Back to Journals » Clinical Ophthalmology » Volume 20
Photic Phenomena and Quality of Vision Following Aspheric Toric Monofocal IOL with a Double C-Loop Haptic Design Implantation
Authors Ang RET ![]() , Tañá-Rivero P, Pastor-Pascual F, Stodulka P
, Tañá-Rivero P, Pastor-Pascual F, Stodulka P ![]() , Slovak M
, Slovak M ![]() , Tetz MR, Fischinger I, Gessa-Sorroche M, Ibarz-Barberá M, Groneberg T
, Tetz MR, Fischinger I, Gessa-Sorroche M, Ibarz-Barberá M, Groneberg T
Received 31 March 2026
Accepted for publication 30 June 2026
Published 15 July 2026 Volume 2026:20 612158
DOI https://doi.org/10.2147/OPTH.S612158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Robert Edward T Ang,1 Pedro Tañá-Rivero,2 Francisco Pastor-Pascual,3 Pavel Stodulka,4,5 Martin Slovak,4 Manfred R Tetz,6 Isaak Fischinger,7 María Gessa-Sorroche,8 Marta Ibarz-Barberá,9 Thomas Groneberg10
1Asian Eye Institute, Makati, Philippines; 2Oftalvist, Alicante, Spain; 3Oftalvist, Valencia, Spain; 4GEMINI Eye Clinic, Zlin, Czech Republic; 5Third Faculty of Medicine, Charles University, Prague, Czech Republic; 6Berlin Eye Research Institute (BERI), Berlin, Germany; 7Berlin Eye Research Institute (BERI), Wittenberg, Germany; 8Miranza Virgen de Luján, Sevilla, Spain; 9Oftalvist, Madrid, Spain; 10Augenzentrum Erding, Erding, Germany
Correspondence: Robert Edward T Ang, Asian Eye Institute, 8th Floor PHINMA Plaza, Rockwell Center, Makati, Philippines, Email [email protected]
Purpose: This study aimed to analyse photic phenomena and quality of vision in cataract patients implanted with a biconvex aspheric toric monofocal intraocular lens (IOL) with a double C-loop haptic design.
Methods: A total of 116 patients (232 eyes) with corneal astigmatism (≥ 0.75D) were implanted bilaterally with the PODEYE toric IOL. Postoperative evaluation at 11– 13 months post-surgery included binocular uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA), and posterior capsule opacification (PCO) grading. Specifically, photic phenomena (halo and glare) and quality of vision (QoV) were assessed at the 4– 6 months postoperative visit using a simulator and a validated patient-reported outcomes questionnaire.
Results: Mean binocular UDVA and CDVA were 0.01± 0.08 logMAR and – 0.03± 0.08 logMAR, respectively. Eleven eyes from our cohort of eyes showed mild PCO (4.8%). The size and intensity of halos decreased compared to the preoperative visit, from 29.63± 22.52 to 16.27± 14.51, and from 42.47± 24.62 to 29.44± 24.51, respectively. A similar trend was found for glare (from 28.38± 19.49 to 11.46± 13.91, and from 33.17± 23.30 to 22.61± 19.36, respectively). The mean Rasch Score analysis showed different improvements of quality of vision from preoperative to 4– 6 months postoperatively for frequency (– 26.19± 24.65), severity (– 22.82± 21.32) and bothersomeness (– 26.47± 26.05).
Conclusion: Bilateral implantation of the PODEYE toric IOL in cataract patients with corneal astigmatism provides good quality of vision. Halo and glare induced by this lens are less intense than those induced by cataracts, thus leading to a subjective reduction in these visual disturbances after surgery.
Keywords: photic phenomena, quality of vision, monofocal toric, double C-loop, intraocular lens, cataract
Introduction
Ocular astigmatism, which is usually present in cataract patients, is one of the most common refractive conditions presenting with 1.0 dioptres (D) or more.1 Specifically, a survey by the United Kingdom National Health Service carried out in eight of its ophthalmology clinics, and including 110, 468 eyes undergoing cataract surgery, showed that 78% of eyes had preoperative corneal astigmatism of ≥0.5D, 42% ≥1.0D, 21% ≥1.5D and 11% ≥2.0D.2 Several systematic reviews and meta-analyses have highlighted the importance of the use of toric intraocular lenses (IOLs) during cataract surgery.3,4 Toric IOLs provided better uncorrected distance visual acuity (UDVA), greater spectacle independence and lower amounts of residual astigmatism than non-toric IOLs,3 and correcting for corneal astigmatism using these lenses contributes to spectacle-free vision in the pseudophakic eye.4
Different toric IOL models have been designed and used worldwide for cataract surgery in pre-existing astigmatic eyes. One of these lenses is the PODEYE toric IOL (Beaver-Visitec International Inc., Waltham, USA), which comprises an aspheric toric optical surface with a double C-loop and posterior angulated haptic design. Retrospective and prospective clinical studies5–11 with this IOL have shown accurate refractive outcomes, high rotational stability and, therefore, good visual performance at different times post-surgery in eyes with pre-existing astigmatism. However, it has been suggested that patient-reported outcomes studies are needed to evaluate standard and premium cataract surgery options, from initial patient expectations to final patient-reported and visual quality outcomes.12 Therefore, in order to provide more information about the performance of these lenses, the main purpose of the present study was to analyse photic phenomena and quality of vision in a large sample of cataract patients with pre-existing astigmatism implanted with the PODEYE toric IOL using a glare and hale simulator and a validated quality of vision questionnaire.
