Back to Journals » Clinical Ophthalmology » Volume 19
Rotational Stability After Implantation of an Aspheric Toric Monofocal IOL with a Double C-Loop Haptic Design in Normal and High Axial Lengths
Authors Ang RET ![]() , Tañá-Rivero P, Pastor-Pascual F, Stodulka P
, Tañá-Rivero P, Pastor-Pascual F, Stodulka P ![]() , Slovak M
, Slovak M ![]() , Tetz M, Fischinger I, Cazal J, Gessa M, Ibarz-Barberá M, Holland D, Groneberg T
, Tetz M, Fischinger I, Cazal J, Gessa M, Ibarz-Barberá M, Holland D, Groneberg T
Received 26 March 2025
Accepted for publication 14 July 2025
Published 19 July 2025 Volume 2025:19 Pages 2393—2403
DOI https://doi.org/10.2147/OPTH.S530593
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Robert Edward T Ang,1 Pedro Tañá-Rivero,2 Francisco Pastor-Pascual,3 Pavel Stodulka,4,5 Martin Slovak,4 Manfred Tetz,6 Isaak Fischinger,7 Jorge Cazal,8 María Gessa,9 Marta Ibarz-Barberá,10 Detlef Holland,11 Thomas Groneberg12
1Asian Eye Institute, Makati City, Philippines; 2Oftalvist, Alicante, Spain; 3Oftalvist, Valencia, Spain; 4GEMINI Eye Clinic, Zlin, Czech Republic; 5Third Faculty of Medicine, Charles University, Prague, Czech Republic; 6Berlin Eye Research Institute (BERI), Berlin, Germany; 7Berlin Eye Research Institute (BERI), Wittenberg, Germany; 8Miranza IMO Barcelona, Barcelona, Spain; 9Miranza Virgen de Luján, Sevilla, Spain; 10Oftalvist, Madrid, Spain; 11Augenzentrum ONE, Kiel, Germany; 12Augenzentrum Erding, Erding, Germany
Correspondence: Robert Edward T Ang, Asian Eye Institute, 8th Floor PHINMA Plaza, Rockwell Center, Makati City, Philippines, Email [email protected]
Purpose: This study focuses on the analysis of the rotational stability after implantation of a biconvex aspheric toric monofocal intraocular lens (IOL) with a double C-loop haptic-design in eyes with normal versus high axial lengths.
Methods: This was a prospective comparative study including 150 eyes with corneal astigmatism (≥ 0.75D) implanted with the biconvex aspheric monofocal PODEYE toric IOL and assessed up to 1 year after surgery. From these 150 eyes, 81 and 69 eyes belonged to normal (≤ 23.9mm) and high (≥ 24mm) axial lengths, respectively. About 4– 6 and 11– 13 months postoperatively, refraction and rotational stability of the PODEYE toric IOL were evaluated to find possible differences among both groups.
Results: At the last postoperative-visit, 74.07% of eyes were within ± 0.50D and 95.06% of eyes were within ± 1.00D of the target-refraction for the normal group and 92.75% and 100% for the high axial length group, respectively. For the normal group, 77.78% and 96.30% of eyes had a postoperative refractive cylinder of ≤ 0.50D and ≤ 1.00D, respectively; and for the high axial length group these percentages were 84.05% and 100%, respectively. About 81.84% of eyes in the normal and 94.20% of eyes in the high axial length group were < 5 degrees of the intended axis. The mean IOL rotation was 2.93 ± 2.48 degrees in the normal axial length group, and 2.17 ± 1.73 degrees in the high axial length group. Based on the mixed ANOVA results, there is no evidence of a significant difference in IOL rotation over time, nor is there evidence that axial length plays a statistically significant role in rotational stability between 4– 6 and 11– 13 months postsurgery. Both groups exhibited similar and stable rotation outcomes.
Conclusion: Our results reveal that the biconvex aspheric monofocal PODEYE toric IOL with double C-loop haptic-design shows excellent rotational stability without significant differences between eyes with normal and high axial lengths.
Keywords: astigmatism, rotation, stability, monofocal toric, double C-loop, intraocular lens
Introduction
It has been reported recently in a sample of 110, 468 eyes undergoing cataract surgery that 78% of eyes had preoperative corneal astigmatism of ≥0.5 dioptres (D), 42% ≥ 1.0 D, 21% ≥ 1.5 D and 11% ≥ 2.0 D.1 The correction of this preoperative existing astigmatism during cataract surgery should be considered by surgeons in their clinical armamentarium. A recent systematic review and meta-analysis recommend that patients undergoing age-related cataract surgery who show regular corneal astigmatism should receive a toric intraocular lens (IOL) if they want to be spectacle independent for distance vision after surgery.2
It should be considered that stability is one of the most important challenges after toric IOL implantation and to reduce postoperative rotation of the lens it is crucial for reducing postoperative residual astigmatism. The amount of postoperative IOL rotation can be affected by an array of factors including capsulorhexis size, axial length, and the IOL material and design, which in turn influences rotational stability.3–5 Taking into account the wide range of factors that can contribute to a possible misalignment, maximising the intrinsic rotational stability of the IOL is an important component in optimising visual outcomes.6
The biconvex aspheric monofocal PODEYE toric IOL with a double C-loop and posterior angulated haptic design (Beaver-Visitec International Inc., Waltham, USA) is a lens, which has been evaluated in different clinical studies, both retrospective7 and prospective,8,9 concluding that this model offers high rotational stability with good visual and refractive outcomes. One factor which has been considered to be a possible cause of postoperative rotation is the presence of high axial length in high myopic eyes due to the large capsular bags. In the initial publications of our trial with this IOL8,9 we have not analysed this factor and whether there is a possible correlation between axial length and postoperative rotation of this IOL model. Therefore, the main purpose of this article is to evaluate the rotational stability of the PODEYE toric IOL in cataract eyes with normal and high preoperative axial lengths and to compare their results during 1 year of follow-up.
