months with cabozantinib compared to 25.8 months with placebo.33 A post-hoc analysis of patients whose Child–Pugh deteriorated from A to B within 8 weeks post-randomization revealed better OS with cabozantinib compared to placebo (8.5 vs 3.8 months; HR=0.32, 95% CI 0.18–0.58)34 and similar rates of adverse events and dose reductions to Child–Pugh A. CELESTIAL allowed patients with more than one previous line of systemic therapy, making cabozantinib the only drug with proven efficacy beyond the second-line setting.
Ramucirumab
Ramucirumab is a fully human immunoglobulin G1 (IgG1) monoclonal antibody that has antiangiogenic and antitumor effects through inhibition of tyrosine kinase VEGF-A by binding to its receptor, VEGFR-2.35 It is the only biomarker-guided approved therapy for HCC with clinical efficacy in patients with elevated AFP. In a phase II study, ramucirumab showed activity in the first-line treatment of HCC. The study included patients with Child–Pugh A or B liver function and revealed a median OS of 4.4 months (95% CI 0.5–9.0) for Child–Pugh B and 18 months (95% CI 6.1–23.5) for Child–Pugh A liver function on ramucirumab. Grade 3 or higher adverse effects included hypertension (14%), gastrointestinal bleeding (7%), and fatigue (5%).36 Subsequently, ramucirumab monotherapy was compared to placebo in a phase III randomized, double-blind trial (REACH trial), which included 565 patients with BCLC stage B or C HCC who progressed or were intolerant to sorafenib and had Child–Pugh A liver function. The trial failed to meet its primary endpoint and no improvement in OS or PFS with ramucirumab was observed in the overall study population. However, in the prespecified subgroup analysis of patients with AFP of ≥400 ng/mL, ramucirumab improved OS compared to placebo (7.8 vs 4.2 months, HR=0.67, 95% CI 0.51–0.90; p=0.006). Therefore, the activity of ramucirumab was further investigated among patients with AFP of ≥400 ng/mL. REACH-2 was a phase III randomized placebo-controlled trial that assessed the efficacy of ramucirumab monotherapy in 292 patients with HCC after progression on sorafenib and AFP ≥400 ng/mL.37 The study showed statistically significant improvement in survival in the ramucirumab group compared to the placebo group, with median OS of 8.5 vs 7.3 months, respectively (HR=0.71, 95% CI 0.5–0.9; p=0.01). Similarly, PFS was better in the ramucirumab arm (2.8 vs 1.6 months; HR=0.452, 95% CI 0.3–0.60; p<0.0001). While ORR did not differ between the two arms, DCR was higher in the ramucirumab arm compared to placebo (59.9% vs 38.9%; p=0.0006). Grade 3 or higher adverse effects included hypertension (13%), hyponatremia (11%), and elevated aspartate transaminase (3%). A pooled analysis of the REACH and REACH-2 trials of 542 patients with AFP ≥400 ng/mL revealed a median OS of 8.1 months with ramucirumab compared to 5 months with placebo (HR=0.69, 95% CI 0.5−0.84; p=0.0002).38 ORR was 5.4% with ramucirumab compared to 0.9% with placebo (p=0.004), DCR was also better with ramucirumab (56.3% vs 37.2%; p<0.0001). Based on these data, ramucirumab was approved by the FDA in May 2019 for patients who have been previously treated with sorafenib and have an AFP level ≥400 ng/mL.39
Immunotherapy
Single-Agent Checkpoint Inhibitors
Nivolumab
CheckMate 040 (NCT01658878) is a phase I/II dose escalation and expansion trial, evaluating nivolumab, a programmed death-1 receptor (PD-1) inhibitor, in patients with advanced HCC and Child–Pugh A liver function in six cohorts: sorafenib-intolerant or -untreated, non-hepatitis B virus (HBV)- or hepatitis C virus (HCV)-infected, previously sorafenib-treated, HBV-infected, HCV-infected, sorafenib-naive or exposed Child–Pugh B HCC, randomized to different combinations of nivolumab with cabozantinib.40 Patients with HBV were required to be on antiviral agents. The dose-escalation phase had 48 patients while the dose-expansion phase included 214 patients using a dose of 3 mg/kg every 2 weeks. The primary endpoints were safety and tolerability for the dose-escalation phase and ORR for the expansion phase. ORR was 15% in the dose-escalation phase and 20% in the dose-expansion phase. A durable response was observed in more than 50% of the responders, with a median duration of response of 16.6 months. Median duration of response (DOR) was as high as 18 months in the dose-escalation phase. Common adverse events included rash (23%), elevation in liver enzymes (21%), and pruritus (19%). No differences in adverse events based on viral etiology were identified. Based on these results, in 2017 the US FDA granted accelerated approval, conditional on further confirmatory results, to nivolumab as a second-line option after progression on sorafenib. Most recently, the results of cohort 5 of this study were presented. This cohort included 25 sorafenib-naïve and 24 sorafenib-treated patients with advanced HCC and Child–Pugh B liver function. At a median follow-up of 16.3 months, nivolumab monotherapy showed a DCR of 55% and an ORR of 12%.41
Since nivolumab showed an ORR of 23% in the treatment-naïve patients, its potential as a first-line systemic treatment compared to sorafenib was evaluated in the phase III CheckMate 459 trial.40 It included 743 patients with advanced HCC and no prior systemic therapy, with the primary endpoint of OS. Unfortunately, the study results were negative and nivolumab failed to show superiority compared to sorafenib, with median OS of 16.4 and 14.7 months, respectively (HR=0.85, 95% CI 0.72–1.02; p=0.0725). The ORR was 15% for nivolumab compared to 7% in the sorafenib arm.40 Given the negative results of the CheckMate 459 and low ORR, ongoing approval was reviewed in April 2021 by the FDA’s oncological drug advisory committee, which voted against maintaining the accelerated approval of nivolumab for second-line treatment following progression on sorafenib.