Methods
Study Design and Patients
This was a prospective multicentre (10 sites) open-label study undertaken at different sites located in the Czech Republic (Gemini Eye Clinic), Philippines (Asian Eye Institute), Spain (IMO, Virgen de Lujan and Oftalvist Alicante, Valencia and Madrid), and Germany (Augenzentrum Erding, Augentagesklinik Spreebogen, Medicum Wittenberg). The study was designed to adhere to the Declaration of Helsinki, with all patients providing informed consent, and was approved by the Ethics Committees of the different centres [SCMC-AEI Ethics Review Committee (2021–008; Asian Eye Institute), Eticka Komise Ocni Kliniky Gemin (2024–04; Zlin, Czech Republic), Ethik-Kommission der Bayerischen Landesärztekammer (mb21053; München, Germany), Ärztekrammer Berlin (Eth-MZ 28/21; Berlin, Germany), Ärztekammer Sachsen-Anhalt (070/21 II; Halle, Germany), and Hospital Clínico San Carlos (21/230-EC_P; Oftalvist Madrid, Valencia and Alicante, IMO Barcelona and Virgen de Lujan)] and registered at the National Institutes of Health with numbers NCT04778501, NCT04866719, NCT04744467 and NCT04987216. All patients were implanted bilaterally with the monofocal PODEYE toric IOL. The PODEYE toric IOL (hydrophobic acrylic GFY material, Abbe number of 42 and refractive index of 1.52), has a double C-loop and a posterior-angulated haptic design (Figure 1). It has a biconvex aspheric toric (posterior surface) optic (–0.11 μm for 5 mm), with a 6.00 mm optical diameter and an 11.40 mm overall diameter. The spherical power ranges from 6.00D to 30.00D in 0.50D steps, and the cylindrical power at the IOL plane can be selected from the following values: 1.00/1.50/2.25/3.00/3.75/4.50/5.25/6.00D. Optical biometry with the IOLMaster instrument (Carl Zeiss Meditec AG, Jena, Germany) was used, and the IOL power, mainly calculated using the online calculator for the Barrett toric formula, was chosen to achieve a residual spherical equivalent of between –0.2D and 0.1D and the lowest residual cylinder possible.
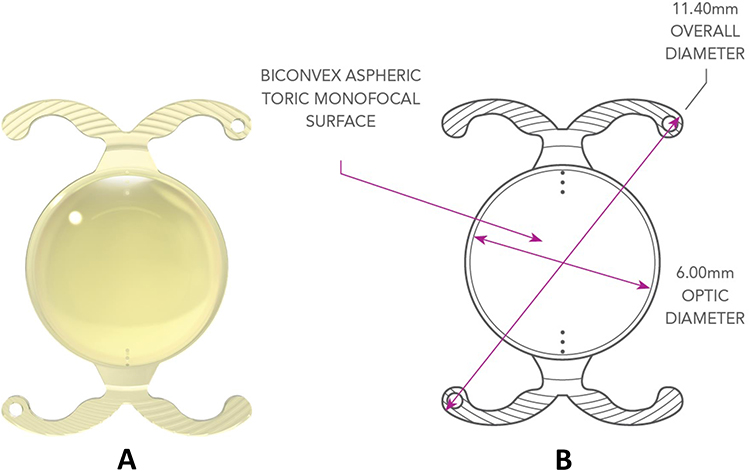 |
Figure 1 PODEYE toric intraocular lens (A) photography; (B) design). Courtesy of Beaver-Visitec International, Inc. [BVI]. |
Study Outcome Parameters
