Back to Journals » Advances in Medical Education and Practice » Volume 13
Routine Application of Lung Ultrasonography in Respiratory Care: Knowledge, Perceptions, and Barriers to Instigate
Authors Sreedharan JK ![]() , Karthika M, Alqahtani JS
, Karthika M, Alqahtani JS ![]() , AlRabeeah SM, Alnasser M, Alqahtani AS
, AlRabeeah SM, Alnasser M, Alqahtani AS ![]() , AlAhmari MD, Zechariah Jebakumar A
, AlAhmari MD, Zechariah Jebakumar A ![]() , AlEnezi M, Ghazwani AA, Sara Mathew C
, AlEnezi M, Ghazwani AA, Sara Mathew C ![]() , Aldhahir AM
, Aldhahir AM ![]() , Nair SG
, Nair SG
Received 8 September 2022
Accepted for publication 9 November 2022
Published 15 November 2022 Volume 2022:13 Pages 1395—1406
DOI https://doi.org/10.2147/AMEP.S389013
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Jithin K Sreedharan,1 Manjush Karthika,2 Jaber S Alqahtani,1 Saad M AlRabeeah,1 Musallam Alnasser,1 Abdullah S Alqahtani,1 Mohammed D AlAhmari,1 Arulanantham Zechariah Jebakumar,3 Meshal AlEnezi,1 Abdullah A Ghazwani,1 Chris Sara Mathew,2 Abdulelah M Aldhahir,4 Suresh G Nair5
1Department of Respiratory Care, Prince Sultan Military College of Health Sciences, Dammam, Saudi Arabia; 2Respiratory Care, Department of Health and Medical Sciences, Khawarizmi International College, Abu Dhabi, United Arab Emirates; 3Vice Deanship of Postgraduate Studies and Research, Prince Sultan Military College of Health Sciences, Dammam, Saudi Arabia; 4Respiratory Therapy Department, Faculty of Applied Medical Sciences, Jazan University, Jazan, Saudi Arabia; 5Department of Anesthesiology and Critical Care Medicine, Aster Medicity, Kochi, Kerala, India
Correspondence: Jithin K Sreedharan, Department of Respiratory Care, Prince Sultan Military College of Health Sciences, Dammam, Saudi Arabia, Email [email protected]
Background: Lung Ultrasound (LUS) had proved to be beneficial in detecting respiratory disorders at the bedside. Understanding the important role of Respiratory Therapists (RTs) in the critical care, we aimed to assess their knowledge, perceived relevance of LUS to clinical practice, current skill gaps, and barriers to practice.
Methods: A cross-sectional, nationwide survey conducted among the RTs working in the Kingdom of Saudi Arabia. The validated questionnaire included 4 sections; the demographics, knowledge and perceptions, applicability and self-reported proficiency, and barriers to the use of LUS by RTs.
Results: A total of 256 RTs across different regions of Saudi Arabia participated in this survey. 71.9% of them were males, and 46.1% of the participants were having < 5 years of working experience. Only (18.1%) of the participants used LUS in their clinical practice, and (43%) of them had never received any training. 66% of the participants perceived LUS as an effective tool in the RT practice and immensely valuable in their daily practice (70%). A large proportion of RTs perceived LUS to be ineffective in calculating the lung score (50.4%), assessing the diaphragm (40.2%), and detecting pulmonary edema (38.3%). Calculating lung score has a lower mean score of 2.55 on both skills, and identifying its applicability to clinical practice with a mean score of 2.71 than other indications. Lack of training and curriculum (154/256; 60.2%) remains the top barrier that prevented RTs from using LUS in their clinical practice.
Conclusion: While many RTs in Saudi Arabia perceived LUS as an effective tool in the RT practice, considerable competence gap exist, indicating the need for LUS training. There is a need for incorporating LUS into the curriculum of RT schools and promoting competency-based training for the current RT workforce to help improve patient care.
Keywords: lung ultrasound, respiratory therapy, curriculum, training
Introduction
Lung ultrasound (LUS) is a point-of-care imaging tool routinely used in acute care settings, primarily to assess the pleura, lung parenchyma, and other associated structures like the ribs, intercostal muscles, and diaphragm. Traditionally, chest x-rays were considered the daily tool to evaluate lung pathologies, supported by longstanding data,1 however, there exists studies that question its diagnostic superiority and clinical impact.2–4 The evolution of the practice of LUS in recent past with superior quality and spatial resolution has yielded greater diagnostic accuracy.5 LUS was reported to be more advantageous than chest x-rays and computed tomography in terms of its availability, portability, reproducibility, absence of radiation, real-time imaging, and documentation.6 This makes LUS a promising diagnostic tool while caring for a person receiving mechanical ventilation. While radiologists are the primary subject experts of diagnostic ultrasound, with its diverse scope, acute care professionals also have adopted this practice. Within the inter-professional team of intensive care units is the Respiratory Therapist (RT), who plays a significant role in the care of ventilated patients. Globally, due to the evolving nature of LUS amongst acute care physicians, it is not yet considered one of the core standard practices of an RT. It is also reported that the scope of RTs in imaging areas, such as LUS is vast, but underutilized.7 A recently published scoping review about the involvement of RTs in ultrasound training and practice strikingly highlighted the paucity of articles, with the inclusion of only seven published studies.8 Although the need for incorporating LUS in the curriculum of RT schools and competency-based training for working RTs are echoed by few authors, there remains a paucity of literature are available to support this as a global approach, except for some anecdotal updates.9
The respiratory therapy profession exists in the Kingdom of Saudi Arabia, since the 1970s, with a current status of 23 respiratory therapy schools, and a total of 1400 working RTs.10,11 It is subjectively reported by some centers that, RTs are being trained on LUS, within their department, and many of them are using this imaging modality. However, there is no objective data to justify the same with regards to the duration of their training, competency checks, and barriers to the practice. Hence, a national survey was planned to assess the scope of practice of LUS among RTs in Saudi Arabia. The domains of this survey included knowledge, perception, and barriers related to the practice of LUS. We hope that the results of this survey will set a reference mark for future projects, focusing on LUS training and thereby expanding the scope of practice of RT professionals in the Kingdom of Saudi Arabia.
Materials and Methods
Study Design and Participants
This is a cross-sectional descriptive study conducted online among RTs. Qualified RTs working in the public and private sector hospitals in the country, from different educational levels, gender and age groups were involved in this study. The survey was administered in the months of February and March 2022. As it is not feasible to conduct a systematic nationwide sampling procedure during this period especially due to the pandemic, therefore we, the researchers opted to use an online survey. A well-organized region-based approach was adopted for conveying information to the target population and we used a popular online survey platform to collect the responses. Questions corresponding to RT’s knowledge and expertise, perception, and potential barriers to active implementation of LUS were employed to archive the response, and a pop-up request turned up to answer the unattended question before moving to the subsequent section. A total of 256 (45.8% of the target sample size) RTs responded to all the survey questions; hence, they were chosen for the study, and considered it for analysis. The target sample size was 560 (535–585), determined by identifying the smallest acceptable size of a demographic subgroup, and by assuming a response distribution of 50% i.e 280 with a ±5% margin of error and a confidence level of 95%.
