Back to Journals » Clinical Ophthalmology » Volume 17
Safety and Tolerability of Bilastine 0.6% Ophthalmic Solution: An 8-Weeks Phase III Study
Authors Kuna P ![]() , Jutel M, Pulka G, Tokarski S, Arranz P, Hernández G, Fernández Hernando N
, Jutel M, Pulka G, Tokarski S, Arranz P, Hernández G, Fernández Hernando N ![]()
Received 18 November 2022
Accepted for publication 9 February 2023
Published 4 March 2023 Volume 2023:17 Pages 735—746
DOI https://doi.org/10.2147/OPTH.S398168
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Piotr Kuna,1 Marek Jutel,2,3 Grazyna Pulka,4 Slawomir Tokarski,5 Paula Arranz,6 Gonzalo Hernández,6 Nieves Fernández Hernando6
1Department of Internal Medicine, Asthma and Allergy, Medical University of Lodz, Lodz, Poland; 2Department of Clinical Immunology, Wroclaw Medical University, Wrocław, Poland; 3All-Med Medical Research Institute, Wrocław, Poland; 4Centrum Medyczne All-Med, Krakòw, Poland; 5Institute of Medical Sciences, Medical College of Rzeszow University, Rzeszow, Poland; 6Department of Research, Development and Innovation, FAES FARMA, Leioa, Bizkaia, Spain
Correspondence: Nieves Fernández Hernando, FAES FARMA, S.A, Av. Autonomía 10, Leioa, Bizkaia, 48940, Spain, Tel +34 94 481 83 00, Email [email protected]
Purpose: The objective of this study was to assess the safety and tolerability of preservative-free bilastine 0.6% ophthalmic solution after 8 weeks of once-daily administration in patients with allergic conjunctivitis (AC).
Patients and Methods: Multi-center, international, randomized, double blind, placebo-controlled, parallel-group, phase III study of adult patients with seasonal or perennial AC. The study was conducted in 26 centers of 5 European countries. Duration of daily treatment with bilastine 0.6% ophthalmic solution or placebo was 8 weeks. Safety was evaluated by analyzing incidence of ocular treatment-emergent adverse events (TEAEs); additionally, and as secondary parameters, ocular tolerability was assessed, in addition efficacy was also assessed by the average daily total eye symptoms score (TESS).
Results: A total of 333 randomized patients with AC were included (bilastine, N=218; placebo, N=115). Mean (SD) age of the patients was 39.9 (13.7) and were 63.7% female. Overall, the percentage of ocular related TEAEs was low, and the percentage of patients with ocular related TEAEs was lower in the bilastine ophthalmic solution group (2.8%) than in the placebo group (4.3%). No severe TEAEs were reported. The ocular symptoms and TESS improved during the trial in both treatment groups. Statistically significant treatment differences were observed at Week 8 for the TESS and all individual ocular symptoms, being significantly better in the bilastine ophthalmic solution group than in placebo group.
Conclusion: Bilastine 0.6% ophthalmic solution revealed no safety concerns in patients with AC after 8 weeks of once-daily administration. Bilastine was effective in reducing ocular symptoms associated with AC in response to both seasonal and perennial allergens.
Keywords: H1-antihistamine, bilastine, safety, allergic conjunctivitis, ocular allergy, ophthalmic solution
Introduction
Allergic conjunctivitis (AC) is an inflammatory process resulting from direct contact of the allergen with the eye conjunctival surface in sensitized patients.1 It is fundamentally caused by an immunoglobulin E (IgE)-mediated immune mechanism or a hypersensitivity mechanism. AC is multifactorial and consists of both, an early acute phase triggered by mast cell degranulation and release of histamine and a late phase involving various pro-inflammatory mediators.2 Following antigen exposure, conjunctival mast cells degranulate and release newly formed and pre-existing inflammatory mediators.3 Histamine is the primary preformed mediator responsible for the typical early phase reaction that triggers itching, vasodilation, and vascular leak leading to ocular redness, chemosis, and blepharitis. These symptoms can be suppressed by blocking the H1 receptor.4,5 The management of AC includes non-pharmacological treatments, such as lacrimal substitutes and protection of the ocular surface. A standard treatment of AC consists of eye drops containing antihistamines, preferably without additives.6–10 The use of allergen immunotherapy can be recommended in severe cases.11
Bilastine is a second-generation non-sedating H1-antihistamine. Oral bilastine was approved in the EU in 2010 (Ilaxen; FAES Farma SA, Spain) for the symptomatic treatment of seasonal or perennial allergic rhinoconjunctivitis and urticaria in patients aged 12 years or older (at a dose of 20 mg daily) and, more recently, for use in children between 6 and 11 years (with a body weight of at least 20 kg, at dose of 10 mg daily).12,13 The safety of oral bilastine was extensively characterized during the clinical trial development, which suggested an excellent safety profile.13–15 Several studies have demonstrated the long-term (up to one year) safety use of oral bilastine.16,17 Oral bilastine has also been tested in children from 2 to 11 years, adolescents, and in elderly patients, and these studies have shown a safety profile similar to that in adults.
If ocular symptoms prevail, topical antihistamines are usually preferred to oral antihistamines because of their faster onset of action and effectiveness together with their lower incidence of side effects.13 For these reasons, and because of the demonstrated efficacy and safety of oral bilastine, a once-daily, preservative-free, ophthalmic formulation to treat AC locally has been developed. Pharmacokinetic studies of the ophthalmic formulation showed that bilastine is distributed predominantly in the intended target tissue, the conjunctiva, and is poorly absorbed in the blood stream.18,19 A Phase II study showed that the ophthalmic bilastine at a concentration of 0.6% was effective up to 16 hours post-treatment, making it suitable for once-daily administration.20 The new formulation was safe and well tolerated.