Pembrolizumab
The efficacy of pembrolizumab in HCC was suggested in the open-label phase II KEYNOTE-224 study, which enrolled 104 patients with Child–Pugh A liver function, BCLC C or B stage HCC, following progression or intolerance to sorafenib.42 Patients with chronic hepatitis B or C were included; those with HBV were required to be on antiviral therapy and have a viral load of <100 IU/mL. The ORR was 17% and DCR was 62%, with a median DOR that was not reached. Based on these results, in 2018 the US FDA granted accelerated approval to pembrolizumab for advanced HCC after progression on sorafenib. The early promising results led to the confirmatory phase III trial (KEYNOTE-240), which randomized 413 patients to pembrolizumab or placebo after progression on sorafenib43 with prespecified cut-offs for statistical significance (p=0.0174 for OS and p=0.002 for PFS). Unfortunately, the study did not meet its primary endpoint and pembrolizumab failed to show superiority compared to placebo in terms of OS (13.9 vs 10.6 months; HR=0.78; p=0.02) and PFS (3 vs 2.8 months; HR=0.77; p=0.01). The ORR was 18.3% for pembrolizumab and DCR was 62.2%. On post-hoc analysis when controlling for subsequent anticancer therapies including TKIs, median OS was longer in the pembrolizumab arm compared to placebo (3.9 vs 9.3 months; HR=0.67, 95% CI 0.48–0.92; p=0.0066). Further data from a similar phase III KEYNOTE-394 trial testing pembrolizumab after progression on sorafenib in Asian patients are awaited. In April 2021, the FDA’s oncological drug advisory committee reviewed its approval in HCC and voted to maintain the accelerated approval of pembrolizumab based on the paucity of options for those ineligible for bevacizumab, based on front-line approval for atezolizumab plus bevacizumab, and also since the results from KEYNOTE-394 are still awaited.
Dual Checkpoint Inhibitors
Preclinical studies indicate that the use of CTLA-4 inhibitors combined with PD-1/PD-L1 inhibitors leads to an increase in CD4+ T-effector cells and a decline in inhibitory Treg cells, indicating a complementary activity of the combination.44 Clinical studies of the dual checkpoint inhibitor combinations in various cancers such as melanoma have reported better ORRs and survival outcomes with the dual ICIs compared to single-agent ICIs,45,46 and therefore the combinations have been investigated in advanced HCC as well.
Nivolumab ± Ipilimumab
Based on the results of nivolumab monotherapy in the CheckMate 040 trial, its efficacy in combination with the CTLA-4 inhibitor ipilimumab was further investigated in another arm of the study.47 Here, 148 patients were randomized to various dose combinations of the two drugs. The ORR was between 31% and 32% (n=16; 95% CI 20–48) across all arms, with DOR ranging between 4.6 and 30.5 months. Responses were observed regardless of PD-L1 status. Patients who had a complete/partial response had substantially improved OS compared to those with stable/progressive disease. Differences in OS based on ipilimumab dosing were observed, with the best OS observed in the arm with nivolumab 1 mg/kg plus ipilimumab 3 mg/kg every 3 weeks for four doses, then nivolumab 240 mg every 2 weeks. Combination treatment had more serious adverse events compared to the monotherapy arm, with nivolumab treatment; however, the frequency of such events was consistent with the adverse events noted in other dual checkpoint inhibitor trials. Based on these results, the combination of nivolumab and ipilimumab was approved by the FDA in March 2020 for patients with HCC who were previously treated with sorafenib. These results suggest the potential for better outcomes using dual checkpoint inhibitors compared to monotherapy. A phase III trial of this combination in first-line treatment in comparison to sorafenib or lenvatinib is ongoing (NCT04039607).
