Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Saudi Arabian Physical Therapists’ Knowledge, Attitudes, and Clinical Practice in Diabetes Prevention and Management
Authors Alhowimel AS ![]() , Alshahrani AA, Abulaban AA, Althobeit AM, Alenazi AM
, Alshahrani AA, Abulaban AA, Althobeit AM, Alenazi AM ![]() , Alshehri MM, Alqahtani BA
, Alshehri MM, Alqahtani BA ![]() , Alodaibi F
, Alodaibi F ![]()
Received 21 June 2023
Accepted for publication 7 September 2023
Published 22 September 2023 Volume 2023:16 Pages 2967—2977
DOI https://doi.org/10.2147/DMSO.S426949
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Ahmed S Alhowimel,1 Abdullah A Alshahrani,1 Aseel A Abulaban,1 Areej M Althobeit,1 Aqeel M Alenazi,1 Mohammed M Alshehri,2 Bader A Alqahtani,1 Faris Alodaibi3
1Department of Health and Rehabilitation Sciences, College of Applied Medical Science, Prince Sattam Bin Abdulaziz University, Alkharj, Saudi Arabia; 2Physical Therapy Department, Jazan University, Jazan, Saudi Arabia; 3Department of Rehabilitation Science, King Saud University, Riyadh, Saudi Arabia
Correspondence: Ahmed S Alhowimel, Department of Health and Rehabilitation Sciences, College of Applied Medical Sciences, Prince Sattam Bin Abdulaziz University, AlKharj, 11942, Saudi Arabia, Tel +966115886354, Email [email protected]
Objective: This study explores physical therapists’ current knowledge, attitudes, and practice toward the management and prevention of diabetes in Saudi Arabia.
Patients and Methods: A cross-sectional survey was distributed among physical therapists in Saudi Arabia. The questionnaire included several sections concerning their knowledge, attitude, and current practice toward diabetic management. A total of 301 physical therapists (32% female) participated in our study.
Results: The results suggest that only half of the participants agreed that diabetes management and prevention were within physical therapy’s scope of service. However, approximately 30% of the participants did not regularly check or ask about the glucose levels of their patients with diabetes. Only 55% of the participants correctly answered the knowledge test questions.
Conclusion: This study found that physical therapists in Saudi Arabia have a modest level of diabetes knowledge. The findings indicate that physical therapy educational programs should address diabetes management. Furthermore, continued education is required for current practicing physical therapists in Saudi Arabia.
Keywords: diabetes, knowledge, practice, physical therapy
Background
Among healthcare providers, physical therapists have a unique role in maintaining, restoring, and improving individuals’ activities, movements, and functioning. By doing so, they aid in a patient’s performance and enhance their health and quality of life.1 Diabetes mellitus (DM) is a group of diseases that cause an increase in the amount of glucose in the blood. It is usually divided into type 1 (lack of insulin) and type 2 (insulin resistance) diabetes. Owing to the disease’s nature, patients with diabetes face many side effects and complications in their lives, which have the potential to compromise their quality of life.2–4 As the number of cases of DM is rising in the Kingdom of Saudi Arabia,5 the role of physical therapy in the current clinical practice of disease treatment is critical to prevent and manage complications. Hence, physical therapists practicing in Saudi Arabia should have sound, up-to-date knowledge about this disease to prevent its rise and manage its complications.
Many patients with neurological and orthopedic conditions who are treated by physical therapists also have DM. In the chronic stages of DM, blood circulation decreases, sensations are altered, and patients may feel premature fatigue, experience hypoglycemia during exercise sessions, or have difficulty with wound healing.6–8 Hence, physical therapists’ knowledge of this disease is essential in managing day-to-day care in physical therapy clinics and departments. Noncommunicable diseases, particularly diabetes, have become common in Saudi Arabia. They contribute significantly to mortality and morbidity,9 and type 2 diabetes affects an estimated 14.1% of the Saudi Arabian population.10 In other words, many patients are likely to have diabetes as their main or secondary illness. This makes screening even more important to reduce the risks of hypoglycemia and hyperglycemia during physiotherapy.
Doehring et al11 surveyed 401 Canadian physical therapists about their knowledge, attitudes, and practices toward DM prevention and management. It revealed that physical therapists were most confident in providing exercise education, but lacked confidence in providing care in crucial areas, including managing secondary complications, glucose level control, and weight management. Moreover, by identifying this clinical gap, they provided some important recommendations, such as providing more education related to DM in entry-level programs, and enhancing continuing physical therapy education opportunities to improve physical therapists’ knowledge of DM.11 However, these findings may not be generalizable to other physical therapists, particularly in the Kingdom of Saudi Arabia, because of differences in cultural backgrounds, educational systems, and healthcare policies, which may affect physical therapist practices in the Kingdom.
Another cross-sectional study was conducted in the United States to assess the knowledge, clinical practices, attitudes, and beliefs of physical therapists toward patients with prediabetes.12 The majority of the 63 physical therapists who had participated agreed that detecting prediabetes in their patients was crucial. They were aware of the important clinical diagnostic tests required for the identification of DM, but not of the prediabetic stage. Many of the physical therapists were unaware of prediabetes screening, and their knowledge of correct weight loss and physical activity recommendations was also poor. Hence, the authors recommended more educational services for physical therapists to combat the disease in its early stages.12 The current literature emphasizes the need for physical therapists to have proper education in the prevention and management of DM; however, research on physical therapists’ current knowledge in preventing and managing DM is lacking. Moreover, the current clinical practices and attitudes of physical therapists in Saudi Arabia need to be explored to clarify future research directions to combat the high prevalence of this disease.
