")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Safety and Efficacy of Atezolizumab and Bevacizumab Combination as a First Line Treatment of Advanced Hepatocellular Carcinoma
Authors Zanuso V , Pirozzi A , Balsano R, Pressiani T , Rimassa L
Received 13 June 2023
Accepted for publication 20 September 2023
Published 2 October 2023 Volume 2023:10 Pages 1689—1708
DOI https://doi.org/10.2147/JHC.S347932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ahmed Kaseb
Valentina Zanuso,1,2 Angelo Pirozzi,1,2 Rita Balsano,2 Tiziana Pressiani,2 Lorenza Rimassa1,2
1Department of Biomedical Sciences, Humanitas University, Milan, Italy; 2Medical Oncology and Hematology Unit, IRCCS Humanitas Research Hospital, Milan, Italy
Correspondence: Lorenza Rimassa, Humanitas University, Via Rita Levi Montalcini 4, 20072 Pieve Emanuele, Milan, Italy, Tel +39 02 82244573, Fax +39 02 82244590, Email [email protected]
Abstract: Hepatocellular carcinoma (HCC) is one of the most common leading causes of cancer death worldwide. As most patients are diagnosed with advanced disease, systemic therapy remains the backbone of treatment. In recent years, we have witnessed the transformation of advanced HCC treatment landscapes from single-agent targeted therapies to immunotherapy combinations, with atezolizumab plus bevacizumab becoming the new first-line standard of care with an increase in overall survival, progression-free survival, and objective response rate compared to sorafenib, and a positive impact on quality of life. Although the efficacy and safety of this combination have been confirmed regardless of ethnicity, age, and etiology, only a subgroup of patients seems to benefit the most from this treatment. Currently, predictive serum and tissue biomarkers to select patients who are most likely to respond to atezolizumab plus bevacizumab are lacking. Moreover, the optimal subsequent therapy for patients who progress on first-line atezolizumab plus bevacizumab remains unknown, clinical trials are ongoing, and real-world data are needed to determine the most effective treatment sequence. Importantly, careful evaluation of bleeding risk and preservation of adequate liver function are fundamental to improve patients’ prognosis, especially when subsequent treatments are administered.
Keywords: HCC, immune checkpoint inhibitors, atezolizumab, bevacizumab, safety, efficacy
Introduction
Hepatocellular carcinoma (HCC) is a global health issue with increasing incidence and mortality worldwide. It generally emerges within a chronic liver disease condition, which includes chronic viral hepatitis (hepatitis C virus [HCV] and hepatitis B virus [HBV]), alcoholic cirrhosis, metabolic conditions (metabolic dysfunction-associated fatty liver disease [MAFLD], previously known as non-alcoholic fatty liver disease [NAFLD], metabolic dysfunction-associated steatohepatitis [MASH], previously known as non-alcoholic steatohepatitis [NASH], diabetes), and aflatoxin exposure.1,2 Unfortunately, most patients are diagnosed with advanced disease or progress after locoregional approaches and therefore, systemic therapies represent the backbone of treatment. Systemic treatment is indicated for patients with advanced or intermediate HCC that are unsuitable for locoregional treatment and with preserved liver function.1,3 After more than a decade of multi-kinase inhibitors (MKIs) monopoly, in 2020, the combination of atezolizumab plus bevacizumab became the new first-line standard of care, introducing immunotherapy in advanced HCC and contributing to the reshaping of HCC treatment algorithm, with an increase in survival. In this review, we will shed light on atezolizumab plus bevacizumab, starting from clinical studies that led to the approval of this combination, focusing on safety and efficacy data, and then moving to more recent exploratory analyses and real-life studies, evaluating future perspectives of HCC treatment strategies and sequential therapies. Moreover, we want to highlight the urgent need to identify predictive biomarkers to properly select patients and obtain durable clinical benefits in those who are more likely to respond, sparing adverse events in non-responders.
Overview of Current Systemic Treatment Landscape
Sorafenib, a MKI, has been the mainstay of advanced or metastatic HCC treatment since 2007.4,5 A decade later, new targeted agents have been approved in either the first or subsequent lines. In detail, lenvatinib was found to be non-inferior to sorafenib in the first-line setting.6 Regorafenib, cabozantinib, and ramucirumab were approved in the refractory context, with cabozantinib showing efficacy even in the third line.7–9 Furthermore, regorafenib demonstrated efficacy in a sorafenib-tolerant population, whereas ramucirumab showed improved survival in patients with alpha-fetoprotein (AFP) levels ≥400 ng/mL at baseline.7,9
Recently, the advent of immunotherapy has dramatically changed the first-line therapeutic scenario, resulting in a widening of treatment opportunities. In 2020, the combination of the anti-programmed death ligand-1 (PD-L1) atezolizumab plus the anti-vascular endothelial growth factor (VEGF) bevacizumab became the new first-line standard of care, outperforming sorafenib.10–12 Similarly, sintilimab (anti-programmed cell death protein-1 [PD-1]) combined with a bevacizumab biosimilar (IBI305) showed significant overall survival (OS) and progression-free survival (PFS) benefit compared to sorafenib in a phase 3 trial only enrolling patients from China.13 More recently, the combination of a single priming dose of the anti-cytotoxic T-lymphocyte antigen-4 (CTLA-4) monoclonal antibody (mAb) tremelimumab plus the anti-PD-L1 mAb durvalumab (STRIDE regimen) obtained the United States Food and Drug Administration (FDA) and European Medicines Agency (EMA) approval as first-line treatment option based on the positive results of the phase III HIMALAYA trial.14 Moreover, single-agent tislelizumab demonstrated non-inferior OS compared to sorafenib, and the combination of camrelizumab plus rivoceranib significantly prolonged survival compared to sorafenib.15,16 Conversely, first-line nivolumab did not significantly improve OS compared with sorafenib, even though clinical activity and a favorable safety profile were observed.17 In the phase III COSMIC-312 trial cabozantinib plus atezolizumab significantly improved only one of the dual primary endpoints (PFS, but not OS) versus sorafenib,18 whereas the combination of pembrolizumab plus lenvatinib was not shown to improve survival versus lenvatinib in the phase III LEAP-002 trial.19
The results of phase III trials with immune-checkpoint inhibitor (ICI)-based treatment in the first-line setting are summarized in Table 1. Table 2 summarizes the efficacy data of the currently approved first-line treatment options.
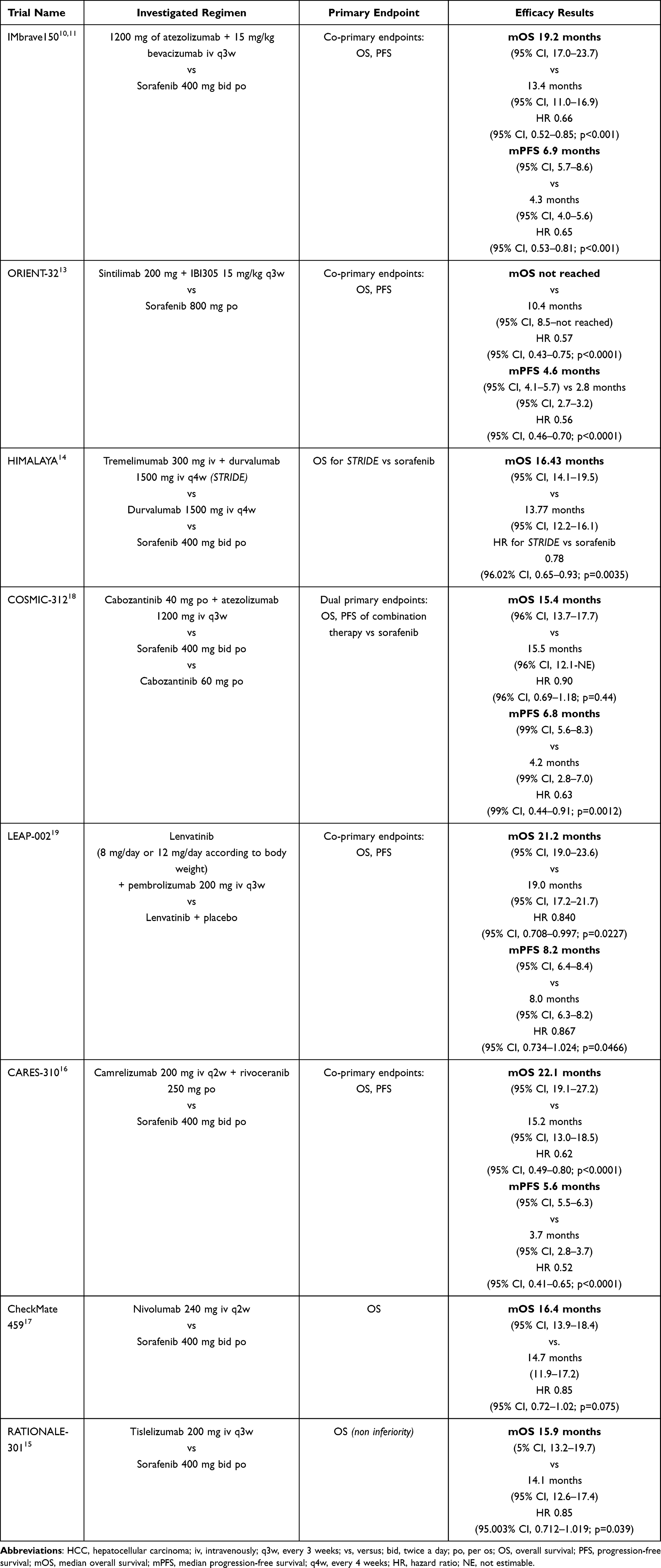 |
Table 1 Phase III Trials of Immune-Checkpoint Inhibitor-Based Treatment in the First-Line Setting |
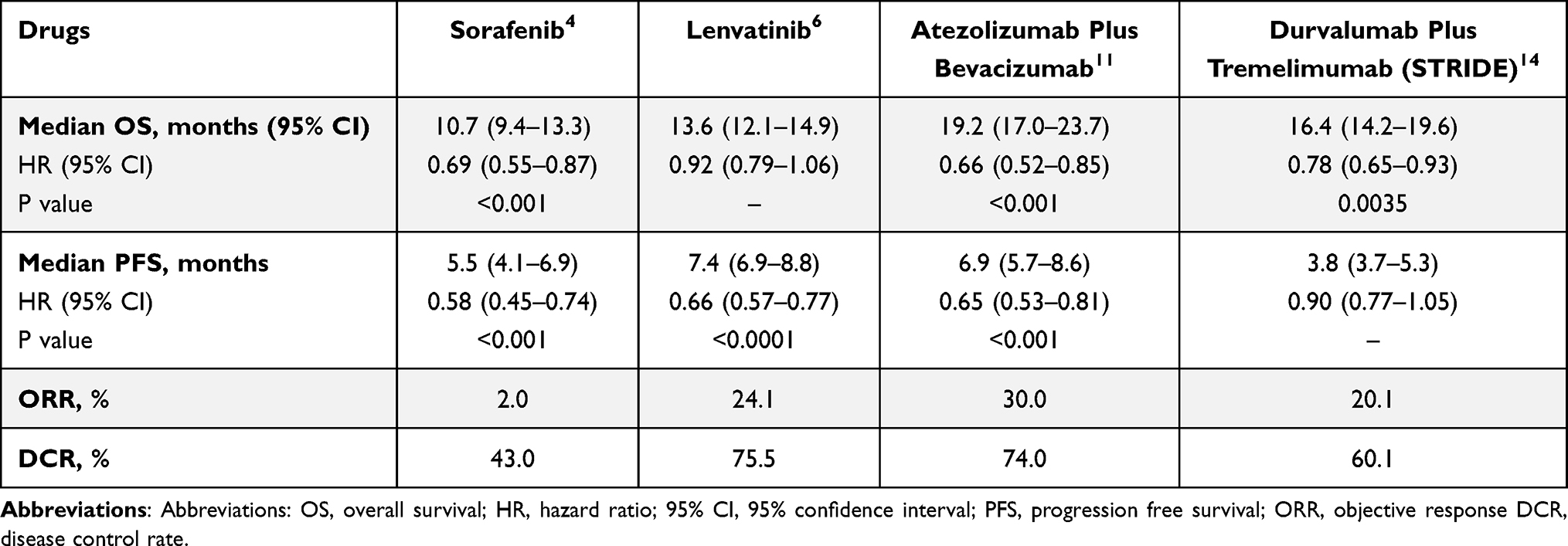 |
Table 2 Efficacy of Currently Approved First-Line Treatment Options for Advanced HCC |
ICIs have also been tested in subsequent studies and have yielded inconsistent results. The combination of nivolumab plus ipilimumab and pembrolizumab monotherapy received FDA approval in the second-line setting after sorafenib failure, based on phase II results.20–22 However, the subsequent phase III trials testing first-line nivolumab and second-line pembrolizumab did not meet their primary endpoints, with the exception of the phase III KEYNOTE-394 trial, which reported positive results for pembrolizumab in an Asian population.17,23,24
Clinical Efficacy and Safety of Atezolizumab Plus Bevacizumab
The Phase Ib GO30140 Trial
GO30140 is an open-label, multi-arm, phase Ib study exploring the combination of atezolizumab plus bevacizumab in multiple solid tumor cohorts, including two cohorts (groups A and F) composed of patients with unresectable HCC, not previously treated with systemic therapy.25 Bevacizumab is an anti-angiogenic agent that normalizes the tumoral vasculature and has additional immunomodulatory effects. In particular, it increases T cell infiltration and decreases the activity of immunosuppressive cells, such as myeloid-derived suppressor cells (MDSCs) and regulatory T cells (Tregs). Moreover, it also promotes dendritic cells (DCs) maturation. In contrast, atezolizumab promotes T-cell activation and restores anticancer immunity by enhancing anti-VEGF-mediated immunomodulatory effects.26 Figure 1 illustrates the mechanism of action of bevacizumab and atezolizumab.