Durvalumab ± Tremelimumab
Tremelimumab is a fully human IgG2 monoclonal antibody that inhibits cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), which plays a role in enhancing T-cell activation and proliferation. In a pilot study of 21 patients with chronic hepatitis C and HCC, the antitumoral effects of tremelimumab were investigated.48 Patients had Child–Pugh A or B liver function, and previous treatment with sorafenib was allowed. Tremelimumab was associated with a DCR of 76.4% with a median time to progression of 6.4 months (95% CI 3.95–9.14). The activity of tremelimumab was also investigated in combination with durvalumab (anti-PD-1) in study 22, which was an open-label four-part multi-center phase II trial (NCT02519348). The first part of the study evaluated the safety and efficacy of the combination, with no reported unexpected safety signals.49 Parts 2 and 3 evaluated durvalumab monotherapy, tremelimumab monotherapy, and combination therapy. The results of the safety and efficacy of the part 2 and 3 arms investigating combination durvalumab and tremelimumab were presented at the annual meeting of American Society of Clinical Oncology (ASCO), 2020.50 A total of 332 patients with advanced HCC who were intolerant, had progressed, or had refused sorafenib were randomized to one of the four arms: two arms containing a combination of durvalumab with two different doses of tremelimumab and two arms utilizing single-agent tremelimumab or durvalumab. Similarly to previous results from a combination of nivolumab and ipilimumab in advanced HCC,51 the arm containing a higher dose of tremelimumab in combination with durvalumab had the highest ORR (22.7%) and median OS (18.7 months; 95% CI 10.8–not reached) at the time of data cut-off. However, this arm also had a higher incidence of grade 3 or 4 treatment-related adverse events (35.1%) compared to the arm with the lower tremelimumab dose in the combination (24.4%). Following these encouraging results, a phase III study, HIMALAYA (NCT03298451), is evaluating durvalumab and tremelimumab in combination in front-line treatment compared to sorafenib, and the results are expected in late 2021.
Other Immunotherapy Combinations
Sintilimab and Bevacizumab
Sintilimab, an anti-PD-1 antibody, in combination with a bevacizumab biosimilar, was studied in the first-line setting for advanced HCC in the phase II/III ORIENT-32 trial.52 Patients were randomized to the combination therapy (n=380) or sorafenib (n=191) and stratified based on extrahepatic metastases, macrovascular invasion, AFP level, and performance status. With a median follow-up of 10 months, median OS was better in the experimental arm (not reached vs 10.4 months; HR=0.57; 95% CI 0.43–0.75; p<0.0001), as was PFS (4.6 vs 2.8 months; HR=0.56, 95% CI 0.46–0.70; p<0.0001), with an ORR of 20.3%. Rates of grade 3 or higher adverse events were comparable between the arms.
Cabozantinib and Atezolizumab
COSMIC 312 is an ongoing global phase III clinical trial evaluating cabozantinib in combination with atezolizumab versus sorafenib in the first-line setting for patients with advanced HCC. It enrolled 840 patients randomized 2:1:1 to cabozantinib (40 mg) in combination with atezolizumab, sorafenib, or cabozantinib (60 mg). In June 2021, a press release53 announced that the study had met one of its primary endpoints at planned primary analysis by demonstrating improved PFS for cabozantinib in combination with atezolizumab compared to sorafenib (HR=0.63, 99% CI 0.44–0.91; p=0.0012). Analysis for OS showed a trend favoring the combination that did not reach statistical significance, with a low probability of reaching statistical significance at the final analysis, anticipated in early 2022.
Sequencing
As delineated above, the landscape of treatment for advanced HCC has significantly changed over the past few years, especially with the exciting results of the IMbrave150 trial showing the survival benefit of atezolizumab with bevacizumab compared to sorafenib. In general, the selection of a second-line regimen is mainly determined based on prior therapy along with comorbidities. Figure 1 depicts our preferred second-line options depending on the first-line treatment used.
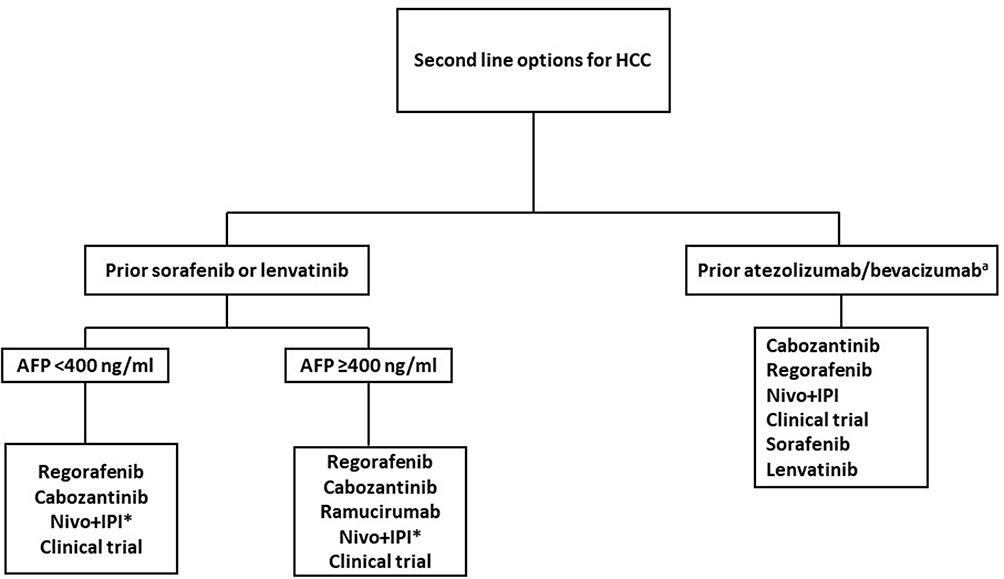 |
Figure 1 Preferred second-line treatment options for advanced hepatocellular carcinoma. Nivo+IPI: nivolumab + ipilimumab. aNone of the options listed below are supported by prospective evidence. *Not supported by level 1 evidence. |
Prior Sorafenib/Lenvatinib
In general, sorafenib or lenvatinib should be used in the first-line setting only if there is a contraindication to using atezolizumab/bevacizumab, as the superiority of the combination has been established in a phase III trial and a recent network meta-analysis.54 As discussed above, all of the second-line options were studied in patient populations that were refractory or intolerant to sorafenib. For such patients, regorafenib and cabozantinib are the preferred options as both agents are supported by level I evidence with phase III trials.20,30 In addition, ramucirumab is an option for patients with AFP of ≥400 ng/mL.37 Given the negative results of KEYNOTE-240, ICI monotherapy in this setting is less preferable. Combination ICI with nivolumab and ipilimumab is an option in this setting if there are no contraindications. Indeed, clinical trial enrollment is always encouraged when possible.
