Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Scientific Evidence of Acupuncture for Post-Stroke Cognitive Impairment: An Overview of Systematic Reviews and Meta-Analyses
Authors Zhou Q, Ji Y, Lv Y, Xue J, Wang Y, Huang Y
Received 3 February 2023
Accepted for publication 22 May 2023
Published 3 July 2023 Volume 2023:19 Pages 1503—1513
DOI https://doi.org/10.2147/NDT.S407162
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yu-Ping Ning
Qiongyang Zhou,1,* Yue Ji,2,* Yanzhu Lv,3 Jing Xue,3 Yuhui Wang,3 Yin Huang4
1Department of Acupuncture and Moxibustion, The First People’s Hospital of Wenling, Wenling, People’s Republic of China; 2First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China; 3Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China; 4Department of Acupuncture, Changshu Hospital Affiliated to Nanjing University of Chinese Medicine, Changshu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yin Huang, Email [email protected]
Background: Acupuncture may be effective to treat post-stroke cognitive impairment (PSCI). We aimed to evaluate the reliability of the systematic reviews/meta-analyses (SRs/MAs) evidence regarding acupuncture treatment of PSCI.
Methods: The methodological quality was appraised with Methodological Quality of Systematic Reviews 2 (AMSTAR-2). We evaluated reporting quality with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and evidence quality with Grade of Recommendation, Assessment, Development and Evaluation (GRADE) system.
Results: The inclusion criteria were met by fifteen reviews. All studies assessed by AMSTAR-2 had critically poor methodological quality due to the limitations on the lack of the provision of the list of excluded trails, screening of duplicate study, and protocol registration. For reporting quality, response rate of “yes” was less than 50% in Q5 (protocol and registration topic), Q8 (Search) and Q23 (Additional analysis). Evidence quality of outcome measures was low or worse with GRADE because when the data was qualitatively synthesized, low quality and small sample size trials provided the data.
Conclusion: Acupuncture may be beneficial for PSCI. Because of limitations and inconsistent conclusions, further research is needed to provide higher evidence for acupuncture on PSCI.
Keywords: acupuncture, treatment, cognitive impairment, stroke, evidence
Introduction
Stroke is a complex systemic disease that is the world’s third leading cause of disability.1 As a frequent complication of stroke, post-stroke cognitive impairment (PSCI) affects approximately 80% of stroke survivors and is characterized by impaired learning and memory and deficits in executive function.2 PSCI tends to be associated with adverse outcomes, including poor functional outcome,3 poor quality of life,4 and high mortality.5 Therefore, effective management of PSCI is essential to promote the recovery of survivors and reduce the burden on society. Stroke rehabilitation methods have developed rapidly, in which cognitive function training (CFT) is used as the basic treatment for PSCI.6 However, no single rehabilitation method was determined to be significantly beneficial for recovery.6 As a result, recent research on the use of complementary therapies for stroke rehabilitation has been conducted.7
Acupuncture is an increasingly widely used alternative treatment worldwide.8,9 The World Health Organization believes that acupuncture is a good complementary treatment option for stroke rehabilitation.10 The positive effects of acupuncture on stroke rehabilitation are mediated by a variety of mechanisms, including the stimulation of neuroprotective factors, regulation of neurochemicals, inhibition of inflammatory damage, neurogenesis stimulation and cell division in the central nervous system, as well as control of cerebral blood flow in the ischemic region.10 Comprehensive evidence suggests that acupuncture is beneficial for recovery from stroke complications, including post-stroke aphasia, post-stroke dysphagia, and post-stroke insomnia.7,11,12 Furthermore, acupuncture has received increasing attention for improvement of cognitive function in stroke patients.13 However, its certainty of evidence has not been systematically assessed.
Systematic reviews (SRs) and meta-analyses (MAs) evidence, which make up the top of the evidence pyramid, is typically thought to provide a trustworthy foundation for judgment in medicine.14 However, the availability of such evidence to provide decision guidance to users of the evidence needs to be further evaluated because of various possible sources of bias in the gathering of evidence.15 To summarize the data from the various SRs/MAs that have been published for overlapping themes in a short length of time, an overview is particularly required.16 An overview has several advantages over traditional SRs/MAs, including the ability to thoroughly assess the same evidence that is currently repeated and not systematically assessed, supplying evidence users with more targeted, high-quality evidence, and spotting significant flaws in the evidence formation process.17 Literature searches have yielded a greater percentage of SRs/MAs evaluating the efficacy on PSCI with acupuncture, but their quality is heterogeneous and no uniform conclusions have been formed. We therefore conducted this study to synthesize the available evidence.
Methods
The Cochrane Handbook18 was followed in conducting this study. On the PROSPERO, the protocol was prospectively registered (CRD42022301171). Ethical approval and consent statement were not required for this meta-analayses study.
Criteria for Inclusion and Exclusion
Following were the inclusion criteria: (a) randomized controlled trials (RCTs) were the only studies that the SRs/MAs included; (b) stroke survivors with PSCI; (c) the application of acupuncture or in combination with CFT as experimental intervention, while CFT as the control intervention; (c) effective rate, or Montreal Cognitive Assessment (MoCA) were applied as outcome measurements. SRs/MAs comparing different types of acupuncture, SRs/MAs comparing the effects of acupuncture with medication, and SRs/MAs for which data were not available were excluded.
