Back to Journals » Journal of Pain Research » Volume 16
Sciatic Nerve Block Combined with Flurbiprofen Inhibits Spinal Cord Inflammation and Improves Postoperative Pain in Rats with Plantar Incision
Authors Li M, Zhang K ![]() , Li T, Chen Y, Zang H, Hu Y, Yao W
, Li T, Chen Y, Zang H, Hu Y, Yao W
Received 31 January 2023
Accepted for publication 28 April 2023
Published 9 May 2023 Volume 2023:16 Pages 1533—1546
DOI https://doi.org/10.2147/JPR.S404226
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Qi Fang
Meihong Li,1 Kaiwen Zhang,1 Ting Li,2 Yuye Chen,1 Hu Zang,1 Yingjie Hu,1 Wenlong Yao1
1Hubei Key Laboratory of Geriatric Anesthesia and Perioperative Brain Health, and Wuhan Clinical Research Center for Geriatric Anesthesia, Department of Anesthesiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China; 2Department of Anesthesiology, Zhongshan Hospital, Fudan University, Shanghai, 200032, People’s Republic of China
Correspondence: Wenlong Yao, Hubei Key Laboratory of Geriatric Anesthesia and Perioperative Brain Health, and Wuhan Clinical Research Center for Geriatric Anesthesia, Department of Anesthesiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China, Tel +86 13720271159, Email [email protected]
Background and Purpose: Peripheral nerve block is often used to relieve postoperative pain. But the effect of nerve block on inflammatory response is not fully understood. Spinal cord is the primary center of pain processing. This study is to investigate the effect of single sciatic nerve block on the inflammatory response of the spinal cord in rats with plantar incision and the combined effect with flurbiprofen.
Methods: The plantar incision was used to establish a postoperative pain model. Single sciatic nerve block, intravenous flurbiprofen or the combination of both were used for intervention. The sensory and motor functions after nerve block and incision were evaluated. The changes of IL-1β, IL-6, TNF-α, microglia and astrocytes in the spinal cord were examined by qPCR and immunofluorescence respectively.
Results: Sciatic nerve block with 0.5% ropivacaine in rats induced sensory block for 2h and motor block for 1.5h. In the rats with plantar incision, the single sciatic nerve block did not alleviate postoperative pain or inhibit the activation of spinal microglia and astrocytes, but the levels of IL-1β and IL-6 in spinal cord were decreased when the nerve block wore off. The combined effect of a single sciatic nerve block and intravenous flurbiprofen not only decreased the levels of IL-1β, IL-6, and TNF-α, but also relieved the pain and alleviated the activation of microglia and astrocytes.
Conclusion: The single sciatic nerve block cannot improve postoperative pain or inhibit the activation of spinal cord glial cells, but can reduce the expression of spinal inflammatory factors. Nerve block combined with flurbiprofen can inhibit spinal cord inflammation and improve postoperative pain. This study provides a reference for rational clinical application of nerve block.
Keywords: sciatic nerve block, inflammatory response, spinal cord, flurbiprofen, plantar incision, postoperative pain
Introduction
More than 313 million surgeries are performed worldwide each year. 49.5% of them suffer from moderate pain after surgery,1 and 20% of them suffer from severe pain.2 If the postoperative pain is not managed properly, it will cause respiratory and circulatory complications, affect postoperative rehabilitation, delay discharge time and increase the risk of wound infection.3 Severe acute pain can even turn into chronic pain,4,5 which affects sleep, mood, daily activities, and reduces the patient’s quality of life.6,7 Therefore, prevention and management of postoperative pain are very important.
In the past 20 years, the development of ultrasound visualization technology has made the clinical application of nerve block more common.8–10 Compared with general anesthesia alone, nerve block can relieve postoperative pain, reduce postoperative opioid requirement, and promote early recovery of patients.11–13 However, some patients suffered from severe pain at 8–24h after the nerve block wore off. This phenomenon is defined as “rebound pain” or “breakthrough pain”. The incidence of rebound pain in orthopedic surgery is as high as 52%,14–19 and this phenomenon may even offset the overall benefit of nerve block to patients. Thus, the effect of preoperative single nerve block on postoperative pain was not definitely determined.
It is known that the development of acute and chronic pain is associated with neuroinflammation.20,21 However, the effect of nerve block on inflammatory response still remains controversial. Beloeil et al used bupivacaine to block the sciatic nerve of rats and found that it alleviated carrageenin-induced inflammation in the hindpaw,22 but other studies have shown that nerve block has a pro-inflammatory effect and can facilitate inflammation around the wound.23,24 Clinical studies have found that, compared with general anesthesia, general anesthesia combined with thoracic paravertebral nerve block can reduce the systemic inflammatory response and the level of inflammatory factors in thoracic surgical patients.25,26 Zhen et al indicated that nerve block significantly alleviated clinical inflammatory manifestations, such as the reduction of knee circumference and skin temperature, but inflammatory factors in tissues and plasma were not decreased.27 However, these studies mostly focused on the changes in local and systemic inflammatory cytokines. In addition, spinal cord is the primary center of pain processing, the effect of nerve block on the inflammatory response of the spinal cord in postoperative rats was not fully understood.
With the development of enhanced recovery after surgery (ERAS), multimodal analgesia has been widely advocated in perioperative pain management, which makes patients to obtain better analgesic effect and lower complications.28 Multimodal analgesia refers to combining different methods or drugs to control pain.29,30 At present, nerve block based analgesia program with low opioid analgesic regimens are recommended. Nonsteroidal anti-inflammatory drugs inhibit cyclooxygenase (COX), and can play a powerful analgesic action on the incision and inflammation tissue with high affinity, which can relieve various postoperative pain. Flurbiprofen is a commonly used auxiliary medication and it can inhibit both fatty acid amide hydrolase and COX, which may be a potential useful analgesic.31,32 Preoperative or intraoperative intravenous application of flurbiprofen can effectively inhibit proinflammatory cytokines, and reduce postoperative pain.33
In this study, we first established the rat model with sciatic nerve block and evaluated the sensory and motor block time; then to investigate the effects of the single sciatic nerve block on postoperative pain, and the expression of glial cells and cytokines in the spinal cord in rats with plantar incision; last, to investigate the combinational effects of the nerve block with intravenous flurbiprofen.
Methods
Animals
Male SD rats (250–300g) were purchased from Tongji Medical College, Huazhong University of Science and Technology. All SD rats were housed in an SPF barrier environment with a temperature of 22–25°C, relative humidity of 45–65%, a light–dark cycle of 12h, and free eating and drinking. The experiments were carried out according to the Guide for the Use of Laboratory Animals and the National Institutes of Health Guide for the Care and approved by the Laboratory Animal Management Committee of Tongji Medical College, Huazhong University of Science and Technology (TJH-202201037).
Grouping
Seven days before the operation, SD rats were adapted to the test environment, and the basal pain threshold and motor function of rats were measured one day before the operation.
In experiment 1, SD rats were divided into two groups: ropivacaine block group (RP group, n = 8) and saline block group (NS group, n = 8).
In experiment 2: SD rats were divided into 4 groups: ropivacaine block plus plantar incision pain group (RP+PI group, n = 32) and normal saline plus plantar incision pain group (NS+PI group, n = 32); intravenous flurbiprofen plus saline block plus plantar incision pain group (F+NS+PI group, n = 32) and intravenous flurbiprofen plus ropivacaine block plus plantar incision pain group (F+RP+PI group, n = 32).
Animals that failed nerve block or died from anesthesia were excluded.
Sciatic Nerve Block
The model of the left sciatic nerve block was performed as previously described.34,35 Briefly, after inhalational anesthesia with 2.5% isoflurane, the greater trochanter and the sciatic tuberosity of rats were touched, and a longitudinal incision was made along the posterolateral thigh of rats. The sciatic nerve was exposed after bluntly separating the biceps femoris muscle and semitendinosus muscle. 0.2mL of 0.5% ropivacaine or 0.9% normal saline was injected into the perineural fascia. After injection, the incision was sutured, and the surgical wound was sprayed with penicillin to prevent infection.