Inclusion and Exclusion Criteria
RTs practicing in the public and private sector hospitals in the Kingdom of Saudi Arabia with internet accessibility and who were willing to participate in the study were included. RTs working in medical equipment companies, and those who are retired from active practice were fully excluded from the study. No personal appeal or gratuity was rendered to participants to take part in the study. None of the RTs who completed the survey were excluded from the study.
Questionnaire Development
The survey questionnaire was created in the English language. Studies describing the applications of LUS and the competencies required for its safe practice were reviewed.2–4,8,12–19 Drawing on this knowledge, two researchers with expertise in medical education, LUS, and survey design developed the questionnaire to investigate RT’s knowledge and perceptions about LUS. A five member expert panel composed by the research group, encompassed professionals who have expertise in survey analysis besides proficiency in the English language carried out the content validation. The panel examined the core content, language, appropriateness of questions for various domains, scoring patterns, etc. The survey piloted with the experimental research group comprised of 25 judiciously selected participants of various ages, genders, and educational credentials. The questions in each domain; knowledge, perception, and barriers underwent content validity and internal consistency and analyzed the responses to each question in the pilot study using Cronbach’s alpha reliability test. The overall Cronbach’s Alpha value is 0.936 (>0.6) which was found to be acceptable. The expert panel appraised their observations and advised for necessary OR no modifications before launching the survey.
The questionnaire was divided into four sections; the socio-demographic segment (Part-1) and the knowledge (Part-2), perception (Part-3), and barrier (Part-3) section. In the socio-demographic portion, respondents’ particulars such as gender, age, nationality, geographical location, educational qualification, designation at the workplace, work experience in years, type of hospital with a number of beds, and details about the specialized area of work were collected. The participants’ training and accreditation in LUS were identified via closed‑ended questions. An incremental scale was utilized to quantify the participants’ LUS practice. Participants were requested to rate the importance of LUS using a Likert scale in addition to their self‑reported proficiency levels and knowledge of LUS. While in the remaining parts ie, questions relevant to the knowledge included a set of answers just as “Yes”, “No” and “Don’t know” and a rating of “very poor” to “very good”. The perception questions confined the answers “Strongly agree”, “Agree”, “Neutral”, “Disagree”, “Strongly Disagree”, and one question with a rating scale of 1–5. Finally, the barrier section with one question listed the potential barriers, the data presented in frequencies, and one open-ended question. Each variable under the data has been scored as per the questionnaire apart from demographic characters.
Ethical Considerations
The survey was conducted after ethical approval from the Prince Sultan Military College of Health Sciences, Dhahran (IRB number: IRB-2022-RC-008). Participants’ consent was taken, while clicking the survey link, the informed consent showed up first, followed by the questionnaire. Those who were not interested to take part in the survey were given the option to decline the participation and opted not to participate in the survey. Participants were appraised about the goals of the study in the informed consent and they were also notified that it is fully an anonymous survey, and warranted the privacy of their data. This study complied with the tenets of the Declaration of Helsinki.
Statistical Analysis