Methods
This was a multicentric, prospective, open-label study carried out at 10 centres: the Asian Eye Institute in Makati City (Philippines), Gemini Eye Clinic in Zlin (Czech Republic), IMO in Barcelona (Spain), Virgen de Lujan in Sevilla (Spain), Augenzentrum Erding in Erding (Germany), Augentagesklinik Spreebogen in Berlin (Germany), Medicum Wittenberg in Wittenberg (Germany), and Oftalvist in Madrid, Valencia and Alicante (Spain). The study was approved by the respective Ethics Committees: SCMC-AEI Ethics Review Committee (Asian Eye Institute), Eticka Komise Ocni Kliniky Gemin (Czech Republic), Ethik-Kommission der Bayerischen Landesärztekammer (Germany), Ärztekrammer Berlin (Germany), Ärztekammer Sachsen-Anhalt (Germany), and Hospital Clínico San Carlos (Oftalvist, IMO and Virgen de Lujan). The study adhered to the tenets of the Declaration of Helsinki with all patients providing informed consent, and registered (NCT04778501, NCT04866719, NCT04744467 and NCT04987216), and inclusion and exclusion criteria were the same as previously reported8,9 (inclusion: cataract patients ≥50 years-old, corneal astigmatism of ≥0.75 D and ≤4.25 D in both eyes; and exclusion: degenerative visual disorders or previous intraocular or corneal surgery, among other criteria).
Eyes were implanted with the aspheric monofocal PODEYE toric IOL made of GFY material (hydrophobic acrylic with refractive index of 1.52 and Abbe number of 42). It presents a double C-loop and a posterior-angulated haptic design with an 11.40-mm overall diameter. The optics of the lens is biconvex aspheric (with −0.11 μm for 5 mm) and toric on the posterior surface with 6.00 mm optical diameter. The IOL is available in different spherical powers ranging from +6.00 D to +30.00 D in 0.50 D, and cylindrical powers at the IOL plane of 1.00, 1.50, 2.25, 3.00, 3.75, 4.50, 5.25 and 6.00 D. All patients were operated for age-related cataracts with standard phacoemulsification cataract surgery through a 2.2 mm incision and a 5.5 mm diameter target for capsulorhexis or femtosecond laser-assisted capsulotomy followed by PODEYE toric IOL implantation. Optical biometry was obtained using the IOLMaster device (Carl Zeiss Meditec AG, Jena, Germany), and the IOL power (sphere and cylinder), mainly calculated using the Barrett toric online calculator, was chosen to achieve a residual spherical equivalent close to emmetropia, between –0.2 D and 0.1 D, and the lowest residual cylinder possible. The eyes of our cohort were divided into 2 groups, based on their preoperative axial lengths as follows: normal group, with an axial length of ≤23.9 mm, and high group with an axial length ≥24.00 mm.
At 4–6 and 11–13 months, we measured subjective refraction with sphere, cylinder and axis for each eye. A double-angle plot tool developed by Abulafia et al10 was used for the astigmatism analysis based on the preoperative corneal astigmatism obtained from the IOLMaster optical biometer and the postoperative subjective refraction obtained at the two follow-up visits. The absolute rotational stability, with mean, standard deviation and range, of the PODEYE toric IOLs was obtained between the baseline, and 4–6 and 11–13 months post-surgery. Specifically, in order to determine the stability of the IOLs after implantation, the IOL orientation was recorded at baseline as the intended surgical position during surgery using a photograph through the surgery microscope or within 1 hour post-surgery using a photograph through a slit lamp. The IOL orientation at the 2 post-surgery follow-up visits was recorded with a dilated retroilluminated photograph using the slit-lamp.
SPSS software was used for statistical analysis. For descriptive statistics and comparison between groups, a non-parametric Mann–Whitney U-test was used (only age was normally distributed). For rotation analysis, a mixed-design (split-plot) repeated-measures ANOVA was performed to examine the effect of time (4–6 versus 11–13 months post-surgery) on IOL rotation and to assess whether this effect was influenced by axial length (normal and high groups). In this design, time is the within-eye factor (the same eyes measured at 2 different time points), and axial length group is the between-eyes factor (2 independent groups based on axial length). The ANOVA evaluates whether there is a significant main effect of time, whether there is a significant main effect of axial length group, and whether there is an interaction between time and axial length group on the measured IOL rotation. A P value of 0.05 or less was considered statistically significant.
Results
A total of 150 eyes from 93 patients implanted with the PODEYE toric IOL were included in the study as part of a previous clinical study.8,9 Eighty-one eyes belonged to the normal axial length group (≤23.9 mm) and 69 eyes to the high axial length group (≥24 mm). Table 1 shows the demographic characteristics of the cohort (mean, standard deviation and range) and specific variables are distributed between normal and high axial length groups. Both groups matched in age and there were statistically significant differences for the other parameters (P < 0.05).
