Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Sebum-Selective 1,726-nm Laser Therapy for Papulopustular Rosacea Associated with Demodex Mite Proliferation: A Case Report
Authors Paichitrojjana A ![]()
Received 13 April 2026
Accepted for publication 17 May 2026
Published 19 May 2026 Volume 2026:19 616644
DOI https://doi.org/10.2147/CCID.S616644
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Anon Paichitrojjana
School of Anti-Aging and Regenerative Medicine, Mae Fah Luang University, Bangkok, Thailand
Correspondence: Anon Paichitrojjana, Email [email protected]
Abstract: Papulopustular rosacea is a chronic inflammatory condition of the pilosebaceous unit, with an unclear exact cause, but it is thought to involve an exaggerated immune response, persistent inflammation, and possibly an increased presence of Demodex mites on the skin. This is a case report of a 22-year-old woman with papulopustular rosacea treated with a 1,726-nm sebum-selective laser over three sessions. Progressive clinical improvement was observed, with a reduction of inflammatory lesions from 234 at baseline to complete clearance, along with improvement in erythema, flushing, and patient-reported symptoms. Demodex density decreased from 58 mites/cm2 to 12 mites/cm2. Treatment was well tolerated, with no adverse events and high patient satisfaction. These findings suggest that sebum-selective laser therapy may offer a non-pharmacologic treatment option for papulopustular rosacea, potentially by modulating sebaceous gland activity. Further studies are needed to confirm efficacy and clarify mechanisms.
Plain Language Summary: Rosacea is a common skin condition that causes facial redness, flushing, and acne-like bumps, often with burning or stinging. In this case, a 22-year-old woman was treated with a laser that targets oil glands in the skin. After three sessions, her skin improved significantly, with complete clearing of bumps and reduced redness and symptoms. The number of Demodex mites also decreased. The treatment was well tolerated with no side effects. This laser may be a useful option for patients who are resistant to conventional treatments, unable to use standard medications, or for whom it serves as an adjunctive therapy; however, further research is needed to confirm its effectiveness.
Keywords: Demodex mite, rosacea, demodicosis, 1, 726-nm laser, sebum-selective laser
Introduction
Rosacea is a chronic inflammatory dermatosis of the central face, characterized by flushing, persistent erythema, papules, pustules, telangiectasia, and occasional phymatous changes, with possible ocular involvement. Owing to its facial distribution and chronic course, rosacea can significantly impair quality of life. Management includes appropriate skin care, topical and systemic therapies, and, for selected features, energy-based treatments such as intense pulsed light, laser therapy, and surgery.1,2
The pathogenesis of rosacea is multifactorial, involving dysregulation of innate and adaptive immunity, neurovascular dysfunction, and abnormalities of the pilosebaceous unit, with an important contribution from microbial factors. Key pathways include activation of toll-like receptor 2 and the NLRP3 inflammasome, abnormal processing of cathelicidin (LL-37), and neurocutaneous signaling via transient receptor potential channels.2
Among these microbial contributors, Demodex mites have been strongly implicated in rosacea, especially papulopustular rosacea (PPR). Multiple studies have demonstrated significantly higher Demodex densities in patients with rosacea compared with healthy controls, and mite density has been shown to correlate with inflammatory lesion severity.3–7
Demodex mites contribute to inflammation through follicular obstruction, disruption of the epidermal barrier, activation of Toll-like receptor-mediated innate immune pathways, and immune responses to mite-associated bacteria.3,8,9 The clinical efficacy of acaricidal therapies, particularly topical ivermectin, further supports the pathogenic role of Demodex in rosacea.10,11 Sebaceous gland activity is central to maintaining the follicular microenvironment that supports Demodex survival and proliferation. Sebum provides a primary nutritional substrate for mites and contributes to cutaneous inflammation by altering lipid composition and inducing oxidative stress.12
Oral isotretinoin, which suppresses sebaceous gland activity and reduces sebum production, has demonstrated efficacy in rosacea. Its mechanisms include modulation of gene expression, reduction of sebaceous gland size, and anti-inflammatory effects, thereby addressing key aspects of immune dysregulation in rosacea.13–15 Isotretinoin therapy has also been associated with reductions in Demodex mite density.16–19 Collectively, these observations support targeting sebaceous gland function as an effective therapeutic strategy for rosacea.
