")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Safeguarding the Right to Health of the Elderly in Rural China: A Legal Analysis
Authors Chen Q , Tian W , Zheng L , Li T
Received 11 May 2023
Accepted for publication 4 August 2023
Published 19 August 2023 Volume 2023:16 Pages 1621—1632
DOI https://doi.org/10.2147/RMHP.S420954
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Haiyan Qu
Qiang Chen,1 Wei Tian,2 Long Zheng,3 Taoying Li1,4
1Law School, Xinjiang University, Urumqi, People’s Republic of China; 2Department of Foreign Languages, Guangxi Science & Technology Normal University, Laibin, People’s Republic of China; 3Graduate School and Open Learning College, Cavite State University, Indang, Philippines; 4Department of Law, Jiangxi Police College, Nanchang, People’s Republic of China
Correspondence: Long Zheng, Graduate School and Open Learning College, Cavite State University, Indang City, Cavite Province, Philippines, Tel +8618279129539, Email [email protected]
Abstract: Older people in rural China enjoy the right to health under Chinese law. However, the problems of economic difficulties, the unbalanced allocation of medical resources between urban and rural areas and the weakening of the traditional function of the family as a provider of old-age care in reality make the elderly in rural areas face a higher risk of health problems. The law is an important tool to mitigate these problems. Although China has made great efforts to legally guarantee the right to health of the rural elderly, it has not yet fully implemented the requirements of Article 12 of the International Covenant on Economic, Social and Cultural Rights, Article 14 of the Madrid Political Declaration and International Plan of Action on Ageing. China needs to further improve the relevant legislation to provide adequate legal support for the exercise of the right to health of the elderly in rural areas.
Keywords: elderly people in rural China, the right to health, legal protection, legislation
Introduction
The process of aging is natural, irreversible, and universal from birth onward.1 We can slow down aging, but there is no way to remove it from human life. The United Nations defines the age of the elderly as 60 years or older,2 and China now has the largest number of elderly people in the world, and this number is still growing.3
 |
Figure 1 Average annual income of urban and rural elderly in China, 2000–2014. |
With the decline of mortality, the life expectancy of the world population has been increasing over the past few centuries, which in turn has contributed to global aging, and the situation of China’s population is in line with this pattern.4 In 1956, the document “Population Ageing and its Socio-Economic Consequences” of the United Nations suggested that when the number of people aged 65 and above exceeded 7% of the total population in a country or region, it meant that the country or region had entered ageing; the Vienna World Assembly on Aging in 1982 revised this criterion to 60 and 10%.5 By the end of 2021, China have 267 million people aged 60 and above, accounting for 18.9% of the total population, and more than 200 million people aged 65 and above, accounting for 14.2% of the total population.6 It is expected that around 2035, the elderly population aged 60 and above will exceed 400 million, accounting for more than 30% of the total population.7 China is entering an aging society, and the degree of aging is much higher in rural areas of China than in urban areas.8 In 2020, data from China’s seventh census showed that the proportions of people aged 60, 65 or over in rural areas were 23.81% and 17.72% respectively, which were 7.99 and 6.61 percentage points higher than those in urban areas.9
In 1948, the United Nations promulgated the Universal Declaration of Human Rights, which states in Article 25, “Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services, and the right to security in the event of unemployment, sickness, disability, widowhood, old age or other lack of livelihood in circumstances beyond his control”.
In 1996, the United Nations adopted the International Covenant on Economic, Social and Cultural Rights, a treaty implementing the economic, social and cultural rights enumerated in the Universal Declaration of Human Rights. China ratified the Covenant in March 2001. Article 12 of the Covenant states “The States Parties to the present Covenant recognize the right of everyone to the enjoyment of the highest attainable standard of physical and mental health”.
In 2002, the Madrid Political Declaration and International Plan of Action on Ageing, which was adopted by the Second World Assembly on Ageing, states in article 5 that “We also recognize that persons, as they age, should enjoy a life of fulfilment, health, security and active participation in the economic, social, cultural and political life of their societies”; states in article 14 that “We commit ourselves to providing older persons with universal and equal access to health care and services, including physical and mental health services, and we recognize that the growing needs of an ageing population require additional policies, in particular care and treatment, the promotion of healthy lifestyles and supportive environments”.10
China has combined the goals set out in Article 25 of the Universal Declaration of Human Rights, Article 12 of the International Covenant on Economic, Social and Cultural Rights, and Articles 5 and 14 of the Madrid Political Declaration and International Plan of Action on Ageing with the actual situation in China. Regulations and policies regarding the elderly have been improved and a series of policy measures have been taken to actively guarantee the right to health of the elderly.11 However, there is still room for further improvement in the protection of the right to health of the elderly in China, especially for the elderly in rural areas. In China, there are large differences in personal income and living environment between the rural elderly and the urban elderly,12 and a large number of the rural elderly are facing problems such as low income, multiple illnesses and mental isolation.13 The long-standing urban-rural dichotomous system in China has led to poorer treatment of rural elders compared to urban elders in terms of health insurance and health care,14 which means that the rural elderly may face higher health risks. In China, the suicide rate among rural elders is three to four times higher than that of urban elders and five times higher than that of the general population,15 and among rural elders with suicidal ideation, most have varying degrees of health problems.16 Although China has made considerable efforts to protect the right to health of rural elderly people, and relevant laws and policies involving the protection of the right to health of rural elderly people have been adjusted several times, there are still certain flaws in the legal protection of the right to health of the rural elderly. Therefore, the article firstly explains the dilemma of exercising the right to health of the rural elderly, then analyzes the legal protection of the right to health of the rural elderly and its shortcomings, and finally puts forward some feasible suggestions. The number of elderly people in rural China is huge, and the risk of health problems is more serious compared to other groups. Exploring the legal protection of the right to health of elderly people in rural China is important for China as well as other developing countries.
