Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Rural–Urban Differences in Mild Cognitive Impairment Among Patients with Chronic Obstructive Pulmonary Disease in ChengDu, China
Authors Chen X, Dong X, Liu J, Liu X, Deng M, Yang Y
Received 4 September 2023
Accepted for publication 30 October 2023
Published 9 November 2023 Volume 2023:18 Pages 2497—2508
DOI https://doi.org/10.2147/COPD.S434743
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Xiaomei Chen,1,2 Xunhu Dong,3 Jia Liu,1 Xiao Liu,1 Menghui Deng,1 Yanni Yang1
1School of Nursing, Army Medical University, Chongqing, People’s Republic of China; 2Nursing Department, Qionglai Medical Center Hospital, Qionglai, Chengdu, People’s Republic of China; 3School of Military Preventive Medicine, Army Medical University, Chongqing, People’s Republic of China
Correspondence: Yanni Yang, School of Nursing, Army Medical University, Chongqing, People’s Republic of China, Email [email protected]
Purpose: The rural–urban gap in sociodemographic, lifestyle, and disease-related characteristics among COPD patients is prevalent. These differences may influence the prevalence of mild cognitive impairment (MCI). This study aimed to compare the prevalence and determinants of MCI between rural and urban areas among COPD patients.
Patients and Methods: The cross-sectional study sample comprised 372 COPD patients from China. We evaluated the cognitive function and lung function, collected sociodemographic, lifestyle, and disease-related information, to compare the prevalence of MCI in rural and urban areas. Using multivariate regression analysis to examine the effects of variables to MCI.
Results: The prevalence of MCI in rural areas was higher than that in urban areas (65.4% vs 47.9%, P=0.001). The prevalence in farm laborers was almost twice as high as that of non-farm laborers in urban areas (82.6% vs 43.1%), but no significant difference in rural areas (P=0.066). However, the data were lower in subjects who insisted on long-term home oxygen therapy (39.7%, CI:27.8– 51.6, P< 0.001), and who with higher monthly household income (49.6%, CI:40.2– 58.9) in rural areas, but no significant difference in urban areas (P=0.985 and 0.502). Multivariate logistic regression analysis indicated that participants aged 71 years and above, former smokers were at a high risk of MCI in both urban and rural areas. However, participants who slept for 6– 8 hours a day, shopping frequently, or exercised for more than 2 hours a day had a lower risk of MCI in urban areas. But rural participants who insisted on long-term home oxygen therapy had a lower probability of developing MCI.
Conclusion: This study revealed that there were significant differences in MCI among COPD patients in rural and urban areas, especially in exercise, sleeping, shopping, and long-term home oxygen therapy. Medical staff should give health guidance according to the actual situation of patients with COPD.
Keywords: chronic obstructive pulmonary disease, mild cognitive impairment, urban, rural
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic respiratory disease characterized by limited airflow and incomplete reversibility, and it is associated with high morbidity and mortality.1 A cross-sectional survey of 24% of China’s population showed that the overall prevalence of COPD in 2018 was 13.6% among 66,752 adults aged >40 years, which was 5.4% higher than that in 2004.2 COPD will seriously affect the quality of life and mental status of patients.3
Cognition is the set of processes that allow the brain to receive and process external information. Cognitive impairment (CI) is a frequent extrapulmonary manifestations in COPD. A previous study found mostly poor performance on cognitive tests of attention, memory, and executive functions in COPD patients.4 Mild cognitive impairment (MCI) refers to cognitive decline without major functional impacts on activities of daily living,5 MCI is one of the complications of COPD and refers to the impairment of one or more cognitive fields, which affects the patients’ social function and quality of life.6,7 A cross-sectional study reported a higher prevalence of MCI in individuals with COPD compared with those without COPD,5 and the prevalence of MCI in COPD patients can be as high as 58%.8 COPD with MCI may reduce the efficiency of treatment and self-management, which not only affects physical functioning in COPD patients but also increases mortality and disability.9 Also, approximately 50% of patients with MCI develop dementia within 5 years, which poses a heavy burden on families and society.6 Therefore, the early identification of modifiable risk factors for MCI of COPD is important for preventing or delaying the onset of dementia.10
Environmental factors may be involved in cognitive impairment or decline. The incidences of MCI differ significantly between urban and rural, primarily due to differences in living environment, quality of life, family income, and level of education.11 Some studies reported rural–urban differences in prevalence of MCI in elderly,11,12 However, this difference in COPD patients has not been reported. Although a large national survey reported the prevalence of cognitive impairment in COPD patients between urban and rural areas, but this study did not describe the associated risk factors. Furthermore, this study included COPD patients in rural and urban areas across different provinces and cities.13 However, there are obvious differences in customs, eating habits, culture, and health policies between different provinces and cities in China.14 Therefore, the results of the study may be more suitable for explaining regional differences than rural–urban differences among COPD patients.11 As such, it is necessary to further explore relevant differences for MCI in COPD patients between urban and rural areas.
To better analyse these differences in MCI, we selected COPD patients living in rural and urban areas under the jurisdiction of the same city. We took into account the baseline information, life style, and disease-related factors that can potentially affect cognition, and excluded potential confounding factors such as regional customs. Thus, our results provide a reference for local medical and health institutions that can help formulate targeted prevention and intervention programs.