Plantar Incision
Under the effect of inhalation of 2.5% isoflurane anesthesia, after the sciatic nerve was blocked, the left plantar incision was performed as previously described.36,37 A longitudinal incision of about 1cm in length was made from 0.5cm proximal plantar to the toe through the skin and fascia of the left paw including the underlying muscle. The plantar muscle was lifted with eye forceps and incised longitudinally and then put it back to the original position with the muscles’ origin and insertion intact. After applying pressure to stop the bleeding, the incision was sutured. Erythromycin ointment was applied to the incision to prevent infection.
Flurbiprofen Administration
After sciatic nerve block and plantar incision, the rat tail was wiped with 75% alcohol and warm water for tail venipuncture. Normal saline or flurbiprofen (3E02IT, Beijing Teide Pharmaceutical Co., LTD.) was administered I.V. with 10mg/kg.
Behavioral Test
Assessment of Sensory Function
- Paw mechanical withdrawal threshold (PMWT): As described previously,38,39 a set of von Frey filaments (Stoelting, Wood Dale, IL, USA) were used to evaluate PMWT by stimulating the middle area of the left hindpaw close to the incision. The rats were put in the plastic box to adapt for 30min, then different von Frey filaments ranging from 2 to 15g were used to stimulate the plantar vertically for at least 3 seconds. Positive reactions were considered if the rats suddenly shrank, shook or licked their paws, and positive reactions were detected by lower von Frey filaments. PMWT was the minimum force required to cause at least three positive reactions in five tests.
- Paw withdrawal Latency (PWL): A thermal pain stimulator (equipment model 37,370, Italy) was used to measure the nociceptive thermal stimulation. The rats were placed in a plastic box for 10–15min before the test, and the infrared light source was moved to the middle area near the incision of the left hindpaw of the rats When the rats lifted the paw due to pain, the device automatically detected and stopped timing, and the time of paw contraction was displayed on the monitor with an accuracy of 0.1s. To avoid tissue damage, 30s was taken as the cut value, and the infrared intensity was adjusted so that the basic PWL of SD rats was 15–20s.40,41
- Cumulative pain score (CPS): the weight bearing of left hindpaw was observed. The rats were placed in a transparent plastic box with a grid pad made of metal wire at the bottom. Before the test, the rats were placed in a transparent plastic box for 20 minutes, and the observation was performed once every 5 minutes, each lasting 1 minute. The sum of 12 scores (range: 0–24) was obtained during the 1h testing period. The CPS was then obtained by subtracting the score for the injured paw from that for the non-injured paw. Scoring method: the hindpaw completely touches the wire, the hindpaw lands on the ground, and the weight gauge scores 0; the wound has deformation when touching the net, landing on the ground but not bearing meter 1 point; the sole does not touch the iron net completely, and the hindpaw does not raise the ground to count 2 points.41,42
Assessment of Motor Function
According to observing the toes’ movement reflex (peroneal nerve motor fibers) to assess the motor function of rats, this is a kind of vestibular reflex, by lifting the rats to observe whether the reaction of the stretching and contraction, to record the rat movement recovery, and motor function was evaluated every 10 minutes until the block effect wore off. Scoring method: no paw extension reflex and grasp count as 2 points; weak paw extension reflex recovery and grasp count as 1 point; total paw reflex and strong grasp count as 0 points.24,43
Immunofluorescent Staining
Rats were sacrificed under deep anesthesia before the operation and at 6h, 24h, 3d, 7d after nerve block. Four samples were taken from each group at each time point. The spinal cord tissue was removed rapidly and fixed in 4% paraformaldehyde at 4°C for 2d. Then the harvested spinal cord was dehydrated in a gradient and sectioned to 20μm thickness in a cryostat (CM, Leica, Germany). The sections were blocked with 5% donkey serum or goat serum for 1 hour at room temperature. The microglial marker Iba1 (AB5076, 1:200, Abcam) and the astrocyte marker GFAP (#3670, 1:200, Cell Signaling Technology) were incubated overnight. Then, donkey anti-goat secondary antibody labeled with Alexa Fluor 488-immune research (Jackson ImmunoResearch, 1:100, West Grove, PA, USA) and Alexa Fluor 488-labeled goat anti-mouse secondary antibody (Jackson ImmunoResearch, 1:200, West Grove, PA, USA) were incubated for 2 hours at room temperature. U-HGLGPS immunofluorescence microscope (Olympus, Japan) was used to obtain images and analyze the changes in the number of microglia. The expression number of microglia per unit area could be calculated by using the average value per 50μm×50μm.
qPCR
Rats were sacrificed under deep anesthesia. The spinal cord tissue was removed rapidly. Total RNA was extracted with Trizol (No.108–95-2, Takara), and 1μg RNA was reversely transcribed into cDNA. Quantitative RT-PCR was performed using PCR system (ABI 7900/Viia, Foster City, CA, USA). SYBR Green was used to detect the amplification of β-actin, IL-1β, IL-6, and TNF-α. The primer sequences are shown in Table 1. The reaction conditions were 95°C for 2min (initial denaturation), followed by 45 cycles each consisting of 95°C for 10s (denaturation) and 60°C for 30s (annealing extension). β-actin was used as the internal parameter to correct the expression of the target genes. The relative level of IL-1β, IL-6, and TNF-α mRNA was calculated using the comparative cycle threshold (CT) method (2−ΔΔCT).
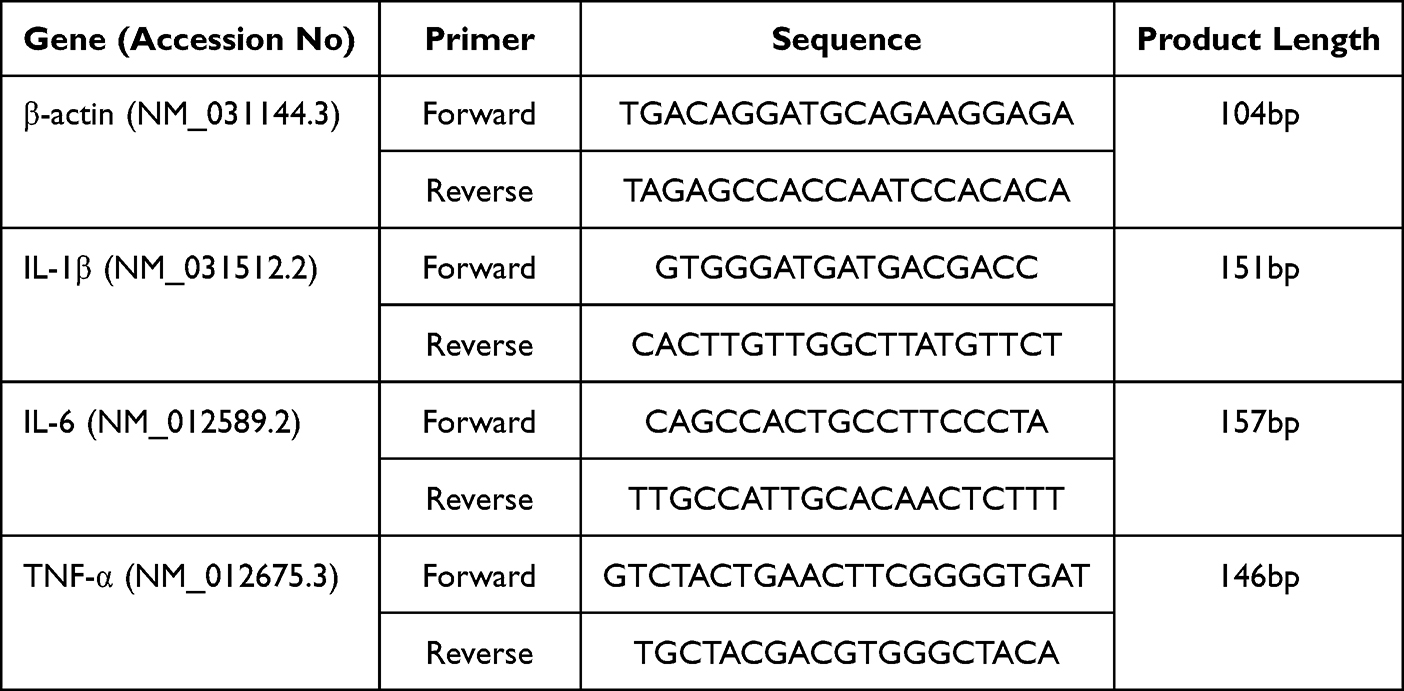 |
Table 1 The Primer Sequences |
Statistical Analysis
Graphpad8.0 software was used for statistical analysis. The motor block results were expressed as mean ± standard error of the mean (X±SEM); Other results were expressed as mean ± standard deviation (X±SD). One-way ANOVA followed by Dunnett’s test was used to analyze the data of PWL, PWMT, CPS, motor block, qPCR, and immunofluorescence within groups. Two-way ANOVA followed by Bonferroni’s test was used to analyze the data among groups. P < 0.05 was considered statistically significant.
Results
Sensory and Motor Effect of Sciatic Nerve Block with 0.5% Ropivacaine
At 0.5h, 1h, 1.5h, 2h, 2.5h, 3h, 4h, and 6h after nerve block, the PWL and motor block scores were detected to evaluate the sensory and motor effect of sciatic nerve block with 0.5% ropivacaine (Figure 1A). Compared with the NS group, the PWL of the hindpaw in the RP group increased from 0.5h after nerve block and lasted for 2h (Figure 1B; P < 0.05), and PWL decreased temporarily at 4h after the operation (P < 0.05). At 0.5h after sciatic nerve block, the paw extension reflex of SD rats disappeared and dragged the floor and the duration of motor block was about 1.5h (Figure 1C; P < 0.05). These results indicated that ropivacaine blocked the rat sciatic nerve successfully.
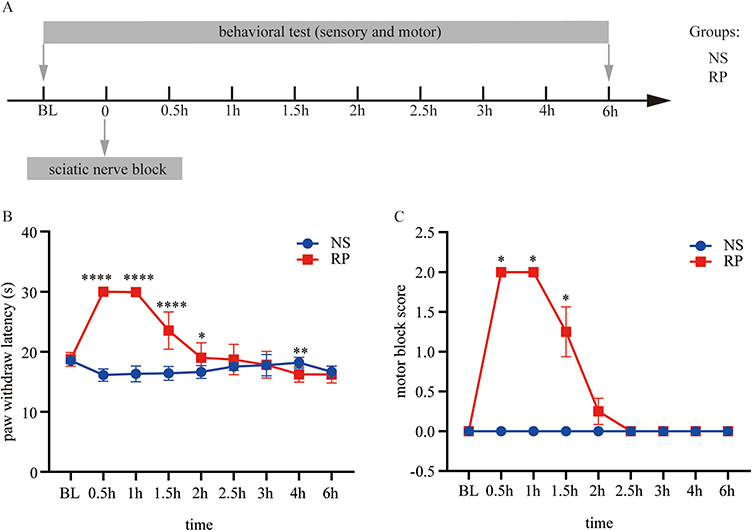 |
Figure 1 Effect of sciatic nerve block with 0.5% ropivacaine. (A) Experimental 1 designs and animal groups. (B) Paw withdrawal latency was assessed for 6h after sciatic nerve block. (C) Motor block scores were assessed by paw extension reflex for 6h after sciatic nerve block. The results of PWL are presented as the mean ± SD and the motor block scores are presented as the mean ± SEM (n = 8). Two-way ANOVA and Bonferroni’s test were used to analyze the inter-group differences. (Compared with NS group, ****P < 0.0001, **P < 0.005, *P < 0.05). Abbreviations: BL, baseline; NS, normal saline; RP, Ropivacaine. |
Effect of Sciatic Nerve Block Combined with Flurbiprofen on Postoperative Pain and Spinal Cord Inflammation in Rats
Pain Behavior
At 0.5h, 2h, 6h, 1d, 2d, 3d, 5d, and 7d after nerve block, PWL, PMWT, and CPS were used to evaluate the analgesic effect of sciatic nerve block, flurbiprofen and their combination (Figure 2A). In NS+PI group, PWL began to decrease at 0.5h (P < 0.05) and returned to baseline at 7d after operation. Compared with the NS+PI group, the PWL in RP+PI group neither increased nor decreased after 2h (P > 0.05). The PWL of the F+NS+PI group returned to baseline at 5d. Compared with RP+PI group, although analgesia of flurbiprofen was not as effective as sciatic nerve block in the first 2h, it was superior to sciatic nerve block after 2h (P < 0.05). Compared with the RP+PI and F+NS+PI groups, PWL was further prolonged in the F+RP+PI group (Figure 2B).
 |
Figure 2 Effect of sciatic nerve block combined with flurbiprofen on postoperative pain in rats with plantar incision. (A) Experimental 2 designs and animal groups. (B) Paw withdrawal latency was assessed for 7d after sciatic nerve block or flurbiprofen injection in rats with incision. (C) Mechanical allodynia evaluated by the paw withdrawal threshold for 7d after sciatic nerve block or flurbiprofen injection in rats with incision. (D) Cumulative pain score was for 7d after sciatic nerve block or flurbiprofen injection in rats with incision. The results are presented as the mean ± SD (n = 8). Two-way ANOVA and Bonferroni’s test were used to analyze the inter-group differences. (Compared with NS+PI group, RP+PI group *P >0.05; Compared with F+NS+PI group, F+RP+PI group #P >0.05; Compared with RP+PI group, F+RP+PI group &P >0.05, F+NS+PI group ΔP >0.05). Abbreviations: BL, baseline; NS, normal saline; RP, Ropivacaine; F, Flurbiprofen; PI, plantar incision pain model. |
The trend of PWMT in the NS+PI group was consistent with that of PWL. The PWMT in RP+PI group returned to baseline at 5d, while the PWMT in F+NS+PI and F+RP+PI groups returned to baseline at 3d, which was earlier than that in NS+PI group. The inter-group comparison of PWMT was consistent with that of PWL (Figure 2C).
In NS+PI group, CPS began to increase at 0.5h (P < 0.05), and returned to baseline at 7d after operation. CPS in RP+PI group began to increase at 2h and returned to baseline at 7d as in NS+PI group. CPS in F+NS+PI group also began to increase at 0.5h but returned to the baseline at 5d. However, CPS in F+NS+PI group was significantly decreased compared with NS+PI group (P < 0.05) and the combination of sciatic nerve block and flurbiprofen could further decrease CPS (Figure 2D). The above results indicated that the sciatic nerve block was less effective than intravenous flurbiprofen, but the combination of the two provided the best analgesia.
Changes in Spinal Glial Cells
Compared with baseline, microglia were mainly activated in the dorsal horn and medial side of the ipsilateral spinal cord at 1d after the operation in NS+PI and RP+PI groups (Figure 3A), which was earlier than those in F+NS+PI and F+RP+PI groups. Microglia were activated in all four groups at 3d after the operation, but the number of activated microglia in NS+PI and RP+PI groups was more than that in F+NS+PI and F+RP+PI groups (Figure 3B; P < 0.05).
