Back to Journals » Clinical Ophthalmology » Volume 17
Visual and Refractive Outcomes After Bilateral Implantation of a Biconvex Aspheric Toric Monofocal Intraocular with a Double C-Loop Haptic Design
Authors Ang RET ![]() , Tañá-Rivero P, Pastor-Pascual F, Stodulka P
, Tañá-Rivero P, Pastor-Pascual F, Stodulka P ![]() , Tetz M, Fischinger I
, Tetz M, Fischinger I
Received 27 July 2023
Accepted for publication 13 September 2023
Published 20 September 2023 Volume 2023:17 Pages 2765—2776
DOI https://doi.org/10.2147/OPTH.S432598
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Robert Edward T Ang,1 Pedro Tañá-Rivero,2 Francisco Pastor-Pascual,3 Pavel Stodulka,4 Manfred Tetz,5 Isaak Fischinger6
1Cataract and Refractive Surgery Department, Asian Eye Institute, Makati City, Philippines; 2Cataract and Refractive Surgery Department, Oftalvist, Alicante, Spain; 3Cataract and Refractive Surgery Department, Oftalvist, Valencia, Spain; 4Cataract and Refractive Surgery Department, Gemini Eye Clinic, Zlin, Czech Republic; 5Cataract and Refractive Surgery Department, Augentagesklinik Spreebogen, Berlin, Germany; 6Medical Faculty, Johannes Kepler University Linz, Linz, Austria
Correspondence: Robert Edward T Ang, Asian Eye Institute, 8th Floor PHINMA Plaza, Rockwell Center, Makati City, Philippines, Email [email protected]
Purpose: To show the visual and refractive outcomes in cataract patients with corneal astigmatism when bilaterally implanted with a biconvex aspheric toric monofocal intraocular lens (IOL) with a double C-loop haptic-design.
Methods: Forty-seven cataract patients (94 eyes) with corneal astigmatism (≥ 0.75D) were implanted with the monofocal PODEYE toric IOL and assessed for 4– 6 months post-surgery. Measurements included monocular and binocular uncorrected-distance visual acuity (UDVA) and corrected-distance visual acuity (CDVA), under both photopic and mesopic lighting conditions. Refraction, photopic and mesopic contrast sensitivity (with and without glare), and rotational stability were also recorded at the last postoperative visit.
Results: At 4– 6 months, 78.2% and 98.9% of eyes were within ± 0.50D and ± 1.00D of the target refraction, respectively. The mean spherical equivalent and refractive cylinder values were 0.09± 0.35D and − 0.36± 0.35D, respectively. 76.5% and 98.8% of eyes presented a postoperative refractive cylinder of ≤ 0.50D and ≤ 1.00D, respectively. 91.5% and 100% of patients had a binocular UDVA and CDVA of ≥ 20/25, respectively. The mean binocular UDVA and CDVA were 0.02± 0.08 and − 0.02± 0.07 logMAR, respectively. Under mesopic conditions, 78.7% and 83.0% of patients presented a binocular UDVA and CDVA ≥ 20/32, respectively. The mean binocular UDVA and CDVA were 0.15± 0.11 and 0.12± 0.11 logMAR, respectively. The patients showed good contrast sensitivity under photopic and mesopic conditions. The mean absolute IOL rotation was 1.22± 2.21 degrees with 97.87% of eyes having a rotation of < 10 degrees.
Conclusion: This study shows good visual and refractive outcomes for the PODEYE toric IOL when implanted bilaterally in cataract patients with corneal astigmatism.
Keywords: monofocal toric, astigmatism, double C-loop, intraocular lens, cataract
Introduction
It is well known that corneal astigmatism is a common condition among cataract patients. One recent study carried out in a large population indicated that in eyes undergoing cataract surgery, a preoperative corneal astigmatism of ≥1.0 diopters (D) was present in 42%, while 11% had a value of ≥2.0D.1 It has been reported that, in most subjects, astigmatism under 0.50 D did not degrade visual acuity, suggesting that under clinical conditions, the visual benefit of precisely correcting astigmatism of less than 0.50D would be limited.2 Therefore, predicted postoperative residual refractive corneal astigmatism of 0.75D should be addressed for those patients looking for spectacle independence.
A meta-analysis and systematic review of toric intraocular lenses (IOLs) for correcting astigmatism during cataract surgery evaluated the benefit and harm (surgical complications and residual astigmatism) associated with the implantation of these lenses, focusing on postoperative uncorrected-distance visual acuity (UDVA) and distance spectacle independence.3 That study analyzed 13 randomized clinical trials with 707 eyes randomized to toric IOLs and 706 eyes randomized to non-toric IOLs. The authors found good-quality evidence that UDVA was better in the toric IOL group, which also provided greater spectacle independence, and moderate-quality evidence that toric IOL implantation was not related to an increased risk of complications. They concluded that toric IOLs provided better UDVA, greater spectacle independence, and lower amounts of residual astigmatism than non-toric IOLs. The authors also pointed out that their conclusions were limited to the range of preoperative astigmatism reported in the studies analyzed (generally 0.75 to 3.00D). The use of toric IOLs is therefore recommended in cataract patients with regular corneal astigmatism who want postoperative spectacle independence for distance vision.
The PODEYE toric IOL is a new monofocal lens with a double C-loop and posterior angulated haptic design. Only one recent study has been published on this lens, a retrospective study aiming to assess rotational stability and clinical outcomes in 136 eyes (102 patients). The conclusion was that the PODEYE toric IOL showed high rotational stability, allowing for the correction of corneal astigmatism during cataract surgery.4 However, to date, there has been no prospective analysis of this lens when implanted bilaterally. The main purpose of this prospective study was to assess the visual and refractive outcomes in cataract patients with corneal astigmatism when bilaterally implanted with the PODEYE toric IOL.
Methods
Study Design and Subjects
This was a multicentric prospective open-label study conducted at five centers: the Asian Eye Institute (Makati City, Philippines), Oftalvist Alicante (Alicante, Spain), Oftalvist Valencia (Valencia, Spain), Gemini Eye Clinic (Zlin, Czech Republic), and Augentagesklinik Spreebogen (Berlin, Germany). The study was approved by the SCMC-AEI Ethics Review Committee (Asian Eye Institute), Hospital Clínico San Carlos (Oftalvist Alicante and Valencia), Eticka Komise OCni Kliniky Gemin (Zlin, Czech Republic), and Ärztekrammer Berlin (Berlin, Germany) and followed the tenets of the Declaration of Helsinki. All participants provided informed consent. The study was registered with the National Institutes of Health (NCT04778501, NCT04866719, NCT04744467 and NCT04987216).
The inclusion criteria were: male or female adults ≥50 years of age on the day of screening who had clinically documented cataracts in both eyes; a calculated IOL power (sphere and cylinder) within the range of the investigational IOL; regular corneal astigmatism (measured by a topographer); corneal astigmatism of ≥0.75D and ≤4.25D (measured by an automatic keratometer) in both eyes; clear intraocular media other than cataract; dilated pupil size large enough to visualize IOL axis markings postoperatively; and a corrected-distance visual acuity (CDVA) projected to be better than 0.2 logMAR after toric IOL implantation. The exclusion criteria were: subjects diagnosed with degenerative visual disorders, such as macular degeneration; subjects with age-related macular degeneration; previous intraocular or corneal surgery; traumatic cataract; a history or presence of macular edema; unstable keratometry or biometry measurements (an acceptable maximum standard deviation for the axial length of ±50 μm, anterior chamber depth ±150 μm, and keratometry ±0.15D); clinically significant, uncontrolled glaucoma with an expected negative impact on contrast sensitivity and/or visual acuity outcomes; clinically significant dry eye (as judged by the physician); and ocular surface disease (clinical symptoms or keratitis), among other things.
The patients were bilaterally implanted with the monofocal PODEYE toric IOL (BVI, Waltham, USA). This lens is based on hydrophobic acrylic GFY biomaterial (with UV and blue light filtration) and has a double C-loop with Ridgetech and a posterior-angulated haptic design. The IOL has a biconvex aspheric toric optic with a refractive index of 1.52 and an Abbe number of 42. The front surface is aspherical to yield an optic with a spherical aberration of −0.11 micrometers at 5.0 mm of aperture and the cylinder is located on the posterior surface. The overall diameter is 11.40 mm, and the optic diameter is 6.00 mm. The spherical power is available from +6.00D to +30.00D in 0.50D steps, and the cylindrical power (IOL plane) is available for 1.00, 1.50, 2.25, 3.00, 3.75, 4.50, 5.25, and 6.00D.
Cataract surgery was performed using standard phacoemulsification with a 2.2 mm incision, targeting a 5.5 mm diameter capsulorhexis or femtosecond laser-assisted capsulotomy to allow the optic to be fully overlapped by the anterior capsular rim.
Preoperative and Postoperative Assessment
All subjects recruited in this study were evaluated prior to the surgery and the following examinations were performed: photopic monocular CDVA, refraction, and optical biometry using the IOLMaster device (Carl Zeiss Meditec AG, Jena, Germany). The IOL power (sphere and cylinder) was chosen to achieve a residual spherical equivalent of between −0.2D and 0.1D and the lowest residual cylinder possible. The IOL power was principally calculated using the Barrett toric formula with the online calculator.
Postoperatively, the following parameters were measured at 4–6 months: refraction (sphere, cylinder, and manifest refraction spherical equivalent (MRSE)), and an astigmatism vector analysis was performed. Monocular and binocular UDVA, and CDVA under both photopic and mesopic (3.5 cd/m2) conditions were also measured using Clinical Trial Suite (M&S Technologies, Niles, IL, USA) at 4 m in logMAR scale. Binocular photopic and mesopic contrast sensitivity, both with and without glare, was also recorded using the Clinical Trial Suite instrument. Absolute rotational stability (mean, standard deviation and range) of the lenses was obtained between 1- and 4–6 months post-surgery. Any adverse events or complications were also recorded.
Statistical Analysis and Sample Size
The outcomes were analyzed using Excel (2019, version 16.43, Microsoft Corporation, Redmond, WA, USA). All measurements are given as the mean ± standard deviation (SD) and ranges. To calculate the sample size, we considered that the primary performance endpoint was to show that the absolute rotation value up to the 4–6 months postoperative visit was less than 10 degrees in 90% of the cases. The sample size calculation was performed assuming a power of 95% with a one-sided 97.5% confidence interval. The following parameters were used: significance level (α): 0.025; power (1-β): 0.95; one-sided test and expected proportion of eyes showing less than 10 degrees in absolute value of rotation between the day of surgery and 4–6 months postoperative visit: 99%. With these assumptions, the calculation5 indicated that a minimum of 70 eyes were needed to confirm the primary study endpoint. Taking into account the figure of 85% of patients having a binocular implantation and 15% a monocular implantation, 38 patients were needed to provide a sample size of 70 eyes implanted with a PODEYE toric lens. With an expected drop-out rate of 15%, approximately, at least 45 patients were needed to prove the primary study goal.
Results
In this study, we evaluated 94 eyes from 47 patients bilaterally implanted with the PODEYE Toric IOL. The mean age of the patients (32 female) was 68.9±8.2 years (ranging from 51 to 86 years). The demographics and preoperative characteristics for the whole sample are summarized in detail in Table 1. No adverse events related to the IOL were reported either during the surgery or up to the final follow-up visit.
 |
Table 1 Demographic Characteristics of Participants |
Refractive and Astigmatism Vector Analysis
Figure 1 shows the refractive accuracy of the procedure. Specifically, it shows the mean MRSE (top) and cylinder (bottom) values at 4–6 months of follow-up. 78.2% of eyes were within ±0.50 D and 98.9% of eyes were within ±1.00 D of the target refraction. The mean MRSE and refractive cylinder values were 0.09±0.35 D and −0.36±0.35 D, respectively. 76.5% and 98.8% of eyes had a postoperative refractive cylinder of ≤0.50 D and ≤1.00 D, respectively. Note that all eyes presented a mean MRSE value close to emmetropia (<0.25 D) and the mean refractive cylinder was less than half a diopter. Figure 2 shows the vector analysis of the preoperative and postoperative data.
 |
Figure 1 Refraction outcomes: distribution of spherical equivalent prediction error (top) and refractive cylinder (bottom) at 4–6 months post-surgery. |
 |
Figure 2 Vector analysis with preoperative and postoperative data. Centroids with standard deviations are also shown. Abbreviation: D, diopters. |
Visual Acuity Outcomes and IOL Rotation
Figure 3 shows the difference between photopic UDVA and CDVA in Snellen lines for monocular and binocular conditions. All eyes/patients showed a UDVA that was the same or better than the CDVA and 38% of eyes and 36% of patients presented better values. Figure 4 shows the cumulative proportion of eyes/patients with given monocular and binocular photopic logMAR UDVA and CDVA values. 69.1% and 89.4% of eyes presented monocular UDVA and CDVA values of 20/25 or better (≤0.10 logMAR), respectively. For patients, these percentages increase to 91.5% and 100% for binocular conditions. Specifically, the mean values of monocular UDVA and CDVA were 0.08±0.10 and 0.02±0.00 logMAR, respectively; and 0.02±0.08 and −0.02±0.07 logMAR for binocular conditions, respectively. Figure 5 shows the cumulative proportion of eyes/patients with given monocular and binocular mesopic logMAR UDVA and CDVA values. 60.6% and 75.5% of eyes presented a monocular UDVA and CDVA of 20/32 or better (≤0.20 logMAR), respectively. These percentages, for patients, increased to 78.7% and 83.0% for binocular conditions. Specifically, the mean values of monocular UDVA and CDVA were 0.21±0.12 and 0.17±0.11 logMAR, respectively; and 0.15±0.11 and 0.12±0.11 logMAR, for binocular conditions, respectively. Our mean absolute rotation was 1.22±2.21 degrees (ranging from 0 to 12 degrees), and 97.87% of eyes had a rotation of <10 degrees.
 |
Figure 3 Difference between uncorrected-distance visual acuity (UDVA) and best corrected-distance visual acuity (CDVA) value at 4–6 months post-surgery for monocular and binocular conditions. |
 |
Figure 4 Cumulative proportion of eyes having a given photopic monocular and binocular logMAR uncorrected-distance visual acuity (UDVA) and best corrected-distance visual acuity (CDVA) value at 4–6 months post-surgery. |
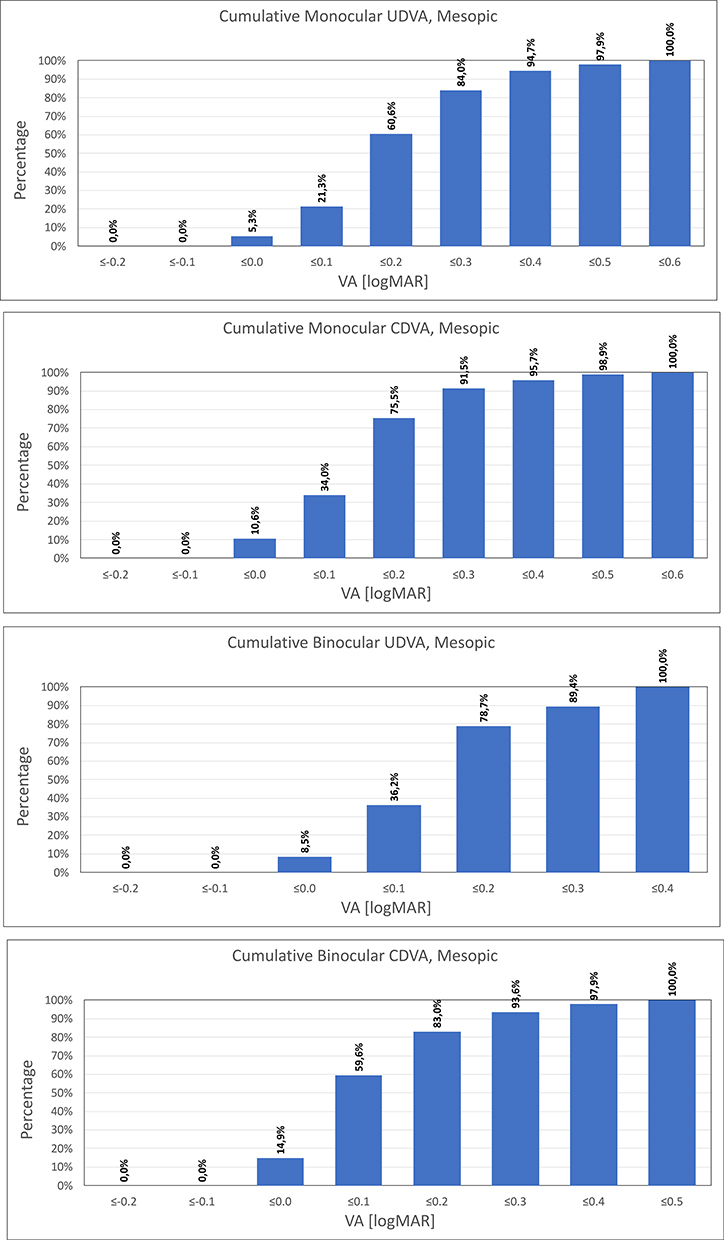 |
Figure 5 Cumulative proportion of eyes having a given mesopic monocular and binocular logMAR uncorrected-distance visual acuity (UDVA) and best corrected-distance visual acuity (CDVA) value at 4–6 months post-surgery. |
Contrast Sensitivity
Figure 6 shows the mean ± standard deviation values for the photopic and mesopic binocular contrast sensitivity functions with and without glare. The patients presented good log contrast sensitivity values at 3, 6, 12, and 18 cycles per degree spatial frequencies analyzed under both lighting conditions. It should be noted that, as expected, the photopic outcomes were slightly better than those found under low lighting conditions (mesopic), as well as those recorded when measured with a glare source.
 |
Figure 6 Mean photopic and mesopic binocular contrast sensitivity function with and without glare at 4–6 months post-surgery. |
Discussion
As mentioned, toric IOLs have been used worldwide as a standard surgical option for correcting preoperative corneal astigmatism during cataract surgery. It has been concluded that, in combination with adequate sphere selection, accurate use of toric IOLs enhances the patient’s vision after the surgery. The various toric IOL models available on the market have shown excellent visual and refractive outcomes, one of the most important parameters being the rotational stability of the lens once implanted. In our study, we analyzed the outcomes of the PODEYE toric IOL when implanted bilaterally in cataract patients with corneal astigmatism.
Our results revealed the good refractive outcomes obtained after the bilateral implantation of PODEYE toric IOLs. Specifically, almost all eyes (98.9%) were within ±1.00D of the target refraction and >75% of eyes were within ±0.50D (see Figure 1 for a detailed description of percentages as a function of the range). Taking into account the mean refraction values, all the eyes presented a mean MRSE value close to emmetropia (0.09±0.35D) with a mean refractive cylinder of <0.50D (−0.36±0.35D). As already stated, there is only one recent study of this IOL. That work, by Chassain et al4 retrospectively analyzed 136 eyes from 102 patients implanted with the PODEYE toric IOL at 1 week, 1 month, and 4 to 6 months after the surgery. As a general conclusion, they indicated that the PODEYE toric lens showed high rotational stability, allowing corneal astigmatism to be corrected during cataract surgery. Specifically, these authors, based on the patient’s needs, considered the target refraction for emmetropia or mild to moderate myopia (monovision). In the case of monovision in emmetropic eyes, they considered a target of 0D for the dominant eye and −1.0D for the non-dominant eye; for myopic eyes, the target was −0.50D for the dominant eye and −1.50D for the non-dominant eye; and for hyperopic eyes it was 0.00/-0.50 D in order to avoid binocular problems. They found a MRSE of −0.67±0.56D (ranging from −2.58 to +0.30D) for the cohort, −1.07±0.44D (ranging from −2.58 to −0.62D) for the myopic eyes, and −0.17±0.17D (ranging from −0.50 to +0.30D) for eyes with a myopic target of >-0.50D. They reported that the mean values for MRSE were −0.30±0.54D at the last postoperative visit (4–6 months). This mean value was slightly more myopic than the mean value recorded in our study, which in both cases was close to emmetropia. For the refractive cylinder, our results revealed that 76.5% and 98.8% of eyes showed a postoperative refractive cylinder of ≤0.50D and ≤1.00D, respectively. See also the reduced distribution of points in the vector analysis plot in Figure 2 (more concentrated values close to (0, 0) show a reduction in astigmatism since this value represents an astigmatism-free eye). Chassain et al4 found values of 84.1% and 98.1% of eyes for ≤0.50D and ≤1.00D, respectively, at the same postoperative visit. They found a mean refractive prediction error of −0.30±0.46D (ranging from −1.74 to +1.23D), and 70% and 92% of eyes were within ±0.50D and ±1.00D of the target refraction, respectively. Our results showed similar percentages: 78.2% and 98.9%, respectively (see Figure 1, top).
The visual acuity results obtained in our series revealed excellent outcomes, with 0.02±0.08 and −0.02±0.07 logMAR for binocular UDVA and CDVA, respectively (about 20/20), and 100% of eyes having a binocular cumulative CDVA of ≤0.10 logMAR. Chassain et al4 obtained a monocular mean CDVA value of −0.08±0.08 logMAR and all the eyes in that study had a cumulative monocular CVDA of ≤0.20 logMAR at 4–6 months. For mesopic conditions (see Figure 5), 78.7% and 83.0% of patients presented a cumulative binocular mesopic UDVA and CDVA of ≥20/32 (≤0.20 logMAR), respectively, with the mean values being 0.15±0.11 and 0.12±0.11 logMAR, respectively. We have to point out that all eyes and patients had a UDVA that was the same or better than the CDVA, and 38% of eyes and 36% of patients had better values (see Figure 3). The outcomes for contrast sensitivity were also good, from 3 to 18 cycles per degree spatial frequencies, and the differences between the four graphs are a result of the different lighting conditions and the use, or not, of a glare source during the measurement (see Figure 5). The best outcomes were found under photopic conditions without glare. Unfortunately, Chassain et al4 did not report outcomes for mesopic visual acuity and contrast sensitivity, so we were unable to make a direct comparison with those authors under the same IOL and follow-up conditions.
We also assessed the rotational stability of the lens as this is extremely important for toric IOLs. Our mean postoperative absolute IOL rotation was 1.22±2.21 degrees. In their study, Chassain et al4 obtained a mean postoperative IOL rotation from the baseline (surgery) of 2.05±2.17 degrees. With the exception of one outlier with 15 degrees of rotation, IOL rotation was ≤10 degrees at the 4–6 months postoperative follow-up in all of the eyes. They pointed out that, with the exception of the outlier, the maximum IOL rotation was 6 degrees at 1 month in 3 eyes, and 10 degrees at the final visit (4–6 months) in 1 eye. These authors also indicated that no surgical IOL re-positioning was required in their sample. Our series revealed that 97.87% of eyes had a rotation of <10 degrees. Another IOL using the same C-loop design, the Akoris toric IOL (BVI, Waltham, USA), also presented a similar absolute mean rotation: 2.16±1.95 degrees.6 The difference between these two lenses is the IOL material: hydrophobic in the case of the PODEYE toric lens versus hydrophilic for the Ankoris toric lens. The double C-loop design has shown good stability when implanted into the capsular bag. One experimental study, in line with the International Organization for Standardization (ISO) 11,979–3:2012, analyzed the behavior of the double C-loop in combination with hydrophobic and hydrophilic acrylic lens materials.7 That study showed that both lenses presented statistically insignificant variations and suggested the suitability of this platform for manufacturing premium IOLs, including multifocal, toric, and multifocal toric models. Another study assessing the biomechanical stability of the double C-loop models (Finevision POD F and Finevision POD FT lenses, BVI, Waltham, USA) found that the rotation was substantially less than the acceptable tolerance limits indicated in ISO 11979–2.8 That study also analyzed 45 eyes of 45 patients implanted with the Finevision POD F, Finevision POD FT (C-loop), and Micro F (four-loop, BVI, Waltham, USA), obtaining mean absolute rotation values of 2.482±1516, 1.590±0.451, and 2.393 degrees, respectively, for the three models (p < 0.001) at 3 months of follow-up. All the lenses presented a mean value of <3 degrees showing high stability, even, as the authors indicated, following potential capsular contractions prior to the surgery. A large study assessing the AcrySof Toric IOL (Alcon Labs, Fort Worth, USA) in 378 eyes, reported a mean absolute rotation for this model of 5.0±4.6 degrees and 4.8±4.4 degrees at 3 and 12-months post-surgery.9 However, another study with 75 eyes implanted with the same lens and analyzed 1 year after the surgery reported a large mean absolute IOL rotation of 8.83±5.26 degrees. It should be noted that high levels of rotation are expected in eyes with a large axial length: >20 degrees of rotation were reported in 6 eyes with axial lengths of >25 mm8, and 29.33% of eyes showed high myopia and consequently a large axial length.10 In addition, eyes with high myopia may have weaker zonules, which may therefore affect the rotational stability of the lens. According to the ISO11979-7:2018, the absolute value of rotation should be <10 degrees in 90% of the eyes implanted.11 In our study, 97.87% of eyes had a rotation of <10 degrees with a mean absolute rotation of 1.22±2.21 degrees. We consider that this rotation is not clinically relevant and, based on these values, we conclude that this lens showed a high degree of rotational stability when implanted in the capsular bag. This stability correlates with the appropriate post-surgery astigmatism correction (mean refractive cylinder of −0.36±0.35D) and hence good unaided distance visual acuity (91.5% of patients had a binocular UDVA of ≤0.10 logMAR).
We consider that the bilateral implantation of the lens is an important characteristic of our study since the binocular outcomes reported in our sample correspond only to the toric model. If both eyes of the same patient show a specific astigmatism value which consider the use of toric IOLs, surgeons may benefit for bilateral implantation with these lenses taken into account or results. Predicted postoperative residual refractive corneal astigmatism of 0.75D should be addressed for those patients looking for spectacle independence. It is expected to provide good visual and refractive outcomes after being implanted when combined with accurate biometric preoperative measurements, an accurate IOL power choice calculation (sphere and cylindrical powers), and an appropriate surgical technique to control for surgically induced astigmatism. Future studies should consider a large sample of patients and, specifically, a longer follow-up time. For example, 1-year follow-up data would be desirable to properly confirm the good rotational stability of the lens once implanted, despite the fact that further rotation is not expected after 6 months post-surgery.
Conclusion
Our results revealed that the PODEYE toric IOL is an effective option for improving distance visual acuity and reliably corrects preoperative corneal astigmatism in patients undergoing cataract surgery when implanted bilaterally. In terms of rotation, this IOL was rotationally stable with a high percentage of eyes presenting small rotation values.
Data Sharing Statement
Data of this trial are not available for sharing.
Funding
This trial was funded by Beaver-Visitec International, Inc. [BVI].
Disclosure
R. Ang obtained research grants from Acevision, Inc., Acufocus, Inc., Bausch&Lomb, Inc.; Beaver-Visitec International, Glaukos Corp., Ivantis, Inc., Johnson&Johnson Vision, and STAAR Surgical. P. Tañá-Rivero obtained research grants from Alcon Labs, AST Products Inc., Carl Zeiss Meditec, Hoya, Humanoptics, Johnson & Johnson, Beaver-Visitec International and STAAR Surgical. F. Pastor-Pascual obtained research grants from Alcon Labs, Carl Zeiss Meditec, Hoya, Humanoptics and Beaver-Visitec International.
Pavel Stodulka obtained research grants from Bausch and Lomb. The authors report no other conflicts of interest in this work.
References
1. Day AC, Dhariwal M, Keith MS, et al. Distribution of preoperative and postoperative astigmatism in a large population of patients undergoing cataract surgery in the UK. Br J Ophthalmol. 2019;103:993–1000. doi:10.1136/bjophthalmol-2018-312025
2. Villegas EA, Alcon E, Artal P. Minimum amount of astigmatism that should be corrected. J Cataract Refract Surg. 2014;40:13–19. doi:10.1016/j.jcrs.2013.09.010
3. Kessel L, Andresen J, Tendal B, Erngaard D, Flesner P, Hjortdal J. Toric intraocular lenses in the correction of astigmatism during cataract surgery: a systematic review and meta-analysis. Ophthalmology. 2016;123(2):275–286. doi:10.1016/j.ophtha.2015.10.002
4. Chassain C, Hallak MK, Lesaffre M. Rotational stability and clinical outcomes after implantation of a new monofocal toric intraocular lens with double C-loop design. J Fr Ophtalmol. 2023;46:571–580. doi:10.1016/j.jfo.2022.07.005
5. Rosner B. Fundamentals of Biostatistics.
6. Chassain C. Évaluation des performances visuelles aprèsimplantation d’une lentille intraoculaire torique à double anseen C. J Fr Ophtalmol. 2014;37:507–513. doi:10.1016/j.jfo.2014.02.007
7. Bozukova D, Werner L, Mamalis N, et al. