")
Back to Journals » International Journal of General Medicine » Volume 16
Safety of Inactivated SARS-CoV-2 Vaccines Among Adults with Experience of Allergies to Food or Medicines
Authors Jin Y, Zheng M, He S, Chen M, Cao C
Received 21 May 2023
Accepted for publication 14 July 2023
Published 21 July 2023 Volume 2023:16 Pages 3105—3113
DOI https://doi.org/10.2147/IJGM.S422337
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Yan Jin,1,2 Mengmeng Zheng,1 Shiyi He,1 Meiping Chen,1 Chao Cao1
1Department of Respiratory and Critical Care Medicine, Key Laboratory of Respiratory Disease of Ningbo, The First Affiliated Hospital of Ningbo University, Ningbo, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, Municipal Hospital Affiliated to Taizhou University, Taizhou, People’s Republic of China
Correspondence: Chao Cao, Email [email protected]
Abstract: The global pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), commonly known as COVID-19, poses significant risk to human health worldwide. The primary strategy for controlling the disease is through vaccination. However, there is an urgent need to establish confidence in the safety of global vaccination efforts, particularly among populations with allergies, as evidence on the adverse effects of SARS-CoV-2 vaccines in this group remains limited. To address this gap, our study aimed to evaluate the safety of inactivated SARS-CoV-2 vaccines in individuals with food and/or drug allergies. The study enrolled a total of 150 participants, who were subjected to a series of questionnaires to evaluate local and systemic reactions within 7 days after each dose. The results revealed that the most prevalent adverse reactions were pain at the injection site (30%) and fatigue (16%) following the initial vaccination. Notably, the incidence of both local and systemic adverse reactions decreased after the second vaccination, which was unexpected. The food allergy and drug allergy subgroups exhibited a similar phenomenon. Furthermore, the incidence of adverse events observed in this study was consistent with the range reported in Phase III clinical trials of inactivated SARS-CoV-2 vaccines. Our findings suggest that individuals with pre-existing food and/or drug allergies have a favorable safety profile when receiving inactivated SARS-CoV-2 vaccination.
Keywords: inactivated SARS-CoV-2 vaccine, COVID-19, food allergy, drug allergy, vaccination safety
Introduction
The COVID-19 pandemic has had a global impact, with 767,518,723 confirmed cases and 6,947,192 deaths reported worldwide as of 28 June 2023. Faced with the highly transmissible, pathogenic nature of the SARS-CoV-2 virus and a population-wide susceptibility to the virus, universal COVID-19 vaccination have emerged as the most effective strategy to manage the outbreak.1–3 Phase I–III clinical trials provided the pre-marketing evidence on the safety, immunogenicity and protective effects of a vaccine.4–8 Nevertheless, the real-world coverage of SARS-CoV-2 vaccination in general populations was not as high as expected. Among these, vaccine hesitancy was found to be responsible for it. Hence, enhancing the public’s acceptance of vaccination is imperative, with safety concerns being the primary determinant of vaccine hesitancy.9
In routine clinical work, we often encounter person come to consult on the safety of COVID-19 vaccines and most of them expressed their concern about the vaccines: “Is the vaccine appropriate for me? What are the potential adverse reactions following vaccination?”. Especially the people who have allergic diseases, such as asthma, allergic dermatitis, or have a history of food or drug allergies. Cumulative researches had focused on the safety of various COVID-19 vaccines, including the incidence and severity of adverse reactions.10–13 Our previous study found that more local and systemic reactions to inactivated SARS-CoV-2 vaccine were reported in patients with allergic disease (asthma, allergic rhinitis, allergic dermatitis) than controls.14 Overall, the inactivated SARS-CoV-2 vaccine was well tolerated and safe for these patients. Although Canadian Society of Allergy and Clinical Immunology (CSACI) provided theoretical suggestion15 that individuals with a history of allergies to food and drug can receive SARS-CoV-2 vaccine without any special precautions, actually these individuals are mostly reluctant to receive vaccination.
To the best of our knowledge, there are no study on the safety of vaccines in individuals with a history of food or drug allergies. It is imperative to establish confidence in global vaccination through the provision of safety data. Thus, the objective of this study is to investigate the safety of the inactivated SARS-CoV-2 vaccine in healthcare workers with a history of food and/or drug allergies.
Methods
Study Design and Population
The Ethics Committee of the First Affiliated Hospital of Ningbo University granted approval for our study protocol (the ethical approval number is 2021-R062-03). Our target populations were staff worked at the First Affiliated Hospital of Ningbo University. The volunteers aged 18–59 years and had received the first dose of inactivated COVID-19 vaccine developed by Sinovac or Sinopharm (Beijing) were invited to complete a questionnaire containing: (1) demographic information, namely their age, sex, comorbidities; (2) Allergic status; (3) relevant information pertaining to established Food Allergy (FA) and Drug Allergy (DA), including allergen and anaphylaxis; (4) local adverse reactions, such as pain at the injection site, redness, swelling, and pruritus, as well as systemic adverse events, including but not limited to vomiting/nausea, diarrhea, skin rash, headache, vertigo, fatigue, chills, sore throat, cough, chest tightness, palpitation of heart, new or worsened muscle pain, new or worsened joint pain, fever, somnolence, stuffy nose, abdominal pain, chest pain, and lymphadenopathy. The occurrence and grade of these adverse events were evaluated within the first week following each vaccination dose based on the FDA Center for Biologics Evaluation and Research (CBER) guidelines, and the grading scales for local and systemic events were shown in Supplement Table 1. The exclusion criteria were as follows: 1. previous SARS-CoV-2 infection; 2. Severe allergic status; 3. diagnosis of immunocompromising or immunodeficiency disorder, or receiving immunosuppressant therapy; 4. Combined with severe liver and kidney failure, tumor or uncontrolled chronic medical disorder; 5. pregnant or lactating women. Prior to participation, all subjects provided informed consent.
Vaccines
The inactivated SARS-CoV-2 vaccines referred in our study were CoronaVac (Sinovac Life Sciences, Beijing, China) and BBIBP-CorV (Sinopharm vaccine, Sinopharm, Beijing, China) which were initially used in China. Both the CoronaVac (CZ02 strain) and BBIBP-CorV (HB02 strain) were inactivated whole virus, aluminum-hydroxide-adjuvanted COVID-19 vaccines. Two-dose-schedule of the two vaccines are recommended and applied in this study.
Definitions of Food Allergy and Drug Allergy
Food and drug remain the most common elicitors of anaphylaxis. The diagnosis of anaphylaxis is still based on the clinical evaluation, of course, laboratory examine, such as serum allergen-sIgE is conducive to diagnosis. Food Allergy and Drug Allergy means food and drug-induced anaphylactic reactions. After exposure to a likely allergen (food or drug), clinical symptoms occurred with involvement of the skin, mucosal tissue, respiratory compromise, cardiovascular associated symptoms or persistent gastrointestinal symptoms according to EAACI (European Academy of Allergy and Clinical Immunology) anaphylaxis guidelines.16
Statistical Analysis
The numerical and percentage representations were utilized to present the categorical variables. The statistical analysis was conducted using the SPSS 25.0 software. Continuous variables were expressed as mean (standard deviation). All data were graphically performed using GraphPad Prism (v 6.1 GraphPad Software, Inc., San Diego, CA, USA).
Results
Participants Characteristics
Our study comprised 150 employees aged 18–59 years who had reported food and/or drug allergy and had received the first dose of inactivated COVID-19 vaccine in the above institution. Of the participants, 50 participants have FA, 91 participants have DA and 9 possess a history of both food and drug allergies. Subsequently, a routine follow-up was carried out, resulting in three participants (one with both food and drug allergies, two with only drug allergy) declining to receive the second dose without providing a reason. The summary of participants’ demographic characteristics, comorbidities and allergy information is provided in Table 1. In the study, seafood and fruits are the leading eliciting allergens in FA. Drug-induced anaphylaxis is mainly caused by antibiotics, especially the beta-lactam antibiotics (Penicillin, Cephalosporin).
