Back to Journals » International Journal of General Medicine » Volume 14
Screening Practices, Knowledge and Adherence Among Health Care Professionals at a Tertiary Care Hospital
Authors Shaheen NA ![]() , Alaskar A, Almuflih A, Muhanna N
, Alaskar A, Almuflih A, Muhanna N ![]() , Barrak Alzomia S, Hussein MA
, Barrak Alzomia S, Hussein MA
Received 16 July 2021
Accepted for publication 6 October 2021
Published 20 October 2021 Volume 2021:14 Pages 6975—6989
DOI https://doi.org/10.2147/IJGM.S329056
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Naila A Shaheen,1– 3 Ahmed Alaskar,2– 5 Abdulrahman Almuflih,2 Naif Muhanna,2 Sufyan Barrak Alzomia,2 Mohammed A Hussein1– 3
1Department of Biostatistics and Bioinformatics, King Abdullah International Medical Research Center, Riyadh, Kingdom of Saudi Arabia; 2King Saud BIN Abdulaziz University for Health Sciences, Riyadh, Kingdom of Saudi Arabia; 3Ministry of National Guard Health Affairs, Riyadh, Kingdom of Saudi Arabia; 4Division of Adult Hematology and SCT, King Abdul-Aziz Medical City, Riyadh, Kingdom of Saudi Arabia; 5King Abdullah International Medical Research Center, Riyadh, Kingdom of Saudi Arabia
Correspondence: Naila A Shaheen
Department of Biostatistics and Bioinformatics, King Abdullah International Medical Research Center, King Saud BIN Abdulaziz University for Health Sciences, Ministry of National Guard-Health Affairs, P.O. Box 22490, Mail Code 1515, Riyadh, 11426, Kingdom of Saudi Arabia
Tel +966 11-4294472
Fax +966 11-4294466
Email [email protected]
Introduction: Screening, a routine procedure done on individuals with or without disease, results in the early detection of disease. The aim of this study was to assess healthcare professionals’ (HCPs) level of knowledge related to and the adherence to screening.
Methods: A survey was conducted in HCPs, using a self-administered questionnaire. Knowledge was defined based on the correct or incorrect responses to the questions. Adherence to screening was considered if a test was done at least once in the past one year.
Results: Of the 379 participants, 61% were nurses, 34% physicians, and 5% pharmacists. The majority 68.78% were female. The average age of pharmacists was 29.17± 7.09, physicians 35.57± 10.08, and nurses 35.46± 8.63 years. The knowledge related to breast cancer screening ranged between 50% and 57% and of a Pap smear, 41– 54%. 94% nurses and 90% pharmacists had recorded an incorrect response to the required age of colon cancer screening. The overall screening adherence to diabetes was 46%, hypertension 68%, liver profile 43%, lipid profile 50%, breast cancer 10.38%, Pap smear 26%, prostate cancer 33%, and colon cancer 2.37%. HCPs aged ≥ 45 years had good adherence to diabetes screening. Pharmacists (88%) had the highest level of adherence to hypertension screening. Female HCPs poorly adhered to breast 38% and cervical cancer 26% screening. Only a third 33% of males, aged > 50 years, were screened for prostate cancer. Among HCPs aged ≥ 50 years (n=32), only three were screened for colon cancer.
Conclusion: Despite the increased incidence of diabetes, breast and colon cancer in Saudi Arabia, HCPs displayed poor knowledge related to screening. The adherence to diabetes screening was good. However, HCPs in a high-risk group displayed poor adherence to screening, specifically for breast, cervical and colon cancer. The medical and cancer screening guidelines should be made available to all HCPs regardless of their specialty.
Keywords: screening, healthcare professionals, prevention, cancer screening, medical screening
Plain Language Summary
Screening is routine testing in healthy subjects with or without disease, but not developed symptoms yet. Screening and early detection of diseases results in better outcomes and reduces mortality. This is a research study focusing on healthcare professionals (including nurses, doctors and pharmacists) of all age groups working in a hospital. The study has focused on all disease areas screening including medical illnesses (eg diabetes, high blood pressure, high cholesterol) and cancer screening, ie colon, breast, cervical and prostate cancer. The study had two main objectives: (i) to assess the knowledge of healthcare professionals related to the required age for specific screening test, (ii) to assess if the healthcare professionals are adhered to the screening tests themselves. The authors had developed a questionnaire to answer the objectives. 68% participants were females, age range between (21–67) years with an average age of 35 years. The results indicated that healthcare professionals knowledge related to breast cancer screening ranged between 50% and 57%. Nurses were the least knowledgeable of colon cancer screening 94%, and diabetes 74%. The screening adherence to diabetes was 46%, checking for high blood pressure 68%, cholesterol levels 49.8%, breast cancer 10.38%, cervical cancer 26%, prostate cancer 33%, and colon cancer 2.37%.
The study results display poor knowledge of the screening guidelines, as well the participants were not adhered to the screening tests by themselves specifically for the groups with higher age or having had a positive family history of cancer in the family. Knowledge of when to request the screening test is important, so the healthcare professional can request the early initiation of the disease detection. Their own adherence is important for their health. The authors have concluded that awareness programs are needed to increase the knowledge and adherence of healthcare professionals.
Introduction
The concept of a periodic health examination was first reported by the Canadian Task Force in 1976 to determine the effect on disease prevention.1 The idea of disease prevention goes back to the 19th Century.2 However, the scope of prevention has evolved overtime.3 Screening is a routine procedure or a medical examination for individuals with or without disease, but it is still asymptomatic. According to the World Health Organization, screening is defined
as the presumptive identification of unrecognized disease in an apparently healthy, asymptomatic population by means of tests, examinations or other procedures that can be applied rapidly and easily to the target population.4
Screening and early detection of disease results in better outcomes. Cancer is the second leading cause of estimated 9.6 million deaths globally.4 The all-cause mortality due to cancer can be reduced by 1–3% by routine cancer screening.5 Early detection reduces the mortality by 15% to 20% in specific chronic diseases.6 For example, the use of a sigmoidoscopy as a screening tool for colorectal cancer resulted in a reduction in mortality from 23% to 38%.7
There are several screening programs in different countries, including the NHS Breast/Cervical screening program,8 Scottish breast screening program,9 National screening program for diabetic retinopathy,10 SeeKD screening program,11 and the Colon Cancer screening program.12 The importance of a screening program is to prevent disease, reduce healthcare cost and the early detection of disease to support effective therapeutic management.