Binocular UDVA and corrected distance visual acuity (CDVA) under photopic conditions were measured at 11–13 months using the Clinical Trial Suite (M and S Technologies, Niles, IL, USA) at 4 m in logMAR scale, along with photic phenomena and quality of vision. The photic phenomena of halo and glare were measured at 4–6 months using a simulator that presented a simulated image of car headlights and traffic lights (Eyeland Design Network GmbH, Germany). Patients were asked to adjust the halo and glare level in a simulated image to the amount of such photic phenomena they perceived. Based on this image, patients adjusted the halo and glare levels on analogous scales from 0 to 100 according to their perception. The higher the value, the worse the perceived outcome, thereby indicating greater severity of halo or glare symptoms reported by the patients. This test was performed pre- and postoperatively, with the preoperative outcomes serving as a baseline measurement. The McAlinden Quality of Vision (QoV) questionnaire13 was used to assess visual symptoms at the same follow-up. It includes questions about glare, halos, starbursts, hazy vision, blurred vision, distortion, seeing multiple images, fluctuating vision, difficulty focusing and difficulty perceiving distance or depth, with scores ranging from 0 to 100 (higher scores indicate poorer vision quality). Photographs are used to simulate visual symptoms (ie, glare and halos), and patients are asked to report how often they experience the symptom (frequency), how severe they find the symptom (severity) and how bothered they are by the symptom (bothersomeness). For analysis, all answers are grouped together under the rating scales frequency, severity and bothersomeness. Subjective PCO grading was performed after pupil dilation at up to 11–13 months of follow-up.14 Any adverse IOL events were registered. Data from all patients were imported into an Excel spreadsheet (Microsoft Corporation, Redmont, USA) for complete analysis and the different variables studied were given as the mean ± standard deviation, 95% confidence interval (CI), median and ranges. Sample size was previously calculated.7
Results
A total of 232 eyes from 116 patients implanted bilaterally with the PODEYE Toric IOL were analysed in this study. In general, no related adverse IOL events were reported either during surgery or up to the final follow-up visit. At the 11–13 months visit, mean binocular UDVA was 0.01 ± 0.08 logMAR (95% CI: 0.00, 0.02; range: –0.16 to 0.26 logMAR) and mean binocular CDVA was –0.03 ± 0.08 logMAR (95% CI: –0.04, –0.01; range: –0.26 to 0.20 logMAR). Significant opacities were only reported for the posterior capsule. Eleven eyes from our cohort of eyes implanted with this toric IOL showed mild PCO (4.8%).