Materials and Methods
Area Surveyed
A cross-sectional study of MCI in COPD was undertaken from March 2022 to December 2022 in Qionglai City, Chengdu, Sichuan province, China. This city has one urban area and 24 rural townships with a population of 0.6 million people. The urban population is 53.53%, and the rural population is 46.47%. This survey was conducted from Qionglai City and 11 neighbouring rural townships.
Sample Size
We used the following formula to calculate the sample size from a known population of COPD patients (N=Zα/22 p(1-p)/d2), and Za/2=level of confidence at 95% (1.96), p=previous prevalence of cognitive impairment in COPD patients (0.58), allowable error(d)=0.1p.15 Based on the calculation, and Considering a 20% sample loss, the sample size of this study should have been 334 COPD patients. A total of 372 COPD patients were enrolled in our study.
Inclusion and Exclusion Criteria
Participants were selected from Qionglai Medical Center Hospital and 11 nearby township hospitals through gratuitous treatment. Suitable COPD patients were selected according to the order of admission. All adult patients of age 40 years and above with COPD, and giving written consent, were enrolled in the study. Those with severe mental illness (such as dementia or Alzheimer’s disease) and active pulmonary tuberculosis were excluded. This study used the STROBE cross-sectional reporting guidelines.16
Data Collection
This study was divided into two stages to recruit participants: In the first stage, using convenient sampling method to recruit COPD patients in a comprehensive hospital in Qionglai city; In the second stage, 11 townships were randomly selected, and then selected participants from the hospitals in the selected 11 townships. The recruitment procedures were as follows: the investigators introduced the purpose and methods of this study to patients via telephone interview, gratuitous treatment or face-to-face communication. Then, if patients meet the inclusion and exclusion criteria of this study and were willing to join this study, they must sign informed consent. This survey was conducted by the authors and other qualified investigators who received unified training. Before the investigation, the researchers and trainers explained the purpose and significance of the study to the participants. The investigation was conducted only after obtaining the consent of each participant. All questionnaires were filled in under the guidance of the researchers. The questionnaires were distributed, filled out, and collected on the spot. Simultaneously, the researchers verified the completeness and accuracy of each questionnaire to avoid wrong or missing data. A total of 372 COPD patients were enrolled in this study.
Measurements
Outcome Variable
MCI Assessment
The MCI assessment was conducted by standardised training and certified researchers after excluding patients with dementia. The diagnosis of dementia was carried out by doctors with standardized training and qualifications in the neurology department based on the Chinese Guidelines for Diagnosis and Treatment of Dementia and Cognitive Impairment (2018).17 The Beijing version of Montreal Cognitive Assessment (MoCA) was used to assess MCI after excluding participants with dementia. MoCA includes eight cognitive domains: orientation, language, working memory, concentration, short-term memory, attention, executive function, and visuospatial ability, and is sensitive to screen out MCI. Considering the impact of education level on cognitive function, the MoCA score can be adjusted for years of education. One point is added to the original MoCA score if a person’s education time less than 12 years. The maximum score of MoCA is 30 points, and a higher score represents a better cognition function and a score <26 indicates MCI.18
Covariates
The analysis included and adjusted other sociodemographic, lifestyle, and disease-related characteristics. The sociodemographic characteristics included sex, age, education level, occupation, marital status, living arrangement, monthly household income, body mass index (BMI), smoking, drinking, decision makers in family, and family history of dementia. Factors related to lifestyle included daily hours of sleep, frequent shopping (more than 3 times a week), daily hours of entertainment and daily hours of exercise. Disease-related characteristics included comorbidity (referring to combined with other chronic diseases such as hypertension and diabetes), long-term home oxygen therapy, and lung function. The lung function of participants were measured according to Global initiative for chronic obstructive lung disease (2020 REPORT),19 we recorded forced vital capacity (FVC), forced expiratory volume in the first second (FEV1), forced vital capacity rate of one second (FEV1/FVC), and percentage of predicted FEV1 (FEV1% pred). Lung function was divided into four degrees according to FEV1%pred: GOLD1:FEV1%pred≥80%; GOLD2: 50%≤FEV1%pred<80%; GOLD 3:30%≤FEV1%pred<50%; GOLD 4: FEV1%pred<30%, and GOLD 1 to GOLD 4 represented mild to extremely severe lung function injury.
Statistical Analyses
We used SPSS Statistics 23.0 (IBM Corp, Armonk, NY, USA) for data analysis. Continuous variables were summarised as mean with SD, while categorical variables were presented as frequencies and percentages. To compare sociodemographic, lifestyle, and disease-related characteristics between rural and urban areas, normally distributed data were tested with a t-test; non-normally distributed data were tested with a Mann–Whitney U-test, and categorical data were tested with a chi-squared test. The Chi-square test was used to compare MCI between urban and rural variables. Finally, binary logistic regression was used to analyse the risk factors of MCI in rural and urban participants. The results are reported as odds ratios (ORs) with 95% confidence intervals (CIs). A value of P < 0.05 was considered statistically significant. We used the Variance Inflation Factor (VIF), all less than 5, to ensure no multicollinearity between variables.
Results
Background Characteristics of the Study Population
In our study, a total of 484 patients agreed to participate in the study, including 249 and 235 in rural and urban areas, respectively. Among them, 401 completed the final effective survey (201 and 200 in rural and urban areas respectively), with an overall response rate of 82.9% (80.7% and 85.1%) for urban and rural areas respectively). A total of 29 patients (19 in rural and 10 in urban areas) were screened as dementia and excluded. Eventually, 372 patients (182 in rural and 190 in urban areas) were included (Figure 1).