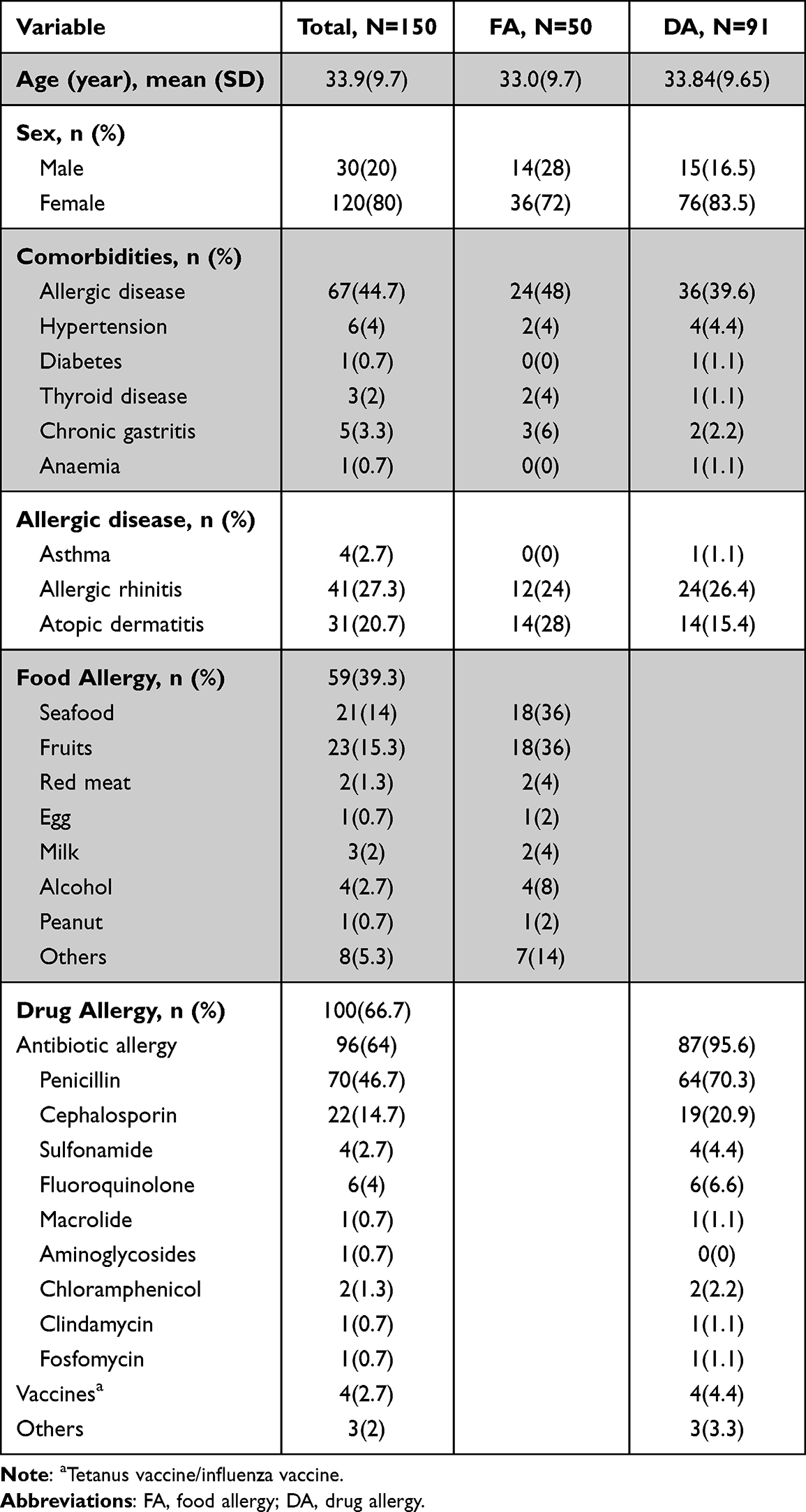 |
Table 1 Baseline Characteristics of the Participants |
Adverse Reactions
The findings of our study indicated that the vast majority of participants did not experience any significant local or systemic adverse reactions, and hospitalization was not required for any of them. Table 2 showed the local and systemic adverse reactions occurred after first and second doses of inactivated SARS-CoV-2 vaccines administration among these participants. Analysis of Table 2 revealed that pain at the injection site was the most prevalent local adverse event, accounting for 30% of the total, followed by local swelling (2%), local redness (1.3%), and pruritus (0.7%) after the initial vaccination. Additionally, 34.7% of the participants reported systemic events, with fatigue being the most commonly reported symptom (16%). The following adverse effects were observed: vertigo (7.3%), diarrhea (6%), sore throat (6%), cough (5.3%), muscle pain (4.7%), skin rash (4.7%), headache (4%), fever (2.7%), vomiting/nausea (2.7%), chills (2%), stuffy nose (2%), abdominal pain (0.7%), joint pain (0.7%), and lymphadenopathy (0.7%). Notably, other discomforts such as chest tightness, chest pain, and cardiopalmus were not reported. Upon analysis, it was observed that the frequency of both local and systemic adverse events exhibited a decline subsequent to the second vaccination, as depicted in Figure 1. A significant proportion of participants, ie, 58.5%, remained unaffected by any adverse reactions. Pain at the injection site continued to be the most frequently reported local adverse reaction, accounting for 22.4% of cases. Systemic reactions were reported by only 25.2% of participants, with fatigue being the most commonly reported symptom (13.6%). The incidence of other symptoms, such as vertigo, headache, sore throat, cough, and others was also lower than that observed after the first vaccination. For further investigation, we performed a comparable analysis on two distinct subgroups, namely FA and DA (Table 2, Figures 2 and 3). And in subgroup exploration, the 9 participants who have both food and drug allergic experience were excluded for academic rigour. Our findings demonstrated that the incidence of adverse reactions in FA group and DA group are 46% and 58%, respectively. Within the FA group, 24% of participants experienced local reactions, while 28% experienced systemic discomforts. The most commonly reported local and systemic reactions were pain at the injection site (22%) and fatigue (14%), respectively. In the DA group, the most commonly reported local reaction was also the pain at the injection site (29.7%), while fatigue (14.3%) was the most frequently reported systemic event. Furthermore, a decrease in the incidence of adverse events was observed after the second dose of inactivated vaccine in comparison to the first dose. In addition, the aforementioned adverse reactions in our study are of mild or moderate severity and are well tolerated, without necessitating hospitalization or specialized medical intervention. Table 2 provided further details regarding the occurrence of other adverse reactions.