Halo and Glare Outcomes
Table 1 shows photic phenomena, halo and glare (type, size and intensity) outcomes registered using the visual simulator in our cohort of patients both preoperatively (n = 109 patients) and at 4–6 months post-PODEYE toric IOL implantation (n = 116 patients). The results post-surgery show that the size and intensity of halos decreased compared to the preoperative visit (from 29.63 ± 22.52 to 16.27 ± 14.51 and from 42.47 ± 24.62 to 29.44 ± 24.51, respectively). A similar trend was found in relation to glare (from 28.38 ± 19.49 to 11.46 ± 13.91 and from 33.17 ± 23.30 to 22.61 ± 19.36, respectively). Note that not all the patients reported preoperative outcomes.
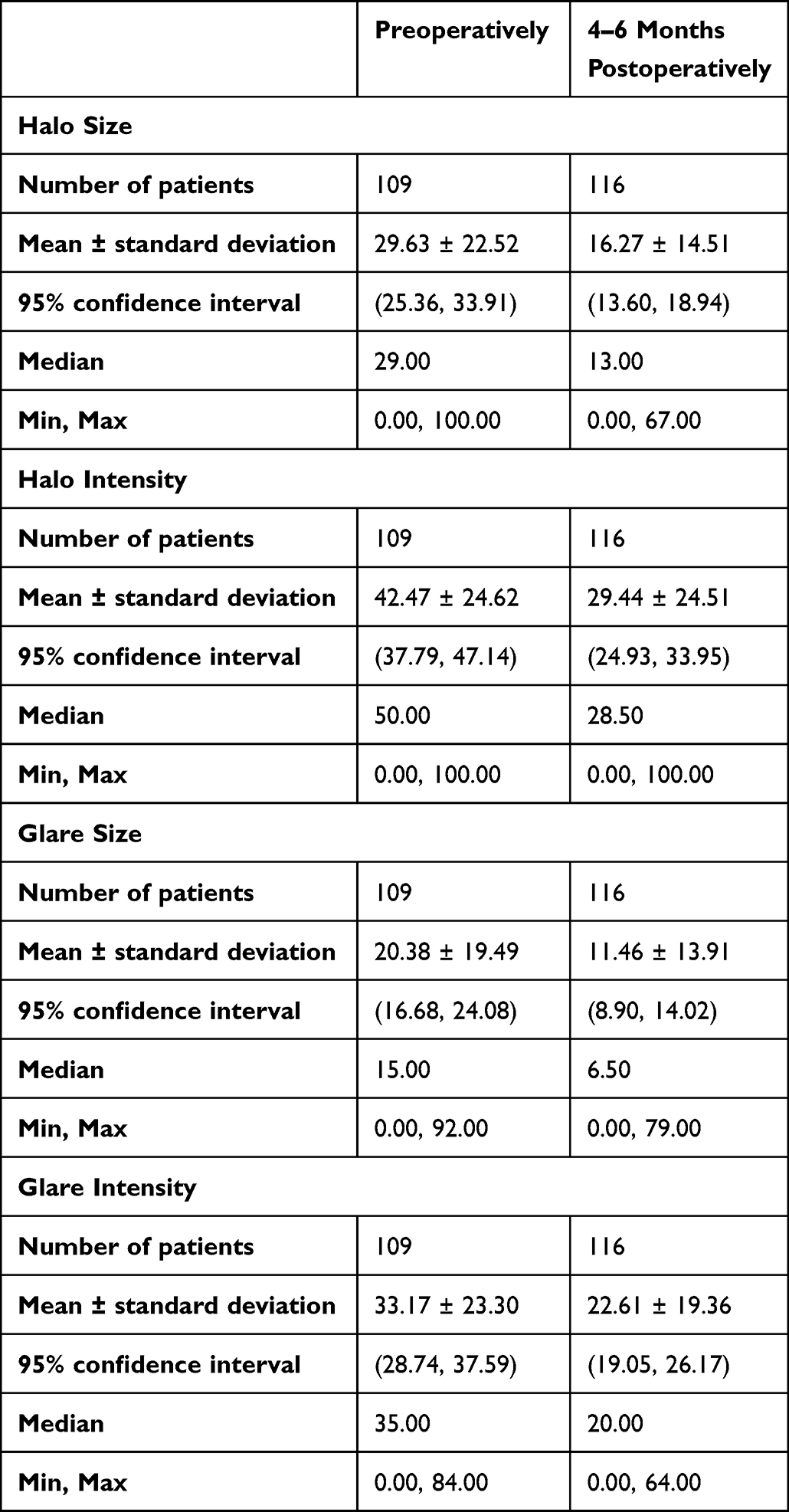 |
Table 1 Halo and Glare Outcomes Obtained Preoperatively and Postoperatively at 4–6 Months After PODEYE Toric Intraocular Lens Implantation |
Quality of Vision (QoV) Questionnaire
Table 2 shows the QoV questionnaire outcomes obtained before (n = 115 patients) and at 4–6 months after PODEYE toric IOL implantation (n = 115 patients). The mean Rasch Score analysis showed different improvements in quality of vision for the three categories evaluated: frequency, severity and bothersomeness. Specifically, the mean changes from preoperative to 4–6 months postoperatively were –26.19 ± 24.65 (95% CI: –30.77, –21.62), –22.82 ± 21.32 (95% CI: –26.78, –18.87) and –26.47 ± 26.05 (95% CI: –31.31, –21.64), respectively.
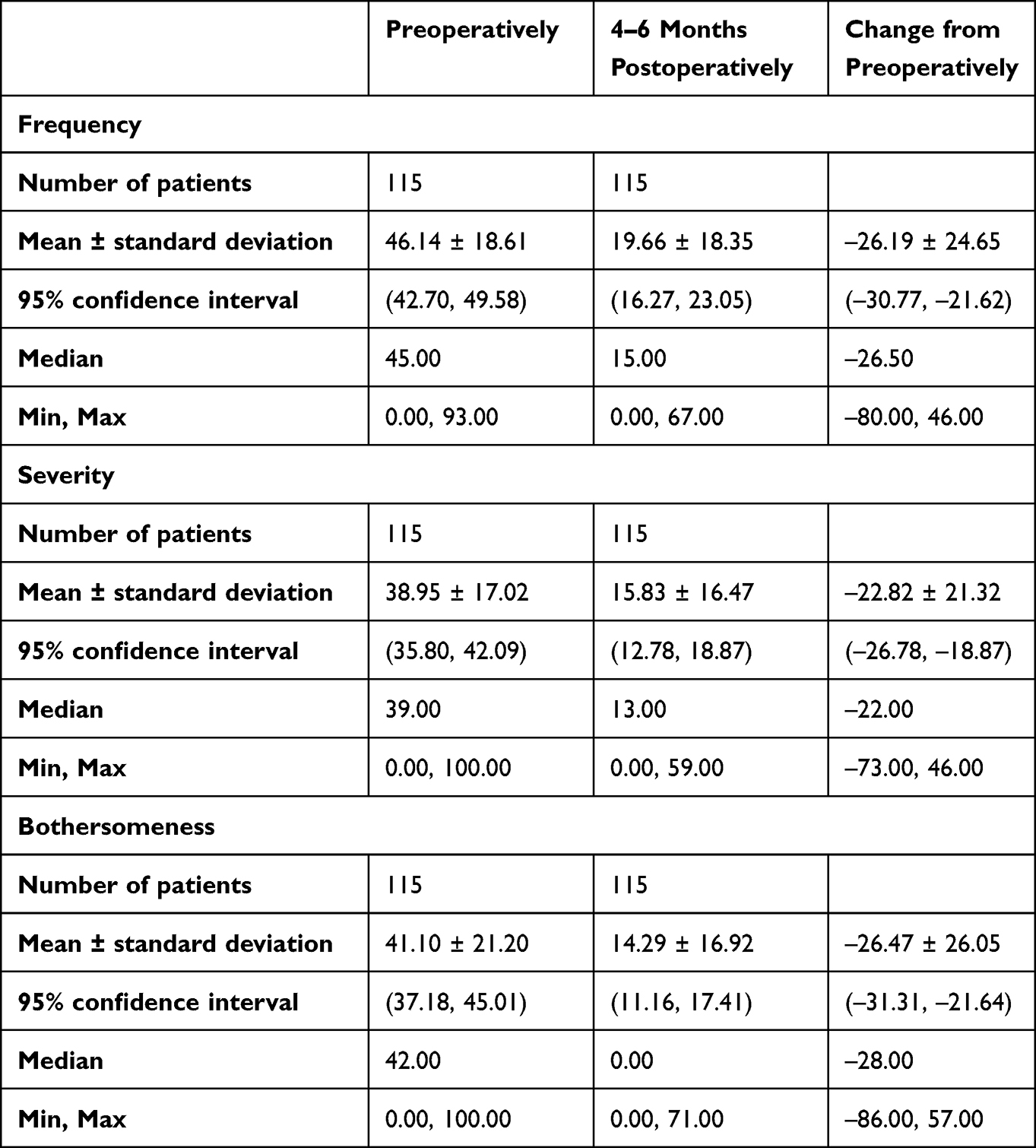 |
Table 2 Quality of Vision (QoV) Questionnaire Outcomes Obtained Preoperatively and Postoperatively at 4–6 Months After PODEYE Toric Intraocular Lens Implantation |
Discussion
It is well known that toric IOLs were developed to enhance the reduced visual acuity caused by cataracts and to correct pre-existing corneal astigmatism during the same surgical procedure. Previous literature concerning the clinical outcomes of the PODEYE toric IOL supports the use of this lens for this purpose.5–11 With regard to binocular visual acuity outcomes, our findings agree with these studies, thus showing that this lens offers good visual performance. Specifically, since this has not been evaluated and reported previously, we focused on the photic phenomena that patients implanted with this IOL model may report post-surgery. To that end, we used a visual simulator and a validated patient-reported outcomes questionnaire.