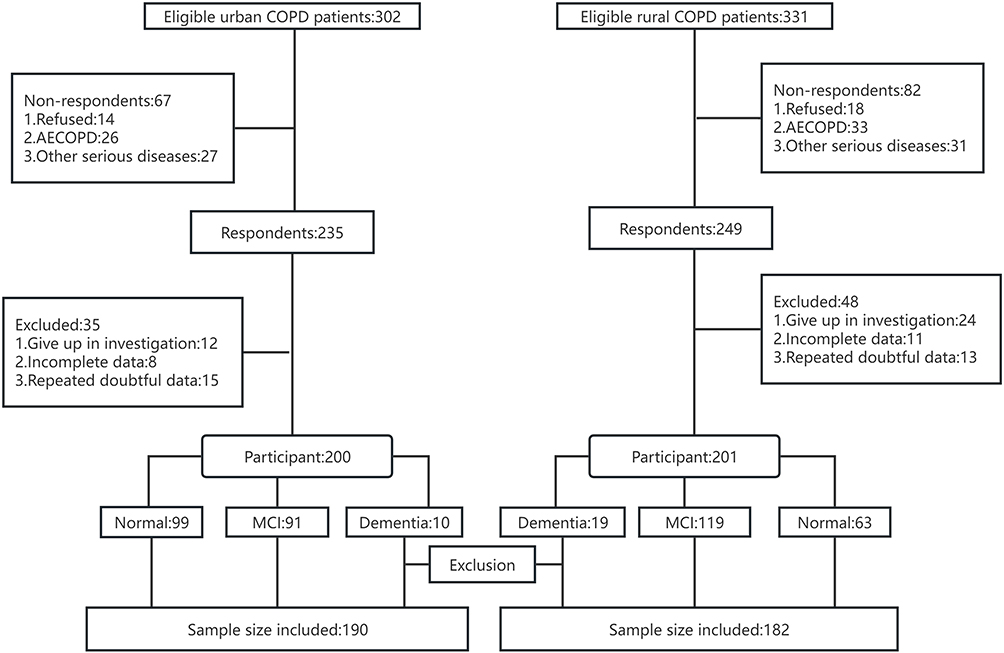 |
Figure 1 Flowchart of subject recruitment for the study participants. |
Table 1 provides the sample distribution of the participants. Around 63.7% (CI:56.8–70.6) of the participants were male in urban areas and 67.6% (CI:60.7–74.4) of respondents in rural areas. Nearly 69.9% (CI: 65.2–74.6) of participants at an education level of junior middle school or below. This data was higher in rural areas at 95.6% (CI:92.6–98.6) compared to urban areas at 45.3% (CI:38.1–52.4) (P<0.001). 29.7% (CI:23.0–36.4) of the participants spent more than 4 hours in entertainment every day in rural areas, whereas this figure was 56.3% (CI:49.2–63.4) in urban areas (P<0.001). It was 27% higher among people whose monthly household income was less than 5000 RMB in rural (37.9%, CI:30.8–45.0) than in urban settings (10.5%, CI:6.1–14.9) (P<0.001), and the participants who insisted on long-term home oxygen therapy in urban areas were 14% higher than that in rural areas [51.6% (CI:44.4–58.7) vs 37.4% (30.3–44.5), P=0.007].
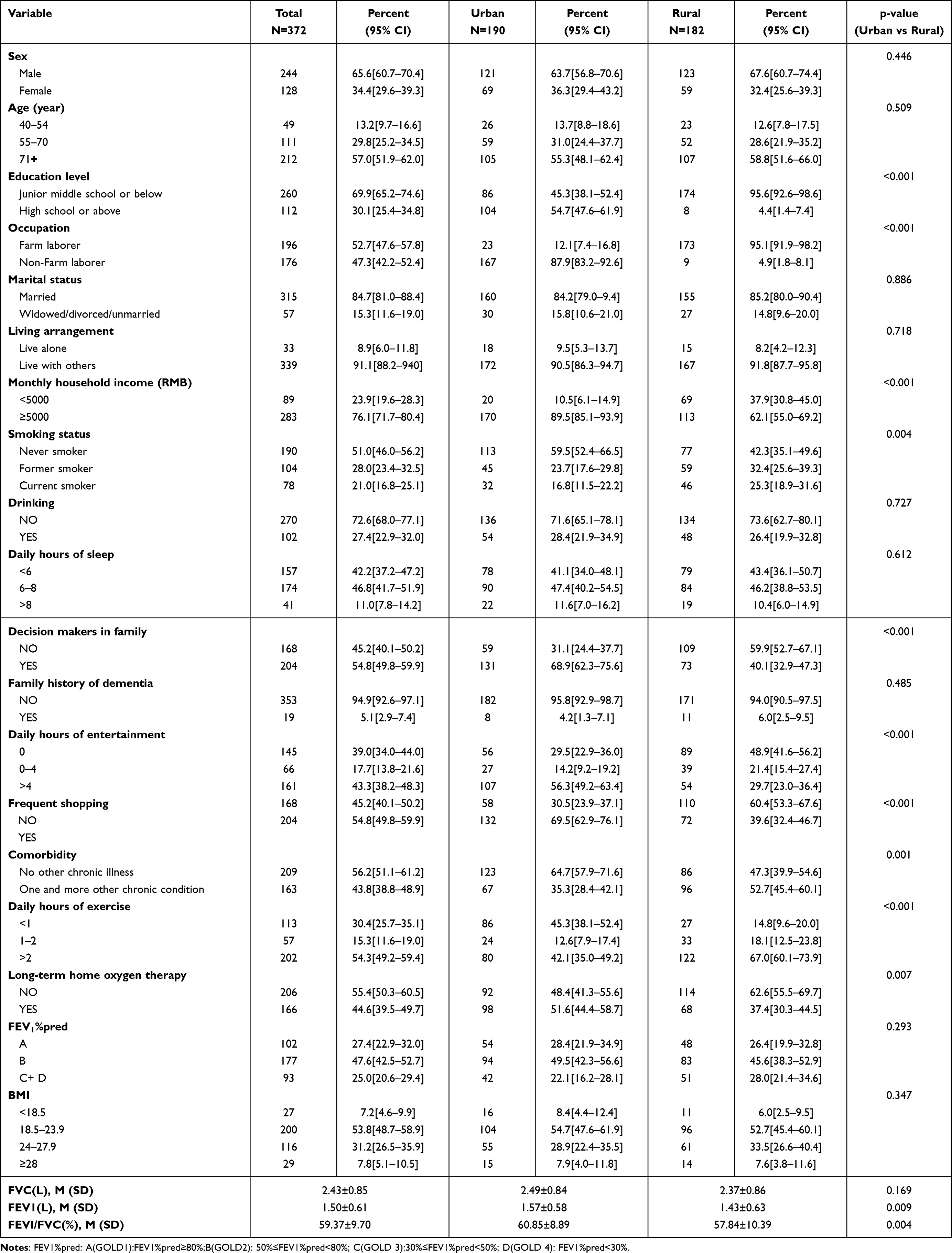 |
Table 1 Characteristics of Participants in Urban and Rural Areas |
Rural–Urban Differences in Prevalence of MCI Among Individuals with COPD
As is shown in Table 2, the prevalence of MCI in rural areas was significantly higher than that in urban areas (65.4% vs 47.9%, P=0.001), and the prevalence increased with age. The prevalence was also observed to be substantially higher among individuals who were at an education level of junior middle school and below both in rural and urban areas (67.8% and 70.9%, P<0.001). Similarly, the prevalence of MCI in participants who slept less than 6 hours a day, not shopping frequently, had one and more other chronic conditions, with serious lung function injury (GOLD 3 + GOLD 4) were higher, irrespective of place of residence (all P<0.001). However, the prevalence of MCI between urban and rural participants was significantly different in certain variables. For example, the prevalence of farm laborers was almost twice as high as that of non-farm laborers in urban areas (82.6% vs 43.1%, P<0.001), but there was no significant difference in rural areas (P=0.066). However, the prevalence of MCI was lower in subjects who insisted on long-term home oxygen therapy (39.7%, CI:27.8–51.6, P<0.001), and who with higher monthly household income (49.6%, CI:40.2–58.9, P<0.001) in rural areas, but no significant difference in urban areas (P=0.985 and 0.502). Furthermore, among the participants who exercised for more than 2 hours a day, the prevalence rate of MCI in urban participants was only 23.8% (CI:14.2–33.3), while that in rural participants was as high as 54.9% (CI:46.0–63.9).