 |
Table 2 Adverse Reactions Following Vaccination in Patients with Food and/or Drug Allergies |
 |
Figure 1 Local and systemic reactions after receiving the inactivated COVID-19 vaccine in the participants with food and/or drug allergies. |
 |
Figure 2 Local and systemic reactions after receiving the inactivated COVID-19 vaccine in the participants with food allergy. |
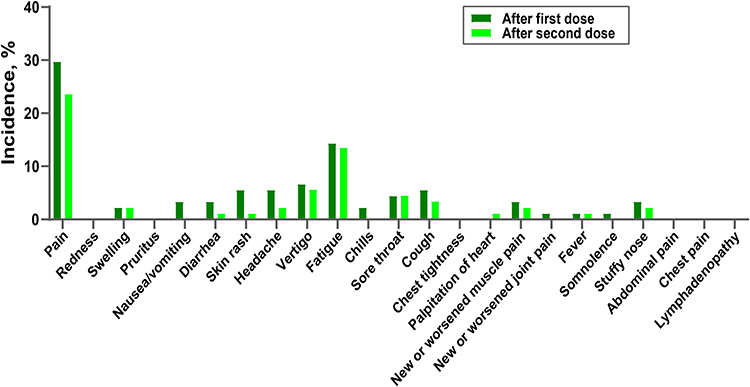 |
Figure 3 Local and systemic reactions after receiving the inactivated COVID-19 vaccine in the participants with drug allergy. |
Discussion
In our survey, a total of 150 hospital staff members with a documented history of food or drug allergy were enrolled to investigate the incidence of local and systemic adverse reactions following the first and second doses of the vaccine. Following the initial vaccination, 56% of the participants had adverse effects, the most prevalent local adverse reaction was pain at the injection site (30%), while systemic events were reported by 34.7% of the participants, with fatigue being the most frequently reported symptom (16%). Following the second vaccination, the frequency of both local and systemic adverse reactions exhibited a decline. Notably, the most prevalent local discomfort was pain at the injection site, affecting 22.4% of the population. Systemic adverse events were reported by 25.2% of the participants, with fatigue being the most commonly reported symptom, affecting 13.6% of the population. Further analysis of the adverse reactions in FA and DA groups indicate that the prevailing local and systemic adverse effects observed in the FA group were in line with those of the DA group, namely injection site pain and fatigue. Furthermore, these adverse effects were mitigated after the second vaccination in comparison to the first, as anticipated. The incidence rate of adverse events displayed in our research did not exceed the range reported in phase III clinical trials of the two vaccines.6–8
One clinical trial of CoronaVac6 showed that the rate of adverse events after first and second dose vaccination were 65.5% and 60.1% in respective. Either after the first vaccination or the second vaccination, the incidence of pain at the injection site was the highest (44.4%, 46%) among the local adverse reactions, and the incidence of systemic adverse reactions, which were mainly the headache (31.4%, 24.7%) and fatigue (13.9%, 9.1%). In the clinical trial of Sinopharm vaccine,7 only 24.4% of the subjects had no adverse reactions. After first vaccination, the incidence of pain at the injection site (44.8%) and