Prior Atezolizumab/Bevacizumab
The optimal second-line regimen for patients with prior atezolizumab/bevacizumab is currently unknown. Cabozantinib or regorafenib (over lenvatinib or sorafenib) may be preferred options given their different mechanisms of action, with wide-ranging multikinase inhibition along with the fact that they are the only TKIs studied with prior exposure to VEGF inhibitors. However, the role of ramucirumab following progression on bevacizumab-containing combination therapy remains unclear and it is unlikely to be effective. Similarly, a single-agent ICI may not be preferred after an atezolizumab-containing combination, although dual checkpoint inhibitors such as nivolumab and ipilimumab remain attractive options, especially considering the high ORR observed in the clinical trials with the combination. A recent retrospective study of 25 patients with advanced HCC evaluated the efficacy of adding ipilimumab to nivolumab or pembrolizumab after prior ICI progression.55 Half of the patients (48%) had primary resistance and the majority (84%) received an ICI as monotherapy. With a median follow-up of 37.7 months, the ORR was 16% (12% complete response + 4% partial response) and the DCR was 40%. Responses were seen regardless of whether the ICI resistance was primary (ORR 16.7%) or acquired (15.4%). Indeed, extrapolation is challenging owing to the retrospective nature of the study along with the fact that only one patient had received prior atezolizumab/bevacizumab.
Future Directions
Enthusiasm for single-agent immunotherapeutic drugs such as nivolumab and pembrolizumab has been dampened with the negative results of phase III trials and the 2021 FDA vote against continued approval of single-agent nivolumab.56
Strategies to enhance responses to ICIs through combinations with immune-modulatory drugs such as TKIs or the use of dual checkpoint inhibitors are an active area of interest. In light of the encouraging results from the IMbrave 150 trial, several other checkpoint inhibitor and anti-VEGF combinations, such as pembrolizumab with lenvatinib, and cabozantinib with nivolumab, are being explored. Table 2 lists some of the ongoing major clinical trials for advanced HCC and the expected dates of completion.
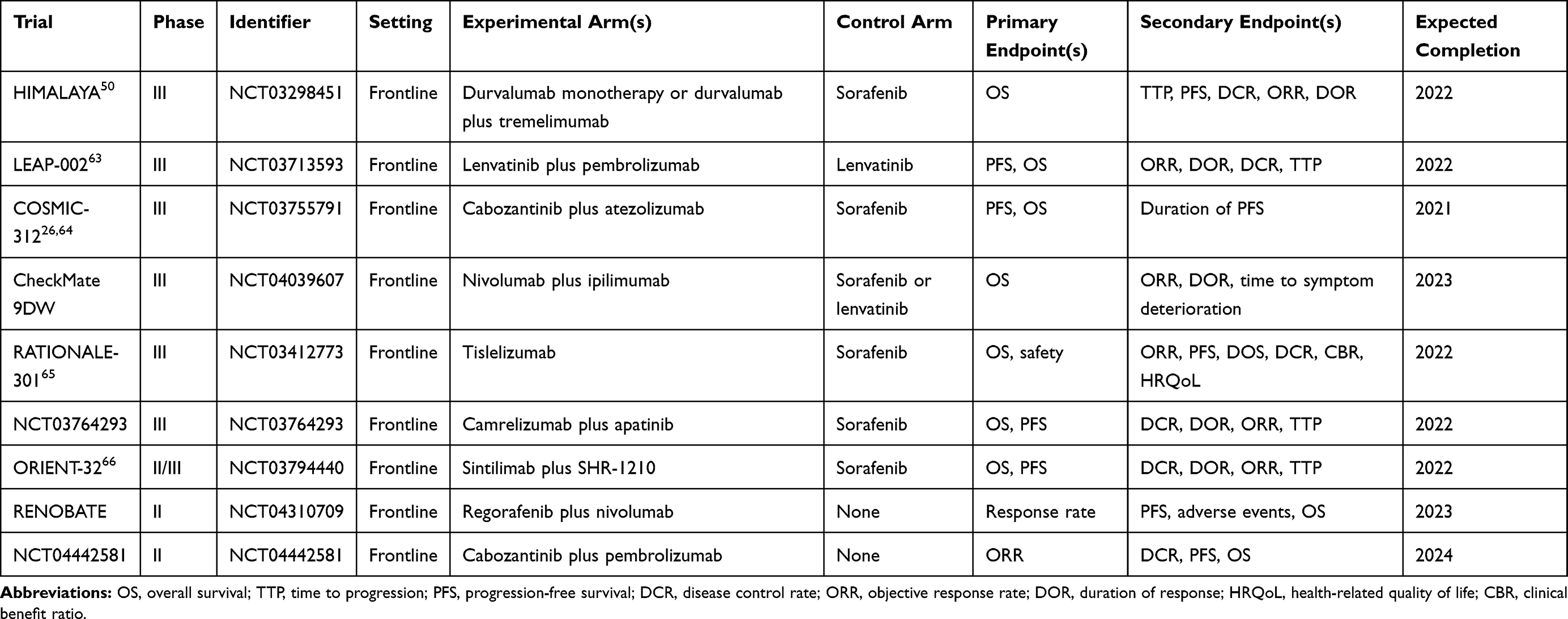 |
Table 2 Ongoing Major Clinical Trials of Systemic Therapies for Advanced Hepatocellular Carcinoma |
