Back to Journals » Veterinary Medicine: Research and Reports » Volume 12
Safety and Clinical Response Following a Repeat Intraarticular Injection of Tin-117m (117mSn) Colloid in Dogs with Elbow Osteoarthritis
Authors Donecker J ![]() , Lattimer JC, Gaschen L, Aulakh KS
, Lattimer JC, Gaschen L, Aulakh KS
Received 23 October 2021
Accepted for publication 9 December 2021
Published 17 December 2021 Volume 2021:12 Pages 325—335
DOI https://doi.org/10.2147/VMRR.S345144
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Young Lyoo
John Donecker,1 Jimmy C Lattimer,2 Lorrie Gaschen,3 Karanvir Singh Aulakh3
1Exubrion Therapeutics, Inc., Buford, GA, USA; 2College of Veterinary Medicine, University of Missouri, Columbia, MO, USA; 3School of Veterinary Medicine, Louisiana State University, Baton Rouge, LA, USA
Correspondence: John Donecker
Exubrion Therapeutics, Inc., 5203 Bristol Industrial Way, Buford, GA, 30518 Tel +1-336-552-6027
Email [email protected]
Objective: To determine if a repeat intraarticular (IA) injection of a tin-117m colloid radiosynoviorthesis (RSO) agent can be safely given in the same joint 12 months after an initial injection for treatment of canine elbow osteoarthritis (OA), and to evaluate the pain reduction effect of the repeat injection.
Methods and Materials: Nine client owned dogs with grade 1 or 2 elbow OA were given an IA injection of tin-117m colloid in both elbows, one of which had been treated ≤ 12 months earlier with the same RSO device. Treatment safety was evaluated by joint fluid analysis at baseline (BL) and at 180 days after treatment, and by urinalysis, CBC, and serum chemistry analysis of diagnostic samples obtained at BL and 180 days. Radiographs, computed tomography, and MRI scans were obtained at BL and 180 days to determine if disease progression differed in elbows given one versus two injections. Clinical response to treatment was assessed subjectively by dog owner responses to the Canine Brief Pain Inventory (CBPI) survey at BL, 90 and 180 days, and objectively by investigator-conducted force plate (FP) analysis of dogs at BL, 90, and 180 days.
Results: All post-treatment urinalysis, CBC and clinical chemistry results were within normal ranges. Joint fluid analysis showed a significant (P=0.0411) reduction in the percentage of monocytes at 180 days, consistent with the tin-117m colloid mode of action of apoptosis of pro-inflammatory macrophages at the injection site. There was no significant difference in OA progression in elbows given one or two injections. The treatment success rate was 55.5% (5/9) on day 90 as determined either by CBPI responses or FP analysis, and 66.6% (6/9) on day 180 as determined by FP analysis.
Conclusion: The tin-117m colloid can be safely given as a repeat injection 12 months after an initial injection, and can potentially provide a durable therapeutic response in dogs with elbow OA.
Keywords: osteoarthritis, canine elbow, radiosynoviorthesis, radionuclide, Canine brief pain inventory, force plate
Introduction
Treatment of osteoarthritis (OA) in companion animals typically employs a multimodal approach, with no single therapy representing a definitive standard of care or treatment modality. The therapeutic goal focuses on relieving pain, inflammation, and clinical signs using an assortment of agents, including non-steroidal anti-inflammatory drugs (NSAIDS), hyaluronic acid injections, piprants, cocorticosteroids, nutraceuticals, and regenerative therapies. In veterinary medicine, radiosynoviorthesis (RSO) is an emerging OA therapy that is unique because it selectively targets the synovium for alleviating the clinical signs of joint disease.
Synovitis is the initial lesion in degenerative joint disease (DJD) and its OA end stage.1–3 Acute or chronic synovitis triggers a pernicious inflammatory process leading to cartilage degradation and loss.4–7 The normal synovium is devoid of inflammatory cells. However, early-onset synovitis results in significant over-expression of pro-inflammatory mediators and cytokines, infiltration of inflammatory cells, production of degradative enzymes, synovial neo-vascularization, and increased expression of the inflammatory biomarker C-reactive protein, as well as marked hyperplasia and permeability of the synovial lining.1,4,5,7–10 In the joint micro-environment, synovitis becomes a potent driver of OA changes including cartilage loss, osteophyte formation, bone remodeling, and joint space narrowing. Studies in dogs have shown that synovitis is a consistent and prominent feature of symptomatic but pre-radiographic joint pathology, occurring well before significant osteoarthritic changes occur.11–14 Large-scale, prospective human studies have shown that even low-grade synovitis is associated with progression of cartilage lesions and more severe baseline chondropathy, more severe OA progression, and progression to joint replacement.15–17 The inflammatory cascade also sensitizes synovial neurons, eliciting a pain response superimposed on the joint degradation process.18,19
The RSO mode of action is macrophage apoptosis and localized ablation of inflamed synovial cells, resulting in some scarring and reduced vascularity. This is the result of IA injection of a radionuclide, an isotope that emits ionizing radiation, which penetrates the two-to-three cell thickness of the synovial membrane. This approach has several noteworthy advantages. By limiting its therapeutic activity to the synovium and avoiding systemic distribution or effects, RSO enables extra-articular co-therapies to be used without restriction, including those with systemic effects such as NSAIDS. When used as a localized co-therapy, RSO can potentially reduce reliance on daily NSAIDS with their known potential for toxicities.20,21 When administered at the outset of or early in the OA pathway, RSO potentially limits, delays, or prevents irreversible osteoarthritic pathology. Radiosynoviorthesis also has a relatively long duration of activity so that its analgesic and anti-inflammatory effects can persist for weeks or months after a single IA injection.22–24
Radiosynoviorthesis originated in Europe, where it has a history of success for outpatient treatment of OA as well as rheumatoid arthritis and psoriatric arthritis in human patients.20,25–27 For example, a review of five studies of rhenium-186 reported a 40–78% reduction in OA symptoms lasting 6–18 months in treated joints (n=133) of human patients.26 Early types of RSO used high-energy, beta-emitting radionuclides such as yttrium-90 (90Y), rhenium-186 (186Rh), and erbium-169 (169Er), which have a relatively wide tissue penetration range of 50–5000 µm and a relatively short half-life (t½) of 3–10 days.20,25–27 While these radionuclides have been widely used in clinical practice, they have two limitations: variable degrees of soft tissue penetration, which risks irradiation of non-target tissue, and short half-lives, which create storage and logistical problems and may deliver irradiation of insufficient duration for optimum effect.