Literature reports on the screening practices of patients globally; however, the screening practices of Healthcare Professionals (HCPs) are not widely assessed. In addition, literature reports varying results in terms of HCPs screening practices and explores primarily the level of awareness of screening of nurses regionally and internationally.13–21 Other studies explored the HCPs’ screening practices for a specific disease.22–28 Only one study with HCPs focused on medical and cancer screening.29 A study, conducted in Israel, reported that the association between the physician and patient preventive health practices indicated that patients whose physicians were adherent to the recommended screening or vaccination practices were more likely to adhere to screening or vaccination practices. HCPs’ health-related behavior and screening practices have a direct impact on patient-healthcare communication. HCPs cannot advise if they do not practice screening.30
A survey conducted in Saudi Arabia in 2015 highlighted that 92% of women, aged 50 years and older, never had a mammogram.31 Literature primarily reports the level of knowledge related to breast cancer screening in nurses,16,18,20,21,32 female healthcare professionals,33,34 or screening for one disease.24–26,35,36 Only a few studies focused on the screening of HCPs.29,37,38 Although the health needs of patients are identified and managed globally, little attention is given to HCPs care of their own health. In Saudi Arabia, a list of published studies, however, had focused on breast cancer awareness among the public.39–49 In terms of HCPs, locally a study had focused on breast cancer awareness among nursing students.32 We hypothesized that HCPs will have a low adherence to screening practices, as well as lack of knowledge of screening guidelines. The current study aimed to determine the HCPs level of knowledge for screening as well as to identify the HCPs screening practice adherence in a tertiary care hospital.
Methods
A survey was conducted with HCPs in a tertiary care hospital in year 2016 after receiving ethical approval from the local Institutional Review Board. International guidelines for screening are followed by the hospital. The screening tests are available for all the HCPs, and the cost is covered by the hospital. A questionnaire in English language was developed to elicit HCPs’ knowledge regarding medical and cancer screening guidelines, as well as their adherence to screening practices in the last year. The questionnaire included 61 questions in five domains (i) demographic and work experience (n=14), (ii) past medical history (n=14), (iii) family history (n=9), (iv) screening knowledge (n=7), and (v) screening practice adherence (n=10) [ie medical screening (n=4), cancer screening (n=6)], and screening care (n=7). The questionnaire was piloted on 10 participants prior to the data collection. The questionnaire was finalized based on the pilot data results, but no formal validation was done.
Definition of Screening Adherence
A HCP was considered to be adhered if a screening test/procedure was done at least once in the last one year.
Cancer Specific Screening
Cancer screening included breast, cervical, prostate and colon cancer screening. The cancer screening was gender specific and focused on the stipulated age for a particular screening: (i) breast cancer screening for female HCPs aged ≥40 years (ii) Pap (Papanicolaou) smear for female HCPs (iii) prostate cancer screening for male HCPs > 50 years or a positive family history for prostate cancer (iv) colon cancer screening for HCPs, aged ≥50 years, or with a positive family history of colon cancer.
Medical Screening
Medical screening for co-morbidities included diabetes mellitus (DM), hypertension, as well as liver and lipid profile screening. Medical screening was assessed for all HCPs, as follows: (i) DM screening if equal or older than 45 years, BMI (Body Mass Index) >25, HCPs with a positive family history of DM, (ii) a positive family history of hypertension, (iii) lipid profile screening if the family history indicates a high lipid profile, for male HCPs aged ≥45 years, and females HCPs aged ≥ 35 years.
Defining Knowledge of Screening Guidelines
The American Cancer Society guidelines were used to define knowledge in terms of the required age for screening for different diseases. The level of knowledge was defined as correct and incorrect responses to the questions. The knowledge regarding breast cancer screening was based on three questions (i) what is your understanding of a mammogram? (screening test vs therapeutic test) (ii) at what age should a woman have a mammogram? (≥30, ≥40 or ≥50 years) (iii) in your opinion, if a woman’s breast self-examination is normal, is a mammogram still required? (No/yes). The answers were correct if the selected choices were “screening test”, “≥40 years” and “No”. Knowledge related to cervical cancer screening was assessed with one question (i) in your opinion, at what age should a woman have a Pap smear? (20, 25 or 30 years or when she becomes sexually active). The correct response was “when she becomes sexually active”. The knowledge of colon cancer screening was assessed by one question (i) in your opinion, at what age, should screening for colon cancer be done? (30, 40 or 50 years). The correct option is 50 years.
The knowledge regarding DM screening was elicited with two questions (i) in your opinion, at what age, should screening for diabetes be done? (30, 40–45 or 50 years), (ii) in your opinion, screening for DM depends on which risk factors? (BMI>25, first-degree relative diagnosed with diabetes, ethnicity (Asian, African American), sedentary life style, all of the above). The choices (i) 40–45 years, and (ii) all of the above, were correct.
Screening Care Questions
The screening care questions explored whether the screening test was requested by the primary care physician, whether the HCP requested or attended the screening, and the reasons for not attending the screening test.
Study Participants
All HCPs (nurses, physicians, and pharmacists) with no restriction in terms of nationality, age, gender or the specialty, who are directly involved in patient management, were invited to participate in the study. Individuals with a healthcare background but not practicing were excluded from the study. The study was approved by Institutional Review Board, number SP15/041. This study was conducted in accordance with the Declaration of Helsinki. All participants were adequately informed of the aims, methods, and risks related to participating in the study, the voluntary nature of participation and confidentiality in the introduction of the survey. Written informed consent was documented by the study team members for agreeing participants.
Sample Size and Sampling Technique
The primary objective of this study was to determine the level of adherence to screening practices of HCPs. Adherence was measured as the proportion of HCPs who complied with at least 50% of the recommended screening tests or procedures in the last year. Assuming 50% of healthcare professionals adhered to the recommended screening practices,50 the relative margin of error of 5%, and finite population, we estimated the sample size to be 372 participants.
The study was conducted in the different healthcare departments in a tertiary care hospital. A formal introduction was provided on the first page of the survey. The self-administered questionnaire was distributed to the HCPs as a hard copy during their working hours by the study team. All eligible participants who agreed to participate were requested to complete the questionnaire upon their feasibility, and it was collected back by the study team. The questionnaire filling took 10–15 minutes on average.