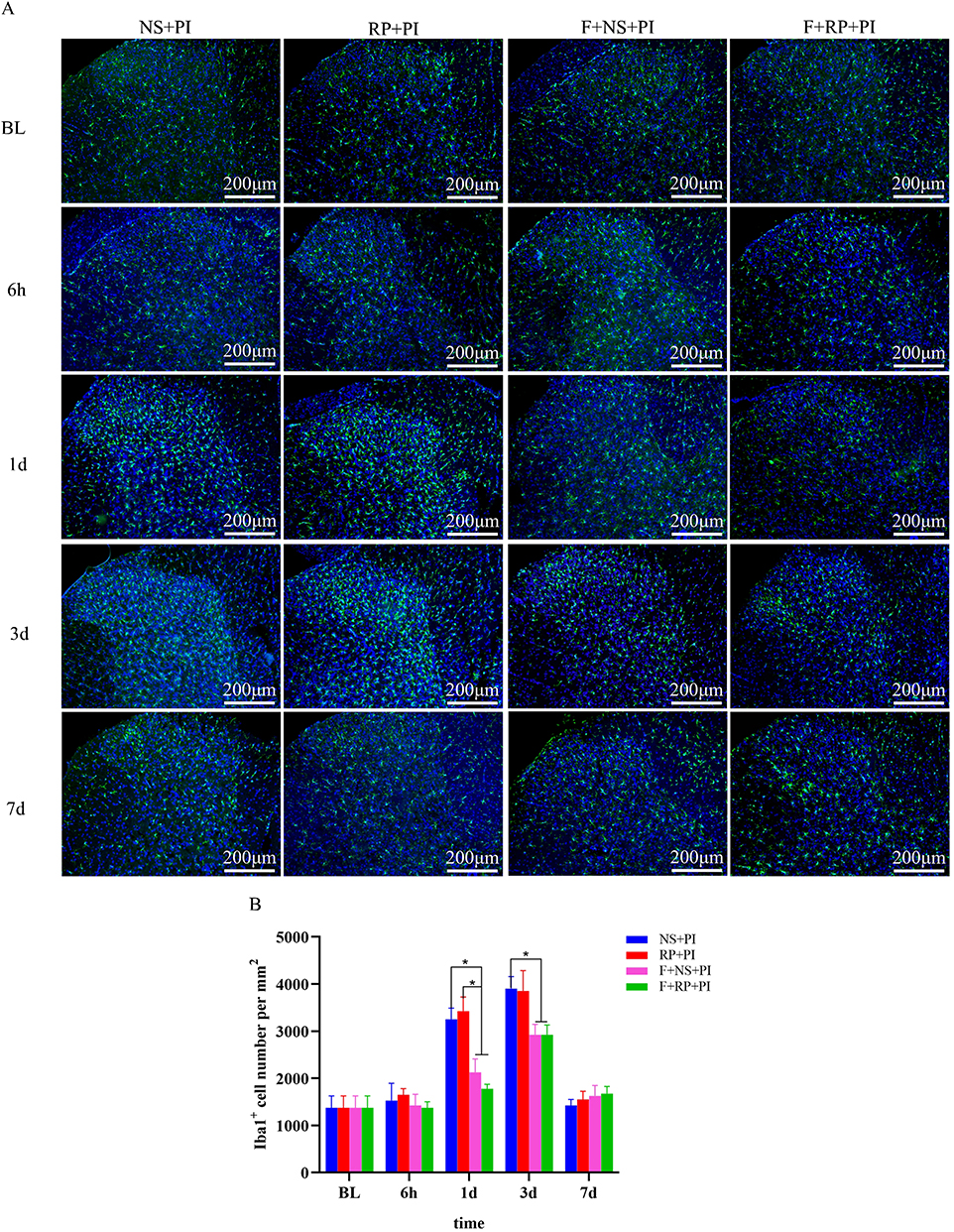 |
Figure 3 Activation of microglia in the spinal dorsal horn of rats with plantar incision. (A) Representative images of one rat from each group. (B) Quantification of the number of Iba1+ cells per square millimeter in the spinal cord horn (scale bar=200μm; Blue represents cell nucleus and green represents microglia). The results are presented as the mean ± SD (n = 4). Two-way ANOVA and Bonferroni’s test were used to analyze the inter-group differences; *P < 0.05. Abbreviations: BL, baseline; NS, normal saline; RP, Ropivacaine; F, Flurbiprofen; PI, plantar incision pain model. |
Astrocytes in NS+PI and RP+PI groups were activated at 1d after the operation and astrocytes were mainly activated in the ipsilateral spinal dorsal horn (Figure 4A), while those in the F+NS+PI group were activated at 3d, which all lasted to 7d after the operation (Figure 4B; P < 0.05). Astrocytes in the F+RP+PI group were not activated at all time points.
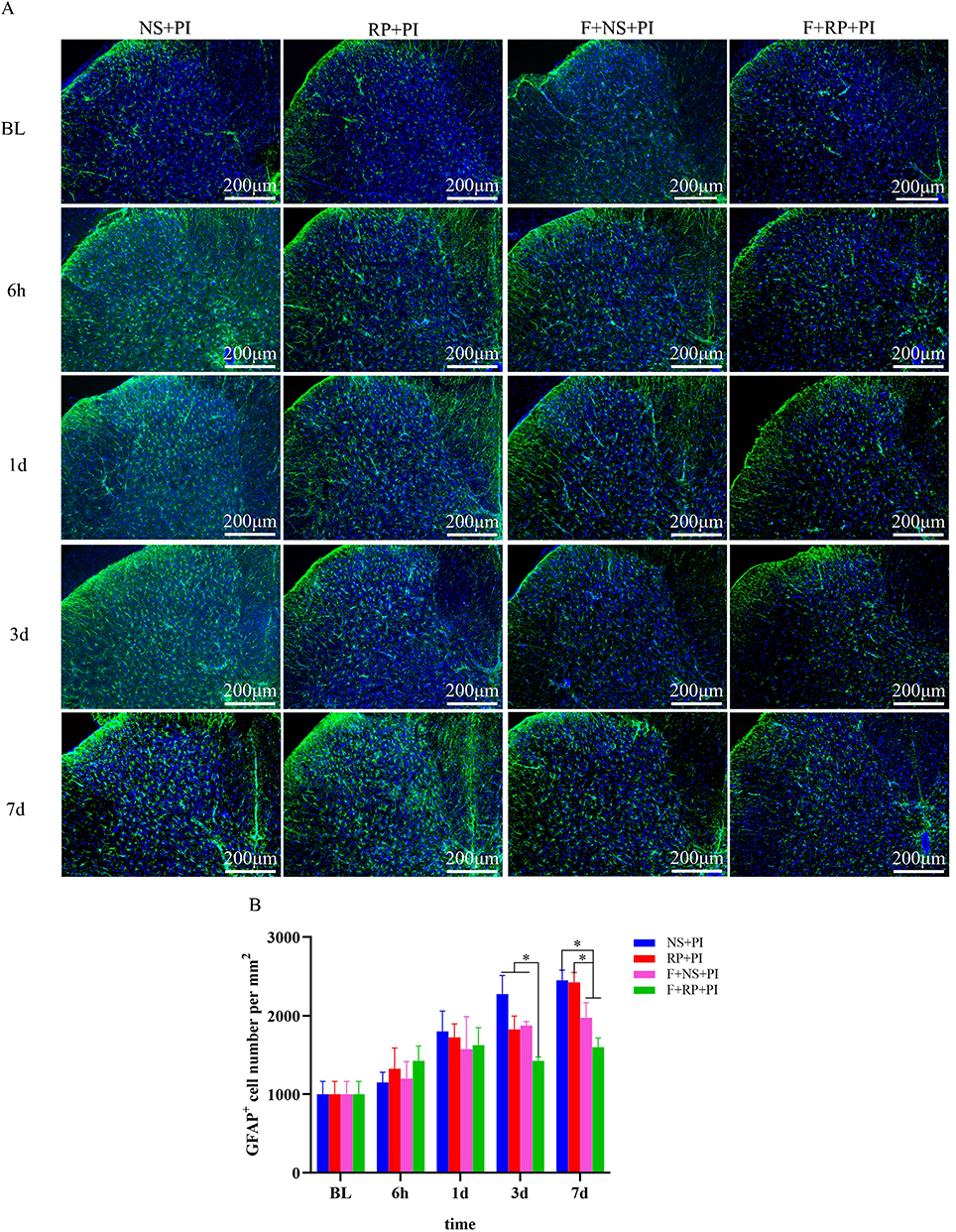 |
Figure 4 Activation of astrocytes in the dorsal horn of spinal cord in rats with plantar incision. (A) Representative images of one rat from each group. (B) Quantification of the number of GFAP+ cells per square millimeter in the spinal cord horn (scale bar=200μm; Blue represents cell nucleus and green represents astrocytes). The results are presented as the mean ± SD (n = 4). Two-way ANOVA and Bonferroni’s test were used to analyze the inter-group differences;*P < 0.05. Abbreviations: BL, baseline; NS, normal saline; RP, Ropivacaine; F, Flurbiprofen; PI, plantar incision pain model. |
Changes of Proinflammatory Factors in the Spinal Cord
Compared with the baseline, the level of IL-1β increased at 6h in NS+PI, RP+PI and F+NS+PI groups, while at 1d in F+RP+PI group (P < 0.05), and returned to the baseline at 7d in all groups (Figure 5A). The level of IL-1β in NS+PI group was significantly higher than that in the other three groups (P < 0.05). IL-6 increased only in the NS+PI group (P < 0.05), but not in the other groups (Figure 5B). The expression of TNF-α in the NS+PI, RP+PI and F+NS+PI groups also increased at 6h (P < 0.05). TNF-α lasted until 24h in F+NS+PI group and 3d in the other two groups, while there was no change in the F+RP+PI group (Figure 5C). This indicates that sciatic nerve block or flurbiprofen can inhibit the expression of inflammatory factors, and the combined effect is better.