Since prior studies evaluated ophthalmic 0.6% bilastine administration in a short period of time, here we report the results of a study designed to assess the safety of this drug in adults with AC for up to 8 weeks of continuous administration. To avoid potential bias, a multi-center, randomized, double blind, placebo controlled, and parallel study design was chosen. The primary endpoint was safety, but ocular tolerability and potential discomfort of ophthalmic bilastine, and its efficacy in reducing AC symptoms were also assessed.
Materials and Methods
This was a multi-center, international, randomized, double blind, placebo-controlled, parallel-group, phase III study to assess the safety, tolerability and efficacy of bilastine 0.6% ophthalmic solution in adult patients with a documented history of seasonal or perennial AC. The trial was conducted in 3 centers in Hungary, 5 in Lithuania, 7 in Poland, 6 in Slovakia, and 5 in Ukraine from June to December of 2019. The protocol as well as information provided to patients were approved by Independent Ethics Committees prior to each center’s initiation (See Table S1). Written informed consent was received from all patients prior to enrolment into the trial, which was conducted in accordance with the Declaration of Helsinki and all local regulations. The trial was registered with EudraCT number 2018–002248-95.
Procedures
See Table S2 for a detailed schedule of trial procedures. At screening (Visits 1a and 1b), after giving informed consent, the patients were checked for eligibility and the use of the patient diary was explained. At Visit 2a, after eligibility had been confirmed, baseline examinations and randomization were performed. Bilastine 0.6% or placebo was dispensed, and the first dose was instilled on-site. At Visit 3a (Week 4) and Visit 4a (Week 8), bilastine was instilled on-site. The patient rated the tolerability and potential discomfort, and the investigator checked the patient diary (e-diary). Ophthalmologic examinations were performed at Visit 1b (up to 2 days after the first screening visit) and at Visit 4b (up to 2 days after Visit 4a) at a separate site, as applicable. In addition, safety and tolerability of bilastine or placebo in terms of adverse events (AEs) and concomitant medication was also assessed via phone calls after 2 weeks (Visit 2b) and after 6 weeks (Visit 3b) of treatment. At Visit 5, the patient was called by phone for a safety follow-up. During the trial, exposure to environmental allergic factors were verified by patient interview.
Patient Population
Included patients were aged ≥18 years with a documented history of AC, a documented positive skin prick test and/or positive validated IgE test to perennial allergen (eg cat dander, dog dander, dust mites and/or cockroach) or to seasonal allergen (eg grass, ragweed, and/ or tree pollen) within 6 months before the study, or a positive skin prick test at Visit 1a and showing signs and symptoms of AC, ie tearing, itching and redness, that were likely to continue for the next weeks. The patients had to have a minimum score of 4 on a 0–10 numeric rating scale (0, no symptom; 10, very severe symptom) in at least one of three categories (ocular itching, ocular redness, and ocular tearing). The main exclusion criteria were a history of known contraindications or sensitivities to the use of the drug or any of its components; intraocular surgery or planned surgery during study participation and within 2 weeks after follow-up; ocular trauma in the 6 months before the study; clinical evidence of ocular herpes simplex or ocular herpes zoster infectious disease; or any clinically significant (CS) external ocular disease within 30 days before study start.
Treatment
Bilastine 0.6% ophthalmic solution (6 mg/mL) was presented in sterile, preserved solution in ampoules for single use (FAES FARMA S.A., Leioa, Spain). Placebo was the vehicle, with same presentation. Bilastine ophthalmic solution and placebo were identical in color and appearance. The packaging and labelling did not allow for any distinction between test and reference drug. One drop of bilastine or placebo was instilled in each eye once daily in the morning (one ampoule for both eyes). On the days of Visit 2a, Visit 3a and Visit 4a, this was done by a medically qualified person onsite. On the other days, the patient administered one drop in each eye once daily. The duration of treatment for the individual patient was 56 days. The complete study duration (including screening and follow-up) was 70 days. Each patient had to document daily the administration of the ophthalmic solutions in an e-diary.
Prior and concomitant treatment with the following medication and therapies was prohibited: anti-allergy immunotherapy, corticosteroid treatment, depot-corticosteroids, any ophthalmic agents (including artificial tears), systemic or intranasal treatment for allergic rhinitis (ie, antihistamines, mast cell stabilizers, or leukotriene inhibitors).
Endpoints and Assessments
The primary objective was to assess the safety of bilastine once-daily ophthalmic solution 0.6% during long-term use, as measured by the incidence of related treatment-emergent ocular adverse events (ocular r-TEAEs). An adverse event (AE) was defined as any unfavorable and unintended sign (including an abnormal laboratory finding), symptom, or disease temporally associated with the use of the product, whether or not considered related to the product. An event that emerged during treatment with bilastine or placebo having been absent prior to treatment, or worsened relative to the pre-treatment state, was defined as a TEAE. All AEs with onset or worsening after first intake of bilastine or placebo until 7 days after last intake of bilastine or placebo were defined as TEAEs.
The secondary objectives of this trial were: (1) to assess the ocular tolerability and potential discomfort of bilastine ophthalmic solution 0.6% during long-term use; and (2) to assess the efficacy of bilastine ophthalmic solution 0.6%. Peak ocular discomfort was assessed for each eye on an integer scale of 0 to 10, where 0 represents no symptoms and 10 represents severe discomfort. Ocular tolerability (burning, stinging, tearing, blurring, and stickiness) was assessed separately for each eye by the patient 3 minutes after drop instillation (Visits 2a, 3a and 4a) on an 11-item numeric rating scale (from 0 to 10), where 0 represents no symptoms and 10 represents unbearable burning or stinging, excessive and continuous tearing or very severe blurring or stickiness. The eye with the worse results was summarized at each visit.
Ophthalmologic assessments, carried out by specialists, included best-corrected visual acuity assessed using an Early Treatment Diabetic Retinopathy Study (ETDRS) chart; slit-lamp biomicroscopy in both eyes to exclude patients with disallowed ocular conditions; intraocular pressure in both eyes measured with a tonometer; and a dilated fundus examination.