Statistical Analysis
All the variables were summarized and reported with descriptive statistics. Age, BMI, years of experience, and number of patients seen per day are reported as the mean and standard deviation or median and interquartile range. Gender, past medical history, and family history are reported as frequency and percentage. The screening practices, adherence and knowledge were compared by gender and HCP, using a Chi-square test for independence or Fisher's exact test. Results were reported as frequency, percentage and p-value. Statistical significance was declared at p-value less than 0.05. The analyses for medical and cancer screening were conditional based on the age, gender, and family history of the HCPs.
Medical Screening
Medical screening for co-morbidities included diabetes mellitus (DM), hypertension, as well as liver and lipid profile screening. Medical screening was assessed for all HCPs, and by specific conditions: (i) DM screening if equal or older than 45 years, BMI (Body Mass Index) >25, HCPs with a positive family history of DM, (ii) a positive family history of hypertension, (iii) lipid profile screening if the family history indicates a high lipid profile, for male HCPs aged ≥45 years, and females HCPs aged ≥35 years.
Cancer Specific Screening
Cancer-specific screening included breast, cervical, prostate and colon cancer screening. The cancer screening was gender specific and focused on the stipulated age for a particular screening: (i) breast cancer screening for female HCPs aged ≥40 years or if it had a positive family history of breast cancer, (ii) Pap (Papanicolaou) smear for all female HCPs (iii) prostate cancer screening for male HCPs age >50 years or a positive family history for prostate cancer (iv) colon cancer screening for HCPs, aged ≥50 years, or if had a positive family history for colon cancer.
Statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Results
Demographic Characteristics and Work Experience of Healthcare Professionals
Of the 379 participants, 231 (61%) were nurses, 129 (34%) physicians, and 19 (5%) pharmacists. A third of the sample 110 (29%) were Saudi, and 260 (68.78%) female. The majority of the nurses were female 224 (97%), and the pharmacists were male 16 (84%). The majority of the HCPs 259 (89%) obtained their professional training locally. Just more than half 208 (55%) of the sample were currently married. The pharmacists were younger (29.17±7.09) than the physicians (35.57±10.08), and nurses (35.46±8.63). The average years of experience was lower for the pharmacists (5.56±6.50), compared to the nurse (11.53±7.13), and physician (10.09±9.24). The majority of the sample 331 (89%) were not smokers (Table 1).
 |
Table 1 Demographic Characteristics of the Study Groups |
Screening Knowledge of the Overall Sample
Almost a third of the participants 116 (30%) responded correctly to the four knowledge questions (Figure 1). Half 199 (53%) responded correctly to the questions regarding the age required for screening breast cancer, and Pap smear 191 (52%). Only 75 (20%) had answered correctly the required age for screening colon cancer. 121 (32%) had answered correctly the required age of DM screening. The risk factors of developing DM was correctly answered by 287 (78%) (Table 2).
 |
Table 2 Medical and Cancer Screening Knowledge by Healthcare Professionals |
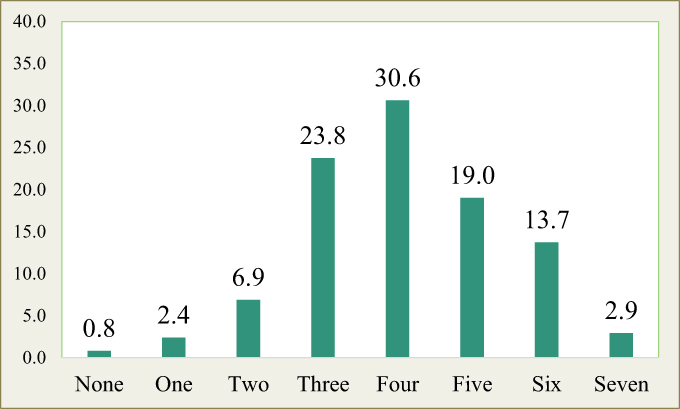 |
Figure 1 Number of correct responses for the knowledge questions. |
Screening Knowledge of HCPs
The HCPs’ knowledge related to medical and cancer screening is displayed in Table 2. The majority of the sample had a correct response of a mammogram as a screening test, the nurses 218 (96%), physicians 120 (100%), and pharmacists 18 (95%). The difference between the HCPs was statistically significant (p=0.033). However, the recommended age (≥40 years) for the first screening mammogram was correctly responded, ranging from 50% to 57%. The screening for cervical cancer (when a woman becomes sexually active) was correctly responded by 122 (54%) nurses, 62 (49%) physicians, and 7(41%) pharmacists (p=0.395). The specified age (50 years) at which colon cancer screening should be initiated, was correctly answered by nurses 13 (6%) nurses, 60 (47%) physicians, and 2(10.5%) (p=<0.0001). The risk factors of developing DM was correctly answered by 173 (78%) nurses, 106 (82%) physicians, and 10 (56%) pharmacists (p=0.001). The screening age (≥40 years) for DM was correctly answered by 58 (26%) nurses, 54 (43%) physicians, and 9(47%), pharmacists (p=0.001) (Table 2).
Screening Knowledge by Gender
Knowledge related to medical and cancer screening in terms of gender is displayed in Table 3. Both the males 118 (99%) and females 247 (97%) had answered correctly the mammogram as a screening test. However, regarding the age (≥40 years) required for the first mammogram, correctly answered by 63 (54%) males, and 136 (53%) females (p=0.962). When to screen for cervical cancer was correctly answered by 51 (45%) males, and 140 (55%) females (p=0.065). The specified age for colon cancer screening was responded correctly by 48 (40%) males, and 27 (11%) females (p=<0.0001). The risk factors of developing DM were correctly answered by 91 (77%) males, and 196 (79%) females. The required age for commencing DM screening was correctly answered by 48 (41%) males, and 73 (29%) females (p=0.019).