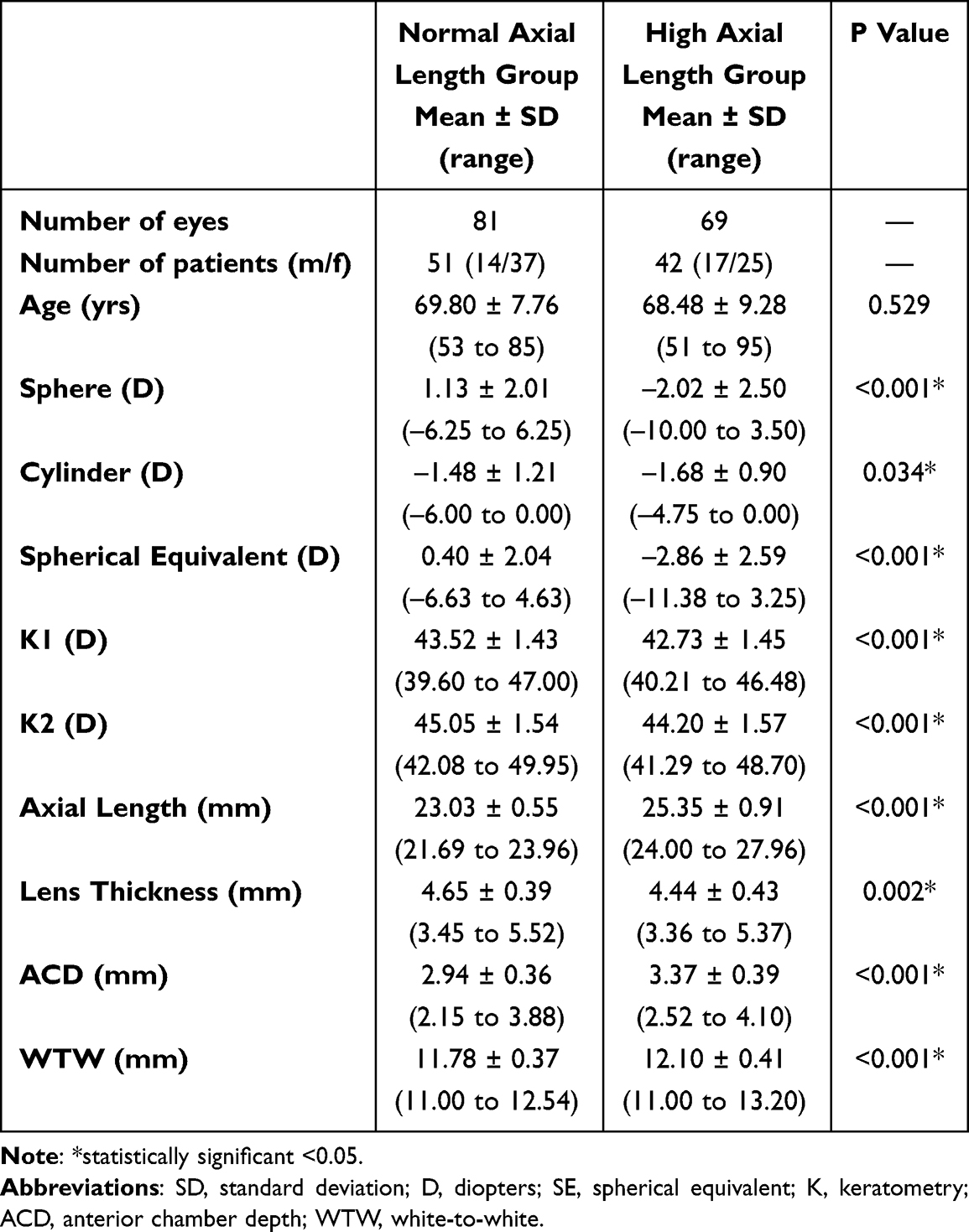 |
Table 1 Preoperative Demographic Characteristics of Patients Included in Both Study Groups |
Refractive Accuracy and Astigmatism Analysis
Figure 1 shows the refractive accuracy of the surgical procedure for the spherical equivalent for the normal axial length group (top) and high axial length group (bottom). For the normal axial length group, at 4–6 months 79.01% of eyes were within ±0.50 D and 95.06% of eyes were within ±1.00 D, and at 11–13 months these values were similar, 74.07% and 95.06%, respectively. For the high axial length group, the percentages at 4–6 months were 91.30% and 100% for ±0.50 D and ±1.00 D, respectively, and at 11–13 months were 92.75% and 100%, respectively. Figure 2 shows the refractive accuracy of the surgical procedure for refractive cylinder for the normal axial length group (top) and high axial length group (bottom). For the normal axial length group, at 4–6 months, 74.07% and 97.53% of eyes had a postoperative refractive cylinder of ≤0.50 D and ≤1.00 D, respectively, and at 11–13 months these values were also similar, 77.78% and 96.30%, respectively. For the high axial length group, the percentages at 4–6 months were 76.81% and 100% for ≤0.50 D and ≤1.00 D, respectively, and at 11–13 months were 84.05% and 100%, respectively.