The efficacy assessments were exploratory, as that the trial was neither designed not powered to demonstrate efficacy. Efficacy was assessed by evaluation of ocular symptoms over the course of the trial period. The efficacy assessment criteria included the verification of environmental allergic factors (evaluated with a patient interview), ocular symptoms, and signs (ocular itching, redness and tearing on an 11-item numeric rating scale). Starting with Visit 1a and ending with Visit 4a, trial patients completed an electronic diary (e-diary), documenting the severity of symptoms associated with AC. The ocular symptoms itching, redness and tearing were assessed daily for each eye on an 11-item numeric rating scale (0 to 10). A value of “10” presented maximum symptom severity (unbearable itching, very severe redness or excessive and continuous tearing) and a value of “0” the absence of the respective symptom. Diary data were pooled into baseline and treatment weeks. For each parameter, the average value was calculated for each week, and was used to calculate relative and absolute changes from the baseline week.
The total eye symptoms score (TESS) was defined as the sum of the ocular itching, redness and tearing scores. The average daily TESS at each week over the 8-week treatment period and overall was analyzed using mixed models for repeated measures (MMRM) with the fixed effects of treatment, week, treatment by week interaction, indication (PAC or SAC), country and baseline score as a covariate. Restricted maximum likelihood (REML) was employed in fitting the model. The LS means associated with treatments and treatment differences were presented overall and at each treatment week with 95% confidence intervals and corresponding p-values.
Statistical Analysis
A total of 300 randomized patients with AC were to be included in this trial. Patients were randomized 2:1 to bilastine: placebo (stratified by indication [SAC/PAC]). Assuming a maximum incidence of ocular TEAEs of 15%, and a sample size of 200 patients in the bilastine group, a two-sided 95% confidence interval for a single proportion using the large sample normal approximation was extended as maximum 4.95% from the observed proportion. Randomization was generated using the validated software Statistical Analysis System® (SAS®), Version 9.4.
All TEAEs were summarized by calculating the number of events and the number and percent of patients with TEAEs by preferred term and primary system organ class for each treatment arm. Also, TEAEs were summarized by severity, seriousness, and relationship to each treatment arm. Number and percent of TEAEs leading to trial termination were scored for each treatment arm. Continuous variables were summarized in terms of descriptive statistics including number of observations, mean, standard deviation, median, minimum, maximum and quartiles. Categorical variables were summarized in terms of frequencies and percentages. Where data were collected over time, both the observed data and the change from baseline were summarized at each time point. All statistical analyses used SAS for Windows (SAS Institute Inc., Cary, NC, USA) version 9.4.