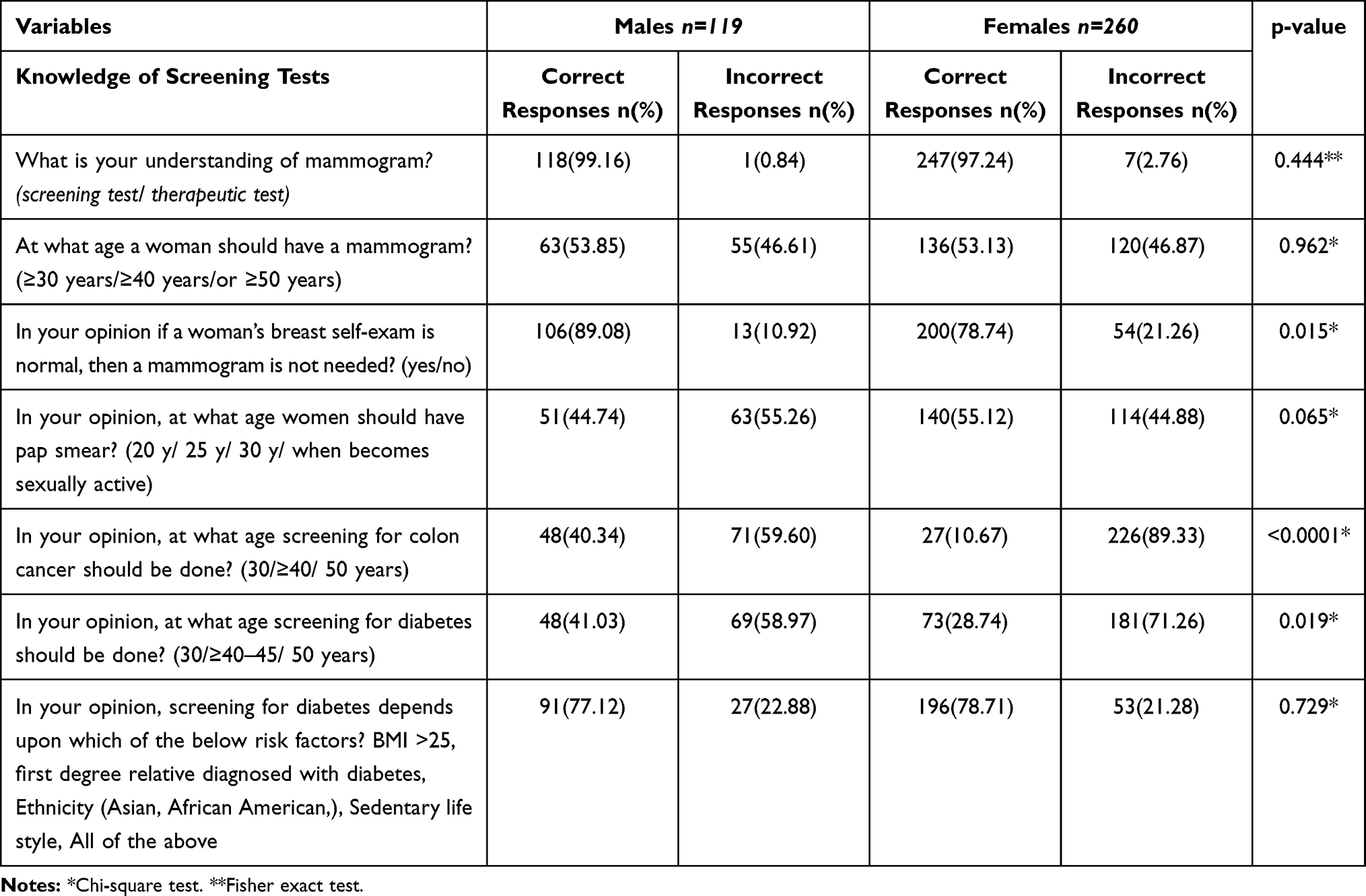 |
Table 3 Medical and Cancer Screening Knowledge by Healthcare Professionals’ Gender |
Screening Adherence of the Overall Sample
The proportions of the overall sample in terms of screening adherence for DM were (176/379;46.4%), hypertension (260/379;68.6%), liver function test (165/379;43.5%), lipid profile (189/379;49.8%), breast cancer screening (27/260;10.38%), Pap smear (36/139;25.89%), prostate cancer screening (10/119;8.40%), and colon cancer screening (9/379;2.37%) (Table 4).
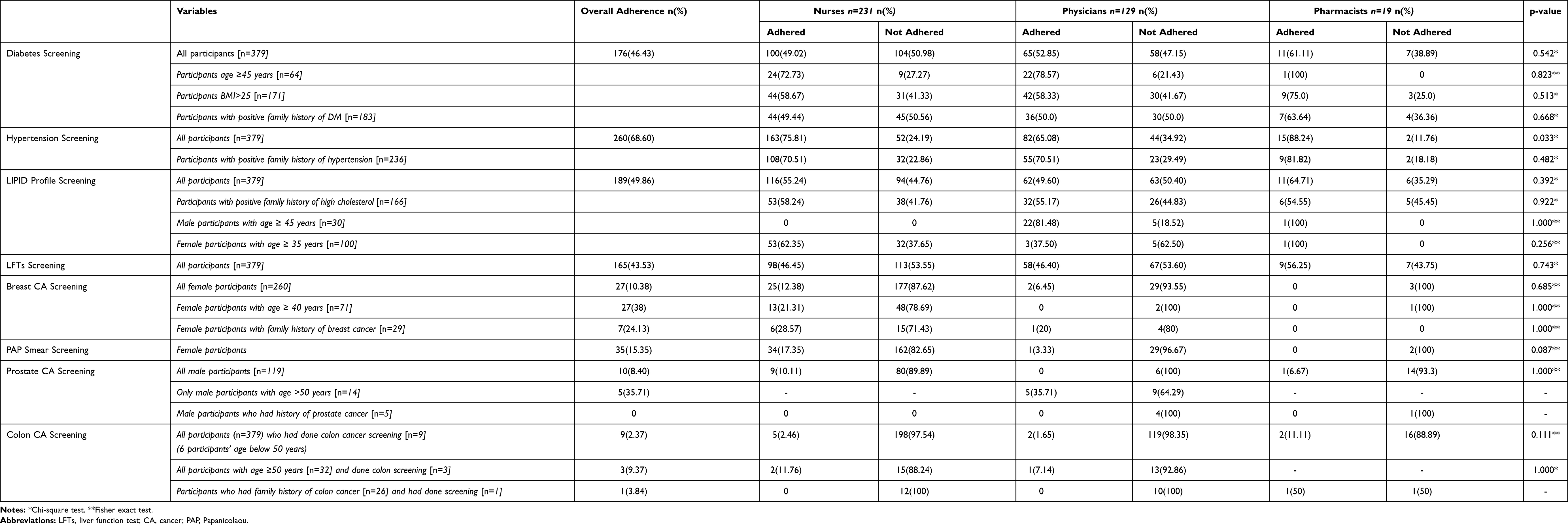 |
Table 4 Distribution of Medical and Cancer Screening Adherence by Healthcare Professionals |
Of the five general screening adherence questions (four medical and one colon cancer), almost a third 105 (28%) of the sample adhered to four questions. Notably, 86 (23.4%) reported no adherence with any of the questions (Figure 2).