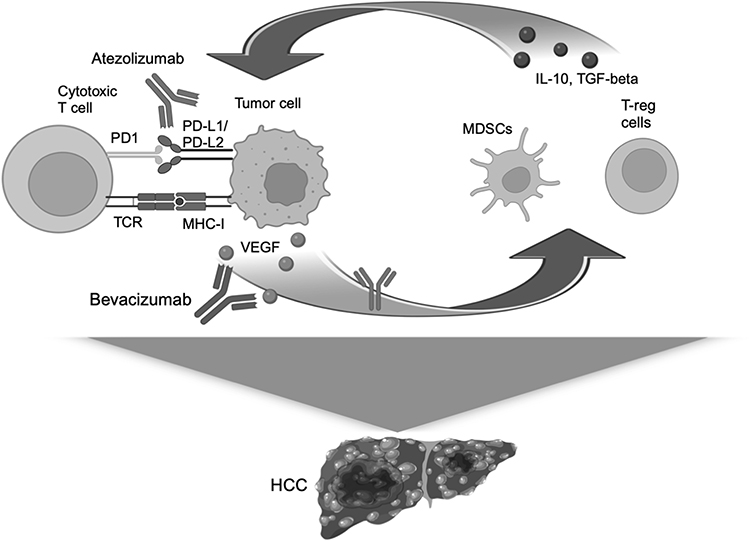 |
Figure 1 Mechanism of action of atezolizumab and bevacizumab. Atezolizumab and bevacizumab act on a positive feedback loop made of VEGF released by tumor cells and inhibitory cytokines produced by MDSCs and T-reg cells. The inhibitory cytokines in turn increase the expression of PD-L1 on tumor cells inducing immune system inhibition. Abbreviations: HCC, hepatocellular carcinoma; IL-10, interleukin 10; MHC-I, major histocompatibility complex I; MDCSs, medullary dendritic stem cells; PD1, programmed cell death protein 1; PD-L1, programmed death-ligand 1; PD-L2, programmed cell death protein ligand 2; TCR, T-cell receptor; TGF-beta, transforming growth factor β; VEGF, vascular endothelial growth factor. Note: Created with BioRender.com. |
In group A, all patients received 1200 mg of atezolizumab plus bevacizumab 15 mg/kg intravenously every 3 weeks. The primary endpoint was objective response rate (ORR) according to independent review facility assessment by response evaluation criteria in solid tumors version 1.1 (RECIST 1.1).27 Secondary endpoints included investigator-assessed ORR according to RECIST 1.1, independent review facility assessment by hepatocellular carcinoma-specific modified RECIST (mRECIST),28 PFS, duration of response (DOR), time to radiographic disease progression, OS, and safety.
In group F, the patients were randomized to receive atezolizumab plus bevacizumab or atezolizumab monotherapy, and the primary endpoint was PFS according to RECIST 1.1, whereas PFS according to mRECIST, ORR, DOR, time to radiographic disease progression, OS, and safety were all secondary endpoints.
Patients were stratified according to geographical region (Asia versus the rest of the world, including Japan), macrovascular invasion (MVI) and/or extrahepatic spread (EHS) (presence versus absence), and baseline AFP levels (<400 versus ≥400 ng/mL). In both groups, most patients were from Asia, had EHS, and baseline AFP levels <400 ng/mL. MVI was most common in group A (53%). Considering baseline liver function, >70% of patients were Child-Pugh A5. Regarding etiology, HBV was the most common underlying cause of HCC. The results demonstrated a benefit for patients receiving a combination of atezolizumab and bevacizumab in both groups A and F. After a median follow-up of 12.4 months (InterQuartile Range [IQR] 8.0–16.2)], among 104 patients enrolled in group A, the ORR was 36% (95% CI, 26–46), comprising 12% of complete response (CR), and 76% of the responders had an ongoing response at the data cutoff. The median DOR was not reached, and responses of 6 months or longer were reported in 24 patients; the median time to radiographic progression was 8.9 months (95% CI, 5.6–13.6). The median OS was 17.1 months (95% CI, 13.8-Not Estimable [NE]), with 55% of the patients alive at the data cut-off.
Similar results were reported in group F, which enrolled 119 patients: 60 in the atezolizumab plus bevacizumab arm and 59 in the monotherapy arm. After a median follow-up of 6.6 months (IQR 5.5–8.5) in the combination arm and 6.7 months (IQR 4.2–8.2) in the monotherapy arm, a longer PFS was observed with atezolizumab plus bevacizumab (median PFS 5.6 months versus 3.4 months [HR 0.55; 80% CI, 0.40–0.74; p=0.011]). Among the secondary endpoints, the median OS was not reached in either group (atezolizumab plus bevacizumab: 95% CI, 8.3-NE; atezolizumab monotherapy: 95% CI, 8.2-NE). ORRs were 20% and 17%, with 2% and 5% of CR, respectively.
Notably, 26 patients crossed over and received combination treatment after the failure of atezolizumab monotherapy. In a post hoc analysis, the addition of bevacizumab showed possible benefits in terms of disease control and PFS.29
The potential correlation between PD-L1 expression and treatment efficacy was investigated in an exploratory analysis, which confirmed the efficacy irrespective of PD-L1 status in groups A and F.
In group A, grade 3–4 adverse events (AEs) were reported in 53% of patients, mainly represented by hypertension (13%) and proteinuria (7%). Serious AEs were reported in 44% of the patients, while treatment-related serious AEs were observed in 24% of the patients, and the most common were esophageal varices, upper gastrointestinal hemorrhage, colitis, and pneumonitis. 48% of patients experienced treatment-related adverse events (TRAEs) leading to dose modification or treatment interruption, whereas AEs leading to treatment discontinuation occurred in 17% of patients.
In group F, 37% of the patients receiving combination therapy had grade 3–4 AEs (most common hypertension in 5% of the patients), while grade 3–4 AEs were observed in 14% of the patients receiving atezolizumab alone (proteinuria in 3%). Serious AEs were reported in 25% of the patients in the atezolizumab plus bevacizumab arm and in 10% of the patients in the monotherapy arm. Moreover, 12% and 3% of the patients in the combination and monotherapy arms, respectively, had serious treatment-related AEs. TRAEs leading to treatment reduction or interruption occurred in 15% of the patients in the combination group and in 9% of the patients in the monotherapy group.
The Phase III IMbrave150 Trial
The efficacy demonstrated in the GO30140 trial led to further evaluation of atezolizumab plus bevacizumab compared with sorafenib in the open-label phase III IMbrave150 study.10,11
The included patients had unresectable, cytologically or histologically confirmed HCC, except for those whose clinical features were suggestive of HCC, according to the American Association for the Study of Liver Diseases (AASLD) criteria. Moreover, they had to be treatment-naïve, with a good performance status (Eastern Cooperative Oncology Group [ECOG] score of 0 or 1) and Child-Pugh class A liver function. Autoimmune diseases, HBV and HCV coinfection, untreated esophageal and gastric varices with bleeding were excluded, and all patients underwent esophagoduodenoscopy (EGD) at baseline before receiving treatment. Stratification factors included geographical region (Asia versus the rest of the world, including Japan), MVI and/or EHS (presence versus absence), and baseline AFP levels (<400 versus ≥400 ng/mL). Differently from the phase Ib trial, most patients were non-Asiatic (60%). MVI was most common in the sorafenib group (43%), whereas EHS was most common in patients receiving atezolizumab plus bevacizumab (63%). As seen in the GO30140 trial, HBV was the most frequent cause of HCC.
The study enrolled 501 patients randomized in a 2:1 ratio to receive atezolizumab 1200 mg plus bevacizumab 15 mg/kg intravenously every 3 weeks or sorafenib 400 mg twice daily until unacceptable toxicity or loss of clinical benefit was observed. In the experimental arm, patients could discontinue atezolizumab or bevacizumab owing to toxicity by investigator choice and continue with single-agent treatment.
The two co-primary endpoints were OS and PFS according to RECIST 1.1. The ORR, DOR per RECIST 1.1 and per mRECIST,27,28 time to deterioration of quality of life, physical functioning, and role functioning according to the EORTC QLQ-C30 were the secondary endpoints.
After a median follow-up of 8.6 months, the combination of atezolizumab and bevacizumab showed a significant benefit in terms of both co-primary endpoints. Median PFS was longer in the combination arm (6.8 months; 95% CI, 5.7–8.3) than sorafenib (4.3 months; 95% CI, 4.0–5.6).10 The updated study results confirmed the advantage of atezolizumab plus bevacizumab versus sorafenib. After a median follow-up of 15.6 months, median OS was 19.2 months (95% CI, 17.0–23.7) versus 13.4 months (95% CI, 11.0–16.9) (HR 0.66; 95% CI, 0.52–0.85; p<0.001), and median PFS was 6.9 months (95% CI, 5.7–8.6) versus 4.3 months (95% CI, 4.0–5.6) (HR 0.65; 95% CI, 0.53–0.81; p<0.001).11 The survival benefit was maintained across most of the prespecified subgroups.
Positive results for atezolizumab plus bevacizumab were also observed at the secondary endpoints. The updated results confirmed the higher ORR of the combination treatment according to RECIST 1.1 (29.8% [95% CI, 24.8–35.0] versus 11.3 [95% CI, 6.9–17.3]) and mRECIST (35.4 [95% CI, 30.2–40.9] versus 13.9 [95% CI, 8.9–20.3]).11
The updated median DOR was 18.1 months (95% CI, 14.6-NE) and 14.9 months (95% CI, 4.9–17.0) in the experimental and control arm, respectively.11 Efficacy data are summarized in Table 3.
 |
Table 3 Efficacy Outcomes of the Phase III IMbrave150 Trial (Updated Analysis)11 |
Regarding safety and tolerability, AEs of any grade were reported in 98.2% and 98.7% of patients receiving atezolizumab plus bevacizumab and sorafenib, respectively.
Serious AEs occurred more frequently in the combination treatment arm (49%) than in the sorafenib arm (33%) and were mainly gastrointestinal hemorrhage (2.4% versus 1.9%), esophageal variceal hemorrhage (2.4% versus 0.6%), and pyrexia (2.1% vs 1.3%).11
Grade 3–4 TRAEs occurred in 43% of the patients in the atezolizumab plus bevacizumab arm and 46% of the patients in the sorafenib arm. The most frequently reported grade 3–4 TRAEs in the combination arm were hypertension (12%), aspartate aminotransferase (AST) increase (5%), and proteinuria (4%), whereas hypertension (9%), palmar-plantar erythrodysesthesia (8%), and diarrhea (4%) were the most frequently reported grade 3–4 sorafenib-related AEs.
Considering upper gastrointestinal bleeding, there were 5 grade 5 events in the combination arm, but only 1 event that occurred within 3 months of the first dose administration was related to the study treatment. The other four bleeding events occurred four or more months after the first dose and were more likely to be related to disease progression. All patients who experienced grade 5 bleeding had macrovascular invasion, 3 had baseline varices, and 1 had hypertensive gastropathy.
AEs leading to dose interruptions or modifications occurred in 44% and 37% of the patients in the sorafenib group, respectively. AEs led to the discontinuation of any treatment component in 15.5% of the patients who received atezolizumab plus bevacizumab and 10.3% of those who received sorafenib. Gastrointestinal AEs were the main cause of the discontinuation of atezolizumab plus bevacizumab. In the sorafenib group, worsening of liver function and skin toxicity were the main causes of treatment discontinuation. The safety data are summarized in Table 4.
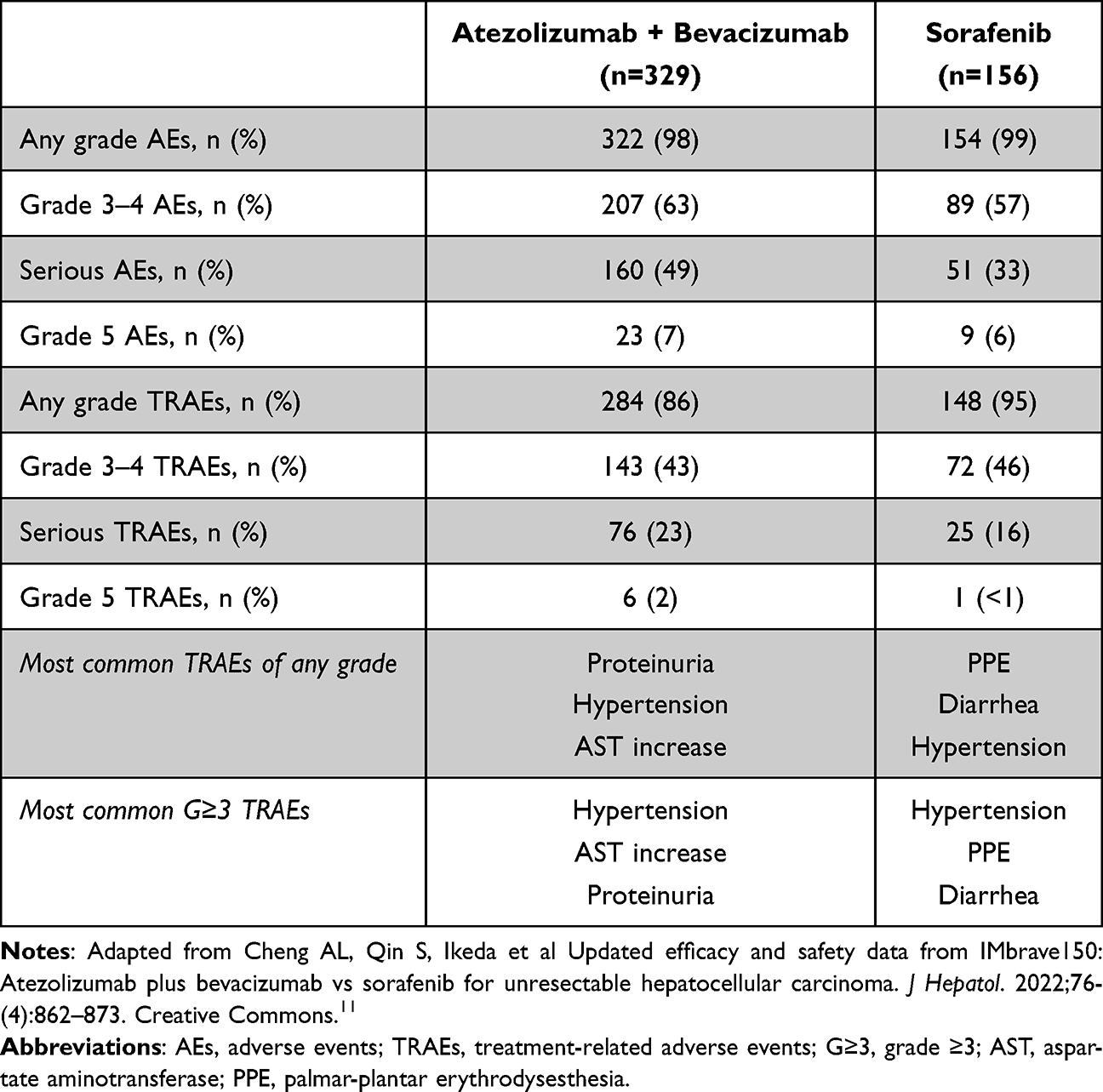 |
Table 4 Safety Profile of the Combination of Atezolizumab Plus Bevacizumab Reported in the Phase III IMbrave150 Trial (Updated Analysis)11 |
A preplanned analysis was conducted among the Chinese population, including 137 patients from the IMbrave150 intention-to-treat (ITT) population and 57 patients from an extension cohort.30 In this group, median OS was 24.0 months (95% CI, 17.1-NE) with atezolizumab plus bevacizumab versus 11.4 months (95% CI, 6.7–16.1) with sorafenib. The ORR were 30% in the combination arm (8% CR) and 8% in the control arm (no CR). Moreover, the combination delayed the median time to deterioration (TTD) in quality of life (QoL) compared with sorafenib.
Quality of Life Assessment
QoL is an essential issue for patients with HCC, mainly due to the impact of the disease on liver function, with remarkable consequences on daily habits. Regarding patient-reported outcomes (PROs) in the IMbrave150 trial, atezolizumab plus bevacizumab showed a statistically significant and clinically meaningful difference in median TTD for QoL (11.2 vs 3.6 months; HR 0.63; 95% CI, 0.46–0.85).11 Similar results in median TTD were recorded for physical functioning (13.1 vs 4.9 months; HR 0.53; 95% CI, 0.39–0.73) and role functioning (9.1 vs 3.6 months; HR 0.62; 95% CI, 0.46, 0.84). As far as the onset of key symptoms and functioning domains is concerned, the combination doubled the median time to fatigue onset (5.7 vs 2.1 months; HR 0.60; 95% CI, 0.45–0.80) assessed by both QLQ-HCC18 and QLQ-C30 questionnaires. Lastly, a striking improvement in median time to pain onset (9.7 vs 2.8 months; HR 0.46; 95% CI, 0.34–0.62) was reported.31,32 These data further support the use of atezolizumab plus bevacizumab, confirming the positive impact of the combination on patients QoL.
IMbrave150 Post-Hoc Exploratory Analyses
Given the clinically meaningful benefits of atezolizumab plus bevacizumab versus sorafenib, these results were also investigated in the specific subgroups of patients included in the trial.
In a post-hoc analysis, the combination of atezolizumab plus bevacizumab showed consistent survival and ORR benefit in older patients (≥ 65 years).33 In the elderly population, median OS was 19.4 months in the combination arm versus 14.9 months in the sorafenib arm (HR 0.80; 95% CI, 0.52–1.23), and median PFS was 7.7 versus 5.3 months (HR 0.67; 95% CI, 0.46–0.98). The ORR was 27.5% with atezolizumab plus bevacizumab versus 13.1% with sorafenib, and 4.9% of patients who received the combination achieved CR. Importantly, despite the higher rate of baseline comorbidities, no significant added toxicities were observed in older patients, and the combination treatment delayed TTD in multiple PROs.
Regarding safety, AEs of special interest (AESI) were analyzed. AESI for atezolizumab included dermatological, gastrointestinal, and endocrinological AEs, whereas AESI for bevacizumab included hypertension and bleeding, mainly from the upper gastrointestinal tract. 76% of patients in the experimental arm reported AESI, and the most common was immune-mediated hepatitis, including diagnostic and laboratory abnormalities. 12% of patients who developed AESI received systemic corticosteroids within 30 days of onset.34
The use of atezolizumab plus bevacizumab is supported also in the subgroup of patients with high risk-factors, defined as tumor invasion of the main trunk of the portal vein and/or the portal vein branch contralateral to the primarily involved lobe (Vp4), and/or bile duct invasion, and/or tumor occupancy ≥50% of the liver.35 Even though the baseline characteristics were poorer, the treatment benefit was maintained and the increased risk in variceal bleeding and gastrointestinal hemorrhage was consistent with the underlying disease condition. Specifically looking at Vp4 patients, median OS and median PFS were 7.6 and 5.4 months respectively (versus 5.5 and 2.8 months with sorafenib).36 Similarly, the survival benefit was consistent in patients with varices at baseline (median OS 17.7 months with atezolizumab plus bevacizumab versus 8.6 months with sorafenib; median PFS 7.0 months versus 4.2 months), as well as the higher ORR (26% versus 7%).37 Considering the higher risk of hemorrhage in this subgroup of patients, grade 3 or higher gastrointestinal bleeding occurred in 20 out of 87 patients (23%), leading to bevacizumab discontinuation in 9% of patients and both drugs discontinuation in 3%.
The benefit of atezolizumab plus bevacizumab was also maintained in patients without MVI or EHS.38 Of the 111 patients without MVI or EHS, 72 received atezolizumab plus bevacizumab and 39 received sorafenib alone. More than half of the patients (51% in the combination arm and 62% in the sorafenib group) had prior locoregional treatment (LRT). The median OS was 24.6 months for atezolizumab plus bevacizumab and 18.1 months for sorafenib alone (HR, 0.58; 95% CI, 0.34–1.01). CR was observed in 10% of the patients receiving combination therapy and in none of the patients in the control group. Grade 3–4 TRAEs occurred in 61 patients (49%) treated with atezolizumab plus bevacizumab and 38 patients (47%) treated with sorafenib. Hence, the safety outcomes were consistent with those reported in the ITT population.
Efficacy results have been confirmed in 74 Barcelona Clinical Liver Cancer (BCLC) stage B patients, supporting the use of atezolizumab plus bevacizumab in patients not suitable for or progressing on LRT.39 In detail, there was a trend towards improved OS and PFS with atezolizumab plus bevacizumab versus sorafenib (HR for OS 0.63; 95%, CI 0.29–1.34; HR for PFS 0.64; 95% CI, 0.36–1.12). The ORRs per RECIST 1.1 and mRECIST were 43% and 50% with the combination treatment and 26% and 30% with sorafenib, respectively.
In addition, the survival benefit seems to be maintained regardless of prior LRT.40 Median OS was 19.4 months in patients without prior LRT, 22.8 months in patients who underwent 1–2 prior LRTs, and 17.4 months in patients receiving at least 3 prior LRTs. Grade ≥3 AEs in patients with none, 1–2, and at least three LRTs were 46%, 39%, and 31%, respectively.