Since physical therapists play an important role in prevention and lifestyle modification for people with DM, understanding the needs in physical therapy practices might help in improving the healthcare system for this population. Therefore, this study quantifies the knowledge, attitudes, and current clinical practices of physical therapists in managing and preventing DM in the Kingdom of Saudi Arabia.
Method
Study Design
This cross-sectional study used a convenience sample of physical therapists practicing in Saudi Arabia.
Sample Size Calculation
According to the Saudi Commission for Health Specialties (SCFHS),13 there were around 6028 registered physical therapists in the Kingdom of Saudi Arabia in 2018. In addition, the SCFHS reported that approximately 920 new physical therapists are credentialed every year. In light of these considerations, we estimated setting the number of physical therapists somewhere between 8500 and 9000. Confidence was set at 90%, while the margin of error was fixed at 5%. Based on these considerations, we determined that a sample size of 265 physical therapists would be adequate for this cross-sectional study.
Inclusion Criteria
The inclusion criteria were any licensed physical therapist practicing in Saudi Arabia, of any gender or educational background.
Exclusion Criteria
Interns and students of physical therapy who had not obtained their practice licenses were excluded from the study.
Procedure
Permission from Doehring et al11 was first obtained to use their questionnaire in the Kingdom of Saudi Arabia. The institutional ethical committee was then approached for their approval (RHPT/021/019). After obtaining ethical approval, the questionnaire was converted to an online format using Google Forms, and an online link was created. This online questionnaire (Google Drive survey) was shared with practicing Saudi Arabian physical therapists in various settings (hospitals, clinics, primary care, and home care), either full- or part-time, in the private or public health sectors, and at all educational levels (bachelor’s, master’s, and PhD).All participants gave their consent to participate in the study and the (SCFHS) registration number was used to verify licensed therapists. All regions in Saudi Arabia were included. The questionnaire was conducted online to make distribution more accessible and at no cost. Data were collected at a single point in time over the course of two months, and captured on Microsoft Excel (version 2010) spreadsheets before being statistically analyzed using IBM’s Statistical Package for Social Sciences (SPSS, Version 23; IBM Corp, Armonk, NY).
Outcome Measure
An existing questionnaire tool had been developed and used by Doehring et al11 to assess the present knowledge, practice, beliefs, and attitudes of physical therapists dealing with patients with diabetes in Canada. Approval to use this questionnaire was received from the authors before conducting this study. The questionnaire consisted of 40 questions divided into four sections:
- Section 1: demographic data.
- Section 2: educational background; the domains of attitudes and beliefs about the physical therapist’s role in preventing and managing DM complications.
- Section 3: current clinical practice.
- Section 4: DM knowledge.
A cover letter explained the purpose of the study to the participants. This survey included closed-ended and multiple-choice questions (yes or no, and Likert-type questions on a 5-point rating scale), and participants were able to furnish further details (if required). All the questions were mandatory, with no identifier information questions. The Google Drive survey settings were set to reject multiple responses from the same IP address.
Questionnaire Validity
The questions were checked by giving the questionnaire to a group of 15 physical therapists from different backgrounds and receiving their feedback concerning clarity, length of time, and relevance.
Questionnaire Distribution
We distributed the questionnaire between November 2021 and February 2022, using an anonymous and voluntary electronic survey and posting it on Twitter, which is one of the most popular social media apps used by health care providers in Saudi Arabia to share health information with the public.13,14 In addition, we used WhatsApp, which is another commonly used app among health care staff for both formal and informal use.15,16 These two applications were appropriate ways to broadcast the survey among registered physical therapists in all provinces of Saudi Arabia (Riyadh, Makkah, Eastern, Al-Baha, Al-Jawf, Northern borders, Al-Qassim, Hail, Tabuk, Asser, Jizan, and Najran).
Data Analysis
The normal distribution of the data was analyzed using frequency histograms. The univariate analysis of the single variable for mean, mode, median, minimum, maximum, range, percentages, ratios, standard deviations, and standard errors was calculated using descriptive statistics and frequencies. For data analysis and grouping responses that were similar, some responses were included in one category. Responses in the attitudes and beliefs section of “strongly agree” and “agree” were categorized as one group, “neutral” formed one group, and “disagree” and “strongly disagree” were another group. Concerning the current practice data, we categorized “always” and “most of the time” as one group, “sometimes” as another group, and “infrequently” and “never” as a third group.
Results
A total of 301 individuals participated in this study, 96 of whom were women. The age range was 20–50 years. However, a majority of the sample (68.4%) was in the 20–29 age group. Around 50.8% were new graduates with less than two years of experience (50.1%) who worked in the government sector at an outpatient clinic (41.9%). A vast majority of the sample (71.8%) had a minimum of a bachelor’s degree in physical therapy, with no further training in DM (73.4%). Table 1 contains further details regarding the participants’ demographic characteristics and practice-related information.