Fatigue (12.2%) had been the top one symptom among local and systemic adverse reactions, respectively. And after the second vaccination, 86% of the participants had adverse reactions, among which the incidence of pain and fatigue were 47.6% and 16.3%. In addition, the aforementioned adverse reactions in our study are of mild or moderate severity and are well tolerated, without necessitating hospitalization or specialized medical intervention. Our study suggests that individuals with pre-existing food and/or drug allergies exhibit a favorable safety profile in the context of inactivated SARS-CoV-2 vaccination, which is in line with our recent clinical report on the safety of said vaccination in those with allergic conditions.
As a single-arm trial, the inadequacy is mainly the subjects in our study and the external control group are not from the same subject population. And, it is imperative to acknowledge the potential presence of recall bias and the limited sample size, which require further validation. It is noteworthy that the screening criterion of the subjects in these clinical trials mentioned above were healthy participants or history of anaphylaxis was listed as the main exclusion criterion factors; Moreover, the participants enrolled in our study are healthcare professionals, which enhances the credibility of this empirical investigation.
Currently, there are 199 vaccines undergoing preclinical trials and 180 vaccines that have received approval for clinical development. When examining the neutralization capabilities of vaccines, it is important to prioritize vaccine safety. Given that COVID-19 vaccination is an essential preventative measure, it is crucial to conduct extensive and practical investigations on the safety of diverse vaccine types across various demographic groups. Such studies are necessary for the future.
Conclusion
Amidst the unparalleled COVID-19 pandemic, the primary means of safeguarding against infection continues to be the administration of an effective vaccine. However, apprehensions regarding the safety of vaccines have emerged. Our research demonstrates that individuals with a prior history of food or drug allergy exhibit an acceptable level of tolerance towards the inactivated SARS-CoV-2 vaccine. To confirm the safety of COVID-19 vaccines and convince people to receive vaccination, further large-scale real-world studies in various populations are in urgent need.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Medicine, the First Affiliated Hospital of Ningbo University. All participants signed informed consent in accordance with the Declaration of Helsinki.
Author Contributions
All authors made substantial contributions to conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
No source of funding and support.
Disclosure
The authors declare no conflict of interest in relation to this work.
