Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Safety and Efficacy of Transarterial Chemoembolization Combined with Tyrosine Kinase Inhibitor and Immune Checkpoint Inhibitors for Unresectable Hepatocellular Carcinoma: A Single Center Experience
Authors Pan X, Wu SJ, Tang Y, Zhou YF, Luo JW ![]() , Fang ZT
, Fang ZT
Received 12 January 2023
Accepted for publication 30 May 2023
Published 9 June 2023 Volume 2023:10 Pages 883—892
DOI https://doi.org/10.2147/JHC.S404500
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Xin Wei Wang
Xian Pan,1,2,* Shao-Jie Wu,1,2,* Yi Tang,1,2,* Yan-Feng Zhou,1,2 Jie-Wei Luo,1,3 Zhu-Ting Fang1,2
1Fujian Provincial Hospital, Shengli Clinical Medical College of Fujian Medical University, Fuzhou, People’s Republic of China; 2Department of Interventional Radiology, Fujian Provincial Hospital, Fuzhou, People’s Republic of China; 3Department of Traditional Chinese Medicine, Fujian Provincial Hospital, Fuzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jie-Wei Luo; Zhu-Ting Fang, Tel +86 59188217540, Email [email protected]; [email protected]
Purpose: In China, many patients with hepatocellular carcinoma (HCC) are diagnosed at an advanced stage. Several studies have shown that triple therapy [transarterial chemoembolization (TACE) combined with tyrosine kinase inhibitors (TKIs) and immune checkpoint inhibitors (ICIs)] is beneficial for patient survival. In this study, we aimed to evaluate the efficacy of triple therapy (TACE + TKIs + ICIs) for unresectable HCC (uHCC) and the conversion rate of surgical resection (SR). The primary endpoints were objective response rate (ORR) and disease control rate (DCR) based on the modified Response Evaluation Criteria in Solid Tumors (mRECIST) and RECIST v1.1 and adverse events (AEs), while the secondary endpoint was the conversion rate of patients with uHCC treated with triple therapy followed by SR.
Patients and Methods: Forty-nine patients with uHCC who received triple therapy at Fujian Provincial Hospital between January 2020 and June 2022 were retrospectively included. The treatment efficacy, SR conversion rate, and associated AEs were recorded.
Results: Among the 49 patients enrolled, the ORRs assessed by mRECIST and RECIST v1.1 were 57.1% (24/42) and 14.3% (6/42), respectively, and the DCRs were 92.9% (39/42) and 88.1% (37/42), respectively. Seventeen (34.7%) patients met the criteria for resectable HCC and underwent resection. The median interval between the start of triple therapy and resection was 113.5 days (range 94.75 to 182 d), and the median number of TACE was 2 (range 1 to 2.5). The patients did not achieve median overall survival or median progression-free survival. Treatment-related AEs occurred in 48 (98%) patients, and 18 (36.7%) patients had grade ≥ 3 AEs.
Conclusion: Triple combination therapy resulted in a relatively high ORR and conversion resection rate following uHCC treatment.
Keywords: TACE, immune checkpoint inhibitors, tyrosine kinase inhibitor, surgical resection
Introduction
Hepatocellular carcinoma (HCC) is the sixth-most common neoplasm and the third leading cause of cancer-related death. HCC has been recognized as a leading cause of death among patients with cirrhosis.1 Hepatitis B virus (HBV) infection is one of the major causes of HCC.2 In addition to alcohol, hepatitis C virus (HCV) and aflatoxin B1, which are driven by a combination of genetic susceptibility, lifestyle, environmental factors, and HBV virus infection, can also contribute to the development of HCC.3
Early- and mid-stage HCC with good liver reserve function are the preferred indications for surgical resection.4 Liver transplantation is a radical treatment for HCC, particularly in patients with portal hypertension or decompensated cirrhosis with early HCC.4 In China, a significant number of patients with HCC are diagnosed with advanced disease at the time of consultation.5,6 Therapeutic options for liver transplantation are limited owing to a shortage of donors. As for the choice of hepatectomy treatment options, patients may not be able to undergo radical hepatectomy for reasons such as liver insufficiency due to insufficient liver volume or cirrhosis and poor prognosis. Transarterial chemoembolization (TACE) is the standard of care for patients with unresectable HCC (uHCC). Studies have shown that postoperative survival is also better for resectable intermediate- to advanced HCC treated with surgery than with non-surgical treatment.7,8 Sun et al illustrated the conversion of uHCC to resectable HCC through the use of tyrosine kinase inhibitors (TKI) and programmed cell death-1 (PD-1), demonstrating the feasibility of the combination of TKI and PD-1 antibody as a conversion therapy.9 Therefore, it is important to control disease progression with local or systemic therapy during the waiting period or downgrade patients who do not meet the criteria for liver transplantation/hepatectomy to meet the criteria.10
Recently, several studies have shown that conversion therapy improves the chances of obtaining radical treatment for uHCC,11–13 and the treatment of uHCC to prolong the survival time of patients is still of interest to many scholars.14 In this study, we assessed the efficacy of triple therapy by observing the extent of tumor remission and conversion rate to surgical resection (SR) in 49 patients with uHCC after triple therapy.
Materials and Methods
Patients
This retrospective study reviewed 49 patients who underwent conventional TACE (C-TACE), drug-eluting bead TACE (DEB-TACE) combined with PD-1 inhibitor, and anti-angiogenic drug (lenvatinib) as first-line treatment for uHCC at Fujian Provincial Hospital from January 2020 to June 2022. We assessed the efficacy of triple therapy by observing the extent of tumor remission and the conversion rate of SR. Triple therapy was defined as treatment with immune checkpoint inhibitors (ICIs) and TKI within one month of the first TACE procedure. This study was approved by the Institutional Ethics Committee of the Fujian Provincial Hospital. This study is consistent with the Declaration of Helsinki. Informed consent was obtained from all patients for the use of data in this study.