The Dilemma of Exercising the Right to Health of the Elderly in Rural China
Economic Hardships Due to Low Income
Income has a significant impact on people’s physical and mental health.17 In developing countries, an increasing number of elders suffer from health problems that are associated with low income, and their dietary and nutritional status plays a role in these conditions.18 Although rural elders deserve the right to health from an ethical and legal perspective, the economic hardships associated with low income make their situation challenging in practice. This is because economic hardship is a major barrier to health care access for older adults.19 The income structure of the elderly in rural China is relatively simple and consists of four main sources: pensions, financial support from children, proceeds from land transfer, and income from agricultural production and management.20 This paper analyzes the economic difficulties faced by rural elders only from the perspective of income sources.
First, for most of China’s rural elderly, the New Rural Pension Program (NRPP) is the main source of income.21 In 2008, China began to implement the NRPP to provide a new guarantee of “institutional retirement” for the rural elderly.22 The policy specifies that the NRPP fund is composed of individual contributions, collective subsidies, and government subsidies. Rural residents who participate in the new rural insurance system should pay the required pension insurance premiums. The contribution standard is currently set at five levels: 100, 200, 300, 400, and 500 yuan (about $14.9, $29.8, $44.8, $59.7, and $74.6) per year, and Localities can set up additional contribution brackets according to the actual situation, with farmers contributing more and subsidizing more. Although five levels of individual contributions are set, from low to high, most farmers prefer the lowest standard of contribution.23 Once eligible rural elderly people reach the age of sixty, they can receive a pension from a government-provided account.24 As shown in Table 1, farmers in only 6 of China’s 31 provinces (excluding Hong Kong, Macau, and Taiwan) receive a monthly basic pension of 200 yuan (about $29.8) or more. With low individual contribution rates, farmers in most provinces across the country receive pensions between 100 and 200 yuan (about $14.9–29.8).25 If one receives only a monthly pension of 100 yuan (about $14.9), it is obvious that it cannot support the farmers’ pension needs. A 78-year-old rural man in Guangxi confessed, “I used to receive a monthly pension of 120 yuan (about $17.9), and I went to the bank once at the end of each month. This is not enough, I can only say that I can subsidize my life, buy some rice and some oil. I have four children, and I still rely on them as my main source of a life of retirement”.20
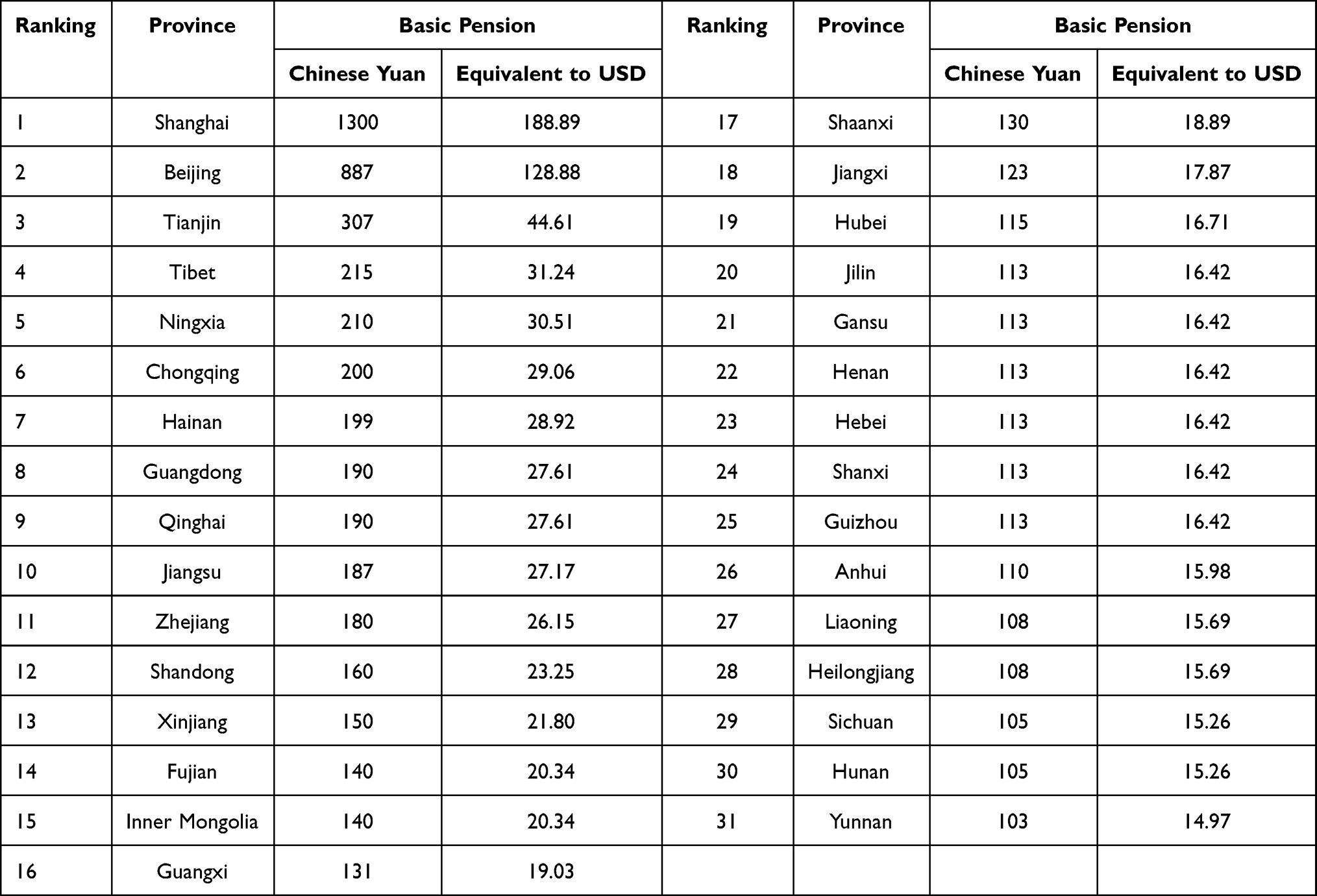 |
Table 1 List of Basic Pension in 31 Provinces (Excluding Hong Kong, Macau, and Taiwan) in China’s Rural Areas |
Second, because the pensions that rural elderly people can receive are not enough to sustain their basic personal life, they mainly rely on their children for their old age.26 Children provide important support for rural elders in their old age and play an irreplaceable role in meeting their economic, material, and spiritual needs.27 The content of children’s support for rural elders’ old age mainly includes both financial support and life care.28 However, in general, there is an exclusionary and substitution relationship between financial support and life care received by rural older adults from their children.29 In other words, if rural older adults receive life care from their children, they have a lower probability of receiving financial support from their children. However, both financial support and life care are indispensable for most rural older adults. In addition, there are also many childless families in China such as the loss of only child families and Dink families. Taking the loss of only child families as an example, over the 30 years of China’s family planning policy, some families have become the loss of only child families due to the death of their only child.30 China annually has approximately 76,000 families bereaved of its only child and has accumulated more than 1 million.31 For such childless families, rural seniors simply do not have access to children for their old age.