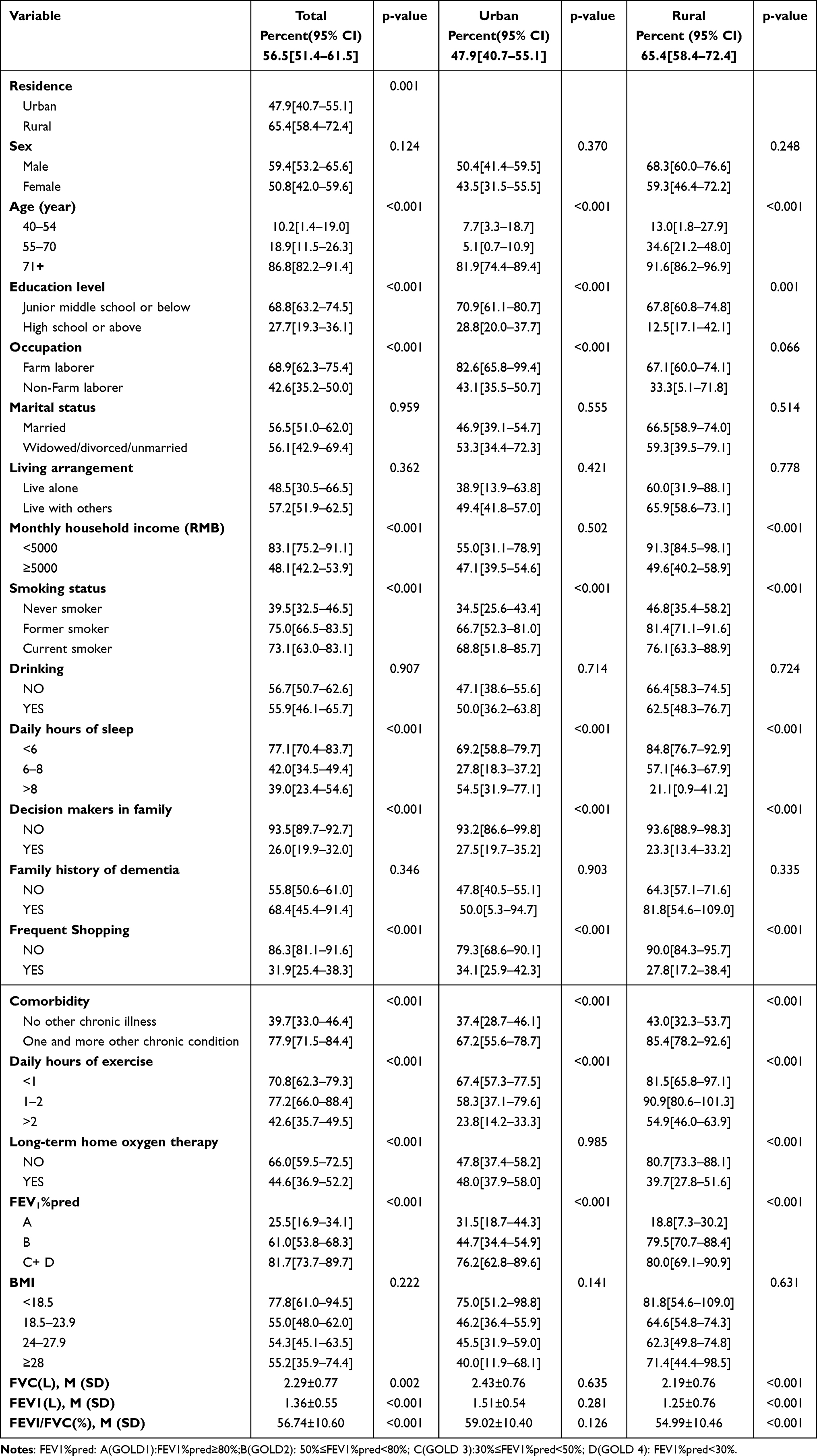 |
Table 2 Prevalence of MCI Among COPD Patients by Variables in Urban and Rural Areas |
Facilitators and Barriers to MCI Among COPD Patients in Rural and Urban Areas
Significant variables from univariate analyses of the presence or absence of MCI in the rural and urban areas were included in a binary logistic regression model. The adjusted estimation of MCI with different socioeconomic, lifestyle, and disease-related characteristics revealed that participants aged 71 years and above, or former smokers were at a high risk of MCI both in urban and rural areas (AOR=94.477, 95% CI:7.587–1176.422 and AOR=22.020, 95% CI:2.112 −229.565; AOR=11.583; 95% CI:1.769–75.866 and AOR=5.216; 95% CI:1.323–20.563). Participants who slept for 6–8 hours a day had a lower risk of MCI in urban (AOR=0.090, 95%:0.017–0.471). Participants who shopping frequently (AOR=0.107; 95% CI:0.020–0.565) exercise for more than 2 hours a day (AOR=0.037; 95% CI:0.007–0.191) were less likely to develop MCI, especially in urban areas. Rural participants who insisted on long-term home oxygen therapy (AOR=0.133; 95% CI:0.041–0.436) had a lower probability of developing MCI (Table 3).
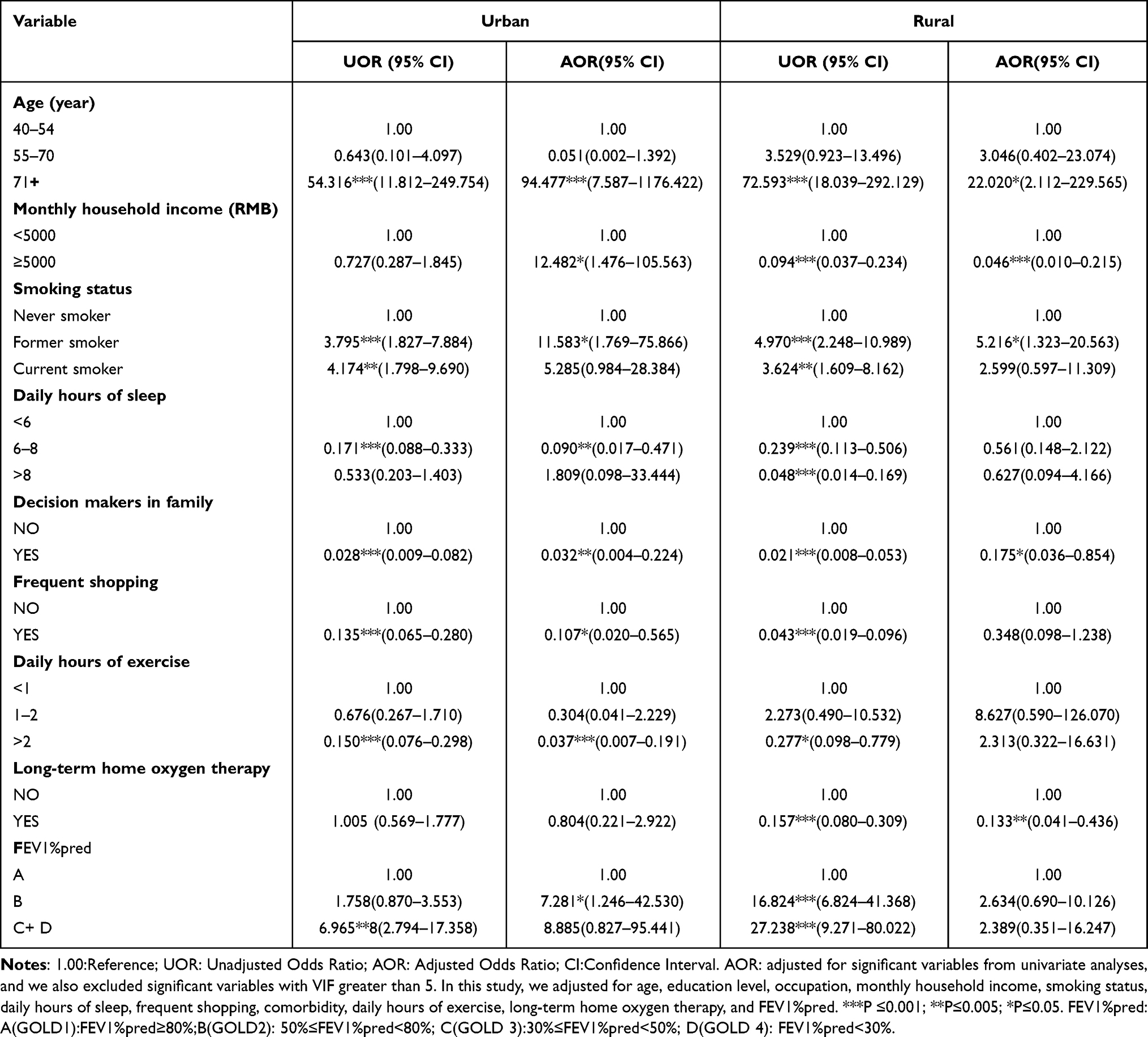 |
Table 3 The Variables Independently Associated with MCI Both in Urban and Rural Areas |
Discussion
To our knowledge, this is the first study to examine the difference in prevalence and influencing factors of MCI among COPD patients in rural and urban areas. According to the results of the study, there were some differences in MCI between rural and urban areas. We provide data that can act as a reference for local policymakers and medical staff.
In this study, 56.5% of participants were screened positive for MCI. The prevalence rate was similar to previous studies (63% and 58%),20,21 The high prevalence rate of MCI in COPD patients may be related to neuronal injury caused by long-term hypoxemia, systemic inflammation, vascular-mediated brain injury, changes in cerebral perfusion caused by chronic hypoxia, or the reduction of grey matter volume.22 These changes cause cognitive impairment in COPD patients, leading to symptoms such as slow information processing speeds, memory delays, and attention deficit.23