Unresectable tumors were defined as those that were surgically or biologically unresectable. Surgically unresectable tumors included:4 (1) patients with poor liver function (massive ascites, jaundice); (2) patients with China Liver Cancer (CNLC) stage IIb to IIIb or Barcelona Clinic Liver Cancer (BCLC) stage B to C who are not suitable for HCC resection (due to tumor size, location, number, extrahepatic metastasis, and others); (3) residual liver volume <30% of the standard liver volume (in patients without cirrhosis) or 40% (in patients with cirrhosis). Biologically unresectable tumors were defined as technically resectable; however, resection did not result in better outcomes than non-surgical treatment.
The inclusion criteria were as follows: 1) patients with HCC diagnosed by pathology or imaging; 2) age between 18 and 80 years; 3) extrahepatic metastases and/or large vessel invasion were allowed; 4) Child-Pugh class A or B; 5) Eastern Cooperative Oncology Group Performance Status (ECOG PS) score 0 to 1; 6) no previous systemic therapy for HCC (including TKIs or ICIs); 7) the systemic therapy used was only PD-1 inhibitors in combination with lenvatinib; 8) the first combination of PD-1 inhibitors and anti-angiogenic drugs were all completed within one month following the first TACE treatment; 9) at least one cycle of immunotherapy and targeted therapy following TACE treatment; 10) at least one target lesion with measurable diameter ≥1 cm according to modified Response Evaluation Criteria in Solid Tumors (mRECIST); 11) prior resection or ablation was allowed. The exclusion criteria were as follows: 1) pathologically/histologically confirmed cholangiocarcinoma, mixed HCC, sarcomatoid HCC, or hepatic fibrous plate laminar carcinoma; and 2) incomplete baseline and review data.
TACE Procedure
All TACE procedures were performed by two interventional radiologists with >10 years of experience. The right femoral artery was punctured using the Seldinger method, and the location, size, and blood supply of the tumor were confirmed intraoperatively using digital subtraction angiography. The microcatheter (Renegade Hi Flo, Boston Scientific Corp, USA) was super-selected to enter the tumor supply artery, and a mixture of iodinated oil (Guerbet, Paris, France (5 mL to 20 mL)), epirubicin ((Hisun Pfizer Pharmaceuticals, Fuyang, China) 20 mg to 30 mg), and oxaliplatin (Hengrui Medical, Suzhou, China (100 mg to 150 mg)) or 1 drug -loaded microsphere (Hengrui Medical, Suzhou, China (100 μm to 300 μm))+ 60 mg of famasin (Hisun Pfizer Pharmaceuticals, Fuyang, China) was injected into the selected tumor artery. Finally, 350 μm to 510 μm gelatin sponge particles (Alicon Pharmaceutical, Hangzhou, China) were bolstered to enhance the tumor supply to the artery. Patients were evaluated every 6 to 8 weeks by assessing alpha-fetoprotein (AFP) levels and tumor remnants using enhanced computed tomography (CT) or nuclear magnetic resonance imaging (MRI) for repeat TACE or surgery. To avoid the effect of the post-TACE embolic syndrome, AEs were recorded from one month after the procedure to the endpoint of follow-up.
Systematic Therapy
Patients weighing ≥60 kg were treated with lenvatinib (Eisai, Tokyo, Japan) at 12 mg orally per day, and those weighing <60 kg were treated with 8 mg orally per day, after which the dose was reduced or discontinued according to patient drug toxicity and adverse effects. PD-1 (200 mg sintilimab (InnoventBiologics, Suzhou, China), 200 mg tislelizumab (BeiGene, Shanghai, China), 200 mg camrelizumab (HengruiPharma, Lianyungang, China), 240 mg toripalimab (ZhongheBiomedicalTechnology, Suzhou, China), and 200 mg pembrolizumab (MerckSharp&Dohme, NewJersey, USA)) was administered intravenously once every three weeks. All procedures (ICIS and lenvatinib) were performed within one month of the first TACE procedure.
TKI and ICIs were withheld for three days before and after TACE. SR was performed at least three weeks after the last dose of PD-1 and one week after the last dose of lenvatinib. All patients with active HBV infections were treated with oral antiviral therapy. Treatment-related adverse events (AEs) were graded according to the National Cancer Institute Common Toxicity Criteria for Adverse Events (CTCAE) version 5.0.
Surgical Resection
In the triple therapy group, patients with HCC who were evaluated by two hepatobiliary surgeons with >10 years of experience and were eligible for surgical resection underwent final SR. All patients who underwent surgery were evaluated by a multidisciplinary team.
Follow-Up
The enrolled patients were treated with ICIs and TKI after the first TACE until imaging confirmed disease progression to progressive disease (PD) or patients experienced intolerable adverse drug reactions. The drug dose was reduced, discontinued, or changed, depending on the patient’s systemic condition and tolerance level. For new intrahepatic lesions, the current treatment schedule was continued if the investigator assessed whether the patient would benefit from continuing the current therapy schedule.
Before treatment, complete baseline data were recorded for all patients. Patients’ age, sex, height, weight, ECOG score, BCLC stage, CNLC stage, portal invasion, history of cirrhosis, Child-Pugh score, platelet count, liver and kidney function, coagulation tests, hepatitis B surface antigen (HBsAg) test, and AFP were recorded through an electronic case system. Preoperative tumor size, tumor location, tumor envelope margin, tumor number, vascular invasion, maximum longest tumor diameter, extrahepatic metastases, and lymph node metastases were recorded using imaging (abdominal enhancement CT and/or MRI).
Tumors were evaluated using mRECIST criteria and RESIST v1.1 criteria based on enhanced CT or MRI, measuring the maximum tumor diameter after enhancement and the longest tumor diameter without enhancement, to assess the effectiveness of triple therapy for unresectable primary HCC. mRECIST and RECIST v1.1 methods were used to classify tumor efficacy into complete response (CR), partial response (PR), stable disease (SD), and PD. Tumor response was evaluated using both measurement modes. Whether the composition ratios differed between DEB-TACE and C-TACE subgroups was analyzed by the chi-square test to assess whether the effectiveness of triple therapy differed between the two approaches. The objective response rate (ORR) was defined as the proportion of patients with CR and PR, and the disease control rate (DCR) was defined as the proportion of patients with CR, PR, and SD. The images were evaluated by a radiologist and a hepatobiliary surgeon, both with 10 years of experience.