Despite its efficacy, isotretinoin use is limited by systemic adverse effects, prompting interest in non-pharmacologic approaches that modulate sebaceous gland activity. While laser and energy-based devices are well established for vascular features of rosacea, sebaceous gland–targeted therapies remain relatively underexplored in rosacea management. The 1,726-nm wavelength corresponds to a lipid absorption peak, allowing selective photothermal targeting of sebaceous glands while minimizing absorption by water and hemoglobin. This sebum-selective mechanism has been shown to reduce sebaceous gland activity and inflammatory lesions in acne vulgaris, providing a mechanism of action analogous to isotretinoin without systemic exposure.20,21 However, evidence for the use of 1,726-nm lasers specifically in rosacea remains limited.
This case demonstrates progressive clinical improvement accompanied by a reduction in Demodex mite density following treatment with a 1,726-nm laser, highlighting a potentially novel, mechanism-based therapeutic approach for papulopustular rosacea. This modality may represent a potential adjunctive or alternative option within current treatment algorithms, particularly for patients who are intolerant of or reluctant to use long-term topical or systemic therapies.
Case Report
A 22-year-old woman presented with two years history of recurrent facial flushing and persistent background erythema, accompanied by stinging sensations. These symptoms were precipitated by sunlight exposure, hot weather, and physical exertion.
The patient was otherwise healthy, with no known chronic medical conditions and no history of regular medication use. Approximately three months prior to presentation, she developed persistent central facial erythema, flushing, and telangiectasia, accompanied by skin dryness, stinging, burning, and intermittent pruritus (Figure 1).
 |
Figure 1 Baseline clinical presentation showing persistent background erythema and facial flushing involving the central face. |
Subsequently, multiple small erythematous papules and pustules appeared on the nasal area and progressively extended to the cheeks and forehead (Figure 2).
 |
Figure 2 Multiple small papulopustular lesions symmetrically distributed over the cheeks, chin, and forehead on a background of erythema and telangiectasia. |
Physical examination revealed numerous small papulopustular lesions on a background of diffuse erythema and flushing involving both cheeks and the forehead, without the presence of comedones. To evaluate the density of Demodex mites, a standardized skin surface biopsy (SSSB) was conducted on the affected areas of the right cheek. This procedure showed a Demodex density of 58 mites/cm2 on the right cheek. In addition, superficial needle scraping (SNS) was performed by gently scraping five pustular lesions using the convex surface of a 22-gauge needle. Microscopic examination of the collected material revealed 6 Demodex mites (Figure 3).
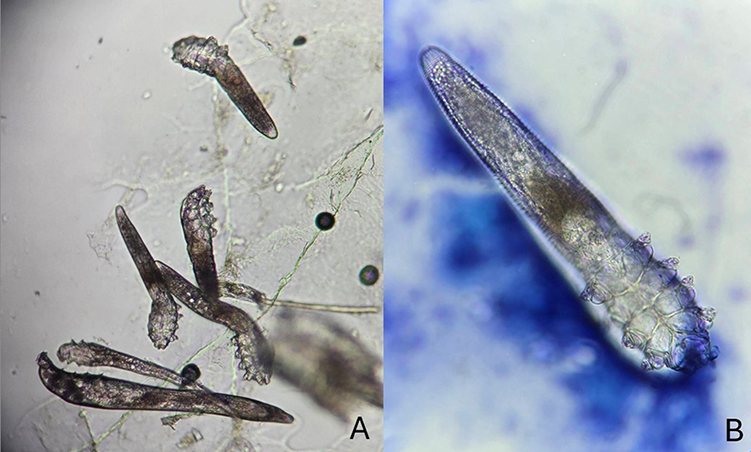 |
Figure 3 Microscopic findings from standardized skin surface biopsy ((A) ×40 magnification) and superficial needle scraping ((B) ×40 magnification with additional digital zoom for enhanced clarity) demonstrating the presence of Demodex mites. |
Based on the clinical presentation and parasitological findings, a diagnosis of papulopustular rosacea associated with increased Demodex mite density was established.
The patient declined systemic pharmacologic therapy and was reluctant to use topical treatments because of persistent facial skin sensitivity and concerns about further irritation. Consequently, she opted for laser therapy as an alternative, non-pharmacologic treatment modality.