In this study, the prevalence of MCI in rural (65.4%) was significantly higher than that in urban (47.9%). Few previous studies reported the difference in the prevalence of MCI among COPD patients between urban and rural areas, but a large survey reported the difference in Chinese elderly, and the prevalence of MCI in rural areas was higher than that in urban areas (25.1% vs 17.9%).12 This regional disparity reported here may be related to difference in the quality of life and approaches to manage COPD. Compared to urban areas, a systematic community culture has not yet been formed in most rural areas, which may lead to the lack of social interaction and cognitive stimulation among rural individuals.24 Social interaction could improve the cognitive reserve of the elderly and reduce the risk of dementia. Moreover, it is a group activity, which not only promote communication among participants but also give them good social support and emotional comfort, and it has also been proved to be helpful in reducing the risk of MCI.25
This study showed that old age and smoking were risk factors for MCI in both rural and urban participants. Similar results were also observed in some previous studies.26,27 Cognitive function will degrade with age,28 and long-term inhalation of nicotine can damage blood vessels, increase oxidative stress, and cause cognitive decline.29 The content of nicotine intake may be related to the duration and the daily amount of smoking,30 but this study did not collect these information of participants, which may be one of the reasons why former smokers were risk factors for MCI, but current smokers could not significantly predict MCI in our adjusted model. Moreover, despite the prevalence of the comorbidity between COPD and smoking, the role of smoking in cognition and brain damage in COPD-Smoking comorbidity is largely unclear. There may be a potential collinear relationship among smoking, lung function, and cognitive function in patients with COPD. The previous study and our study believed that COPD patients who were smokers had a higher risk of cognitive impairment,31 but Zeng et al confirmed that nicotine had a protective effect on dopaminergic neurons, and presumably, nicotine may preempt a protective mechanism that buffers cognitive impairment in COPD-Smoking comorbidity.32 Therefore, the relationship between smoking and cognitive function among COPD patients need to be further explored.