The primary study endpoints were ORR and DCR, which were assessed according to the mRECIST and RECIST v1.1 criteria and AEs. The secondary endpoint was the proportion of feasible surgical resections after triple therapy (conversion rate). Patients had at least one piece of imaging evidence one month before the first TACE procedure and received postoperative imaging follow-up. The postoperative AFP levels and enhanced CT or MRI of the liver were evaluated. The choice of subsequent treatment was based on the residual tumor or recurrence, combined with the assessment of liver function and systemic conditions. All patients were followed-up until death or the end date of December 2022.
Statistical Analysis
Statistical analyses were performed using the SPSS version 26 software (IBM, New York). Data conforming to a normal distribution are presented as mean (standard deviation), and data not conforming to a normal distribution are presented as median (P25, P75). Categorical data were compared using the chi-squared test or Fisher’s exact test. Statistical significance was set at P < 0.05.
Results
Patients
A total of 49 patients with uHCC received triple therapy at Fujian Provincial Hospital between January 2020 and June 2022. Among the 49 patients, the median follow-up time was 196 days (143, 411); 38 patients (77.6%) were <65 years old, and 11 patients (22.4%) were ≥65 years old; 46 (93.9%) were men, and 3 (6.1%) were women. A total of 33 patients (67.3%) had an ECOG-PS score of 0, and 16 patients (32.7%) had an ECOG PS score of 1; 40 patients (81.6%) were Child-Pugh grade A, and 9 patients (18.4%) were Child-Pugh grade B; 5 patients (10.2%) were BCLC stage A, 14 patients (28.6%) were BCLC stage B, and 30 patients (61.2%) were BCLC stage C; PVTT patients were 27 (55.1%), 6 patients (12.2%) had extrahepatic metastases, 14 patients (28.6%) had hepatic vein tumor thrombosis, 4 patients (8.2%) had inferior vena cava tumor thrombosis, and 28 patients (57.1%) had baseline AFP ≥400 ng/mL. Demographic and baseline characteristics of the patients are shown in Table 1.
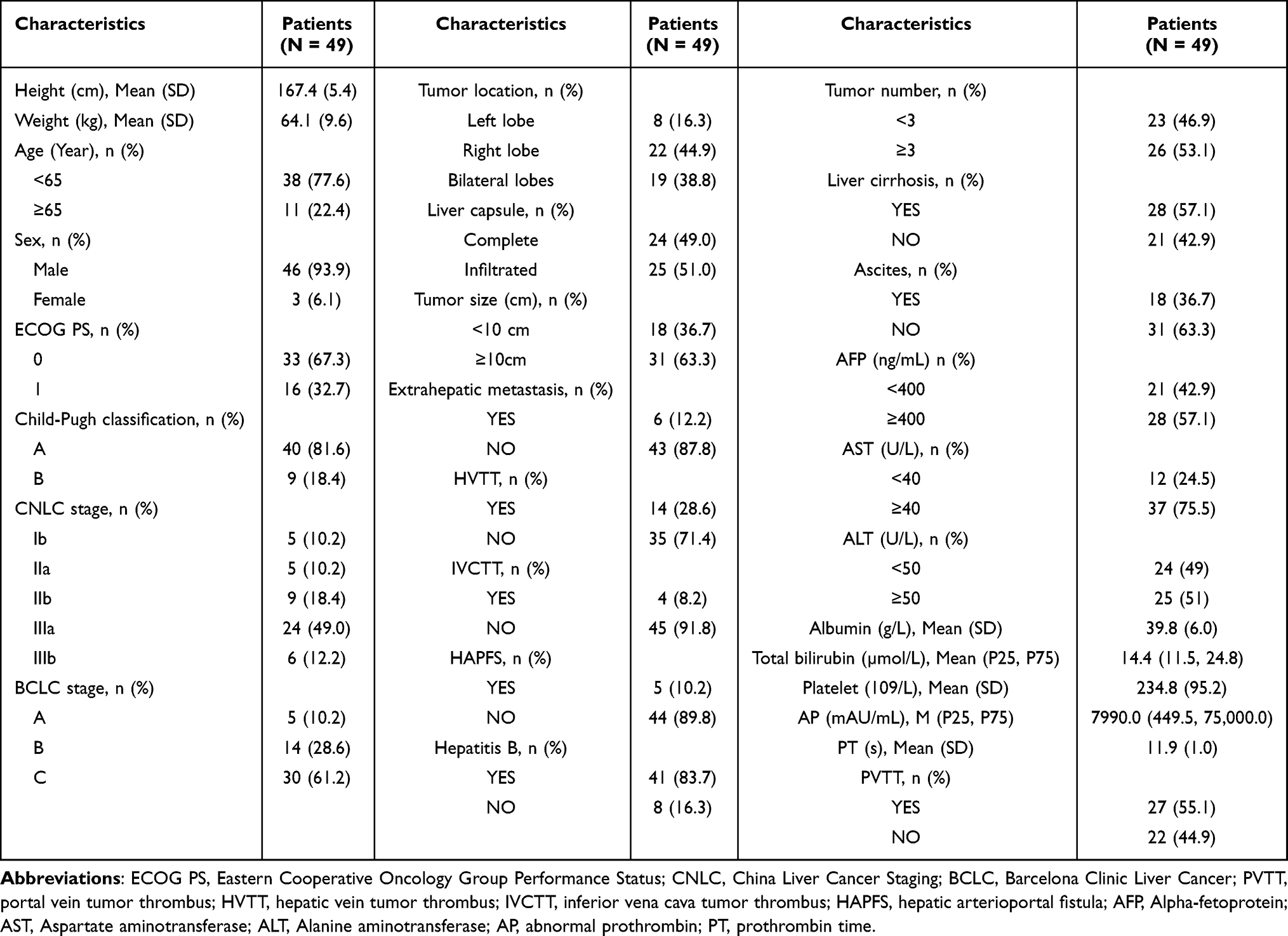 |
Table 1 Baseline Characteristics of 49 Patients |
Efficacy
According to the mRECIST criteria, the patients’ best responses were 2 CR, 22 PR, 15 SD, 3 PD, and 7 not evaluable. Patients who were not evaluable were excluded from the assessment of ORR and DCR owing to incomplete data (confirmed response time <6 weeks). According to the RECIST v1.1 criteria, the patient’s best responses were 0 CR, 6 PR, 31 SD, 5 and PD, and 7 were not evaluated. The ORR assessed by mRECIST and RECIST v1.1 was 57.1% (24/42) and 14.3% (6/42), respectively. The DCR assessed by mRECIST and RECIST v1.1 was 92.9% (39/42) and 88.1% (37/42), respectively. (Table 2).