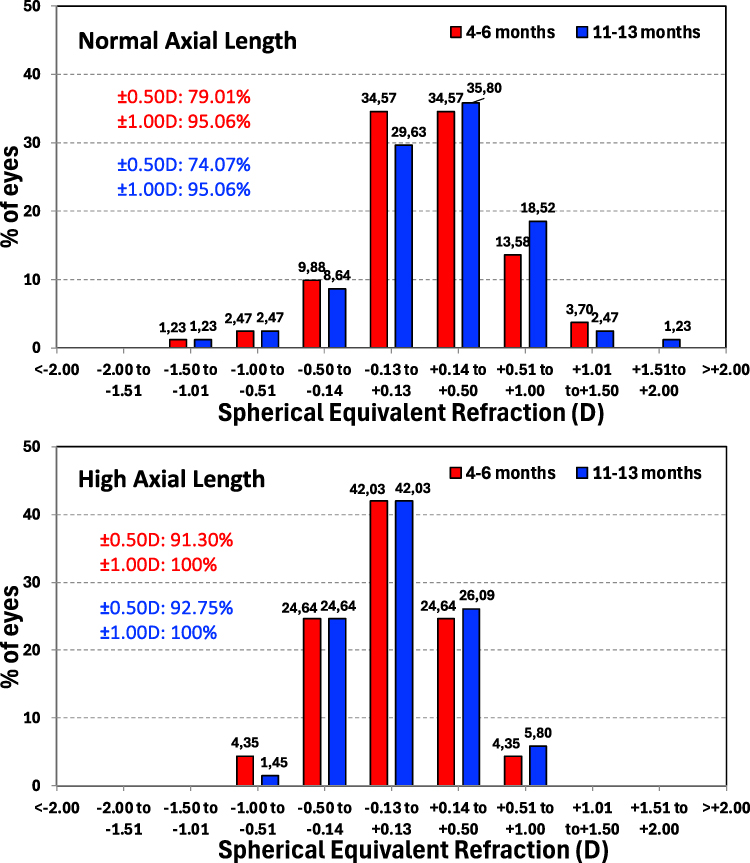 |
Figure 1 Spherical equivalent histograms showing accuracy at 4–6 and 11–13 months for the normal axial length group (top) and the high axial length group (bottom). |
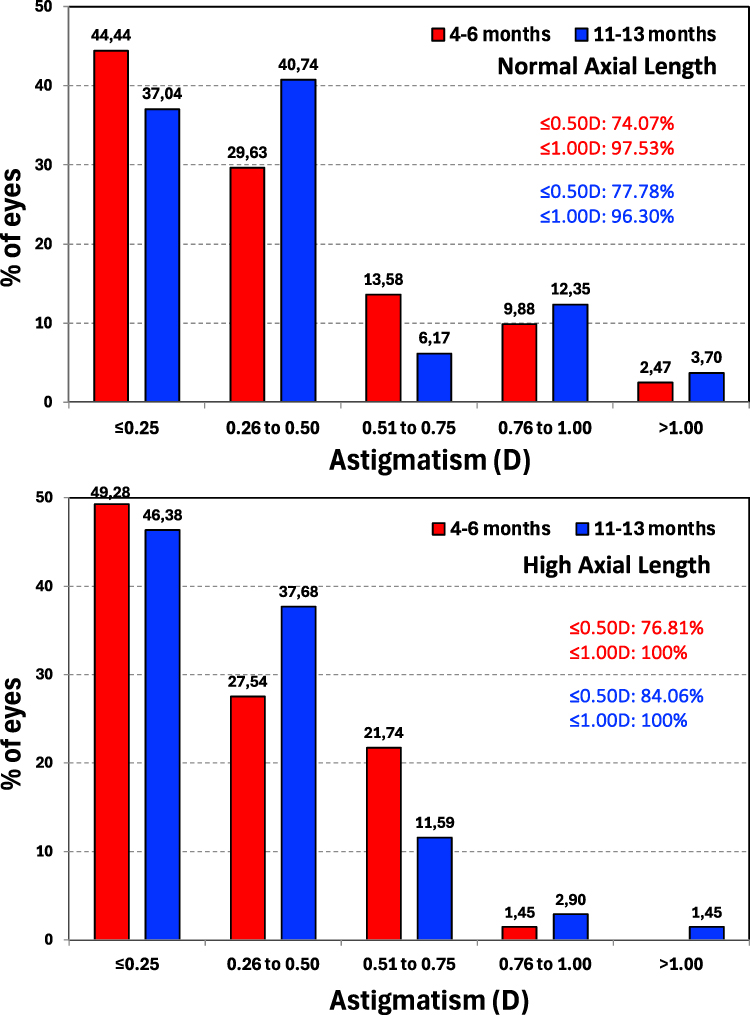 |
Figure 2 Refractive cylinder histograms showing accuracy at 4–6 and 11–13 months for the normal axial length group (top) and the high axial length group (bottom). |
Table 2 shows the mean refractive spherical equivalent and refractive cylinder values for both groups at the two follow-up visits. Less than or about a quarter of a dioptre was found for the mean refractive spherical equivalent and less than half a dioptre for the refractive cylinder in both groups at the two follow-up visits. Figure 3 shows the double angle plots of preoperative corneal astigmatism and refractive astigmatism postoperatively at 4–6 and 11–13 months postsurgery for normal and high axial lengths groups. This figure revealed that there is a correction of the astigmatism postsurgery at the two follow-up periods, which is similar in both groups.
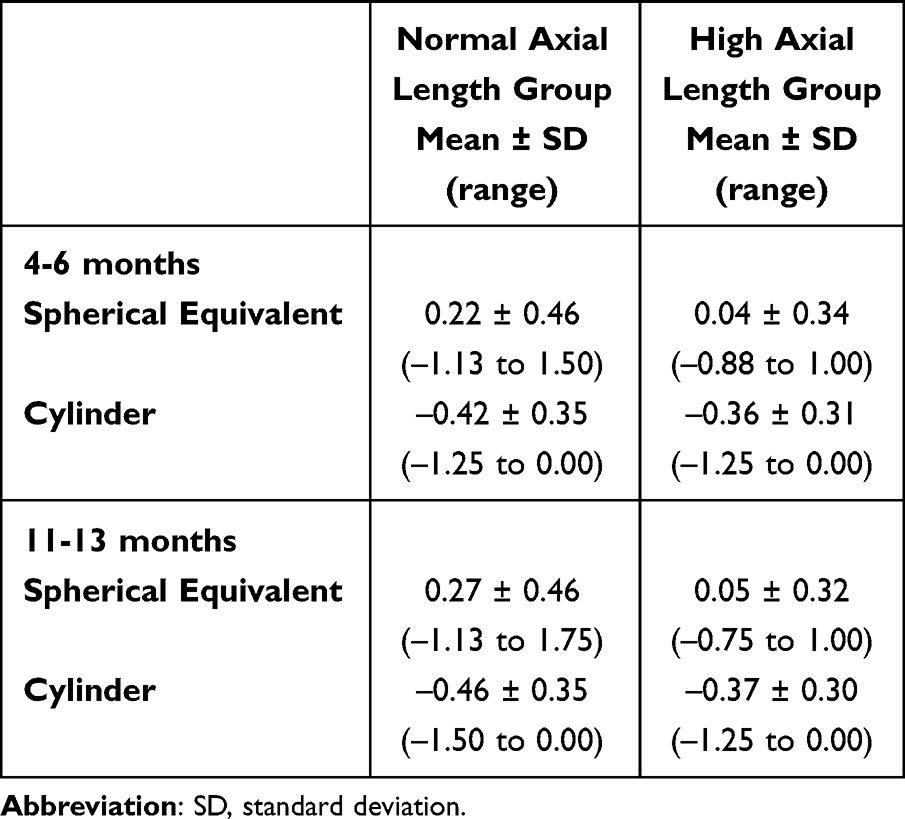 |
Table 2 Mean Values of Spherical Equivalent and Refractive Cylinder of Both Study Groups at 4–6 and 11–13 Months Postoperatively |
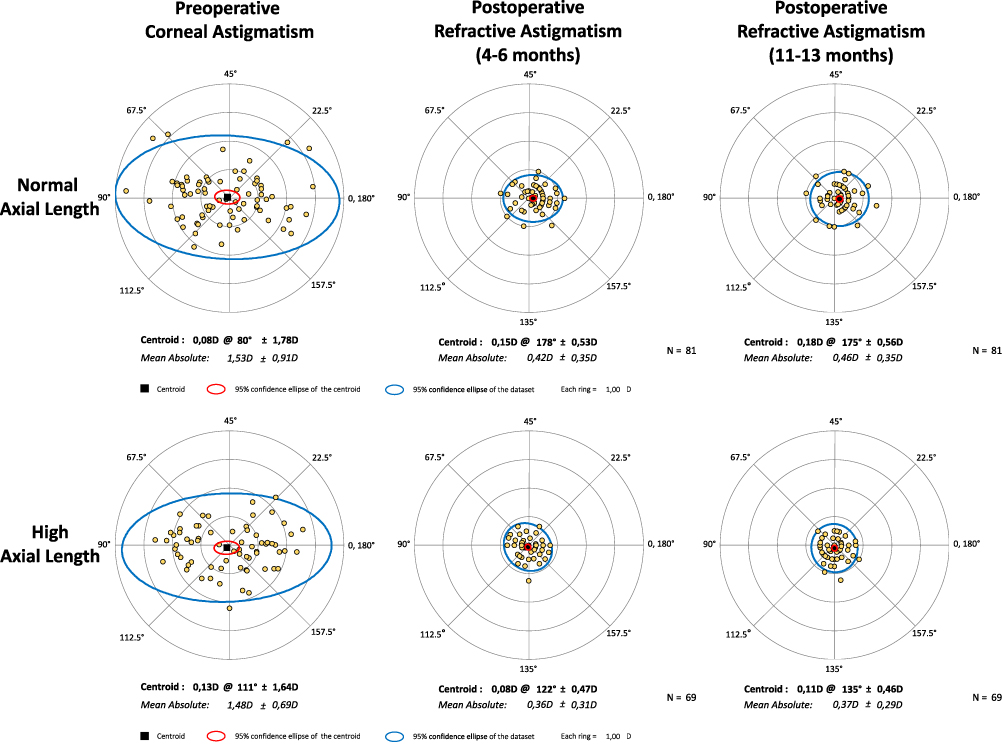 |
Figure 3 Double-angle plots for preoperative corneal astigmatism and postoperative refractive astigmatism at 4–6 and 11–13 months of follow-up for the normal axial length group (top) and the high axial length group (bottom). Centroids, mean absolute values with standard deviations, 95% confidence ellipse of the centroid and 95% confidence ellipse of the dataset are also shown. |
Rotational Stability and Relationship with Axial Length