All completed survey responses were evaluated and recorded in an excel spreadsheet and the statistical analysis has been performed with SPSS (Statistical Package for Social Sciences) Package with version 28. The dissemination of all qualitative variables both demographic and other variables (i.e, close-ended) values of samples have been examined with frequency tables among samples. The comparison tables have been calculated to find the association for comparing the qualitative variables about the use of ultrasound devices with regards to the training and RTs perceptions of the applicability of LUS and their self-reported proficiency in LUS by applying the chi-square test. Two-sided statistical tests with a p-value of ≤0.05 (95%) have been considered significant.
Results
A total of 256 RTs accepted the invitation to participate in this survey. Respondents included people from different nationalities but active in the professional practice in the Kingdom of Saudi Arabia and from its all four geographic regions. Of the 256 participants, 184 (71.9%) were males; the mean age was 30.7 (SD ± 7.7) years; 234 (91.4%) were Saudi nationals. A total of 186 (72.7%) participants reported a bachelor’s degree in RT as their highest degree of education; 44 (17.2%) Master and 14 (5.5%) Ph.D. as the highest degree of their education. The practice regions and practice experience (in years) of the participants were diverse; however, 105 (41%) of the sample practicing in the eastern region and 118 (46.1%) had less than 5 years of clinical experience. Table 1 explains about the demographic characteristics of the study participants.
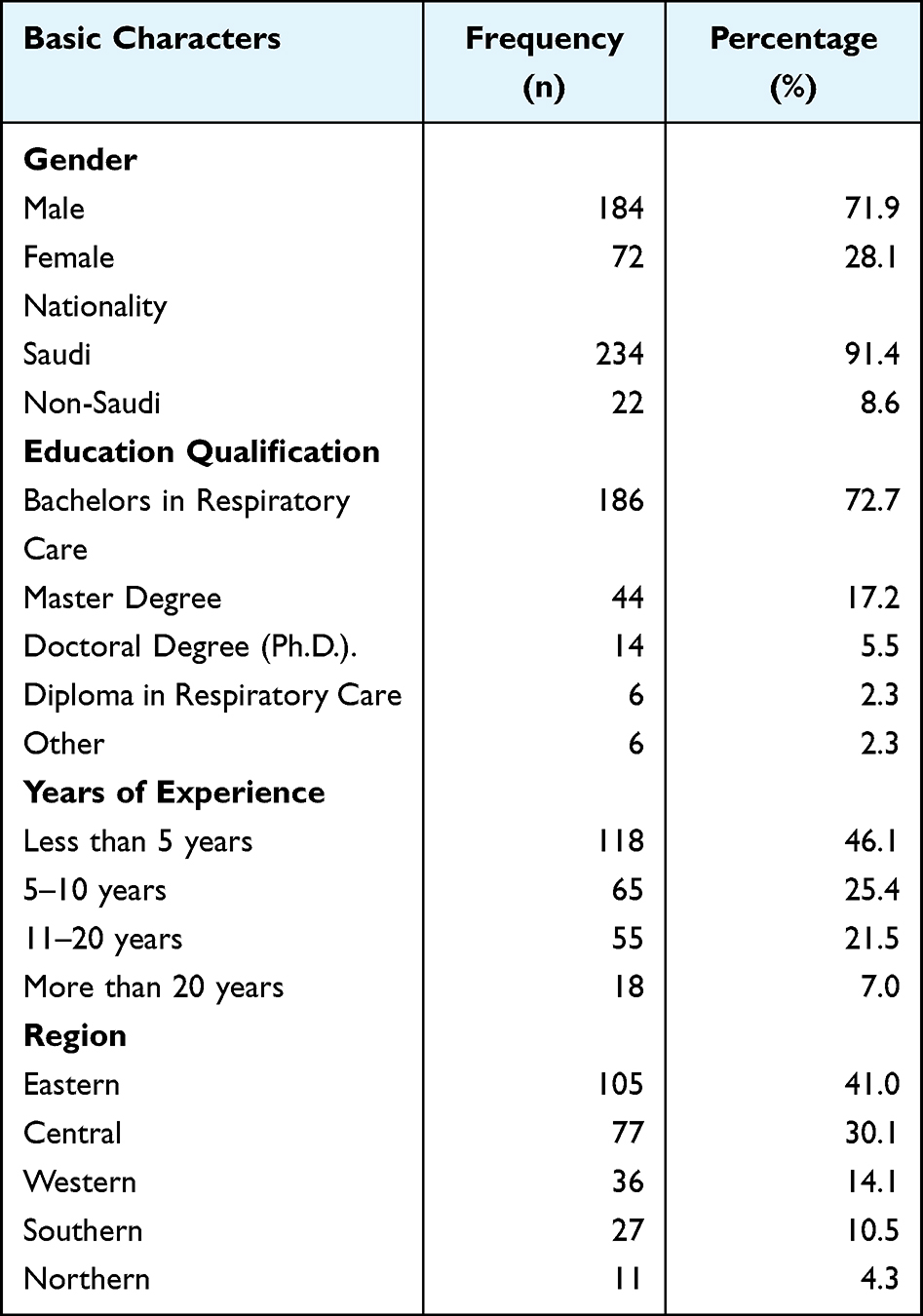 |
Table 1 Participants’ Demographic Characteristics |
Knowledge About Lung Ultrasound
The first part of the questionnaire concerns questions about the current use and knowledge of LUS. Forty-eight (18.8%) participants used ultrasound devices in their clinical practice, and 24 (50%) of them had never received any training. Conversely, a couple of them has received formal training but has not applied it in their daily practice (50/208; 24%) (Chi-square = 19.24; P-value=0.001) (Table-2). Furthermore, it is also noted that majority of the RTs are not using LUS because they have not received any formal training (69.9%), however the alarming fact is that 43.8% (21/48) of the RTs those who are using the LUS also have not received any formal training. The majority of them were working in government hospitals (75%), with an average bed capacity of 100–399 (43.8%) under the title of “respiratory therapist” (48.4%). The participants attained basic knowledge to perform a diagnostic study (32.4%) or elementary knowledge to perform an LUS examination (29.7%); however, (32.8%) reported having no knowledge about LUS. Knowledge of the participants on various aspects concerning the LUS scan was assessed (Table 3). Notwithstanding the participant’s present work profiles, level of knowledge, and primary training the large majority (81.6%) believe LUS is a promising diagnostic tool for an RT.
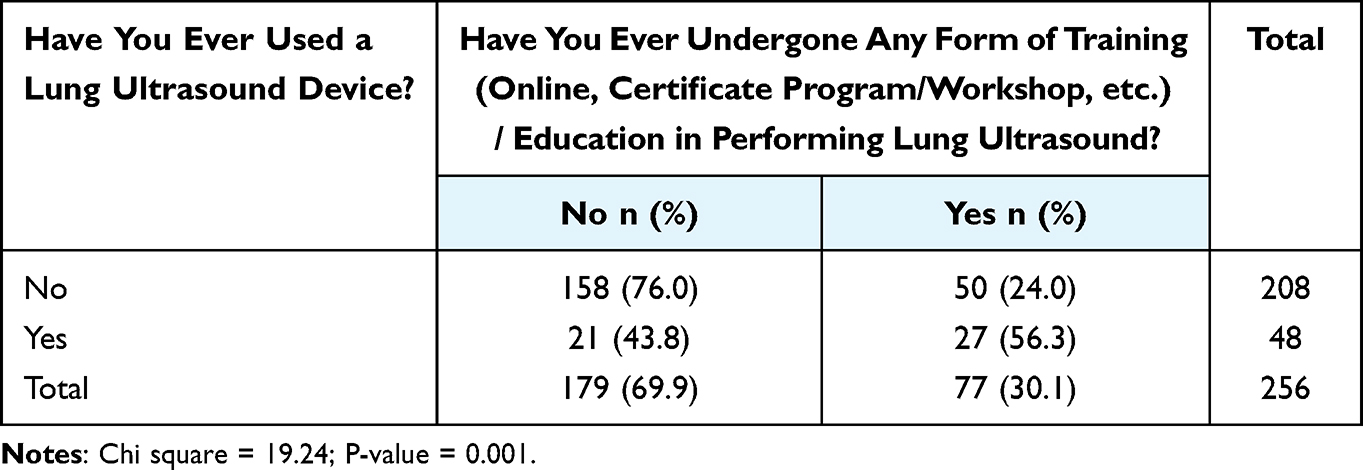 |
Table 2 The Significance of the Use of Ultrasound Devices with Regards to the Training |
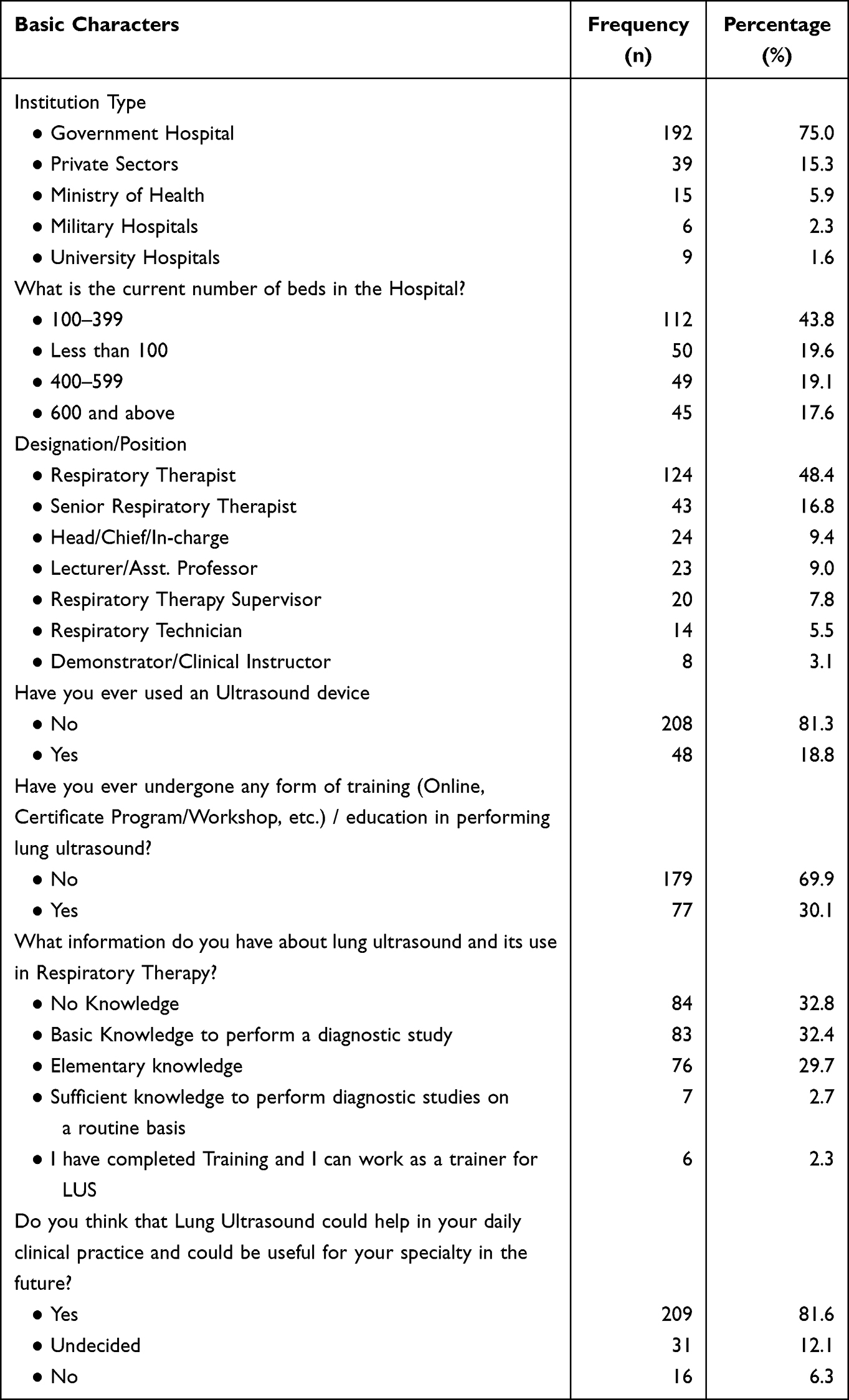 |
Table 3 The Knowledge of Participants Concerning Lung Ultrasound Scan |
Perceived Applicability, Self-Reported Skills, and Skill Gap in Diagnostic Applications of LUS
Ultrasound was perceived to be highly useful (66%) in the practice of Respiratory Therapy. The participants had greater confidence and agree that non-physicians (80.6%) can perform LUS, and it is highly valuable in their daily practice (70.7%). A significant majority (79%) highly recommended incorporating the LUS training formally into the RT curriculum. Half of the respondents expressed a lack of institutional support (50.4%) but expressed interest to receive continuous training (79.3%) (Table 4).