Clinical and molecular biomarkers that can guide treatment selection and sequencing are of considerable interest. For example, most of the major clinical trials stratified patients based on HBV status, macrovascular invasion, and extrahepatic metastases. CELESTIAL reported better responses in those with non-HBV status compared to HBV status. The predictive value of AFP in the REACH-2 trial led to FDA approval of ramucirumab. Based on preclinical models, FGF, AFP, transforming growth factor beta-1, and epithelial cell adhesion molecules (EpCAM) have potential predictive value.57–59 Biomarkers for immunotherapy, such as PD-L1 and TMB, have not shown differential activity in the HCC trials. This was manifested in the CheckMate 040 and KEYNOTE-224 trials, where no difference in responses was observed based on the PD-L1 status. Therefore, there is an unmet need for further development of predictive biomarkers that can help in guiding therapies. In a recent study of 111 tissue samples of patients with HCC, an 11-gene signature was defined and found to be predictive of a better response to ICIs in the front-line setting.60 However, the same signal was not found in patients who received checkpoint inhibitors after prior VEGF TKIs. Biomarker analyses from the single arm of a trial evaluating lenvatinib plus pembrolizumab reported a decrease in TIMP1 and an increase in MCP1 associated with maximum tumor shrinkage and objective response.61
Lastly, there is a need for clinical evidence to inform the optimal treatment strategy after the new first-line atezolizumab plus bevacizumab combination. As experience grows with the use of these combinations, treatment algorithms are expected to evolve that take into consideration the relevant clinical and safety signals.
Conclusions
The landscape of systemic therapy for advanced HCC is undergoing an exciting transformation with the advent of ICIs, new molecular targeted TKIs, and their combinations with immunotherapies. There is a need for clinically relevant biomarkers to guide the multiple available treatment choices. The treatment paradigm will likely undergo major shifts as we learn the optimal sequencing of the available and the potential future targets.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mak L-Y, Cruz-Ramón V, Chinchilla-López P, et al. Global epidemiology, prevention, and management of hepatocellular carcinoma. Am Soc Clin Oncol Educ B. 2018;(38):262–279. doi:10.1200/edbk_200939
2. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. doi:10.3322/caac.21590
3. (No Title). Available from: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2021/cancer-facts-and-figures-2021.pdf.