In another exploratory analysis, patients with albumin-bilirubin (ALBI) grade 1 had a greater survival benefit with atezolizumab plus bevacizumab than with sorafenib, with a longer time to liver function deterioration. The safety profile of atezolizumab plus bevacizumab was maintained regardless of the ALBI grade and was consistent with the drug safety profile as well as the underlying liver condition.41 Interestingly, neither hepatic impairment nor geographical origin had a clinically relevant impact on the pharmacokinetics of the combination, as well as its safety.42
In a further analysis of survival by type of response, patients treated with atezolizumab plus bevacizumab experienced a confirmed response (CR or partial response [PR]) and improved OS (HR 0.13, p<0.01). Similarly, improved OS was observed in patients with SD (HR 0.36, p<0.01).43
According to the trial design, patients could continue treatment beyond progression if clinical benefits were maintained, and in the absence of signs and symptoms unequivocally attributed to progressive disease (PD). Patients treated with atezolizumab beyond radiological progression had a median OS from baseline and from PD of 24.1 months (95% CI, 20.2-NE) and 14.5 months (95% CI, 11.5–16.7), respectively.44 Patients who received other treatment than atezolizumab or did not receive any treatment after PD had a median OS of 6.8 months (95% CI, 4.9–11.5) and 2.0 months (95% CI, 1.6–3.0) from PD. Grade 3–4 TRAEs occurred in 21 patients (16%) who continued atezolizumab beyond progression.
The effects of anti-drug antibodies (ADAs) on clinical outcomes were also evaluated. Although almost 30% of patients developed ADAs, the efficacy of the combination was confirmed, and ADA development during treatment did not significantly affect the AE rate.45
Regarding etiology, in the non-viral population, a relative benefit in PFS and ORR of atezolizumab plus bevacizumab versus sorafenib has been suggested, whereas OS was similar between the two treatment arms.46 In a recently published post-hoc analysis, there was no significant difference in the proportion of patients with an objective response across different etiologies. Moreover, there was no significant difference in terms of median PFS and median OS.47
Further analyses were performed to evaluate the potential effects of the concomitant medications. 21.5% of the patients treated with atezolizumab plus bevacizumab and 21.8% of those receiving sorafenib were exposed to early antibiotic use. Interestingly, early antibiotic exposure was associated with a negative impact on survival, suggesting a potential effect of gut dysbiosis on treatment response, which requires further investigation.48
Finally, in a recent analysis, skipping bevacizumab did not have a consistent effect on the efficacy of atezolizumab plus bevacizumab.49
The Phase IIIb AMETHISTA Study and Real-World Evidence
The ongoing Italian phase IIIb AMETHISTA study enrolled 152 patients treated with atezolizumab plus bevacizumab to further explore the safety and efficacy of the combination, and the preliminary results were consistent with those of the IMbrave150 trial.50,51
The AB-real study collected data from 433 patients treated with atezolizumab plus bevacizumab for advanced HCC across Europe, Asia, and USA.52 They were Child-Pugh A patients, mainly with BCLC-C stage (68%), cirrhosis (75%), and history of viral hepatitis (65.9%). Portal vein tumor thrombosis (PVTT) and EHS were observed in 35.0% and 51.7% of the patients, respectively. The median PFS was 6.9 months (95% CI, 6.1–8.3), whereas the median OS was 15.7 months (95% CI, 14.5-NE). The ORR was 30.8% (2.9% of CR and 27.8% of PR), with a median time to best response of 1.6 months (IQR 1.3–2.8). Grade 3 or 4 TRAEs were reported by 23.6% of patients, and the most common were hepatotoxicity and proteinuria. Overall, these results are comparable to those reported in the IMbrave150 trial, demonstrating the external validity of the outcomes of atezolizumab plus bevacizumab in advanced HCC. In addition, the study evaluated the role of possible prognostic factors. In the multivariate analysis, the presence of PVTT and higher ALBI grade were independent prognostic factors for OS. Furthermore, the presence of PVTT and a higher ALBI grade and Child-Pugh score were associated with a higher incidence of bleeding events. Considering the ALBI grade, median OS was NE (95% CI, 16.9-NE) in patients with ALBI grade 1 and 10.0 months (95% CI, 8.6–12.3) in patients with ALBI grade 2, whereas median OS was 10.0 months (95% CI, 8.88-NE) and 17.0 months (95% CI, 15.0-NE) in patients with and without PVTT, respectively. Moreover, the presence of EHS was an independent prognostic factor for PFS, and patients with radiological response had a significantly longer OS.
Likewise, the results of the multicenter European Field of Practice Study of Atezolizumab And Bevacizumab in Hepatocellular Carcinoma (EURAB-HCC) study support the survival outcomes of the IMbrave150 trial and highlight the importance of liver function as a fundamental determinant of outcome.53 This study included data from 471 patients receiving atezolizumab plus bevacizumab between 1st July 2020 and 31st March 2022 at 15 European centers. The median OS was 16.6 months in patients with Child-Pugh A liver function versus 6.0 months in Child-Pugh B patients. Regarding AEs, 23 episodes of gastrointestinal bleeding were reported, of which four resulted in patient death.
Considering the bevacizumab-related risk of acute variceal bleeding (AVB), we still lack useful predictive factors in clinical practice. In a prospective study including 43 cirrhotic patients treated with atezolizumab plus bevacizumab, no significant difference in hepatic venous pressure gradient (HVPG) was observed between baseline, and after 3 and 6 months from treatment start. Moreover, there was no significant variation in the size of esophageal varices between baseline and after 6 months of treatment. Interestingly, a previous history of AVB was associated with a higher risk of relapse during treatment (HR 10.58, p=0.03).54 Due to the increased risk of bleeding, primary prophylaxis with non-selective beta-blockers or band ligation is recommended in all patients with esophageal varices, as beta-blockers are helpful also to treat portal hypertension. In addition, the combination of non-selective beta-blockers and band ligation should be the first treatment choice to prevent re-bleeding.55,56
In a retrospective real-world study, the efficacy and safety of atezolizumab plus bevacizumab were evaluated in 202 patients with advanced HCC.57 The median OS was 14.9 months (95% CI, 13.6–16.3). Median OS in Child-Pugh A patients was 16.8 months (95% CI, 14.1–23.9) and 6.7 months in Child-Pugh B patients (95% CI, 4.5–15.6) (p=0.0003). Median PFS was 7.6 months (95% CI, 6.2–8.9) and 3.4 months (95% CI, 2.6–4.2) in patients with Child-Pugh A and Child-Pugh B class, respectively (p=0.03). The ORR was similar across Child-Pugh classes (26% versus 21%) and was not influenced by BCLC stage, ECOG performance status (PS), or etiology. Moreover, there were no differences in toxicity. Bevacizumab-related AEs were reported in 48% and 46% of Child-Pugh A and B patients, respectively, whereas bevacizumab-related grade 3–4 AEs were reported in 16% and 15% of patients, respectively. Gastrointestinal bleeding events were also comparable (14% versus 15% for any grade and 4% versus 10% for grade 3 or higher). Moreover, bleeding events were not associated with BCLC stage, presence of varices at pre-treatment EGD, administration of prophylactic treatment for varices, or baseline PVTT. Overall, these data support the use of atezolizumab plus bevacizumab in clinical practice and suggest further evaluation of its application in Child-Pugh class B patients.
In another retrospective real-world study of 216 patients treated with first-line atezolizumab plus bevacizumab, the combination confirmed its safety profile and ALBI grade and ECOG PS were reported as independently associated with survival.58 In a further recent study, the ALBI grade was independently associated with OS and PFS in multivariate models (p<0.001).59 Furthermore, pre-treatment ALBI was associated with higher risk of bleeding (3.1% in ALBI 1 versus 10.2% in ALBI 2/3).
Considering the Asiatic population, in a Japanese retrospective, real-world clinical practice study including 61 patients with unresectable HCC, median PFS was 5.4 months, and the overall ORR was 35.3%.60 The incidence of grade 3 or higher AEs was 29.4%, mainly represented by AST and alanine aminotransferase (ALT) increase and hypertension. Additionally, there was no significant difference in efficacy or AEs according to ALBI grade. ORR was similar in patients previously treated with targeted agents, suggesting the potential efficacy of atezolizumab plus bevacizumab, even in pretreated patients. In a more recent retrospective study, the rate of bevacizumab interruption due to TRAEs was significantly higher in patients with hypertension and/or diabetes.61 Since metabolic syndrome prevalence is increasing worldwide, this evidence is worth of further evaluation. Similar safety and efficacy profiles have been observed in Thailand and Korea.62,63
The efficacy and safety of atezolizumab plus bevacizumab in older patients was confirmed in clinical practice.64 191 consecutive patients from 8 centers were stratified according to their age: 116 elderly (age ≥65 years) and 75 younger (age <65 years) patients. Median OS was similar between younger and older patients (15.1 months vs 14.9 months; HR 1.15; 95% CI, 0.65–2.02; p=0.63), as well as median PFS (7.1 months versus 15.1 months; HR 1.11; 95% CI, 0.54–1.02; p=0.72) and ORR (27.6% versus 20.0%; p=0.27). TRAEs of grade 3 or higher were comparable between the two groups (20.7% vs 20.0%; p=0.9).
Finally, contrary to what was reported in the IMbrave150 trial, high ADA levels were shown to be associated with reduced exposure to atezolizumab, thus limiting its antitumor activity. In a cohort study, serum ADA levels were analyzed at baseline and at 3 weeks, and highly elevated ADAs at 3 weeks (≥1000 ng/mL) were associated with poor clinical outcomes.65 However, this analysis was conducted in a limited number of Korean patients in an endemic HBV region, requiring further evaluation in a larger number of patients with other ethnicities and etiologies. Moreover, the study was conducted focusing on an early time point and did not evaluate the prevalence of neutralizing antibodies that occurred later.
Biomarkers
The combination of atezolizumab and bevacizumab has become the new first-line standard of care for patients with advanced HCC; however, the potential predictive biomarkers and mechanisms of response and resistance remain unclear.
The most informative data were obtained from an extensive biomarker analysis of 358 baseline tumor tissues, including 181 samples from the GO30140 trial and 177 samples from the IMbrave150 trial.10,25 The analysis consisted in collection of transcriptomic and genomic data. Transcriptomic tests evaluated genome wide-differential gene expression analysis (GSEA) as well as pathway/immune subset signatures and their association with RECIST response and survival. Genomic data included tumor mutation burden (TMB), neoantigen load, somatic mutations assessment and their association with efficacy outcomes.66 At the final analysis, high expression of CD274, T-effector signature and intra-tumoral CD8+ T cell density were associated with positive outcomes of efficacy, whereas worse outcomes were reported with high Treg to effector T cell (Teff) ratio and expression of oncofetal genes (GPC3, AFP).
Data from the GO30140 trial allowed the identification of molecular and cell patterns as predictors of response matching with either the combination of atezolizumab plus bevacizumab or atezolizumab alone. Interestingly, this combination was more effective in patients with higher vascular endothelial growth factor receptor 2 (VEGFR-2) expression, Tregs, and myeloid inflammation signatures.66
A still debated question is using AFP as a surrogate endpoint for OS and PFS. An exploratory analysis of both GO30140 and IMbrave150 trials elicited remarkable results. The goal was to identify AFP cutoffs to divide patients into responders and non-responders, and to assess the correlation between OS and PFS. AFP cutoff values of ≥75% decrease and ≤10% increase from baseline at 6 weeks were derived to distinguish responders from non-responders and patients with disease control from those with progressive disease.