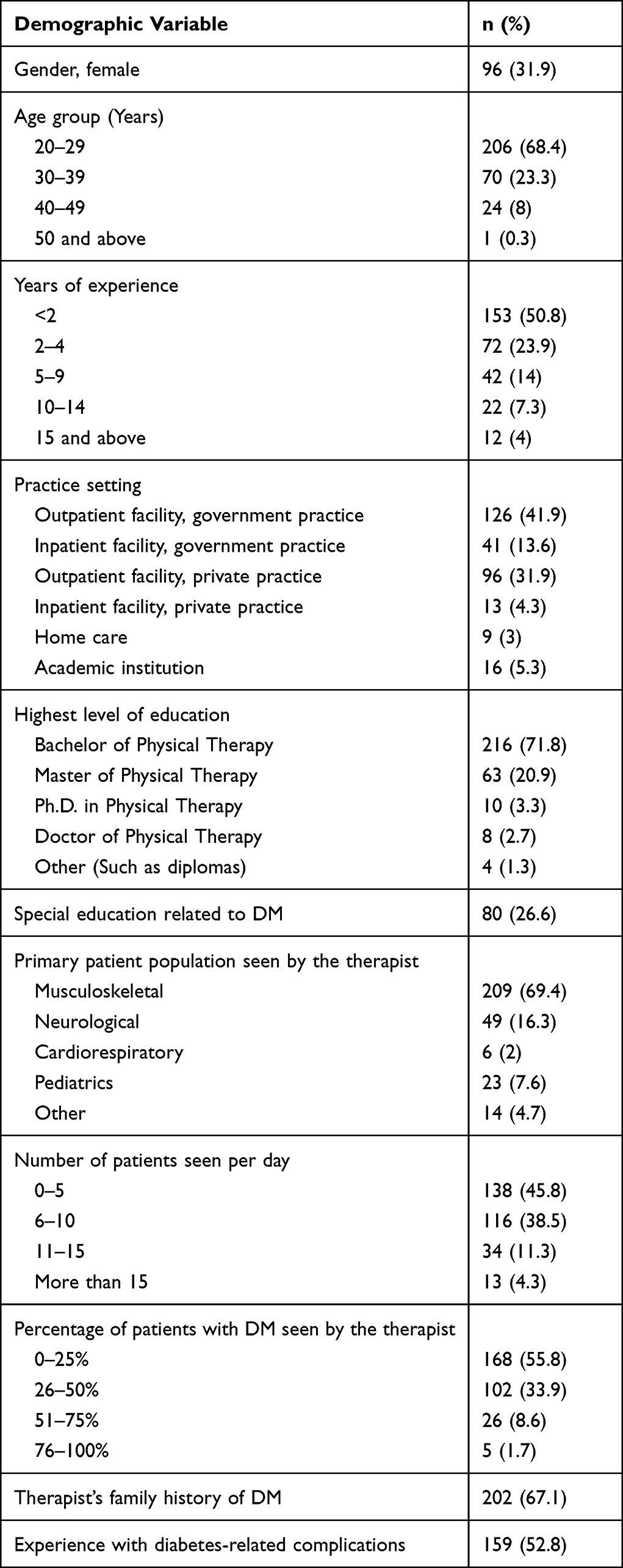 |
Table 1 Demographic Characteristics of the Participants |
The answers to the individual items were grouped into three sections: attitude and behavior, the therapist’ current practice and knowledge about DM, and the role of the physical therapist in treating DM difficulties.
Attitudes and Behavior
The findings revealed that the therapists’ attitudes and conduct toward patients with diabetes varied. Although they felt that the therapist played an important role in prescribing exercise (88%), they believed their role was less important with DM-related management, such as nutrition, managing weight, blood glucose, stress, and secondary problems. Physical therapists were most confident in exercise prescriptions (87%), compared with other treatment options. Approximately 75% of the physical therapists felt physical therapy might play a preventive role, and knew when and where to recommend patients for the appropriate treatment. Table 2 presents detailed answers from the study sample.
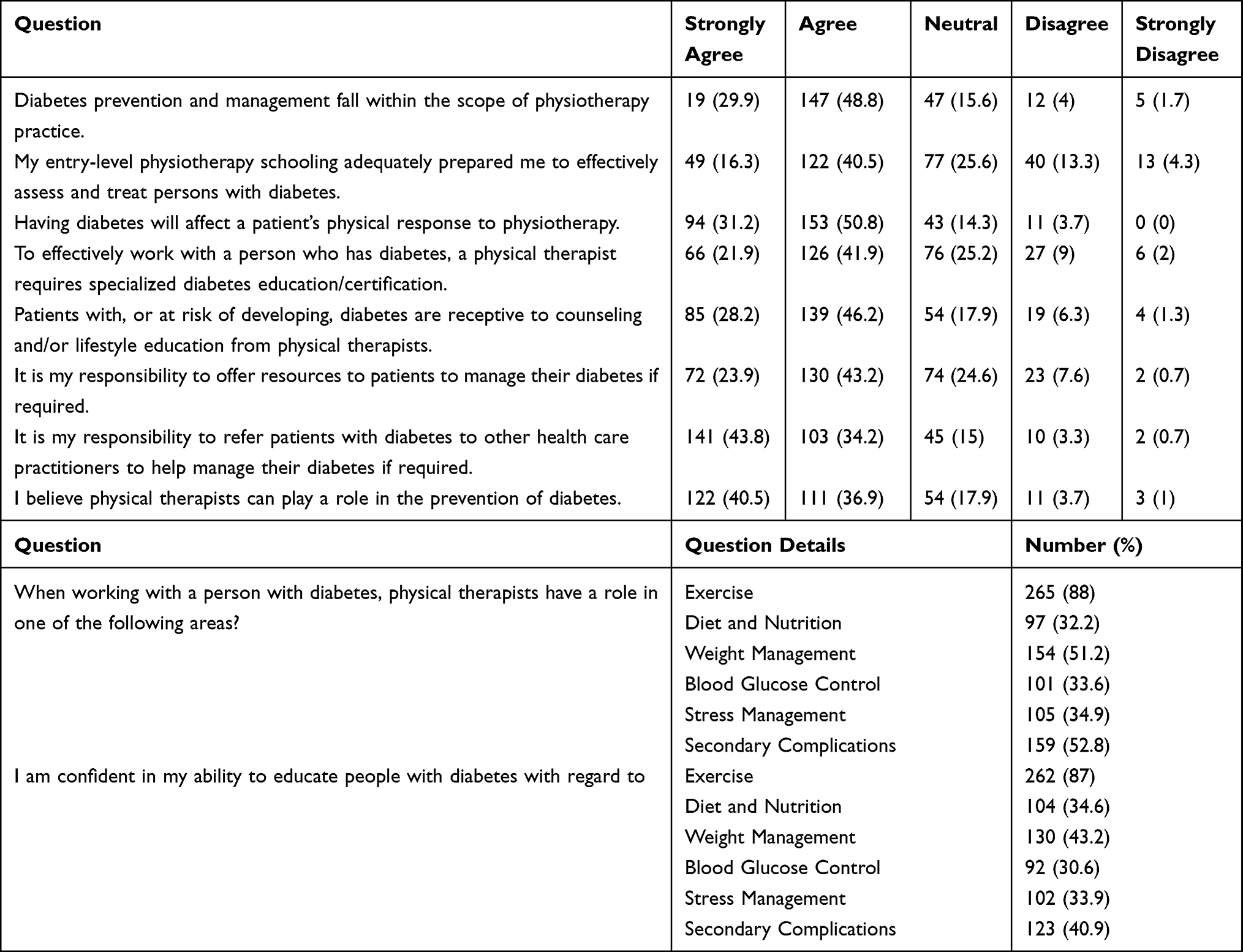 |
Table 2 Descriptive Data for Attitudes and Beliefs |
Current Practice
Many physical therapists (73.4%) had no specialized education related to DM, and most of the treated patient group complained of musculoskeletal diseases (69.4%). The majority of the therapists (84.3%) saw up to 10 patients with DM every day, and almost 50% of their total patients suffered from DM (89.7%).
According to the responses, the current practice of physical therapy for patients with DM varied. Only 70% of physical therapists checked their patients for DM, and only 70% inquired about blood glucose management if their patients reported having DM. Half of the participants asked patients to monitor their blood glucose levels. Interestingly, only 53% watched for low blood glucose warning indicators during exercise and therapy. However, 60% stated that they were counseling patients with DM. The impediments to counseling were a lack of time (18%), lack of training (18%), and a notion that DM was beyond their scope of practice (16%). Table 3 illustrates detailed responses from the sample.
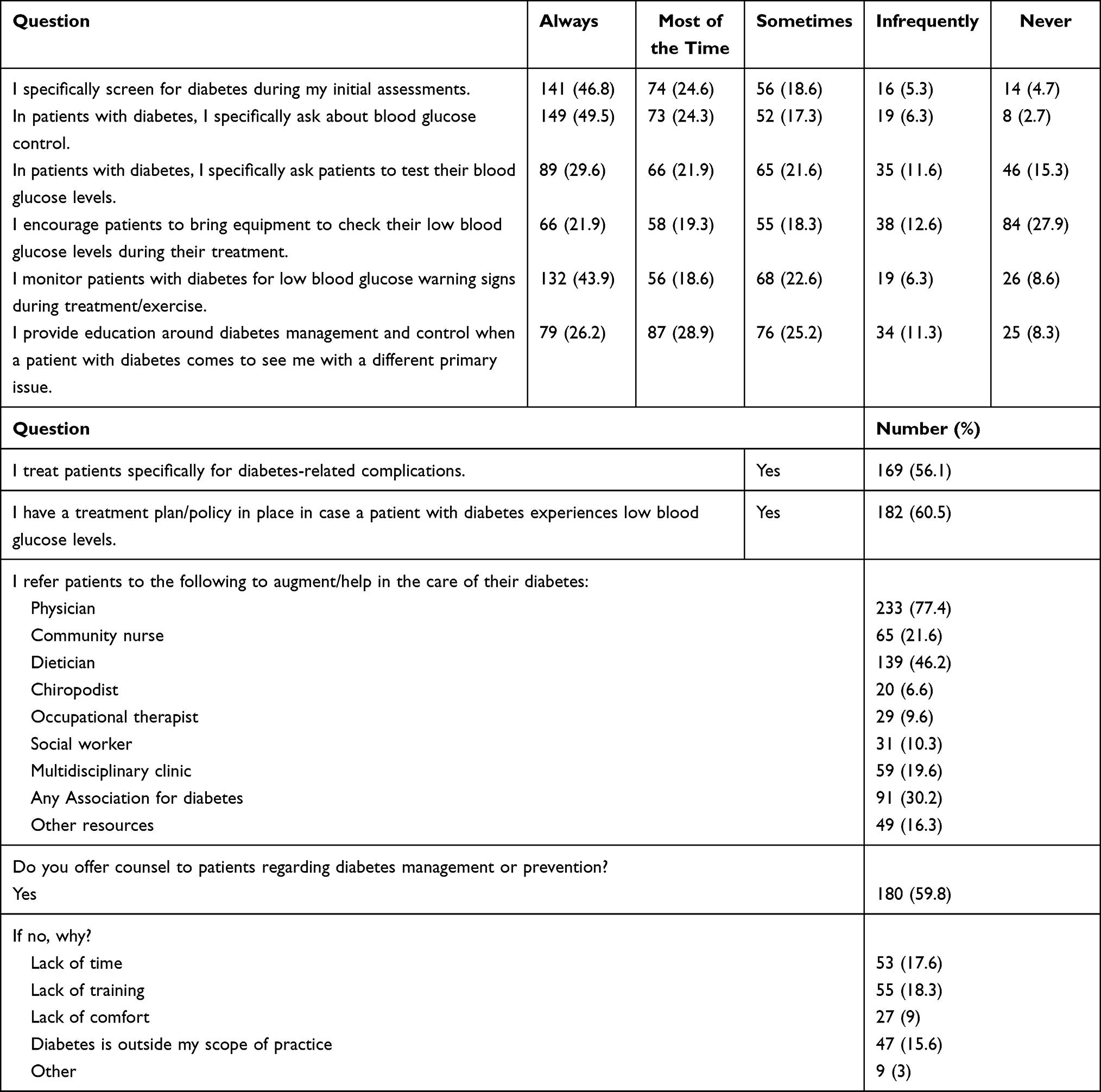 |
Table 3 Descriptive Data for Current Practices |
Knowledge
This part had two multiple-choice questions on exercise type and intensity, as well as two questions about the management of low blood glucose in practice. In all four questions, the response rate of correct answers was less than 55% (Table 4).
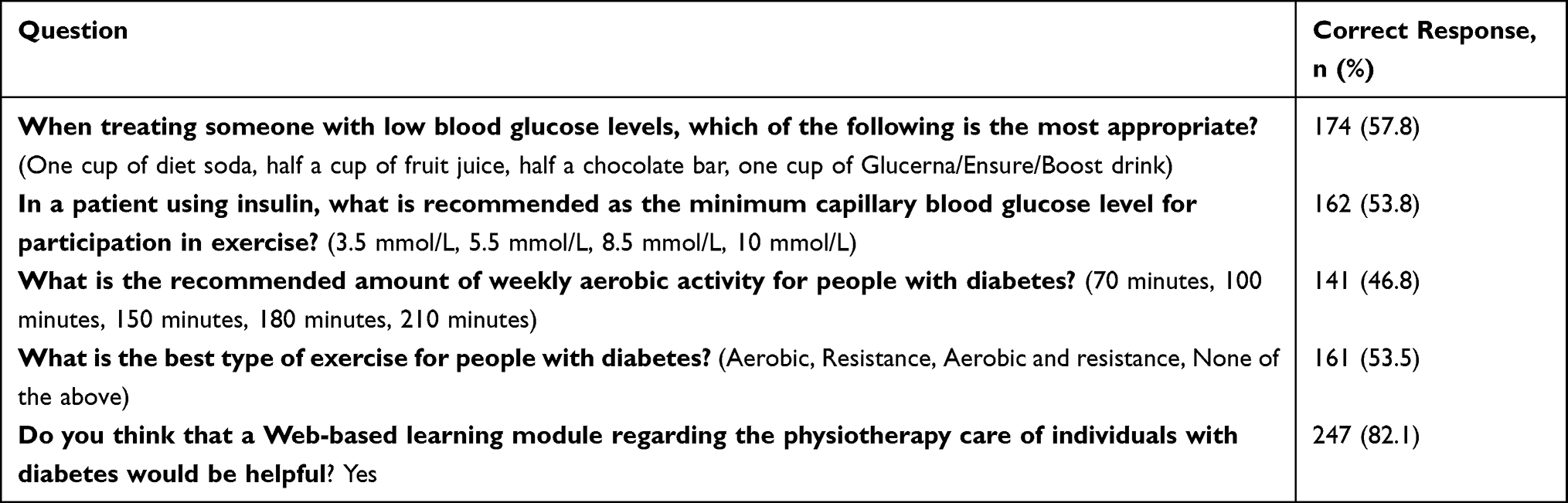 |
Table 4 Descriptive Data for Knowledge |
Discussion
This was the first study in Saudi Arabia to assess physical therapists’ knowledge, attitudes, and existing practices in relation to DM prevention and management. The findings highlighted that although 75% of the surveyed sample acknowledged the role of a physical therapist in the management and prevention of DM, only 30% screened for DM before therapy, and half of the sample did not monitor warning signs for blood glucose during exercise. Furthermore, the knowledge part of the survey revealed that half of the participants lacked knowledge about DM management.
Most participants in this study believed that physiotherapy was a significant health provision in preventing and treating DM. This was in line with the World Health Organization’s global action plan (2013–2020) for all health professionals to have a role in non-communicable disease prevention and control.17 Physical therapists played an important role in the multidisciplinary healthcare team through at least three different means, including recommending physical activity to patients, identifying diabetes risk factors, and advocating for regular physical activity as an essential component of managing chronic diseases.18
The majority (72%) believed that physical therapists should counsel and educate patients with DM, or those at risk of getting it, on the importance and relevance of lifestyle changes. It was also suggested that physical therapists played coaching roles in the prevention and management of diabetes through a variety of means, beginning with exercise and physical activity prescription, diet and weight management, glucose education, and the management of secondary complications.19–22
These findings may represent a mismatch between the expected and current practices of a physical therapist in Saudi Arabia, which may be explained by an absence of diabetes knowledge and clinical practice in formal education.23 A lack of confidence might be a result of insufficient knowledge or practical experience of the issues affecting patients with primary or secondary diabetes, suggesting the need to modify the education curriculum to include a focus on DM management and prevention. Moreover, current clinical practice needs to adapt to the International Classification of Functioning, Disability, and Health’s contextual factors, which are supported by the second physical therapy summit on global health for health promotion in daily practice to reduce the burden of non-communicable diseases.20,21
Doehring et al11 surveyed 401 Canadian physical therapists about their knowledge, attitudes, and practice toward DM prevention and management. It transpired that physical therapists were most confident in providing exercise education, but lacked confidence in providing care in crucial areas, including managing secondary complications, glucose level control, and weight management. By identifying this clinical gap, they provided some important recommendations, such as providing more education related to DM in entry-level programs and enhancing continuing physical therapy education opportunities to improve physical therapists’ knowledge of DM.11 However, these findings may not be generalizable to other physical therapists, particularly in the Kingdom of Saudi Arabia, because of differences in cultural backgrounds, educational systems, and healthcare policies, which may affect physical therapist practices in the Kingdom.
Another cross-sectional study was conducted in the United States to assess the knowledge, clinical practices, attitudes, and beliefs of physical therapists toward patients with prediabetes.12 The majority of the 63 physical therapists who had participated agreed that detecting prediabetes in their patients was crucial. They were aware of the important clinical diagnostic tests required for the identification of DM, but not of the prediabetic stage. Many of the physical therapists were unaware of prediabetes screening, and their knowledge of correct weight loss and physical activity recommendations was also poor. Hence, the authors recommended more educational services for physical therapists to combat the disease in its early stages.12 Existing literature emphasizes the need for physical therapists to have proper education in the prevention and management of DM, but research on physical therapists’ current knowledge in preventing and managing DM is lacking. Moreover, the current clinical practices and attitudes of physical therapists in Saudi Arabia need to be explored to clarify future research directions to combat the high prevalence of this disease.
Only 57% of the participants knew that a patient with diabetes with low blood glucose levels should be treated with half a cup of fruit juice, while the other half (43%) treated them incorrectly, such as with chocolate bars, diet soda, or nutritional drinks. Knowledge of the treatment is fundamental for providing first aid to patients with DM. This information is readily available online and in community education to raise awareness on how to manage patients with diabetes with low blood glucose levels; such material is for the cognizance of the general public, not just healthcare providers.11,21 A surprising result was that less than half of those surveyed recognized the volume and intensity of weekly aerobic activities suggested for DM patients. The American College of Sports Medicine’s 2nd edition on physical activity guidelines for adults and adult patients with diabetes include guidelines for all people who engage in physical activity, not just patients with DM.24,25 This is similar to the findings of prior research by Canadian physical therapists.11 Furthermore, only half of the participants understood the best types of exercises for patients with DM, suggesting that physical therapists need further training to help healthcare professionals treat DM.
A few participants stated that their entry-level education did not adequately educate them on how to cope with patients with DM. By contrast, a sizable proportion (82.4%) believed the opposite. This result was explained by the significant number of surveyed physical therapists who opined that extra education or sub-specialties in diabetes were necessary. All these findings point to a significant dearth of understanding of DM as a disease and its care in entry-level education. This could explain why 82% of the participants believed that a web-based learning module on DM patient physiotherapy would be effective. There is evidence of the effectiveness of providing continuing medical education on DM to healthcare workers in improving their knowledge and clinical practices.26 To address these gaps, changes in practice are required, and consideration should be given to the possibility of establishing higher education or diploma courses in DM for registered Saudi physical therapists to help them gain additional specific knowledge, thereby allowing them to better care for patients with DM.
For the current practice of physical therapists, less than half (46.8%) always screened for DM during initial evaluations, and only half (50%) frequently inquired about blood glucose management. It should be mentioned that frequent blood glucose checks are important for those who are recently diagnosed with diabetes, but they are probably unnecessary for those who have had diabetes for a while, or who are active in their leisure or occupation. In fact, for the light to moderate exercise conducted within a physiotherapy clinic, blood glucose is likely to temporarily rise, and then decline substantially > 0.5–1 hour after the cessation of exercise.27 A similar study in Nigeria was conducted among physical therapists on how frequently they asked older people about previous falls during first evaluations, and the results revealed that approximately half of them (56.5%) regularly asked their patients about that.28 This shows that physical therapists may not be very good at screening during the first examination, and that interdisciplinary training was insufficient. To minimize exercise-related damage, pre-evaluation measures are required before beginning any physical activity training, as is modifying medication dosage for insulin consumption in patients with DM to avoid hypoglycemia throughout the session.29–31
The results highlight that more than half of the participants were aware of the minimal capillary blood glucose level required for a patient to begin a physical activity in order to prevent further difficulties and dangers. However, only a handful required patients with DM to carry their equipment so as to constantly monitor their blood glucose levels throughout treatment. This signifies a failure to assess blood glucose levels before beginning exercises, which may result in significant safety concerns, a high risk of hypoglycemia during physical therapy sessions, and other consequences for patients with DM.
Physical therapists agreed that they could assist patients with DM, but they perceived hurdles to controlling the disease, such as a lack of specialized professional training or understanding. Our study showed that most physical therapists identified a role for themselves in preventing and managing DM. They could demonstrate sound knowledge in this regard; however, physical therapists with many years of experience or a higher academic degree performed only averagely when dealing with patients with DM. Physical therapists who had undergone DM management courses displayed a wealth of information and improved performance and outcomes with their patients with DM. Their expertise appeared to be positively reflected in their practice routines.
This study has some limitations. First, despite the fact that we included all genders in our study, we received fewer responses from female therapists. Second, most participants were under 30 years old and had less than five years’ experience. This study’s sample size was appropriate, but the diversity of participants’ practice locations was limited, which may not accurately represent the viewpoint of the entire country. Consequently, future research should ensure equitable gender, age, and location distribution in its sample. In addition, the study indicated that 46% of the participants saw < 5 patients per day; academic physical therapists and physical therapists with limited experience (ie, < 2 years of experience) dealt with only a few patients per day. Future researchers should control for years of experience to better evaluate factors associated with diabetes management and physical therapists’ practice in Saudi Arabia. If similar numbers of participants were recruited from all regions, the outcomes would be more generalizable. This study may foster a new perspective on the role physical therapists play in DM management. It may also serve as a springboard for further research into current knowledge, attitudes, and practices among physical therapists regarding DM, and help guide future research on how to support physical therapists in caring for their patients with DM.
Conclusion
This study found that physical therapists in Saudi Arabia had a modest level of diabetes knowledge and a positive attitude toward exercise education, but they exhibited lower educational behaviors in other areas. In their regular clinical practice, many of them do not screen for DM or assess blood glucose during exercise sessions for patients with DM. This indicates a need to develop educational programs and clinical practice guidelines that address DM for practicing physical therapists in Saudi Arabia. The healthcare system in Saudi Arabia must provide physical therapists with the education and tools for quality DM assessment and management.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author (Ah.A) upon reasonable request.
Ethics Approval and Consent to Participate
This project was approved by Prince Sattam Bin Abdulaziz University’s Ethical Committee (RHPT/021/019). All methods were carried out in accordance with relevant guidelines and regulations according to the Declaration of Helsinki. The participants agreed to participate before the questionnaires were disseminated. Informed consent was obtained from all participants involved in the study.
Acknowledgments
We are immensely grateful to all participants in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The authors extend their appreciation to the Deputyship of Research and Innovation, Ministry of Education in Saudi Arabia for funding this research study, project number: IF2/PSAU/2022/03/21121.
Disclosure
The authors declare that they have no competing interests.
References
1. Pagliarulo MA. Introduction to Physical Therapy. E-book. Elsevier Health Science; 2021. Available from: https://books.google.com.sa/books?id=5DgEEAAAQBAJ.
2. Kaul K, Tarr JM, Ahmad SI, Kohner EM, Chibber R. Introduction to Diabetes Mellitus. In: Ahmad SI, editor. Diabetes. Advances in Experimental Medicine and Biology. Vol. 771. New York, NY: Springer; 2013:1–11.
3. American Diabetes Association. Classification and diagnosis of diabetes: standards of medical care in diabetes—2019. Diabetes Care. 2019;42(suppl 1):S13–S28. doi:10.2337/dc19-S002
4. Al-Qerem W, Al-Maayah B, Ling J. Developing and validating the Arabic version of the Diabetes Quality of Life questionnaire. East Mediterr Health J. 2021;27(4):414–426. doi:10.26719/emhj.20.112
5. Alotaibi A, Perry L, Gholizadeh L, Al-Ganmi A. Incidence and prevalence rates of diabetes mellitus in Saudi Arabia: an overview. J Epidemiol Glob Health. 2017;7(4):211–218. doi:10.1016/j.jegh.2017.10.001
6. Cannata F, Vadalà G, Russo F, Papalia R, Napoli N, Pozzilli P. Beneficial effects of physical activity in diabetic patients. J Funct Morphol Kinesiol. 2020;5(3):70. doi:10.3390/jfmk5030070
7. Papatheodorou K, Banach M, Bekiari E, Rizzo M, Edmonds M. Complications of diabetes 2017. J Diabetes Res. 2018;2018:3086167. doi:10.1155/2018/3086167
8. Das KV, Jayakumar RV, Unnikrishnan AG, Poulose KP. Complications of diabetes mellitus. In: Textbook of Medicine. Jaypee Brothers Medical Publishers Ltd; 2008:556. Available from: https://www.jaypeedigital.com/book/9788184483888/chapter/ch91.
9. Mabry R, Koohsari MJ, Bull F, Owen N. A systematic review of physical activity and sedentary behaviour research in the oil-producing countries of the Arabian Peninsula. BMC Public Health. 2016;16(1):1003. doi:10.1186/s12889-016-3642-4
10. Lee I-M, Shiroma EJ, Lobelo F, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380(9838):219–229. doi:10.1016/S0140-6736(12)61031-9
11. Doehring K, Durno S, Pakenham C, Versi B, DePaul VG. Knowledge, attitudes, and current practices of Canadian physical therapists in preventing and managing diabetes. Physiother Can. 2016;68(3):298–306. doi:10.3138/ptc.2015-63
12. Ross M, Purrington B, Zuniga C, Farnand B, Pattacciato F. Survey of physical therapists’ knowledge of screening and management practices for patients with prediabetes. Physiother Pract Res. 2021;41(2):213–223.
13. Saudi Commission for Health Specialties Health Workforce; 2018. Available from: https://www.scfhs.org.sa/Media/DigitalLibrary/DocumentLibrary/OtherPublications/Pages/default.aspx.