Search Strategy
The keywords of acupuncture, stroke, and cognition disorder were applied to systematically search Web of Science, Cochrane Library, PubMed, Embase, SinoMed, Wanfang, CNKI, and Chongqing VIP on October 2022. The detailed search strategy applied to each database is presented as Additional File 1.
Eligibility Assessment and Data Extraction
Publications were read by two reviewers independently. A third party intervened to resolve any discrepancies. General study characteristics, subject characteristics, intervention characteristics, outcome measurements, and primary results were among the data that were extracted.
Review Quality Evaluation
The methodological quality was appraised with Methodological Quality of Systematic Reviews 2 (AMSTAR-2).19 We evaluated reporting quality with the list of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and evidence quality with Grade of Recommendation, Assessment, Development and Evaluation (GRADE) system.20 By bringing in a third reviewer for judgment, any disagreements were resolved. Additional File 2 offers comprehensive items for AMSTAR-2 and PRISMA.
Results
Eligible Studies
A total of 177 citations were identified. After removal of duplicates, 130 citations were screened by two reviewers independently. By further screening, 115 citations were excluded, and 15 articles21–34 were included finally. The procedure for locating the qualified articles is shown in Figure 1.
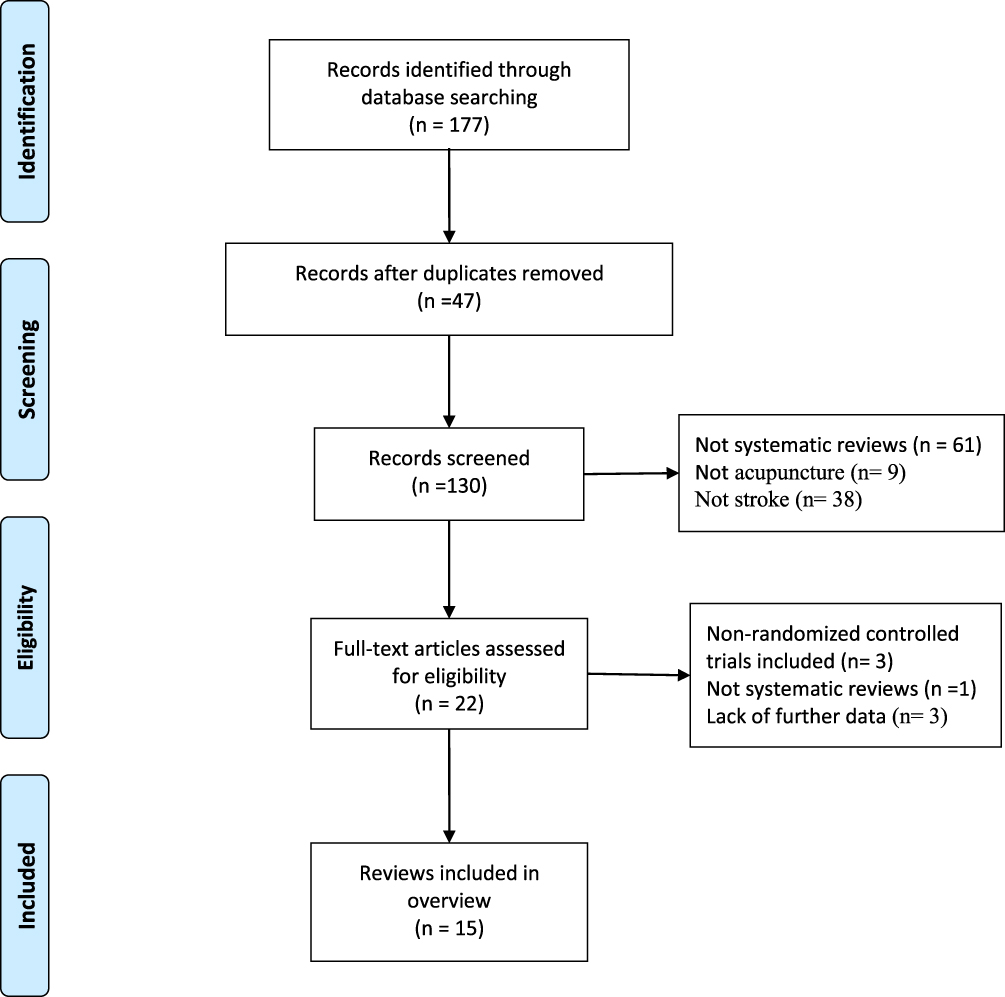 |
Figure 1 Literature selection procedure. |
Studies Characteristics
Fifteen studies that were conducted in China and published between 2010 and 2021 were included. The samples varied widely among the included studies (RCTs ranged from 8 to 37, subjects ranged from 504 to 2869). CFT alone served as the control intervention, while acupuncture was used as an experimental intervention. All studies conducted a meta-analysis. More details are outlined in Table 1.