Finally, in addition to pensions, land-based income is another relatively stable income for rural elderly people,32 which includes income from land transfer and income from agricultural production and management. For one thing, China’s rural land is under the “three rights” of collective ownership, contractual rights of farmers, and land management rights, and rural land transfer refers to the transfer of rural land management rights. The transfer of rural land management rights refers to the act of the contractor handing over part or all of the land management rights to others to carry out agricultural production and operation independently for a certain period of time and receiving income, provided that the contracting relationship between the contractor and the issuer remains unchanged.33 Older rural people who have the right to contract rural land can earn a certain amount of income through such land transfer. However, given the current average contracted land area and rent level in China, the income from land transfer may have very limited impact on the economic income and quality of life of the rural elderly.34 On the other hand, in fact, close to 70% of the income of the rural elderly in China comes from agricultural production and operation.35 However, around the age of 70 is the dividing line between the income and living status of the rural elderly. Before the age of 70, most of the rural elderly are still able to earn income through agricultural production and operation, and after the age of 70, with the uneven decline of labor capacity, the rural elderly group enters a predicament of both low income and highly unequal distribution and lacks endogenous motivation to get out of it.35
A survey report by the China Scientific Center for Research on Aging shows that in 2014, the annual per capita income of elderly people in urban China reached 23,930 yuan (about $3570.4) and rural elderly people reached 7621 yuan (about $1137.1) (Figure1).36 Despite the large difference in annual income, rural elders have the same needs as urban older adults for health care services. However, rural older adults in financial hardship are less likely to use increasingly expensive health services frequently because they have little cash available.37 Finally, the report shows that only 27.7% of rural older adults rated their health status as “good”, which is significantly lower than the 37.6% of urban older adults.36 It is certain that financial difficulties are the core reason for the self-conscious unhealthiness of some rural older adults.
Irrational Allocation of Medical Resources Between Urban and Rural Areas
In China, a large amount of high-quality medical resources are concentrated in large cities and large hospitals, and the problem of unreasonable allocation of medical resources between urban and rural areas still exists.38 By analyzing data from the 2022 China Health Care Statistics Yearbook39 developed by the National Health Care Commission of China, it is clear that in terms of medical funding, in 2016, the health expenditure invested in rural areas was 1,088,687,000,000 yuan (about $162,490,597,000), and the health expenditure invested in urban areas was 3,545,801,000,000 yuan (about $529,224,030,000), with urban areas being 3.26 times higher than rural areas; in terms of health personnel, in 2021, the ratio of urban and rural health technicians per 1000 population is 1.57:1, the ratio of urban and rural licensed (assistant) physicians per 1000 population is 1.54:1, and the ratio of urban and rural registered nurses per 1000 population is 1.73:1; in terms of facility configuration, in 2021, the number of beds in medical and health institutions per 1000 population in urban areas is 7.47, and the number of beds in medical and health institutions per 1000 population in rural areas is 6.01, that is to say urban areas is 1.24 times more than in rural areas (Figure2). Obviously, compared to urban areas, medical resources in rural areas are scarcer. In this context, rural seniors need to spend more time and money to travel to big cities, which are farther away, in order to get better medical services. However, traveling long distances to large cities may not be the best option for rural elders because it may increase their financial burden.40
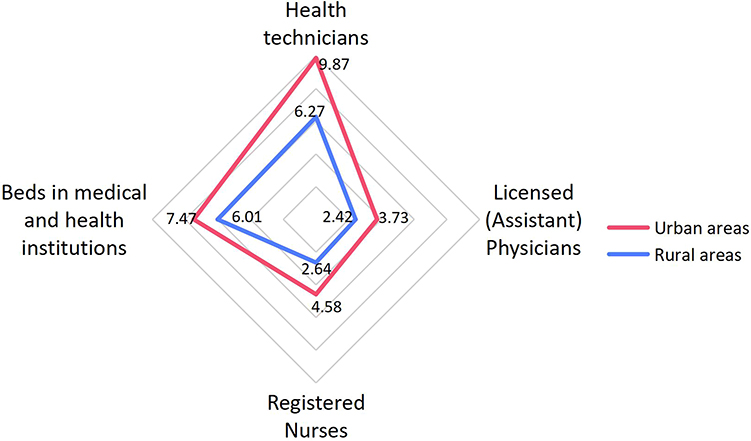 |
Figure 2 The number of health personnel and the distribution of health facilities per 1,000 population in urban and rural areas, China, 2021. |