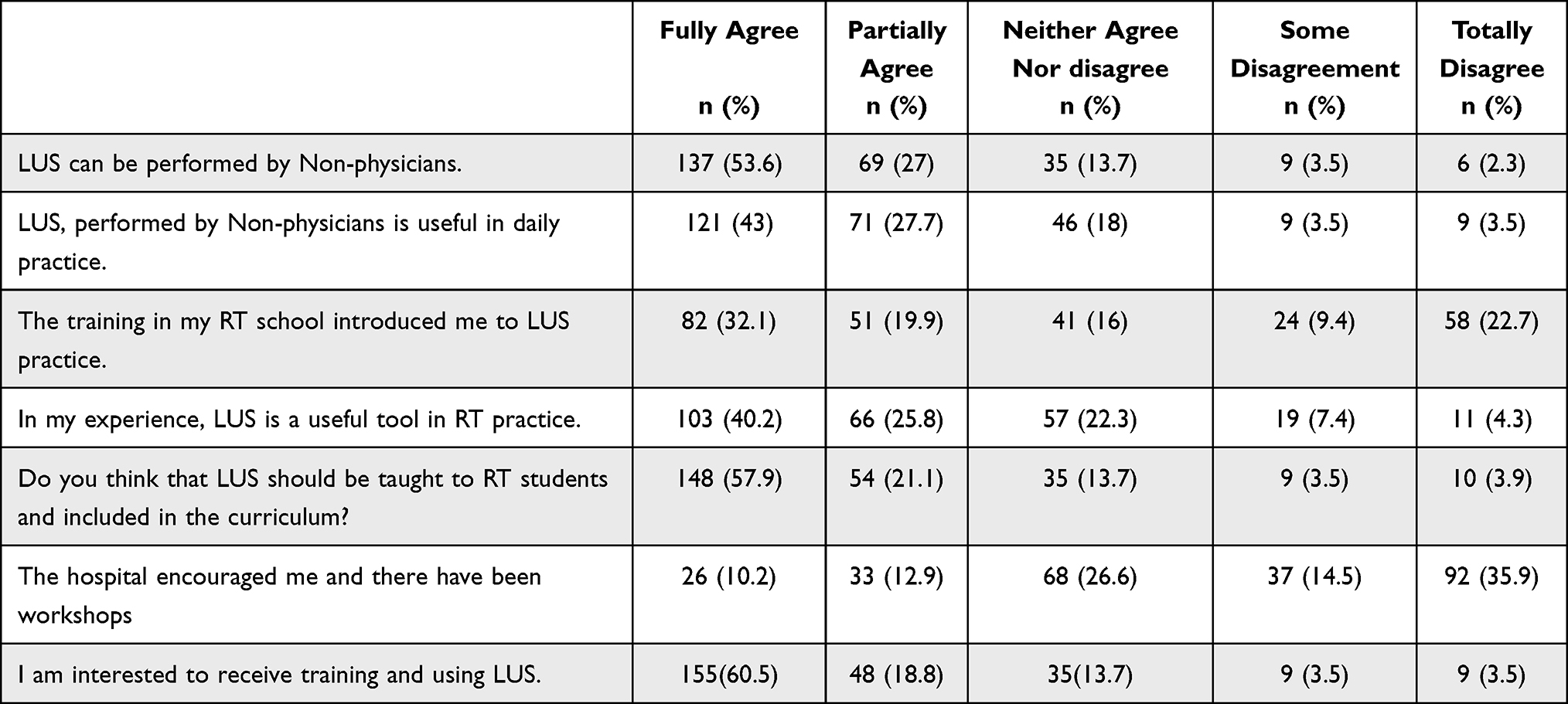 |
Table 4 Respiratory Therapists’ Perception About the LUS in Their Clinical Practice |
When comparing the applicability in clinical practice and participant skills and knowledge, a significant difference was found, with the indications such as Identifying pneumothorax, identifying lung consolidation/pneumonia, identifying pleural effusion and identifying pulmonary edema on current skills or knowledge (p = 0.001). The other indications were not statistically significant and the participants observed those indications were not much applicable to their clinical practice and current skills and knowledge (Table 5).