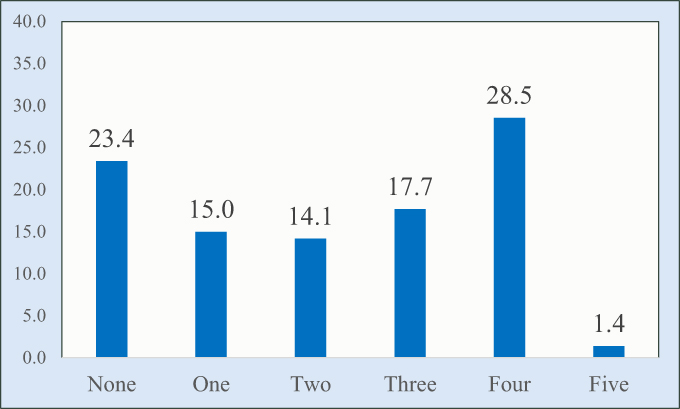 |
Figure 2 Number of screening questions adhered. |
Specific Screening Adherence by HCPs and Gender
Diabetes Screening Adherence
The HCPs aged ≥45 years (n=64) reported good adherence to DM screening, among nurses 24 (72%), physicians 22 (78%), and pharmacists 1(100%). For the HCPs with a BMI>25 (n=171), the majority of the pharmacists 9(75%) adhered to DM screening compared to the nurses 44 (58%) and the physicians 42 (58%) (p=0.513). The HCPs with a positive family history for DM (n=183), for all HCPs, approximately half adhered to DM screening, the nurses 44 (50%), physicians 36 (50%), and pharmacists 7(63%) (p=0.668) (Table 4). Among participants aged ≥45 years, 23 (82%) males, and 24 (70%) females were adherent to DM screening (p=0.290). For the participants with a BMI > 25 (n=171), both males 46 (61%) and females 49 (58%) displayed good adherence to DM (p=0.777). For the participants with a positive family history of DM (n=183), both genders were adherent to DM screening (p=0.265) (Table 5).
 |
Table 5 Distribution of Medical and Cancer Screening Adherence by Gender |
Hypertension Screening Adherence
Among the HCPs with a positive family history of hypertension (n=236), pharmacists 9(81%), were mostly adhered to hypertension screening, followed by nurses 108 (70%), and physicians 55 (70%) (p=0.482) (Table 4). 51 (77%) males and 121 (74%) females with a positive family history for hypertension (n=236), were adherent to hypertension screening (p=0.629) (Table 5).
Lipid Profile Screening Adherence
The HCPs with a positive family history of high cholesterol (n=166) had displayed good adherence to lipid profile screening, among nurses 53 (58%), physicians 32 (55%), and pharmacists 6(54%) (p=0.922). The males aged ≥45 years (n=30), were mostly adherent to hypertension screening for the physicians 22 (81%), and the pharmacists 1(100%). For the females, aged ≥35 years (n=100), the physicians were least likely three (37%) to screen for the lipid profile, compared with the nurses 53 (62%), and the pharmacists 1(100%), (p=0.256) (Table 4). Among the participants with a positive family history for high cholesterol (n=160), both males 26 (52%) and females 65 (59%) had displayed good adherence to lipid profile screening (p=0.401) (Table 5).
Liver Profile Screening Adherence
Screening for the liver profile was low for nurses 98 (46%), physicians 58 (46%) and pharmacists 9(56%) (p=0.743) (Table 4). For the overall sample (n=379), 54 (48%) males and 111 (46%) females had displayed good adherence to liver profile screening (p=0.730) (Table 5).
Colon Cancer Screening Adherence
For HCPs, aged ≥50 years (n=32), only three screened for colon cancer, nurses two (11.7%), and a physician 1(7.14%). The HCPs with a positive family history for colon cancer (n=26), only one pharmacist was adhered to colon cancer screening (Table 4). For the participants aged ≥50 years (n=32), adherence to colon cancer screening was very poor in both males 1(7%) and females 2(13%) (Table 5).
Breast Cancer Screening Adherence
The females, aged ≥40 years (n=71), displayed poor adherence to breast cancer screening, among the nurses 13 (21%), none of the two physicians, and a pharmacist. For the females with a positive family history for breast cancer (n=29), only six (28%) of the nurses, and one (20%) physician had adhered to breast cancer screening (Table 4).
PAP Smear Screening Adherence
Among the females (n=260), the adherence to pap smear screening was poor among nurses 34 (17%), and physicians 1(3.3%) (p=0.087) (Table 4).
Prostate Cancer Screening Adherence
All males, aged >50 years (n=14) were physicians. Only five (35.7%) had displayed adherence to prostate cancer screening. There were only five males with a positive family history of prostate cancer, four physicians and one pharmacist, but none was adherent to prostate cancer screening (Table 4).
Screening Care Practices
For the overall sample, the majority 353 (94%) indicated that a reminder for a screening test would be helpful. Only 96 (25%) reported that their treating physician referred them for screening. A third of the participants 124 (33%) had reported requesting a screening test, and a small proportion 63 (17%) reported not attending a screening test. The reason for non-attendance was a busy schedule 195 (79%), or being scared of a positive result 31 (12.6%). The majority 181 (71%) of the females had never attended the well women clinic (Supplemental Table 1).