Table 3 shows the mean values of postoperative rotational stability of both study groups and the whole sample at the two follow-up visits. In all cases mean values were less than 3 degrees and for the whole sample mean values were about 2 degrees and half for the two post-operative visits. Figure 4 shows the histogram distribution of rotation from 0 to 10 degrees for the normal and high axial length groups. All eyes in both groups were noted to have an IOL rotation of 10 degrees or less. Only one eye in the normal axial group showed 10 degrees of rotation at the 11–13 months of follow up. At the last follow-up visit 37.04% eyes and 31.88% eyes showed no rotation or 1 degree of rotation in the normal and high axial length groups, respectively. The percentages for rotation ≤5 degrees at this visit were 81.48% and 94.20%, for the normal and high axial length groups, respectively.
 |
Table 3 Mean Values of Postoperative Rotational Stability of Both Study Groups and the Whole Sample at 4–6 and 11–13 Months Postoperatively |
 |
Figure 4 Postoperative rotational stability histogram for the normal axial length group (top) and the high axial length group (bottom)at 4–6 and 11–13 months postoperatively. |
In order to display the relationship between rotational stability with axial length, several scatterplots were plotted. Figure 5 illustrates the relationship with axial length for both study groups at 4–6 and 11–13 months of follow up. This figure shows a weak relationship between rotation and axial length. The ANOVA test revealed, for the main effect of time (within-eyes), that there is no statistically significant difference in mean IOL rotation between 4–6 and 11–13 months when considering the whole sample (P = 0.769). For the main effect of the group (between-eyes), although normal axial length group had slightly higher rotation means, the difference does not reach significance (P = 0.082), thus, overall, there is no statistically significant difference in rotation based solely on axial length group. And considering the interaction (time per axial length group) there is no significant interaction between both variables. In other words, any change from 4–6 to 11–13 months does not differ significantly between normal and high axial length groups (P = 0.138).