4. Llovet JM, Zucman-Rossi J, Pikarsky E, et al. Hepatocellular carcinoma. Nat Rev Dis Prim. 2016;2:6. doi:10.1038/nrdp.2016.18
5. Villanueva A. Hepatocellular Carcinoma. N Engl J Med. 2019;380(15):1450–1462. doi:10.1056/NEJMra1713263
6. Le GM, Biagini MR, Tarocchi M, Polvani S, Galli A. Chemotherapy for hepatocellular carcinoma: the present and the future. World J Hepatol. 2017;9(21):907–920. doi:10.4254/wjh.v9.i21.907
7. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–390. doi:10.1056/nejmoa0708857
8. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
9. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/nejmoa1915745
10. Finn RS, Qin S, Ikeda M, et al. IMbrave150: updated overall survival (OS) data from a global, randomized, open-label phase III study of atezolizumab (atezo) + bevacizumab (bev) versus sorafenib (sor) in patients (pts) with unresectable hepatocellular carcinoma (HCC). J Clin Oncol. 2021;39(3_suppl):267. doi:10.1200/jco.2021.39.3_suppl.267
11. Shin JW, Chung YH. Molecular targeted therapy for hepatocellular carcinoma: current and future. World J Gastroenterol. 2013;19(37):6144–6155. doi:10.3748/wjg.v19.i37.6144
12. da Fonseca LG, Reig M, Bruix J. Tyrosine kinase inhibitors and hepatocellular carcinoma. Clin Liver Dis. 2020;24(4):719–737. doi:10.1016/j.cld.2020.07.012
13. Fujimoto A, Furuta M, Totoki Y, et al. Whole-genome mutational landscape and characterization of noncoding and structural mutations in liver cancer. Nat Genet. 2016;48(5):500–509. doi:10.1038/ng.3547
14. Flecken T, Schmidt N, Hild S, et al. Immunodominance and functional alterations of tumor-associated antigen-specific CD8+ T-cell responses in hepatocellular carcinoma. Hepatology. 2014;59(4):1415–1426. doi:10.1002/hep.26731
15. Prieto J, Melero I, Sangro B. Immunological landscape and immunotherapy of hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2015;12(12):681–700. doi:10.1038/nrgastro.2015.173
16. Breous E, Thimme R. Potential of immunotherapy for hepatocellular carcinoma. J Hepatol. 2011;54(4):830–834. doi:10.1016/j.jhep.2010.10.013
17. Wilhelm SM, Dumas J, Adnane L, et al. Regorafenib (BAY 73-4506): a new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. Int J Cancer. 2011;129(1):245–255. doi:10.1002/ijc.25864
18. Bruix J, Tak WY, Gasbarrini A, et al. Regorafenib as second-line therapy for intermediate or advanced hepatocellular carcinoma: multicentre, open-label, Phase II safety study. Eur J Cancer. 2013;49(16):3412–3419. doi:10.1016/j.ejca.2013.05.028
19. Bruix J, Qin S, Merle P, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;389(10064):56–66. doi:10.1016/S0140-6736(16)32453-9
20. Bruix J, Merle P, Granito A, et al. Updated overall survival (OS) analysis from the international, phase 3, randomized, placebo-controlled RESORCE trial of regorafenib for patients with hepatocellular carcinoma (HCC) who progressed on sorafenib treatment. Ann Oncol. 2017;28:iii140. doi:10.1093/annonc/mdx262.008
21. Finn RS, Merle P, Granito A, et al. Outcomes of sequential treatment with sorafenib followed by regorafenib for HCC: additional analyses from the phase III RESORCE trial. J Hepatol. 2018;69(2):353–358. doi:10.1016/j.jhep.2018.04.010
22. FDA. FDA expands approved use of Stivarga to treat liver cancer. Available from: https://www.fda.gov/news-events/press-announcements/fda-expands-approved-use-stivarga-treat-liver-cancer.
23. Grothey A, Blay JY, Pavlakis N, Yoshino T, Bruix J. Evolving role of regorafenib for the treatment of advanced cancers. Cancer Treat Rev. 2020;86:101993. doi:10.1016/j.ctrv.2020.101993
24. Bekaii-Saab TS, Ou FS, Ahn DH, et al. Regorafenib dose-optimisation in patients with refractory metastatic colorectal cancer (ReDOS): a randomised, multicentre, open-label, phase 2 study. Lancet Oncol. 2019;20(8):1070–1082. doi:10.1016/S1470-2045(19)30272-4
25. Yakes FM, Chen J, Tan J, et al. Cabozantinib (XL184), a novel MET and VEGFR2 inhibitor, simultaneously suppresses metastasis, angiogenesis, and tumor growth. Mol Cancer Ther. 2011;10(12):2298–2308. doi:10.1158/1535-7163.MCT-11-0264
26. D’Alessio A, Prete MG, Cammarota A, Personeni N, Rimassa L. The role of cabozantinib as a therapeutic option for hepatocellular carcinoma: current landscape and future challenges. J Hepatocell Carcinoma. 2021;8:177–191. doi:10.2147/jhc.s268310
27. Xiang Q, Chen W, Ren M, et al. Cabozantinib suppresses tumor growth and metastasis in hepatocellular carcinoma by a dual blockade of VEGFR2 and MET. Clin Cancer Res. 2014;20(11):2959–2970. doi:10.1158/1078-0432.CCR-13-2620