Laser treatment was performed using a 1,726-nm sebum-selective laser (Aviclear®, Cutera, Inc.) targeting lipid-rich sebaceous glands via selective photothermolysis. After gentle facial cleansing, no topical anesthetic was applied. The treatment parameters were standardized to a fluence of 19–20 J/cm2 and a spot size of 10 mm. Two passes were applied to the cheeks, forehead, nose, and chin, for a total of 300 pulses per session. Throughout the procedure, dynamic contact cooling was utilized to protect the epidermis and enhance patient comfort.
The patient underwent three treatment sessions at four-week intervals. Each session achieved mild, transient erythema as the clinical endpoint, without blistering or epidermal disruption, and was well tolerated. Post-treatment care involved gentle cleansing, applying a bland moisturizer, and daily sunscreen application. No topical or systemic therapies were administered.
At baseline, the total inflammatory lesion count (ILC) was 234 papulopustular lesions involving the cheeks, forehead, and chin, accompanied by moderate erythema, flushing, telangiectasia, and prominent burning and stinging.
Two weeks after the initial treatment, the pustules had disappeared, and the inflamed papules were smaller and less red. However, the facial skin was notably dry and flaky, with itching.
By four weeks after the first treatment session, the ILC had decreased to 108 papular lesions. Additionally, Demodex density decreased to 50 mites/cm2, along with improvements in symptoms, including reduced erythema, stinging, and burning.
Four weeks after the second treatment session, the ILC had 15 papular lesions remaining. Symptoms were significantly improved, with only mild skin dryness noted, and the density of Demodex mites further decreased to 35 mites/cm2.
By four weeks after the third treatment session, complete clearance of the lesions was achieved. Background erythema and flushing were substantially reduced, and Demodex density had declined to 12 mites/cm2 (Figure 4).
 |
Figure 4 Post-treatment clinical outcome at four weeks after the third laser session showing complete clearance of papulopustular lesions with marked reduction in background erythema and flushing. |
No adverse events were observed throughout the treatment period, and the patient reported high satisfaction with the outcomes.
Discussion
Papulopustular rosacea is increasingly conceptualized as a disorder of the pilosebaceous unit, driven by interactions among sebaceous gland activity, Demodex mite proliferation, and dysregulated innate immune responses. Accumulating evidence demonstrates that increased Demodex density correlates with inflammatory lesion burden, indicating a contributory or possibly causative role in disease development.3–7,11,22–24 In this context, the present case provides clinically and parasitologically concordant evidence that targeting sebaceous gland function may represent a rational therapeutic strategy. Treatment with a 1,726-nm sebum-selective laser resulted in marked clinical improvement, accompanied by a stepwise, quantitatively documented reduction in Demodex density.
The temporal association between decreasing Demodex density and progressive clinical improvement, including reductions in inflammatory lesions, burning, stinging, and flushing, suggests a mechanistic link between modulation of the follicular microenvironment and attenuation of disease activity. While causality cannot be definitively established in a single case, this concordance strengthens the biological plausibility of sebaceous gland-targeted intervention in papulopustular rosacea.
Sebaceous gland activity is central to maintaining the follicular niche required for Demodex survival, with sebum functioning as both a nutritional substrate and a pro-inflammatory mediator. Demodex mites can further amplify inflammation by modulating sebocyte function and activating Toll-like receptor pathways, thereby increasing cytokine production and sustaining immune activation.12 A key pathogenic mechanism involves activation of Toll-like receptor 2 (TLR2) by increased mite density, triggering downstream cascades including abnormal cathelicidin (LL-37) processing, angiogenesis, and vascular hyperreactivity.4,25,26 In parallel, qualitative alterations in sebum composition may impair epidermal barrier integrity and contribute to heightened cutaneous sensitivity,27 while sebaceous hyperplasia underlies structural changes observed in phymatous disease.28 Collectively, these findings position the sebaceous unit as a central interface linking microbial, immunologic, and inflammatory pathways in rosacea.