This study found that the prevalence of MCI among participants who slept less than 6 hours, was higher both in rural and urban areas, and the prevalence of MCI was low among participants shopping regularly and exercise for more than 2 hours a day. The results of adjusted multivariate regression analysis showed that urban participants who slept for 6–8 hours a day, shopping frequently and exercise for more than 2 hours a day had a lower risk of MCI, but it was not significant for rural participants. There were significant differences between rural and urban participants in living environment, lifestyle, and disease-management knowledge, which might explain these significant differences between urban and rural areas, but the mechanism of the differences needs further discussion.11
In this study, the incidence of MCI in participants who insisted on long-term home oxygen therapy was lower, and the incidence in participants with the most serious lung function damage were higher than others in total. Similar results were found in a previous study, which reported independent links between lung function and cognition, and impairment of lung function may lead to more serious cognitive impairment.33 A study suggested that intermittent and persistent hypoxia may be caused by poor pulmonary dysfunction in COPD patients.34 In the case of hypoxia, cerebral blood perfusion is reduced, which may increase ischemia in some brain areas and may lead to subcortical atrophy.35 Hypoxia events or chronic hypoxia in the brain can also lead to the production of free radicals and neuronal damage.36 This may be why hypoxia is one of the risk factor for cognitive impairment. Our logistic regression analysis showed that patients with COPD who insisted on long-term home oxygen therapy were less likely to suffer from MCI, especially in rural areas, and the previous study also indicated that the treatment with supplemental oxygen markedly decreased the risk of cognitive impairment.37 However, there was no significant correlation in urban participants in our study. This may be related to the compliance with oxygen therapy or oxygen therapy equipment of rural patients with COPD.