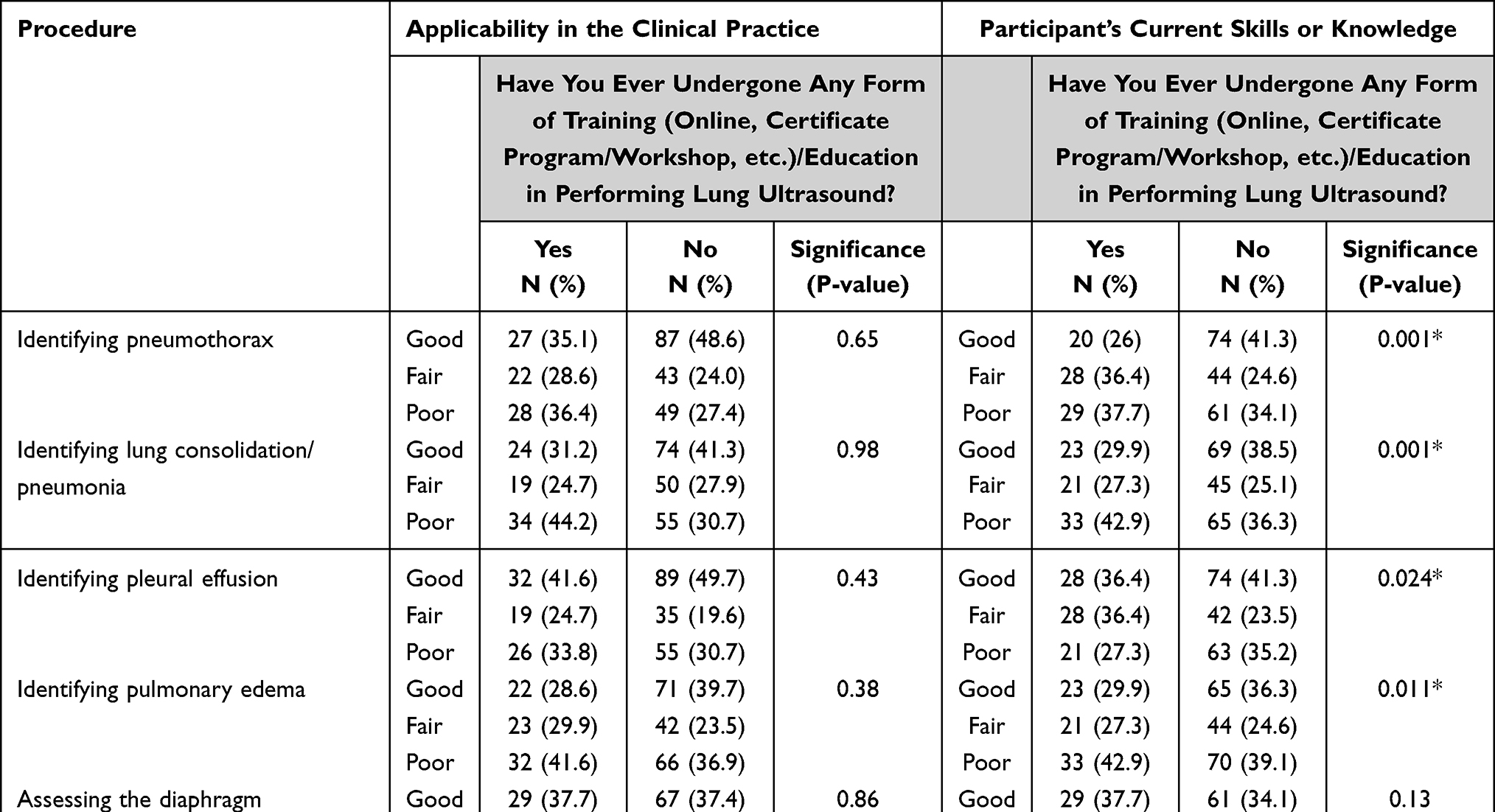 |
Table 5 RTs Perceptions of the Applicability of LUS and Their Self-Reported Proficiency |
The survey respondents perceived that LUS was least applicable in the following areas; calculating the lung score (50.4%), assessing the diaphragm (40.2%), identifying pulmonary edema (38.3%), and assessing the airway/intubation (38.4%). On the contrary, the largest perceived skill gap reported was also reported in calculating the lung score (50.4%), identifying pulmonary edema (40.2%), and assessing the diaphragm (39.8%) (Table 6). Skill gap was defined as the difference between the perceived applicability of an application or procedure and self-rated skills/knowledge in that application or procedure.14 A comparison was carried out between each reported skill, and between skill and application in clinical practice in relation to all the indications. Calculating lung score based on examination of 12 regions of interest has been proposed to assess lung aeration changes has a lower mean score on both skills (Mean score 2.55) and identifying its applicability to clinical practice (Mean score 2.71) than other indications with almost mean scores of 3 and 4 (Figure 1).
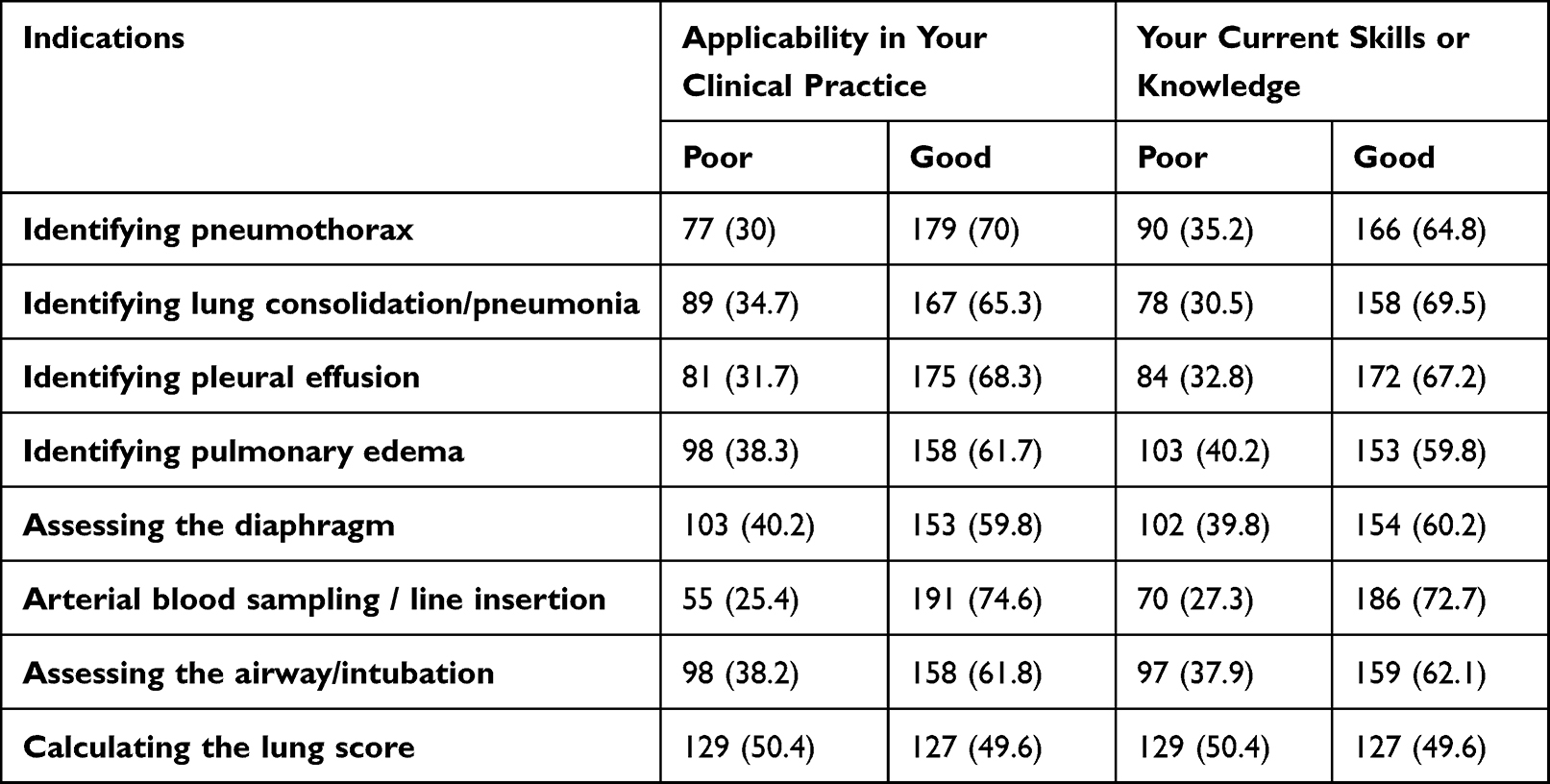 |
Table 6 RTs Perceptions About the Applicability and Current Level of Skills or Knowledge in LUS |
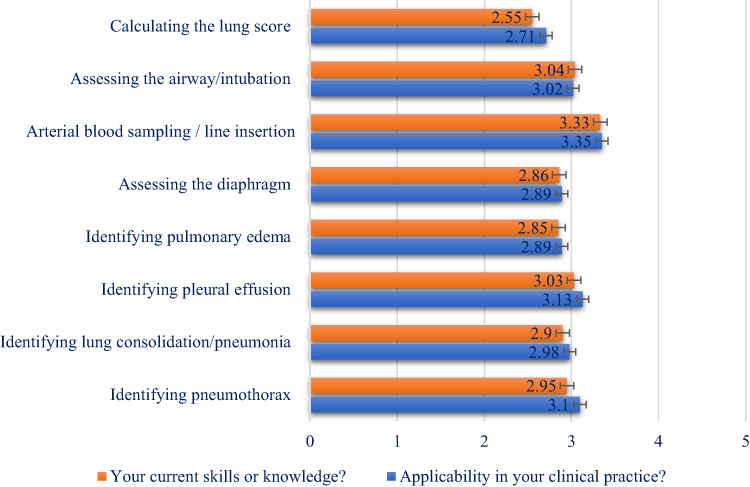 |
Figure 1 Skill gap of ultrasound diagnostic applications and bedside procedures in Respiratory Care. Skill gap of ultrasound diagnostic applications is demarcated as the variance between comprehended appropriateness of an application and self-scaled skills in carrying out bedside procedures, in the basic ground of proper training, showed as mean gap (Likert scale 1–5); error bars point out standard deviations. |
Barriers to Use LUS
A proportion (90/256; 35.2%) of respondents were having no interest to implement LUS in their practice; however, lack of proper training and curriculum (154/256; 60.2%) remains the top reason and a barrier that prevented them from using LUS. Numerous barriers were identified of which the top two were as follows: lack of available USG machines on site (113/256; 44.1%) or lack of learner time (84/256; 32.8%) (Figure 2).
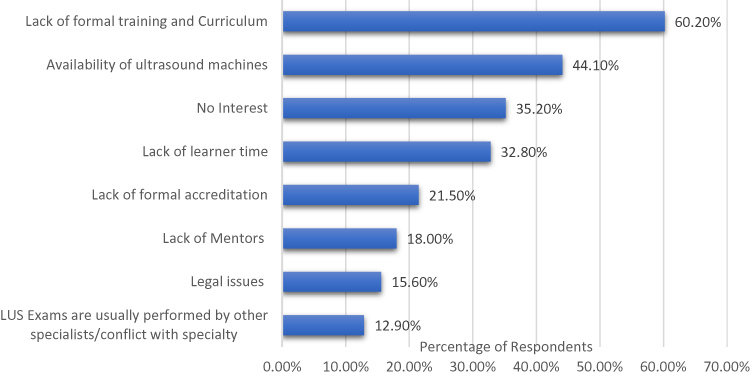 |
Figure 2 Barriers to implement LUS in RT practice: Perceived barriers to LUS use by RTs. RTs were asked the question “What are some barriers to the use of LUS in your clinical practice?” Respondents were allowed to select more than one response. Percentages calculated as the number of responses divided by total (n= 256). Abbreviation: LUS, Lung Ultrasound. |
Discussion
Acquiring the skill in LUS will be a benchmark in current practice of RTs, and it may assist then in reducing adverse events in ventilated patients. LUS appears to be closely related and promising tool for RTs considering their scope of practice in the acute care settings such as ICUs and Emergency rooms.7 Being available at the bedside of these units, RTs offer better diagnostic accuracy in resource- and time limited settings. Since RTs are one of the primary practitioners of mechanical ventilation, if equipped with LUS, will have positive outcomes in terms of; real-time confirmation of tracheal intubation; early recognition of pneumothorax; facilitation of weaning; and optimization of the PEEP in worsening ARDS patients, by evaluating the B-line patterns and LUS score.8 This study was the first to investigate Saudi Arabia’s RTs about their use (or lack of use) of LUS. Even though the sample size captured only a small section (17.4%) of Saudi Arabia’s RTs, the key demographic and professional variables of RTs in the Kingdom were reflective of the survey sample. A greater part of the participants was male, worked in a clinical capacity, and was employed in government practice and practiced within the respiratory care field. These findings are not surprising as they reflect the demographic and professional trends seen in Saudi Arabia.11 The findings from the current study might indicate decreased use of LUS by RTs. However, it is imperative to remark that the current study only surveyed around 17.4% of RTs in the Kingdom, and therefore the level of LUS practice reported may not necessarily be a true representation of the whole cohort. A large international study is also warranted to offer a more accurate overview of the use of LUS by RTs.8