Both AFP cutoff values were associated with statistically significant improvements in OS and PFS, especially in HBV positive patients (HR <0.50; p <0.05).67 Results from this analysis may be clinically useful for predicting the efficacy of the combination during treatment, helping with patient management. Furthermore, interesting results were obtained from a retrospective analysis of 371 patients from the IMbrave150 trial, which evaluated the combination of baseline insulin-like growth factor 1 (IGF-1) and Child-Pugh score as independent prognostic factors. Circulating IGF-1 levels were categorized as high (>50 ng/mL; point 1), normal (26–50 ng/mL; point 2), or low (<26 ng/mL; point 3). For the combination score (IGF-Child-Pugh score), the subjective variables in the original Child-Pugh score (encephalopathy and ascites) were replaced with IGF-1 levels. The results showed that the baseline IGF-Child-Pugh score was a prognostic factor for OS in both the atezolizumab-bevacizumab (HR, 0.33; 95% CI, 0.20–0.56; p<0.001) and sorafenib (HR 0.32; 95% CI, 0.16–0.65; p=0.002) arms. Consequently, the novel combination of IGF-1 levels and Child-Pugh scores may help improve patient stratification in clinical practice.68
HCC progression is influenced by chronic inflammation and the activity of ICIs might be influenced by cytokines and immune cell populations.69 Based on this hypothesis, easy accessible and measurable parameters related to the inflammatory response such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and interleukin-6 (IL-6), have been studied as potential useful prognostic markers.70 In a retrospective analysis of patients treated with atezolizumab plus bevacizumab in clinical practice, high NLR (≥5) and high PLR (≥300) were associated with worse OS, but only high NLR was an independent prognostic factor of worse OS in multivariate analysis. In addition, univariate analysis showed that both high NLR and PLR were correlated with worse PFS, but neither variable was independently prognostic of PFS. Finally, more solid evidence exists regarding the association between high IL-6 levels and poor clinical outcome. In a prospective study enrolling 165 patients with unresectable HCC treated with atezolizumab and bevacizumab, baseline IL-6 serum levels correlated with poor ORR and low peripheral T cell proliferation and tumor-infiltrating T cells, as assessed using flow cytometry bead array and ribonucleic acid (RNA) sequencing.71
Discussion
Currently, atezolizumab plus bevacizumab is used in clinical practice. Nonetheless, there are still some grey areas that need to be addressed.
This combination has only been tested against sorafenib. Since no other direct first-line comparisons have been evaluated, several network meta-analysis (NMA) have been conducted, suggesting improved survival benefit of atezolizumab plus bevacizumab against other front-line treatment options, including MKIs, immunotherapy, and locoregional therapies.72,73 A recent NMA demonstrated a reduced risk of death with atezolizumab plus bevacizumab compared to placebo (HR 0.40; 95% CI, 0.28–0.57), sorafenib (HR 0.58; 95% CI, 0.42–0.80), lenvatinib (HR 0.63; 95% CI, 0.44–0.89), atezolizumab plus cabozantinib (HR 0.64; 95% CI, 0.43–0.97), and nivolumab (HR 0.69; 95% CI, 0.48–0.98).74 However, atezolizumab plus bevacizumab was not statistically significantly superior to durvalumab plus tremelimumab (HR 0.74; 95% CI, 0.52–1.06) and sintilimab plus IBI035 (HR 1.02; 95% CI, 0.67–1.55). The association of durvalumab and tremelimumab demonstrated a lower rate of TRAEs and discontinuation than anti-PD-1 plus anti-VEGF and anti-PD-1 plus MKI. Another NMA confirmed this evidence, supporting the combination of anti-PD-(L)-1 plus anti-VEGF as first-line treatment option, showing an OS benefit over all other therapies except durvalumab plus tremelimumab.75 Similarly, ICIs plus anti-VEGF and dual ICIs combination led to the greatest OS benefit compared with sorafenib, whereas ICIs plus MKIs were associated with greater PFS but higher toxicities rates.76 Furthermore, according to another indirect analysis, the highest ORR was reached with sintilimab plus IBI305, whereas atezolizumab plus bevacizumab reached the highest DCR.77
Some matched-adjusted indirect comparisons (MAICs) also confirmed better survival outcomes of atezolizumab plus bevacizumab versus both sorafenib (HR 0.58, 95% CI, 0.42–0.79) and lenvatinib (HR 0.59; 95% CI, 0.46–0.75).78,79 Some analysis conducted on non-viral HCC patients suggested a survival benefit with lenvatinib compared to atezolizumab plus bevacizumab in patients with MAFLD/MASH.80 This was suggested also in a large real-life worldwide population, although similar survival was seen between atezolizumab plus bevacizumab and lenvatinib.81
In the absence of direct comparisons between new first-line therapeutic options, evaluation of clinical features and their association with potential treatment benefits is becoming crucial. Although some evidence has indicated a lower benefit of immunotherapy for non-viral etiology, particularly MASH-related HCC, it has recently been shown that baseline liver disease etiology is not associated with significant differences in ORR, PFS, or OS.47 Moreover, reporting etiology as non-viral may be misleading, as it includes heterogeneous subgroups of patients with different risk factors (alcohol-related liver disease, MAFLD/MASH, metabolic syndrome) that frequently overlap in the process of HCC development. This poorly informative classification and the lack of stratification in randomized controlled trials is still a main issue to address. Another major challenge is related to Child-Pugh B patients. Although atezolizumab plus bevacizumab has been tested in this setting, showing a safety and efficacy profile similar to that observed in Child-Pugh class A patients, further evaluation of immunotherapy in this population is strongly encouraged. To better explore first-line treatment options in patients with impaired liver function, several treatments including atezolizumab plus bevacizumab, nivolumab, and sorafenib have been evaluated in Child-Pugh B patients, showing better survival than best supportive care.82
The occurrence of immune-related AEs (irAEs) seems to predict treatment benefits, as it has been previously shown for dermatological AEs and hypertension in patients with MKIs. The development of grade 2 or higher irAEs has been shown to be associated with better survival from ICIs.83 Moreover, patients with grade ≥3 irAEs reported better ORR and survival than those with grade 1–2 or no irAEs.84 Of note, the use of systemic steroids to treat irAEs was associated with a trend towards longer PFS and OS. This could be explained by the fact that systemic steroids were administered to patients with grade ≥3 irAEs, which were associated with longer survival. Therefore, the management of toxicities is a priority for clinicians, since any strategies to avoid treatment discontinuation or delay should be proposed, especially for patients who derive benefits from ICIs to ensure the best long-term outcomes. Furthermore, it is crucial to better define the prognostic stratification of the patients. The prognostic role of AFP as an early response marker and its combination with ALBI grade were tested in a prospective clinical trial that enrolled 75 patients with AFP levels >20 ng/mL treated with atezolizumab and bevacizumab. An early AFP response was defined as a ≥20% decline in AFP level at 3 weeks. The combination of ALBI grade at the start of treatment and AFP early response was significantly associated with OS (p=0.046) and PFS (p=0.012), with a poorer prognosis in patients belonging to the ALBI2-AFP non-responder’s class.85 Recently, the C-reactive protein (CRP) and AFP in Immunotherapy (CRAFITY) prognostic score was evaluated in patients treated with atezolizumab plus bevacizumab. Before atezolizumab plus bevacizumab initiation, the score was derived from CRP and AFP serum levels by adding one point each for CRP level ≥1 mg/dL and AFP ≥100 ng/mL. Median PFS and OS were significantly worse in patients with higher CRAFITY scores.86 Moreover, CRAFITY was independently associated with PFS and OS and significantly associated with radiological response. The atezolizumab plus bevacizumab (ABE) index has recently been proposed as a prognostic indicator, identifying three groups of patients based on the Child-Pugh score, ALBI grade, MVI, AFP levels, and NLR. OS was better in low-risk patients compared to both intermediate-risk and high-risk ones (22.5 months versus 14.2 months versus 7.0 months) [high-risk HR 3.99 (95% CI, 2.76, 5.77); intermediate-risk HR 1.76 (95% CI, 1.26, 2.46); low-risk HR 1 (reference group), p<0.01].87
With the introduction of atezolizumab plus bevacizumab in the treatment algorithm, the optimal treatment sequence for the second- and further-lines remains unclear. Currently, phase III trials evaluating treatment strategies after ICIs progression are ongoing, and the choice of the most adequate sequential treatment after atezolizumab plus bevacizumab remains empirical with patients’ clinical features, prior tolerability, and regulatory approval driving the decision-making process.88,89 As seen in the front-line setting, only indirect comparisons may provide some guidance on treatment choice, even though methodological concerns may limit the interpretation of the results. MKIs are a valid treatment option after immunotherapy. In a multicenter retrospective study, both sorafenib and lenvatinib showed efficacy and tolerability profiles similar to those reported in phase III trials.90 Moreover, the efforts to assess the net health benefit of sequential treatment options brought to the introduction of the incremental safety-effectiveness ratio (ISER), resulting from a Markov model analysis of outcomes from available trials. The ISER index embodies Life-year gained (LYG) and rates of severe AEs related to a specific sequence of systemic treatments. It is calculated as the difference in probability of developing severe AEs divided by LYG between two or more sequences. Based on the ISER index, the comparison of sequences including first-line atezolizumab plus bevacizumab followed by five second-line treatments (sorafenib, lenvatinib, regorafenib, cabozantinib, and ramucirumab) showed that lenvatinib (median OS 24 months) and sorafenib (median OS 23 months) were the most effective sequential treatment options, producing a LYG of 0.50 and 0.42 year, respectively.91 Ramucirumab, regorafenib, and cabozantinib have demonstrated efficacy and safety after immunotherapy when administered beyond second-line therapy. Ramucirumab was evaluated in patients with baseline AFP ≥400 ng/mL after non-sorafenib-based prior systemic therapy.92 Prior systemic regimens included ICIs monotherapy, ICIs plus antiangiogenic agents, and dual ICIs. In the REFINE real-world study, 9% of patients receiving regorafenib had been treated with at least one previous line of immunotherapy (most commonly nivolumab and pembrolizumab monotherapy).93 The safety and efficacy of cabozantinib was confirmed in 14 patients who progressed on prior immunotherapy in the phase III CELESTIAL trial.94 In a phase II trial of cabozantinib post-ICIs, median PFS and median OS were 4.1 months and 9.9 months, respectively.95 Among the 19 patients with prior atezolizumab plus bevacizumab treatment, median OS was 14.3 months (95% CI, 5.5–14.4), whereas median OS was 8.9 months (95% CI, 6.1-NR) for prior non-atezolizumab plus bevacizumab regimen, thus suggesting a more favorable outcome for the atezolizumab plus bevacizumab-cabozantinib sequence. Moreover, preliminary real-world evidence has shown that nivolumab plus ipilimumab may be efficacious after other ICIs regimens.96 The purpose of ICI rechallenge has been investigated in an international, retrospective, multicenter study enrolling patients receiving at least two lines of ICI-based therapy (first-line, ICI-1, and second-line, ICI-2) either as monotherapy or a dual ICI regimen or combined with MKI/anti-VEGF. The ORR was 22% for ICI-1 and 26% for ICI-2, underpinning the rationale for further investigation of the use of ICI-based therapy beyond disease progression in patients receiving first-line immunotherapy.97
Another sequential approach is the replacement of the anti-VEGF agent with MKI to restore immunotherapy sensitivity, bypassing VEGF resistance. Ongoing clinical trials are evaluating the administration of the same ICI after PD, replacing the anti-VEGF agent with MKI (IMbrave251, NCT04770896; NCT05168163).