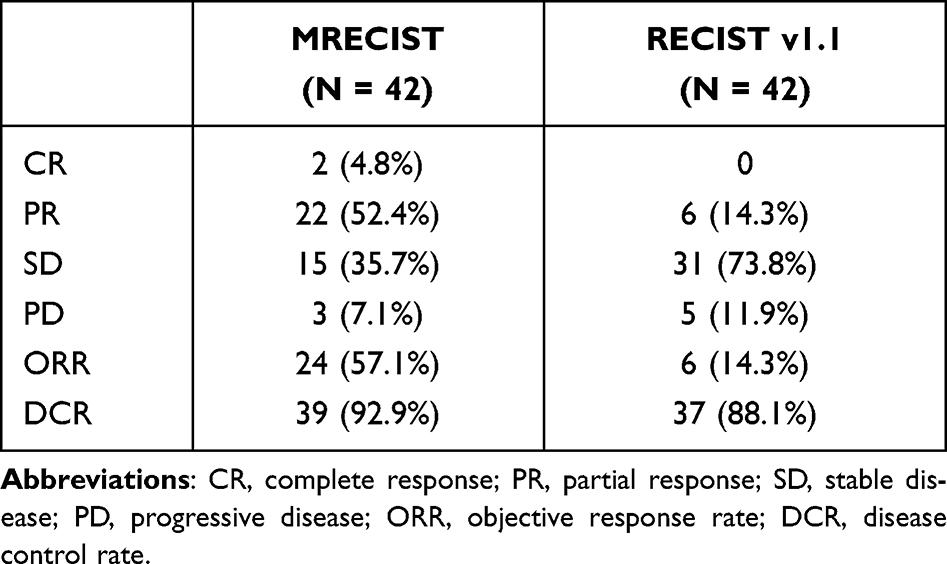 |
Table 2 Radiological Response According to mRECIST and RECISTv1.1 |
Among the five patients with uHCC in BCLC stage A, no patient achieved CR, two patients (40%) achieved PR, two patients (40%) achieved SD, no patient achieved PD, and one patient (20%) was not evaluable. Of the 14 patients with uHCC in BCLC stage B, 1 (7.14%) achieved CR, 8 (57.14%) achieved PR, 3 (21.43%) achieved SD, 0 achieved PD, and 2 (14.29%) were not evaluable. Of the 30 patients with uHCC in BCLC stage C, 1 (3.3%) achieved CR, 12 (40%) achieved PR, 10 (33.3%) achieved SD, 3 (10%) achieved PD, and 4 (13.3%) were not evaluable. (Table 3).
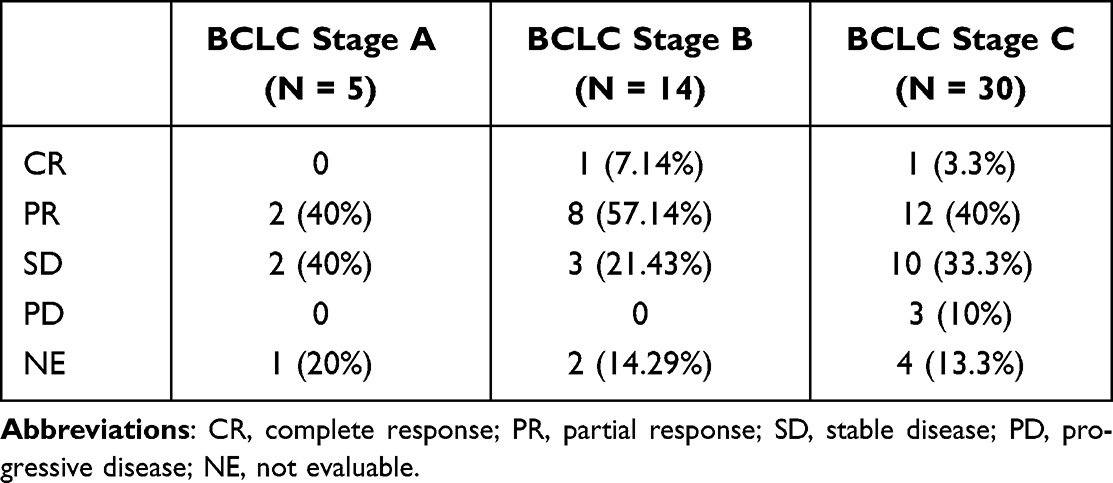 |
Table 3 Radiological Response in the Subgroups According to mRECIST |
In the subgroup analysis of DEB-TACE vs C-TACE, the ORRs were 61.1% (11/18) and 54.2% (13/24), respectively, and the differences were not statistically significant. The DCRs were 88.9% (16/18) and 95.8% (23/24), respectively, and the results were not statistically significant (Table 4).
 |
Table 4 Radiological Response in the Subgroups (d-TACE and c-TACE) According to mRECIST |
Of the 49 patients treated with triple therapy, a total of 17 patients (34.7%) underwent surgical resection (1 BCLC A, 7 BCLC B, and 9 BCLC C), with a median interval between initiation of triple therapy and resection of 113.5 days (range 94.75 days to 182 days) and a median number of TACEs (range 1 to 2.5). The mean tumor size was 11.4 cm ± 3.7 cm. Two patients had extrahepatic metastases, ten had vascular invasion, eight had tumor numbers <3, nine had tumor numbers ≥3, four had a tumor located in the left lobe, eight had a tumor located in the right lobe, and five patients had tumors located in both lobes (Table 5). One patient died of hepatic function failure 12 days postoperatively, and one patient experienced recurrence 53 days postoperatively; the remaining patients had no significant postoperative discomfort, and no tumor recurrence was observed during the follow-up period. Median overall survival (OS) and progression-free survival (PFS) were not determined. The OS rate in the triple therapy group at 12 months was 97.4%.