The radionuclide 117mSn (tin-117m) embedded in a homogeneous colloid is a novel RSO designed for IA administration to treat synovial inflammation and mitigate OA in dogs.22,24,28–31 In contrast to the high-energy beta radiation emitted by earlier RSO agents, tin-117m emits low-energy conversion electrons, which have a short, non-diminishing, well defined tissue penetration range of ~300 µm (0.3 mm), approximating the synovial thickness, and a t½ if 14 days.22,24,30,31 These properties give tin-117m radio-emissions a precise range of penetration that avoids exposing non-synovial tissues to radiation, and a duration of effect that spans several half-lives (approximately 42–90 days), sufficient to exert a sustained therapeutic effect for up to a full year.27
Earlier studies in client-owned dogs with elbow OA demonstrated that tin-117m reliably avoids treatment-associated adverse effects and provides significant analgesia lasting up to 12 months following a single IA injection.28,29 In one study, the investigators reported a 89.5% (17/19) positive treatment success rate in dogs with grade 1 and 2 elbow OA as determined by force plate analysis. In a study of dogs with more advanced grade 3 elbow OA, the success rate varied from 66.7% to 72.% depending on the post-treatment interval, which ranged from 90 to 365 days.24 The study reported here is an extension of an earlier study that evaluated clinical effectiveness of tin-117m in dogs with grade 1–2 elbow OA.31 Our objective was to determine if a repeat injection of tin-117m can be safely given in the same joint a year after the original IA dose, and if a favorable clinical response was observed six months after administration of the repeat injection (18 months after the original IA injection).
Materials and Methods
Study Animals
Ten client owned dogs (N=8 male, 2 female) residing with their caretakers were enrolled in the study. Dogs ranged in age from 3.75–12.0 yrs (mean 7.5 yrs) and in weight from 14.7–47.5 kg (mean, 32.1 kg). All dogs were previously diagnosed with naturally occurring, clinically apparent grade 1 or 2 elbow OA, and participated in an earlier study evaluating the clinical response to IA injection of tin-117m colloid into the elbow joint.31 Owners provided written consent for experimental RSO treatment of their dogs and participation in the 12-month repeat injection study. Dogs were managed in accordance with the Institutional Care and Use Committee (IACUC) welfare protocols at their respective centers. The University of Missouri College of Veterinary Medicine study reference number is 49062 and the Louisiana State University (LSU) School of Veterinary Medicine study reference number is 44181. The amendment to IACUC protocol #16-008 to conduct this re-injection study was reviewed and approved by the LSU School of Veterinary Medicine Clinical Protocol Committee and by the LSU Institutional Animal Care and Use Committee.
Therapeutic Device
The radio-therapeutic device was a sterile, homogeneous colloid of tin-117m in ammonium hydroxide solution with a pH of 6.5–9.0, supplied as a 2–4 mCi (74–148 MBq)/mL) sterile suspension packaged in single-patient vials (Synovetin OA®, Exubrion Therapeutics, Buford, GA). Each dose had a potency of 1.75 mCi (64.75 MBq) for an IA dose administered to a 22.7 kg (50 lb) dog. Individual dosages were calculated based on the dog’s body surface area adjusted relative to a 22.7 kg dog. Prior to administration, the vial was gently shaken for approximately 10 seconds to ensure proper mixing of the tin-117m colloid, and then administered by IA injection with a 22-guage needle. The procedure was performed during general anesthesia while the dog was in lateral or dorsal recumbency depending on the clinician’s preference. A detailed description of the anesthesia protocol and injection procedure has been previously described.24,31
Study Sites
The study was conducted at two centers, the School of Veterinary Medicine at Louisiana State University, and the College of Veterinary Medicine at the University of Missouri. The primary investigator at each site performed all diagnostic evaluations, clinical assessments of pain, and ensured compliance with the study protocol and animal welfare guidelines.
Study Design
The study was an extension of an earlier, pilot study where dogs with bilateral grade 1–2 elbow OA were treated with IA injection of tin-117m colloid in one of the affected joints.31 The tin-117m dosage in the pilot study varied from 1.0 to 2.5 mCi per injection. In the follow-up study described in this report, dogs were given an injection of the same therapeutic device at the recommended dosage of 1.75 mCi in both elbows, one of which had been previously treated ≤12 months earlier. This format allowed comparison of elbows that had been treated once or twice in each dog.
Dogs that received the recommended tin-117m dose were classified as per-protocol (PP) animals. Dogs that received a dose >20% greater or less than the recommended dose were designated as intent-to-treat (ITT) animals. Diagnostic samples for purposes of safety evaluation were obtained at the pre-treatment baseline (BL) and at 180 days after treatment. All testing of diagnostic samples was performed by an independent laboratory. A nuclear scintigraphy scan of each treated joint was performed within 24 hours and 90 days after treatment to confirm in situ retention of the tin-117m colloid and to determine if there was distribution of the radionuclide beyond the synovial target tissue. Disease progression in treated elbows was evaluated by various diagnostic imaging methods performed at BL of the original grade 1–2 elbow OA study, at BL of the repeat-injection study, and 180 days thereafter. Pain assessments in the repeat-injection study were performed on-site at BL, 90, and 180 days by clinicians and clients.
Disease Progression
Disease progression in treated joints was determined by three imaging methods performed under general anesthesia at BL and at 180 days: radiographs, computed tomography (CT), and magnetic resonance imaging (MRI). All diagnostic images were evaluated by a board-certified radiologist. The presence of grade 1 or 2 elbow OA at BL was radiographically confirmed in each treated elbow. Elbows were assigned a disease progression score at the 180-day time point. A score of −1 (worse), 0 (no change), or +1 (improved) was determined based on osteoarthritic changes from BL as indicated by joint space changes and presence of erosions, bony fragments, sclerosis ankylosis, osteochondrosis dissecans (OCD) lesions, or periarticular osteophytes.
Radiography was performed with dogs placed in two positions, lateral recumbency with the x-ray centered on the medial epicondyles of the elbow, and sternal recumbency with the x-ray centered over the elbow joint and angled 20 degrees from vertical. Computed tomography and MRI scans of treated elbows were performed to identify elbow OA lesions not evident on radiographic evaluation.