Discussion
This study focused on the knowledge of HCPs regarding the specified age for the initiation of screening for cancer and medical conditions, as well as the adherence of the HCPs to the screening tests. The results of the current study indicated that the HCPs had a poor knowledge of the specified age for various screening tests. The comparison of HCPs’ knowledge across studies is challenging since studies have assessed different aspects of the screening, differences in HCPs (nurses, physicians, technicians, paramedics, interns, and medical students), different age inclusion criteria of the participants, and due to heterogeneity in defining knowledge.
A study had reported good knowledge in HCPs (physicians, nurses, interns, and medical students) of mammogram as a screening test similar to the current study,51 while another study had reported very poor knowledge (20%) of mammogram as a screening method.52 A study had concluded to improve the knowledge and practices of female HCPs for breast and cervical cancer screening, similar to the current study.34 In the current study, screening for breast, cervical and colon cancer was poor. The adherence to Pap smear was poor among the nurses (24%) and physicians (7%). The finding supports a Sri Lankan study reporting (17%) adherence.34 In contrast, a study done in Brazil reported (95%) adherence to have a Pap smear done at least once.29
Adherence to breast cancer screening was very poor for the nurses and physicians. This is concerning as the level of adherence was poor even with a positive history of breast cancer in the family. The results of the current study are aligned with a national survey conducted in Saudi Arabia, which reported that for women aged 50 years and above, 92% never had a mammogram.31 It should be noted that the population for the current study was HCPs. Literature reports breast cancer screening ranging from 3% to 35%.34–37 A study conducted in Sri Lanka reported the need to improve the knowledge and screening practices of female healthcare workers.34 However, a study conducted in Brazil with HCPs (females n=228) reported an adherence rate of (72%) for mammography. Moreover, the age inclusion criteria (40 and above) are of note compared with the current study.29
Colon cancer is the most prevalent cancer (11.1%) in Saudi Arabia, second to breast cancer (14.2%).54,55 The data reported from Saudi Cancer Registry, 2015 had reported colorectal cancer (14.9%)56 as a most common cancer in men and third most common in females (9.9%). The reported median age at diagnosis is 59 years (range 8–94) in males, and 57 years (range 15–102) years in females. The younger age at presentation warrants a change in the colon cancer screening guidelines locally.55 In the current study, similar to breast cancer screening, the adherence to colon cancer screening was very poor (9%) in the participants aged 50 years and above. Of concern is that in the participants with a family history of colon cancer, only one was screened. A study among HCPs (physicians, nurses, and nurse assistants) in Brazil had reported only (6/333;1.6%) adherence with colon cancer screening.29 The current study results are in contrast with a study conducted with family physicians, as almost half (47%) were screened,36 a study from Germany (2018) reported a screening rate of 72% for physicians,27 and a study with primary care physicians reported 50% cancer screening.50
In the current study, screening for medical conditions (DM, hypertension, high cholesterol) were above 50%. The screening of DM (46% vs. 78%), hypertension (68% vs. 71%), and the lipid profile (50% vs. 61%) in the current study is low compared with a study reported among HCPs in Brazil. However, the included participants in our study are all age groups compared to studies in Brazil (40 and above).29 The current study reports low adherence to screening, however higher to a study conducted among physicians (38/138; 27%).57 The reported adherence was low despite the fact that (59.4%) physicians had realized the importance of the screening tests.
The main reasons for not adhering to screening were ‘lack of time (55.6%), supporting the current study as (79%) indicated a “busy schedule” as the reason for non-adherence.57 The current study results indicate that the majority (66%) of the participants had received an influenza vaccination, compared to a prior study (46%).57
Doing a screening test has been linked with the level of knowledge.53 In the current study, both knowledge and adherence to screening were poor. A positive association between physicians and their patients’ screening practices has been reported.30 To improve the HCP-patient communication, we recommend identifying the barriers underpinning poor adherence to screening practices.
Limitations
Knowledge was only assessed in terms of the stipulated age for screening. We did not include other factors of screening for various diseases, to prevent a low response rate due to a lengthy questionnaire. A specific cancer screening assessment resulted in a low sample size. Only very few participants had the oncology specialty. However, we assume that they might have more knowledge compared to non-oncology HCPs, which requires further exploration.
Conclusion
Screening and early detection are key in disease prevention. The HCPs had good knowledge related to the risk factors of developing DM, but poor knowledge of the age at which DM screening should be initiated. Despite the high prevalence of breast and colon cancer in Saudi Arabia, the HCPs had poor knowledge regarding the age stipulated for disease-specific cancer screening. The adherence to DM screening was good, but poor for breast, cervical and colon cancer in the high-risk groups. The medical and cancer screening guidelines should be made available to all HCPs regardless of their specialty. Educational programs, targeting HCPs, are recommended. Additional studies are recommended to explore the barriers underpinning non-adherence to screening in HCPs.
Abbreviations
HCPs, health care professionals; NHS, National Health Service; Pap, Papanicolaou; WHO, World Health Organization.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to the institutional rules and regulations but are available from the author on a reasonable request.
Acknowledgment
The authors would like to thank Dr. Susana Wright for editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the arctile; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this research.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. The periodic health examination. Canadian task force on the periodic health examination. Can Med Assoc J. 1979;121(9):1193–1254
2. Britannica E Preventive medicine. Available from: https://www.britannica.com/science/preventive-medicine.
3. Starfield B, Hyde J, Gérvas J, Heath I. The concept of prevention: a good idea gone astray? J Epidemiol Community Health. 2008;62(7):580–583. doi:10.1136/jech.2007.071027
4. World Health Organization. Available from: https://www.who.int/news-room/fact-sheets/detail/cancer.
5. Stang A, Jockel K-H. The impact of cancer screening on all-cause mortality. Dtsch Arztebl Int. 2018;115(29–30):481–486. doi:10.3238/arztebl.2018.0481
6. World Health Organization. Early detection of cancer. Available from: http://www.who.int/cancer/detection/en/.
7. Robert H, Thomas J. Tests for screening for colorectal cancer: stool tests, radiologic imaging and endoscopy; 2014. Available from: http://www.uptodate.com/contents/tests-for-screening-for-colorectal-cancer-stool-tests-radiologic-imaging-and.