The correct timing of switching to a subsequent treatment line is an emerging issue. The use of combination treatment beyond disease progression in cases of sustained clinical benefit should be carefully evaluated. In fact, delayed response and pseudoprogression are observed with the administration of immunotherapy, even if they are rare events in HCC.98,99 In the IMbrave150 study, >50% of patients received atezolizumab with or without bevacizumab beyond progression, with reported sustained benefit and prolonged survival.11,44 Importantly, the selection of patients who could benefit from treatment beyond progression appears to be crucial, and the pattern of progression could be an instructive parameter. In addition, preservation of liver function is crucial in HCC and a complex issue is prompt recognition of hepatic decompensation signs (ie, ascites, hepatic encephalopathy, variceal bleeding) in patients with liver cirrhosis to allow continuation of therapeutic course and avoid misdiagnosing of disease progression which does not always coincide with liver function declining.100 The risk of hepatic decompensation has never been properly assessed in clinical trials and there are no data on the difference between the impact of MKIs and ICIs on hepatic decompensation. Therefore, endpoints related to liver function deterioration (time-to-decompensation and decompensation-free survival), should be evaluated and reported in clinical trials and could be helpful as measures of effectiveness and safety of advanced HCC treatment. Recently, several studies have focused on the administration of ICI combinations at earlier stages. In the adjuvant setting, the IMbrave050 phase III trial showed improved recurrence-free survival (RFS) with atezolizumab plus bevacizumab versus active surveillance in 662 patients with HCC who were at a high risk of recurrence after curative surgery or ablation (radiofrequency ablation [RFA] or microwave ablation [MVA] only), with a 12-month RFS rate of 78% versus 65% after a median follow-up of 17.4 months. This benefit was maintained across subgroups, but more mature results, including OS benefits, are needed to better understand the potential impact on the therapeutic scenario.101 Similarly, other phase III trials are evaluating the role of adjuvant immunotherapy (CheckMate 9DX, NCT03383458; KEYNOTE-937, NCT03867084).
Regarding the pre/peri-operative setting, in a phase Ib study, neoadjuvant cabozantinib and nivolumab were administered in HCC patients for which upfront surgery was not recommended because of high-risk tumor features. 12 out of 15 patients underwent R0 resection, whereas 5 patients had major pathologic responses (MPRs).102 Moreover, in a phase II trial, 27 patients with resectable HCC received nivolumab alone or nivolumab plus ipilimumab up to 4 doses before and after surgery. More than one third of patients reached a MPR and, after a median follow up of 24.6 months, no recurrences were observed in these patients.103 The phase I PRIME-HCC study showed promising response rates (ORR 29%, DCR 95%, MPR 56%) and a good safety profile (24% of grade 3 AEs) in 25 HCC patients receiving nivolumab plus ipilimumab prior liver resection.104 In another single-arm, phase II trial, patients with resectable HCC received two cycles of neoadjuvant cemiplimab every 3 weeks, followed by surgical resection. Twenty out of 21 patients underwent successful surgical resection: 4 patients had significant tumor necrosis, 3 had a PR, and 13 maintained an SD.105 These studies provided preliminary data that support further investigation of neoadjuvant immunotherapy in HCC and raise questions such as the most appropriate combinations of agents, the optimal therapy duration, and potential predictors of efficacy that deserve to be explored.106
In the intermediate stage, clinical trials are evaluating atezolizumab plus bevacizumab versus trans-arterial chemoembolization (TACE) (ABC-HCC trial, NCT04803994), in combination with either synchronous or on-demand selective intra-arterial therapies, to be performed in cases of radiological progression (DEMAND study, NCT04224636).
Finally, the economic sustainability of the combination must be considered. In fact, even though regulatory agencies positively recommend atezolizumab plus bevacizumab in an advanced setting, including a cost-effectiveness analysis in their evaluation, its use may have different impacts on different health systems.107–109
Conclusion and Future Perspectives
The positive results of the IMbrave150 trial introduced atezolizumab plus bevacizumab into clinical practice, making this combination a new first-line standard of care for patients with advanced HCC. Although these agents have demonstrated clinical activity in HCC and have been supported by post-hoc analyses and real-world data, identifying patients who are most likely to derive major clinical benefits from the combination therapy is crucial for improving treatment results. Further studies are required to properly address the patient stratification and biomarker selection. In particular, future research efforts should focus on the implementation of palliative care in order to treat the underlying liver disease, increase the survival rate, and possibly allow patients with worse liver function to benefit from systemic treatment. Currently, the available serum and tissue biomarkers are not adequate in terms of prognostic and predictive stratification. Therefore, the association of these biomarkers with genomic and epigenetic data, as well as the characterization of tumor microenvironment should be deeply studied to identify those features that can influence patients’ response to treatment. Finally, prospective trials on subsequent strategies are urgently required to define proper treatment algorithms for HCC. In detail, a deeper understanding of drugs resistance and the development of new active drugs are research areas to carry on in the near future.
Abbreviations
AASLD, American Association for the Study of Liver Diseases; ABE, atezolizumab plus bevacizumab index; ADAs, anti-drug antibodies; AEs, adverse events; AESI, Adverse events of special interest; AFP, alpha-fetoprotein; ALBI, albumin-bilirubin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; AVB, acute variceal bleeding; BCLC, Barcelona Clinic Liver Cancer; CR, complete response; CRP, C-reactive protein; CTLA-4, Cytotoxic T-lymphocyte antigen-4; DCs, dendritic cells; DOR, duration of response; ECOG, Eastern Cooperative Oncology Group; EGD, esophagogastroduodenoscopy; EHS, extrahepatic spread; EMA, European Medicines Agency; European Field of Practice Study of Atezolizumab And Bevacizumab in Hepatocellular Carcinoma (EURAB-HCC); FDA, Food and Drug Administration; GSEA, genome wide-differential gene expression analysis; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; HPVG, hepatic venous pressure gradient; ICI, immune-checkpoint inhibitor; IGF-1, insulin growth factor 1; IL-6, interleukin-6; irAEs, immune-related adverse events; ISER, incremental safety-effectiveness ratio; IQR, interquartile range; ITT, intention-to-treat; mAb, monoclonal antibody; LRT, locoregional treatment; LYG, life-year gained (LYG); MAFLD, metabolic dysfunction-associated fatty liver disease; MAICS, matched-adjusted indirect comparisons; MASH, metabolic dysfunction-associated steatohepatitis; MDSCs, medullary dendritic suppressor cells; MKI, multikinase inhibitor; MPRs, major pathologic responses; mRECIST, modified-RECIST; MVA, microwave ablation; MVI, macrovascular invasion; NAFLD, non-alcoholic fatty liver disease; NE, not estimable NLR, neutrophil-to-lymphocyte ratio; NMA, network meta-analysis; NASH, non-alcoholic steatohepatitis; OS, overall survival; ORR, objective response rate; PD, progressive disease; PD-1, programmed cell death protein-1; PD-L1, programmed death ligand-1; PFS, progression-free survival; PLR, platelet-to-lymphocyte ratio; PR, partial response; PROs, patient-reported outcomes; PS, Performance Status; PVTT, portal vein tumor thrombosis; QoL, quality of life; RECIST1.1, response evaluation criteria in solid tumors version 1.1; RFA, radiofrequency ablation; RFS, recurrence-free survival; ribonucleic acid, RNA; TACE, trans-arterial chemoembolization; Teff, effector T cell; TMB, tumor mutation burden; TRAE, treatment-related adverse event; Tregs, regulatory T cells; TTD, time to deterioration; VEGF, vascular endothelial growth factor; VEGFR-2, vascular endothelial growth factor receptor 2.
Funding
This study did not receive any grant or other type of financial support.
Disclosure
LR reports consulting fees from AstraZeneca, Basilea, Bayer, BMS, Eisai, Exelixis, Genenta, Hengrui, Incyte, Ipsen, IQVIA, Jazz Pharmaceuticals, MSD, Nerviano Medical Sciences, Roche, Servier, Taiho Oncology, Zymeworks; lecture fees from AstraZeneca, Bayer, BMS, Eisai, Incyte, Ipsen, Merck Serono, Roche, Servier; travel expenses from AstraZeneca; research grants (to institutions) from Agios, AstraZeneca, BeiGene, Eisai, Exelixis, Fibrogen, Incyte, Ipsen, Lilly, MSD, Nerviano Medical Sciences, Roche, Zymeworks. TP reports consulting fees from Bayer, Ipsen, and Astra Zeneca; institutional research funding from Roche, Bayer, and Astra Zeneca; and travel expenses from Roche. VZ, AP, RB declare no conflicts of interest in this work.
References
1. Vogel A, Meyer T, Sapisochin G, Salem R, Saborowski A. Hepatocellular carcinoma. Lancet. 2022;400(10360):1345–1362. doi:10.1016/S0140-6736(22)01200-4
2. Rinella ME, Lazarus JV, Ratziu V, et al. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023;2023:1.
3. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
4. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–390. doi:10.1056/NEJMoa0708857
5. Cheng AL, Kang YK, Chen Z, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10(1):25–34. doi:10.1016/S1470-2045(08)70285-7
6. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
7. Bruix J, Qin S, Merle P, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;389(10064):56–66. doi:10.1016/S0140-6736(16)32453-9
8. Abou-Alfa GK, Meyer T, Cheng AL, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med. 2018;379(1):54–63. doi:10.1056/NEJMoa1717002
9. Zhu AX, Kang YK, Yen CJ, et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(2):282–296. doi:10.1016/S1470-2045(18)30937-9
10. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
11. Cheng AL, Qin S, Ikeda M, et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022;76(4):862–873. doi:10.1016/j.jhep.2021.11.030
12. National Comprehensive Cancer Network. Hepatobiliary cancers. Version 1; 2023. Available from: https://www.nccn.org/professionals/physician_gls/pdf/hepatobiliary.pdf.
13. Ren Z, Xu J, Bai Y, et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, Phase 2–3 study. Lancet Oncol. 2021;22(7):977–990. doi:10.1016/S1470-2045(21)00252-7
14. Abou-Alfa GK, Lau G, Kudo M, et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evid. 2022;2022:EVIDoa2100070.
15. Qin S, Kudo M, Meyer T, et al. Final analysis of RATIONALE-301: randomized, phase III study of tislelizumab versus sorafenib as first-line treatment for unresectable hepatocellular carcinoma. Ann Oncol. 2022;33(suppl_7):S808–S869.
16. Qin S, Chan SL, Gu S, et al. Camrelizumab plus rivoceranib versus sorafenib as first-line therapy for unresectable hepatocellular carcinoma (CARES-310): a randomised, open-label, international phase 3 study. Lancet. 2023;2023:S0140–6736(23)00961–3.
