")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Case Series of Demodicosis in Acne Vulgaris Patients
Authors Paichitrojjana A , Paichitrojjana A
Received 11 October 2023
Accepted for publication 14 November 2023
Published 18 November 2023 Volume 2023:16 Pages 3363—3368
DOI https://doi.org/10.2147/CCID.S441581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Anon Paichitrojjana,1 Anand Paichitrojjana2
1School of Anti-Aging and Regenerative Medicine, Mae Fah Luang University, Bangkok, Thailand; 2Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Anon Paichitrojjana, School of Anti-Aging and Regenerative Medicine, Mae Fah Luang University, 36/87-88 PS Tower 25Fl, Asoke Road, Sukhumvit 21, Klong Toey Nua, Wattana, Bangkok, 10110, Thailand, Email [email protected]
Abstract: An abnormal density of Demodex mites can trigger many skin disorders known as demodicosis. Clinical manifestations of demodicosis may resemble other skin diseases and can coexist with other skin disorders, resulting in underdiagnosis and a more challenging diagnosis. Here, we report three cases of demodicosis in acne vulgaris patients. These case series have discussed their clinical features along with optimal strategies for diagnosis and treatment.
Keywords: Demodex, mite, demodicosis, acne vulgaris, rosacea
Introduction
Demodex mites are pervasive parasites that inhabit the human pilosebaceous units. Most people have Demodex mites living on their skin without experiencing any noticeable symptoms. However, an abnormally high density of Demodex mites can become a pathogenic organism and trigger various skin disorders, which are called demodicosis. This situation occurs when the balance between Demodex mites, the skin microenvironment, and the human immune system is disrupted.1
Clinical manifestations of demodicosis often mimic other skin diseases and lead to underdiagnosis, such as eczema, folliculitis, rosacea, and perioral dermatitis. In addition, demodicosis may coexist with other skin disorders, making diagnosis more challenging.2 This report presents three cases of demodicosis in acne vulgaris patients, along with optimal strategies for diagnosis and treatment.
Case Report
The first case was a 40-year-old woman who visited our dermatology clinic complaining of acne, dryness, itching, and a stinging sensation on her face for the last three months. She also mentioned occasional itchy bumps on her face that resembled insect bites and healed spontaneously within 1–2 days. During the examination, it was observed that the patient had multiple white and blackheads on her face with some tiny itchy bumps, inflammatory papules, and pustules, mostly on the right cheek, chin, and mandibular region. Additionally, some parts of her facial skin appeared to be slightly red, dry, and rough to the touch, which was different from other areas of the skin that were still oily (Figure 1). A standardized skin surface biopsy from her cheek revealed 38 mites/ cm2, while the superficial needle-scrapings from five pustules found 3 mites with multiple bacteria (Figure 2). Upon evaluation of the clinical symptoms, physical examination, and laboratory results, the diagnosis of acne with demodicosis was made. The patient underwent a two-month treatment with oral doxycycline (200mg/day) and ivermectin (200 μg/kg/week) combined with permethrin cream 5%.
 |
Figure 1 Multiple whiteheads, blackheads, erythematous papules, and pustules, mainly on the right cheek, chin, and mandibular area, with some areas of redness, dryness, and roughness. (Case 1). |
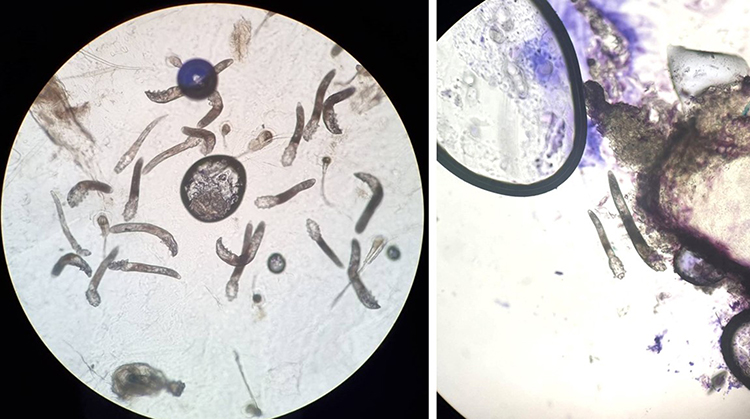 |
Figure 2 Standard skin surface biopsy revealed multiple Demodex mites on the right cheek, and superficial needle-scrapings confirmed their presence in the pustule. (Case 1). |
The second case is a 41-year-old woman who had been diagnosed with acne and treated with oral doxycycline (200mg/day) combined with clindamycin lotion 1% and benzoyl peroxide 2.5% for 1 month. However, two weeks ago, she noticed her face was unusually dehydrated, preventing the makeup from sticking properly. She occasionally felt itching and irritation on her face as well. Upon the physical examination, it was observed that the patient had multiple inflammatory papules and pustules on her face, especially on the chin area, with whiteheads and blackheads. Additionally, there were erythematous, dry patches with follicular scales on both cheeks (Figure 3). A standardized skin surface biopsy from her cheek showed 84 mites /cm2. Superficial needle-scrapings from five pustules found 4 mites with numerous bacteria. The patient was diagnosed with demodicosis and acne. Additional treatment consisted of oral ivermectin (200 μg/kg/week), topical permethrin cream 5%, and oral doxycycline for three months.