Magnetic resonance imaging was performed to identify pre-existing conditions not evident on radiographs. Following induction of anesthesia, dogs were placed in either dorsal or sternal recumbency, whichever provided the most stable positioning on the imaging table. The elbow joints were encircled with an imaging coil, which receives the signal from the tissue. The dog’s position was maintained using a vacuum‐locked positioning device. The dog was then moved into the imaging volume of the MRI scanner using the incorporated table. Once the dog was in position within the scanner, 2‐5 scanning sequences lasting from 4‐8 minutes each were obtained. The scan sequences chosen were optimized for evaluation of the joint structures including subchondral bone, cartilage, supporting ligaments and synovium. The continuous MRI variables used to measure disease progression were cranial joint pouch width, caudal joint pouch width, cranial synovial body width, and caudal synovial body width. Categorical MRI variables were medial coronoid process fragmentation presence, radial ulnar subchondral joint erosion, and the disease progression rating from BL or previous visit. Categorical variables assessed by CT to measure disease progression included medial coronoid process fragments, radial ulnar joint erosion, presence of OCD lesions in the humerus or proximal radius, sclerosis of the semilunar notch, width of the humeral ulnar or humeral radial joint, presence of periarticular osteophytes, and disease progression rating. A four-point scoring system was used to grade OA lesions such as osteophyte formation using the following scale:
Grade 0 = absence of lesions
Grade 1 = minor lesion severity
Grade 2 = moderate lesion severity
Grade 3 = severe lesion severity
Safety Assessment
Blood samples were collected from each dog by venipuncture to obtain complete blood count and serum chemistry values. Urinalysis was performed for a 20–30 mL sample obtained from each dog by free catch or ultrasound-guided cystocentesis. Joint fluid aspiration of a 0.5–1.0 mL sample from both elbows of each dog was performed immediately before tin-117m injection and 180 days after treatment to evaluate cellular and protein composition of the joint fluid samples.
Nuclear scintigraphy was performed for each dog at BL and 90 days after injection. An Anger camera collimator was positioned for a one minute period on each treated joint and the dog’s abdomen immediately after IA injection of tin −117m colloid and at 90 days post treatment. Lymph nodes and the liver were scanned for each dog to determine if extra-articular uptake of colloid occurred at these sites.
Pain Assessment
Joint pain in the study animals was measured by two methods, dog owner subjective assessments of pain severity and pain interference with normal activity, and an objective force plate analysis performed by the study investigators. Dog owners completed a CBPI survey at BL, 90 and 180 days. The CBPI instrument has been validated for canine OA and cancer pain,32–35 and consists of two components, a four-item pain severity score (PSS) and a six-item pain interference score (PIS). Numerical PSS scores were assigned on a scale ranging from 0 indicating no pain to 10 indicating extreme pain. The scale for the PIS (pain interference scale) is 0, indicating no interference, to 10, indicating complete interference The CBPI success rate was defined as an improvement of ≥1.0 in the PSS score or Improvement of ≥2.0 in the PIS score. Because the study animals were client owned and did not reside at the study center, clinical exams to assess pain or treatment safety were performed only at 90-day intervals from BL to 180 days.
Force plate analyses were conducted at BL, 90, and 180 days for dogs in the PP population. Investigators at both study sites used the same commercially available FP software (Acquire version 7.3, Sharon Software, Inc., Dewitt, MI) and gait analysis platform (Model OR6-WP-1000, Advanced Medical Technology, Newton, MA). Each dog underwent five successive FP trials at each time point, with the data analyzed for peak vertical force (PVF) and mean vertical impulse (MVI) as previously described.31 If the change in PVF or MVI was found to be ≥5% greater than at BL for either forelimb at either the 90 or 180 day time point, the RSO treatment was considered to be successful.
Statistical Analysis
Data analyses were performed with statistical analysis software (SAS, version 9.4, SAS Institute Inc, Cary, NC). For those variables that were assessed for each elbow, the elbow was the experimental unit. For those variables that could only be evaluated for the whole animal, the dog was the experimental unit. For determination of treatment success, tests of statistical significance were completed at a two-sided alpha level of 0.05. Safety variables were evaluated at a two-sided alpha level of 0.10. Within-group P-values for the changes from BL to day 180 were generated by either the paired t-test or Wilcoxson signed rank test, depending on the distribution of data. For the CBPI assessments, comparisons were made for mean values obtained at BL and Days 90 and 180. No hypothesis testing was performed for the CBPI or FP results.
Results
Study Population
Of the 10 dogs originally enrolled, nine received the intended IA dose of tin-117m colloid and were considered PP animals. One dog that received a delivered dose that was >20% below the intended dose (1.65 mCi vs 2.19 mCi) was considered an ITT animal. Safety of the tin-117m device was evaluated for all 10 dogs. Pain was assessed only in the nine PP dogs.
Safety Assessment
There were no local or systemic adverse events associated with tin-117m injection in any of the study dogs. Joint fluid cellular composition in treated elbows at 180 days varied from BL as shown in Table 1. There was an increased percentage of joint fluid neutrophils and lymphocytes, and a significant (P=0.0411) decrease in the percentage of monocytes. There were some significant variations compared to BL in some CBC and clinical chemistry values in ITT dogs (Table 2), but none of the mean values for these parameters was outside the diagnostic reference range. There were no statistically significant differences in urinalysis parameters from BL to day 180, and none of the mean urinalysis values were outside the reference range.