Halo and glare outcomes are shown in Table 1 indicating size and intensity pre- and post-surgery (4–6 months). The size and intensity of both visual phenomena decreased after PODEYE toric IOL implantation. Other studies using the same visual simulator but analysing different cohorts have been published.15,16 For example, Kretz et al15 assessed 28 cataract patients (56 eyes) after trifocal toric AT LISA tri toric 939MP (Carl Zeiss Meditec, Jena, Germany) implantation at 3 months postoperatively. Their analysis with the halo and glare simulator revealed the presence of halos with a mean size of 50.67 ± 15.69 (median: 53; range: 31 to 75) and a mean intensity of 54.89 ± 17.86 (median: 62; range: 33 to 79). With regard to glare, the mean size and intensity were 39.67 ± 3.51 (median: 40; range: 0 to 49) and 44.67 ± 15.01 (median: 36; range: 14 to 68), respectively. The mean values reported for the two visual phenomena in terms of both size and intensity were higher than those reported in our study. It should be considered, however, that the diffractive profile of the trifocal toric lens may play a significant role in comparison to the monofocal aspheric surface of the PODEYE toric. The optical principle of diffractive surfaces means that the light is distributed between different foci, thereby creating a superimposition of the retinal images. This creates the perception of halos reported by patients. Glare, in turn, can arise due to scattering of the light from the diffractive steps. Savini et al16 investigated the clinical performance of an enhanced depth-of-focus (EDOF) IOL in comparison with a diffractive bifocal IOL. These authors studied 20 patients implanted with the Mini Well IOL (Sifi, Catania, Italy) and 37 patients implanted with the AcrySof ReSTOR SV25T IOL (Alcon Labs, Fort Worth, TX, USA) at 4–8 weeks post-surgery and found that halos had a mean size of 34.8 ± 22.08 and a mean intensity of 38.50 ± 16.47 with the Mini Well IOL. In contrast, the mean halo size and intensity were significantly higher with the diffractive bifocal AcrySof ReSTOR IOL (53.57 ± 23.67 (P = 0.0439) and 54.76 ± 20.53 (P = 0.0222), respectively). These values are in agreement with those reported previously by Kretz et al15 with the trifocal diffractive toric IOL. In contrast, when glare was evaluated by Savini et al16 no statistically significant differences were reported for glare size (4.40 ± 8.69 for the Mini Well IOL and 8.52 ± 14.54 for the AcrySof ReSTOR IOL) or intensity (15.70 ± 26.33 for the Mini Well IOL and 13.81 ± 23.70 for the AcrySof ReSTOR IOL).