 |
Figure 3 Red, dry patches with scaly follicles on both cheeks accompanied by multiple whiteheads, blackheads, and inflamed papules on the chin area. (Case 2). |
In the third case, a 44-year-old female patient complained of painful nodular lumps, bumps, redness, and a burning sensation on her face for one month due to an acne breakout. She had never experienced severe acne like this before. During the physical examination, oily skin with multiple black and whiteheads, inflammatory nodules, and pustules was observed on her face, particularly around the nose and mouth, accompanied by swelling and redness (Figure 4). A standardized skin surface biopsy from her cheek showed 63 mites/cm2, while superficial needle-scrapings from five pustules found 2 Demodex mites and numerous bacteria. The patient was diagnosed with moderate to severe acne and demodicosis. The acne was treated with a combination of oral doxycycline (200 mg/day) and intralesional steroid injection (2.5mg/mL), while demodicosis was effectively treated with oral ivermectin (200 μg/kg/week) and topical permethrin cream 5% for 10 weeks. After the treatment, the patient still had post-inflammatory hyperpigmentation with comedones and some inflamed papules on the cheeks and chin (Figure 5).
 |
Figure 4 Multiple inflammatory papules, nodules, pustules, and whiteheads around the mouth accompany redness and swelling on the face. (Case 3). |
 |
Figure 5 Post-inflammatory hyperpigmentation with comedones and some inflamed papules on both cheeks and chin. (Case 3). |
Discussion
Based on the literature, demodicosis presents varying clinical features. The pityriasis folliculorum type appears as an erythematous patch on the face with dry, rough skin due to increased scaling within the hair follicle.3 The rosacea-like type causes dry, itchy, and burning skin with papulopustular facial lesions.4 The folliculitis-like type appears as localized follicular pustules that look like acne or folliculitis.5,6 The perioral dermatitis-like type presents papulopustular lesions around the mouth, resembling perioral dermatitis.7,8 The most common clinical type is pityriasis folliculorum, followed by rosacea-like and perioral dermatitis-like types.8 Moreover, abnormal Demodex mite proliferation in patients with other known skin or systemic diseases can cause secondary demodicosis, which is often mistaken for inflammatory dermatoses.9–11
The diagnosis criteria should include a correlation between clinical skin lesions and abnormal Demodex mite proliferation, confirmed by complete clinical improvement and normalization of Demodex mite density with acaricidal agents. A dermoscopy can be used to detect Demodex tails and follicular openings of Demodex mites on suspicious skin lesions.11,12
Demodex mite density is critical for diagnosing demodicosis. Standardized skin surface biopsy (SSSB) is commonly used to determine the density of Demodex mites per square centimeter, and a diagnosis of demodicosis is made when the density exceeds 5 mites /cm2,8,13 A method known as “superficial needle scraping” (SNS) is used to assess the density of Demodex mites in papulopustular lesions. Demodicosis is diagnosed when there is an abnormally high density of Demodex mites, defined as having ≥3 mites /5 pustules.14
This report has documented three cases of demodicosis in patients with acne vulgaris. The diagnosis of acne is based on clinical manifestations, which include blackheads, whiteheads, inflammatory papules, nodules, and scarring. Meanwhile, demodicosis is identified by relating the clinical presentation with the abnormal density of Demodex mite. After completing treatment with ivermectin and permethrin cream, all patients showed complete clinical improvement, and the density of Demodex mite returned to normal.