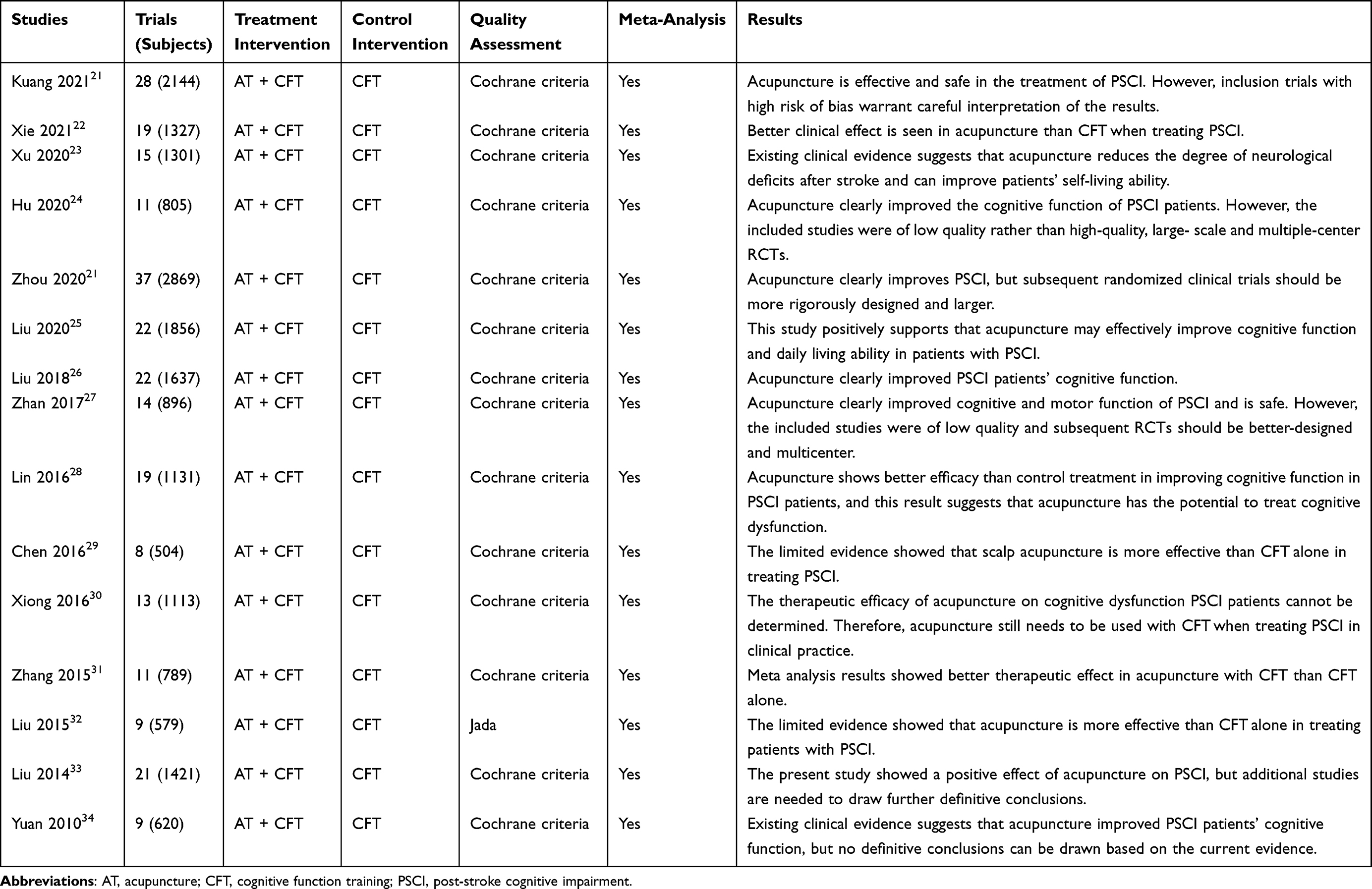 |
Table 1 Studies Characteristics |
Methodological Quality
Figures 2 and 3 show the results of methodological quality. The major methodological flaws were as follows: (a) item 2 (almost all studies did not state the protocol); item 7 (a list of excluded studies was missing in all reviews, which failed to justify exclusion). Thus, all reviews were rated low or very low in methodological quality.