References
1. McNamara LA, Wiegand RE, Burke RM, et al. Estimating the early impact of the US COVID-19 vaccination programme on COVID-19 cases, emergency department visits, hospital admissions, and deaths among adults aged 65 years and older: an ecological analysis of national surveillance data. Lancet. 2022;399(10320):152–160. doi:10.1016/S0140-6736(21)02226-1
2. Nordstrom P, Ballin M, Nordstrom A. Risk of infection, hospitalisation, and death up to 9 months after a second dose of COVID-19 vaccine: a retrospective, total population cohort study in Sweden. Lancet. 2022;399(10327):814–823. doi:10.1016/S0140-6736(22)00089-7
3. Li M, Wang H, Tian L, et al. COVID-19 vaccine development: milestones, lessons and prospects. Signal Transduct Target Ther. 2022;7(1):146. doi:10.1038/s41392-022-00996-y
4. Han B, Song Y, Li C, et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (CoronaVac) in healthy children and adolescents: a double-blind, randomised, controlled, Phase 1/2 clinical trial. Lancet Infect Dis. 2021;21(12):1645–1653. doi:10.1016/S1473-3099(21)00319-4
5. Xia S, Zhang Y, Wang Y, et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: a randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect Dis. 2021;21(1):39–51. doi:10.1016/S1473-3099(20)30831-8
6. Palacios R, Patiño EG, de Oliveira Piorelli R, et al. Double-blind, randomized, placebo-controlled phase iii clinical trial to evaluate the efficacy and safety of treating healthcare professionals with the adsorbed COVID-19 (Inactivated) vaccine manufactured by Sinovac - PROFISCOV: a structured summary of a study protocol for a randomised controlled trial. Trials. 2020;21(1):853. doi:10.1186/s13063-020-04775-4
7. Saeed BQ, Al-Shahrabi R, Alhaj SS, Alkokhardi ZM, Adrees AO. Side effects and perceptions following Sinopharm COVID-19 vaccination. Int J Infect Dis. 2021;111:219–226. doi:10.1016/j.ijid.2021.08.013
8. Tanriover MD, Doğanay HL, Akova M, et al. Efficacy and safety of an inactivated whole-virion SARS-CoV-2 vaccine (CoronaVac): interim results of a double-blind, randomised, placebo-controlled, Phase 3 trial in Turkey. Lancet. 2021;398(10296):213–222. doi:10.1016/S0140-6736(21)01429-X
9. Chen M, Li Y, Chen J, et al. An online survey of the attitude and willingness of Chinese adults to receive COVID-19 vaccination. Hum Vaccin Immunother. 2021;17(7):2279–2288. doi:10.1080/21645515.2020.1853449
10. Benjamanukul S, Traiyan S, Yorsaeng R, et al. Safety and immunogenicity of inactivated COVID-19 vaccine in health care workers. J Med Virol. 2022;94(4):1442–1449. doi:10.1002/jmv.27458
11. Zhang M-X, Zhang T-T, Shi G-F, et al. Safety of an inactivated SARS-CoV-2 vaccine among healthcare workers in China. Expert Rev Vaccines. 2021;20(7):891–898. doi:10.1080/14760584.2021.1925112
12. Choudhary OP, Mohammed TA, Singh I, Singh I. Intranasal COVID-19 vaccines: is it a boon or bane? Int J Surg. 2021;94:106119. doi:10.1016/j.ijsu.2021.106119
13. Choudhary OP, Choudhary OP. Vaccine efficacy against COVID-19: a foresight on the host-associated factors. J Formos Med Assoc. 2021;120(6):1405–1407. doi:10.1016/j.jfma.2020.11.021
14. Cao C, Qiu F, Lou C, et al. Safety of inactivated SARS-CoV-2 vaccines in patients with allergic diseases. Respir Res. 2022;23(1):133. doi:10.1186/s12931-022-02054-1
15. Vander Leek TK, Chan ES, Connors L, et al. COVID-19 vaccine testing & administration guidance for allergists/immunologists from the Canadian Society of Allergy and Clinical Immunology (CSACI). Allergy Asthma Clin Immunol. 2021;17(1):29. doi:10.1186/s13223-021-00529-2
16. Muraro A, Worm M, Alviani C, et al. EAACI guidelines: anaphylaxis (2021 update). Allergy. 2022;77(2):357–377. doi:10.1111/all.15032
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.