Results
A total of 333 patients were randomized, 218 patients to the bilastine ophthalmic solution and 115 patients to placebo (Figure 1). Of these, 96.8% patients in the bilastine group and 94.8% in the placebo group completed the trial. The mean (SD) age of the patients was 39.0 (13.7) years and ranged from 18 to 81 years with similar age ranges and mean ages in both treatment groups (Table 1). Most patients were female (63.7%). Allergy baseline characteristics including the type of allergic conjunctivitis (SAC/PAC) and allergens are listed in Table 1. The number of patients with a history of PAC (122, 36.6%) was lower than the number of patients with a history of SAC (211, 63.4%). Concomitant allergic rhinitis was present in 53.5% of patients, and asthma in 22.2%. The prior medications reported by the patients included various systemic and ophthalmic antihistamines and nasal preparations (fluticasone, mometasone) for the treatment of allergic symptoms.
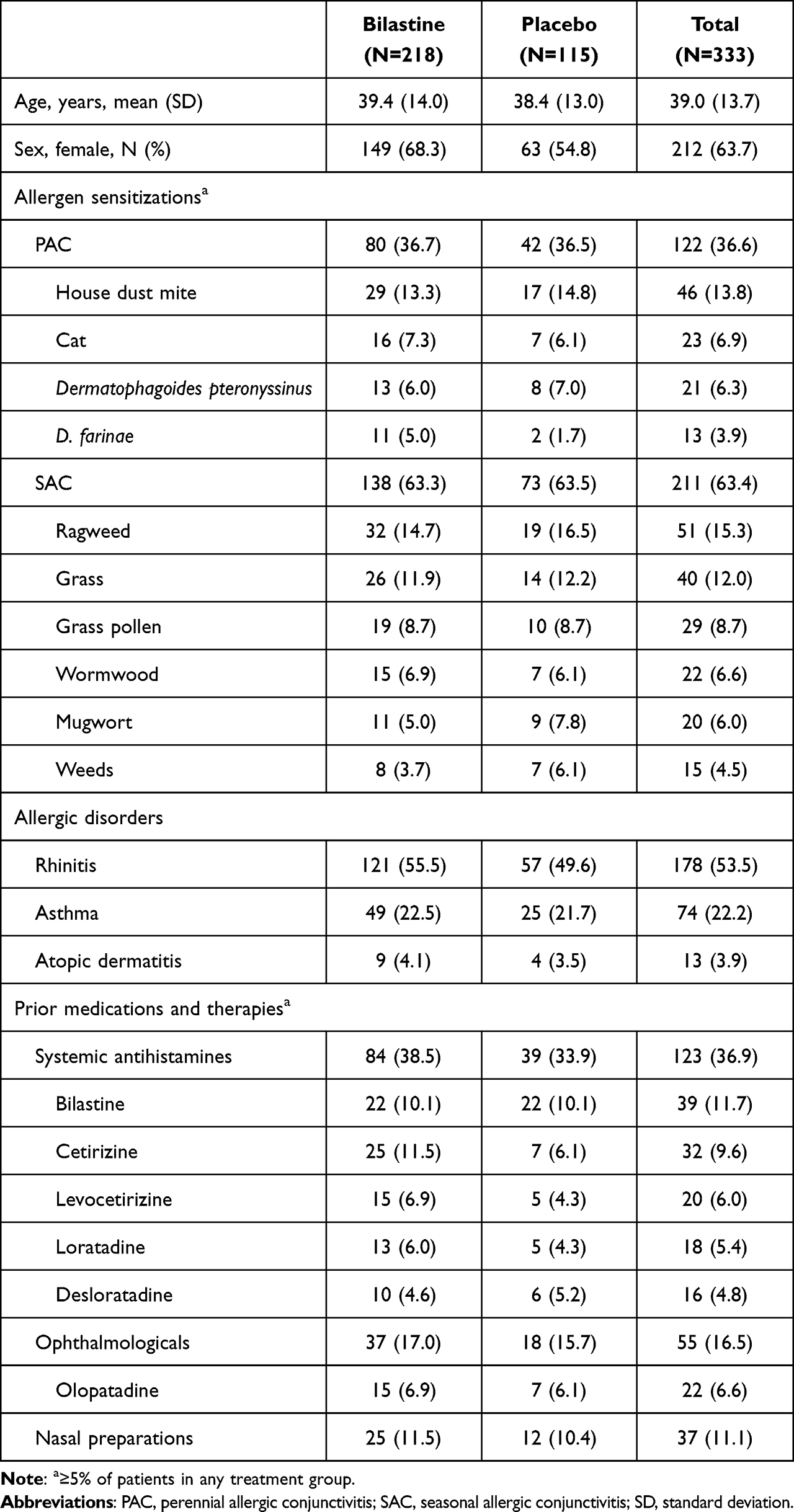 |
Table 1 Baseline Characteristics of the Patients |
 |
Figure 1 Patient disposition (safety population). Abbreviations: PAC, perennial allergic conjunctivitis; SAC, seasonal allergic conjunctivitis. |
The adherence to the treatment was very high, with a mean (SD) of 100.6% (5.9) and 94.5% (11.3) based on drug accountability (dispensed and returned ampoules) or on the number of administrations (during on-site visits and according to e-diary records), respectively, and was very similar between the groups.
Safety
An overall summary of TEAEs including patients with ocular TEAEs and ocular r-TEAEs is presented in Table 2. A total of 46 (13.8%) patients reported 62 TEAEs during the course of the trial: 28 (12.8%) patients with 40 TEAEs in the bilastine group and 18 (15.7%) patients with 22 TEAEs in the placebo group. All TEAEs were classified as mild or moderate. No severe TEAEs were reported.
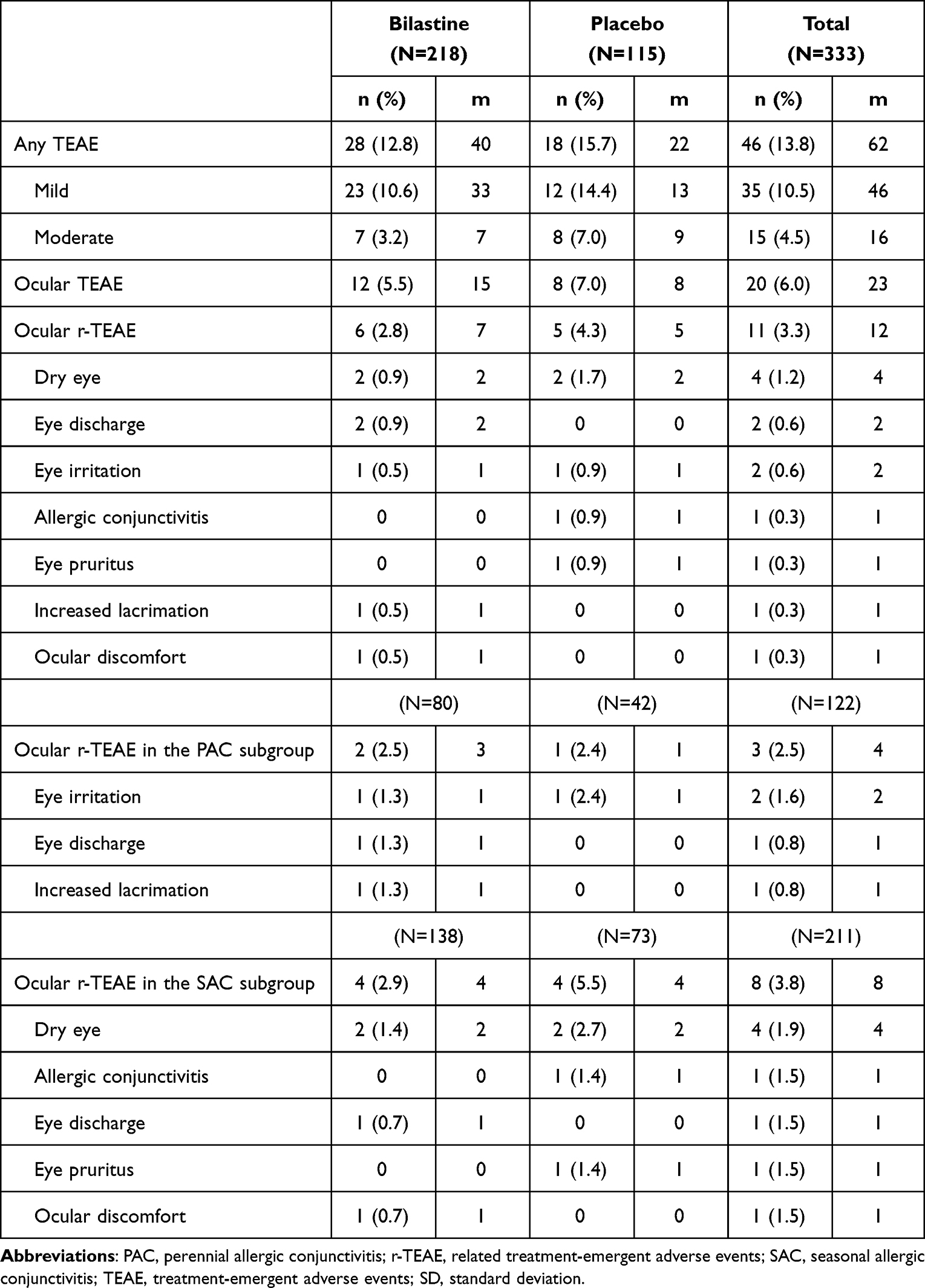 |
Table 2 Ocular TEAEs |
Overall, 11 (3.3%) patients reported 12 ocular r-TEAEs, 6 (2.8%) patients in the bilastine group (7 events) and 5 (4.3%) patients in the placebo group (5 events). A total of 2 ocular r-TEAEs experienced by 2 (0.6%) patients including one patient in each treatment group led to discontinuation of the trial. One (0.3%) patient in the placebo group experienced one ocular related-TEAE that required treatment with medication. Dry eye (4 patients, 1.2%), eye discharge (2 patients, 0.6%) and eye irritation (2 patients, 0.6%) were the most frequent total ocular r-TEAEs, with similar percentages in both treatment groups (Table 2). No frequency differences of more than 1% of patients between the treatment groups were observed for any individual ocular r-TEAE.