The Phenomenon of Labor Migration Has Weakened the Traditional Family Retirement Function
With the rapid development of industrialization and urbanization in China after the reform and opening up, a large number of young and middle-aged rural population migrated to large and medium-sized cities to work and earn higher income than in agricultural production and operation.41 At the same time, a special group of elderly people left behind in rural areas emerged as a result of labor migration. Older people left behind in rural areas refer to parents who live alone or with their grandchildren in rural areas while their children are working and living in large and medium-sized cities for a long time.42 According to a preliminary mapping survey conducted by the Chinese Ministry of Civil Affairs in 2016, there are about 16 million rural elderly people left behind in China, accounting for about 12% of the total rural elderly population.43 The reduction in the number of potential breadwinners for the elderly in rural areas due to China's strict three-decade-long one-child policy, as well as the large number of young and middle-aged people in rural areas moving to the cities to work and live, have combined to weaken the traditional internal care model of the rural family for the elderly.44 However, the existing social support system does not provide adequate support for this new structure of families in which family members live separately in urban and rural areas.45 The “high income” of their children in the city makes the rural elderly left behind relatively secure in material life, but their psychological and emotional needs are often not met due to the lack of specialized social support services, and their overall quality of life is not high.46 The lack of a good social security system has accelerated the deterioration of the health status of the rural elderly left behind,44 especially in terms of mental health.47,48
Legislative Progress in Protecting the Right to Health of the Rural Elderly in Mainland China
The rule of law has a fundamental and decisive role in guaranteeing the right to health of citizens.49 The State ensures the right to health of its citizens by means of constitutional obligations, laws and regulations.50
In practice, many factors have contributed to the difficulties faced in securing the right to health of the elderly in rural areas in mainland China, including the economic difficulties of the elderly in rural areas, the unreasonable allocation of medical resources between urban and rural areas, the inadequacy of social security, and the inevitable changes in rural family structure in the post-family planning era. Does mainland China’s legislation concerning the right to health of rural elderly people help alleviate these problems? This article argues that, despite the desirable progress of recent legal reforms, many deficiencies remain.
Legislation at the National Level
In China, legislation at the national level refers mainly to laws enacted by the National People’s Congress and its Standing Committee. Based on the Constitution, China has adopted the following laws to protect the right to health of the elderly in rural areas (Table 2).
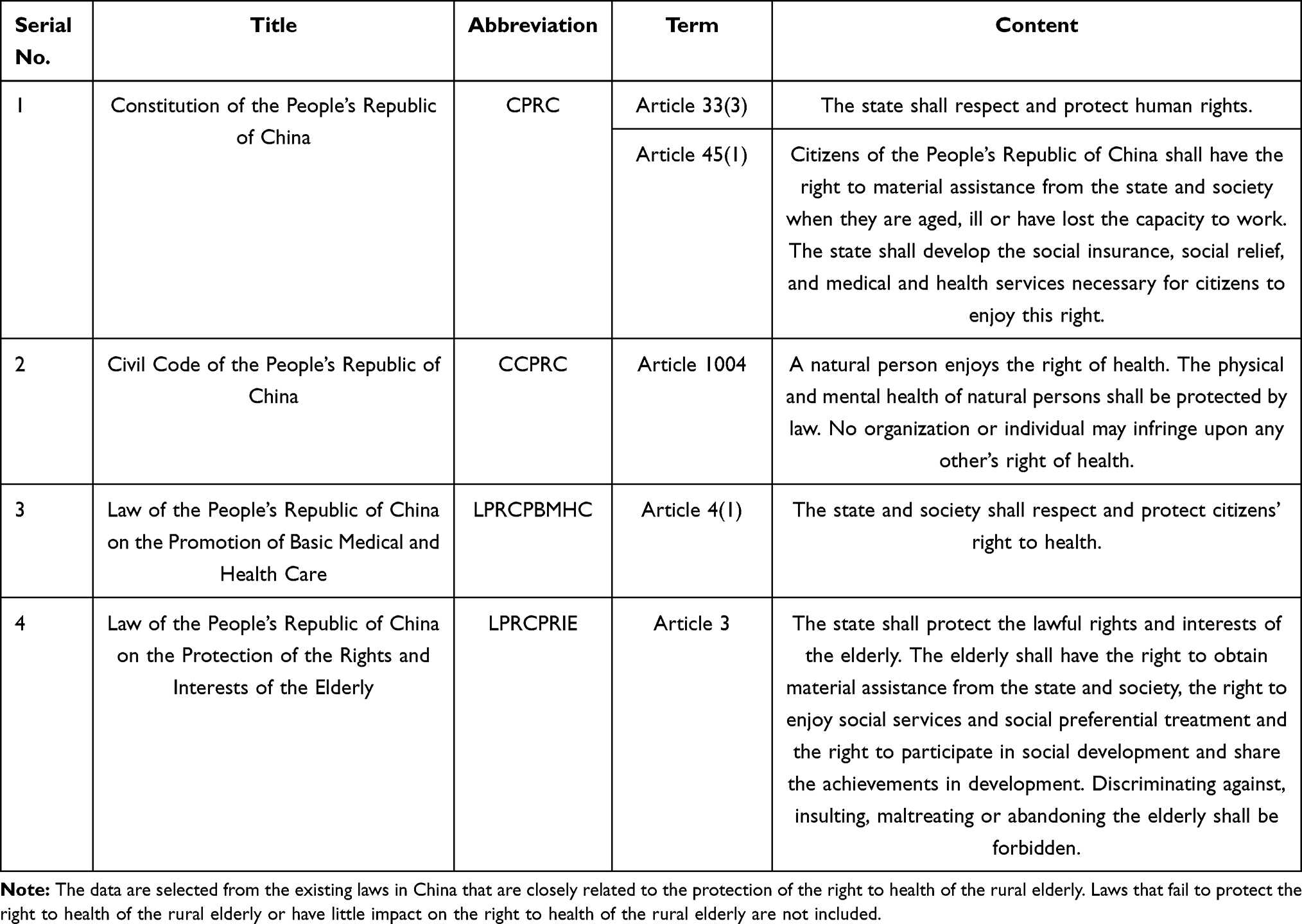 |
Table 2 China’s Legal Provisions to Protect the Right to Health of the Elderly in Rural Areas |
The Constitution of the People’s Republic of China
The Constitution of the People’s Republic of China (CPRC) is the basic law of China and the basis for all legal norms in China, which is applicable to all citizens of China. Article 33(3) of the CPRC provides that “The state shall respect and protect human rights.” Article 45(1) of the CPRC stipulates that “Citizens of the People’s Republic of China shall have the right to material assistance from the state and society when they are aged, ill or have lost the capacity to work. The state shall develop the social insurance, social relief, and medical and health services necessary for citizens to enjoy this right.” Although the CPRC does not directly specify the legal status of the right to health of rural elderly people, the above two articles provide for the state’s obligation to guarantee human rights and provide material assistance and are often seen as an indirect constitutional basis for guaranteeing the right to health of rural elderly people.