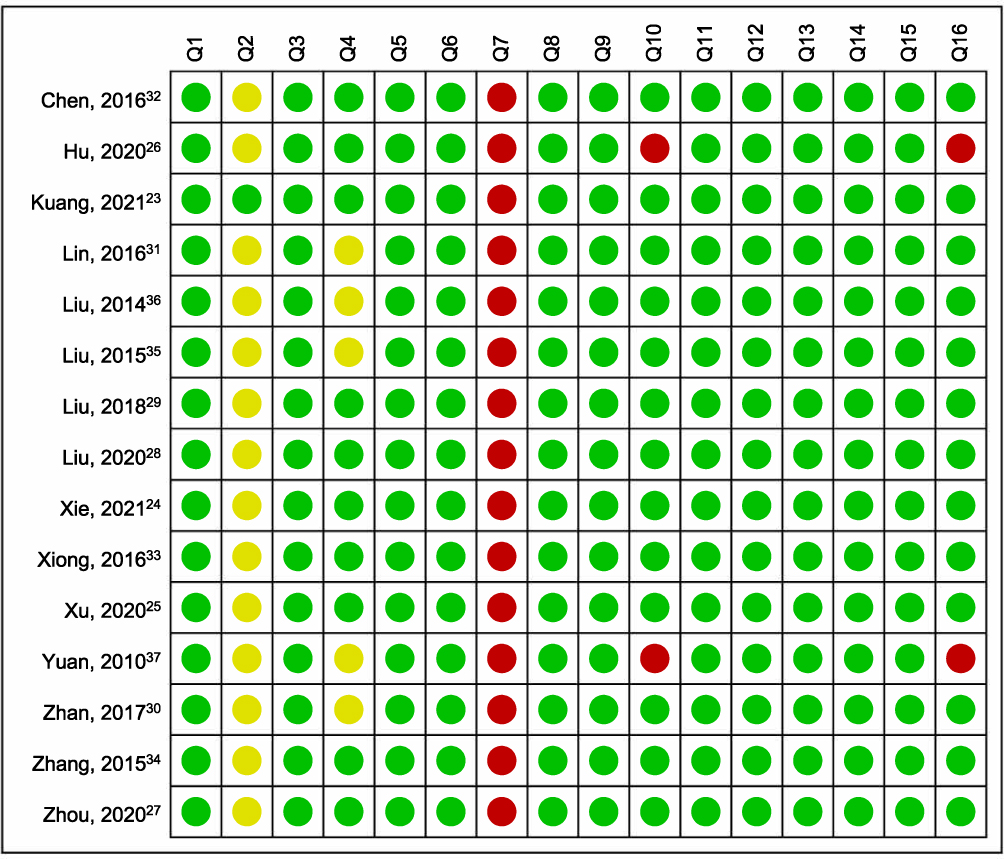 |
Figure 2 Methodological quality summary. Note: Red represents no; yellow represents partially yes; green represents yes. |
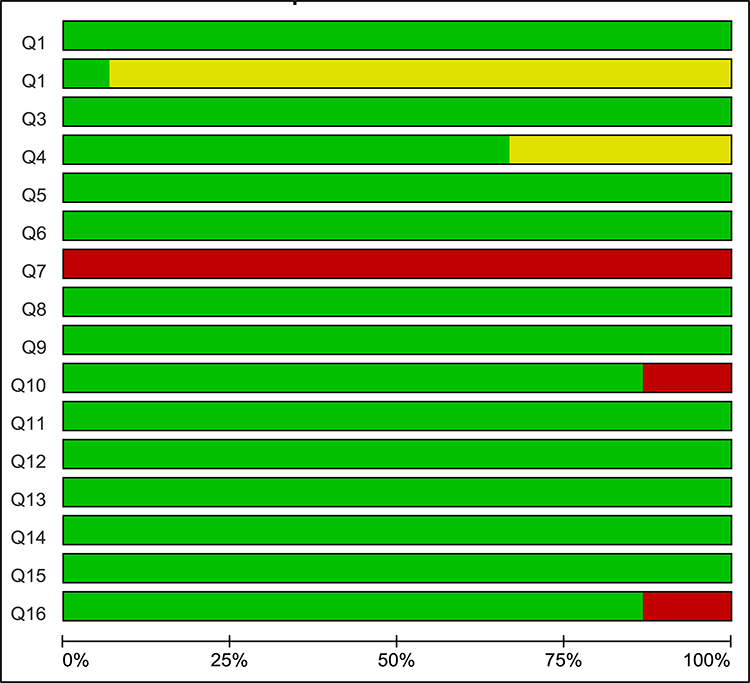 |
Figure 3 Methodological quality graph. Note: Red represents no; yellow represents partially yes; green represents yes. |
Reporting Quality
Sections of “Title”, “Abstract”, “Introduction”, “Discussion”, and “Funding” were all well-reported (100%) according to the PRISMA statement. However, some items had reporting deficiencies. In “Methods”, response rate of “yes” was less than 50% in Q5 (topic of protocol and registration) and Q8 (Search); in “Results”, response rate of “yes” was less than 50% in Q23 (Additional analysis). Details of the reporting quality are outlined in Table 2.
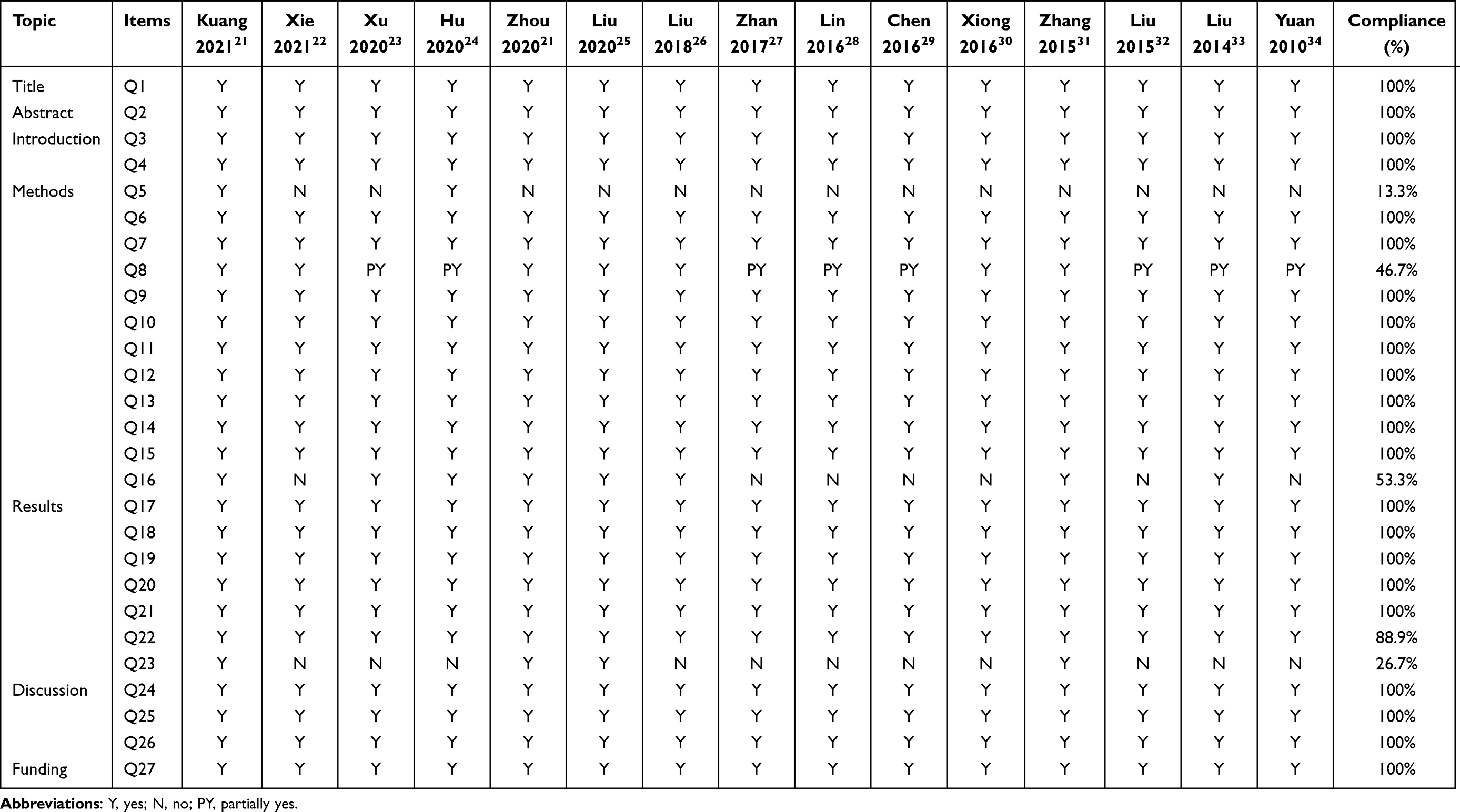 |
Table 2 Result of the PRISMA Assessments |