The exposure-adjusted incidence rates were low in both treatment groups. They ranged between 0 and 0.05 events (dry eye and eye discharge) per 1 patient year in the bilastine ophthalmic solution group and between 0 and 0.10 events (dry eye) per 1 patient year in the placebo group. Similar incidence rates were observed in both treatment groups with regard to individual ocular r-TEAEs.
Tolerability
The peak ocular discomfort score was assessed at baseline and at Week 8 for both groups (Figure 2A). At baseline, most patients (>80%) reported no or only slight discomfort (scores 0, 1 and 2) at all timepoints in both treatment groups. At endpoint, most patients reported no or only slight discomfort (scores 0, 1 and 2) in both treatment groups, (bilastine 0.6% and placebo) and the percentage of these patients increased compared to baseline.
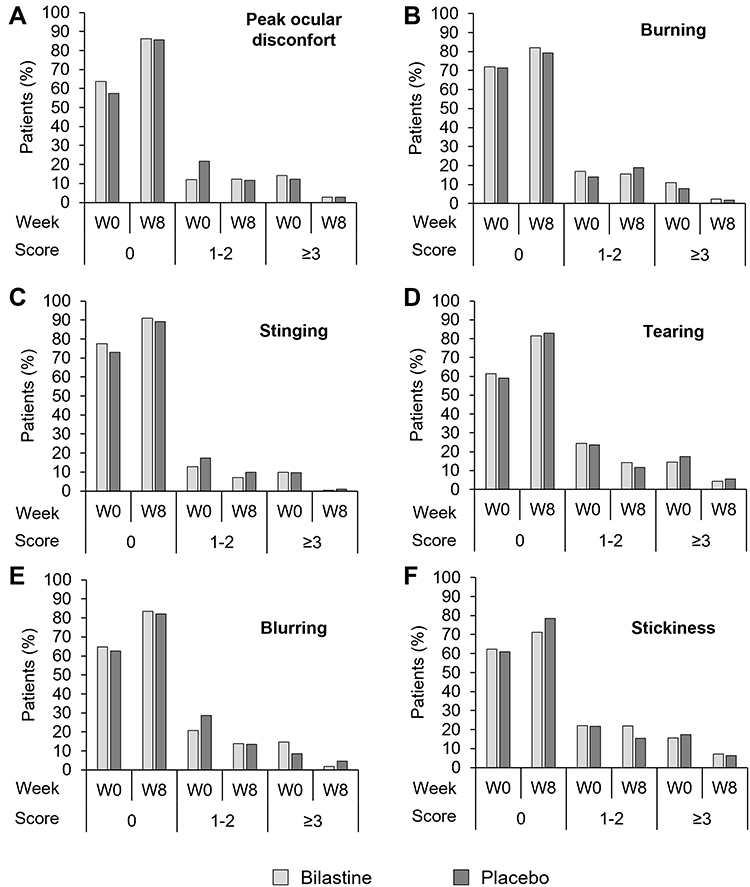 |
Figure 2 Peak ocular discomfort and ocular tolerability for the bilastine and placebo groups at baseline (Week 0) and Week 8. Peak ocular discomfort was assessed for each eye on an integer scale of 0 to 10, where 0 represents no symptoms and 10 represents severe discomfort. Ocular symptoms were similarly rated on an integer scale of 0 to 10, where 0 represents no symptoms and 10 represents unbearable burning or stinging, excessive and continuous tearing or very severe blurring or stickiness. (A) Peak ocular discomfort; (B) burning; (C) stinging; (D) tearing; (E) blurring; (F) stickiness. |
At baseline, after the first administration of the study drug, most patients reported no or only slight symptoms of ocular burning, stinging, tearing, blurring or stickiness (scores 0, 1 and 2) in both treatment groups including ranges between 84.4% (stickiness) and 90.3% (stinging) in the bilastine ophthalmic solution group and between 82.6% (stickiness and tearing) and 92.2% (burning) in the placebo group (Figure 2B-F). No patients reported unbearable burning or stinging, excessive and continuous tearing or very severe blurring or stickiness (scores 9 and 10) in both treatment groups except for single patient in the placebo group. At endpoint, most patients reported no or only symptoms of slight ocular burning, stinging, tearing, blurring or stickiness (scores 0, 1 and 2) in both treatment groups compared to baseline.
Efficacy
TESS and ocular symptoms improved during the trial in both treatment groups (Figure 3). Statistically significant treatment differences were observed at Week 8 for the TESS and all individual ocular symptoms. The patients in the bilastine group consistently had lower symptom scores and a lower TESS than patients in the placebo group across the symptoms. In the PAC subgroup, no statistically significant TESS treatment differences were reported, which can be explained by the low number of patients in this group. However, in the SAC subgroup, statistically significant treatment differences in favor of the bilastine ophthalmic solution group were observed in Week 8.
