")
Back to Journals » Psoriasis: Targets and Therapy » Volume 13
Safety and Efficacy of Covid-19 Vaccination in Patients Undergoing Biological Treatments for Psoriasis
Authors Potestio L , Martora F , Fabbrocini G, Battista T, Megna M
Received 15 February 2023
Accepted for publication 6 April 2023
Published 12 April 2023 Volume 2023:13 Pages 11—18
DOI https://doi.org/10.2147/PTT.S398135
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Uwe Wollina
Luca Potestio,* Fabrizio Martora,* Gabriella Fabbrocini, Teresa Battista, Matteo Megna
Section of Dermatology, Department of Clinical Medicine and Surgery, University of Naples Federico II, Naples, Italy
*These authors contributed equally to this work
Correspondence: Fabrizio Martora, Section of Dermatology, Department of Clinical Medicine and Surgery, University of Naples Federico II, Naples, Italy, Tel +39 081 7462457, Fax +39 081 7462442, Email [email protected]
Abstract: The introduction of biologic drugs revolutionized the treatment of psoriasis, shifting treatment goals to higher treatment outcomes and less frequent safety issues. The outbreak of Coronavirus disease 2019 (COVID-19) represented a worldwide challenge, strongly affecting lifestyle, global economy, and overall health. Among the strategies adopted to contain the spreading of the infection, vaccination is the main one. In this context, the introduction of COVID-19 vaccines raised several doubts about their effectiveness and safety in patients undergoing therapy with biological for psoriasis. Even if molecular and cellular mechanisms by which COVID-19 vaccines lead to psoriasis development have not yet been fully elucidated, vaccination itself can trigger the release of interleukin (IL)-6, interferon (IFN) and tumor necrosis factor (TNF) α by T-helper (Th)1/Th17 cells. All these cytokines are involved in psoriasis pathogenesis. Thus, the aim of this manuscript is to review current literature on the safety and effectiveness of COVID-19 vaccination in psoriasis patients undergoing treatment with biologics, in order to clarify any concerns.
Keywords: psoriasis, COVID-19 vaccinations, biologic therapies, efficacy, safety
Introduction
Psoriasis is a common, chronic-recurrent, immune-mediated skin disease affecting up to 3% of worldwide population.1,2 Clinically, it is usually characterized by erythemato-desquamative plaques that are well delineated from surrounding normal skin.3 Several comorbidities (obesity, hypertension, anxiety/depression, hyperlipidemia, diabetes mellitus and inflammatory bowel disease) may be associated with psoriasis, impacting the psychological health of affected patients.4–7 On consequence, early diagnosis and appropriate treatment play a key role.8,9
Even if mild forms of disease are usually treated with topicals, systemic treatments are often required for moderate-to-severe forms of the disease.10,11 However, conventional systemic drugs (acitretin, cyclosporine, methotrexate, dimethyl fumarate) are often contraindicated or linked to adverse events.10,11 Fortunately, the introduction of biologic drugs revolutionized the treatment of psoriasis, shifting treatment goals to higher treatment outcomes and less frequent safety issues. Indeed, biologics act against specific cytokines, receptors, or other cellular pathways that play a key role in psoriasis pathogenesis, allowing a directed and personalized treatment with generally fewer systemic adverse effects when compared to other systemic agents.12–15 Several biologic drugs have been approved for psoriasis management [anti-Tumor Necrosis Factor (TNF) α, anti-interleukins (IL) 12/23, anti-IL17 and anti-IL23], showing excellent results in terms of effectiveness,16,17 also in erythrodermic forms.18 As regards the safety of biologic drugs, promising results have been reported, particularly for anti-IL17 and anti-IL23 classes.19–22
The outbreak of Coronavirus disease 2019 (COVID-19) represented a worldwide challenge, strongly affecting lifestyle, global economy, and overall health.23,24 In this context, several measures have been adopted to reduce the spreading of the infection.25–29 Among these, vaccination is the most important one to fight against the pandemic. Four vaccines have been approved by European Medicines Agency (EMA): 2 mRNA-based vaccines (Pfizer/BioNTech; BNT162b2 and Moderna; mRNA-1273) and 2 viral-vector-based vaccines (AstraZeneca; AZD1222 and Johnson & Johnson; Ad26.COV2.S).30,31 Similar to other drugs, mild-to-moderate adverse events (AEs) following vaccination have been reported, including fatigue, diarrhea, headache, fever, muscle aches, pain or redness at the injection site, chills, etc. Fortunately, most of these AEs were mild and self-limited.32,33 Moreover, several cutaneous reactions have been described following COVID-19 vaccination such as local injection reactions (erythema, swelling, tenderness, pain, induration, and pruritus), hypersensitivity reactions, rashes, etc.34–37
As regards the use of biologic treatments during the pandemic period, several concerns were raised on their safety.38 However, several data confirmed that undergoing biologic treatment did not increase the risk of contracting COVID-19 neither worsening its natural course.38 Similarly, the introduction of COVID-19 vaccines raised several doubt about their effectiveness and safety in patients undergoing therapy with biological for psoriasis.39–41 Even if molecular and cellular mechanisms by which COVID-19 vaccines lead to psoriasis development have not yet been fully elucidated, vaccination itself can trigger the release of IL-6, interferon and TNF by T-helper (Th)1/Th17 cells.42,43 All these cytokines are involved in psoriasis pathogenesis.42,43 Thus, the aim of this manuscript is to review current literature on the safety and effectiveness of COVID-19 vaccination in psoriasis patients undergoing treatment with biologics, in order to clarify any concerns.