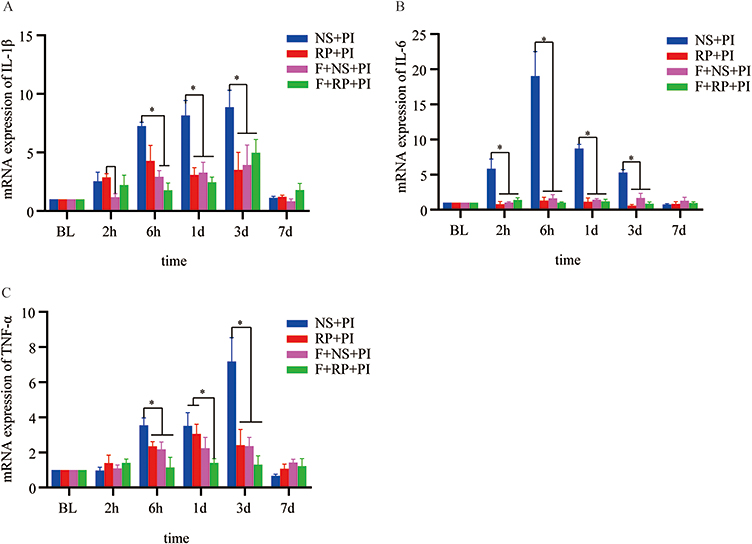 |
Figure 5 Changes of proinflammatory factors in the spinal dorsal horn of rats with plantar incision. (A–C) The expressions of IL-1β, IL-6 and TNF-α in the spinal dorsal horn. The results are presented as the mean ± SD (n = 4). Two-way ANOVA and Bonferroni’s test were used to analyze the inter-group differences (comparison between two groups,*P<0.05). |
Discussion
In this study, we found that: (1) The single sciatic nerve block with 0.5% ropivacaine in rats induced about 2 hours of sensory block and 1.5 hours of motor block. (2) In rats with plantar incision, PWL and PMWT decreased and CPS increased at 0.5h and returned to baseline at 7d. Spinal inflammatory factors IL-1β, IL-6 and TNF-α increased significantly at 6h, and spinal microglia and astrocytes were activated at 24h. (3) Compared with the NS+PI group, the sciatic nerve block with 0.5% ropivacaine neither improved postoperative pain after 2h of operation when the block wore off, nor decrease the number of microglia and astrocytes in the spinal cord, but it decreased the expression of inflammatory factors. (4) Flurbiprofen could relieve the plantar incision pain. Although the analgesic effect was not as good as that of a single sciatic nerve block for the first 2h, the analgesic effect was better than that of a single sciatic nerve block after 2h, and it could relieve spinal cord inflammation. (5) The analgesic effect of a single sciatic nerve block combined with flurbiprofen was superior to that of the two alone, and could directly inhibit the activation of astrocytes.
Generally, the methods of sciatic nerve block in rats include direct nerve exposure,34,35,44–46 anatomical localization,47 or guided by nerve stimulator.48,49 Anatomically located sciatic nerve block have the risk of incomplete block due to anatomic variation and low dose used. At present, the most commonly used method is direct nerve exposure. Although there is some trauma, direct exposure of the sciatic nerve is more accurate, and no significant changes in PWL, PWMT, and CPS of the ipsilateral paw occurred after the nerve block wears off.35 After sciatic nerve block with 0.5% ropivacaine in rats, the PWL was prolonged, the left hindpaw was dragged to the ground, and the paw extension reflex was absent. The sensory block time was about 2h, and the motor block time was about 1.5h, which is consistent with previous studies.45
The animal models of acute pain include the injection of chemical inflammatory substances such as complete Freudenberg’s adjuvant, carrageenan, and plantar incision.41,50–52 The pain caused by chemical inflammatory substances reached the peak at 6h and returned to normal at 3d. In the model of plantar incision, the pain threshold decreased at 1h after the operation, reached the peak at 24h, and returned to baseline at 7d, which was consistent with the trend of postoperative pain in clinical patients.53,54 Therefore, the plantar incision model was used to simulate the patients’ pain after surgery. The study found that the PWL and PWMT decreased significantly, and CPS increased at 0.5h in the NS+PI group, which returned to the baseline at 7d.
The spinal cord is the primary center of pain processing. Neuroinflammation is mediated by the activation of microglia and astrocytes, which plays an important role in the generation and maintenance of pain.55,56 Previous studies have shown that the activation of spinal microglia and astrocytes and the release of inflammatory factors could be induced at 24h after plantar incision.57,58 Studies have found that the up-regulation of p38 at 1h after plantar incision resulted in the release of brain-derived neurotrophic factor (BDNF) and pro-inflammatory cytokines IL-1β, IL-6, and TNF-α, while the number of microglia was increased at 3d after operation.59,60 Other studies have also found that the release of inflammatory factors from microglia was not consistent with its morphological changes.61 Consistently, in our study, microglia and astrocytes were activated significantly at 24h after plantar incision. Microglia were mainly activated in the dorsal horn and medial side of the ipsilateral spinal cord, and astrocytes were mainly activated in the ipsilateral spinal dorsal horn. The levels of TNF-α, IL-1β, and IL-6 in the spinal cord significantly increased at 6h.
Our study found the single sciatic nerve block with 0.5% ropivacaine did not improve the postoperative pain after 2h of operation in rats with plantar incision, compared with the NS+PI group. It was consistent with the study of Yamada et al,24 which may be due to the short block time. In addition, studies have shown that the sciatic nerve mainly innervated the lateral side of the paw, and the saphenous nerve mainly innervated the medial side of the paw.62 In our study, the incision was made in the middle of the plantar area. It was possible that an incomplete nerve block led to nociceptive stimulus afferent to the spinal cord.
Rebound pain was manifested as sudden onset of severe pain within 8–24 hours after the nerve block, with numerical rating scale (NRS) ≥7. The pain lasted for 3 to 6 hours, and the nature of the pain was mostly burning, electric shock, needle-like or numbness. It could occur in a resting or moving state, and most occurred in orthopedic surgery.14–16,63 Although rebound pain occurred in some patients after the nerve block wore off, it was not observed in this study. The possible reason was that the trauma caused by the plantar incision was not enough to induce rebound pain.
In Ding et al study, sciatic nerve block was performed before the plantar incision in neonatal mice, and then 3 times of sciatic nerve block was administered every 2 hours after the incision. They found multiple sciatic nerve block reduced the activation of microglia in the spinal dorsal horn and down-regulated BDNF and its downstream receptors, thereby alleviated neonatal incision-induced exaggravation of incision pain in adulthood.64 This study found that although sciatic nerve block could reduce the levels of inflammatory factors in the spinal cord, it could not inhibit the activation of microglia and astrocytes, which may be due to the short duration of nerve block. In addition, Kroin et al also did not inhibit spinal cord inflammation in rats with plantar incision,65 indicating that spinal cord inflammation was not entirely mediated by afferent nerve activity. Studies have found that the mRNA expression of IL-1β, IL-6 and TNFα in local plantar tissues was significantly increased after the plantar incision.66 Peripheral inflammatory factors could cause the increase of inflammatory factors in the blood, some of which could spread to the spinal cord through the blood-brain barrier, and then caused the activation of glial cells, thus leading to spinal cord inflammation.67
COX-2/PG pathway is involved in the transmission of noxious stimuli at the spinal cord and plays an important role in central hyperalgesia.65,68 Studies have found that the expression of COX-2 in the spinal cord was increased rapidly in rats with plantar incision,65 and non-steroidal anti-inflammatory drugs could relieve hyperalgesia.69 Flurbiprofen is widely used for postoperative analgesia. It is composed of lipid microspheres as a targeted drug delivery carrier, which can selectively accumulate in the surgical wound site.33,70 Some animal studies have found that the administration of flurbiprofen could reduce the plantar inflammatory factors IL-6 and TNF-α in LPS-induced inflammatory pain models.71
It has been found that arachidonic acid, the substrate of COX1/2, can be released by the hydrolysis of endocannabinoids by fatty acid amide hydrolase and monoacylglycerol lipase.72 CB1 receptor is the major receptors of the endocannabinoid system,73,74 and may be a novel target to alleviate inflammation, peripheral neuropathy, and pain.75,76 Flurbiprofen can lead to increased levels of 2-AG and AEA by inhibiting COX-2-mediated oxidation of endocannabinoids,31,32 which are known to alleviate hyperalgesia.77 In addition, flurbiprofen can contribute to the activation of CB1 and CB2 receptors.71 We found that flurbiprofen alone could increase PWL and PWMT and decrease CPS, and the mechanical and thermal pain thresholds returned to baseline at 3d and 5d after operation, respectively, which could also inhibit the activation of microglia and reduce the levels of IL-1β, IL-6 and TNF-α. This indicates that flurbiprofen axetil has a powerful analgesic effect.