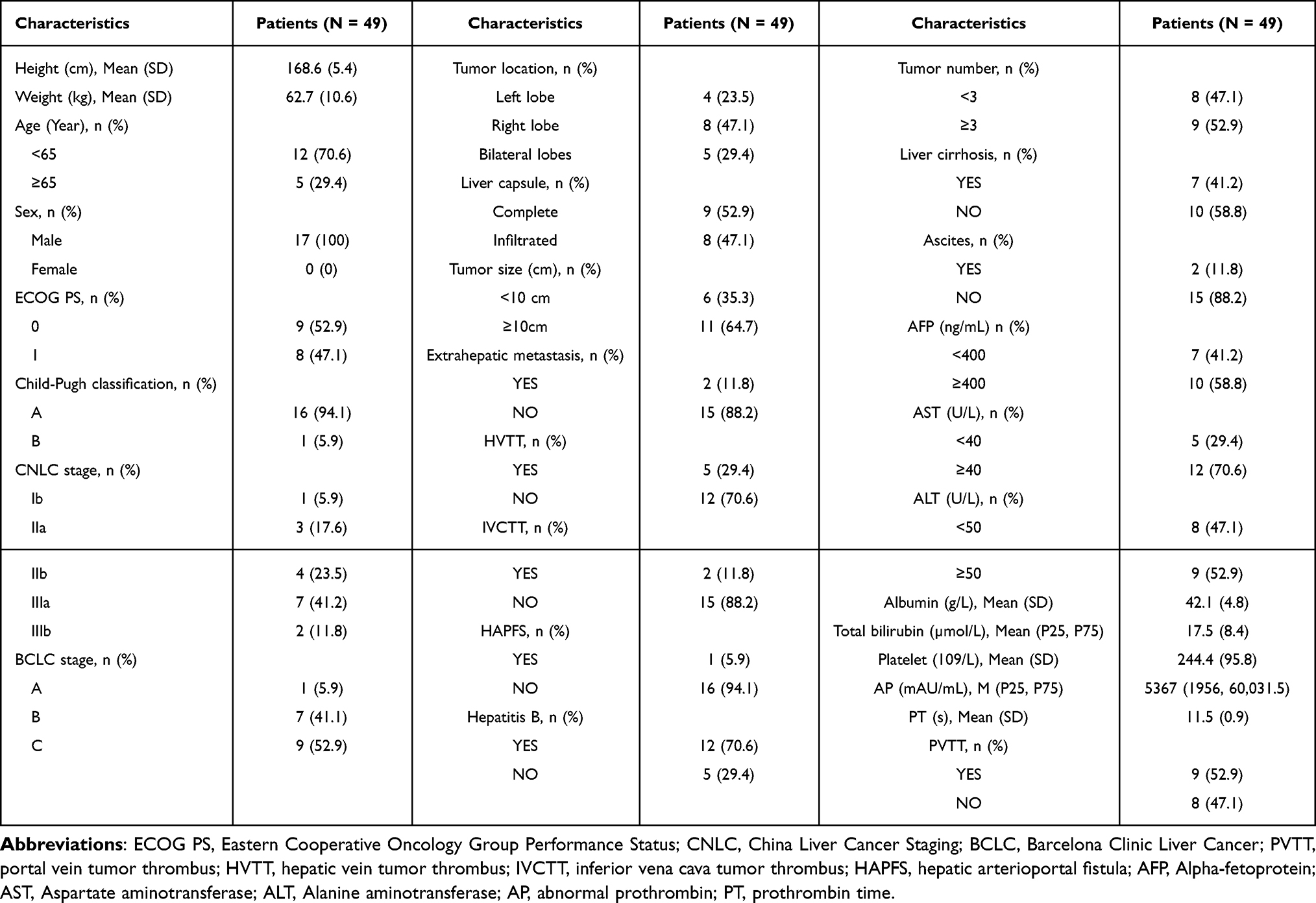 |
Table 5 Baseline Characteristics in 17 Patients for Surgical Resection |
Safety
Forty-eight patients (98%) experienced at least one AE during treatment, with an incidence of >10%, including hypertension, increased aspartate aminotransferase, increased alanine aminotransferase, decreased platelet count, fatigue, proteinuria, decreased appetite, pyrexia, abdominal pain, nausea, alopecia, and hypothyroidism (Table 6). Eighteen patients (36.7%) had a high AE classification grade (grade ≥3), including hypertension, aspartate aminotransferase increase, alanine aminotransferase levels, platelet count reduction, nausea, and bleeding from fundic varices. The main adverse effects after TACE were high aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels, which gradually decreased over time. No deaths occurred due to adverse effects.