Materials and Methods
For the current review, literature research was performed on the PubMed, Cochrane Skin, Embase, EBSCO, MEDLINE and Google Scholar databases (until February 1, 2023). Studies were identified, screened and extracted for relevant data following the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines using the following keywords: “COVID-19”, “vaccine”, “cutaneous”, “vaccination”, “side effects”, “adverse events”, “safety”, “efficacy”, “skin manifestations”, “mRNA”, “viral-vector, ‘Pfizer/BioNTech’, ‘BNT162b2’, ‘Moderna’, ‘mRNA-1273’, ‘AstraZeneca’, ‘Johnson & Johnson’, ‘Ad26.COV2.S’, ‘AZD1222’, ‘psoriasis’, biologic therapy, “biologics”, “adalimumab”, “etanercept”, “certolizumab”, “infliximab”, “brodalumab”, “ixekizumab”, “secukinumab”, “guselkumab”, “risankizumab”, “tildrakizumab”. Analyzed manuscripts included reviews, metanalyses, letter to editor, real-life studies, case series. The most relevant manuscripts were considered. Studies were collected if they provided information on psoriasis worsening following COVID-19 vaccination with BNT162b2, mRNA-1273, AZD1222 and Ad26.COV2.S in patients undergoing biologic treatment for psoriasis. Articles regarding other skin reactions were not considered. Moreover, manuscripts where the type of vaccine leading to psoriasis exacerbation was not specified were excluded. Similarly, manuscripts assessing the effectiveness and safety of COVID-19 vaccines in patients undergoing biological treatment for psoriasis were considered. Thus, the research was refined by reviewing the texts and the abstracts of collected articles. The bibliography was also reviewed to include articles that could have been missed. Only English language manuscripts were considered. This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
Results
A total of 10 articles were included in this review. Even if several cases of psoriasis exacerbation or new-onset psoriasis have been reported in literature following COVID-19 vaccination,44–53 few of these cases have been described in patients undergoing biologic treatment for psoriasis (Table 1). Interestingly, psoriasis flare during biologic treatment have been reported also in patients contracting COVID-19 infection.54
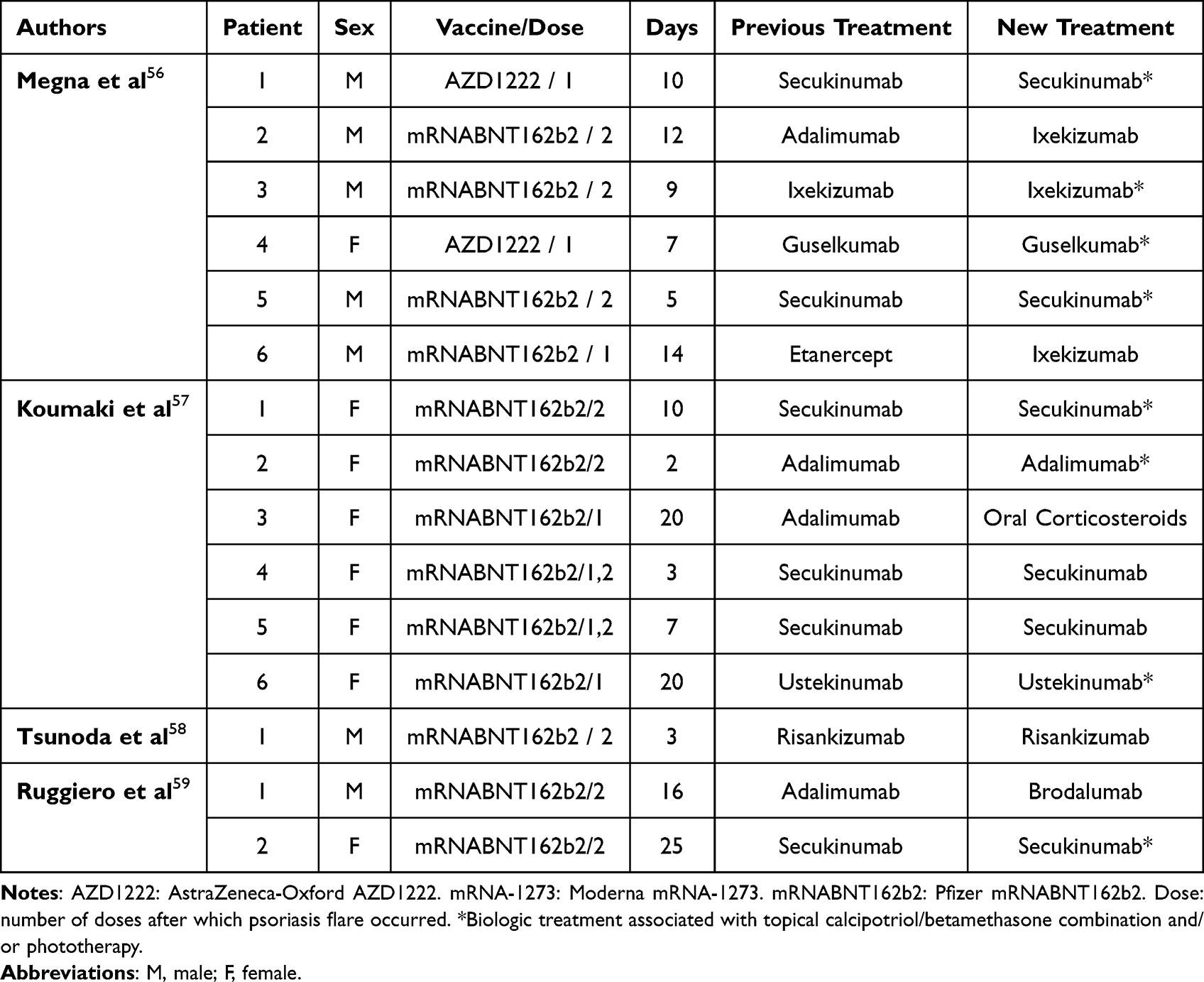 |
Table 1 Cases of Psoriasis Exacerbation Following COVID-19 Vaccination in Patients Undergoing Treatment with Biologics for Psoriasis |
Sotiriou et al firstly highlighted the possibility of psoriasis exacerbation after vaccination reporting a case series of 14 patients who developed a flare of psoriasis following COVID-19 vaccination. However, none of these patients was treated with biologic at the moment of vaccine administration.55 Subsequently, Megna et al reported 11 cases of patients developing psoriasis following vaccination. For the first time, they showed the possibility of psoriasis worsening also in patients receiving biologic therapies since 6 patients were receiving biologics at the moment of vaccination (secukinumab:2, adalimumab:1, ixekizumab:1, guselkumab:1, etanercept:1).56 Of note, in two cases biologic switch was required.56 Similarly, Koumaki et al reported 6 cases of psoriasis exacerbation following COVID-19 vaccination in patients undergoing biological treatment for psoriasis (secukinumab:3, adalimumab:2, ustekinumab:1).57 No biologic switch was required. However, one patient discontinued the treatment.57 Finally, Tsunoda et al reported a case of psoriasis exacerbation in a patient undergoing treatment with risankizumab.58
Of interest, Ruggiero et al reported 2 cases of patients who developed nail psoriasis following vaccination during biologic treatment with adalimumab (n = 1) or secukinumab (n = 1).59
As regards the effectiveness and safety of COVID-19 vaccination, they have been poorly investigated. Talamonti et al reported their real-life experience including 369 patients with moderate-to-severe psoriasis undergoing therapy with anti-IL (ani-IL12/23: 192; anti-IL17: 93; anti-IL23: 84).60 None of these patients discontinued treatment during the study period (5 months).60 No serious AEs were reported as well as about one-third of patients reported mild AEs seen in the general population (injection site pain, fever, fatigue, etc).60 The safety of COVID-19 vaccines in psoriatic patients treated with biologics has been also investigated by Musumeci et al on a cohort of 50 patients with stable plaque psoriasis treated with biologics (anti-TNFα: 24; anti-IL17: 14; anti-IL12/23: 7: anti-IL23: 5) for at least 2 months who received COVID-19 vaccination.61 All patients discontinued their biological agents 10 days before and 10 days after each dose of vaccine. After the vaccines, all