It is important to note that Demodex mites do not cause acne, although demodicosis can sometimes mimic acne.6 Nevertheless, if there is an overabundance of these mites leading to demodicosis, it can exacerbate the symptoms of acne and cause dry, scaly, itchy, stinging, burning, and irritated skin. Acne treatment may not improve these symptoms. Additionally, some topical acne treatments can also worsen symptoms of demodicosis, causing acne treatment to be more complicated.
Demodicosis, a skin disease with varied clinical symptoms, is often underdiagnosed. It is imperative that dermatologists become well-versed in identifying this condition to prevent misdiagnosis and provide appropriate treatment.
Treatment for demodicosis aims to reduce excessive Demodex mites and improve the clinical symptoms of the patients using topical acaricides such as ivermectin, permethrin, benzoyl benzoate, crotamiton, lindane, and sulfur.1,15–17 Tea tree oil and many essential oils have been found to be effective in killing Demodex mites in laboratory studies.18
All Topical treatments should be used cautiously because of sensitive skin in demodicosis patients, as many of these therapies can cause irritation. In severe cases with an excessive number of Demodex mites or sensitive skin patients, oral therapy should be considered. Oral administration of ivermectin and fluralaner can inhibit overlapping molecular pathways that regulate neuron activity. This can lead to paralysis, lack of feeding, and an indirect killing effect on Demodex mites. Studies have shown that these treatments effectively reduce Demodex mite density and improve clinical symptoms of demodicosis.19–21 Combining isotretinoin with oral ivermectin has been reported as a successful treatment for patients who do not respond to ivermectin alone.22 It is important to continue treatment until symptoms have fully resolved and mite density has returned to normal, as relapse is common in demodicosis.
Conclusion
Demodex infestation causes demodicosis, a skin condition that may resemble or coexist with other skin disorders. Accurate diagnosis can be challenging. This report describes three cases of demodicosis in acne vulgaris patients, including their symptoms, clinical presentations, and treatments. Dermatologists should be aware that demodicosis is not an uncommon skin disease. This condition can cause various symptoms in acne patients, such as redness, dryness, scaliness, itchiness, burning, and sensitive skin. Treatment specifically for acne may not improve these symptoms. A standardized skin surface biopsy and superficial needle-scraping method effectively diagnose demodicosis and reduce misdiagnosis.
Data Sharing Statement
All data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.
Statement of Ethics
The authors state that all three patients provided written informed consent for their case details and images to be published. This research complies with all Ethical Guidelines for human studies in accordance with the World Medical Association Declaration of Helsinki. This paper is exempt from The Mae Fah Luang Ethics Committee on Human Research approval with a reference number COE 177/2023. Since it is a case report with at most 3 cases, the report is derived from a review of medical records and can only be linked to an individual if the patient’s written consent is obtained.
Funding
This study did not receive any funding.
Disclosure
The authors declare no conflicts of interest.