Pharmacologic suppression of sebaceous gland activity with oral isotretinoin has demonstrated efficacy in refractory papulopustular rosacea and is associated with reductions in Demodex density, supporting the therapeutic relevance of targeting sebaceous function.14–19 However, its use is limited by systemic adverse effects, teratogenicity, and monitoring requirements. In contrast, the 1,726-nm sebum-selective laser offers a mechanism-based, non-systemic approach that selectively targets lipid-rich sebaceous glands via photothermolysis, inducing glandular atrophy and reducing sebum production while preserving surrounding tissue integrity.29
The clinical effects observed in this case may be explained by several complementary mechanisms. First, reduction of sebum production likely disrupts the follicular microenvironment necessary for Demodex proliferation, thereby decreasing mite density. Second, suppression of sebaceous-derived inflammatory mediators may attenuate local immune activation. Third, normalization of sebum composition may contribute to the restoration of epidermal barrier function and a reduction in cutaneous sensitivity. Together, these effects suggest that sebaceous gland-targeted laser therapy may modulate multiple downstream pathways central to rosacea pathogenesis.
Further support for this approach comes from studies of acne vulgaris, in which sebaceous gland hyperactivity is a primary driver of pathogenesis. Previous studies have demonstrated that the 1,726-nm wavelength corresponds to a lipid absorption peak, enabling selective photothermal targeting of sebaceous glands and resulting in sustained reductions in sebum production and inflammatory lesion counts.20,21 These studies also demonstrate favorable safety profiles without the need for adjunctive systemic therapy. Although acne and papulopustular rosacea are distinct entities, their shared involvement of the pilosebaceous unit provides a mechanistic rationale for extrapolating sebaceous-targeted interventions across these conditions.
Notably, improvements in background erythema and flushing were observed despite the 1,726-nm wavelength not being optimized for vascular targeting. This finding suggests that attenuation of follicular inflammation and Demodex-associated immune activation may secondarily improve neurovascular dysregulation, consistent with contemporary models of rosacea pathophysiology.4,25,30 This indirect vascular benefit warrants further investigation, as it may expand the therapeutic implications of sebaceous-targeted approaches beyond purely inflammatory lesions.
The magnitude and temporal pattern of Demodex reduction in this case are comparable to those reported with acaricidal therapies, particularly topical ivermectin.31 However, in contrast to pharmacologic approaches, sebum-selective laser therapy is non-antimicrobial and may therefore mitigate concerns related to antimicrobial resistance, treatment adherence, and medication intolerance. This distinction is particularly relevant in patients with sensitive skin or those unwilling or unable to tolerate conventional therapies.
This report has several limitations. As a single-case observation, the findings are inherently limited in generalizability, and spontaneous disease fluctuation cannot be excluded. In addition, histopathologic confirmation of sebaceous gland changes was not performed, and the relative contribution of laser-induced sebaceous suppression versus other potential mechanisms cannot be definitively determined.
In conclusion, this case supports the concept that sebum-selective 1,726-nm laser therapy may represent a promising, mechanism-based, non-pharmacologic treatment option for papulopustular rosacea, particularly in patients with elevated Demodex density. These findings highlight the sebaceous gland as a therapeutic target in rosacea and suggest that modulation of the follicular microenvironment may have clinically meaningful effects. Further controlled studies are required to define efficacy, durability, optimal treatment parameters, and the role of this modality within combination treatment strategies.
Data Sharing Statement
All data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.
Statement of Ethics
The author states that the patient gave written informed consent for the case to be published (including publication of images). This research complies with all Ethical Guidelines for human studies in accordance with the World Medical Association Declaration of Helsinki. This paper is exempt from The Mae Fah Luang Ethics Committee on Human Research approval, with reference number COE 61/2026. Since it is a case report with no more than three cases, the information is derived from a review of medical records and cannot be linked to an individual unless written patient consent is obtained.
Acknowledgments
The author would like to thank the School of Anti-aging and Regenerative Medicine at Mae Fah Luang University for its research facilities.
Funding
This study did not receive any funding.
Disclosure
The author declares no conflicts of interest in this work.