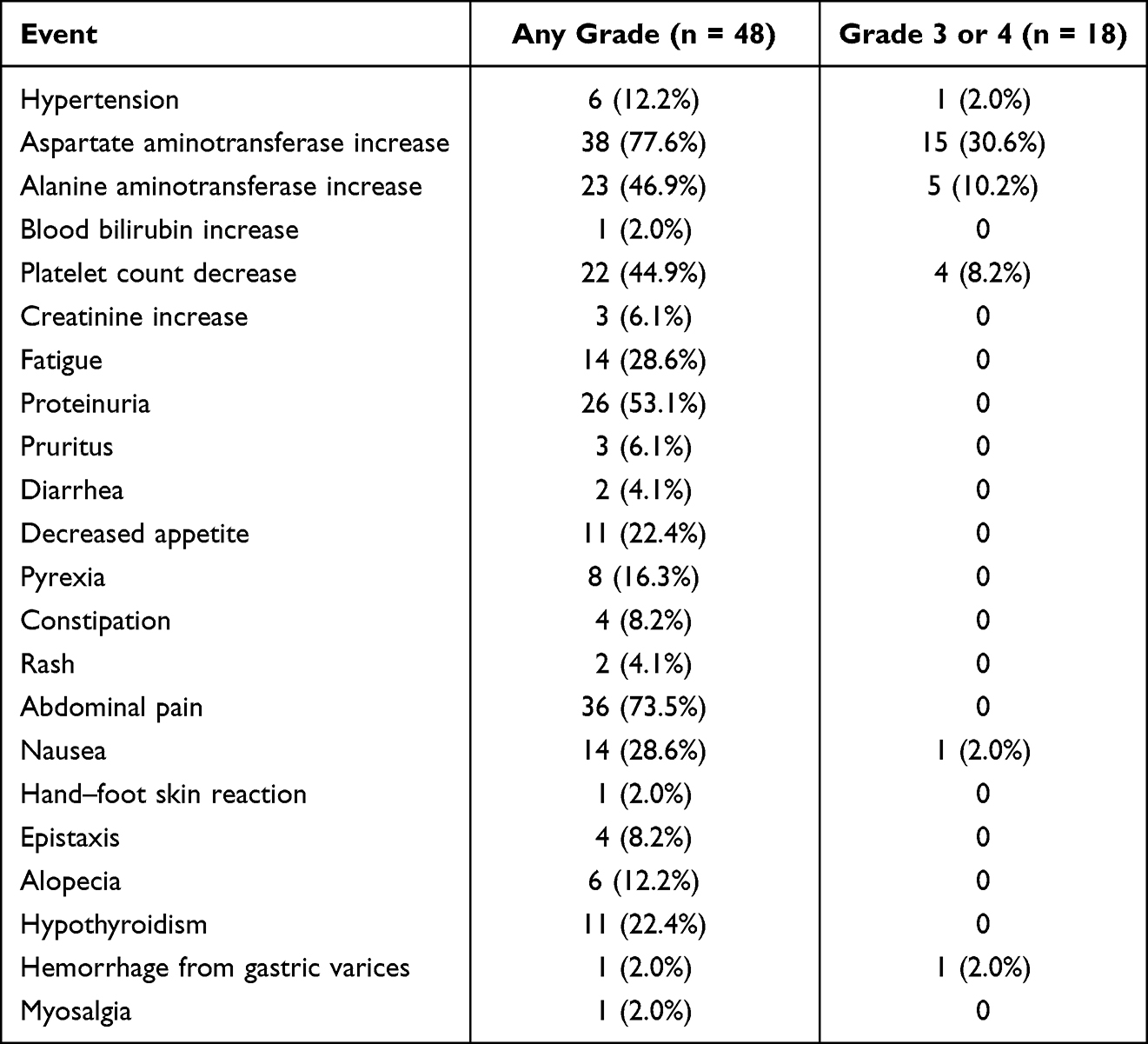 |
Table 6 Adverse Events |
Discussion
In China, most patients with HCC are diagnosed with middle- to advanced-stage disease, mostly accompanied by cirrhosis and poor liver function. They often miss the opportunity for radical SR, which is the main reason for the poor overall survival of Chinese patients with HCC.6 In recent years, the nonsurgical treatment for HCC has been the focus of research. Several studies have shown that systemic treatment is associated with good long-term survival.15,16 Translational therapy to transform uHCC into resectable HCC, followed by hepatectomy, offers the possibility of radical resection in patients with intermediate to advanced HCC. In this study, we retrospectively evaluated the effectiveness of triple-conversion therapy and the subsequent conversion rate to hepatic cancer resection in 49 patients with uHCC.
TACE is the standard of care for uHCC. HCC is a blood-supply-rich tumor that shows rapid enhancement in the arterial phase and rapid outlines in the portal phase on imaging. Hepatic artery chemoembolization leads to hypoxic necrosis of the tumor owing to the interruption of the target artery of the tumor. However, because of the dual blood supply to the liver, a one-time TACE procedure frequently cannot completely kill the tumor tissue.17 Enhanced CT/MRI is reviewed 4 to 6 weeks after the first TACE procedure to determine whether to continue subsequent TACE treatment based on the extent of residual surviving tumor tissue. In addition, multiple TACE treatments often cause liver function impairment.14,18 For patients with non-responsive HCC, abandonment of TACE therapy is recommended after three cycles.19
Based on the Imbrave150 study, atezolizumab combined with bevacizumab for advanced HCC had significantly higher OS than sorafenib [overall survival at 6 months and 12 months were 84.8% (95% CI, 80.9 to 88.7) and 67.2% (95% CI, 61.3 to 73.1), respectively, in the atezolizumab–bevacizumab group and 72.2% (95% CI, 65.1 to 79.4) and 54.6% (95% CI, 45.2 to 64.0) in the sorafenib group].15 Atezolizumab–bevacizumab is now recommended as a first-line therapy for advanced HCC.20 In a multicenter phase Ib single-arm study, lenvatinib plus pembrolizumab resulted in a median OS of 22.0 months with a manageable safety profile for uHCC.16 The REFLECT study showed that the OS with lenvatinib was not inferior to that with sorafenib. A study by Lau et al reported sequential resection of 15 patients with uHCC following systemic immunotherapy, and the 1-, 2-, and 3-year survival rates were 100%, 100%, and 53%, respectively.21 These studies suggest that systemic therapy plays an important role in the treatment of uHCC.
TACE has the dual effect of interrupting tumor blood supply and releasing tumor antigens after destroying tumor cells (the cytotoxic effect).22,23 While causing tumor hypoxia, tumor cells release vascular endothelial growth factor, leading to vascular remodeling, which affects the prognosis of TACE treatment.24,25 However, newly produced blood vessels are immature and aberrant and impair T-cell extravasation, interfering with the trafficking and infiltration of T cells.26 Anti-angiogenic TKI can remodel tumor vasculature (vascular normalization) and promote lymphocyte infiltration of the tumor microenvironment (TME).27
ICIs are antibodies that target the PD-1/programmed cell death ligand-1 pathway.28 The use of immunotherapy can increase the infiltration of CD4+ and CD8+ cells.29 Thus, immunotherapy appears to be a therapeutic approach; however, not all patients respond to immunotherapy because of the formation of an immunosuppressive microenvironment filled with immunosuppressive regulatory (Treg) cells.22 In addition, TACE has a positive regulatory effect in promoting partial recovery of lymphocyte function.22 Depletion of Treg cells and control of their function through TACE can enhance the anti-tumor immune response.10
In this single-center retrospective study, we examined the effectiveness and conversion rate of triple therapy in patients with uHCC and documented the treatment-related AEs. To avoid the effect of the post-TACE embolic syndrome, AEs were recorded from one month after the procedure to the endpoint of follow-up. According to the mRECIST assessment, the ORR and DCR of triple therapy patients were 49% and 79.6% in this study, 64.5% and 77.4% in a study by Yang et al,27 56.1% and 85.4% in a study by Cai et al,30 48.7% and 84.6% in a study by Feng et al,31 and 41.7% and 79.2% in a study by Huang et al, respectively. Furthermore, the ORR and DCR of triple therapy patients in Huang et al presented better outcomes than ICIs + TKI groups (12.5% and 50.0%),32 42% and 80% in a study by Han et al presented better outcome thanTACE groups (31.1% and 51.1%) and TACE+TKI groups (35.5% and 65.8%), respectively.33 These studies show that triple therapy has an advantage in terms of efficacy. Our results are comparable to those of other single-center investigative studies. In this study, the subgroup analysis of DEB-TACE and C-TACE showed no significant difference in the effectiveness of the two interventional procedures (Table 4).