Multimodal analgesia is the combination of different analgesic regimens or techniques to achieve an effective analgesic effect and reduce the consumption of opioids and their related adverse reactions.29,78 Nerve block based analgesic program with few opioids is recommended in clinical practice. Our study also found that the combined application of nerve block and flurbiprofen not only increased PWL and PWMT and decreased CPS, but also relieved spinal cord inflammation in rats with plantar incision, and the effect was better than that of the two alone. It indicated nerve block and non-steroidal drugs had a synergistic effect. They were better than single analgesia.
In clinical practice, some studies have found that compared with general anesthesia, brachial plexus block has no significant difference in perioperative pain control and analgesic drug consumption in patients with internal fixation of distal radius fractures, and the proportion of patients who seek medical treatment again due to pain after discharge is significantly higher. Therefore, researchers suggest that patients take analgesics actively before the end of regional anesthesia to control pain.16,79 The effect of nerve block on postoperative pain relief is limited, and the role of nerve block should be viewed rationally. In addition, some studies have found that compared with the use of nerve block alone, the combined use of nerve block and non-steroidal anti-inflammatory drugs can reduce postoperative complications, reduce VAS scores, and improve patient satisfaction.80 Therefore, the effect of multimodal analgesia is better and more worthy of promotion. Consistent with the above clinical phenomena, this study found that the combined application of flurbiprofen and sciatic nerve block was superior to the single method, which provided a theoretical basis for the implementation of the concept of multimodal analgesia.
This study has the following limitations. First, this study did not detect the changes of inflammatory factors in the incision site and serum. Numerous studies have found that various noxious stimuli could cause the activation of spinal microglia, which in turn caused the release of many inflammatory factors and induced hyperalgesia. This study found that the earliest activation time of microglia and astrocytes was 24 hours, and the inflammatory factors were significantly increased at 6 hours, so the source of inflammatory factors needs to be further studied. Second, we did not observe the effects of adjuvant or continuous nerve block on postoperative pain. Continuous peripheral nerve block has risks of catheter obstruction, displacement, and accidental prolapse. It is difficult to control the position of the catheter in animal studies. Future studies can use adjuvant or multiple nerve blocks to explore the effect of long-term nerve block on postoperative pain.
Conclusion
In summary, to simulate a clinical scenario, the effect of preoperative sciatic nerve block on postoperative pain and spinal cord inflammation was observed in rats with plantar incision in this study. This study found that single sciatic nerve block could not improve postoperative pain or inhibit the activation of glial cells in the spinal cord, but could reduce the expression of inflammatory factors in the spinal cord. Nerve block combined with flurbiprofen could not only inhibit spinal cord inflammation but also improve postoperative pain, indicating that multimodal analgesia had a better effect, which provided a reference for the rational application of nerve block in clinical practice.
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of P.R. China (Grant No. 82171228).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weiser TG, Haynes AB, Molina G, et al. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet. 2015;385(Suppl 2):S11. doi:10.1016/S0140-6736(15)60806-6
2. Small C, Laycock H. Acute postoperative pain management. Br J Surg. 2020;107(2):e70–e80. doi:10.1002/bjs.11477
3. Daksla N, Wang A, Jin Z, Gupta A, Bergese SD. Oliceridine for the management of moderate to severe acute postoperative pain: a narrative review. Drug Des Devel Ther. 2023;17:875–886. doi:10.2147/DDDT.S372612
4. Richebe P, Capdevila X, Rivat C. Persistent postsurgical pain: pathophysiology and preventative pharmacologic considerations. Anesthesiology. 2018;129(3):590–607. doi:10.1097/ALN.0000000000002238
5. Ishida Y, Okada T, Kobayashi T, Funatsu K, Uchino H. Pain management of acute and chronic postoperative pain. Cureus. 2022;14(4):e23999. doi:10.7759/cureus.23999
6. Glare P, Aubrey KR, Myles PS. Transition from acute to chronic pain after surgery. Lancet. 2019;393(10180):1537–1546. doi:10.1016/S0140-6736(19)30352-6
7. Campanelli G. Primary inguinal hernia, postoperative chronic pain and quality of life. Hernia. 2023;27(1):1–2. doi:10.1007/s10029-023-02750-x
8. Saranteas T, Koliantzaki I, Savvidou O, et al. Acute pain management in trauma: anatomy, ultrasound-guided peripheral nerve blocks and special considerations. Minerva Anestesiol. 2019;85(7):763–773. doi:10.23736/S0375-9393.19.13145-8
9. Prasetia R, Albana R, Herman H, Lesmana R, Chernchujit B, Rasyid HN. Ultrasound-guided suprascapular nerve block at spinoglenoid notch and glenohumeral joint hydrodilation. Arthrosc Tech. 2022;11(7):e1233–e1238. doi:10.1016/j.eats.2022.03.009
10. Chen J, Song D, Zheng G, Luo Y. Systematic review and meta-analysis of the effect of nerve block under ultrasound in ilioinguinal/iliohypogastric in children. Transl Pediatr. 2022;11(10):1604–1614. doi:10.21037/tp-22-308
11. Chan JJ, Garden E, Chan JC, et al. Peripheral nerve block use in ankle arthroplasty and ankle arthrodesis: utilization patterns and impact on outcomes. J Anesth. 2021;35(6):879–888. doi:10.1007/s00540-021-02994-w
12. Polshin V, Petro J, Wachtendorf LJ, et al. Effect of peripheral nerve blocks on postanesthesia care unit length of stay in patients undergoing ambulatory surgery: a retrospective cohort study. Reg Anesth Pain Med. 2021;46(3):233–239. doi:10.1136/rapm-2020-102231
13. Genc C, Kaya C, Bilgin S, Dost B, Ustun YB, Koksal E. Pectoserratus plane block versus erector spinae plane block for postoperative opioid consumption and acute and chronic pain after breast cancer surgery: a randomized controlled trial. J Clin Anesth. 2022;79:110691. doi:10.1016/j.jclinane.2022.110691
14. Lavand’homme P. Rebound pain after regional anesthesia in the ambulatory patient. Curr Opin Anaesthesiol. 2018;31(6):679–684. doi:10.1097/ACO.0000000000000651
15. Sort R, Brorson S, Gogenur I, Nielsen JK, Moller AM. Rebound pain following peripheral nerve block anaesthesia in acute ankle fracture surgery: an exploratory pilot study. Acta Anaesthesiol Scand. 2019;63(3):396–402. doi:10.1111/aas.13290
16. Dada O, Gonzalez Zacarias A, Ongaigui C, et al. Does rebound pain after peripheral nerve block for orthopedic surgery impact postoperative analgesia and opioid consumption? A narrative review. Int J Environ Res Public Health. 2019;16:18. doi:10.3390/ijerph16183257
17. Hade AD, Okano S, Pelecanos A, Chin A. Factors associated with low levels of patient satisfaction following peripheral nerve block. Anaesth Intensive Care. 2021;49(2):125–132. doi:10.1177/0310057X20972404
18. Barry GS, Bailey JG, Sardinha J, Brousseau P, Uppal V. Factors associated with rebound pain after peripheral nerve block for ambulatory surgery. Br J Anaesth. 2021;126(4):862–871. doi:10.1016/j.bja.2020.10.035
19. Fang J, Shi Y, Du F, et al. The effect of perineural dexamethasone on rebound pain after ropivacaine single-injection nerve block: a randomized controlled trial. BMC Anesthesiol. 2021;21(1):47. doi:10.1186/s12871-021-01267-z
20. Haddad M, Alsalem M, Aldossary SA, et al. The role of adenosine receptor ligands on inflammatory pain: possible modulation of TRPV1 receptor function. Inflammopharmacology. 2023;31(1):337–347. doi:10.1007/s10787-022-01127-3
21. Alsalem M, Aldossary SA, Haddad M, et al. The desensitization of the transient receptor potential vanilloid 1 by nonpungent agonists and its resensitization by bradykinin. Neuroreport. 2020;31(11):781–786. doi:10.1097/WNR.0000000000001485
22. Beloeil H, Gentili M, Benhamou D, Mazoit JX. The effect of a peripheral block on inflammation-induced prostaglandin E2 and cyclooxygenase expression in rats. Anesth Analg. 2009;109(3):943–950. doi:10.1213/ane.0b013e3181aff25e
23. Yin Q, Zhang Y, Lv R, et al. A fixed-dose combination, QXOH/ levobupivacaine, produces long-acting local anesthesia in rats without additional toxicity. Front Pharmacol. 2019;10:243. doi:10.3389/fphar.2019.00243
24. Yamada T, Hasegawa-Moriyama M, Kurimoto T, Saito T, Kuwaki T, Kanmura Y. Peripheral nerve block facilitates acute inflammatory responses induced by surgical incision in mice. Reg Anesth Pain Med. 2016;41(5):593–600. doi:10.1097/AAP.0000000000000458
25. Zhang W, Cong X, Zhang L, et al. Effects of thoracic nerve block on perioperative lung injury, immune function, and recovery after thoracic surgery. Clin Transl Med. 2020;10(3):e38. doi:10.1002/ctm2.38
26. Zhen SQ, Jin M, Chen YX, Li JH, Wang H, Chen HX. Ultrasound-guided paravertebral nerve block anesthesia on the stress response and hemodynamics among lung cancer patients. World J Clin Cases. 2022;10(7):2174–2183. doi:10.12998/wjcc.v10.i7.2174
27. Martin F, Martinez V, Mazoit JX, et al. Antiinflammatory effect of peripheral nerve blocks after knee surgery: clinical and biologic evaluation. Anesthesiology. 2008;109(3):484–490. doi:10.1097/ALN.0b013e318182c2a1
28. Ma K, Bebawy JF, Hemmer LB. Multimodal analgesia and intraoperative neuromonitoring. J Neurosurg Anesthesiol. 2023;35(2):172–176.