14. Roland D, Spurr J, Cabrera D. Preliminary evidence for the emergence of a health care online community of practice: using a netnographic framework for Twitter hashtag analytics. J Med Internet Res. 2017;19(7):e252. doi:10.2196/jmir.7072
15. Alassiri SA, Alowfi AS. Public’s attitudes toward health information on Twitter: a cross-sectional survey based on the Saudi population. Cureus. 2019;11(10):e5863. doi:10.7759/cureus.5863
16. Rashidi Y, Vaniea K, Camp JL Understanding Saudis’ privacy concerns when using WhatsApp.
17. Pahwa P, Broughton E. Strengthening quality improvement work in hospitals using WhatsApp: an exploratory qualitative study from an Indian hospital. Int J Qual Health Care. 2017;29:25. doi:10.1093/intqhc/mzx125.37
18. Ruof J, Cieza A, Wolff B, et al. ICF Core Sets for diabetes mellitus. J Rehabil Med. 2004:100–106. doi:10.1080/16501960410016802
19. Harris-Hayes M, Schootman M, Schootman JC, Hastings MK. The role of physical therapists in fighting the type 2 diabetes epidemic. J Orthop Sports Phys Ther. 2020;50(1):5–16. doi:10.2519/jospt.2020.9154
20. Dean E, Al-Obaidi S, De Andrade AD, et al. The first physical therapy summit on global health: implications and recommendations for the 21st century. Physiother Theory Pract. 2011;27(8):531–547. doi:10.3109/09593985.2010.544052
21. Dean E, de Andrade AD, O’Donoghue G, et al. The Second Physical Therapy Summit on Global Health: developing an action plan to promote health in daily practice and reduce the burden of non-communicable diseases. Physiother Theory Pract. 2014;30(4):261–275. doi:10.3109/09593985.2013.856977
22. Dean E, Skinner M, Myezwa H, et al. Health competency standards in physical therapist practice. Phys Ther. 2019;99(9):1242–1254. doi:10.1093/ptj/pzz087
23. O’Brien MW, Shields CA, Campbell KL, Crowell SJ, Fowles JR. Perceptions and practices of providing physical activity counselling and exercise prescriptions among physical therapists in Nova Scotia. Physiother Can. 2020;72(3):230–238. doi:10.3138/ptc-2018-0098
24. Alodaibi FA, Alotaibi MA, Almohiza MA, Alhowimel AS. Physical therapists’ role in health and wellness promotion for people with musculoskeletal disorders: a cross-sectional description study conducted in Saudi Arabia. J Multidiscip Healthc. 2022;15:567–576. doi:10.2147/JMDH.S356932
25. Piercy KL, Troiano RP, Ballard RM, et al. The physical activity guidelines for Americans. JAMA. 2018;320(19):2020–2928. doi:10.1001/jama.2018.14854
26. Colberg SR. Key points from the updated guidelines on exercise and diabetes. Front Endocrinol (Lausanne). 2017;8:33. doi:10.3389/fendo.2017.00033
27. Lim SC, Mustapha FI, Aagaard-Hansen J, Calopietro M, Aris T, Bjerre-Christensen U. Impact of continuing medical education for primary healthcare providers in Malaysia on diabetes knowledge, attitudes, skills and clinical practices. Med Educ Online. 2020;25(1):1710330. doi:10.1080/10872981.2019.1710330
28. Moore J, Bartholomae EM, Ward K, Hooshmand S, Kressler J. Three minutes of moderate-intensity stair walking improves glucose and insulin but not insulin sensitivity or total antioxidant capacity. Nutr Metab Cardiovasc Dis. 2022;32(2):479–486. doi:10.1016/j.numecd.2021.10.016
29. Kalu ME, Vlachantoni A, Norman KE. Knowledge about risk factors for falls and practice about fall prevention in older adults among physical therapists in Nigeria. Physiother Res Int. 2019;24(1):e1742. doi:10.1002/pri.1742
30. Mendes R, Sousa N, Reis VM, Themudo-Barata JL. Prevention of exercise-related injuries and adverse events in patients with type 2 diabetes. Postgrad Med J. 2013;89(1058):715–721. doi:10.1136/postgradmedj-2013-132222
31. Colberg SR, Sigal RJ, Fernhall B, et al. Exercise and type 2 diabetes: the American College of Sports Medicine and the American Diabetes Association: joint position statement. Diabetes Care. 2010;33(12):e147–e167. doi:10.2337/dc10-9990
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessment of Knowledge, Practice, and Associated Factors Towards Airway and Breathing Management Among Nurses Working in the Emergency Departments of Selected Public Hospitals in Addis Ababa, Ethiopia: A Cross-Sectional Study
Nigatu M, Debebe F, Tuli W
Open Access Emergency Medicine 2022, 14:235-247
Published Date: 27 May 2022
Knowledge and Practice of Wound Care and Associated Factors among Nurses Working in South Wollo Zone Government Hospitals, Ethiopia
Tegegne B, Yimam F, Mengesha Yalew Z, Wuhib M, Mekonnen L, Asmamaw Yitayew Y, Ademe S, Tsegaye D, Eshetie Y, Chanie M
Chronic Wound Care Management and Research 2022, 9:1-11
Published Date: 20 July 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Current Perspectives, Practices, and Barriers Faced by Community Pharmacists Regarding Pharmaceutical Care Services for Diabetes Mellitus in the United Arab Emirates
Jairoun AA, Al-Hemyari SS, Shahwan M, Jairoun SA, Alorfi NM, Zyoud SH, Suliman AA, Shahwan MK, Alnuaimi G, Shahwan M, Al-Qirim T, El-Dahiyat F
Journal of Multidisciplinary Healthcare 2024, 17:2563-2576
Published Date: 23 May 2024
Knowledge, Attitudes, and Practices of Elderly Diabetic Patients and Their Families Regarding Comorbid Non-Alcoholic Fatty Liver Disease: A Structural Equation Modeling Analysis
Wang Q, Zhang Y, Guo X, Zhao L
Diabetes, Metabolic Syndrome and Obesity 2025, 18:3833-3844
Published Date: 15 October 2025