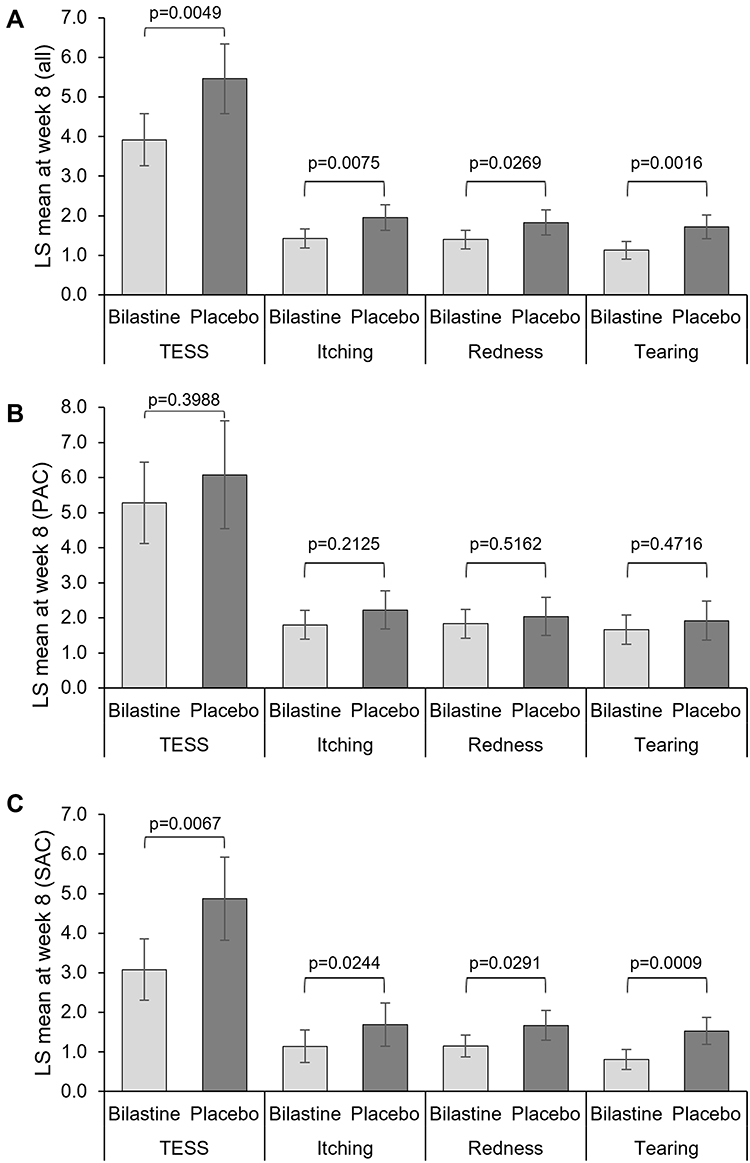 |
Figure 3 Eye symptoms scores (TESS and ocular symptoms) at week 8. (A) Total population (Bilastine, N=194; Placebo, N=107); (B) PAC population (Bilastine, N=69; Placebo, N=40); (C) SAC population (Bilastine, N=125; Placebo, N=67). Error bars represent 95% confidence interval. A value of “10” presented maximum symptom severity and a value of “0” the absence of the respective symptom. Abbreviations: PAC, perennial allergic conjunctivitis; SAC, seasonal allergic conjunctivitis; TESS, total eye symptom score. |
Discussion
In this study the safety, tolerability, and efficacy of bilastine 0.6% ophthalmic formulation administered for a period 8 weeks was evaluated. Overall, the percentage of ocular r-TEAEs was low and the percentage of patients with ocular r-TEAEs was lower in the bilastine ophthalmic solution group (2.8%) than in the placebo group (4.3%). In general, dry eye, eye discharge and eye irritation were the ocular r-TEAEs reported in more than one patient in the study. All TEAEs were classified as mild or moderate. No severe TEAEs were reported. Further, bilastine ophthalmic solution revealed no safety concerns as evaluated by TEAEs, laboratory parameters, visual acuity, slit-lamp biomicroscopy findings, intraocular pressure, dilated fundus examination, peak ocular discomfort and ocular tolerability. Regarding efficacy in improving AC ocular symptoms, the TESS improved during the course of the trial in both treatment groups. Statistically significant treatment differences were observed at Week 8 for the TESS and all individual ocular symptoms.
The efficacy and safety of bilastine ophthalmic solution was evaluated in a recently published clinical trial.20 In this double-masked, randomized, vehicle-controlled Phase 2 dose ranging study with bilastine ophthalmic solution 0.2%, 0.4%, and 0.6% in adult patients with allergic conjunctivitis (N=121), bilastine 0.6% demonstrated efficacy for ocular itching (primary endpoint) at 15 minutes, 8 hours, and 16 hours post-treatment. No ocular TEAEs were reported for bilastine ophthalmic solution 0.6%. Only one (3.2%) mild unrelated non-ocular TEAE (hypoaesthesia) was reported which led to trial discontinuation.20 In a second clinical trial, still unpublished, the efficacy of ophthalmic bilastine 0.6% was evaluated against ketotifen 0.025% ophthalmic solution and vehicle (ClinicalTrials.gov identifier: NCT03479307). Again, ophthalmic bilastine was safe and well tolerated. Mean drop comfort scores were significantly better (p<0.05) for bilastine compared with ketotifen immediately upon instillation, and similar compared with vehicle.
The observed safety profile of bilastine ophthalmic solution in this trial is similar to other H1 receptor antagonists, such as levocabastine,21 emedastine,22 olopatadine,7 ketotifen,23 and azelastine.24 Dry eye, eye discharge and eye irritation were the related TEAEs reported in more than one patient (4, 2, 2, respectively) in the current trial. Apart from eye discharge, these are common adverse reactions reported for H1 receptor agonists. A recent study of cetirizine ophthalmic solution 0.24% showed a comparable safety and tolerability, with low incidence of adverse effects.9 Nedocromil sodium 2% ophthalmic solution also presented a favorable safety profile in the treatment of seasonal AC.25 A comparative study of safety of alcaftadine 0.25%, olopatadine hydrochloride 0.2%, and bepotastine besilate 1.5% ophthalmic solutions showed that all three drugs were safe and well tolerated for the treatment of AC.10
The efficacy results showed that in allergic conjunctivitis patients, the mean absolute change from baseline in the TESS and the ocular symptom scores was significantly better in the bilastine ophthalmic solution group than in the placebo group. The analysis of TESS and the individual ocular symptoms confirmed that bilastine ophthalmic solution 0.6% was more effective than placebo in treating individual ocular symptoms.