29. O’Neill A, Lirk P. Multimodal analgesia. Anesthesiol Clin. 2022;40(3):455–468.
30. Pirie K, Traer E, Finniss D, Myles PS, Riedel B. Current approaches to acute postoperative pain management after major abdominal surgery: a narrative review and future directions. Br J Anaesth. 2022;129(3):378–393. doi:10.1016/j.bja.2022.05.029
31. Deplano A, Karlsson J, Moraca F, et al. Design, synthesis and in vitro and in vivo biological evaluation of flurbiprofen amides as new fatty acid amide hydrolase/cyclooxygenase-2 dual inhibitory potential analgesic agents. J Enzyme Inhib Med Chem. 2021;36(1):940–953. doi:10.1080/14756366.2021.1875459
32. Khasabova IA, Uhelski M, Khasabov SG, Gupta K, Seybold VS, Simone DA. Sensitization of nociceptors by prostaglandin E(2)-glycerol contributes to hyperalgesia in mice with sickle cell disease. Blood. 2019;133(18):1989–1998. doi:10.1182/blood-2018-11-884346
33. Zhou ZJ, Tang J, Li WH, Tao WD. Preoperative intravenous flurbiprofen reduces postoperative pain and inflammatory cytokines in elderly patients after Hip arthroplasty. Exp Ther Med. 2019;17(1):354–358. doi:10.3892/etm.2018.6911
34. Davis B, Erickson S, Wojtalewicz S, et al. Entrapping bupivacaine-loaded emulsions in a crosslinked-hydrogel increases anesthetic effect and duration in a rat sciatic nerve block model. Int J Pharm. 2020;588:119703. doi:10.1016/j.ijpharm.2020.119703
35. Xue X, Fan J, Ma X, et al. Effects of local dexmedetomidine administration on the neurotoxicity of ropivacaine for sciatic nerve block in rats. Mol Med Rep. 2020;22(5):4360–4366. doi:10.3892/mmr.2020.11514
36. Guo R, Qiu H, Li H, Ma D, Guan Y, Wang Y. The preemptive analgesic effect of capsaicin involves attenuations of epidermal keratinocytes proliferation and expression of pro-inflammatory mediators after plantar incision in rats. J Pain Res. 2023;16:141–149. doi:10.2147/JPR.S395065
37. Kang Y, Xue J, Zheng J, Liang J, Cai C, Wang Y. Upregulation of Hevin contributes to postoperative pain hypersensitivity by inducing neurexin1beta/neuroligin1-mediated synaptic targeting of GluA1-containing AMPA receptors in rat dorsal horn. Brain Res. 2022;1792:148004. doi:10.1016/j.brainres.2022.148004
38. Li T, Liu T, Chen X, et al. Microglia induce the transformation of A1/A2 reactive astrocytes via the CXCR7/PI3K/Akt pathway in chronic post-surgical pain. J Neuroinflammation. 2020;17(1):211. doi:10.1186/s12974-020-01891-5
39. Sun J, Song FH, Wu JY, et al. Sestrin2 overexpression attenuates osteoarthritis pain via induction of AMPK/PGC-1alpha-mediated mitochondrial biogenesis and suppression of neuroinflammation. Brain Behav Immun. 2022;102:53–70. doi:10.1016/j.bbi.2022.02.015
40. Ishida K, Kawamata T, Tanaka S, Shindo T, Kawamata M. Calcitonin gene-related peptide is involved in inflammatory pain but not in postoperative pain. Anesthesiology. 2014;121(5):1068–1079. doi:10.1097/ALN.0000000000000364
41. Sun J, Li N, Duan G, et al. Increased Nav1.7 expression in the dorsal root ganglion contributes to pain hypersensitivity after plantar incision in rats. Mol Pain. 2018;14:1744806918782323. doi:10.1177/1744806918782323
42. Yoshiyama Y, Sugiyama Y, Ishida K, Fuseya S, Tanaka S, Kawamata M. Plantar incision with severe muscle injury can be a cause of long-lasting postsurgical pain in the skin. Life Sci. 2021;275:119389. doi:10.1016/j.lfs.2021.119389
43. Yu ZY, Geng J, Li ZQ, et al. Dexmedetomidine enhances ropivacaine-induced sciatic nerve injury in diabetic rats. Br J Anaesth. 2019;122(1):141–149. doi:10.1016/j.bja.2018.08.022
44. Zhou C, Tang L, Yin Q, et al. Novel compound LL-a produces long and nociceptive-selective regional anesthesia via TRPV1 channels in rodents sciatic nerve block model. Reg Anesth Pain Med. 2020;45(6):412–418. doi:10.1136/rapm-2019-101057
45. Brummett CM, Amodeo FS, Janda AM, Padda AK, Lydic R. Perineural dexmedetomidine provides an increased duration of analgesia to a thermal stimulus when compared with a systemic control in a rat sciatic nerve block. Reg Anesth Pain Med. 2010;35(5):427–431. doi:10.1097/AAP.0b013e3181ef4cf0
46. Geyik FD, Eker D, Yuce Y, et al. The effect of sugammadex on time of sciatic block by perineural bupivacaine in rats. J Invest Surg. 2022;35(5):955–961. doi:10.1080/08941939.2021.1968982
47. Sinnott CJ, Strichartz GR. Levobupivacaine versus ropivacaine for sciatic nerve block in the rat. Reg Anesth Pain Med. 2003;28(4):294–303. doi:10.1016/s1098-7339(03)00188-3
48. Williams BA, Butt MT, Zeller JR, Coffee S, Pippi MA. Multimodal perineural analgesia with combined bupivacaine-clonidine-buprenorphine-dexamethasone: safe in vivo and chemically compatible in solution. Pain Med. 2015;16(1):186–198. doi:10.1111/pme.12592
49. Sousa AM, Ashmawi HA, Costa LS, Posso IP, Slullitel A. Percutaneous sciatic nerve block with tramadol induces analgesia and motor blockade in two animal pain models. Braz J Med Biol Res. 2012;45(2):147–152. doi:10.1590/S0100-879X2011007500164
50. Mehrzadi S, Khalili H, Fatemi I, Malayeri A, Siahpoosh A, Goudarzi M. Zingerone mitigates carrageenan-induced inflammation through antioxidant and anti-inflammatory activities. Inflammation. 2021;44(1):186–193. doi:10.1007/s10753-020-01320-y
51. Mert T, Sahin E, Yaman S, Pain-Relieving SM. Effectiveness of co-treatment with local tramadol and systemic minocycline in carrageenan-induced inflammatory pain model. Inflammation. 2018;41(4):1238–1249. doi:10.1007/s10753-018-0771-1
52. Xiang HC, Lin LX, Hu XF, et al. AMPK activation attenuates inflammatory pain through inhibiting NF-kappaB activation and IL-1beta expression. J Neuroinflammation. 2019;16(1):34. doi:10.1186/s12974-019-1411-x
53. Xing F, Zhang W, Wen J, et al. TLR4/NF-kappaB signaling activation in plantar tissue and dorsal root ganglion involves in the development of postoperative pain. Mol Pain. 2018;14:1744806918807050. doi:10.1177/1744806918807050