The Civil Code of the People’s Republic of China
The Civil Code of the People’s Republic of China (CCPRC), enacted in May 2020 and came into force on January 1, 2021, is structurally identical to the Japanese and German civil codes. It is not a new private law, nor is it a reinterpretation of an existing legal text, but rather an integration of existing rules in the Chinese civil sphere.51 From the legislative history of China’s civil sphere, Article 98 of the General Principles of the Civil Law (implemented in 1987 and repealed after the CCPRC came into force in 2021), Article 2 of the Tort Liability Law (implemented in 2010 and repealed after the CCPRC came into force in 2021), and Article 110 of the General Provisions of the Civil Law (implemented in 2017 and repealed after the CCPRC came into force in 2021), all successively specify “the right to health”. Article 1004 of the CCPRC also specifies that “A natural person enjoys the right of health. The physical and mental health of natural persons shall be protected by law. No organization or individual may infringe upon any other’s right of health.” This article clarifies that in the civil sphere, the elderly in rural areas have the right to health, both physical and psychological.
The Law of the People’s Republic of China on the Promotion of Basic Medical and Health Care
Promulgated on December 28, 2019, and effective on June 1, 2020, the Law of the People’s Republic of China on the Promotion of Basic Medical and Health Care (LPRCPBMHC) is a law enacted by China to develop medical and health care, guarantee citizens’ access to basic medical and health services, improve their health, and promote the construction of a healthy China. It is the first basic and comprehensive law in the field of health in China, and is known as the de facto constitution of China’s health system.52 Article 4(1) of the LPRCPBMHC states that “The state and society shall respect and protect citizens’ right to health.” This provision expresses the law’s quest to protect citizens’ right to health and reflects the shift in China’s medical and health care from a cure-centered to a health-centered philosophy. The law seeks to transform the right to health from a negative right to a positive right by requiring the state to promote health through social policies and to establish government agencies to provide medical and health services.53
The LPRCPBMHC has five articles 25, 28, 36, 74, 76 referring to the special characteristics of the elderly subjects, including developing health care and mental health care for the elderly, providing safe and convenient medical and health services for the elderly, carrying out nutrition improvement actions for the elderly, and formulating and implementing health work plans for the elderly. A total of three articles 34, 56, 72 mention the special characteristics of rural citizen subjects, including the establishment of a sound rural medical and health service network, the strengthening of rural medical and health teams, and the construction of healthy villages and towns.
The Law of the People’s Republic of China on the Protection of the Rights and Interests of the Elderly
The Law of the People’s Republic of China on the Protection of the Rights and Interests of the Elderly (LPRCPRIE), which was promulgated on August 29, 1996, came into force of the same year on October 1, and was amended four times in 2009, 2012, 2015, and 2018, is a basic law to protect the rights and interests of the elderly, and is of great significance to the participation of the elderly in social life and the construction of harmonious and stable social relations.54 Article 3(1) of the LPRCPRIE stipulates that “The state shall protect the lawful rights and interests of the elderly.” Obviously, the right to health belongs to the rights and interests of the elderly according to the law. This law is the main legal basis to protect the rights and interests of rural elderly people, and it fixes the rights of rural elderly people, such as the right to participate in social development and the right to medical care in the form of law. In general, it provides the basis for the legal guarantee of the right to health of the rural elderly.
Three articles 29, 33, 55 of the LPRCPRIE mention the special characteristics of rural elderly subjects, of which only Article 29, “The government shall subsidize the portion of individual contributions required for eligible rural elderly persons from low-income families to participate in the new type of rural cooperative medical care”, has a significant impact on the right to health of rural elderly persons.
Legislation at the Local Level
Article 80 of the Legislation Law of the People’s Republic of China (LLPRC) provides that “The people's congress and its standing committee of a province, autonomous region, or municipality directly under the Central Government may, according to the specific circumstances and actual needs of the administrative region, enact local regulations, provided that such regulations do not contravene the Constitution, laws, and administrative regulations”. Article 93 of the LLPRC provides that “The people's government of a province, an autonomous region, a municipality directly under the Central Government, a districted city, or an autonomous prefecture may develop rules in accordance with laws, administrative regulations, and the local regulations of the province, autonomous region, or municipality”.
Although local legislation has received less attention from scholars, it is critical to safeguarding the right to health of older people in rural China. Because of the complex relationship between the central and local levels in China, the implementation of national policies may vary from region to region.55 In fact, Shanghai produced China’s first regulations on the protection of the elderly in 1988, eight years before the LPRCPRIE.