patients were assessed at day 2, 7, and 14.61 None of them reported any side effects or a psoriatic flare except for one patient treated with infliximab biosimilar who referred an exacerbation of psoriasis after BNT162b2 vaccine.61 Damiani et al reported a case series on 4 health-care workers with moderate-to-severe psoriasis undergoing treatment with biologics at the moment of COVID-19 vaccination (BNT162b2) to assess the immune response and safety to vaccines. No safety issues were collected as well as all patients developed IgG antibodies toward SAR-CoV-2.62 Marovt et al conducted a prospective observational study to evaluate antibody response against SARS‐CoV‐2 following two doses of BNT162b2 vaccine in patients with psoriasis receiving biologics, and compare it with that of healthy controls.63 Blood samples were collected before the first vaccination and 4 weeks following the second one. Biologic treatment was not interrupted. Globally, 32 patients and 22 controls were enrolled.63 All patients showed positive antibody response, statistically significant differences among the two groups. However, antibody titres were significantly lower in patients than healthy controls (1024.4 ± 870.3 vs 3055.8 ± 2450.9, P < 0.001).63 Moreover, no significant difference in antibody titres in patients aged ≤55 years and patients aged >55 years (1150.7 ± 966.8 vs 898.1 ± 772.4, P < 0.45), or between different treatment groups (P = 0.11) were reported.63 Similarly, Megna et al conducted a similar prospective study assessing blood samples 4 weeks (range 3–6 weeks) following the second dose of COVID‐19 vaccination with mRNA vaccines on 44 patients with psoriasis under biologics (anti-TNFα: 19; anti-IL17: 18; anti-IL12/23: 2: anti-IL23: 5).64 A total of 57 subjects were enrolled in the healthy control group.64 A positive antibody response was detected in 43 (97.7%) patients and 56 (98.2%) healthy subjects, with no significant difference between the groups. Despite mean antibody titres being slightly higher in the healthy cohort (586.5 ± 408.3 BAU/mL vs 468.4 ± 420.3 BAU/mL), no statistically significant differences were found between the study groups.64 Moreover, no statistically significant differences in antibody titres between patients >55 years (426.3 ± 403.5 BAU/mL) and those aged <55 years (497.5 ± 437.0 BAU/mL) and between the different treatment groups in the psoriasis cohort were observed.64
Finally, Cristaudo et al investigated the immunogenicity and safety of anti-SARS-CoV-2 BNT162b2 vaccine in psoriasis patients treated with biologic drugs on a cohort of 48 patients (anti-TNFα: 21; anti-IL17: 6; anti-IL12/23: 8: anti-IL23: 13) and 48 healthy controls.65 Neutralizing IgG titers anti–SARS-CoV-2 were evaluated at baseline (day 0, first injection), after 3 weeks (day 21, second injection, TP1) and four weeks post booster (day 51, TP2).65 Treatment suspension or dose modification of the biologic therapy was not planned.65 A statistically significant increase of antibody titers on TP1 and TP2 was observed in both psoriatic patients and control group when compared to baseline, without statistically significant differences on the antibody response between psoriatic patients versus controls.65 Moreover, older age resulted independently associated with a reduced antibody response to vaccine (P = 0.004). In line with other studies, biologics administration as well as the type of biological treatment minimally affect the immune response to the vaccine.65 Moreover, the authors reported that the Body Mass Index did not affect the response to BNT162b2 as well. No significant AEs were collected, and no psoriasis flares were observed.65 Finally, Mercuri et al reported a real-life, multicenter, case-control study on 160 patients undergoing biologic treatment for psoriasis or psoriatic arthritis showing that heterologous vs homologous primary and booster COVID-19 vaccination do not increase psoriasis flare rate.66
Discussion
Major knowledge on dermatological diseases led to the development of new drugs.67–70 Biological drugs changed the treatment scenario of several diseases.71–73 In particular, the introduction of biologic treatment revolutionized the management of psoriasis,12,74,75 with a high profile in terms of efficacy and safety.76–78 However, several concerns about their safety were raised at the beginning of COVID-19 pandemic period.79–81 Fortunately, their safety was confirmed even during COVID-19 pandemic82 which led to the adoption of several measures in order to contain the spreading of the infection allowing the continuity of biologic treatment, opening new era also after COVD-19 pandemic period.25,83,84 However, the introduction of COVID-19 