It is possible that the paucity of definite guidelines or position statements for the RTs to perform LUS may have led to the uncertainty as reflected in the survey results. Furthermore, this uncertainty is likely to be perpetuated given that LUS is an emerging tool for RTs and its prodigious use in the respiratory care field is still evolving.7 It is anticipated that the outcomes of this research will improve the understanding in this regard. There is clearly a need for both national and international regulatory bodies to acknowledge this situation and to work with professional leaders to establish guidelines to provide certainty for the scope of practice and training.19 We also found there is a strong association between the utility of lung ultrasound devices with training and without training. Table 4 shows the majority of samples who have not received training are not using the device and its significance. At the same time, it is worth mentioning, that an insignificant share of participants who did not receive any formal training is using LUS in their clinical practice (Table 4). This aspect has to be investigated in the context of the proliferation of ultrasound machines in the hands of untrained health professionals. Perhaps as discussed by Filly. R in his editorial 30 years ago, these findings can be an unfortunate realization that diagnostic sonography truly is the next stethoscope: used by many, understood by few.20
The results of the survey showed a significant gap between perceived applicability and self-reported skill and knowledge in many ultrasound diagnostic applications and procedures in respiratory patient care (Figure 1). The current study was conducted momentarily after the pandemic of coronavirus disease, and yet the usage of LUS in calculating the lung score based on examination of 12 regions of interest has been proposed to assess lung aeration changes and correlating it with the clinical findings and laboratory markers in ascertaining the severity were considered least relevant.21 The point should be made that the ultrasound expertise and competence of the participants to execute LUS were both limited. Thus, participants were unlikely to be conversant with the latest research on the role of LUS in the assessment of coronavirus disease.22,23
The participants expressed greater confidence in their ability in performing LUS (80.6%), and they strongly believe that it is highly useful in effective patient management (70.7%) as customary. These findings are supported by Swamy et al; they advise that nurses, allied healthcare professionals, and students can precisely obtain and interpret LUS images after a transitory training period in most cases.24 Disappointingly, our findings also indicate that RTs were unable to implement LUS into practice because of the lack of mentors (18%). Prioritizing institutional support for staff training and infrastructure for continuous quality assurance activities, including implementing a service option, is essential for expeditiously incorporating LUS into the scope of practice of an RT. The scores relating to the applicability of each indication of LUS studied were higher than that of the sample’s self-reported proficiency in that skill except for arterial blood gas sampling and line insertion (Figure 1). It is suggestive of the presence of significant skill gaps relating to LUS among RTs. These gaps can only be addressed by the institution of a training program with formal processes for supervision, governance, and accreditation.25 Furthermore, our efforts for assessing the skill gaps can guide educational interventions to resolve these deficiencies.