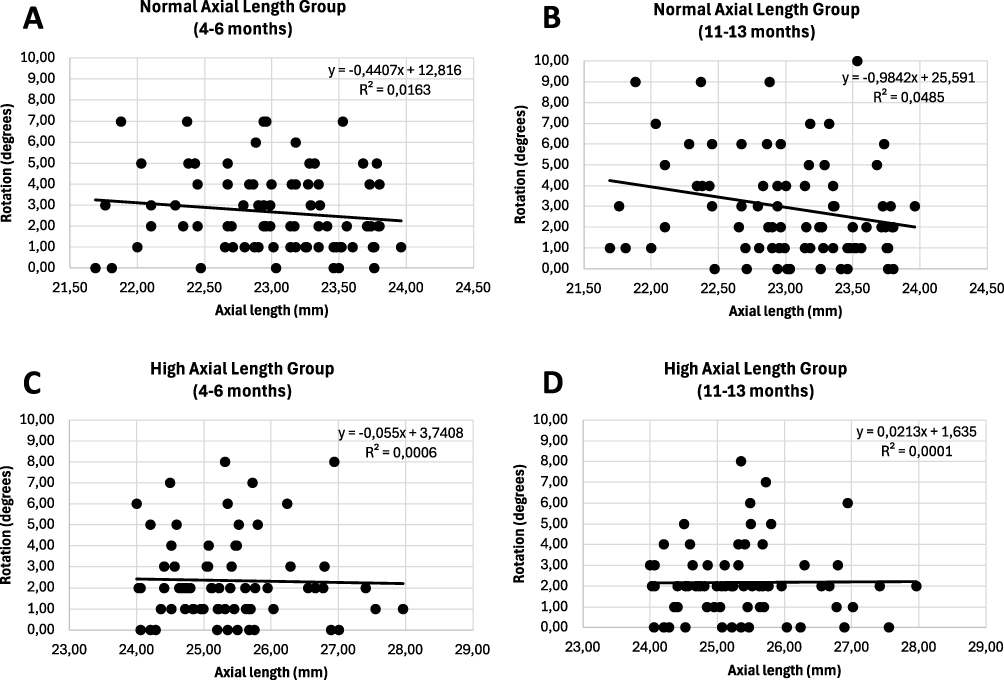 |
Figure 5 Scatterplot showing the relationship between rotation (degrees) and axial length (mm) for the normal axial length group ((A) 4–6 months, and (B) 11–13 months) and the high axial length group ((C): 4–6 months, and (D) 11–13 months). Linear equations and R2 values are shown in the different graphs. |
Discussion
We have performed a clinical study to analyse the rotational stability of the PODEYE toric IOL in patients with age-related cataracts and pre-existing regular corneal astigmatism to discover any possible relationship of this parameter with the axial length of the eye. Our outcomes revealed good rotational stability of the PODEYE toric IOL being attributed to the double C-loop haptic design created to provide good postoperative stability after its implantation.
The refractive accuracy in terms of spherical equivalent and cylinder was good (see Table 2 for the mean values obtained both for spherical equivalent and cylinder) with 95.06% and 100% of eyes within ±1.00D of the target refraction for the normal and high axial length groups, respectively (Figure 1). The percentages for postoperative refractive cylinder were 96.30% and 100% of ≤1.00D for both groups, respectively (Figure 2). Figure 3 also shows the correction of the astigmatism post-surgery at the two follow-up periods, which is similar in both groups (note the concentration of the points to 0,0 coordinates in the four graphs post-surgery). Our results in terms of refractive accuracy are in agreement with the outcomes previously published regarding this IOL model. For example, Chassain et al7 in a retrospective study with 136 cataract eyes at 4–6 months post-surgery with target refraction of emmetropia or mild to moderate myopia for monovision obtained a mean spherical equivalent of –0.30 ± 0.54D with 70% and 92% of eyes within ±0.50D and ±1.00D of the target refraction. Prospectively, Ang et al8 at the same follow-up time with 94 eyes, found 78.2% and 98.9% of eyes within ±0.50 D and ±1.00D, respectively, and with 236 eyes at 11–13 months of follow-up these values were 74.6% and 95.8%, respectively.9 For the refractive cylinder, Chassain et al7 found that 84.1% and 98.1% of eyes showed a refractive cylinder of ≤0.50D and ≤1.00D, respectively; Ang et al8 found 76.5% and 98.8% of eyes, respectively, and Ang et al9 78% and 97.5% of eyes, respectively.
Focusing now on the main purpose of the study, we have obtained good rotational stability outcomes both for the whole sample and separating the eyes as a function of their axial length. In general, all values were less than 3 degrees during the entire follow-up (see Table 3 for detailed values as function of the group and post-operative period). Specifically, considering the whole sample the mean values at both periods were about 2 and a half degrees. In this sense, Li et al6 in a recent publication (systematic review and single-arm meta-analysis study of 4863 eyes in 51 studies) analysed the rotational stability of different toric IOLs available in the market according to lens model and haptic design, reporting that the pooled mean absolute rotation for all the lenses was 2.36 degrees (with a 95% CI: 2.08–2.64), a value which agrees with that found in our cohort. It is interesting to note that the high percentage of eyes in our sample with a rotation ≤5 degrees at the last postoperative visit: 81.48% and 94.20%, for the normal and high axial length groups, respectively (Figure 4). Previous publications with this IOL also revealed stable outcomes in terms of rotation. Chassain et al7 found that more than 85% of eyes rotated ≤3 degrees, with 58.0% of eyes rotating clockwise and 42.0% of eyes rotating counterclockwise. The mean axial length of this cohort was 23.81 ± 1.34 mm, ranging from 21.13 to 28.71 mm (mean age of 74 ± 7.9 years) and the mean rotation value was 2.05 ± 2.17 degrees, ranging from 0 to 15 degrees. Our preliminary studies on the same lens supported these good outcomes, with 97.87%8 and 98.56%9 of eyes having a rotation of <10 degrees. In the first study,8 94 eyes with a mean axial length of 23.90 ± 1.32 mm showed a mean rotation value of 1.22 ± 2.21 degrees, ranging from 0 to 10 degrees, at 4–6 months; and in the second one,9 118 eyes with a mean axial length of 24.03 ± 1.40 mm showed a mean rotation value of 2.52 ± 2.59 degrees, from 0 to 12 degrees, at 11–13 months. The ISO11979-7:2018 indicates that the absolute value of rotation in toric IOL should be <10 degrees in 90% of the eyes implanted.11 In our series of eyes, the outcomes obtained broadly fulfill this criterion since our percentage for this value was 100% in both groups (see Figure 4). The POD platform of this toric IOL shows a double C-loop with symmetrical quadripod design with 2-by-2 oppositely oriented haptics allowing 4 contact points for fixing the IOL in the capsular bag. Bozukova et al12 carried out an analysis of the behaviour of the double C-loop platform using a computer simulation, under in vivo (animal) and in vitro conditions, showing the benefit of the haptic design in ensuring axial and centration stability. It should be noted that one characteristic of this platform is good manoeuvrability, since the IOL allows rotation in both senses (clockwise and counterclockwise). This possibility facilitates the proper alignment of the toric IOL with the desired axis during the surgical procedure.