vaccination newly raised doubt on their efficacy and safety among psoriasis patients receiving biologics. Indeed, the immunologic reaction and immune system dysregulation caused by vaccination may lead to epidermal changes and onset or worsening of certain cutaneous diseases such as psoriasis85 Moreover, the induction of neutralizing antibodies and T‐cell responses by vaccines can lead to increased IFNγ and TNFα production.86 In addition, vaccination may activate plasmacytoid and dermal myeloid dendritic cells might.86 All of these conditions can be a trigger for psoriasis cascade.87 Finally, vaccinations might induce IL‐6 production. This cytokine may be a trigger for Th17 cells to produce IL‐22, which itself stimulates keratinocyte proliferation.88 On one hand, the worsening or new onset of several dermatological diseases cutaneous reactions (lichen planus, bullous disorders, pityriasis rosea, atopic dermatitis, hidradenitis suppurativa, etc.) have been reported following COVID-19 vaccination,89–92 also after the third dose,93,94 and, on the other hand, the mechanism of action of biologic drugs was suggested as a potential cause of vaccine inefficacy. Even if limited, current evidence indicates that the use of biologics in psoriatic patients does not seem to be associated with a reduced effect of COVID-19 vaccination and with an increased risk of COVID-19 severe disease. Moreover, biologic treatments seem to reduce the risk of psoriasis worsening following vaccination. However, uncertainty remains due to the limitations of current studies which are often of short duration and limited sample sizes. Furthermore, a sub-analysis investigating on specific biologic classes is lacking.95
In our hypothesis, biologic drugs do not reduce the immune response to COVID-19 as they are immunomodulating and not immunosuppressive agents, unlike traditional systemic drug.96 Moreover, the immunological protection caused by vaccines is not fully understood, as well as the utility of serological tests.
COVID-19 vaccination is the main weapon to overcome the pandemic period. Globally, worldwide vaccination campaign was a success, showing to be the most effective weapon to prevent and control COVID-19 epidemic, disease progression, hospitalization and mortality. Current guidelines strongly recommend vaccination in all subjects affected by chronic inflammatory skin diseases, also undergoing biological treatments.97,98
Strengths and Limitations
The use of PRISMA guidelines for reviewing the current literature is the main strength of our manuscript. Main limitation is the reduced number of studies investigating the effectiveness and safety of COVID-19 vaccination in patients undergoing biologic therapies for psoriasis.
Conclusion
Current data seem to confirm the safety and efficacy of COVID-19 vaccination in patients undergoing biological treatments for psoriasis. The risk of psoriasis worsening induced by COVID-19 vaccine seems to be very low. Certainly, vaccination should not be discouraged.
Data Sharing Statement
Data are reported in the current study and are on request by corresponding author.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Griffiths CE, Barker JN. Pathogenesis and clinical features of psoriasis. Lancet. 2007;370(9583):263–271. doi:10.1016/S0140-6736(07)61128-3
2. Megna M, Potestio L, Fabbrocini G, Camela E. Treating psoriasis in the elderly: biologics and small molecules. Expert Opin Biol Ther. 2022;1–18. doi:10.1080/14712598.2022.2089020
3. Petit RG, Cano A, Ortiz A, et al. Psoriasis: from pathogenesis to pharmacological and nano-technological-based therapeutics. Int J Mol Sci. 2021;22(9):4983. doi:10.3390/ijms22094983
4. Takeshita J, Grewal S, Langan SM, et al. Psoriasis and comorbid diseases: epidemiology. J Am Acad Dermatol. 2017;76(3):377–390. doi:10.1016/j.jaad.2016.07.064
5. Megna M, Ocampo-Garza SS, Potestio L, et al. New-onset psoriatic arthritis under biologics in psoriasis patients: an increasing challenge? Biomedicines. 2021;9(10):1482. doi:10.3390/biomedicines9101482
6. Boehncke WH. Systemic inflammation and cardiovascular comorbidity in psoriasis patients: causes and consequences. Front Immunol. 2018;9:579. doi:10.3389/fimmu.2018.00579
7. Kamiya K, Kishimoto M, Sugai J, Komine M, Ohtsuki M. Risk factors for the development of psoriasis. Int J Mol Sci. 2019;20(18):4347. doi:10.3390/ijms20184347
8. Megna M, Camela E, Battista T, et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part I: focus on pediatric patients. Expert Opin Drug Saf. 2023:1–17. doi:10.1080/14740338.2023.2173170
9. Megna M, Camela E, Battista T, et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part II: focus on elderly patients. Expert Opin Drug Saf. 2023:1–16. doi:10.1080/14740338.2023.2173171