54. Brennan TJ, Zahn PK, Pogatzki-Zahn EM. Mechanisms of incisional pain. Anesthesiol Clin North Am. 2005;23(1):1–20. doi:10.1016/j.atc.2004.11.009
55. Wang C, Yue H, Hu Z, et al. Microglia mediate forgetting via complement-dependent synaptic elimination. Science. 2020;367(6478):688–694. doi:10.1126/science.aaz2288
56. Prinz M, Jung S, Priller J. Microglia biology: one century of evolving concepts. Cell. 2019;179(2):292–311. doi:10.1016/j.cell.2019.08.053
57. Fan YX, Hu L, Zhu SH, et al. Paeoniflorin attenuates postoperative pain by suppressing Matrix Metalloproteinase-9/2 in mice. Eur J Pain. 2018;22(2):272–281. doi:10.1002/ejp.1116
58. Liu B, Liu Y, Li N, Zhang J, Zhang X. Oxycodone regulates incision-induced activation of neurotrophic factors and receptors in an acute post-surgery pain rat model. J Pain Res. 2018;11:2663–2674. doi:10.2147/JPR.S180396
59. Wen YR, Suter MR, Ji RR, et al. Activation of p38 mitogen-activated protein kinase in spinal microglia contributes to incision-induced mechanical allodynia. Anesthesiology. 2009;110(1):155–165. doi:10.1097/ALN.0b013e318190bc16
60. Wen YR, Tan PH, Cheng JK, Liu YC, Ji RR. Microglia: a promising target for treating neuropathic and postoperative pain, and morphine tolerance. J Formos Med Assoc. 2011;110(8):487–494. doi:10.1016/S0929-6646(11)60074-0
61. Norden DM, Trojanowski PJ, Villanueva E, Navarro E, Godbout JP. Sequential activation of microglia and astrocyte cytokine expression precedes increased Iba-1 or GFAP immunoreactivity following systemic immune challenge. Glia. 2016;64(2):300–316. doi:10.1002/glia.22930
62. Wang CF, Pancaro C, Gerner P, Strichartz G. Prolonged suppression of postincisional pain by a slow-release formulation of lidocaine. Anesthesiology. 2011;114(1):135–149. doi:10.1097/ALN.0b013e3182001996
63. Henningsen MJ, Sort R, Moller AM, Herling SF. Peripheral nerve block in ankle fracture surgery: a qualitative study of patients’ experiences. Anaesthesia. 2018;73(1):49–58. doi:10.1111/anae.14088
64. Ding X, Liao FF, Su L, et al. Sciatic nerve block downregulates the BDNF pathway to alleviate the neonatal incision-induced exaggeration of incisional pain via decreasing microglial activation. Brain Behav Immun. 2022;105:204–224. doi:10.1016/j.bbi.2022.07.010
65. Kroin JS, Ling ZD, Buvanendran A, Tuman KJ. Upregulation of spinal cyclooxygenase-2 in rats after surgical incision. Anesthesiology. 2004;100(2):364–369. doi:10.1097/00000542-200402000-00027
66. Chen X, Zhang B, Li J, et al. Celastrol attenuates incision-induced inflammation and pain associated with inhibition of the NF-kappaB signalling pathway via SARM. Life Sci. 2018;205:136–144. doi:10.1016/j.lfs.2018.05.020
67. Samad TA, Moore KA, Sapirstein A, et al. Interleukin-1beta-mediated induction of Cox-2 in the CNS contributes to inflammatory pain hypersensitivity. Nature. 2001;410(6827):471–475. doi:10.1038/35068566
68. Jiang M, Deng H, Chen X, Lin Y, Xie X, Bo Z. The efficacy and safety of selective COX-2 inhibitors for postoperative pain management in patients after total knee/Hip arthroplasty: a meta-analysis. J Orthop Surg Res. 2020;15(1):39. doi:10.1186/s13018-020-1569-z
69. Reddyjarugu B, Pavek T, Southard T, Barry J, Singh B. Analgesic efficacy of firocoxib, a selective inhibitor of cyclooxygenase 2, in a mouse model of incisional pain. J Am Assoc Lab Anim Sci. 2015;54(4):405–410.
70. Zhao X, Ji L. Flurbiprofen axetil: analgesic effect and adverse reaction. Pak J Pharm Sci. 2018;31(3):1163–1167.
71. Buisseret B, Guillemot-Legris O, Ben Kouidar Y, Paquot A, Muccioli GG, Alhouayek M. Effects of R-flurbiprofen and the oxygenated metabolites of endocannabinoids in inflammatory pain mice models. FASEB J. 2021;35(4):e21411. doi:10.1096/fj.202002468R
72. Wojcik P, Biernacki M, Domian N, Zarkovic N, Skrzydlewska E. Influence of Inhibition of COX-2-dependent lipid metabolism on regulation of UVB-induced keratinocytes apoptosis by cannabinoids. Biomolecules. 2022;12(6):842. doi:10.3390/biom12060842
73. Haddad M. The impact of CB1 receptor on nuclear receptors in skeletal muscle cells. Pathophysiology. 2021;28(4):457–470. doi:10.3390/pathophysiology28040029
74. Haddad M. The impact of CB1 receptor on inflammation in skeletal muscle cells. J Inflamm Res. 2021;14:3959–3967. doi:10.2147/JIR.S322247
75. Samandar F, Tehranizadeh ZA, Saberi MR, Chamani J. CB1 as a novel target for Ginkgo biloba’s terpene trilactone for controlling chemotherapy-induced peripheral neuropathy (CIPN). J Mol Model. 2022;28(9):283. doi:10.1007/s00894-022-05284-8
76. Gomez-Canas M, Rodriguez-Cueto C, Satta V, Hernandez-Fisac I, Navarro E, Fernandez-Ruiz J. Endocannabinoid-binding receptors as drug targets. Methods Mol Biol. 2023;2576:67–94. doi:10.1007/978-1-0716-2728-0_6
77. Jiang Z, Li Y, Wang Q, et al. Combined-acupoint electroacupuncture induces better analgesia via activating the endocannabinoid system in the spinal cord. Neural Plast. 2022;2022:7670629. doi:10.1155/2022/7670629
78. Dunkman WJ, Manning MW. Enhanced recovery after surgery and multimodal strategies for analgesia. Surg Clin North Am. 2018;98(6):1171–1184. doi:10.1016/j.suc.2018.07.005
79. Iwashita S, Hashiguchi H, Okubo A, Yoneda M, Takai S. Nerve block for pain relief during arthroscopic rotator cuff repair. J Nippon Med Sch. 2020;87(2):87–91. doi:10.1272/jnms.JNMS.2020_87-206
80. Lee JK, Kang C, Hwang DS, et al. An innovative pain control method using peripheral nerve block and patient-controlled analgesia with ketorolac after bone surgery in the ankle area: a prospective study. J Foot Ankle Surg. 2020;59(4):698–703. doi:10.1053/j.jfas.2019.12.001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.