28. Rimassa L, Abbadessa G, Personeni N, et al. Tumor and circulating biomarkers in patients with second-line hepatocellular carcinoma from the randomized phase II study with tivantinib. Oncotarget. 2016;7(45):72622–72633. doi:10.18632/oncotarget.11621
29. Firtina Karagonlar Z, Koc D, Iscan E, Erdal E, Atabey N. Elevated hepatocyte growth factor expression as an autocrine c-Met activation mechanism in acquired resistance to sorafenib in hepatocellular carcinoma cells. Cancer Sci. 2016;107(4):407–416. doi:10.1111/cas.12891
30. Kelley RK, Verslype C, Cohn AL, et al. Cabozantinib in hepatocellular carcinoma: results of a phase 2 placebo-controlled randomized discontinuation study. Ann Oncol. 2017;28(3):528–534. doi:10.1093/annonc/mdw651
31. Abou-Alfa GK, Meyer T, Cheng A-L, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med. 2018;379(1):54–63. doi:10.1056/nejmoa1717002
32. Yau T, Cheng A-L, Meyer T, et al. Outcomes by prior transarterial chemoembolization (TACE) in the phase III CELESTIAL trial of cabozantinib (C) versus placebo (P) in patients (pts) with advanced hepatocellular carcinoma (HCC). Ann Oncol. 2018;29:viii237–viii238. doi:10.1093/annonc/mdy282.087
33. Kelley RK, Ryoo BY, Merle P, et al. Second-line cabozantinib after sorafenib treatment for advanced hepatocellular carcinoma: a subgroup analysis of the phase 3 CELESTIAL trial. ESMO Open. 2020;5(4):4. doi:10.1136/esmoopen-2020-000714
34. El-Khoueiry A, Meyer T, Cheng A, et al. SO-9 Outcomes for patients with advanced hepatocellular carcinoma and Child-Pugh B liver function in the phase 3 CELESTIAL study of cabozantinib vs placebo. Ann Oncol. 2020;31:S220. doi:10.1016/j.annonc.2020.04.024
35. Spratlin JL, Cohen RB, Eadens M, et al. Phase I pharmacologic and biologic study of ramucirumab (IMC-1121b), a fully human immunoglobulin G1 monoclonal antibody targeting the vascular endothelial growth factor receptor-2. J Clin Oncol. 2010;28(5):780–787. doi:10.1200/JCO.2009.23.7537
36. Zhu AX, Finn RS, Mulcahy M, et al. A phase II and biomarker study of ramucirumab, a human monoclonal antibody targeting the VEGF receptor-2, as first-line monotherapy in patients with advanced hepatocellular Cancer. Clin Cancer Res. 2013;19(23):6614–6623. doi:10.1158/1078-0432.CCR-13-1442
37. Zhu AX, Kang YK, Yen CJ, et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(2):282–296. doi:10.1016/S1470-2045(18)30937-9
38. Zhu A, Finn R, Galle P, et al. Ramucirumab as second-line treatment in patients with advanced hepatocellular carcinoma (HCC) and elevated alpha-fetoprotein (AFP) following first-line sorafenib: pooled efficacy and safety across two global randomized Phase 3 studies (REACH-2 and REACH). Ann Oncol. 2018;29:v122. doi:10.1093/annonc/mdy208
39. FDA. FDA approves ramucirumab for hepatocellular carcinoma. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-ramucirumab-hepatocellular-carcinoma.
40. Yau T, Park JW, Finn RS, et al. CheckMate 459: a randomized, multi-center phase III study of nivolumab (NIVO) vs sorafenib (SOR) as first-line (1L) treatment in patients (pts) with advanced hepatocellular carcinoma (aHCC). Ann Oncol. 2019;30:v874–v875. doi:10.1093/annonc/mdz394.029
41. Kudo M, Matilla A, Santoro A, et al. CheckMate 040 cohort 5: a phase I/II study of nivolumab in patients with advanced hepatocellular carcinoma and Child-Pugh B cirrhosis. J Hepatol. 2021;75(3):600–609. doi:10.1016/j.jhep.2021.04.047
42. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol. 2018;19(7):940–952. doi:10.1016/S1470-2045(18)30351-6
43. Finn RS, Ryoo BY, Merle P, et al. Pembrolizumab as second-line therapy in patients with advanced hepatocellular carcinoma in KEYNOTE-240: a randomized, double-blind, phase III trial. J Clin Oncol. 2020;38(3):193–202. doi:10.1200/JCO.19.01307
44. Chae YK, Arya A, Iams W, et al. Current landscape and future of dual anti-CTLA4 and PD-1/PD-L1 blockade immunotherapy in cancer; lessons learned from clinical trials with melanoma and non-small cell lung cancer (NSCLC). J Immunother Cancer. 2018;6(1):1. doi:10.1186/s40425-018-0349-3
45. Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. 2019;381(16):1535–1546. doi:10.1056/nejmoa1910836
46. Lipson EJ, Tawbi -HA-H, Schadendorf D, et al. Relatlimab (RELA) plus nivolumab (NIVO) versus NIVO in first-line advanced melanoma: primary phase III results from RELATIVITY-047 (CA224-047). J Clin Oncol. 2021;39(15_suppl):9503. doi:10.1200/JCO.2021.39.15_suppl.9503
47. Yau T, Kang YK, Kim TY, et al. Efficacy and safety of nivolumab plus ipilimumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib: the checkmate 040 randomized clinical trial. JAMA Oncol. 2020;6(11):e204564. doi:10.1001/jamaoncol.2020.4564