As of March 2023, 155 (108 at the provincial and 47 at the municipal level) effective local regulations concerning the right to health of rural older adults can be found in 31 provinces in mainland China through the Chinalawinfo database. Local-level legislation refines national laws and provides more comprehensive and targeted protection for the right to health of rural older adults in each region in a variety of areas, including elderly services, lifelong education, medical care, and fitness. In Guangdong Province, for example, a number of local regulations, including the Regulations on the Protection of the Rights and Interests of the Elderly in Guangdong Province, the Regulations on Elderly Services in Guangdong Province, the Regulations on National Fitness in Guangdong Province, the Regulations on Volunteer Services in Guangdong Province and the Measures on Preferential Treatment for the Elderly in Guangdong Province, provide more local refinements of national laws in different aspects.
Legal Barriers to Exercising the Right to Health of the Elderly in Rural China
The Constitutional Status of the Right to Health of Rural Older Adults is Controversial
In China, the current text of the CPRC does not explicitly state that “the right to health” is a fundamental right of citizens. This is because, according to the existing text of the Constitution, in the section on fundamental rights in Chapter III, there is no direct health-related content, except for Article 36, which states that no one may use religion for activities that harm the physical health of citizens. Therefore, is there the right to health in the sense of modern human rights in Chinese constitutional texts? Does the right to health of rural elderly people have constitutional status? These questions remain controversial.56
Lack of Content of the Right to Health of the Rural Elderly at the National Legal Level
For the protection of the right to health of the elderly in rural areas, two main legal frameworks currently exist in China: one is the legal framework of citizens’ right to health, with the LPRCPBMHC as the core; the other is the legal framework for the protection of the rights of special groups, with the LPRCPRIE as the core. Other national laws need to be based on these two laws when formulating provisions involving the right to health of the elderly. However, there is still a lack of content on the right to health of the rural elderly at the national legal level. First, the LPRCPBMHC and the LPRCPRIE themselves do not have much content that addresses the right to health of the elderly. Second, both the LPRCPBMHC and the LPRCPRIE protect the elderly as a whole in almost all cases, lacking special protection for the rural elderly who are more vulnerable in terms of economic and social status.
The Content of Legislative Texts at the Local Level Has the Problem of Duplication of Superior Laws
Repetition of the content of local legislation is a hot issue in Chinese legislation, and it is inevitable in local legislation concerning the right to health of the elderly in rural areas. When local legislatures enact local regulations, they often adopt three ways to duplicate legislation, including directly copying, simply piecing together or applying the basic form to repeat the content of the higher law without substantive changes. Taking the Regulations on the Protection of the Rights and Interests of the Elderly in Shandong Province (revised in 2014) as an example, the statute has 61 articles, and the duplicated content of the LPRCPRIE reaches about 60%, among which the chapters of “participation in social development” and “legal responsibility” are exactly the same as the higher law. In fact, this kind of local-level legislation, which only makes appropriate refinements in a few articles and has a very high repetition rate, cannot give full play to the function of refining the higher law, and the simple patchwork of repetitive legislation will seriously affect the authority of the legislature and social credibility, and it is difficult to achieve the purpose of local-level legislation to provide more comprehensive and local-specific protection for the right to health of rural elderly people.
Feasible Recommendations
The law as a tool has an important role to play in advancing the right to health57 and contributes to the success of the goal of a healthier population in the future.58 Enacting a law does not mean the end, and the government should continuously monitor and evaluate the law’s interventions and their impact, and update the law accordingly.57,59 China should further improve its domestic laws to provide comprehensive protection for the right to health of rural elderly people.
First, the right to health is a human right,60 and guaranteeing citizens’ right to health should be explicitly written into the CPRC. Currently, more and more countries have included the right to health in their constitutions and have proven that this approach is beneficial to people’s health.61 The Constitution is at the tip of China’s legal pyramid and is the most important law in China.62 The inclusion of the right to health in the Constitution not only complements Article 33(3) of the Constitution, but also provides guidance for the formulation, amendment, repeal, and interpretation of national laws and local regulations, and is conducive to more comprehensive protection of the right to health of all Chinese citizens, including the elderly in rural areas.
Second, add provisions for special protection of the right to health of the rural elderly to the content of national laws, especially the LPRCPBMHC and the LPRCPRIE.
Third, when formulating legislation at the local level, it should extend, supplement and refine the higher law, taking into account the actual needs of the right to health of the rural elderly in the local area, and avoid completely repeating the content of the higher law.
Conclusion
Older people have accumulated valuable wisdom and experience, and have contributed significantly to social development. As their physiological functions gradually decline due to age, their right to health protection requirements should be fully met. The increasing urbanization in China has widened the gap between urban and rural areas, and the number of elderly people in rural areas is high, and there is a significant gap in health protection compared to urban elderly people. Therefore, the state needs to continuously strengthen the protection of the right to health of the elderly in rural areas in terms of legislation, and to guard the rule of law for the protection of the right to health. In this paper, the study of the right to health of the rural elderly is only from the legal perspective, which is inevitably limited. The protection of the right to health of the rural elderly is undoubtedly a complex issue that needs to be explored and studied in greater depth by experts and scholars from various fields.
Abbreviations
NRPP, New Rural Pension Program; CPRC, Constitution of the People’s Republic of China; CCPRC, Civil Code of the People’s Republic of China; LPRCPBMHC, Law of the People’s Republic of China on the Promotion of Basic Medical and Health Care; LPRCPRIE, Law of the People’s Republic of China on the Protection of the Rights and Interests of the Elderly; LLPRC, Legislation Law of the People’s Republic of China.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Arti, Mittal JK. Health of the elderly in India: a socio-legal study. Indian J Public Health Res Dev. 2020;11(1):7–11. doi:10.37506/v11/i1/2020/ijphrd/193774
2. Kowal P, Dowd JE. Definition of an Older Person. Proposed Working Definition of an Older Person in Africa for the MDS Project. Geneva: World Health Organization; 2001.