Evidence Quality
Using the GRADE system, 30 outcome measurements of interests were assessed. The evidence quality for these outcome measurements was very low for 8 (26.67%), low for 16 (53.33%), moderate for 6 (20%), and high for 0 (0%). Details of the evidence quality are outlined in Table 3.
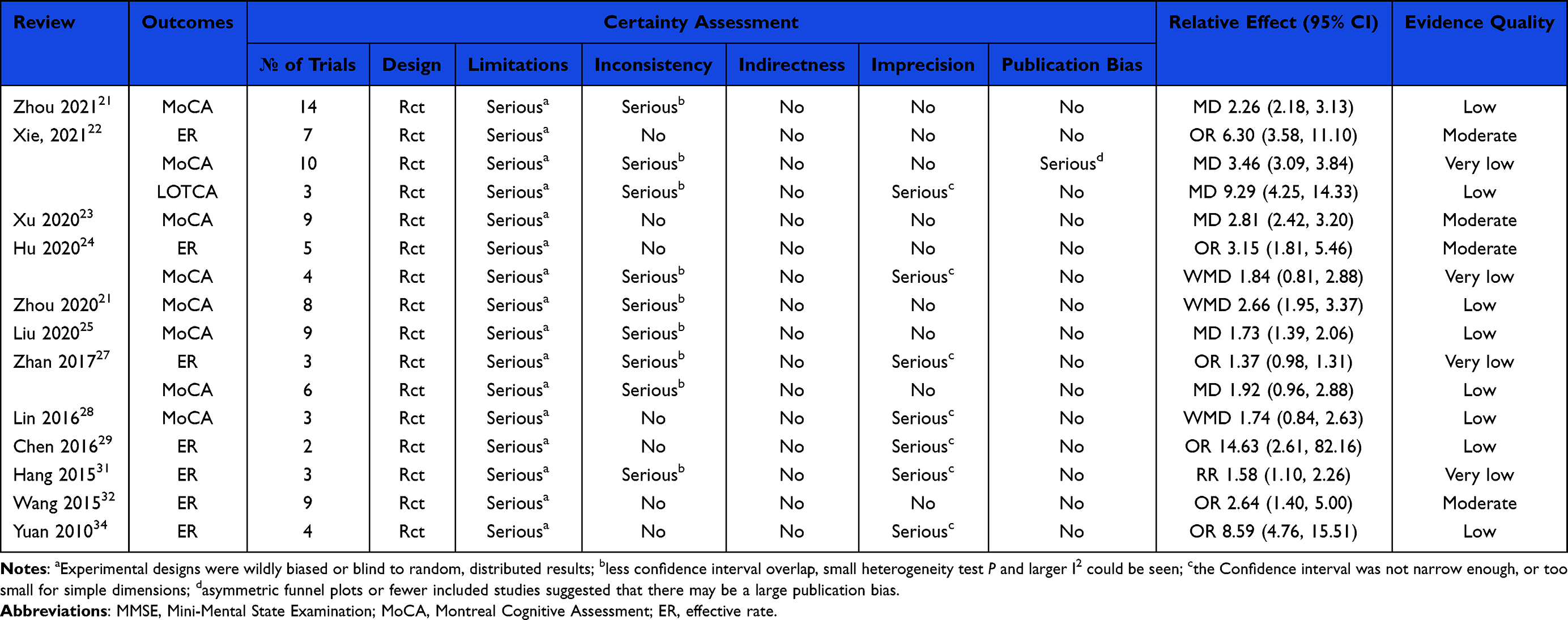 |
Table 3 Evidence Quality Results |
Efficacy Evaluation
The combined effects of acupuncture and CFT were significantly superior to CFT alone, according to the pooled results of eight SRs/MAs.21–25,27,28 The pooled results of six reviews22,24,28,31,32,34 revealed that CFT plus acupuncture was significantly superior to CFT alone. Nevertheless, the other review27 reported no significant difference in effective rate. More details of relative effects for all outcome measurements are outlined in Table 3.