This survey is the first published research that has specifically explored the barriers that prevent RTs from using LUS. The barriers identified included lack of training, no interest, lack of learner time, legal issues, availability of ultrasound machines, lack of formal training and curriculum, lack of mentors, lack of formal accreditation, and LUS exams were usually performed by other specialists/conflict with the specialty. Lack of formal training was a major barrier (60.2%), as there are very limited LUS training opportunities in Saudi Arabia and the Respiratory Care bachelor’s program at Prince Sultan Military College of Health Sciences (PSMCHS) is the only program that has incorporated LUS formally into the curriculum in the recent past. This requisite was further substantiated by the response of the participants, the majority of them (66%) felt LUS training is useful for their professional practice and opined LUS must be taught to RC students and integrated into their curriculum (79%). The PSMCHS-RC curriculum for LUS was designed to offer organized, interdisciplinary LUS training to RT students through their final year courses by recognizing the importance of ultrasound as an imaging modality in Respiratory Care practice.26 Other medical residency programs such as emergency medicine and internal medicine that have incorporated LUS learning into core curricula have proven benefits from a longitudinal model, given the ability of beginners to retain and reuse core concepts.14,19 With this incorporation of LUS training in the RT curriculum, we hypothesize that more recent cohorts of learners would enter respiratory care practice with higher LUS knowledge and skills.27,28 Another key barrier identified was the shortage of ultrasound equipment, which can be assumed to be due to the views about the prohibitive cost of ultrasound equipment. This issue was compounded by the lack of a clear structure to specifically document the LUS service or as a stand-alone service provided by the RTs. However, to our knowledge, there are currently no studies nationally or internationally that assessed the primary need of LUS training for RTs, and evaluate changes in learning needs over time, thus it remains unknown whether the lack of baseline LUS knowledge and skills is a verdict unique to this country or that this finding is also existing elsewhere.
Since LUS is not included in the daily clinical practice of RTs, the level of training, the number of scans, and the duration of training required to achieve competency in LUS is still unknown. There is a paucity in the literature are substantial gaps identified from the current available literature regarding RTs’ education and exposure in diagnostic ultrasound, although it clearly influences their daily practices.29 Considering the specific scope of practice and expected positive outcomes, RTs can be assigned for LUS after sufficient training and competency assessment. Regarding the training, there observed a significant difference in the duration and methodology of LUS training programs that are currently available.30 It is also observed from several small studies and conference abstracts that LUS skills can be satisfactorily attained by the healthcare professionals by a 2 hour- to- 4 months of training, with at least 20–80 supervised scans.31 Hence, it is highly recommended that professional respiratory care bodies across the globe initiate training programs on LUS for RTs to have competency certification. This also includes inclusion of a comprehensive respiratory care–related ultrasound-training module within the existing worldwide respiratory care curriculum.
Strengths and Limitations
This is the first nationwide survey on the practice of LUS amongst RTs. The strength of the study includes a fair response rate. However, the COVID-19 pandemic has caused a surge in the overall research activity while restricting data collection methods, leading to a rise in survey-based studies. Anecdotal evidence suggests this increase in online survey dissemination has led to a phenomenon of survey fatigue, characterized by decreased response rates, which is assumed to be a reason for low response rate in our study. Participation bias is possible as RTs who use LUS regularly may be keener to participate in the survey. Learners may in fact know more (or less) than they report. However, regardless of whether our participants were under-estimating their self-reported skills and knowledge, the fact that learners feel their skills are inadequate mandates an educational response from the programs or leadership, at least for skills where competencies are an expectation.
Conclusions
Ultrasound is certainly one of the most user-dependent diagnostic technologies that exist. As underscored by the participants LUS can be a prevailing tool to improve patient safety through enhanced and expedited diagnosis and procedural guidance. Even though some very elementary uses of ultrasound can be picked up rapidly, substantial skill is necessary to acquire and interpret fitting information. Building an LUS program for the RTs, optimizes patient-centered and safety outcomes, necessitates judgment and oversight of this influential tool. The establishment of applicable resources together with robust training and competency assessment, image processing, policy to ensure quality, and defining and empowering a qualified person as accountable will ensure the best outcomes. The results of this study suggest that training curricula must-have modules that take account of the learning needs of the students at the undergraduate level. Additionally, the RT program would need to develop mentors and be as affordable as possible.
Future studies should evaluate not only the quantitative but the content and quality of LUS education at the undergraduate level despite the perceived widespread integration of LUS, there continues to be a large LUS skill and knowledge gap. Therefore, LUS educators should not yet assume any significant learner baseline LUS knowledge or skills when developing their LUS curriculum for RTs. It is necessary to establish the scope of practice and institutional privileges. RTs need to be aware of their limitations while performing LUS, and it is critical to know when to call for help from an expert professional (such as a radiologist or an intensivist) when needed.
Abbreviations
LU, Lung Ultrasound; RT, Respiratory Therapy; RTs, Respiratory Therapists; RC, Respiratory Care; PSMCHS, Prince Sultan Military College of Health Sciences; SPSS, Statistical Package for Social Sciences; SD, Standard Deviation.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Ethics Declarations
This study was approved by the ethics committee of the Prince Sultan Military College of Health Sciences, Dhahran (IRB number: IRB-2022-RC-008). Participants provided informed consent electronically and anonymously. All study procedures were performed in accordance with the relevant institutional guidelines and regulations and complied with the tenets of the Declaration of Helsinki.
Acknowledgments
The authors wish to thank the Vice Deanship of Postgraduate Studies and Research at PSMCHS for their continuous support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Henscke CI, Pasternack GS, Schoroeder S, Hart KK, Herman PG. Bedside chest radiography. Diagn Efficacy Radiol. 1983;149(1):23–26.