The conversion rate in this study was 34.7% (17/49) for triple therapy, while the study by Zhu et al showed a conversion resection rate of 15.9% (10/63) for uHCC with the combination of TKI and PD-1,13 and a conversion rate of 28% (30/107) was reported in the study by Yi et al.12 In comparison, triple therapy may result in higher conversion rates than diphtherapy (TKI+ICIs). However, in the present study, 18 patients (36.7%) had high-grade AEs (grade ≥3), as distinguished by increased ALT and AST after TACE. In this study, the effect of TACE surgery on patients’ postoperative liver function was unavoidable, probably because most of the enrolled patients had mid- to late-stage cancer with poor baseline liver function, although we routinely administered anti-hepatitis B virus and hepatoprotective drugs to all patients postoperatively.
This study has several limitations. First, because this was a retrospective study, there was inevitable selection bias and limited sample size. Second, this was a single-arm study and lacked a control group to analyze the efficiency and conversion rate with the duplex or TACE-alone groups. Third, this study had a short follow-up period, OS and PFS were not achieved, whether triple therapy was beneficial for survival was not observed, and the recurrence rate of HCC following surgical resection was not observed.
Conclusion
Based on the results of this study, triple therapy presented a high rate of tumor response and conversion resection in patients with uHCC. No deaths occurred due to AEs. In summary, the efficiency and conversion resection rates of triple therapy are promising. However, because of the many shortcomings of our study, the analysis of the relationship between baseline (vascular invasion, tumor size, etc) and study outcomes (conversion to resectable) failed to identify meaningful suggestive indicators and still needs to be validated in a large multicenter study.
Funding
This work was supported by the Fujian Province Natural Science Fund Project (2020J011096, 2020J011064), Fujian Province Medical Innovation Foundation (2021CXB001, 2022CXB002,2022CXA001), and the Special Research Foundation of Fujian Provincial Department of Finance (2022-840; 2021-848), China.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Kulik L, El-Serag HB. Epidemiology and management of hepatocellular carcinoma. Gastroenterology. 2019;156(2):477–491 e1. doi:10.1053/j.gastro.2018.08.065
3. Jia L, Gao Y, He Y, Hooper JD, Yang P. HBV induced hepatocellular carcinoma and related potential immunotherapy. Pharmacol Res. 2020;159:104992. doi:10.1016/j.phrs.2020.104992
4. Zhou J, Sun H, Wang Z, et al. Guidelines for the diagnosis and treatment of hepatocellular carcinoma (2019 edition). Liver Cancer. 2020;9(6):682–720. doi:10.1159/000509424
5. Fan W, Zhu B, Yue S, et al. Idarubicin-Loaded DEB-TACE plus Lenvatinib versus Lenvatinib for patients with advanced hepatocellular carcinoma: a propensity score-matching analysis. Cancer Med. 2022. doi:10.1002/cam4.4937
6. Yang JD, Hainaut P, Gores GJ, Amadou A, Plymoth A, Roberts LR. A global view of hepatocellular carcinoma: trends, risk, prevention and management. Nat Rev Gastroenterol Hepatol. 2019;16(10):589–604. doi:10.1038/s41575-019-0186-y
7. Zhong JH, Ke Y, Gong WF, et al. Hepatic resection associated with good survival for selected patients with intermediate and advanced-stage hepatocellular carcinoma. Ann Surg. 2014;260(2):329–340. doi:10.1097/SLA.0000000000000236
8. Wang K, Guo WX, Chen MS, et al. Multimodality treatment for hepatocellular carcinoma with portal vein tumor thrombus: a large-scale, multicenter, propensity matching score analysis. Medicine. 2016;95(11):e3015. doi:10.1097/MD.0000000000003015
9. Sun H-C, X-d Z, Huang C, et al. Initially unresectable hepatocellular carcinoma treated by combination therapy of tyrosine kinase inhibitor and anti-PD-1 antibody followed by resection. J Clin Oncol. 2020;38(15_suppl):e16690. doi:10.1200/JCO.2020.38.15_suppl.e16690
10. Pinato DJ, Murray SM, Forner A, et al. Trans-arterial chemoembolization as a loco-regional inducer of immunogenic cell death in hepatocellular carcinoma: implications for immunotherapy. J Immunother Cancer. 2021;9(9):e003311. doi:10.1136/jitc-2021-003311
11. Lau WY, Lai EC. Salvage surgery following downstaging of unresectable hepatocellular carcinoma--A strategy to increase resectability. Ann Surg Oncol. 2007;14(12):3301–3309. doi:10.1245/s10434-007-9549-7
12. Yi Y, Sun BY, Weng JL, et al. Lenvatinib plus anti-PD-1 therapy represents a feasible conversion resection strategy for patients with initially unresectable hepatocellular carcinoma: a retrospective study. Front Oncol. 2022;12:1046584. doi:10.3389/fonc.2022.1046584
13. Zhu XD, Huang C, Shen YH, et al. Downstaging and resection of initially unresectable hepatocellular carcinoma with tyrosine kinase inhibitor and anti-PD-1 antibody combinations. Liver Cancer. 2021;10(4):320–329. doi:10.1159/000514313