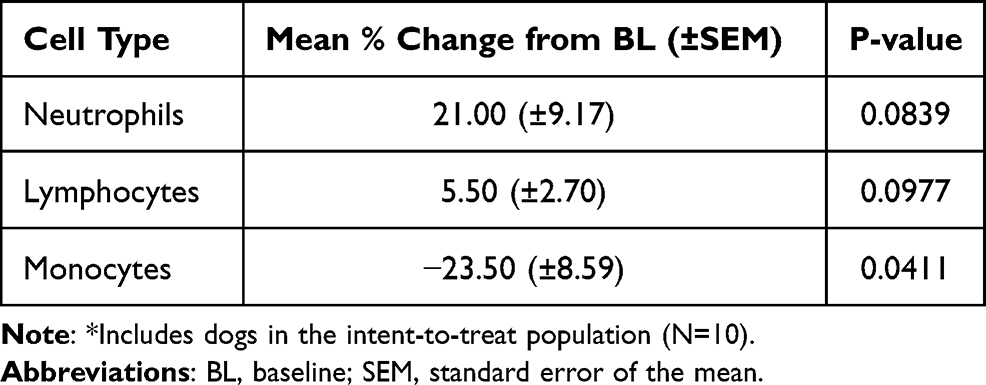 |
Table 1 Mean Variations from Baseline in Joint Fluid Cellular Composition in Dogs* 180 Days After Repeat Injection with Tin-117m Colloid |
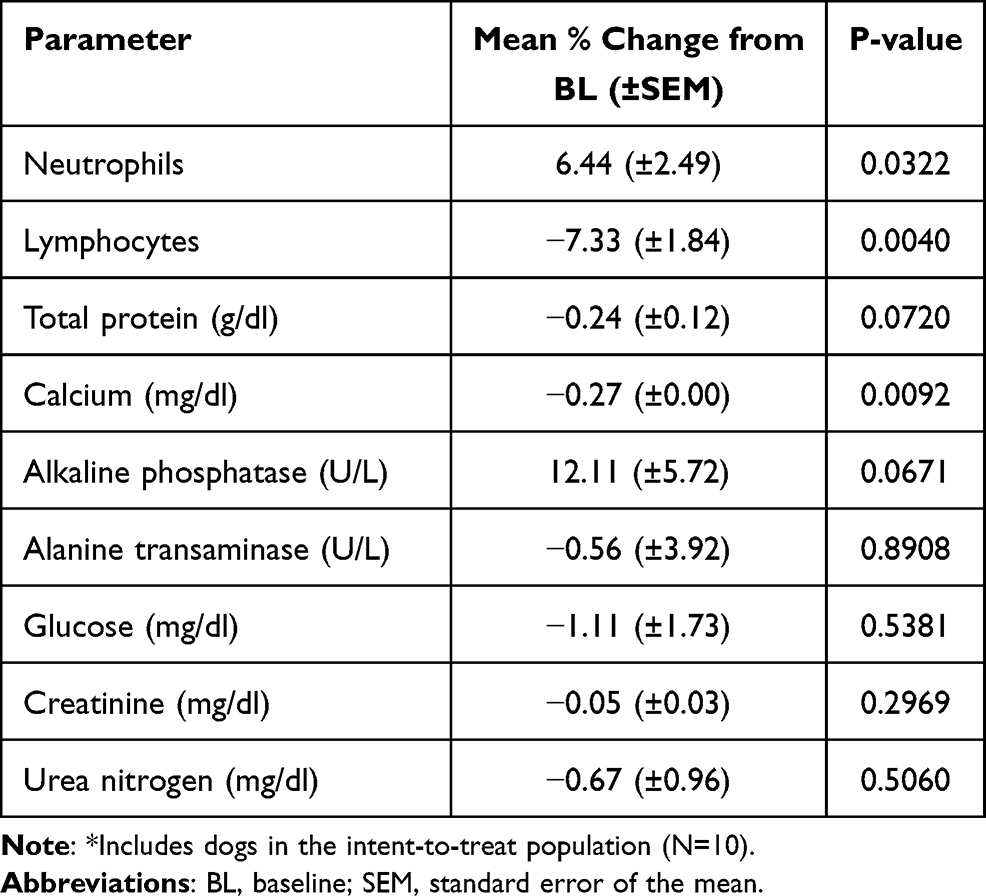 |
Table 2 Mean Variations from Baseline in Blood Count and Clinical Chemistry Values in Dogs* 180 Days After Repeat Injection with Tin-117m Colloid |
Nuclear scintigraphy confirmed the presence of >99% of tin-117m colloid in all 20 treated joints of the ITT population within 24 hrs after IA injection. At 90 days after injection, scintigraphy showed the colloid was still retained in situ in all dogs. There was no uptake in draining lymph nodes in eight dogs at either time point. There was minor accumulation in the draining lymph nodes of two dogs, one on day 1 and another on day 90. The dog that had minor lymph node colloid presence on day 1 also had slight accumulation in the liver on day 90. Colloid presence was not detected in other abdominal organs of any treated dog.
Disease Progression
Disease progression from BL to day 180 in treated elbows of dogs in the PP group as determined by the three imaging modalities (radiograph, CT, and MRI) is summarized in Table 3. For elbows that received two IA tin-117m injections, radiographic analysis showed a significant (P<0.05) increase in mean OA severity from BL of the original grade 1–2 study to day 180 of the repeat-injection study (an 18-month period). For elbows that received one tin-117m injection, the difference in mean OA severity from the repeat-injection BL to day 180 (a 6-month period) was non-significant.
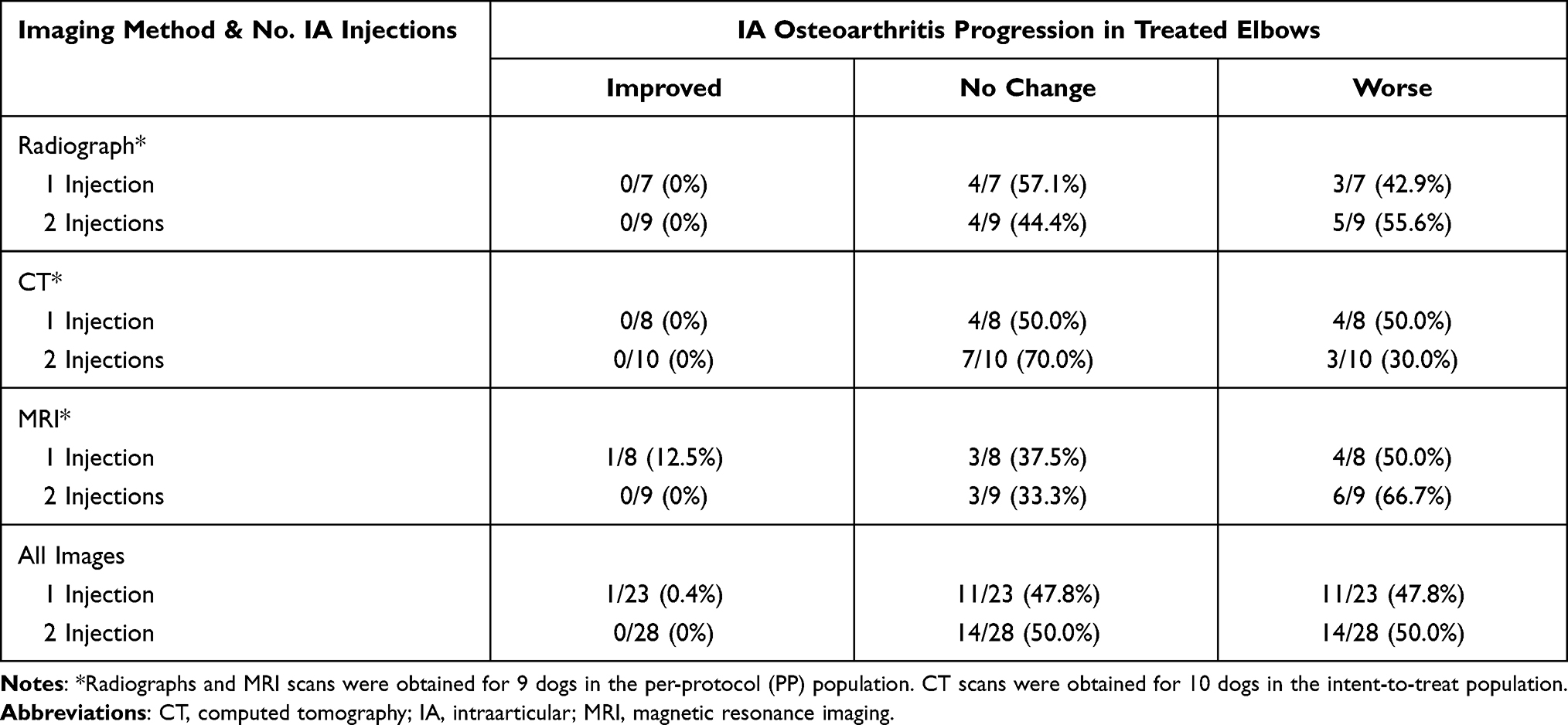 |
Table 3 Summary of Disease Progression Outcomes Determined by Diagnostic Imaging of Canine Elbow Joints 180 Days After Injection with Tin-117m |
There was little difference in the incidence of disease progression in elbows that received one or two IA injections of tin-117m colloid. Disease progression was shown in 11/23 (47.8%) images of elbows that received one IA injection versus 14/28 (50.0%) images of elbows that received two IA injections. Only one imaging study showed improvement in osteoarthritic lesions, an MRI scan of an elbow that was treated with a single IA dose of tin-117m colloid. All other images showed no change in OA progression in elbows given one or two IA injections.