This study has some limitations too. First, this was a cross-sectional study, and no causality can be established from this study. Second, while every effort is made to control for some confounding factors, it might be that there were some potential collinearity relationships, potential confounders, and bias between some variables, and some potential confounding factors remain were not taken into account, for example, we did not consider the quantity and duration of smoking. Third, our study could not exclude some recall bias because some self-reported data were collected. Fourth, the physical condition of several participants may not have been evaluated accurately, for example, some participants may not have visited a hospital for a comprehensive examination, and they may have provided unreliable answers when asked about comorbidities. Nevertheless, our study still provides a reference for the differences in cognitive impairment and risk factors among COPD patients in urban and rural areas.
Conclusion
In summary, the results of this study showed that the prevalence of MCI was significantly higher in rural areas than in urban areas, and the risk factors of MCI in rural and urban COPD patients were not completely the same in lifestyle and disease-related factors, especially in exercise, sleeping, shopping, and long-term home oxygen therapy. Medical staff should pay more attention to the daily activities and physical exercise for urban COPD patients, and the compliance of oxygen therapy for rural patients.
Ethical Approval
The study was approved by the Bioethics Committee of Qionglai Medical Center Hospital, China (NO,202203), and informed consent was obtained from all subjects involved in the study. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Acknowledgments
We would like to thank all COPD patients who completed questionnaires for their participation; we gratefully acknowledge Qionglai Medical Center Hospital for providing a platform for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by the National Social Science Funding Project (20BRK039).
Disclosure
The authors declare no conflict of interest, and the sponsors had no role in the design, execution, interpretation, or writing of the study.
References
1. Ruvuna L, Sood A. Epidemiology of chronic obstructive pulmonary disease. Clin Chest Med. 2020;41(3):315–327. doi:10.1016/j.ccm.2020.05.002
2. Fang LW, Gao P, Bao HL, et al. Chronic obstructive pulmonary disease in China: a nationwide prevalence study. Lancet Respir Med 2018;6(6):421–430. doi:10.1016/S2213-2600(18)30103-6
3. Criner GJ, Dreher M, D’Ambrosio CM, et al. COPD advanced patient management. Chest. 2018;153 (6) :1497–1498. doi:10.1016/j.chest.2018.03.054
4. Dodd JW, Getov SV, Jones PW. Cognitive function in COPD. Eur Respir J. 2010;35(4):913–922. doi:10.1183/09031936.00125109
5. Villeneuve S, Pepin V, Rahayel S, et al. Mild cognitive impairment in moderate to severe COPD: a preliminary study. Chest. 2012;142(6):1516–1523. doi:10.1378/chest.11-3035
6. Han YL, Jia JJ, Li X, et al. Expert consensus on the care and management of patients with cognitive impairment in China. Neurosci Bull. 2020;36(3):307–320. doi:10.1007/s12264-019-00444-y
7. Dag E, Bulcun E, Turkel Y, et al. Factors influencing cognitive function in subjects with COPD. Respir Care. 2016;61(8):1044–1050. doi:10.4187/respcare.04403
8. Dodd JW, Novotny P, Sciurba FC, et al. Executive function, survival, and hospitalization in chronic obstructive pulmonary disease. A longitudinal analysis of the National Emphysema Treatment Trial(NETT). Ann Am Thorac Soc. 2015;12 (10) :1473–1481 doi:10.1513/AnnalsATS.201506-373OC.
9. Park MO, Oh HS, Seo WS. Effects of a cognitive rehabilitation programme on cognitive function, self-management and quality of life in patients with chronic obstructive pulmonary disease. Int J Nurs Pract. 2021;27(4):e12932. doi:10.1111/ijn.12932
10. Singh B, Mielke MM, Parsaik AK, et al. A prospective study of chronic obstructive pulmonary disease and the risk for mild cognitive impairment. JAMA Neurol. 2014;71(5):581–588. doi:10.1001/jamaneurol.2014.94
11. Nakamura K, Kitamura K, Watanabe Y, et al. Rural-urban differences in the prevalence of cognitive impairment in independent community-dwelling elderly residents of Ojiya city, Niigata Prefecture, Japan. Environ Health Prev Med. 2016;21 (6) :422–429. doi:10.1007/s12199-016-0542-2
12. Jia JP, Zhou AH, Wei CB, et al. The prevalence of mild cognitive impairment and its etiological subtypes in elderly Chinese. Alzheimers Dement. 2014;10(4):439–447. doi:10.1016/j.jalz.2013.09.008
13. Yin P, Ma QF, Wang LM, et al. Chronic obstructive pulmonary disease and cognitive impairment in the Chinese elderly population: a large national survey. Int J Chron Obstruct Pulmon Dis. 2016;11:399–406. doi:10.2147/COPD.S96237
14. Yang Y, Deng H, Yang QQ, et al. Mental health and related influencing factors among rural elderly in 14 poverty state counties of Chongqing, Southwest China: a cross-sectional study. Environ Health Prev Med. 2020;25(1):51. doi:10.1186/s12199-020-00887-0
15. Xu M, Jiang YY, Yin JH, et al. Risk factors for clonorchis sinensis infection in residents of Binyang, Guangxi: a Cross-Sectional and Logistic Analysis Study. Front Public Health. 2021;9:588325. doi:10.3389/fpubh.2021.588325
16. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
17. China D, China P Guidelines for the diagnosis and treatment of dementia and cognitive impairment in China in (1):Dementia and its classification and diagnostic criteria. Natl Med J China. 2018;13:965–970. (Chinese).