17. Yau T, Park JW, Finn RS, et al. Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2022;23(1):77–90. doi:10.1016/S1470-2045(21)00604-5
18. Kelley RK, Rimassa L, Cheng AL, et al. Cabozantinib plus atezolizumab versus sorafenib for advanced hepatocellular carcinoma (COSMIC-312): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2022;23(8):995–1008. doi:10.1016/S1470-2045(22)00326-6
19. Finn RS, Kudo M, Merle P, et al. Primary results from the phase III LEAP-002 study: lenvatinib plus pembrolizumab versus lenvatinib as first-line (1L) therapy for advanced hepatocellular carcinoma (aHCC). Ann Oncol. 2022;33(suppl_7):S808–S869. doi:10.1016/j.annonc.2022.08.031
20. Yau T, Kang YK, Kim TY, et al. Efficacy and safety of nivolumab plus ipilimumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib: the checkmate 040 randomized clinical trial. JAMA Oncol. 2020;6(11):e204564. doi:10.1001/jamaoncol.2020.4564
21. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol. 2018;19(7):940–952. doi:10.1016/S1470-2045(18)30351-6
22. Kudo M, Finn RS, Edeline J, et al. Updated efficacy and safety of KEYNOTE-224: a phase II study of pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib. Eur J Cancer. 2022;167:1–12. doi:10.1016/j.ejca.2022.02.009
23. Finn RS, Ryoo BY, Merle P, et al. Pembrolizumab as second-line therapy in patients with advanced hepatocellular carcinoma in KEYNOTE-240: a randomized, double-blind, phase III trial. J Clin Oncol. 2020;38(3):193–202. doi:10.1200/JCO.19.01307
24. Qin S, Chen Z, Fang W, et al. Pembrolizumab versus placebo as second-line therapy in patients from Asia with advanced hepatocellular carcinoma: a randomized, double-blind, phase III trial. J Clin Oncol. 2023;41(7):1434–1443. doi:10.1200/JCO.22.00620
25. Lee MS, Ryoo BY, Hsu CH, et al. Atezolizumab with or without bevacizumab in unresectable hepatocellular carcinoma (GO30140): an open-label, multicentre, phase 1b study. Lancet Oncol. 2020;21(6):808–820. doi:10.1016/S1470-2045(20)30156-X
26. Faivre S, Rimassa L, Finn RS. Molecular therapies for HCC: looking outside the box. J Hepatol. 2020;72(2):342–352. doi:10.1016/j.jhep.2019.09.010
27. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
28. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. doi:10.1055/s-0030-1247132
29. He ARR, Numata K, Lee K-H, et al. Efficacy of atezolizumab (atezo) + bevacizumab (bev) after disease progression with atezo monotherapy in patients with previously untreated, unresectable hepatocellular carcinoma (HCC). Ann Oncol. 2020;31:S690–S690. doi:10.1016/j.annonc.2020.08.1102
30. Finn RS, Qin S, Ikeda M, et al. IMbrave150: updated overall survival (OS) data from a global, randomized, open-label phase III study of atezolizumab (atezo) + bevacizumab (bev) versus sorafenib (sor) in patients (pts) with unresectable hepatocellular carcinoma (HCC). J Clin Oncol. 2021;39(suppl_3):267. doi:10.1200/JCO.2021.39.3_suppl.267
31. Galle PR, Finn RS, Qin S, et al. Patient-reported outcomes with atezolizumab plus bevacizumab versus sorafenib in patients with unresectable hepatocellular carcinoma (IMbrave150): an open-label, randomised, phase 3 trial. Lancet Oncol. 2021;22(7):991–1001. doi:10.1016/S1470-2045(21)00151-0
32. Personeni N, Rimassa L. Gauging the quality-of-life benefits of immunotherapy in hepatocellular carcinoma. Lancet Oncol. 2021;22(7):896–898. doi:10.1016/S1470-2045(21)00258-8
33. Li D, Toh H, Merle P, et al. Atezolizumab + bevacizumab vs sorafenib for unresectable hepatocellular carcinoma: results from older adults enrolled in IMbrave150. Ann Oncol. 2020;31:234. doi:10.1016/j.annonc.2020.04.061
34. Ikeda M, Zhu AX, Qin S, et al. IMbrave150: management of adverse events of special interest (AESIs) for atezolizumab (atezo) and bevacizumab (bev) in unresectable HCC. Ann Oncol. 2020;3:S629–S644.
35. Finn RS, Qin S, Ikeda M, et al. IMbrave150: updated efficacy and safety by risk status in patients (pts) receiving atezolizumab (atezo) + bevacizumab (bev) vs sorafenib (sor) as first-line treatment for unresectable hepatocellular carcinoma (HCC).
36. Breder VV, Vogel A, Merle P, et al. IMbrave150: exploratory efficacy and safety results of hepatocellular carcinoma (HCC) patients (pts) with main trunk and/or contralateral portal vein invasion (Vp4) treated with atezolizumab (atezo) + bevacizumab (bev) versus sorafenib (sor) in a global Ph III study. J Clin Oncol. 2021;39(suppl_15):4073. doi:10.1200/JCO.21.01440
37. Merle P, Ducreux M, Finn RS, et al. IMbrave150: efficacy and safety of atezolizumab plus bevacizumab vs sorafenib by baseline varices status in patients with hepatocellular carcinoma.
38. Kudo M, Finn RS, Galle PR, et al. IMbrave150: exploratory efficacy and safety results in patients with hepatocellular carcinoma without macrovascular invasion (MVI) or extrahepatic spread (EHS) treated with atezolizumab (atezo) + bevacizumab (bev) or sorafenib (sor). Ann Oncol. 2021;32(suppl_5):S818–S818. doi:10.1016/j.annonc.2021.08.152
39. Kudo M, Finn RS, Galle P, et al. IMbrave150: efficacy and safety of atezolizumab plus bevacizumab versus sorafenib in patients with Barcelona clinic liver cancer stage B Unresectable hepatocellular carcinoma: an exploratory analysis of the phase III study. Liver Cancer. 2023;12(3):238–250. doi:10.1159/000528272
40. Salem R, Galle P, Finn RS, et al. IMbrave150: exploratory efficacy and safety results of atezolizumab + bevacizumab vs sorafenib in patients with unresectable hepatocellular carcinoma (HCC) who had prior locoregional therapy (LRT).
41. Kudo M, Finn RS, Cheng A-L, et al. Albumin-bilirubin grade analyses of atezolizumab plus bevacizumab versus sorafenib in patients with unresectable hepatocellular carcinoma: a post hoc analysis of the phase III imbrave150 study. Liver Cancer. 2023;2023:1–15.
42. Shemesh CS, Chan P, Shao H, et al. Atezolizumab and bevacizumab in patients with unresectable hepatocellular carcinoma: pharmaco- kinetic and safety assessments based on hepatic impairment status and geographic region. Liver Cancer. 2021;10(5):485–499. doi:10.1159/000515817
43. Finn RS, Qin S, Ikeda M, et al. Complete responses (CR) in patients receiving atezolizumab (atezo) + bevacizumab (bev) versus sorafenib (sor) in IMbrave150: a phase III clinical trial for unresectable hepatocellular carcinoma (HCC). J Clin Oncol. 2020;38(suppl_15):4596. doi:10.1200/JCO.2020.38.15_suppl.4596
44. Toh HC, Galle P, Zhu AX, et al. IMbrave150: exploratory efficacy and safety in patients with unresectable hepatocellular carcinoma (HCC) treated with atezolizumab beyond radiological progression until loss of clinical benefit in a global phase III study. J Clin Oncol. 2022;40(suppl_4):470. doi:10.1200/JCO.2022.40.4_suppl.470
45. Galle P, Finn RS, Cheng A-L, et al. Assessment of the impact of anti-drug antibodies on PK and clinical outcomes with atezolizumab + bevacizumab in HCC.
46. Zhu AX, Finn RS, Ducreux M, et al. Exploratory Efficacy and safety of atezolizumab + bevacizumab vs sorafenib in patients with Hepatocellular Carcinoma (HCC) with non-viral etiology in a global phase III study.
47. Espinoza M, Muiquith M, Lim M, Zhu H, Singal AG, Hsiehchen D. Disease etiology and outcomes after atezolizumab plus bevacizumab in hepatocellular carcinoma: post-hoc analysis of imbrave150. Gastroenterology. 2023;165:286–288.e4. doi:10.1053/j.gastro.2023.02.042
48. Fulgenzi CAM, Murphy C, D’Alessio A, et al. IMbrave150 - Effect of early antibiotic exposure on survival of patients receiving atezolizumab plus bevacizumab but not sorafenib for unresectable HCC: a sub-analysis of the phase III IMbrave150 study.
49. Kudo M, Tsuchiya K, Shao -Y-Y, et al. IMbrave150: exploratory analysis to examine the association between bevacizumab (bev) ever being skipped and bev never being skipped in patients with unresectable hepatocellular carcinoma (HCC) treated with atezolizumab (atezo) + bev in a global phase 3 study.
50. Piscaglia F, Masi G, Martinelli E, et al. Atezolizumab in combination with bevacizumab in patients with unresectable hepatocellular carcinoma not previously treated with systemic therapy: safety results from the interim analysis of the phase IIIb Italian AMETHISTA trial.
51. Piscaglia F, Masi G, Martinelli E, et al. Efficacy of atezolizumab in combination with bevacizumab in patients with unresectable hepatocellular carcinoma not previously treated with systemic therapy: efficacy results from the interim analysis of the Phase IIIb Italian AMETHISTA trial.
52. Fulgenzi CAM, Cheon J, D’Alessio A, et al. Reproducible safety and efficacy of atezolizumab plus bevacizumab for HCC in clinical practice: results of the AB-real study. Eur J Cancer. 2022;175:204–213. doi:10.1016/j.ejca.2022.08.024
53. Aidoo-Micah G, Pinter M, Scheiner B, et al. EURopean field of practice study of atezolizumab and bevacizumab in hepatocellular carcinoma (EURAB-HCC).
54. Larrey E, Campion B, Evain M, et al. A history of variceal bleeding is associated with further bleeding under atezolizumab-bevacizumab in patients with HCC. Liver Int. 2022;42(12):2843–2854. doi:10.1111/liv.15458
55. Villa E, Bianchini M, Blasi A, et al. EASL Clinical Practice Guidelines on prevention and management of bleeding and thrombosis in patients with cirrhosis. J Hepatol. 2022;76(5):1151–1184.
56. De Franchis R. Expanding consensus in portal hypertension: report of the baveno VI consensus workshop: stratifying risk and individualizing care for portal hypertension. J Hepatol. 2015;63(3):743–752. doi:10.1016/j.jhep.2015.05.022
57. D’Alessio A, Fulgenzi CAM, Nishida N, et al. Preliminary evidence of safety and tolerability of atezolizumab plus bevacizumab in patients with hepatocellular carcinoma and Child-Pugh A and B cirrhosis: a real-world study. Hepatology. 2022;76(4):1000–1012. doi:10.1002/hep.32468
58. de Castro T, Jochheim LS, Bathon M, et al. Atezolizumab and bevacizumab in patients with advanced hepatocellular carcinoma with impaired liver function and prior systemic therapy: a real-world experience. Ther Adv Med Oncol. 2022;14:17588359221080298. doi:10.1177/17588359221080298
59. D’Alessio A, Fulgenzi CAM, Scheiner B, et al. The ALBI grade refines prognostic prediction in advanced hepatocellular cancer and enables risk stratification for bleeding events following atezolizumab plus bevacizumab.