Computed tomography results showed a significant increase (P=0.0169) in severity of periarticular osteophytes from the BL of the original grade 1–2 study to day 180 of the current study (Table 4). For example, the incidence of grade 1 osteophyte formation at the original grade 1–2 study BL declined from 44.4% (8/18 elbows) to 5.6% (1/18) at 180 days, while the incidence of severe, grade 3 osteophyte formation increased from 5.6% (1/18) prior to treatment to 27.7% (5/18) at 180 days.
 |
Table 4 Computed Tomography Evaluation of Periarticular Osteophyte Severity in Elbow Joints of Dogs at Baseline and 180 Days After Intraarticular Injection with Tin-117m Colloid |
Pain Assessment
The mean CBPI scores reported by owners of dogs in the PP population showed reductions in pain severity and pain interference at the 90 and 180-day time points compared to BL (Table 5). The mean PSS and PIS both declined by >1.0 point at 90 days and remained lower than BL by 0.9–1.1 points at 180 days. The CBPI success rate was 55.5% (5/9 dogs) at 90 days and 44.4% (4/9) at 180 days. One of the nine PP dogs had a PSS score that increased from BL (by 0.75 points at 90 days). Another dog had a PIS score that increased from BL (by 0.83 points at 90 days and 1.33 points at 180 days). Thus, while 5/9 PP dogs met the CBPI criteria for treatment success, only two dogs had an increased pain score at either the 90- or 180-day time points.
 |
Table 5 Clinical Assessments of Pain in Dogs* Receiving Repeat Elbow Joint Injections of Tin-117m Colloid |
Force plate results (Table 5) measured by the study investigators for the PP dogs showed ≥5% improvement in PVF or MVI in 5/9 dogs (55.5%) at 90 days and 6/9 dogs at 180 days (66.6%) after RSO treatment. Table 6 shows FP symmetry indices for eight PP dogs comparing the PVF and MVI ratios. The indices were calculated as the ratio of FP values for elbows treated twice divided by the values for the elbows treated once. One PP dog was excluded from the symmetry index calculation because both elbows received two injections.
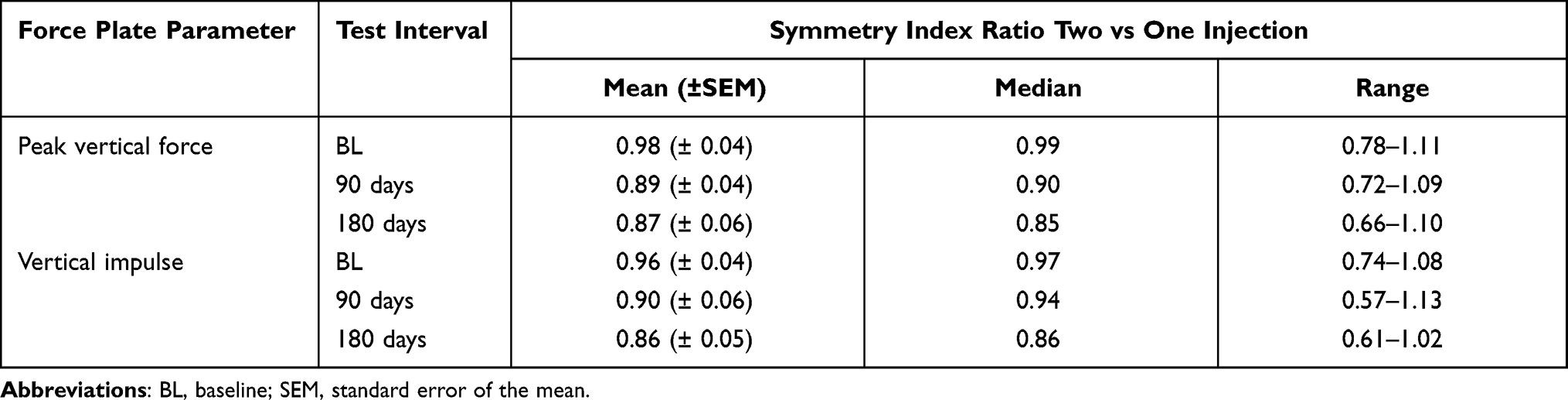 |
Table 6 Ratio of Force Plate Values for Canine Elbows Given Two versus One Tin-117m Injections |
Discussion
The possibility of therapeutic overuse leading to adverse side effects is a concern for any novel treatment, particularly one involving a radionuclide. This is the first study to evaluate the extent of adverse sequelae occurring after a repeat dose of tin-117m colloid in the same joint. The absence of any post-injection local or systemic side effects in any of the treated joints or treated dogs was a strong affirmation that tin-117m colloid is suitable for multi-dose treatment of the same joint, with an appropriate interval between doses.