3. Chen XX, Giles J, Yao Y, et al. The path to healthy ageing in China: a Peking University-Lancet Commission. Lancet Comm. 2022;400(10367):1967–2006. doi:10.1016/S0140-6736(22)01546-X
4. Huang G, Guo F, Chen G. Multidimensional healthy life expectancy of the older population in China. Popul Stud. 2021;75(3):421–442. doi:10.1080/00324728.2021.1914854
5. First world assembly on ageing, 26 July-6 August 1982, Vienna. Available from: https://www.un.org/en/conferences/ageing/vienna1982.
6. National Bureau of Statistics of China. Statistical bulletin of the national economic and social development of the People’s Republic of China for 2021. Available from: http://www.gov.cn/xinwen/2022-02/28/content_5676015.htm.
7. National Health Commission of the People’s Republic of China. Around 2035, the population of elderly people aged 60 and above will break 400 million, accounting for more than 30% of the population. Available from: http://news.cctv.com/2022/09/20/ARTInjejQDvmMaZi5jzTPHYT220920.shtml.
8. The level of population aging in rural is higher than those in urban areas. Available from: http://bgimg.ce.cn/xwzx/gnsz/gdxw/202201/19/t20220119_37267841.shtml.
9. The seventh national census results announced that these data are about the “old” topic. Available from: https://www.mca.gov.cn/n152/n166/c45021/content.html.
10. United Nations. Madrid political declaration and international plan of action on ageing, 2002. https://www.un.org/esa/socdev/documents/ageing/MIPAA/political-declaration-en.pdf
11. Summary of the high-level meeting on the regional assessment of the implementation of the ESCAP madrid international plan of action on ageing attended by deputy director Cao Bingliang. China Ageing Work Yearbook; 2007:438. Chinese.
12. Xing YA, Pei RJ, Qu J, et al. Urban-rural differences in factors associated with willingness to receive eldercare among the elderly: a cross-sectional survey in China. BMJ Open. 2018;8(5):e020225. doi:10.1136/bmjopen-2017-020225
13. Chen Q, Shen BS. Mental loneliness of rural empty-nesters and the social assistance. J Yanbian Univ. 2020;53(6):80–87. Chinese.
14. Zhang C, Hu H. Urban-rural differences: the impact of social support on the use of multiple healthcare services for older people. Front Public Health. 2022;10:851616. doi:10.3389/fpubh.2022.851616
15. Li X, Xiao ZP, Xiao SF. Suicide among the elderly in mainland China. Psychogeriatrics. 2009;9(2):62–66. doi:10.1111/j.1479-8301.2009.00269.x
16. Hu CY, Zhao DD, Gong FF, et al. Risk factors for suicidal ideation among the older people living alone in rural region of China A path analysis. Medicine. 2020;99(29):21330. doi:10.1097/MD.0000000000021330
17. Ettner SL. New evidence on the relationship between income and health. J Health Econ. 1996;15(1):67–85. doi:10.1016/0167-6296(95)00032-1
18. Oldwage-Theron W, Francis Z, Christine SV, Venter C. Health status of an elderly population in Sharpeville, South Africa. Health SA Gesondheid. 2008;13(3):3–17. doi:10.4102/hsag.v13i3.282
19. Darkwa OK, Mazibuko FNM. Population aging and its impact on elderly welfare in Africa. Int J Aging Hum Dev. 2002;54(2):107–123. doi:10.2190/XTQG-6DXD-9XWE-9X85
20. Rural retirement survey: nearly 1/4 of the population over 60 years old rely on four main sources of funding for their old age. Available from: https://baijiahao.baidu.com/s?id=1704784678654132480&wfr=spider&for=pc.
21. Zhou M, Sun XT, Huang L. Does social pension expansion relieve depression and decrease medical costs? Evidence from the rural elderly in China. Int J Public Health. 2022;67:1604296. doi:10.3389/ijph.2022.1604296
22. The new rural insurance: let hundreds of millions of farmers have a sense of security in old age. Available from: https://gmrb.cloud.gmw.cn/gmrb/html/2021-04/15/content_77790.htm.
23. Lei X, Zhang C, Zhao Y. Incentive problems in China’s new rural pension program. Res Labor Econ. 2013;37:181–201.
24. Chen X, Hu LP, Sindelar JL. Leaving money on the table? Suboptimal enrollment in the new social pension program in China. J Econ Ageing. 2020;15:100233. doi:10.1016/j.jeoa.2019.100233
25. Farmers at age 60 only receive pensions which are slightly above 100 RMB: how to build a fair pension system for urban and rural residents. Available from: http://www.ceweekly.cn/2022/1130/400535.shtml.
26. In the past, rural people relied on their children for their retirement, but now, do the traditional methods still work? How to solve. Available from: https://baijiahao.baidu.com/s?id=1743368679056855882&wfr=spider&for=pc.
27. Guo L. Optimal Allocation of Social Elderly Service Resources in China. Beijing: Social Sciences Academic Press (CHINA); 2020.
28. Is it the son’s responsibility or the daughter’s responsibility for caring the retired elderly. Available from: http://www.shehui.pku.edu.cn/second/index.aspx?nodeid=2030&contentid=10491.
29. Nie JL. Can raising children still protect against old age risk? Demographic and economic characteristics of children, relation between generations and the acquisition of resources for the aged in rural areas. J Huazhong Univ Sci Technol. 2018;32(6):33–41. Chinese.
30. Proposal on the implementation of support policies for families without a single person. Available from: https://www.mj.org.cn/mjzt/content/2016-05/12/content_224778.htm.
31. Focus on population security and unbalanced and insufficient development. Available from: http://www.ce.cn/xwzx/gnsz/gdxw/201807/09/t20180709_29667979.shtml.