8. NHS population screening programs. Available from: https://www.gov.uk/topic/population-screening-programmes.
9. NHS health Scotland. Available from: http://www.healthscotland.scot/health-topics/screening/breast-screening.
10. The national diabetic retinal screening programme. Available from: http://www.diabeticretinascreen.ie/.
11. Galbraith LE, Ronksley PE, Barnieh LJ, et al. The See Kidney Disease Targeted Screening Program for CKD. Clin J Am Soc Nephrol. 2016;11(6):964–972. doi:10.2215/CJN.11961115
12. Quality A for HR. Automated calls followed by mailed kits significantly increase colorectal cancer screening rate in those overdue for testing. Available from: https://innovations.ahrq.gov/profiles/automated-calls-followed-mailed-kits-significantly-increase-colorectal-cancer-screening.
13. Odusanya OO, Tayo OO. Breast cancer knowledge, attitudes and practice among nurses in Lagos, Nigeria. Acta Oncol. 2001;40(7):844–848. doi:10.1080/02841860152703472
14. Haji-Mahmoodi M, Montazeri A, Jarvandi S, Ebrahimi M, Haghighat S, Harirchi I, Breast self-examination: knowledge, attitudes, and practices among female health care workers in Tehran, Iran. Breast J. 2002;8(4):222–225. doi:10.1046/j.1524-4741.2002.08406.x
15. Ceber E, Soyer MT, Ciceklioglu M, Cimat S. Breast cancer risk assessment and risk perception on nurses and midwives in Bornova Health District in Turkey. Cancer Nurs. 2006;29(3):244–249. doi:10.1097/00002820-200605000-00013
16. Cavdar Y, Akyolcu N, Ozbas A, Oztekin D, Ayogu T, Akyuz N. Determining female physicians’ and nurses’ practices and attitudes toward breast self-examination in Istanbul, Turkey. Oncol Nurs Forum. 2007;34(6):1218–1221. doi:10.1188/07.ONF.1218-1221
17. Chong P, Krishnan M, Hong CY, Swah TS. Knowledge and Practice of Breast Cancer Screening Amongst Public Health Nurses in Singapore. Singapore Med J. 2002;43:509–516.
18. Yaren A, Ozkilinc G, Guler A, Oztop I. Awareness of breast and cervical cancer risk factors and screening behaviours among nurses in rural region of Turkey. Eur J Cancer Care (Engl). 2008;17(3):278–284. doi:10.1111/j.1365-2354.2007.00856.x
19. Alsaif A. Breast self-examination among Saudi female nursing students in Saudi-Arabia. Saudi Med J. 2004;25:1574–1578.
20. Sreedharan J, Muttappallymyalil J, Venkatramana M, Thomas M. Breast self-examination: knowledge and practice among nurses in United Arab Emirates. Asian Pac J Cancer Prev. 2010;11(3):651–654.
21. Awodele O, Adeyomoye AAA, Awodele DF, Kwashi V, Awodele IO, Dolapo DC. A study on cervical cancer screening amongst nurses in Lagos University Teaching Hospital, Lagos, Nigeria. J Cancer Educ. 2011;26(3):497–504. doi:10.1007/s13187-010-0187-6
22. Zahedi L, Sizemore E, Malcolm S, Grossniklaus E, Nwosu O. Knowledge, attitudes and practices regarding cervical cancer and screening among Haitian health care workers. Int J Environ Res Public Health. 2014;11(11):11541–11552. doi:10.3390/ijerph111111541
23. Shin HY, Suh M, Park B, Jun JK, Choi KS. Perceptions of colorectal cancer screening and recommendation behaviors among physicians in Korea. BMC Cancer. 2017;17(1):860. doi:10.1186/s12885-017-3881-5
24. Manners D, Wilcox H, McWilliams A, Piccolo F, Liira H, Brims F. Current lung cancer screening practice amongst general practitioners in Western Australia: a cross-sectional study. Intern Med J. 2018;48(1):78–80. doi:10.1111/imj.13670
25. Hallowell BD, Puricelli Perin DM, Simoes EJ, et al. Breast cancer related perceptions and practices of health professionals working in Brazil’s network of primary care units. Prev Med (Baltim). 2018;106:216–223. doi:10.1016/j.ypmed.2017.11.002
26. Nguyen-Truong CKY, Hassouneh D, Lee-Lin F, et al. Health Care Providers’ Perspectives on Barriers and Facilitators to Cervical Cancer Screening in Vietnamese American Women. J Transcult Nurs off J Transcult Nurs Soc. 2018;29(5):441–448. doi:10.1177/1043659617745135
27. Fischbach W, Al-Taie O. How do Doctors Manage Their Own Colorectal Cancer Screening and What Do They Recommend Their Patients? - Results of a Survey Under General Physicians and Internists. Dtsch Med Wochenschr. 2018;143(19):e172–e176. doi:10.1055/a-0629-5894
28. Currie S, Mercer CH, Dunbar KJ, Saunders J, Woodhall SC. Do healthcare professionals and young adults know about the National Chlamydia Screening Programme? Findings from two cross-sectional surveys. Int J STD AIDS. 2019;30(1):72–78. doi:10.1177/0956462418797849
29. Gonçalves-Silva AC, Murta-Nascimento C, Eluf-Neto J. Assessing screening practices among health care workers at a tertiary-care hospital in Sao Paulo, Brazil. Clinics (Sao Paulo). 2010;65(2):151–155. doi:10.1590/S1807-59322010000200006
30. Frank E, Dresner Y, Shani M, Vinker S. The association between physicians’ and patients’ preventive health practices. CMAJ. 2013;185(8):649–653. doi:10.1503/cmaj.121028
31. El Bcheraoui C, Basulaiman M, Wilson S, et al. Breast cancer screening in Saudi Arabia: free but almost no takers. PLoS One. 2015;10(3):e0119051. doi:10.1371/journal.pone.0119051
32. Yousuf S. Breast Cancer Awareness among Saudi Nursing Students. JKAU Med Sci. 2010;17:67–78. doi:10.4197/Med.17-3.6
33. Deniz S, Coskun F, Oztas D, Kurt AO. Knowledge, attitudes and behaviors of breast and cervical cancers and screenings of women working in primary health care services. J BUON. 2018;23(7):44–52.