The outcomes of the QoV questionnaire are shown in Table 2. This table shows different improvements in quality of vision for the three categories evaluated (frequency, severity and bothersomeness). Al-Shymali et al17 assessed patient dissatisfaction outcomes using the QoV questionnaire in 15 dissatisfied patients following multifocal IOL implantation by IOL exchange with another multifocal IOL using another optical profile. Postoperatively, the mean Rasch score values for frequency, severity and bothersomeness were 35.87 ± 29.40, 34.20±32.26, and 32.33 ± 35.97, respectively. In another study, Al-Shymali et al18 also assessed patient dissatisfaction outcomes using the same questionnaire in 16 patients following multifocal IOL implantation, in this case by IOL exchange with a monofocal IOL. Postoperatively, the mean Rasch score values for frequency, severity and bothersomeness were 34.46 ± 16.33, 28.46±14.09, and 28.85 ± 16.22, respectively, when the multifocal IOL was exchanged with a monofocal IOL. These authors found no statistically significant difference in quality of vision after the exchange between both types of groups (multifocal and monofocal IOLs).19 The corresponding values in our study were lower than those reported by these authors (about 20 for frequency, and about 15 for severity and bothersomeness; see Table 2), thereby highlighting the good quality of vision obtained in our cohort of patients. Note that photic phenomena increase after trifocal IOL implantation. A review of multifocal versus monofocal IOLs found that photic phenomena are 3.5-times more likely to occur with the former than with the latter.20 This study finds that multifocal IOLs improve near vision compared to monofocal IOLs, despite uncertainty about the exact size of the benefit. Whether these gains justify side effects like glare and halos remain a matter of individual patient experience.
PCO is a postoperative complication that can directly contribute to asymmetric contraction of the capsular bag, thereby leading to rotational instability of toric IOLs.21 Therefore, in addition to the reduction in quality of vision, PCO should also be taken into account, specifically in toric IOLs, in order to avoid any rotation that may reduce visual performance. It is well known that there is a difference in PCO rate between hydrophobic and hydrophilic lenses. A meta-analysis of randomized controlled trials reported lower PCO rates for hydrophobic versus hydrophilic IOLs at one and two years of follow-up, as well as significantly lower rates of Nd:YAG capsulotomy.22 A prospective multicentre (16 sites in USA) study analysing 342 patients implanted with the Clareon hydrophobic IOL (SY60CL, Alcon Labs, Fort Worth, TX, USA) reported a PCO rate of 5.4% at one-year post-surgery.23 Our study showed a comparable performance at the same post-operative follow-up period (4.8%).
We need to consider that our study has several limitations. First, neither additional patient-reported outcome questionnaires nor other IOL groups were included to evaluate potential differences. Second, given the short follow-up period of our study, longer-term data are needed to validate these initial results. And third, other factors such as the size of capsulorhexis, size of the pupil, type of cataract and the multicenter study may affect and should be considered. Future studies should further explore, with a larger sample, how these perceptions evolve over time across a broader range of questionnaires and IOL models.
Conclusions
The results of this study suggest that bilateral PODEYE toric IOL implantation provides high-quality vision in patients with pre-existing corneal astigmatism undergoing cataract surgery. Although photic phenomena are a known side-effect of IOLs, the halo and glare induced by the PODEYE toric IOL are lower than those induced by cataracts, thereby leading to a subjective reduction in visual disturbances after surgery.
Data Sharing Statement
Data of this trial are not available for sharing.
Acknowledgments
The authors would like to thank Drs. Jorge Cazal and Detlef Holland, who gave their time to take part in this trial.
Funding
This trial was funded by Beaver-Visitec International, Inc. [BVI].