Joint fluid analysis showed a nearly 25% (P=0.0411) percentage reduction in the mean monocyte population in the ITT dogs (Table 1). Synovitis leads to massive over-expression of macrophages derived from their monocyte precursors in synovial tissue as an expression of joint inflammation in cases of OA.1,12,36 Synovial macrophages then proceed to mediate osteophyte formation in osteoarthritic joints.12,37 Macrophages in the inflamed synovium phagocytize tin-117m colloid particles, where they remain in situ until macrophage apoptosis occurs, thereby exerting a therapeutic effect by eliminating the inflammatory cells.28 Thus, marked reduction in the IA monocyte population in treated joints was an indirect confirmation of the tin-117m colloid mode of action, and an indicator that RSO mitigates the pro-inflammatory process in the joints of treated dogs. The fact that significant monocyte reduction persisted at the 180-day time point after RSO treatment indicates that tin-117m colloid has a durable therapeutic effect lasting six months or more. This extended therapeutic response was not unexpected. Recent studies in human patients with knee OA reported a sustained clinical benefit at 12 months after RSO treatment with yttrium-90.38,39
A recent study in laboratory animals using an artificially induced arthritis model provided a convincing demonstration that (1) insufficient apoptosis of inflammatory macrophages and osteoclasts in joints with advanced arthritis contributes to persistent joint inflammation and pervasive joint destruction, and (2) joint-specific apoptosis of inflammatory cells can restore normal joint function and enable bone erosion repair.40 The investigators found that each major component of the arthritic inflammatory environment was positively correlated with a superabundance of CD68+ synovial macrophages and synovial hyperplasia in test animals. Investigators treated arthritic joints with targeted delivery of celastrol, a cytotoxic chemotherapy drug that selectively induced apoptosis of synovial macrophages and osteoclasts. Used as the sole therapy in rats with advanced arthritis, the joint-specific inflammatory-cell apoptosis significantly (P<0.0011) reduced the number of osteoclasts and inflammatory synovial macrophages compared to normal control joints. While the study evaluated a different therapy than RSO, it confirmed that OA therapy should target synovial inflammation as the principal lesion in DJD, and it demonstrated that apoptosis of synovial inflammatory cells is a therapeutic concept that is both effective and practical.
The scintigraphy results showed virtually complete in situ retention of the tin-117m colloid, with scant dispersal to the lymphatic system or liver of two of 10 ITT dogs. This result indicated that uptake of the RSO agent is almost entirely limited to the synovial target tissue and posed little if any periarticular or extra-articular safety risk. This finding is consistent with earlier studies demonstrating high synovial retention (ie, >99%) of the tin-117m homogeneous colloid.28,29 While the carefully controlled size of the colloid particles in the tin-117m RSO device is small enough to be phagocytized by synovial macrophages, it is too large to escape the joint confines.28 Normal clinical chemistry, CBC, and urinalysis results for all ITT dogs were further confirmation that the tin-117m colloid does not pose a systemic safety risk.
Results across multiple imaging modalities indicated that approximately half the treated elbow joints underwent some degree of joint remodeling and OA disease progression over the 180-day study period. Disease progression was similar whether one or two IA doses of tin-117m were administered, 47.8% and 50.0% respectively, indicating that the repeat RSO injection had no effect, either positive or negative, on the extent or speed of joint remodeling. Periarticular osteophyte severity in some dogs increased significantly (P<0.05) from BL of the original grade 1–2 study to 180 days (ie, 18 months after the first tin-117m injection) as measured by CT, an imaging method with greater sensitivity than radiographs for osteophyte and loose body detection.41
The possibility that tin-117m colloid can modify OA disease progression has been suggested.24 The fact that there was no change in OA progression in approximately half the treated joints in PP dogs over a six-month period (Table 3) would support this hypothesis. However, once joint remodeling and arthritic changes occur, reversal of this pathology is not possible. Thus, any potential for RSO-mediated disease modification assumes treatment early in the OA pathogenesis when synovitis is the sole lesion and before onset of radiographic changes and progression to irreversible chronic disease. This likely explains why approximately half the treated limbs experienced some degree of post-RSO disease progression.
Although disease progression occurred in some dogs during the six-month study period, it had little correlation to limb function as determined by CBPI or FP pain assessments, a key finding of the study. Although not limb-specific, dog owners’ subjective CBPI pain assessment indicated that treatment was successful at 90 days in slightly more than half (5/9, 55.5%) of the PP dogs. Importantly, only two of the nine PP dogs had increased 90- or 180-day CBPI pain scores. The fact that all of the other PP dogs had stable or improved CBPI pain scores for the duration of the study indicates that the RSO treatment with tin-117m colloid has an extended analgesic benefit lasting as long as six months. This conclusion is supported by results of the objective FP analysis showing improved weight bearing as well as treatment success rates of 55.5% (5/9) at 90 days and 66.6% (6/9) at 180 days. The positive CBPI and FP results were obtained despite radiographic evidence of OA disease progression in some dogs. This outcome suggests that suppression of joint inflammation rather than mitigation of joint remodeling is the principal factor in pain reduction. In fact, human studies using sensitive, contrast-enhanced MRI have found that synovitis and inflammatory cell infiltration are highly correlated with pain severity in cases of OA.18,42 In the Multicenter Osteoarthritis Study (MOST), patients with extensive knee joint synovitis had 4.8 times the odds of mild pain (vs no pain) and 9.2 times the odds of severe knee pain compared to individuals without synovitis, with the amount of pain correlating to the extent of the synovitis.42 In contrast, a large number of MOST patients without radiographic evidence of OA had knee pain concurrent with synovitis. Experts have noted that structural, radiographic evidence of OA is poorly correlated with pain symptoms.18
A limitation of the study was the small number of dogs evaluated. This was due primarily to the difficulty of maintaining dog owner participation for the 12-month duration of the original grade 1–2 study followed for an additional six-month study period for the repeat-injection study. In addition, using a placebo or control group was impractical since dog owners would have to be advised for ethical reasons if a patient was treated with a radionuclide. Given these factors, the study is suitably described as observational rather than experimental in design. The joint fluid analysis did not compare the cytology results with synovial biopsy or electron microscopy of tissue samples. This would be a suitable topic for further study. Histopathologic evidence of synovitis in the test animals was not determined, and would have contributed to more definitive conclusions on the therapeutic effect of RSO. Study animals did not reside at the test sites, limiting the frequency of post-treatment clinical exams to 90-day intervals. However, dog owners consistently reported absence of adverse treatment effects in elbows that were injected either once or twice with tin-117m.
As other investigators have noted, there are an assortment of factors that cause variances in FP results.43,44 The 5% threshold for clinically relevant FP improvement is consistent with standards used in other studies,35,45 and is an objective indicator of pain reduction in more than half of the RSO-treated dogs. In our analysis, FP data was not compared for the twice-treated vs contralateral limb but analyzed for the dog as the unit of variance.
An important aspect of RSO with the tin-117m colloid is that it can be used either as an effective stand-alone treatment or in a multimodal regimen. As clinical experts have noted, there is a critical need for agents other than NSAIDS for treatment of DJD in dogs.46 Evidence in this and earlier studies indicates that tin-117m can provide significant clinical benefit when used as a sole therapy.22,24,29,31 Using tin-117m colloid with other treatment modalities is always an option; the device has no contraindications for use as a co-therapy. Radiosynoviorthesis is the only OA modality that selectively targets the synovium as the primary lesion in DJD. It is one of the few treatments with a long-term therapeutic effect following an initial dose.