10. Nast A, Smith C, Spuls PI, et al. EuroGuiDerm guideline on the systemic treatment of Psoriasis vulgaris - Part 1: treatment and monitoring recommendations. J Eur Acad Dermatol Venereol. 2020;34(11):2461–2498. doi:10.1111/jdv.16915
11. Nast A, Smith C, Spuls PI, et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris - Part 2: specific clinical and comorbid situations. J Eur Acad Dermatol Venereol. 2021;35(2):281–317. doi:10.1111/jdv.16926
12. Dave R, Alkeswani A. An overview of biologics for psoriasis. J Drugs Dermatol. 2021;20(11):1246–1247. doi:10.36849/jdd.6040
13. Camela E, Potestio L, Ruggiero A, Ocampo-Garza SS, Fabbrocini G, Megna M. Towards personalized medicine in psoriasis: current progress. Psoriasis. 2022;12:231–250. doi:10.2147/PTT.S328460
14. Honma M, Hayashi K. Psoriasis: recent progress in molecular-targeted therapies. J Dermatol. 2021;48(6):761–777. doi:10.1111/1346-8138.15727
15. Camela E, Potestio L, Fabbrocini G, Ruggiero A, Megna M. New frontiers in personalized medicine in psoriasis. Expert Opin Biol Ther. 2022;1–3. doi:10.1080/14712598.2022.2113872
16. Megna M, Potestio L, Camela E, Fabbrocini G, Ruggiero A. Ixekizumab and brodalumab indirect comparison in the treatment of moderate to severe psoriasis: results from an Italian single-center retrospective study in a real-life setting. Dermatol Ther. 2022;35:e15667. doi:10.1111/dth.15667
17. Megna M, Tommasino N, Potestio L, et al. Real-world practice indirect comparison between guselkumab, risankizumab, and tildrakizumab: results from an Italian 28-week retrospective study. J Dermatolog Treat. 2022:1–8. doi:10.1080/09546634.2022.2081655
18. Megna M, Potestio L, Fabbrocini G, Cinelli E. Tildrakizumab: a new therapeutic option for erythrodermic psoriasis? Dermatol Ther. 2021;34:e15030. doi:10.1111/dth.15030
19. Marasca C, Fornaro L, Martora F, Picone V, Fabbrocini G, Megna M. Onset of vitiligo in a psoriasis patient on ixekizumab. Dermatol Ther. 2021;34(5):e15102. doi:10.1111/dth.15102
20. Ruggiero A, Potestio L, Camela E, Fabbrocini G, Megna M. Bimekizumab for the Treatment of psoriasis: a review of the current knowledge. Psoriasis. 2022;12:127–137. doi:10.2147/PTT.S367744
21. Ruggiero A, Camela E, Potestio L, Fabbrocini G, Megna M. Drug safety evaluation of tildrakizumab for psoriasis: a review of the current knowledge. Expert Opin Drug Saf. 2022;21(12):1445–1451. doi:10.1080/14740338.2022.2160447
22. Kamata M, Tada Y. Safety of biologics in psoriasis. J Dermatol. 2018;45(3):279–286. doi:10.1111/1346-8138.14096
23. Shivalkar S, Pingali MS, Verma A, et al. Outbreak of COVID-19: a detailed overview and its consequences. Adv Exp Med Biol. 2021;1353:23–45. doi:10.1007/978-3-030-85113-2_2
24. Sharma A, Ahmad Farouk I, Lal SK. COVID-19: a review on the novel coronavirus disease evolution, transmission, detection, control and prevention. Viruses. 2021;13(2):202. doi:10.3390/v13020202
25. Marasca C, Annunziata MC, Camela E, et al. Teledermatology and Inflammatory skin conditions during COVID-19 era: new perspectives and applications. J Clin Med. 2022;11(6):1511. doi:10.3390/jcm11061511
26. De Lucia M, Potestio L, Costanzo L, Fabbrocini G, Gallo L. Scabies outbreak during COVID-19: an Italian experience. Int J Dermatol. 2021;60(10):1307–1308. doi:10.1111/ijd.15809
27. Ruggiero A, Megna M, Fabbrocini G, Martora F. Video and telephone teledermatology consultations during COVID-19 in comparison: patient satisfaction, doubts and concerns. Clin Exp Dermatol. 2022;47:1863–1864. doi:10.1111/ced.15286
28. Martora F, Marasca C, Fabbrocini G, Ruggiero A. Strategies adopted in a southern Italian referral centre to reduce Adalimumab discontinuation: comment on “Can we increase the drug survival time of biologic therapies in hidradenitis suppurativa? Clin Exp Dermatol. 2022;47:1864–1865. doi:10.1111/ced.15291
29. Martora F, Fabbrocini G, Nappa P, Megna M. Impact of the COVID-19 pandemic on hospital admissions of patients with rare diseases: an experience of a Southern Italy referral center. Int J Dermatol. 2022;61(7):e237–e238. doi:10.1111/ijd.16236
30. Hadj Hassine I. Covid-19 vaccines and variants of concern: a review. Rev Med Virol. 2022;32(4):e2313. doi:10.1002/rmv.2313
31. Meo SA, Bukhari IA, Akram J, Meo AS, Klonoff DC. COVID-19 vaccines: comparison of biological, pharmacological characteristics and adverse effects of Pfizer/BioNTech and moderna vaccines. Eur Rev Med Pharmacol Sci. 2021;25(3):1663–1669. doi:10.26355/eurrev_202102_24877
32. Soiza RL, Scicluna C, Thomson EC. Efficacy and safety of COVID-19 vaccines in older people. Age Ageing. 2021;50(2):279–283. doi:10.1093/ageing/afaa274