34. Nilaweera RIW, Perera S, Paranagama N, Anushyanthan AS. Knowledge and practices on breast and cervical cancer screening methods among female health care workers: a Sri Lankan experience. Asian Pac J Cancer Prev. 2012;13(4):1193–1196. doi:10.7314/apjcp.2012.13.4.1193
35. Triantafillidis JK, Vagianos C, Gikas A, Korontzi M, Papalois A. Screening for colorectal cancer: the role of the primary care physician. Eur J Gastroenterol Hepatol. 2017;29(1):e1–e7. doi:10.1097/MEG.0000000000000759
36. Sahin MK, Aker S. Family Physicians’ Knowledge, Attitudes, and Practices Toward Colorectal Cancer Screening. J Cancer Educ. 2017;32(4):908–913. doi:10.1007/s13187-016-1047-9
37. Sanchis-Gomar F, Moran M, Lucia A. Time for doctors to practise what they preach and preach what they practise. Br J Sports Med. 2016;50(20):1288. doi:10.1136/bjsports-2016-096076
38. Kirschen GW, Lane DS, Messina CR, Fisher PR. Do they practice what we preach: findings from over a decade of breast imaging CME. Breast J. 2018;24(1):101–102. doi:10.1111/tbj.12845
39. Hussein DM, Alorf SH, Al-Sogaih YS, et al. Breast cancer awareness and breast self-examination in Northern Saudi Arabia. A preliminary survey. Saudi Med J. 2013;34(7):681–688.
40. Radi SM. Breast Cancer awareness among Saudi females in Jeddah. Asian Pac J Cancer Prev. 2013;14(7):4307–4312. doi:10.7314/apjcp.2013.14.7.4307
41. Al-Zalabani AH, Alharbi KD, Fallatah NI, Alqabshawi RI, Al-Zalabani AA, Alghamdi SM. Breast Cancer Knowledge and Screening Practice and Barriers Among Women in Madinah, Saudi Arabia. J Cancer Educ off J Am Assoc Cancer Educ. 2018;33(1):201–207. doi:10.1007/s13187-016-1057-7
42. Al-Musa HM, Awadalla NJ, Mahfouz AA. Male Partners’ Knowledge, Attitudes, and Perception of Women’s Breast Cancer in Abha, Southwestern Saudi Arabia. Int J Environ Res Public Health. 2019;16:17. doi:10.3390/ijerph16173089
43. Al Otaibi S, Al Harbi M, Al Kahmoas A, et al. General Breast Cancer Awareness among Women in Riyadh City. Asian Pac J Cancer Prev. 2017;18(1):159–163. doi:10.22034/APJCP.2017.18.1.159
44. Nageeti TH, Abdelhameed AAN, Jastania RA, Felemban RM. Perspective of Saudi women in the Makkah region on breast cancer awareness. J Family Community Med. 2017;24(2):97–101. doi:10.4103/2230-8229.205116
45. Ashareef B, Yaseen W, Jawa W, et al. Breast Cancer Awareness among Female School Teachers in Saudi Arabia: a Population Based Survey. Asian Pac J Cancer Prev. 2020;21(2):337–342. doi:10.31557/APJCP.2020.21.2.337
46. Binhussien BF, Ghoraba M. Awareness of breast cancer screening and risk factors among Saudi females at family medicine department in security forces hospital, Riyadh. J Fam Med Prim Care. 2018;7(6):1283–1287. doi:10.4103/jfmpc.jfmpc_286_18
47. Alsareii SA, Alqahtani SM, Alamri AM, et al. Awareness of Breast Cancer among Female Students and Faculty from Najran University, Najran, Saudi Arabia. Asian Pac J Cancer Prev. 2020;21(5):1415–1422. doi:10.31557/APJCP.2020.21.5.1415
48. Alsowiyan AA, Almotyri HM, Alolayan NS, Alissa LI, Almotyri BH, AlSaigh SH. Breast cancer knowledge and awareness among females in Al-Qassim Region, Saudi Arabia in 2018. J Fam Med Prim Care. 2020;9(3):1712–1718. doi:10.4103/jfmpc.jfmpc_1065_19
49. Farsi NJ, Al-Wassia R, Merdad L. Do Men and Women in Saudi Arabia Have the Same Level of Awareness and Knowledge of Breast Cancer? A Cross-Sectional Study. Breast Cancer (Dove Med Press. 2020;12:131–139. doi:10.2147/BCTT.S262544
50. Seong H-Y, Park E-W, Cheong Y-S, Choi E-Y, Kim K-S, Seo S-W. Health-promotion and disease-prevention behaviors of primary-care practitioners. Korean J Fam Med. 2014;35(1):19–27. doi:10.4082/kjfm.2014.35.1.19
51. Kumar S, Imam AM, Manzoor NF, Masood N. Knowledge, attitude and preventive practices for breast cancer among health care professionals at Aga Khan Hospital Karachi. J Pak Med Assoc. 2009;59(7):474–478.
52. Akhigbe AO, Omuemu VO. Knowledge, attitudes and practice of breast cancer screening among female health workers in a Nigerian urban city. BMC Cancer. 2009;9:203. doi:10.1186/1471-2407-9-203
53. Ibrahim NA, Odusanya OO. Knowledge of risk factors, beliefs and practices of female healthcare professionals towards breast cancer in a tertiary institution in Lagos, Nigeria. BMC Cancer. 2009;9(1):76. doi:10.1186/1471-2407-9-76
54. Bazarbashi S, Al Eid H, Minguet J. Cancer Incidence in Saudi Arabia: 2012 Data from the Saudi Cancer Registry. Asian Pac J Cancer Prev. 2012;18(9):2437–2444. doi:10.22034/APJCP.2017.18.9.2437
55. Alsanea N, Abduljabbar AS, Alhomoud S, Ashari LH, Hibbert D, Bazarbashi S. Colorectal cancer in Saudi Arabia: incidence, survival, demographics and implications for national policies. Ann Saudi Med. 2015;35(3):196–202. doi:10.5144/0256-4947.2015.196
56. Cancer Incidence Report; 2015. Saudi Arabia: Saudi Health Council National Health Information Center Saudi Cancer Registry. Available from: https://nhic.gov.sa/eServices/Documents/E%20SCR%20final%206%20NOV.pdf. Accessed October 17, 2021.
57. Peleg R, Ostermich A, Gienco V, Portughiez E. Screening tests among family doctors: do we do as we preach? Public Health. 2013;127(3):282–289. doi:10.1016/j.puhe.2012.12.010
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.