Most topical treatments require repeated daily administration, contributing to lack of treatment adherence and consequently suboptimal control of AC symptoms.26,27 In contrast, bilastine 0.6% ophthalmic solution can be administered only once daily. Also, formulations containing preservatives could have a higher risk of adverse events that may induce ocular surface changes and have a negative impact on adherence.28 An advantage with respect to other formulations available on the market is that bilastine ophthalmic formulation is available as a preservative-free, phosphates-free sterile solution containing hyaluronic acid. The use of preservative-free ophthalmic formulations can increase the tolerability and decrease the risk of eye tissues damage (eg, keratopathy caused by the excipient benzalkonium chloride).29
A possible limitation that must be considered when interpreting the results of this study is that all the patients with AC were of Caucasian ethnicity. Further studies should be carried out to evaluate if the results presented here are consistent in other ethnicities. In this study all patients were adults, but a clinical trial to assess the safety, tolerability and efficacy of bilastine 0.6% ophthalmic solution in children is currently underway (ClinicalTrials.gov identifier: NCT04810390).
Conclusion
In conclusion, bilastine ophthalmic solution revealed no safety concerns as evaluated by TEAEs, laboratory parameters, visual acuity, slit lamp biomicroscopy findings, intraocular pressure, dilated fundus examination, peak ocular discomfort and ocular tolerability. The study suggests that bilastine 0.6% ophthalmic solution is safe and well tolerated after long-term administration and exposure in adults with AC. This drug is effective in reducing ocular symptoms associated with AC in response to both seasonal and perennial allergens, as reported in previous studies.
Data Sharing Statement
Data available from the corresponding author upon reasonable request due to privacy/ethical reasons.
Ethics Approval and Informed Consent
The protocol for this study was approved by Independent Ethics Committees prior to each center’s initiation (See Table S1). Written informed consent was received from all patients prior to enrolment into the trial, which was conducted in accordance with the Declaration of Helsinki and all local regulations.
Acknowledgments
Francisco López de Saro (Trialance SCCL) provided medical writing assistance with the preparation of this manuscript.
Funding
This study was funded by FAES Farma SA (Leioa, Spain). This work was partially supported by the Basque Country Government (Economic Development and Infrastructures Department) through the HAZITEK program (grant number: ZE-2019/00004, 2019).
Disclosure
PA, GH and NFH are employees of FAES FARMA. In addition, GH NFH have a patent EP3740191B1 issued to FAES FARMA. MJ reports personal fees from FAES PHARMA, during the conduct of the study; personal fees from Allergopharma, ALK, Stallergenes, Hal, Allergy Therapeutics, Leti, GSK, Novartis, Genentech, TEVA, TAKEDA, Chiesi, Shire, Janssen, Celltrion, Sanofi, Regeneron, outside the submitted work. PK reports personal fees from Adamed, AstraZeneca, Boehringer Ingelheim, Berlin Chemie Menarini, Celon Pharma, FAES, Novartis, Glenmark, Polpharma, GSK, Sandoz, and Teva, outside the submitted work. GP is affiliated with Centrum Medyczne All-Med. The authors report no other conflicts of interest in this work.
References
1. Dupuis P, Prokopich CL, Hynes A, Kim H. A contemporary look at allergic conjunctivitis. Allergy Asthma Clin Immunol. 2020;16:5. doi:10.1186/s13223-020-0403-9403
2. Bielory L, Delgado L, Katelaris CH, Leonardi A, Rosario N, Vichyanoud P. ICON: diagnosis and management of allergic conjunctivitis. Ann Allergy Asthma Immunol. 2020;124(2):118–134. doi:10.1016/j.anai.2019.11.014
3. Leonardi A, Castegnaro A, Valerio AL, Lazzarini D. Epidemiology of allergic conjunctivitis: clinical appearance and treatment patterns in a population-based study. Curr Opin Allergy Clin Immunol. 2015;15(5):482–488. doi:10.1097/ACI.0000000000000204
4. Castillo M, Scott NW, Mustafa MZ, Mustafa MS, Azuara-Blanco A. Topical antihistamines and mast cell stabilisers for treating seasonal and perennial allergic conjunctivitis. Cochrane Database Syst Rev. 2015;(6):CD009566. doi:10.1002/14651858.CD009566.pub2
5. Leonardi A, Silva D, Perez Formigo D, et al. Management of ocular allergy. Allergy. 2019;74(9):1611–1630. doi:10.1111/all.13786
6. Torkildsen G, Narvekar A, Bergmann M. Efficacy and safety of olopatadine hydrochloride 0.77% in patients with allergic conjunctivitis using a conjunctival allergen-challenge model. Clin Ophthalmol. 2015;9:1703–1713. doi:10.2147/OPTH.S83263
7. Meier E, Narvekar A, Iyer GR, et al. Pharmacokinetics and safety of olopatadine hydrochloride 0.77% in healthy subjects with asymptomatic eyes: data from 2 independent clinical studies. OPTH. 2017;11:669–681. doi:10.2147/OPTH.S126690
8. Meier EJ, Torkildsen GL, Gomes PJ, Jasek MC. Phase III trials examining the efficacy of cetirizine ophthalmic solution 0.24% compared to vehicle for the treatment of allergic conjunctivitis in the conjunctival allergen challenge model. Clin Ophthalmol. 2018;12:2617–2628. doi:10.2147/OPTH.S185835opth-12-2617
9. Malhotra RP, Meier E, Torkildsen G, Gomes PJ, Jasek MC. Safety of cetirizine ophthalmic solution 0.24% for the treatment of allergic conjunctivitis in adult and pediatric subjects. Clin Ophthalmol. 2019;13:403–413. doi:10.2147/OPTH.S186092opth-13-403
10. Ayyappanavar S, Sridhar S, Kumar K, et al. Comparative analysis of safety and efficacy of Alcaftadine 0.25%, Olopatadine hydrochloride 0.2% and Bepotastine besilate 1.5% in allergic conjunctivitis. Indian J Ophthalmol. 2021;69(2):257–261. doi:10.4103/ijo.IJO_2083_20
11. Roberts G, Pfaar O, Akdis CA, et al. EAACI Guidelines on Allergen Immunotherapy: allergic rhinoconjunctivitis. Allergy. 2018;73(4):765–798. doi:10.1111/all.13317
12. MHRA. Summary of product characteristics Ilaxten 10 mg orodispersible tablets, bilastine 2018; 2018. Available from: https://mhraproductsproduction.blob.core.windows.net/docs/2f799931ac3572bd33b801e5b15e6168c95b156a.