33. Sharif N, Alzahrani KJ, Ahmed SN, Dey SK. Efficacy, immunogenicity and safety of COVID-19 vaccines: a systematic review and meta-analysis. Front Immunol. 2021;12:714170. doi:10.3389/fimmu.2021.714170
34. Martora F, Picone V, Fabbrocini G, Marasca C. Hidradenitis suppurativa flares following COVID-19 vaccination: a case series. JAAD Case Rep. 2022;23:42–45. doi:10.1016/j.jdcr.2022.03.008
35. Martora F, Picone V, Fornaro L, Fabbrocini G, Marasca C. Can COVID-19 cause atypical forms of pityriasis rosea refractory to conventional therapies? J Med Virol. 2022;94(4):1292–1293. doi:10.1002/jmv.27535
36. Martora F, Fabbrocini G, Marasca C. Pityriasis rosea after Moderna mRNA-1273 vaccine: a case series. Dermatol Ther. 2022;35(2):e15225. doi:10.1111/dth.15225
37. Zagaria O, Villani A, Ruggiero A, Potestio L, Fabbrocini G, Gallo L. New-onset lichen planus arising after COVID-19 vaccination. Dermatol Ther. 2022;35(5):e15374. doi:10.1111/dth.15374
38. Ciechanowicz P, Dopytalska K, Mikucka-Wituszyńska A, et al. The prevalence of SARS-CoV-2 infection and the severity of the course of COVID-19 in patients with psoriasis treated with biologic therapy. J Dermatolog Treat. 2022;33(3):1581–1584. doi:10.1080/09546634.2020.1861177
39. He M, Ferris LK, Gabriel N, Tadrous M, Hernandez I. COVID-19 and adherence to biologic therapies for psoriasis: an analysis of nationwide pharmacy claims data. J Manag Care Spec Pharm. 2022;28(11):1213–1218. doi:10.18553/jmcp.2022.28.11.1213
40. Ebrahimi A, Sayad B, Rahimi Z. COVID-19 and psoriasis: biologic treatment and challenges. J Dermatolog Treat. 2022;33(2):699–703. doi:10.1080/09546634.2020.1789051
41. Megna M, Ruggiero A, Marasca C, Fabbrocini G. Biologics for psoriasis patients in the COVID-19 era: more evidence, less fears. J Dermatolog Treat. 2020;31(4):328–329. doi:10.1080/09546634.2020.1757605
42. Khosravi-Hafshejani T, Ghoreishi M, Vera Kellet C, Crawford RI, Martinka M, Dutz JP. Small plaque psoriasis re-visited: a type of psoriasis mediated by a type-I interferon pathway. Exp Dermatol. 2022;31(5):753–763. doi:10.1111/exd.14513
43. Catapano M, Vergnano M, Romano M, et al. IL-36 promotes systemic IFN-I responses in severe forms of psoriasis. J Invest Dermatol. 2020;140(4):816–826.e3. doi:10.1016/j.jid.2019.08.444
44. Piccolo V, Russo T, Mazzatenta C, et al. COVID vaccine-induced pustular psoriasis in patients with previous plaque type psoriasis. J Eur Acad Dermatol Venereol. 2022;36(5):e330–e332. doi:10.1111/jdv.17918
45. Ricardo JW, Lipner SR. Case of de novo nail psoriasis triggered by the second dose of Pfizer-BioNTech BNT162b2 COVID-19 messenger RNA vaccine. JAAD Case Rep. 2021;17:18–20. doi:10.1016/j.jdcr.2021.09.009
46. Romagnuolo M, Pontini P, Muratori S, Marzano AV, Moltrasio C. De novo annular pustular psoriasis following mRNA COVID-19 vaccine. J Eur Acad Dermatol Venereol. 2022;36(8):e603–e605. doi:10.1111/jdv.18114
47. Lamberti A, Lora V, Graceffa D, Bonifati C, Cota C. Nail psoriasis: a rare mRNA COVID −19 vaccine reaction. J Eur Acad Dermatol Venereol. 2022;36. doi:10.1111/jdv.18255
48. Elamin S, Hinds F, Tolland J. De novo generalized pustular psoriasis following Oxford-AstraZeneca COVID-19 vaccine. Clin Exp Dermatol. 2022;47(1):153–155. doi:10.1111/ced.14895
49. Frioui R, Chamli A, Zaouak A, et al. A case of new-onset acute generalized pustular psoriasis following Pfizer-BioNTech COVID-19 vaccine. Dermatol Ther. 2022;35(6):e15444. doi:10.1111/dth.15444
50. Durmaz I, Turkmen D, Altunisik N, Toplu SA. Exacerbations of generalized pustular psoriasis, palmoplantar psoriasis, and psoriasis vulgaris after mRNA COVID-19 vaccine: a report of three cases. Dermatol Ther. 2022;35(4):e15331. doi:10.1111/dth.15331
51. Pavia G, Gargiulo L, Spinelli F, et al. Generalized pustular psoriasis flare in a patient affected by plaque psoriasis after BNT162b2 mRNA COVID-19 vaccine, successfully treated with risankizumab. J Eur Acad Dermatol Venereol. 2022;36(7):e502–e505. doi:10.1111/jdv.18032
52. Krajewski PK, Matusiak Ł, Szepietowski JC. Psoriasis flare-up associated with second dose of Pfizer-BioNTech BNT16B2b2 COVID-19 mRNA vaccine. J Eur Acad Dermatol Venereol. 2021;35(10):e632–e634. doi:10.1111/jdv.17449
53. Perna D, Jones J, Schadt CR. Acute generalized pustular psoriasis exacerbated by the COVID-19 vaccine. JAAD Case Rep. 2021;17:1–3. doi:10.1016/j.jdcr.2021.08.035
54. Shah H, Busquets AC. Psoriasis flares in patients with COVID-19 infection or vaccination: a case series. Cureus. 2022;14(6):e25987. doi:10.7759/cureus.25987
55. Sotiriou E, Tsentemeidou A, Bakirtzi K, Lallas A, Ioannides D, Vakirlis E. Psoriasis exacerbation after COVID-19 vaccination: a report of 14 cases from a single centre. J Eur Acad Dermatol Venereol. 2021;35(12):e857–e859. doi:10.1111/jdv.17582