Radiosynoviorthesis is a localized, conservative therapy, potentially precluding the need for more aggressive treatment options including joint replacement or chronic pharmacotherapy with NSAIDS or other agents with known toxicities. Radiosynoviorthesis has a high margin of safety and a rapid onset of effect. In view of its record of safety and clinical effectiveness in this and other studies, veterinarians are justified in considering the use of RSO with tin-117m colloid as a component of their treatment protocol for canine elbow OA, one of the most common arthritides of dogs. A comprehensive review of RSO as a medical procedure has recently been published by the International Atomic Energy Agency.47
Study results for the six-month period after repeat IA injection with tin-117m colloid revealed that the 10 dogs in the ITT group were free from clinical or laboratory diagnosed adverse effects, the primary finding of this study. This indicated that a repeat dosage of tin-117m colloid in the same joint at a one-year interval has minimal safety risks. Stable radiographic and other imaging results in some dogs indicate that repeat IA injection of tin-117m colloid can potentially delay OA progression during a one-year post-treatment period, and may extend the therapeutic effects of RSO in a subset of dogs with grade 1–2 elbow OA. Pain reduction results in tin-117m colloid-treated dogs at 90 and 180 days indicate that RSO can improve the quality of life of dogs with elbow OA.
Acknowledgments
Mark Dana of Scientific Communications Services, LLC prepared the manuscript.
Disclosure
The study was funded by Exubrion Therapeutics, Inc. Dr. Aulakh is an advisory board member for Exubrion Therapeutics, Inc. Dr John Donecker reports personal fees from Exubrion Therapeutics, during the conduct of the study; personal fees from Exubrion Therapeutics, outside the submitted work. Dr Jimmy C Lattimer reported grants from Exubrion Therapeutics, during the conduct of the study. Dr Karanvir Singh Aulakh reports grant from Exubrion Therapeutics, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Benito MJ, Veale DJ, FitzGerald O, et al. Synovial tissue inflammation in early and late osteoarthritis. Ann Rheum Dis. 2005;64:1263–1267. doi:10.1136/ard.2004.025270
2. Sellam J, Berenbaum F. The role of synovitis in pathophysiology and clinical symptoms of osteoarthritis. Nat Rev Rheumatol. 2010;6:625–635. doi:10.1038/nrrheum.2010.159
3. Wenham CY, Conaghan PG. The role of synovitis in osteoarthritis. Ther Adv Musculoskelet Dis. 2010;2:349–359. doi:10.1177/1759720X10378373
4. Bondeson J, Wainwright SD, Lauder S, et al. The role of synovial macrophages and macrophage-produced cytokines in driving aggrecanases, matrix metalloproteinases, and other destructive and inflammatory responses in osteoarthritis. Arthritis Res Ther. 2006;8:R187. doi:10.1186/ar2099
5. de Lange-brokaar BJ, Ioan-Facsinay A, van Osch GJ, et al. Synovial inflammation, immune cells and their cytokines in osteoarthritis: a review. Osteoarthritis Cartilage. 2012;12:1484–1499. doi:10.1016/j.joca.2012.08.027
6. Scanzello CR, Umoh E, Pessler F, et al. Local cytokine profiles in knee osteoarthritis: elevated synovial fluid interleukin-15 differentiates early from end-stage disease. Osteoarthritis Cartilage. 2009;17:1040–1048. doi:10.1016/j.joca.2009.02.011
7. Sokolove J, Lepus CM. Role of inflammation in the pathogenesis of osteoarthritis: latest findings and interpretations. Ther Adv Musculoskelet Dis. 2013;5:77–94. doi:10.1177/1759720X12467868
8. Poole AR. An introduction to the pathophysiology of osteoarthritis. Front Biosci. 1999;4(1–3):D662–D670. doi:10.2741/Poole
9. Yang X, Ruan G, Xu J, et al. Associations between suprapatellar pouch effusion-synovitis, serum cartilage oligomeric matrix protein, high sensitivity C-reaction protein, knee symptom, and joint structural changes in patients with knee osteoarthritis. Clin Rheumatol. 2020;39:1663–1670.
10. Ostojic M, Zevrnja A, Vukojevic K, et al. Immunofluorescence analysis of NF-kB and iNOS expression in different cell populations during early and advanced knee osteoarthritis. Int J Mol Sci. 2021;22:6461. doi:10.3390/ijms22126461
11. Klocke NW, Snyder PW, Widmer WR, et al. Detection of synovial macrophages in the joint capsule of dogs with naturally occurring rupture of the cranial cruciate ligament. Am J Vet Res. 2005;66:493–499. doi:10.2460/ajvr.2005.66.493
12. Doom M, de Bruin T, de Rooster H, et al. Immunopathological mechanisms in dogs with rupture of the cranial cruciate ligament. Vet Immunol Immunopathol. 2008;125:143–161. doi:10.1016/j.vetimm.2008.05.023
13. Bleedorn JA, Greuel EN, Manley PA, et al. Synovitis in dogs with stable stifle joints and incipient cranial cruciate ligament rupture: a cross-sectional study. Vet Surg. 2011;40:531–543. doi:10.1111/j.1532-950X.2011.00841.x
14. Hayashi K, Manley PA, Muir P. Cranial cruciate ligament pathophysiology in dogs with cruciate disease: a review. J Am Anim Hosp Assoc. 2004;40:385–390. doi:10.5326/0400385
15. Loeser RF, Goldring SR, Scanzello CR, et al. Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum. 2012;64:1697–1707. doi:10.1002/art.34453
16. Ayral X, Pickering EH, Woodworth TG, et al. Synovitis: a potential predictive factor of structural progression of medial tibiofemoral knee osteoarthritis – results of a 1-year longitudinal arthroscopic study in 422 patients. Osteoarthritis Cartilage. 2005;13:361–367. doi:10.1016/j.joca.2005.01.005
17. Conaghan PG, D’Agostino MA, Le Bars M, et al. Clinical and ultrasonographic predictors of joint replacement for knee osteoarthritis: results from a large, 3-year, prospective EULAR study. Ann Rheum Dis. 2010;69:644–647. doi:10.1136/ard.2008.099564
18. O’Neill TW, Felson DT. Mechanisms of osteoarthritis (OA) pain. Curr Osteoporosis Rep. 2018;16:611–616. doi:10.1007/s11914-018-0477-1
19. McDougall JJ. Arthritis and pain: neurogenic origin of joint pain. Arthritis Res Ther. 2006;8:220. doi:10.1186/ar2069
20. Kampen WU, Voth M, Pinkert J, et al. Therapeutic status of radiosynoviorthesis of the knee with yttrium [90Y] colloid in rheumatoid arthritis and related indications. Rheumatology. 2007;46:16–24. doi:10.1093/rheumatology/kel352
21. Lascelles BD, McFarland JM, Swann H. Guidelines for safe and effective use of NSAIDs in dogs. Vet Ther. 2005;6:237–251.