13. Church MK, Tiongco-Recto M, Ridolo E, Novak Z. Bilastine: a lifetime companion for the treatment of allergies. Curr Med Res Opin. 2020;36(3):445–454. doi:10.1080/03007995.2019.1681134
14. Okubo K, Gotoh M, Asako M, et al. Efficacy and safety of bilastine in Japanese patients with perennial allergic rhinitis: a multicenter, randomized, double-blind, placebo-controlled, parallel-group phase III study. Allergol Int. 2017;66(1):97–105. doi:10.1016/j.alit.2016.05.014
15. Togawa M, Yamaya H, Rodriguez M, Nagashima H. Pharmacokinetics, Pharmacodynamics and Population Pharmacokinetic/Pharmacodynamic Modelling of Bilastine, a Second-Generation Antihistamine, in Healthy Japanese Subjects. Clin Drug Investig. 2016;36(12):1011–1021. doi:10.1007/s40261-016-0447-2
16. Sastre J, Mullol J, Valero A, Valiente R. Efficacy and safety of bilastine 20 mg compared with cetirizine 10 mg and placebo in the treatment of perennial allergic rhinitis. Curr Med Res Opin. 2012;28(1):121–130. doi:10.1185/03007995.2011.640667
17. Yagami A, Furue M, Togawa M, Saito A, Hide M. One-year safety and efficacy study of bilastine treatment in Japanese patients with chronic spontaneous urticaria or pruritus associated with skin diseases. J Dermatol. 2017;44(4):375–385. doi:10.1111/1346-8138.13644
18. Ochoa D, Román M, Belmonte C, et al. Pharmacokinetics and safety of a bilastine once-daily, preservative-free, ophthalmic formulation. Adv Ther. 2021;38(7):4070–4081. doi:10.1007/s12325-021-01801-y
19. Torrens Prat I, Gonzalo A, Ganza Á, Hernández G, Zazpe A. Ocular biodistribution of once‐daily bilastine eye drops reveals highest levels in conjunctiva up to 24 hours post‐administration. Acta Ophthalmol. 2022;100(S267):1755–3768. doi:10.1111/j.1755-3768.2022.182
20. Gomes PJ, Ciolino JB, Arranz P, Hernández G, Fernández N. Efficacy of once-daily ophthalmic bilastine for the treatment of allergic conjunctivitis: a dose-finding study. J Investig Allergol Clin Immunol. 2022;33(4). doi:10.18176/jiaci.0800
21. Allaire C, Siou-Mermet R, Bassols A. Safety and efficacy of a new preservative-free levocabastine ophthalmic solution (Levofree®) using the conjunctival provocation test. J Fr Ophtalmol. 2012;35(7):491–498. doi:10.1016/j.jfo.2011.08.016
22. Verin P, Easty DL, Secchi A, et al. Clinical evaluation of twice-daily emedastine 0.05% eye drops (Emadine eye drops) versus levocabastine 0.05% eye drops in patients with allergic conjunctivitis. Am J Ophthalmol. 2001;131(6):691–698. doi:10.1016/S0002-9394(00)00947-8
23. Greiner JV, Mundorf T, Dubiner H, et al. Efficacy and safety of ketotifen fumarate 0.025% in the conjunctival antigen challenge model of ocular allergic conjunctivitis. Am J Ophthalmol. 2003;136(6):1097–1105. doi:10.1016/S0002-9394(03)00708-6
24. Giede-Tuch C, Westhoff M, Zarth A. Azelastine eye-drops in seasonal allergic conjunctivitis or rhinoconjunctivitis. A double-blind, randomized, placebo-controlled study. Allergy. 1998;53(9):857–862. doi:10.1111/j.1398-9995.1998.tb03991.x
25. Melamed J, Schwartz RH, Blumenthal MN, Zeitz HJ. Efficacy and safety of nedocromil sodium 2% ophthalmic solution b.i.d. in the treatment of ragweed seasonal allergic conjunctivitis. Allergy Asthma Proc. 2000;21(4):235–239. doi:10.2500/108854100778248863
26. Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther. 2001;23(8):1296–1310. doi:10.1016/s0149-2918(01)80109-0
27. Richter A, Anton SF, Anton SE, Koch P, Dennett SL. The impact of reducing dose frequency on health outcomes. Clin Ther. 2003;25(8):2307–2335. doi:10.1016/s0149-2918(03)80222-9
28. Baudouin C, Labbé A, Liang H, Pauly A, Brignole-Baudouin F. Preservatives in eyedrops: the good, the bad and the ugly. Prog Retin Eye Res. 2010;29(4):312–334. doi:10.1016/j.preteyeres.2010.03.001
29. Goldstein MH, Silva FQ, Blender N, Tran T, Vantipalli S. Ocular benzalkonium chloride exposure: problems and solutions. Eye. 2022;36(2):361–368. doi:10.1038/s41433-021-01668-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.