56. Megna M, Potestio L, Gallo L, Caiazzo G, Ruggiero A, Fabbrocini G. Reply to “Psoriasis exacerbation after COVID-19 vaccination: report of 14 cases from a single centre. J Eur Acad Dermatol Venereol. 2022;36(1):e11–e13. doi:10.1111/jdv.17665
57. Koumaki D, Krueger-Krasagakis SE, Papadakis M, et al. Psoriasis flare-up after AZD1222 and BNT162b2 COVID-19 mRNA vaccines: report of twelve cases from a single centre. J Eur Acad Dermatol Venereol. 2022;36(6):e411–e415. doi:10.1111/jdv.17965
58. Tsunoda K, Watabe D, Amano H. Exacerbation of psoriasis following vaccination with the Pfizer-BioNTech BTN162b2 mRNA COVID-19 vaccine during risankizumab treatment. J Dermatol. 2023;50(2):e79–e80. doi:10.1111/1346-8138.16505
59. Ruggiero A, Potestio L, Battista T, Fabbrocini G, Megna M. Reply to “Nail psoriasis: a rare mRNA COVID-19 vaccine reaction”. J Eur Acad Dermatol Venereol. 2023;37(1):e41–e42. doi:10.1111/jdv.18537
60. Talamonti M, Galluzzo M. Safety of COVID-19 vaccines in patients with psoriasis undergoing therapy with anti-interleukin agents. Expert Opin Biol Ther. 2021;21(11):1535–1537. doi:10.1080/14712598.2021.1965985
61. Musumeci ML, Caruso G, Trecarichi AC, Micali G. Safety of SARS-CoV-2 vaccines in psoriatic patients treated with biologics: a real life experience. Dermatol Ther. 2022;35(1):e15177. doi:10.1111/dth.15177
62. Damiani G, Allocco F, Malagoli P. COVID-19 vaccination and patients with psoriasis under biologics: real-life evidence on safety and effectiveness from Italian vaccinated healthcare workers. Clin Exp Dermatol. 2021;46(6):1106–1108. doi:10.1111/ced.14631
63. Marovt M, Deželak P, Ekart R, Marko PB. Immune response to SARS-CoV-2 mRNA vaccine in patients with psoriasis treated with biologics. Clin Exp Dermatol. 2022;47(11):2041–2043. doi:10.1111/ced.15347
64. Megna M, Potestio L, Battista T, et al. Immune response to Covid-19 mRNA vaccination in psoriasis patients undergoing treatment with biologics. Clin Exp Dermatol. 2022;47:2310–2312. doi:10.1111/ced.15395
65. Cristaudo A, Graceffa D, Pimpinelli F, et al. Immunogenicity and safety of anti-SARS-CoV-2 BNT162b2 vaccine in psoriasis patients treated with biologic drugs. J Eur Acad Dermatol Venereol. 2022;36(4):e266–e268. doi:10.1111/jdv.17861
66. Mercuri SR, Pacifico A, Malagoli P, et al. Heterologous Vs homologous primary and booster COVID-19 vaccination do not increase flare rate in patients with psoriasis and/or psoriatic arthritis: insights from a real-life, multicenter, case-control study. J Eur Acad Dermatol Venereol. 2023. doi:10.1111/jdv.18943
67. Napolitano M, Maffei M, Patruno C, et al. Dupilumab effectiveness for the treatment of patients with concomitant atopic dermatitis and chronic rhinosinusitis with nasal polyposis. Dermatol Ther. 2021;34:e15120. doi:10.1111/dth.15120
68. Cantelli M, Martora F, Patruno C, Nappa P, Fabbrocini G, Napolitano M. Upadacitinib improved alopecia areata in a patient with atopic dermatitis: a case report. Dermatol Ther. 2022;35(4):e15346. doi:10.1111/dth.15346
69. Napolitano M, Fabbrocini G, Genco L, Martora F, Potestio L, Patruno C. Rapid improvement in pruritus in atopic dermatitis patients treated with upadacitinib: a real-life experience. J Eur Acad Dermatol Venereol. 2022;36(9):1497–1498. doi:10.1111/jdv.18137
70. Napolitano M, Fabbrocini G, Martora F, Picone V, Morelli P, Patruno C. Role of aryl hydrocarbon receptor activation in inflammatory chronic skin diseases. Cells. 2021;10(12):3559. doi:10.3390/cells10123559
71. Martora F, Martora L, Fabbrocini G, Marasca C. A case of Pemphigus Vulgaris and Hidradenitis Suppurativa: may systemic steroids be considered in the standard management of Hidradenitis Suppurativa? Ski Appendage Disord. 2022;8(3):265–268. doi:10.1159/000521712
72. Ruggiero A, Martora F, Picone V, Marano L, Fabbrocini G, Marasca C. Paradoxical Hidradenitis Suppurativa during biologic therapy, an emerging challenge: a systematic review. Biomedicines. 2022;10(2):455. doi:10.3390/biomedicines10020455
73. Martora F, Megna M, Battista T, et al. Adalimumab, Ustekinumab, and Secukinumab in the management of Hidradenitis Suppurativa: a review of the real-life experience. Clin Cosmet Investig Dermatol. 2023;16:135–148. doi:10.2147/CCID.S391356
74. Megna M, Potestio L, Fabbrocini G, Ruggiero A. Long-term efficacy and safety of Guselkumab for moderate to severe psoriasis: a 3-year real-life retrospective study. Psoriasis. 2022;12:205–212. doi:10.2147/PTT.S372262
75. Kamata M, Tada Y. Efficacy and safety of biologics for psoriasis and psoriatic arthritis and their impact on comorbidities: a literature review. Int J Mol Sci. 2020;21(5):1690. doi:10.3390/ijms21051690