References
1. Paichitrojjana A. Demodex: the worst enemies are the ones that used to be friends. Dermatol Rep. 2022;14(3):9339. doi:10.4081/dr.2022.9339
2. Aktaş Karabay E, Aksu Çerman A. Demodex folliculorum infestations in common facial dermatoses: acne vulgaris, rosacea, seborrheic dermatitis. An Bras Dermatol. 2020;95(2):187–193. doi:10.1016/j.abd.2019.08.023
3. Karincaoglu Y, Bayram N, Aycan O, et al. The clinical importance of demodex folliculorum presenting with nonspecific facial signs and symptoms. J Dermatol. 2004;31(8):618–626. doi:10.1111/j.1346-8138.2004.tb00567.x
4. Forton F, De Maertelaer V. Rosacea-like demodicosis and papulopustular rosacea may be two phenotypes of the same disease, and pityriasis folliculorum may be their precursor: response to the comment of Tatu. J Eur Acad Dermatol Venereol. 2019;33(1):e47–e48. doi:10.1111/jdv.15162
5. Helou W, Avitan-Hersh E, Bergman R. Demodex folliculitis of the scalp: clinicopathological study of an uncommon entity. Am J Dermatopathol. 2016;38(9):658–663. doi:10.1097/DAD.0000000000000512
6. Paichitrojjana A. Demodicosis imitating acne vulgaris: a case report. Clin Cosmet Investig Dermatol. 2022;15:497–501. doi:10.2147/CCID.S358000
7. Akilov OE, Butov YS, Mumcuoglu KY. A clinico-pathological approach to the classification of human demodicosis. J Dtsch Dermatol Ges. 2005;3(8):607–614. doi:10.1111/j.1610-0387.2005.05725.x
8. Yun CH, Yun JH, Baek JO, Roh JY, Lee JR. Demodex mite density determinations by standardized skin surface biopsy and direct microscopic examination and their relations with clinical types and distribution patterns. Ann Dermatol. 2017;29(2):137–142. doi:10.5021/ad.2017.29.2.137
9. Chen W, Plewig G. Human demodicosis: revisit and a proposed classification. Br J Dermatol. 2014;170(6):1219–1225. doi:10.1111/bjd.12850
10. Donnelly A, Kenney A, DiCaudo D. Demodicosis: clinical, dermatoscopic, 114 and microscopic correlation. J Am Acad Dermatol. 2013;68(4):AB117. doi:10.1016/j.jaad.2012.12.484
11. González HP, Santas MD, Domper LF, et al. Ex vivo dermoscopy in demodicosis. J Am Acad Dermatol. 2023;88(3):e127–e128. doi:10.1016/j.jaad.2021.07.031
12. Friedman P, Sabban EC, Cabo H. Usefulness of dermoscopy in the diagnosis and monitoring treatment of demodicidosis. Dermatol Pract Concept. 2017;7(1):35–38. doi:10.5826/dpc.0701a06
13. Forton F, Seys B. Density of Demodex folliculorum in rosacea: a case-control study using standardized skin-surface biopsy. Br J Dermatol. 1993;128(6):650–659. doi:10.1111/j.1365-2133.1993.tb00261.x
14. Huang HP, Hsu CK, Lee JY. A new superficial needle-scraping method for assessing Demodex density in papulopustular rosacea. J Cosmet Dermatol. 2020;19(4):896–900. doi:10.1111/jocd.13082
15. Sarac G. A comparison of the efficacy and tolerability of topical agents used in facial Demodex treatment. J Cosmet Dermatol. 2019;18(6):1784–1787. doi:10.1111/jocd.12986
16. Trave I, Merlo G, Cozzani E, et al. Real-life experience on effectiveness and tolerability of topical ivermectin in papulopustular rosacea and antiparasitic effect on Demodex mites. Dermatol Ther. 2019;32(6):e13093. doi:10.1111/dth.13093
17. Hecht I, Melzer-Golik A, Sadi Szyper N, Kaiserman I. Permethrin cream for the treatment of Demodex Blepharitis. Cornea. 2019;38(12):1513–1518. doi:10.1097/ICO.0000000000002013
18. Paichitrojjana A, Chalermchai T. Comparison of in vitro killing effect of Thai herbal essential oils, tea tree oil, and metronidazole 0.75% versus ivermectin 1% on Demodex folliculorum. Clin Cosmet Investig Dermatol. 2023;16:1279–1286. doi:10.2147/CCID.S414737
19. Salem DA, El-Shazly A, Nabih N, et al. Evaluation of the efficacy of oral ivermectin in comparison with ivermectin-metronidazole combined therapy in the treatment of ocular and skin lesions of Demodex folliculorum. Int J Infect Dis. 2013;17(5):e343–e347. doi:10.1016/j.ijid.2012.11.022
20. da Rocha MC, Travassos AR, Uva L, et al. Demodicosis treatment with systemic ivermectin. Skinmed. 2017;15(4):293–295.
21. Nakata Y, Fuse T, Yamato K, et al. A single amino acid substitution in the third transmembrane region has opposite impacts on the selectivity of the parasiticides fluralaner and ivermectin for ligand-gated chloride channels. Mol Pharmacol. 2017;92(5):546–555. doi:10.1124/mol.117.109413
22. Paichitrojjana A, Paichitrojjana A. Successful treatment of ivermectin refractory demodicosis with isotretinoin and permethrin cream. JAAD Case Rep. 2022;26:98–100. doi:10.1016/j.jdcr.2022.06.017
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.