2. Greenbaum DM, Marschall KE. The value of routine daily chest x-rays in intubated patients in the medical intensive care unit. Crit Care Med. 1982;10(1):29–30. doi:10.1097/00003246-198201000-00007
3. Bekemeyer WB, Crapo RO, Calhoon S, Cannon CY, Clayton PD. Efficacy of chest radiography in a respiratory intensive care unit. A prospective study. Chest. 1985;88(5):691–696. doi:10.1378/chest.88.5.691
4. Rouby JJ, Puybasset L, Cluzel P, Richecoeur J, Lu Q, Grenier P. Regional distribution of gas and tissue in acute respiratory distress syndrome. II. Physiological correlations and definition of an ARDS severity score. CT Scan ARDS Study Group. Intensive Care Med. 2000;26(8):1046–1056. doi:10.1007/s001340051317
5. Xirouchaki N, Kondili E, Prinianakis G, Malliotakis P, Georgopoulos D. Impact of lung ultrasound on clinical decision making in critically ill patients. Intensive Care Med. 2014;40(1):57–65. doi:10.1007/s00134-013-3133-3
6. Alqahtani J, Oyelade T, Sreedharan J, et al. Diagnostic and clinical values of non-cardiac ultrasound in COPD: a systematic review. BMJ Open Respir Res. 2020;7(1):e000717. doi:10.1136/bmjresp-2020-000717
7. Karthika M, Wong D, Nair SG, Pillai LV, Mathew CS. Lung Ultrasound: the Emerging Role of Respiratory Therapists. Respir Care. 2019;64(2):217–229. doi:10.4187/respcare.06179
8. Kappel C, Chaudhuri D, Hassall K, et al. Point-of-care ultrasound training for respiratory therapists: a scoping review. Can J Respir Ther. 2022;58:28–33. doi:10.29390/cjrt-2021-065
9. Wagner C. Loma Linda University incorporates lung ultrasound training in respiratory care program. Available from: https://news.llu.edu/academics/loma-linda-university-incorporates-lung-ultrasound-training-respiratory-care-program.
10. Mohammed A, Alshehri Z, Alqahtani J, et al. Respiratory care education in Saudi Arabia: national survey of local universities. Respir Care. 2021;66(Suppl 10):3610526.
11. Alotaibi G. Status of respiratory care profession in Saudi Arabia: a national survey. Ann Thorac Med. 2015;10(1):55–60. PMID: 25593609; PMCID: PMC4286847. doi:10.4103/1817-1737.146878
12. Arora S, Cheung AC, Tarique U, Agarwal A, Firdouse M, Ailon J. First-year medical students use of ultrasound or physical examination to diagnose hepatomegaly and ascites: a randomized controlled trial. J Ultrasound. 2017;20:199–204. doi:10.1007/s40477-017-0261-6
13. Koratala A, Segal MS, Kazory A. Integrating point-of-care ultrasonography into nephrology fellowship training: a model curriculum. Am J Kidney Dis. 2019;74:1–5. doi:10.1053/j.ajkd.2019.02.002
14. Watson K, Lam A, Arishenkoff S, et al. Point of care ultrasound training for internal medicine: a Canadian multi-centre learner needs assessment study. BMC Med Educ. 2018;18:217. doi:10.1186/s12909-018-1326-8
15. Brown GM, Otremba M, Devine LA, Gray C, Millington SJ, Ma IW. Defining competencies for ultrasound- guided bedside procedures: consensus opinions from Canadian physicians. J Ultrasound Med. 2016;35:129–141. doi:10.7863/ultra.15.01063
16. Price S, Via G, Sloth E, et al. Echocardiography practice, training and accreditation in the intensive care: document for the World Interactive Network Focused on Critical Ultrasound (WINFOCUS). Cardiovasc Ultrasound. 2008;6:49. doi:10.1186/1476-7120-6-49
17. Smallwood N, Matsa R, Lawrenson P, Messenger J, Walden A. A UK wide survey on attitudes to point of care ultrasound training amongst clinicians working on the Acute Medical Unit. Acute Med. 2015;14:158–164. doi:10.52964/AMJA.0523
18. Day J, Davis J, Riesenberg LA, et al. Integrating sonography training into undergraduate medical education: a study of the previous exposure of one institution’s incoming residents. J Ultrasound Med. 2015;34:1253–1257. doi:10.7863/ultra.34.7.1253
19. Anstey JE, Jensen TP, Afshar N. Point-of-care ultrasound needs assessment, curriculum design, and curriculum assessment in a large academic internal medicine residency program. South Med J. 2018;111(7):444–448. doi:10.14423/SMJ.0000000000000831
20. Filly R. Ultrasound: the stethoscope of the future, alas. Radiology. 1988;167(2):400. doi:10.1148/radiology.167.2.3282260
21. Soummer A, Perbet S, Brisson H, et al.; Lung Ultrasound Study Group. Ultrasound assessment of lung aeration loss during a successful weaning trial predicts postextubation distress. Crit Care Med. 40;2012:2064–2072. doi:10.1097/CCM.0b013e31824e68ae
22. Guitart C, Suárez R, Girona M, et al. Lung ultrasound findings in pediatric patients with COVID-19. Eur J Pediatr. 2021;180:1117–1123. doi:10.1007/s00431-020-03839-6
23. Trias-Sabrià P, Molina-Molina M, Aso S, et al. Lung ultrasound score to predict outcomes in COVID-19. Respir Care. 2021;66(8):1263–1270. doi:10.4187/respcare.08648
24. Swamy V, Brainin P, Biering-Sørensen T, Platz E. Ability of non-physicians to perform and interpret lung ultrasound: a systematic review. Eur J Cardiovasc Nurs. 2019;18(6):474–483. PMID: 31018658; PMCID: PMC6919316. doi:10.1177/1474515119845972
25. Liu RB, Donroe JH, McNamara RL, Forman HP, Moore CL. The practice and implications of finding fluid during point-of-care ultrasonography. JAMA Intern Med. 2017;177:1818–1825. doi:10.1001/jamainternmed.2017.5048
26. Student Handbook-Respiratory care program (page 8, 21-course description). Dhahran: Prince Sultan Military College of Health Sciences. Available from: http://www.psmchs.edu.sa/wp-content/uploads/2020/09/Respiratory-Care-Student-Handbook.pdf.
27. Heldeweg M, Vermue L, Kant M, et al. The impact of lung ultrasound on clinical-decision making across departments: a systematic review. Ultrasound j. 2022;14(1):5. doi:10.1186/s13089-021-00253-3
28. See KC, Ong V, Wong SH, et al. Lung ultrasound training: curriculum implementation and learning trajectory among respiratory therapists. Intensive Care Med. 2016;42:63–71. doi:10.1007/s00134-015-4102-9
29. Chalumeau-Lemoine L, Baudel JL, Das V, et al. Results of short-term training of naïve physicians in focused general ultrasonography in an intensive-care unit. Intensive Care Med. 2009;35(10):1767–1771. doi:10.1007/s00134-009-1531-3
30. Uppalapati A, Oropello J, Mukkera SR, Jamkhana ZA, DelGiudice R, Sherman B. Efficacy of a training program to achieve competence in lung and pleural ultrasound. Chest. 2011;140(4):1033. doi:10.1378/chest.1119868
31. Mukherjee T, Mehta S, Walker D. The development of an in-house thoracic ultrasound teaching programme on a UK intensive care unit. Intensive Care Med. 2011;37:1. doi:10.1007/s00134-010-2034-y
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.