References
1. Volk K, Ulfers A, Yi RC, Feldman S, Taylor SL. Treatment management for rosacea: current pharmacological and non-pharmacological options. Expert Rev Clin Pharmacol. 2025;18(8):589–7. doi:10.1080/17512433.2025.2550727
2. van Zuuren EJ, Arents BWM, van der Linden MMD, Vermeulen S, Fedorowicz Z, Tan J. Rosacea: new concepts in classification and treatment. Am J Clin Dermatol. 2021;22(4):457–465. doi:10.1007/s40257-021-00595-7
3. Wei F, Li L, Kong Y, et al. Evidence for the clinical association between Demodex and rosacea: a review. Dermatology. 2024;240(1):95–102. doi:10.1159/000534245
4. Forton FMN. The pathogenic role of Demodex mites in rosacea: a potential therapeutic target already in erythematotelangiectatic rosacea? Dermatol Ther. 2020;10(6):1229–1253. doi:10.1007/s13555-020-00458-9
5. Forton FMN. Rosacea, an infectious disease: why rosacea with papulopustules should be considered a demodicosis. A narrative review. J Eur Acad Dermatol Venereol. 2022;36(7):987–1002. doi:10.1111/jdv.18049
6. Forton FMN, De Maertelaer V. Papulopustular rosacea and rosacea-like demodicosis: two phenotypes of the same disease? J Eur Acad Dermatol Venereol. 2018;32(6):1011–1016. doi:10.1111/jdv.14885
7. Zhao YE, Wu LP, Peng Y, Cheng H. Retrospective analysis of the association between Demodex infestation and rosacea. Arch Dermatol. 2010;146(8):896–902. doi:10.1001/archdermatol.2010.196
8. Paichitrojjana A. Demodex: the worst enemies are the ones that used to be friends. Dermatology Reports. 2022;14(3):9339. doi:10.4081/dr.2022.9339
9. Lacey N, Delaney S, Kavanagh K, Powell FC. Mite-related bacterial antigens stimulate inflammatory cells in rosacea. Br J Dermatol. 2007;157(3):474–481. doi:10.1111/j.1365-2133.2007.08028.x
10. Paichitrojjana A, Khuancharee K, Paichitrojjana A. Efficacy of topical ivermectin in controlling human Demodex infestation: evidence from a systematic review and meta-analysis. Parasite Epidemiol Control. 2025;31e00461. doi:10.1016/j.parepi.2025.e00461
11. Trave I, Micalizzi C, Cozzani E, Gasparini G, Parodi A. Papulopustular rosacea treated with ivermectin 1% cream: remission of the Demodex mite infestation over the time and evaluation of clinical relapses. Dermatol Prac Concept. 2022;12(4):e2022201. doi:10.5826/dpc.1204a201
12. Lacey N, Russell-Hallinan A, Zouboulis CC, Powell FC. Demodex mites modulate sebocyte immune reaction: possible role in the pathogenesis of rosacea. Br J Dermatol. 2018;179(2):420–430. doi:10.1111/bjd.16540
13. King A, Tan MG, Kirshen C, Tolkachjov SN. Low-dose isotretinoin for the management of rosacea: a systematic review and meta-analysis. J Eur Acad Dermatol Venereol. 2025;39(4):785–792. doi:10.1111/jdv.20315
14. Desai S, Friedman A. Isotretinoin for rosacea: a systematic review. Dermatol Ther. 2024;16:112–118. doi:10.1007/s13555-024-01026-5
15. Sticchi A, Fiorito F, Kaleci S, Paganelli A, Manfredini M, Longo C. Rosacea and treatment with retinoids: a systematic review and meta-analysis. Ther Adv Chronic Dis. 2025;16:20406223251339964. doi:10.1177/20406223251339964
16. Chakmakchi AMJ, Alatas ET, Yurekli A, Aydoğdu CT, Demir Pektas S. Therapeutic modulation of Demodex density via isotretinoin: insights from a prospective dermatological investigation. J Cosmet Dermatol. 2025;24(6):e70249. doi:10.1111/jocd.70249
17. Demirtaş ŞN, Serarslan G, Kaya ÖM. Evaluation of the effect of systemic isotretinoin treatment on Demodex infestation in acne vulgaris patients. Turkderm Turk Arch Dermatol Venereol. 2025;59(4):116–119. doi:10.4274/turkderm.galenos.2025.05506
18. Paichitrojjana A, Paichitrojjana A. Successful treatment of ivermectin refractory demodicosis with isotretinoin and permethrin cream. JAAD Case Rep. 2022;26:98–100. doi:10.1016/j.jdcr.2022.06.017
19. Clanner‐Engelshofen BM, Ständer LM, Steegmüller T, et al. First ex vivo cultivation of human Demodex mites and evaluation of different drugs on mite proliferation. J Eur Acad Dermatol Venereol. 2022;36(12):2499–2503. doi:10.1111/jdv.18468
20. Goldberg D, Ronan S, Bhatia A, et al. Safe and effective acne treatment across skin types with a 1726 nm sebum-selective laser: one year data from a prospective multicenter study. J Am Acad Dermatol. 2026;94(2):517–524. doi:10.1016/j.jaad.2025.09.077
21. Bittar J, Hooper P, Dover JS. 1726 nm lasers for the treatment of Acne Vulgaris. Skin Therapy Letter. 2024;29(1):5–7.