76. Ruggiero A, Potestio L, Cacciapuoti S, et al. Tildrakizumab for the treatment of moderate to severe psoriasis: results from a single center preliminary real-life study. Dermatol Ther. 2022;35(12):e15941. doi:10.1111/dth.15941
77. Megna M, Potestio L, Ruggiero A, Camela E, Fabbrocini G. Risankizumab treatment in psoriasis patients who failed anti-IL17: a 52-week real-life study. Dermatol Ther. 2022;35(7):e15524. doi:10.1111/dth.15524
78. Megna M, Potestio L, Ruggiero A, Camela E, Fabbrocini G. Guselkumab is efficacious and safe in psoriasis patients who failed anti-IL17: a 52-week real-life study. J Dermatolog Treat. 2022;1–18. doi:10.1080/09546634.2022.2036674
79. Ruggiero A, Martora F, Picone V, et al. The impact of COVID-19 infection on patients with psoriasis treated with biologics: an Italian experience. Clin Exp Dermatol. 2022;47:2280–2282. doi:10.1111/ced.15336
80. Elmas ÖF, Demirbaş A, Kutlu Ö, et al. Psoriasis and COVID-19: a narrative review with treatment considerations. Dermatol Ther. 2020;33(6):e13858. doi:10.1111/dth.13858
81. Conforti C, Giuffrida R, Dianzani C, Di Meo N, Zalaudek I. Biologic therapy for psoriasis during the COVID-19 outbreak: the choice is to weigh risks and benefits. Dermatol Ther. 2020;33(4):e13490. doi:10.1111/dth.13490
82. Mahil SK, Dand N, Mason KJ, et al. Factors associated with adverse COVID-19 outcomes in patients with psoriasis-insights from a global registry-based study. J Allergy Clin Immunol. 2021;147(1):60–71. doi:10.1016/j.jaci.2020.10.007
83. Ruggiero A, Martora F, Fabbrocini G, et al. The role of teledermatology during the COVID-19 pandemic: a narrative review. Clin Cosmet Investig Dermatol. 2022;15:2785–2793. doi:10.2147/CCID.S377029
84. Megna M, Camela E, Villani A, Tajani A, Fabbrocini G, Potestio L. Teledermatology: a useful tool also after COVID-19 era? J Cosmet Dermatol. 2022;21(6):2309–2310. doi:10.1111/jocd.14938
85. Shi CR, Nambudiri VE. Widespread psoriasis flare following influenza vaccination. Vaccine. 2017;35(36):4785–4786. doi:10.1016/j.vaccine.2017.06.067
86. Ewer KJ, Barrett JR, Belij-Rammerstorfer S, et al. T cell and antibody responses induced by a single dose of ChAdOx1 nCoV-19 (AZD1222) vaccine in a Phase 1/2 clinical trial. Nat Med. 2021;27(2):270–278. doi:10.1038/s41591-020-01194-5
87. Farkas A, Tonel G, Nestle FO. Interferon-alpha and viral triggers promote functional maturation of human monocyte-derived dendritic cells. Br J Dermatol. 2008;158(5):921–929. doi:10.1111/j.1365-2133.2008.08508.x
88. Takayama K, Satoh T, Hayashi M, Yokozeki H. Psoriatic skin lesions induced by BCG vaccination. Acta Derm Venereol. 2008;88(6):621–622. doi:10.2340/00015555-0496
89. Potestio L, Genco L, Villani A, et al. Reply to ‘Cutaneous adverse effects of the available COVID −19 vaccines in India: a questionnaire-based study’. J Eur Acad Dermatol Venereol. 2022;36. doi:10.1111/jdv.18341
90. Picone V, Fabbrocini G, Martora L, Martora F. A case of new-onset lichen planus after COVID-19 vaccination. Dermatol Ther. 2022;12(3):801–805. doi:10.1007/s13555-022-00689-y
91. Picone V, Martora F, Fabbrocini G, Marano L. “Covid arm”: abnormal side effect after Moderna COVID-19 vaccine. Dermatol Ther. 2022;35(1):e15197. doi:10.1111/dth.15197
92. Martora F, Villani A, Battista T, Fabbrocini G, Potestio L. COVID-19 vaccination and inflammatory skin diseases. J Cosmet Dermatol. 2023;22(1):32–33. doi:10.1111/jocd.15414
93. Potestio L, Villani A, Fabbrocini G, Martora F. Cutaneous reactions following booster dose of COVID-19 mRNA vaccination: what we should know? J Cosmet Dermatol. 2022;21:5339–5340. doi:10.1111/jocd.15331
94. Potestio L, Fabbrocini G, D’Agostino M, Piscitelli I, Martora F. Cutaneous reactions following COVID-19 vaccination: the evidence says “less fear”. J Cosmet Dermatol. 2023;22(1):28–29. doi:10.1111/jocd.15533
95. Gisondi P, Geat D, Bellinato F, Girolomoni G. Use of biologics during the COVID-19 pandemic: lessons learned from psoriasis. Expert Opin Biol Ther. 2022;1–9. doi:10.1080/14712598.2022.2110467
96. Papp KA, Haraoui B, Kumar D, et al. Vaccination guidelines for patients with immune-mediated disorders on immunosuppressive therapies. J Cutan Med Surg. 2019;23(1):50–74. doi:10.1177/1203475418811335
97. Stingeni L, Bianchi L, Peris K, et al. SARS-CoV-2 vaccines and biological treatments: dermatological perspectives. Ital J Dermatol Venereol. 2021;156(2):118–120. doi:10.23736/S2784-8671.21.07055-9
98. Martora F, Fabbrocini G, Nappa P, Megna M. Reply to ‘development of severe pemphigus vulgaris following SARS-CoV-2 vaccination with BNT162b2’ by Solimani et al. J Eur Acad Dermatol Venereol. 2022;36(10):e750–e751. doi:10.1111/jdv.18302
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.