48. Sangro B, Gomez-Martin C, De La Mata M, et al. A clinical trial of CTLA-4 blockade with tremelimumab in patients with hepatocellular carcinoma and chronic hepatitis C. J Hepatol. 2013;59(1):81–88. doi:10.1016/j.jhep.2013.02.022
49. Kelley RK, Abou-Alfa GK, Bendell JC, et al. Phase I/II study of durvalumab and tremelimumab in patients with unresectable hepatocellular carcinoma (HCC): phase I safety and efficacy analyses. J Clin Oncol. 2017;35(15_suppl):4073. doi:10.1200/jco.2017.35.15_suppl.4073
50. Kelley RK, Sangro B, Harris WP, et al. Efficacy, tolerability, and biologic activity of a novel regimen of tremelimumab (T) in combination with durvalumab (D) for patients (pts) with advanced hepatocellular carcinoma (aHCC). J Clin Oncol. 2020;38(15_suppl):4508. doi:10.1200/jco.2020.38.15_suppl.4508
51. Yau T, Zagonel V, Santoro A, et al. Nivolumab (NIVO) + ipilimumab (IPI) + cabozantinib (CABO) combination therapy in patients (pts) with advanced hepatocellular carcinoma (aHCC): results from CheckMate 040. J Clin Oncol. 2020;38(4_suppl):478. doi:10.1200/jco.2020.38.4_suppl.478
52. Ren Z, Xu J, Bai Y, et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, phase 2–3 study. Lancet Oncol. 2021;22(7):977–990. doi:10.1016/S1470-2045(21)00252-7
53. Business Wire. Exelixis and ipsen announce cabozantinib in combination with an immune checkpoint inhibitor significantly improved progression-free survival in phase 3 COSMIC-312 pivotal trial in patients with previously untreated advanced liver cancer. Available from: https://www.businesswire.com/news/home/20210627005058/en/Exelixis-and-Ipsen-Announce-Cabozantinib-in-Combination-with-an-Immune-Checkpoint-Inhibitor-Significantly-Improved-Progression-Free-Survival-in-Phase-3-COSMIC-312-Pivotal-Trial-in-Patients-with-Previously-Untreated-Advanced-Liver-Cancer.
54. Sonbol MB, Bin RI, Naqvi SAA, et al. Systemic therapy and sequencing options in advanced hepatocellular carcinoma: a systematic review and network meta-analysis. JAMA Oncol. 2020;6(12):e204930. doi:10.1001/jamaoncol.2020.4930
55. Wong JSL, Kwok GGW, Tang V, et al. Ipilimumab and nivolumab/pembrolizumab in advanced hepatocellular carcinoma refractory to prior immune checkpoint inhibitors. J Immunother Cancer. 2021;9(2):2. doi:10.1136/jitc-2020-001945
56. (No Title). Available from: https://www.fda.gov/media/147861/download.
57. Yamashita T, Forgues M, Wang W, et al. EpCAM and α-fetoprotein expression defines novel prognostic subtypes of hepatocellular carcinoma. Cancer Res. 2008;68(5):1451–1461. doi:10.1158/0008-5472.CAN-07-6013
58. Galle PR, Foerster F, Kudo M, et al. Biology and significance of alpha-fetoprotein in hepatocellular carcinoma. Liver Int. 2019;39(12):2214–2229. doi:10.1111/liv.14223
59. De Stefano F, Chacon E, Turcios L, Marti F, Gedaly R. Novel biomarkers in hepatocellular carcinoma. Dig Liver Dis. 2018;50(11):1115–1123. doi:10.1016/j.dld.2018.08.019
60. Haber PK, Torres-Martin M, Dufour J-F, et al. Molecular markers of response to anti-PD1 therapy in advanced hepatocellular carcinoma. J Clin Oncol. 2021;39(15_suppl):4100. doi:10.1200/JCO.2021.39.15_suppl.4100
61. Zhu AX, Llovet JM, Kobayashi M, et al. Exploratory circulating biomarker analyses: lenvatinib + pembrolizumab (L + P) in a phase 1b trial in unresectable hepatocellular carcinoma (uHCC). J Clin Oncol. 2021;39(15_suppl):4084. doi:10.1200/JCO.2021.39.15_suppl.4084
62. El-Khoueiry AB, Sangro B, Yau T, et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet. 2017;389(10088):2492–2502. doi:10.1016/S0140-6736(17)31046-2
63. Llovet JM, Kudo M, Cheng A-L, et al. Lenvatinib (len) plus pembrolizumab (pembro) for the first-line treatment of patients (pts) with advanced hepatocellular carcinoma (HCC): Phase 3 LEAP-002 study. J Clin Oncol. 2019;37(15_suppl):TPS4152–TPS4152. doi:10.1200/jco.2019.37.15_suppl.tps415265
64. Kelley RK, W Oliver J, Hazra S, et al. Cabozantinib in combination with atezolizumab versus sorafenib in treatment-naive advanced hepatocellular carcinoma: COSMIC-312 Phase III study design. Futur Oncol. 2020;16(21):1525–1536. doi:10.2217/fon-2020-028366
65. Qin S, Finn RS, Kudo M, et al. RATIONALE 301 study: Tislelizumab versus sorafenib as first-line treatment for unresectable hepatocellular carcinoma. Futur Oncol. 2019;15(16):1811–1822. doi:10.2217/fon-2019-009767
66. Ren Z, Fan J, Xu J, et al. LBA2 Sintilimab plus bevacizumab biosimilar vs sorafenib as first-line treatment for advanced hepatocellular carcinoma (ORIENT-32)2. Ann Oncol. 2020;31:S1287. doi:10.1016/j.annonc.2020.10.134
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.