Axial length has traditionally been considered to be an important factor contributing to the early postoperative rotation of lenses after cataract surgery,13–15 however no significant correlation has been found between axial length and rotation in other studies.16–20 Guo et al16 in their study of 39 eyes (21 with emmetropia or low myopia and 18 with high myopia) reported an equal astigmatism-correction efficiency and rotational stability in eyes with normal versus high myopia after implantation of the AcrySof IQ toric IOL. It should be noted, for example, that Chassain et al7 found good rotational stability for the PODEYE toric IOLs, even for the 25% of eyes with an axial length greater than 24.5 mm. He et al19 retrospectively assessed 64 eyes with long axial length (≥25 mm) implanted with the TECNIS toric IOL and reported that there was no correlation between IOL rotation and axial length (P = 0.876). Brar et al20 recently, retrospectively compared the rotational stability in 113 eyes implanted with the HOYA Vivinex toric monofocal XY1A-SP IOL, of which 62 and 52 eyes belonged to normal (≤23.9 mm) and high (≥24 mm) axial length, respectively. They assessed these eyes at 1 week and 3 months postoperatively and found that all eyes in the normal and 96.15% eyes in the high myopia group were <5 degrees of the intended axis, without any significant correlation between axial length with 1-week postoperative rotation values. These authors concluded that there were no significant differences in postoperative rotational stability between eyes of normal and high axial length irrespective of the preoperative axial length values. Our results, based on the mixed ANOVA results, show that there is no evidence of a significant difference in IOL rotation over time, nor is there evidence that axial length (≤23.9 mm versus <24 mm) plays a statistically significant role in rotational stability between 4–6 and 11–13 months post-surgery. We may observe Figure 5, which shows different scatterplots of the relationship between rotation of the toric IOL with axial length for both groups at the two different follow-up periods. Then, both groups, independent of the preoperative axial length, exhibited similar and stable rotation outcomes.
Conclusions
This study analysed the rotational stability outcomes of the biconvex aspheric monofocal PODEYE toric IOL with a double C-loop haptic design in eyes with pre-existing corneal astigmatism as a function of the axial length submitted to cataract surgery at 1 year of follow-up. Our study shows the good rotational stability of this lens both in normal and high axial length eyes, and reveals that, in our cohort, there is no evidence that axial length plays a significant role in rotational stability after implantation of this IOL model.
Data Sharing Statement
Data of this trial are not available for sharing.
Funding
This trial was funded by Beaver-Visitec International, Inc. [BVI].
Disclosure
Robert Edward T. Ang declares grants for studies from Acevision, Inc., Acufocus, Inc., Bausch&Lomb, Inc., Beaver-Visitec International Inc., Glaukos Corp., Hoya, Ivantis, Inc., Johnson&Johnson Vision, Spyglass, STAAR Surgical and Vialase. Pedro Tañá-Rivero declares grants for studies from Alcon Healthcare SA, AST Products Inc., Beaver-Visitec International Inc., Carl Zeiss, Hoya Surgical AG, Humanoptics Holding AG, Johnson & Johnson Surgical Vision, Staar Surgical AG and Vialase Inc. Francisco Pastor-Pascual declares grants for studies from Alcon Healthcare SA, Beaver-Visitec International Inc., Carl Zeiss, Hoya Surgical AG and Humanoptics Holding AG. Pavel Stodulka declares grants for studies from Bausch and Lomb. Marta Ibarz-Barberá declares grants for studies from Beaver-Visitec International Inc., Cutting-Edge, ELIOS Vision Inc., and Hoya Surgical AG. The authors report no other conflicts of interest in this work.
References
1. Day AC, Dhariwal M, Keith MS, et al. Distribution of preoperative and postoperative astigmatism in a large population of patients undergoing cataract surgery in the UK. Br J Ophthalmol. 2019;103:993–1000. doi:10.1136/bjophthalmol-2018-312025
2. Kessel L, Andresen J, Tendal B, Erngaard D, Flesner P, Hjortdal J. Toric intraocular lenses in the correction of astigmatism during cataract surgery: a systematic review and meta-analysis. Ophthalmology. 2016;123(2):275–286. doi:10.1016/j.ophtha.2015.10.002
3. Kaur M, Shaikh F, Falera R, Titiyal JS. Optimizing outcomes with toric intraocular lenses. Indian J Ophthalmol. 2017;65:1301–1313. doi:10.4103/ijo.IJO_810_17
4. Patnaik JL, Kahook MY, Berdahl JP, et al. Association between axial length and toric intraocular lens rotation according to an online toric back-calculator. Int J Ophthalmol. 2022;15:420–425. doi:10.18240/ijo.2022.03.08
5. Wu J, Yang C, Yin Y, Liu L, Wang H. Impact of material and lens design on repositioning surgery of toric intraocular lenses: a single-arm meta-analysis. J Ophthalmol. 2022;2022:6699596. doi:10.1155/2022/6699596
6. Li ES, Vanderford EK, Xu Y, Kang PC. Rotational stability of toric intraocular lenses by lens model and haptic design: systematic review and single-arm meta-analysis. J Cataract Refract Surg. 2024;50(9):976–984. doi:10.1097/j.jcrs.0000000000001486
7. Chassain C, Hallak MK, Lesaffre M. Rotational stability and clinical outcomes after implantation of a new monofocal toric intraocular lens with double C-loop design. J Fr Ophtalmol. 2023;46:571–580. doi:10.1016/j.jfo.2022.07.005
8. Ang RET, Tañá-Rivero P, Pastor-Pascual F, Stodulka P, Tetz M, Fischinger I. Visual and refractive outcomes after bilateral implantation of a biconvex aspheric toric monofocal intraocular with a double C-loop haptic design. Clin Ophthalmol. 2023;17:2765–2776. doi:10.2147/OPTH.S432598
9. Ang RET, Tañá-Rivero P, Pastor-Pascual F, et al. One-year clinical outcomes following aspheric toric monofocal IOL with a double C-loop haptic design implantation. Clin Ophthalmol. 2024;18:3515–3525. doi:10.2147/OPTH.S494313
10. Abulafia A, Koch DD, Holladay JT, Wang L, Hill W. Pursuing perfection in intraocular lens calculations: IV. Rethinking astigmatism analysis for intraocular lens-based surgery: suggested terminology, analysis, and standards for outcome reports. J Cataract Refract Surg. 2018;44:1169–1174. doi:10.1016/j.jcrs.2018.07.027