18. Gong D, Peng Y, Liu X, et al. Dose health education on dementia prevention have more effects on community residents when a community physician/nurse leads it? A cross-sectional study. Front Public Health. 2023;11:1101913. doi:10.3389/fpubh.2023.1101913
19. Wang FY, Zhang DY, Liang ZY. Interpretation of Guideline for the Diagnosis and Treatment of COPD (2021 revision) for general practitioners. Chin Gen Pract. 2021;24:3660–3663,3667.
20. Dulohery MM, Schroeder DR, Benzo RP. Cognitive function and living situation in COPD: is there a relationship with self-management and quality of life? Int JChron Obstruct Pulmon Dis. 2015;10:1883–1889. doi:10.2147/COPD.S88035
21. Yohannes AM, Eakin MN, Holbrook JT, et al. Association of mild cognitive impairment and characteristic of COPD and overall health status in a cohort study. Expert Rev Respir Med. 2021;15(1):153–159. doi:10.1080/17476348.2021.1838278
22. Cleutjens FA, Franssen FM, Spruit MA, et al. Domain-specific cognitive impairment in patients with COPD and control subjects. Int J Chron Obstruct Pulmon Dis. 2016;12:1–11. doi:10.2147/COPD.S119633
23. Wang T, Mao LJ, Wang JH, et al. Influencing factors and exercise intervention of cognitive impairment in elderly patients with chronic obstructive pulmonary disease. Clin Interv Aging. 2020;15:557–566. doi:10.2147/CIA.S245147
24. Wu YT, Prina AM, Brayne C. The association between community environment and cognitive function: a systematic review. Soc Psychiatry Psychiatr Epidemiol. 2015;50(3):351–362. doi:10.1007/s00127-014-0945-6
25. Tian G, Shuai JL, Li R, et al. Association between playing cards/mahjong and risk of incident dementia among the Chinese older adults: a prospective cohort study. Front Aging Neurosci. 2022;14:966647. doi:10.3389/fnagi.2022.966647
26. Barnes JN. Exercise, cognitive function, and aging. Adv Physiol Educ. 2015;39(2):55–62. doi:10.1152/advan.00101.2014
27. Rusanen M, Ngandu T, Laatikainen T, et al. Chronic obstructive pulmonary disease and asthma and the risk of mild cognitive impairment and Dementia: a population based CAIDE Study. Curr Alzheimer Res. 2013;10(5):549–555. doi:10.2174/1567205011310050011
28. Drachman DA. Aging of the brain, entropy, and Alzheimer disease. Neurology. 2006;67(8):1340–1352. doi:10.1212/01.wnl.0000240127.89601.83
29. Hill RD, Nilsson LG, Nyberg L, et al. Cigarette smoking and cognitive performance in healthy Swedish adults. Age Ageing. 2003;32(5):548–550. doi:10.1093/ageing/afg067
30. Valentine G, Sofuoglu M. Cognitive Effects of Nicotine: recent Progress. Curr Neuropharmacol. 2018;16(4):403–414. doi:10.2174/1570159X15666171103152136
31. Xie F, Xie L. COPD and the risk of mild cognitive impairment and dementia: a cohort study based on the Chinese Longitudinal Health Longevity Survey. Int J Chron Obstruct Pulmon Dis. 2019;14:403–408. doi:10.2147/COPD.S194277
32. Zeng F, Hong W, Zha R, et al. Smoking related attention alteration in chronic obstructive pulmonary disease-smoking comorbidity. BMC Pulm Med. 2022;22(1):182. doi:10.1186/s12890-022-01964-6
33. Pathan SS, Gottesman RF, Mosley TH, et al. Association of lung function with cognitive decline and dementia: the Atherosclerosis Risk in Communities (ARIC) Study. Eur J Neurol. 2011;18(6):888–898. doi:10.1111/j.1468-1331.2010.03340.x
34. Gibson GE, Pulsinelli W, Blass JP, Duffy TE. Brain dysfunction in mild to moderate hypoxia. Am J Med. 1981;70(6):1247–1254. doi:10.1016/0002-9343(81)90834-2
35. Antonelli Incalzi R, Marra C, Giordano A, et al. Cognitive impairment in chronic obstructive pulmonary disease – a neuropsychological and spect study. J Neurol. 2003;250(3):325–332. doi:10.1007/s00415-003-1005-4
36. Ryu CW, Jahng GH, Choi CW, et al. Microstructural change of the brain in chronic obstructive pulmonary disease: a voxel-based investigation by MRI. COPD. 2013;10(3):357–366. doi:10.3109/15412555.2012.752808
37. Thakur N, Blanc PD, Julian LJ, et al. COPD and cognitive impairment: the role of hypoxemia and oxygen therapy. Int J Chron Obstruct Pulmon Dis. 2010;5:263–269. doi:10.2147/copd.s10684
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.