Discussion
A poor-quality SR/MA may mislead decision-making.35 The assessment of recent evidence from SRs and MAs on numerous related topics forms the basis of an overview and verifies the validity of the evidence.36 Current evidence from SRs/MAs regarding acupuncture for PSCI is inconclusive. Hence, we performed this overview.
Summary of Main Findings
First, the evidence for using acupuncture to treat PSCI currently available has a great deal of room for improvement. In this study, we rigorously assessed methodological and evidence quality of the included SRs/MAs, and it was discovered that the current evidence deficiencies were frequent and challenging to satisfy the evidence users. With methodological quality, all SRs/MAs were found to have one or more critical items major flaws, and it was precisely because of such flaws that all SRs/MAs were deemed with low or worse methodological quality. Almost no studies showed that the review technique was developed before the SAs/MAs were conducted, hence they were unable to support any substantial programming changes. Additionally, all studies did not provide excluded trials list and therefore failed to justify the exclusion. For evidence quality, all outcome measurements were graded between moderate and very low quality. The most frequent cause of evidence degradation came from the risk of bias resulting from RCTs.
Second, based on the available evidence from SRs/MAs, there are no conclusive findings regarding the effects of acupuncture on PSCI. It was well-known that high-quality SRs contribute to providing valuable evidence and conversely might mislead clinical decisions.37–40 The findings of the methodology quality assessment and the quality of evidence assessment were unsatisfactory, suggesting that the findings of these studies might not be fully consistent with the actual application, and the reliability of the evidence has to be further examined. In addition, although all included studies suggested that acupuncture may have a positive effect on PSCI, most authors were reluctant to draw definitive conclusions because of the high risk of bias or small sample size of the trails. Therefore, acupuncture for PSCI rehabilitation should only be suggested with caution.
Practice and Research Implications
The findings of this overview revealed recurring fields for improvement that could help guide the conduct of future high-quality SRs/MAs. The rigor of an SR/MA must be ensured firstly, and any potential risk of bias must be avoided, by designing and registering study protocols in advance. Second, to ensure the study can be replicated, a thorough search strategy and list of excluded studies should be given. Third, when conducting data analysis, due consideration should be given to the scientific character of the analysis strategies. For example, performing subgroup analysis or sensitivity analysis may be considered when the heterogeneity of included studies is significant. In addition, any conflicts of interest and the source of funding must be adequately disclosed, as studies that are paid for by industry may produce findings that are more geared in their favor. In summary, the currently published SRs/MAs were identified with critical flaws, and for the purpose of providing high-quality evidence, future researchers should conduct SRs/MAs strictly follow with the criteria.
Limitations
Limitations should be acknowledged. Firstly, although the evaluation process establishes objective criterion tools, there may still be inevitable subjective factors in the assessment process. Furthermore, all of the studies that were included were carried out in China, though this finding is not unexpected given that acupuncture originated in China and has been most frequently used there. Acupuncture has been gaining international recognition in recent years, but patients are generally unfamiliar with this treatment, so it is still not universally used internationally.41 All of these factors pose challenges to the internationalization of acupuncture and therefore limit the development of international acupuncture research. Given that the included reviews were performed in China, which inevitably poses a potential risk of bias, it remains necessary to encourage further international studies of acupuncture for PSCI in other countries or regions outside of China.
Conclusion
Acupuncture may be beneficial for PSCI. Because of limitations and inconsistent conclusions, further research is needed to provide higher evidence for acupuncture on PSCI.
Disclosure
Qiongyang Zhou and Yue Ji are the co-first authors. The authors report no conflicts of interest in this work.