11. ISO 11979-7:2018 ophthalmic implants — intraocular lenses — part 7: clinical investigations. 2018.
12. Bozukova D, Werner L, Mamalis N, et al. Double-C loop platform in combination with hydrophobic and hydrophilic acrylic intraocular lens materials. J Cataract Refract Surg. 2015;41(7):1490–1502. doi:10.1016/j.jcrs.2014.10.042
13. Miyake T, Kamiya K, Amano R, Iida Y, Tsunehiro S, Shimizu K. Long-term clinical outcomes of toric intraocular lens implantation in cataract cases with preexisting astigmatism. J Cataract Refract Surg. 2014;40:1654–1660. doi:10.1016/j.jcrs.2014.01.044
14. Shah GD, Praveen MR, Vasavada AR, Vasavada VA, Rampal G, Shastry LR. Rotational stability of a toric intraocular lens: influence of axial length and alignment in the capsular bag. J Cataract Refract Surg. 2012;38:54–59. doi:10.1016/j.jcrs.2011.08.028
15. Zhu X, He W, Zhang K, Lu Y. Factors influencing 1-year rotational stability of AcrySof toric intraocular lenses. Br J Ophthalmol. 2016;100:263–268. doi:10.1136/bjophthalmol-2015-306656
16. Guo T, Gao P, Fang L, Guo L, Fan Y, Liu C. Efficacy of toric intraocular lens implantation in eyes with high myopia: a prospective, case-controlled observational study. Exp Ther Med. 2018;15:5288–5294. doi:10.3892/etm.2018.6102
17. Tataru CP, Dogaroiu AC, Tataru CI, Dogaroiu C. Enhancing rotational stability of toric intraocular lenses using a type 2l cionni capsular tension ring in patients with high myopia. J Cataract Refract Surg. 2019;45:1219–1221. doi:10.1016/j.jcrs.2019.05.045
18. Zhu X, Meng J, He W, Rong X, Lu Y. Comparison of the rotational stability between plate-haptic toric and c-loop haptic toric IOLs in myopic eyes. J Cataract Refract Surg. 2020;46:1353–1359. doi:10.1097/j.jcrs.0000000000000259
19. He S, Chen X, Wu X, Ma Y, Yu X, Xu W. Early-stage clinical outcomes and rotational stability of TECNIS toric intraocular lens implantation in cataract cases with long axial length. BMC Ophthalmol. 2020;20:204. doi:10.1186/s12886-020-01465-2
20. Brar S, Ganesh S, Karegowda M. Clinical outcomes and rotational stability after implantation of a monofocal toric intraocular lens with textured haptics in normal vs high axial lengths. J Cataract Refract Surg. 2024;50:718–723. doi:10.1097/j.jcrs.0000000000001429
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Visual and Refractive Outcomes After Bilateral Implantation of a Biconvex Aspheric Toric Monofocal Intraocular with a Double C-Loop Haptic Design
Ang RET, Tañá-Rivero P, Pastor-Pascual F, Stodulka P, Tetz M, Fischinger I
Clinical Ophthalmology 2023, 17:2765-2776
Published Date: 20 September 2023
Comparing Rotational Stability Over Time Between Four Monofocal Toric Intraocular Lenses
Hoffmann P, Potvin R, Anello RD, Hengerer F, Auffarth G, Guldenfels Y, Bertelmann E, Ruiz Mesa R, Fischinger I, Krawczyk S, Seitz B, Antolin-Garcia D, Schmickler S, Hoffart L, Kohnen T, Relucio AS
Clinical Ophthalmology 2025, 19:1345-1355
Published Date: 23 April 2025
Double C-Loop Haptic Lenses Are Rotationally Stable – A Systematic Review
Daya S, Chassain C, Pagnoulle C
Clinical Ophthalmology 2025, 19:2259-2269
Published Date: 12 July 2025
Clinical Outcomes of a Multicenter Study Following Implantation of an Isofocal Optic IOL with Double C-Loop Haptics
Daya S, Akahoshi T, Bosc C, Mouchel R, Chassain C, Van Acker E, Di Maria A, Fogagnolo P
Clinical Ophthalmology 2025, 19:3121-3131
Published Date: 2 September 2025
Photic Phenomena and Quality of Vision Following Aspheric Toric Monofocal IOL with a Double C-Loop Haptic Design Implantation
Ang RET, Tañá-Rivero P, Pastor-Pascual F, Stodulka P, Slovak M, Tetz MR, Fischinger I, Gessa-Sorroche M, Ibarz-Barberá M, Groneberg T
Clinical Ophthalmology 2026, 20:612158
Published Date: 15 July 2026