60. Iwamoto H, Shimose S, Noda Y, et al. Initial experience of atezolizumab plus bevacizumab for unresectable hepatocellular carcinoma in real-world clinical practice. Cancers. 2021;13(11):2786. doi:10.3390/cancers13112786
61. Nakagawa M, Inoue M, Ogasawara S, et al. Clinical effects and emerging issues of atezolizumab plus bevacizumab in patients with advanced hepatocellular carcinoma from Japanese real-world practice. Cancer. 2023;129(4):590–599. doi:10.1002/cncr.34559
62. Cheon J, Yoo C, Hong JY, et al. Efficacy and safety of atezolizumab plus bevacizumab in Korean patients with advanced hepatocellular carcinoma. Liver Int. 2022;42(3):674–681. doi:10.1111/liv.15102
63. Charonpongsuntorn C, Tanasanvimon S, Korphaisarn K, et al. Efficacy, safety, and patient-reported outcomes of atezolizumab plus bevacizumab for unresectable hepatocellular carcinoma in Thailand: a multicenter prospective study. JCO Glob Oncol. 2022;8:e2200205. doi:10.1200/GO.22.00205
64. Vithayathil M, D’Alessio A, Fulgenzi CAM, et al. Impact of older age in patients receiving atezolizumab and bevacizumab for hepatocellular carcinoma. Liver Int. 2022;42(11):2538–2547. doi:10.1111/liv.15405
65. Kim C, Yang H, Kim I, et al. Association of high levels of antidrug antibodies against atezolizumab with clinical outcomes and T-cell responses in patients with hepatocellular carcinoma. JAMA Oncol. 2022;8(12):1825–1829. doi:10.1001/jamaoncol.2022.4733
66. Zhu AX, Abbas AR, de Galarreta MR, et al. Molecular correlates of clinical response and resistance to atezolizumab in combination with bevacizumab in advanced hepatocellular carcinoma. Nat Med. 2022;28(8):1599–1611. doi:10.1038/s41591-022-01868-2
67. Zhu AX, Dayyani F, Yen CJ, et al. Alpha-fetoprotein as a potential surrogate biomarker for atezolizumab + bevacizumab treatment of hepatocellular carcinoma. Clin Cancer Res. 2022;28(16):3537–3545. doi:10.1158/1078-0432.CCR-21-3275
68. Kaseb AO, Guan Y, Gok Yavuz B, et al. Serum IGF-1 scores and clinical outcomes in the phase III imbrave150 study of atezolizumab plus bevacizumab versus sorafenib in patients with unresectable hepatocellular carcinoma. J Hepatocell Carcinoma. 2022;9:1065–1079. doi:10.2147/JHC.S369951
69. Tian Z, Hou X, Liu W, Han Z, Wei L. Macrophages and hepatocellular carcinoma. Cell Biosci. 2019;9:79. doi:10.1186/s13578-019-0342-7
70. Wu YL, Fulgenzi CAM, D’Alessio A, et al. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as prognostic biomarkers in unresectable hepatocellular carcinoma treated with atezolizumab plus bevacizumab. Cancers. 2022;14(23):5834. doi:10.3390/cancers14235834
71. Chon H, Kim C, Yang H, et al. Correlation of high serum interleukin-6 with clinical outcome and T cell response in patients with unresectable hepatocellular carcinoma treated with atezolizumab and bevacizumab. J Clin Oncol. 2023;41(suppl_4):596. doi:10.1200/JCO.2023.41.4_suppl.596
72. Sonbol MB, Riaz IB, Naqvi SAA, et al. Systemic therapy and sequencing options in advanced hepatocellular carcinoma: a systematic review and network meta-analysis. JAMA Oncol. 2020;6(12):e204930. doi:10.1001/jamaoncol.2020.4930
73. Vogel A, Rimassa L, Sun HC, et al. Comparative efficacy of atezolizumab plus bevacizumab and other treatment options for patients with unresectable hepatocellular carcinoma: a network meta-analysis. Liver Cancer. 2021;10:240–248. doi:10.1159/000515302
74. Fulgenzi CAM, D’Alessio A, Airoldi C, et al. Comparative efficacy of novel combination strategies for unresectable hepatocellular carcinoma: a network metanalysis of phase III trials. Eur J Cancer. 2022;174:57–67. doi:10.1016/j.ejca.2022.06.058
75. Fong KY, Zhao JJ, Sultana R, et al. First-line systemic therapies for advanced hepatocellular carcinoma: a systematic review and patient-level network meta-analysis. Liver Cancer. 2022;12(1):7–18. doi:10.1159/000526639
76. Lei Q, Yan X, Zou H, et al. Efficacy and safety of monotherapy and combination therapy of immune checkpoint inhibitors as first-line treatment for unresectable hepatocellular carcinoma: a systematic review, meta-analysis and network meta-analysis. Discov Oncol. 2022;13(1):95. doi:10.1007/s12672-022-00559-1
77. Fulgenzi CAM, Scheiner B, Korolewicz J, et al. Efficacy and safety of frontline systemic therapy for advanced HCC: a network meta-analysis of landmark phase III trials. JHEP Rep. 2023;5(5):100702. doi:10.1016/j.jhepr.2023.100702
78. Casadei-Gardini A, Tada T, Shimose S, et al. Is atezolizumab plus bevacizumab for unresectable hepatocellular carcinoma superior even to lenvatinib? A matching-adjusted indirect comparison. Target Oncol. 2021;16(2):249–254. doi:10.1007/s11523-021-00803-8
79. Jiang Y, Cai D, Shi S. Indirect comparisons via sorafenib for the comparative effectiveness of two PD-1/PD-L1 inhibitors to treat advanced hepatocellular carcinoma patients without prior systemic therapies. Clin Epidemiol. 2022;14:581–590. doi:10.2147/CLEP.S352045
80. Rimini M, Rimassa L, Ueshima K, et al. Atezolizumab plus bevacizumab versus lenvatinib or sorafenib in non-viral unresectable hepatocellular carcinoma: an international propensity score matching analysis. ESMO Open. 2022;7(6):100591. doi:10.1016/j.esmoop.2022.100591
81. Casadei-Gardini A, Rimini M, Tada T, et al. Atezolizumab plus bevacizumab versus lenvatinib for unresectable hepatocellular carcinoma: a large real-life worldwide population. Eur J Cancer. 2023;180:9–20. doi:10.1016/j.ejca.2022.11.017
82. Fulgenzi CAM, D’Alessio A, Scheiner B, et al. Feasibility of systemic anti-cancer therapy as an alternative to best supportive care in patients with advanced HCC and Child-Pugh B liver dysfunction.
83. Pinato DJ, Marron TU, Mishra-Kalyani PS, et al. Treatment-related toxicity and improved outcome from immunotherapy in hepatocellular cancer: evidence from an FDA pooled analysis of landmark clinical trials with validation from routine practice. Eur J Cancer. 2021;157:140–152. doi:10.1016/j.ejca.2021.08.020
84. Kyy N, Tan SH, Tan JJE, et al. Impact of Immune-related adverse events on efficacy of immune checkpoint inhibitors in patients with advanced hepatocellular carcinoma. Liver Cancer. 2021;11(1):9–21. doi:10.1159/000518619
85. Campani C, Bamba-Funck J, Campion B, et al. Baseline ALBI score and early variation of serum AFP predict outcomes in patients with HCC treated by atezolizumab-bevacizumab. Liver Int. 2023;43(3):708–717. doi:10.1111/liv.15487
86. Scheiner B, Sartoris S, D’Alessio A, et al. Validation of the CRAFITY score in patients with hepatocellular carcinoma treated with atezolizumab and bevacizumab.
87. Persano M, Rimini M, Tada T, et al. Identification of atezolizumab plus bevacizumab prognostic index via recursive partitioning analysis in HCC: the ABE index. Anticancer Res. 2023;43(4):1599–1610. doi:10.21873/anticanres.16310
88. Bruix J, Chan SL, Galle PR, et al. Systemic treatment of hepatocellular carcinoma: an EASL position paper. J Hepatol. 2021;75:960–974. doi:10.1016/j.jhep.2021.07.004
89. Rimassa L, Finn RS, Sangro B. Combination immunotherapy for hepatocellular carcinoma. J Hepatol. 2023;79:S0168–8278(23)00178–2. doi:10.1016/j.jhep.2023.03.003
90. Yoo C, Kim JH, Ryu MH, et al. Clinical outcomes with multikinase inhibitors after progression on first-line atezolizumab plus bevacizumab in patients with advanced hepatocellular carcinoma: a multinational multicenter retrospective study. Liver Cancer. 2021;10(2):107–114. doi:10.1159/000512781
91. Cabibbo G, Reig M, Celsa C, et al. First-line immune checkpoint inhibitor-based sequential therapies for advanced hepatocellular carcinoma: rationale for future trials. Liver Cancer. 2021;11(1):75–84. doi:10.1159/000520278
92. Finn RS, Yau T, Hsu CH, et al. Ramucirumab for patients with advanced hepatocellular carcinoma and elevated alpha fetoprotein following non-sorafenib systemic therapy: an expansion cohort of REACH-2. Oncologist. 2022;2022:oyac183.
93. Finn RS, Kudo M, Klümpen HJ, et al. Regorafenib in patients with unresectable hepatocellular carcinoma (uHCC) in routine clinical practice: exploratory analysis of overall survival (OS) in the prospective, observational REFINE study. J Clin Oncol. 2022;40(suppl_4):433. doi:10.1200/JCO.2022.40.4_suppl.433
94. Abou-Alfa G, Cheng A-L, Saletan S, Kelley RK, El-Khoureiry A. Clinical activity of cabozantinib in patients with advanced hepatocellular carcinoma previously treated with anti-VEGF and immuno-oncology therapy: subgroup analysis from the phase 3 CELESTIAL trial.
95. Chan SL, Ryoo B, Mo F, et al. A phase II clinical trial to study the efficacy of cabozantinib in patients with hepatocellular carcinoma refractory to immune checkpoint inhibitor-based treatment. Ann Oncol. 2022;33(suppl_9):S1454–S1484. doi:10.1016/j.annonc.2022.10.099
96. Wong JSL, Kwok GGW, Tang V, et al. Ipilimumab and nivolumab/pembrolizumab in advanced hepatocellular carcinoma refractory to prior immune checkpoint inhibitors. J Immunother Cancer. 2021;9(2):e001945. doi:10.1136/jitc-2020-001945
97. Scheiner B, Roessler D, Phen S, et al. Efficacy and safety of immune checkpoint inhibitor rechallenge in individuals with hepatocellular carcinoma. JHEP Rep. 2022;5(1):100620. doi:10.1016/j.jhepr.2022.100620
98. Chiou VL, Burotto M. Pseudoprogression and immune-related response in solid tumors. J Clin Oncol. 2015;33:3541–3543. doi:10.1200/JCO.2015.61.6870
99. Wang Q, Gao J, Wu X. Pseudoprogression and hyperprogression after checkpoint blockade. Int Immunopharmacol. 2018;58:125–135. doi:10.1016/j.intimp.2018.03.018
100. Cabibbo G, Aghemo A, Lai Q, et al. Optimizing systemic therapy for advanced hepatocellular carcinoma: the key role of liver function. Dig Liver Dis. 2022;54(4):452–460. doi:10.1016/j.dld.2022.01.122
101. Chow P, Chen M, Cheng A-L, et al. IMbrave050: phase 3 study of adjuvant atezolizumab + bevacizumab versus active surveillance in patients with hepatocellular carcinoma (HCC) at high risk of disease recurrence following resection or ablation.
102. Ho WJ, Zhu Q, Durham J, et al. Neoadjuvant cabozantinib and nivolumab converts locally advanced HCC into resectable disease with enhanced antitumor immunity. Nat Cancer. 2021;2(9):891–903. doi:10.1038/s43018-021-00234-4
103. Kaseb AO, Hasanov E, Cao HST, et al. Perioperative nivolumab monotherapy versus nivolumab plus ipilimumab in resectable hepatocellular carcinoma: a randomised, open-label, phase 2 trial. Lancet Gastroenterol Hepatol. 2022;7(3):208–218. doi:10.1016/S2468-1253(21)00427-1
104. D’Alessio A, Pai M, Spalding D, et al. Neoadjuvant immunotherapy with ipilimumab plus nivolumab and radiologically and pathologically quantifiable responses through modulation of the tumour microenvironment in resectable hepatocellular carcinoma.
105. Marron TU, Fiel MI, Hamon P, et al. Neoadjuvant cemiplimab for resectable hepatocellular carcinoma: a single-arm, open-label, phase 2 trial. Lancet Gastroenterol Hepatol. 2022;7(3):219–229. doi:10.1016/S2468-1253(21)00385-X
106. Personeni N, Rimassa L. Exploring novel avenues for neoadjuvant treatment of hepatocellular carcinoma. Lancet Gastroenterol Hepatol. 2022;7(3):198–199. doi:10.1016/S2468-1253(21)00462-3
107. Su D, Wu B, Shi L. Cost-effectiveness of atezolizumab plus bevacizumab vs sorafenib as first-line treatment of unresectable hepatocellular carcinoma. JAMA Netw Open. 2021;4(2):e210037. doi:10.1001/jamanetworkopen.2021.0037
108. Zhang X, Wang J, Shi J, et al. Cost-effectiveness of atezolizumab plus bevacizumab vs sorafenib for patients with unresectable or metastatic hepatocellular carcinoma. JAMA Netw Open. 2021;4(4):e214846. doi:10.1001/jamanetworkopen.2021.4846
109. Hou Y, Wu B. Atezolizumab plus bevacizumab versus sorafenib as first-line treatment for unresectable hepatocellular carcinoma: a cost-effectiveness analysis. Cancer Commun. 2020;40:743–745. doi:10.1002/cac2.12110
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.