32. Wang XB, Weaver N, You J. The social security function of agriculture in China. J Int Dev. 2013;25(1):1–10. doi:10.1002/jid.2827
33. What is rural land transfer? How to transfer rural contracted land legally? Available from: http://www.qdnsb.gov.cn/xzjdbsc/mhz/zfxxgk/fdzdgknr/nctdcb/202203/t20220301_72806261.html.
34. Wang W, Luo X, Zhang CM, et al. Can land transfer alleviate the poverty of the elderly? Evidence from rural China. Int J Environ Res Public Health. 2021;18(21):11288. doi:10.3390/ijerph182111288
35. Hu Y, Wei HK. Income structure and income inequality of the elderly in rural China: the present situation of the elderly in rural China. J Nanjing Agric Univ. 2022;22(4):45–57. Chinese.
36. Briefing on the data of the sample survey on the living conditions of the elderly in urban and rural China (2015). Available from: http://www.crca.cn/index.php/19-life/27-2015.html.
37. Jun G, Raven JL, Tang SL. Hospitalisation among the elderly in urban China. Health Policy (New York). 2007;84(2–3):210–219. doi:10.1016/j.healthpol.2007.03.007
38. Wu H, Rong XB, Zhao MF. Do high-speed rails improve the allocation level of medical resources? Front Sustain Cities. 2022;4:802104. doi:10.3389/frsc.2022.802104
39. National Health Commission of the People’s Republic of China. 2022 China Health Care Statistics Yearbook. Beijing: Peking Union Medical College Press; 2022.
40. Zhao PJ, Yu Z. Rural poverty and mobility in China: a national-level survey. J Transp Geogr. 2021;93:103083. doi:10.1016/j.jtrangeo.2021.103083
41. Yi FJ, Liu C, Xu ZG. Identifying the effects of migration on parental health: evidence from left-behind elders in China. China Econ Rev. 2019;54:218–236. doi:10.1016/j.chieco.2018.11.005
42. Shen GC, Shen SJ. An analysis of the issue of rural left-behind elderly from the perspective of sociology. High Educ Soc Sci. 2014;7(3):132–136.
43. Country cares about those 16 million old people who left behind in rural areas. Available from: http://journal.crnews.net/nmwz/2019n/2019nd3q/927256_20190326031042.html.
44. Huang BH, Lian YJ, Li WS. How far is Chinese left-behind parents’ health left behind? China Econ Rev. 2016;37:15–26. doi:10.1016/j.chieco.2015.07.002
45. Chen FG, Henry L, Gerry B, et al. Household structure, leaf-Behind elderly, and rural migration in China. J Agric Appl Econ. 2016;48(3):279–297. doi:10.1017/aae.2016.16
46. Lin K, Yin PJ, Loubere N. Social support and the ‘left behind’ elderly in rural China: a case study from Jiangxi Province. J Community Health. 2014;39(4):674–681. doi:10.1007/s10900-014-9864-4
47. He GP, Xie JF, Zhou JD, et al. Depression in left-behind elderly in rural China: prevalence and associated factors. Geriatr Gerontol Int. 2016;16(5):638–643. doi:10.1111/ggi.12518
48. Zhou L, Wang GJ, Jia CX, et al. Being left-behind, mental disorder, and elderly suicide in rural China: a case–control psychological autopsy study. Psychol Med. 2018;49(3):458–464. doi:10.1017/S003329171800106X
49. Ouma S, Mori HO, Amutete CAM. Engendering rule of law in health care delivery in Kenya. Wis Int Law J. 2017;35(1):81–137.
50. Meier BM, Evans DP, Kavanagh MM, et al. Human rights in public health: deepening engagement at a critical time. Health Hum Rights. 2018;20(2):85–91.
51. You W. Parent-child relationship in the civil code of China. Laws. 2023;12:1. doi:10.3390/laws12010001
52. Ip EC. The political determinants of China’s new health constitution. Med Law Rev. 2021;29(1):3–23. doi:10.1093/medlaw/fwaa030
53. Zhao ZJ. Recent legislative progress on healthcare law in China: establishing “Right to Health” as a basic right (2018). Available from: https://ohrh.law.ox.ac.uk/recent-legislative-progress-on-healthcare-law-in-china-establishing-right-to-health-as-a-basic-right/.
54. Du P, Xie LL. The use of law to protect and promote age-friendly environment. J Soc Work Pract. 2015;29(1):13–21. doi:10.1080/02650533.2014.993945
55. Wang H, Jiang CX. Local nuances of authoritarian environmentalism: a legislative study on household solid waste sorting in China. Sustainability. 2020;12(6):2522. doi:10.3390/su12062522
56. Fang Y, Wang HT, Ouyang Z. An overview report on the situation of elderly people in urban and rural China: 2000–2015. China Popul Dev Stud. 2019;2:323–345. doi:10.1007/s42379-018-0016-x
57. Gostin LO, Magnusson RS, Krech R, et al. Advancing the right to health-the vital role of law. Am J Public Health. 2017;107(11):1755–1756. doi:10.2105/AJPH.2017.304077
58. The Lancet. Law: an underused tool to improve health and wellbeing for all. Lancet. 2017;389(10067):331. doi:10.1016/S0140-6736(17)30194-0
59. Gostin LO, Monahan JT, Kaldor J, et al. The legal determinants of health: harnessing the power of law for global health and sustainable development. Lancet. 2019;393(10183):1857–1910. doi:10.1016/S0140-6736(19)30233-8
60. World Health Organization. Health and human rights. Available from: https://www.who.int/zh/news-room/fact-sheets/detail/human-rights-and-health.
61. Kavanagh MM. The right to health: institutional effects of constitutional provisions on health outcomes. Stud Comp Int Dev. 2016;51(3):328–364. doi:10.1007/s12116-015-9189-z
62. Qi F, Hu LJ, Wu YQ. Rhetoric and reality: litigation rights of Chinese disabled people. Disabil Soc. 2019;35(8):1343–1348. doi:10.1080/09687599.2019.1708560
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.