22. Kubanov A, Gallyamova Y, Kravchenko A. Clinical picture, diagnosis and treatment of rosacea, complicated by Demodex mites. Dermatology Reports. 2019;11(1):7675. doi:10.4081/dr.2019.7675
23. Chang Y-S, Huang Y-C. Role of Demodex mite infestation in rosacea: a systematic review and meta-analysis. J Am Acad Dermatol. 2017;77(3):441–447.e6. doi:10.1016/j.jaad.2017.03.040
24. Forton F, Seys B. Density of Demodex folliculorum in rosacea: a case-control study using standardized skin-surface biopsy. Br J Dermatol. 1993;128(6):650–659. doi:10.1111/j.1365-2133.1993.tb00261.x
25. Yamasaki K, Gallo RL. The molecular pathology of rosacea. J Dermatol Sci. 2009;55(2):77–81. doi:10.1016/j.jdermsci.2009.04.007
26. Yamasaki K, Di Nardo A, Bardan A, et al. Increased serine protease activity and cathelicidin promotes skin inflammation in rosacea. Nat Med. 2007;13(8):975–980. doi:10.1038/nm1616
27. Ní Raghallaigh S, Bender K, Lacey N, Brennan L, Powell FC. The fatty acid profile of the skin surface lipid layer in papulopustular rosacea. Br J Dermatol. 2012;166(2):279–287. doi:10.1111/j.1365-2133.2011.10662.x
28. Farshchian M, Daveluy S. Rosacea. StatPearls; 2026.
29. Sakamoto FH, Doukas AG, Farinelli WA, et al. Selective photothermolysis to target sebaceous glands: theoretical estimation of parameters and preliminary results using a free electron laser. Lasers Surg Med. 2012;44(2):175–183. doi:10.1002/lsm.21132
30. Galluccio G, D’Onghia M, Malvaso D, et al. Advances in the pathogenesis and treatment of rosacea: a phenotype-based therapeutic approach. Cosmetics. 2024;11(1):11. doi:10.3390/cosmetics11010011
31. Stein L, Kircik L, Fowler J, et al. Efficacy and safety of ivermectin 1% cream in treatment of papulopustular rosacea: results of two randomized, double-blind, vehicle-controlled pivotal studies. J Drugs Dermatol. 2014;13(3):316–323.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of in vitro Killing Effect of Thai Herbal Essential Oils, Tea Tree Oil, and Metronidazole 0.75% versus Ivermectin 1% on Demodex folliculorum
Paichitrojjana A, Chalermchai T
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1279-1286
Published Date: 18 May 2023
Case Series of Demodicosis in Acne Vulgaris Patients
Paichitrojjana A, Paichitrojjana A
Clinical, Cosmetic and Investigational Dermatology 2023, 16:3363-3368
Published Date: 18 November 2023
The Association Between Acne Vulgaris, Acne Vulgaris with Nonspecific Facial Dermatitis, and Demodex Mite Presence
Paichitrojjana A, Chalermchai T
Clinical, Cosmetic and Investigational Dermatology 2024, 17:137-146
Published Date: 22 January 2024
Evaluating the Efficacy of Oral Ivermectin on Clinical Symptoms and Demodex Densities in Patients with Demodicosis
Paichitrojjana A, Chalermchai T
Drug Design, Development and Therapy 2024, 18:5299-5306
Published Date: 19 November 2024