14. Kobayashi K, Ogasawara S, Takahashi A, et al. Evolution of survival impact of molecular target agents in patients with advanced hepatocellular carcinoma. Liver Cancer. 2022;11(1):48–60. doi:10.1159/000519868
15. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
16. Finn RS, Ikeda M, Zhu AX, et al. Phase Ib study of lenvatinib plus pembrolizumab in patients with unresectable hepatocellular carcinoma. J Clin Oncol. 2020;38(26):2960–2970. doi:10.1200/JCO.20.00808
17. Tsurusaki M, Murakami T. Surgical and Locoregional Therapy of HCC: TACE. Liver Cancer. 2015;4(3):165–175. doi:10.1159/000367739
18. Kawamura Y, Kobayashi M, Shindoh J, et al. Lenvatinib-transarterial chemoembolization sequential therapy as an effective treatment at progression during lenvatinib therapy for advanced hepatocellular carcinoma. Liver Cancer. 2020;9(6):756–770. doi:10.1159/000510299
19. Chen S, Peng Z, Zhang Y, et al. Lack of response to transarterial chemoembolization for intermediate-stage hepatocellular carcinoma: abandon or repeat? Radiology. 2021;298(3):680–692. doi:10.1148/radiol.2021202289
20. Huang J-T, Zhang S, Yang Y-H, et al. Recent update on immunotherapy and its combination with interventional therapies for hepatocellular carcinoma. Clin Med Insights. 2022;16:11795549221134832. doi:10.1177/11795549221134832
21. Lau WY, Leung TW, Lai BS, et al. Preoperative systemic chemoimmunotherapy and sequential resection for unresectable hepatocellular carcinoma. Ann Surg. 2001;233(2):236–241. doi:10.1097/00000658-200102000-00013
22. Ren Z, Yue Y, Zhang Y, et al. Changes in the peripheral blood treg cell proportion in hepatocellular carcinoma patients after transarterial chemoembolization with microparticles. Front Immunol. 2021;12:624789. doi:10.3389/fimmu.2021.624789
23. Pol J, Vacchelli E, Aranda F, et al. Trial Watch: immunogenic cell death inducers for anticancer chemotherapy. Oncoimmunology. 2015;4(4):e1008866. doi:10.1080/2162402X.2015.1008866
24. Shim JH, Park JW, Kim JH, et al. Association between increment of serum VEGF level and prognosis after transcatheter arterial chemoembolization in hepatocellular carcinoma patients. Cancer Sci. 2008;99(10):2037–2044. doi:10.1111/j.1349-7006.2008.00909.x
25. Fu Z, Li X, Zhong J, et al. Lenvatinib in combination with transarterial chemoembolization for treatment of unresectable hepatocellular carcinoma (uHCC): a retrospective controlled study. Hepatol Int. 2021;15(3):663–675. doi:10.1007/s12072-021-10184-9
26. Li SJ, Chen JX, Sun ZJ. Improving antitumor immunity using antiangiogenic agents: mechanistic insights, current progress, and clinical challenges. Cancer Commun. 2021;41(9):830–850. doi:10.1002/cac2.12183
27. Yang F, Yang J, Xiang W, et al. Safety and efficacy of transarterial chemoembolization combined with immune checkpoint inhibitors and tyrosine kinase inhibitors for hepatocellular carcinoma. Front Oncol. 2021;11:657512. doi:10.3389/fonc.2021.657512
28. Cheng AL, Hsu C, Chan SL, Choo SP, Kudo M. Challenges of combination therapy with immune checkpoint inhibitors for hepatocellular carcinoma. J Hepatol. 2020;72(2):307–319. doi:10.1016/j.jhep.2019.09.025
29. Kikuchi H, Matsui A, Morita S, et al. Increased CD8+ T-cell infiltration and efficacy for multikinase inhibitors after PD-1 blockade in hepatocellular carcinoma. J Natl Cancer Inst. 2022;114(9):1301–1305. doi:10.1093/jnci/djac051
30. Cai M, Huang W, Huang J, et al. Transarterial chemoembolization combined with lenvatinib plus PD-1 inhibitor for advanced hepatocellular carcinoma: a retrospective cohort study. Front Immunol. 2022;13:848387. doi:10.3389/fimmu.2022.848387
31. Feng JK, Liu ZH, Fu ZG, et al. Efficacy and safety of transarterial chemoembolization plus antiangiogenic- targeted therapy and immune checkpoint inhibitors for unresectable hepatocellular carcinoma with portal vein tumor thrombus in the real world. Front Oncol. 2022;12:954203. doi:10.3389/fonc.2022.954203
32. Huang JT, Zhong BY, Jiang N, et al. Transarterial chemoembolization combined with immune checkpoint inhibitors plus tyrosine kinase inhibitors versus immune checkpoint inhibitors plus tyrosine kinase inhibitors for advanced hepatocellular carcinoma. J Hepatocell Carcinoma. 2022;9:1217–1228. doi:10.2147/JHC.S386672
33. Han Z, Yang F, Zhang Y, et al. Prognostic efficacy and prognostic factors of TACE plus TKI with ICIs for the treatment of unresectable hepatocellular carcinoma: a retrospective study. Front Oncol. 2022;12:1029951. doi:10.3389/fonc.2022.1029951
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Immune Indicator Changes in Hepatocellular Carcinoma Undergoing TACE Plus ICIs and Anti-VEGF Antibodies/TKIs: A Prognostic Biomarker Analysis
Xu XY, Wang Z, Liu CY, Wu HD, Hu ZX, Lin YY, Zhang S, Shen J, Zhong BY, Zhu XL
Journal of Hepatocellular Carcinoma 2024, 11:2019-2032
Published Date: 22 October 2024
Prognostic Impact of the Systemic Immune-Inflammation Index in Unresectable Hepatocellular Carcinoma Undergoing Second-Line Combination Therapy: A Multicenter Study
Chen X, Li X, Jiang Y, Xie Q, Zhang P, Zhou X, Wei C, Xie P, Cao L
Cancer Management and Research 2026, 18:613658
Published Date: 3 June 2026