22. Doerr C, Stevenson N, Gonzales G, et al. Homogeneous Sn-117m colloid radiosynovectomy results in rat models of joint disease. J Nucl Med. 2015;suppl 3:1243.
23. Doerr C, Bendele A, Simon J, et al. Validation of the use of homogeneous Sn-117m colloid radiosynoviorthesis in a GLP osteoarthritis rat model (abstract). J Nucl Med. 2016;suppl2:323.
24. Donecker J, Fabiani M, Gaschen L, et al. Treatment response in dogs with naturally occurring grade 3 elbow osteoarthritis following intra-articular injection of 117mSn (tin) colloid. PLoS One. 2021;16(7):e0254613. doi:10.1371/journal.pone.0254613
25. Karavida N, Notopoulos A. Radiation synovectomy: an effective alternative treatment for inflamed small joints. Hippokratia. 2010;14:22–27.
26. Klett R, Lange U, Haas H, et al. Radiosynoviorthesis of medium-sized joints with rhenium-186-sulfide colloid: a review of the literature. Rheumatology. 2007;46:1531–1537. doi:10.1093/rheumatology/kem155
27. Modder G. Radiosynoviorthesis (Radiation Synovectomy). In: Ahmnadzadehfar H, Biersack HJ, Freeman L, Zuckier L, editors. Clinical Nuclear Medicine, 2nd ed. Berlin: Springer; 2020: 1015-1024.
28. Stevenson NR, Lattimer J, Selting K, et al. Abstract S6-03: homogenous SN-117m colloid–a novel radiosynovectomy agent. World J Nucl Med. 2015;14(Suppl 1):S15–S68.
29. Stevenson NR, St. George G, Simon J, et al. Methods of producing high specific activity Sn-117m with commercial cyclotrons. J Radioanal Nucl Chem. 2015;305:99–108. doi:10.1007/s10967-015-4031-7
30. Lattimer JC, Selting KA, Lunceford JM, et al. Intraarticular injection of a TIN-117m radiosynoviorthesis agent in normal canine elbows causes no adverse effects. Vet Radiol Ultrasound. 2019;60:567–0574. doi:10.1111/vru.12757
31. Aulakh KS, Lopez MJ, Hudson C, et al. Prospective clinical evaluation of intra-articular injection of tin-117m (117mSn) radiosynoviorthesis agent for management of naturally occurring elbow osteoarthritis in dogs: a pilot study. Vet Med Res Rep. 2021;12:1–12.
32. Brown DC, Boston RC, Coyne JC, et al. Development and psychometric testing of an instrument designed to measure chronic pain in dogs with osteoarthritis. Am J Vet Res. 2007;68(6):631–637. doi:10.2460/ajvr.68.6.631
33. Brown DC, Boston RC, Coyne JC, et al. Ability of the Canine Brief Pain Inventory to detect response to treatment in dogs with osteoarthritis. J Am Vet Med Assoc. 2008;233:1278–1283. doi:10.2460/javma.233.8.1278
34. Brown DC, Boston R, Coyne JC, et al. A novel approach to the use of animals in studies of pain: validation of the Canine Brief Pain Inventory in canine bone cancer. Pain Med. 2009;10:133–142. doi:10.1111/j.1526-4637.2008.00513.x
35. Brown DC, Boston RC, Farrar JT. Comparison of force plate gait analysis and owner assessment of pain using the Canine Brief Pain Inventory in dogs with osteoarthritis. J Vet Intern Med. 2013;27:22–30. doi:10.1111/jvim.12004
36. Döring AK, Junginger J, Hewicker-Trautwein M. Cruciate ligament degeneration and stifle joint synovitis in 56 dogs with intact cranial cruciate ligaments: correlation of histological findings and numbers and phenotypes of inflammatory cells with age, body weight and breed. Vet Immunol Immunopathol. 2018;196:5–13. doi:10.1016/j.vetimm.2017.12.006
37. Blom AB, van Lent PL, Holthuysen AE, et al. Synovial lining macrophages mediate osteophyte formation during experimental osteoarthritis. Osteoarthritis Cartilage. 2004;12:627–635. doi:10.1016/j.joca.2004.03.003
38. Oztemür Z, Bulut O, Korkmaz M, et al. Surgical synovectomy combined with yttrium 90 in patients with recurrent joint synovitis. Rheumatol Int. 2013;33:1321–1326. doi:10.1007/s00296-012-2540-z
39. Zeiadin N, Rampakakis E, Turcotte E, et al. Safety and therapeutic value of radiosynoviorthesis with yttrium-90: a Canadian single-centre experience. Rheumatology (Oxford). 2021;60:2434–2439. doi:10.1093/rheumatology/keaa637
40. Deng C, Zhang Q, He P, et al. Targeted apoptosis of macrophages and osteoclasts in arthritic joints is effective against advanced inflammatory arthritis. Nature Commun. 2021;12:2174. doi:10.1038/s41467-021-22454-z
41. Alnusif NS, Matache BA, AlQahtani SM, et al. Effectiveness of radiographs and computed tomography in evaluating primary elbow osteoarthritis. J Shoulder Elbow Surg. 2021;30(7S):S8–S13. doi:10.1016/j.jse.2021.04.001
42. Baker K, Grainger A, Niu J, et al. Relation of synovitis to knee pain using contrast-enhanced MRIs. Ann Rheum Dis. 2010;69:1779–1783.
43. Budsberg SC, Jevens DJ, Brown J, et al. Evaluation of limb symmetry indices, using ground reaction forces in healthy dogs. Am J Vet Res. 1993;54:1569–1574.
44. Jevens DJ, Hauptman JG, DeCamp CE, et al. Contributions to variance in force-plate analysis of gait in dogs. Am J Vet Res. 1993;54:612–615.
45. Vijarnsorn M, Kwananocha I, Kashemsant N, et al. The effectiveness of marine based fatty acid compound (PCSO-524) and firocoxib in the treatment of canine osteoarthritis. BMC Vet Res. 2019;15:349. doi:10.1186/s12917-019-2110-7
46. Lascelles BD, Knazovicky D, Case B, et al. A canine-specific anti-nerve growth factor antibody alleviates pain and improves mobility and function in dogs with degenerative joint disease-associated pain. BMC Vet Res. 2015;11:101. doi:10.1186/s12917-015-0413-x
47. International Atomic Energy Agency. Production, quality control, and clinical applications of radiosynovectomy agents. IAEA Technical Report Series. Available from: https://www.iaea.org/sites/default/files/19/09/radiosynovectomy-agents.pdf.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.