Disclosure
Robert Edward T. Ang declares grants for studies from Acevision, Inc., Acufocus, Inc., Alcon, Bausch & Lomb, Inc.; Beaver-Visitec International, Forsight Robotics, Glaukos Corp., Hoya, Ivantis, Inc., Johnson&Johnson Vision, Teleon, Spyglass, and STAAR Surgical. Pedro Tañá-Rivero declares grants for studies from Alcon Healthcare SA, AST Products Inc., BVI Inc., Carl Zeiss, Hoya Surgical AG, Humanoptics Holding AG, Johnson & Johnson Surgical Vision, Staar Surgical AG, Vialase Inc, Z Optics Inc. Francisco Pastor-Pascual declares grants for studies from Alcon Healthcare SA, BVI Inc., Carl Zeiss, Hoya Surgical AG and Humanoptics Holding AG. Pavel Stodulka declares grants for studies from Bausch and Lomb. He is also an advisor for Hanita Lenses and Carl Zeiss Meditec AG; consultant of Bausch & Lomb; and stock or stock options from Pollux Nova a.s., outside the submitted work. Marta Ibarz-Barberá declares grants for studies from BVI Inc., Cutting-Edge, ELIOS Vision Inc, and Hoya Surgical AG. The authors report no other conflicts of interest in this work.
References
1. Verstraaten JH, Buzzi M, Masalkhi M, et al. Correcting astigmatism using toric intraocular lenses during cataract surgery. Am J Ophthalmol. 2026;S0002-9394(26):00107–8. doi:10.1016/j.ajo.2026.02.043
2. Day AC, Dhariwal M, Keith MS, et al. Distribution of preoperative and postoperative astigmatism in a large population of patients undergoing cataract surgery in the UK. Br J Ophthalmol. 2019;103:993–8. doi:10.1136/bjophthalmol-2018-312025
3. Kessel L, Andresen J, Tendal B, Erngaard D, Flesner P, Hjortdal J. Toric intraocular lenses in the correction of astigmatism during cataract surgery: a systematic review and meta-analysis. Ophthalmology. 2016;123(2):275–286. doi:10.1016/j.ophtha.2015.10.002
4. Goggin M. Toric intraocular lenses: evidence-based use. Clin Exp Ophthalmol. 2022;50(5):481–489. doi:10.1111/ceo.14106
5. Bozukova D, Werner L, Mamalis N, et al. Double-C loop platform in combination with hydrophobic and hydrophilic acrylic intraocular lens materials. J Cataract Refract Surg. 2015;41(7):1490–1502. doi:10.1016/j.jcrs.2014.10.042
6. Chassain C, Hallak MK, Lesaffre M. Rotational stability and clinical outcomes after implantation of a new toric intraocular lens with double C-loop design. J Fr Ophtalmol. 2023;46:571–580. doi:10.1016/j.jfo.2022.07.005
7. Ang RET, Tañá-Rivero P, Pastor-Pascual F, Stodulka P, Tetz M, Fischinger I. Visual and refractive outcomes after bilateral implantation of a biconvex aspheric toric monofocal intraocular with a double C-loop haptic design. Clin Ophthalmol. 2023;17:2765–2776. doi:10.2147/OPTH.S432598
8. Ang RET, Tañá-Rivero P, Pastor-Pascual F, et al. One-year clinical outcomes following aspheric toric monofocal IOL with a double C-Loop haptic design implantation. Clin Ophthalmol. 2024;18:3515–3525. doi:10.2147/OPTH.S494313
9. Nemet AY, Reitblat O, Levy A, Nemet A, Assia EI. Clinical outcomes following toric intraocular lens implantation: a case series study. J Clin Med. 2025;14(7):2316. doi:10.3390/jcm14072316
10. Ang RET, Tañá-Rivero P, Pastor-Pascual F, et al. Rotational stability after implantation of an aspheric toric monofocal IOL with a double C-Loop haptic design in normal and high axial lengths. Clin Ophthalmol. 2025;19:2393–2403. doi:10.2147/OPTH.S530593
11. Mori Y, Miyata K, Kojima T, et al. Clinical performance of a hydrophobic acrylic toric intraocular lens with a double C-loop haptics in Japanese patients. Jpn J Ophthalmol. 2025. doi:10.1007/s10384-025-01274-4
12. Wang SY, Stem MS, Oren G, Shtein R, Lichter PR. Patient-centered and visual quality outcomes of premium cataract surgery: a systematic review. Eur J Ophthalmol. 2017;27(4):387–401. doi:10.5301/ejo.5000978
13. McAlinden C, Pesudovs K, Moore JE. The development of an instrument to measure quality of vision: the Quality of Vision (QoV) questionnaire. Invest Ophthalmol Vis Sci. 2010;51(11):5537–5545. doi:10.1167/iovs.10-5341
14. Findl O, Buehl W, Menapace R, et al. Comparison of 4 methods for quantifying posterior capsule opacification. J Cataract Refract Surg. 2003;29(1):106–111. doi:10.1016/s0886-3350(02)01509-2
15. Kretz FT, Breyer D, Klabe K, et al. Clinical outcomes after implantation of a trifocal toric intraocular lens. J Refract Surg. 2015;31(8):504–510. doi:10.3928/1081597X-20150622-01
16. Savini G, Schiano-Lomoriello D, Balducci N, Barboni P. Visual performance of a new extended depth-of-focus intraocular lens compared to a distance-dominant diffractive multifocal intraocular lens. J Refract Surg. 2018;34(4):228–235. doi:10.3928/1081597X-20180125-01
17. Al-Shymali O, McAlinden C, Alio Del Barrio JL, Canto-Cerdan M, Alio JL. Patients’ dissatisfaction with multifocal intraocular lenses managed by exchange with other multifocal lenses of different optical profiles. Eye Vis. 2022;9(1):8. doi:10.1186/s40662-022-00280-8
18. Al-Shymali O, Alió Del Barrio JL, McAlinden C, Canto M, Primavera L, Alio JL. Multifocal intraocular lens exchange to monofocal for the management of neuroadaptation failure. Eye Vis. 2022;9(1):40. doi:10.1186/s40662-022-00311-4
19. Al-Shymali O, Cantó-Cerdán M, Alió Del Barrio JL, McAlinden C, Yebana P, Alio JL. Managing dissatisfaction after multifocal intraocular lens implantation through lens exchange using monofocal or alternative multifocal IOLs. Acta Ophthalmol. 2024;102(7):e1040–e1049. doi:10.1111/aos.16720
20. de Silva SR, Evans JR, Kirthi V, Ziaei M, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2016;12(12):CD003169. doi:10.1002/14651858.CD003169.pub4
21. Vukich JA, Ang RE, Straker BJK, et al. Evaluation of intraocular lens rotational stability in a multicenter clinical trial. Clin Ophthalmol. 2021;15:3001–3016. doi:10.2147/opth.S309214
22. Li Y, Wang J, Chen Z, Tang X. Effect of hydrophobic acrylic versus hydrophilic acrylic intraocular lens on posterior capsule opacification: meta-analysis. PLoS One. 2013;8(11):e77864. doi:10.1371/journal.pone.0077864
23. Lehmann R, Maxwell A, Lubeck DM, Fong R, Walters TR, Fakadej A. Effectiveness and safety of the clareon monofocal intraocular lens: outcomes from a 12-month single-arm clinical study in a large sample. Clin Ophthalmol. 2021;15:1647–1657. doi:10.2147/OPTH.S295008
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Refractive and Visual Outcomes of a Monofocal Non-Constant Aberration Aspheric Intraocular Lens
Hernández-Martínez A, Díaz-del-Rio MA, Ruiz-Santos M, Ruiz-Mesa R, Tañá-Rivero P
Clinical Ophthalmology 2022, 16:2521-2530
Published Date: 10 August 2022
Visual and Refractive Outcomes After Bilateral Implantation of a Biconvex Aspheric Toric Monofocal Intraocular with a Double C-Loop Haptic Design
Ang RET, Tañá-Rivero P, Pastor-Pascual F, Stodulka P, Tetz M, Fischinger I
Clinical Ophthalmology 2023, 17:2765-2776
Published Date: 20 September 2023
Rotational Stability After Implantation of an Aspheric Toric Monofocal IOL with a Double C-Loop Haptic Design in Normal and High Axial Lengths
Ang RET, Tañá-Rivero P, Pastor-Pascual F, Stodulka P, Slovak M, Tetz M, Fischinger I, Cazal J, Gessa M, Ibarz-Barberá M, Holland D, Groneberg T
Clinical Ophthalmology 2025, 19:2393-2403
Published Date: 19 July 2025
Visual and Refractive Outcomes After Implantation of an Isofocal Optic-Design Intraocular Lens with Double C-Loop Haptics in Japanese Eyes
Akahoshi T
Clinical Ophthalmology 2025, 19:2453-2462
Published Date: 29 July 2025
Clinical Outcomes of a Multicenter Study Following Implantation of an Isofocal Optic IOL with Double C-Loop Haptics
Daya S, Akahoshi T, Bosc C, Mouchel R, Chassain C, Van Acker E, Di Maria A, Fogagnolo P
Clinical Ophthalmology 2025, 19:3121-3131
Published Date: 2 September 2025