References
1. GBD 2016 Stroke Collaborators. Global, regional, and national burden of stroke, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):439–458. doi:10.1016/S1474-4422(19)30034-1
2. Sun JH, Tan L, Yu JT. Post-stroke cognitive impairment: epidemiology, mechanisms and management. Ann Transl Med. 2014;2(8):80. doi:10.3978/j.issn.2305-5839.2014.08.05
3. Jokinen H, Melkas S, Ylikoski R, et al. Post-stroke cognitive impairment is common even after successful clinical recovery. Eur J Neurol. 2015;22(9):1288–1294. doi:10.1111/ene.12743
4. Park JH, Kim BJ, Bae HJ, et al. Impact of post-stroke cognitive impairment with no dementia on health-related quality of life. J Stroke. 2013;15(1):49–56. doi:10.5853/jos.2013.15.1.49
5. Rajan KB, Aggarwal NT, Wilson RS, Everson-Rose SA, Evans DA. Association of cognitive functioning, incident stroke, and mortality in older adults. Stroke. 2014;45(9):2563–2567. doi:10.1161/STROKEAHA.114.005143
6. Mijajlović MD, Pavlović A, Brainin M, et al. Post-stroke dementia - a comprehensive review. BMC Med. 2017;15(1):11. doi:10.1186/s12916-017-0779-7
7. Huang J, Wu M, Liang S, et al. A critical overview of systematic reviews and meta-analyses on acupuncture for poststroke insomnia. Evid Based Complement Alternat Med. 2020;2020:2032575. doi:10.1155/2020/2032575
8. Liu BY, Chen B, Guo Y, et al. Acupuncture – a national heritage of China to the world: international clinical research advances from the past decade. Acupunct Herb Med. 2021;1(2):65–73. doi:10.1097/HM9.0000000000000017
9. Guo Y, Li YM, Xu TL, et al. An inspiration to the studies on mechanisms of acupuncture and moxibustion action derived from 2021 Nobel Prize in Physiology or Medicine. Acupunct Herb Med. 2022;2(1):1–8. doi:10.1097/HM9.0000000000000023
10. Chavez LM, Huang SS, MacDonald I, et al. Mechanisms of acupuncture therapy in ischemic stroke rehabilitation: a literature review of basic studies. Int J Mol Sci. 2017;18(11):2270. doi:10.3390/ijms18112270
11. Huang J, Qin X, Shen M, et al. An overview of systematic reviews and meta-analyses on acupuncture for post-stroke aphasia. Eur J Integr Med. 2020;37(37):101133. doi:10.1016/j.eujim.2020.101133
12. Huang J, Shi Y, Qin X, et al. Clinical effects and safety of electroacupuncture for the treatment of poststroke dysphagia: a comprehensive systematic review and meta-analysis. Evid Based Complement Alternat Med. 2020;2020:1560978. doi:10.1155/2020/1560978
13. Johansson K, Lindgren I, Widner H, et al. Can sensory stimulation improve the functional outcome in stroke patients? Neurology. 1993;43(11):2189–2192. doi:10.1212/wnl.43.11.2189
14. Siddaway AP, Wood AM, Hedges LV. How to do a systematic review: a best practice guide for conducting and reporting narrative reviews, meta-analyses, and meta-syntheses. Annu Rev Psychol. 2019;70:747–770. doi:10.1146/annurev-psych-010418-102803
15. Yao L, Sun R, Chen YL, et al. The quality of evidence in Chinese meta-analyses needs to be improved. J Clin Epidemiol. 2016;74:73–79. doi:10.1016/j.jclinepi.2016.01.003
16. Huang J, Qin X, Cai X, et al. Effectiveness of acupuncture in the treatment of Parkinson’s disease: an overview of systematic reviews. Front Neurol. 2020;11:917. doi:10.3389/fneur.2020.00917
17. Huang J, Shen M, Qin X, et al. Acupuncture for the treatment of Alzheimer’s disease: an overview of systematic reviews. Front Aging Neurosci. 2020;12:574023. doi:10.3389/fnagi.2020.574023
18. Cumpston M, Li T, Page MJ, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev. 2019;10:ED000142. doi:10.1002/14651858.ED000142
19. Shea BJ, Reeves BC, Wells G, et al. AMSTAR-2: a critical appraisal tool for systematic reviews that include randomized or non-randomized studies of healthcare interventions, or both. BMJ. 2017;358:1. doi:10.1136/bmj.j4008
20. Atkins D, Best D, Briss PA, et al. Grading quality of evidence and strength of recommendations. BMJ. 2004;328(7454):1490. doi:10.1136/bmj.328.7454.1490
21. Zhou L, Wang Y, Qiao J, et al. Acupuncture for improving cognitive impairment after stroke: a meta-analysis of randomized controlled trials. Front Psychol. 2020;11:549265. doi:10.3389/fpsyg.2020.549265
22. Xie DL, Yang K, Xie HH, et al. Meta-analysis of the effectiveness of scalp acupuncture for post stroke cognitive impairment. Guiding J Trad Chin Med Pharmacol. 2021;27(12):130–136. doi:10.13862/j.cnki.cn43-1446/r.2021.12.032
23. Xu ZM, Liao X, Jia M, et al. A systematic review on the efficacy and safety of acupuncture for cognitive impairment after stroke. Beijing J Trad Chin Med. 2020;39(11):1117–1122. doi:10.16025/j.1674-1307.2020.11.001
24. Hu ST, Pi M. Systematic review and meta-analysis of acupuncture at Baihui (GV20) and Shuigou (GV26) points for the treatment of cognitive impairment after stroke. Guangzhou Univ Trad Chin Med. 2020;37:2035–2042. doi:10.13359/j.cnki.gzxbtcm.2020.10.037
25. Liu W, Rao C, Du Y, et al. The effectiveness and safety of manual acupuncture therapy in patients with poststroke cognitive impairment: a meta-analysis. Neural Plast. 2020;2020:8890521. doi:10.1155/2020/8890521
26. Liu F, Yao LQ, Chen JH. Therapeutic efficacy of acupuncture at Baihui (GV 20) and Shenting (GV 24) for post-stroke cognitive impairment: a systematic review. Shanghai J Acupunct Moxibustion. 2018;37(01):104–111. doi:10.13460/j.issn.1005-0957.2018.01.0104
27. Zhan J, Wang XW, Cheng NF, et al. Electroacupuncture for post stroke cognitive impairment: a systematic review and meta-analyses. Chin Acupunct Moxibust. 2017;37(10):1119–1125. doi:10.13703/j.0255-2930.2017.10.025
28. Lin XL, Liu WL, Lin EZ. Systematic evaluation of acupuncture for cognitive dysfunction after stroke. Fujian J Trad Chin Med. 2016;47(03):35–36. doi:10.13260/j.cnki.jfjtcm.011152
29. Chen LZ, Li W, Wang JQ, et al. Meta-analysis of scalp acupuncture on cognitive disorder after stroke. Guiding J Trad Chin Med Pharmacol. 2016;22(22):84–87. doi:10.13862/j.cnki.cn43-1446/r.2016.22.030
30. Xiong J, Liao WJ, Liu Q, et al. A systematic review of scalp acupuncture for post-stroke cognitive dysfunction. Chin J Rehabil Med. 2016;31(03):333–339. doi:10.3969/j.issn.1001-1242.2016.03.017
31. Hang Y, Tang W, Song XG, et al. Systematical review and meta analysis of the efficacy of acupuncture and moxibustion plus cognitive rehabilitation training in treating post-stroke cognitive disorder. Shanghai J Acupunct Moxibustion. 2015;34(10):1013–1020. doi:10.13460/j.issn.1005-0957.2015.10.1013
32. Wang M, Pan W, Xu Y, et al. Microglia-mediated neuroinflammation: a potential target for the treatment of cardiovascular diseases. J Inflamm Res. 2022;15:3083–3094. doi:10.2147/JIR.S350109
33. Liu F, Li ZM, Jiang YJ, et al. A meta-analysis of acupuncture use in the treatment of cognitive impairment after stroke. J Altern Complement Med. 2014;20(7):535–544. doi:10.1089/acm.2013.0364
34. Yuan SS, Zhang SY. Meta-analysis of acupuncture for cognitive impairment after stroke. Chin J Ethnomed Ethnopharm. 2010;19(09):47–48.
35. Huang J, Qin X, Shen M, et al. The effects of tai chi exercise among adults with chronic heart failure: an overview of systematic review and meta-analysis. Front Cardiovasc Med. 2021;8:589267. doi:10.3389/fcvm.2021.589267
36. Huang J, Shen M, Qin X, et al. Acupuncture for the treatment of tension-type headache: an overview of systematic reviews. Evid Based Complement Alternat Med. 2020;2020:4262910. doi:10.1155/2020/4262910
37. Huang J, Lu M, Zheng Y, et al. Quality of evidence supporting the role of acupuncture for the treatment of irritable bowel syndrome. Pain Res Manag. 2021;2021:2752246. doi:10.1155/2021/2752246
38. Huang J, Zhang J, Wang Y, et al. Scientific evidence of Chinese herbal medicine (Gegen Qinlian Decoction) in the treatment of ulcerative colitis. Gastroenterol Res Pract. 2022;2022:7942845. doi:10.1155/2022/7942845
39. Huang J, Liu J, Liu Z, et al. Reliability of the evidence to guide decision-making in acupuncture for functional dyspepsia. Front Public Health. 2022;10:842096. doi:10.3389/fpubh.2022.842096
40. Huang J, Wang Y, Huang S, et al. A critical overview of systematic reviews of shenfu injection for heart failure. Cardiovasc Ther. 2021;2021:8816590. doi:10.1155/2021/8816590
41. Sun Y, Liu B, He L, et al. The current situation of acupuncture definition in international organizations and legislation of some countries. Zhongguo Zhen Jiu. 2017;37(12):1329–1332. doi:10.13703/j.0255-2930.2017.12.020
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Altered Functional Activity and Functional Connectivity of Seed Regions Based on ALFF Following Acupuncture Treatment in Patients with Stroke Sequelae with Unilateral Limb Numbness
Peng J, Su J, Song L, Lv Q, Gao Y, Chang J, Zhang H, Zou Y, Chen X
Neuropsychiatric Disease and Treatment 2023, 19:233-245
Published Date: 25 January 2023
Influence of Acupuncture and Other Clinical Factors on the Recovery of Limb Motor Function in Patients After Stroke: A Retrospective Study
Wu B, Ding Y, Peng M, Wang X, Li Y, Cheng X
Journal of Multidisciplinary Healthcare 2023, 16:463-474
Published Date: 21 February 2023
Prevalence and Associated Factors of Cognitive Impairment Among Stroke Survivors at Comprehensive Specialized Hospitals in Northwest Ethiopia: Multi-Centered Cross-Sectional Study
Cherkos K, Jember G, Mihret T, Fentanew M
Vascular Health and Risk Management 2023, 19:265-277
Published Date: 27 April 2023
Bibliometric Analysis: Research Trends and Performances of Stroke on Acupuncture
Yang F, Cui Y, Zhao Y, Jiao H
Journal of Pain Research 2024, 17:1837-1851
Published Date: 22 May 2024
Clinical Efficacy of Acupuncture Combined with Escitalopram Oxalate in the Treatment of Mild-to-Moderate Post-Stroke Depression
Liu Y, Zhang G, Li J, Lv Y, Qi R
Neuropsychiatric Disease and Treatment 2025, 21:917-925
Published Date: 17 April 2025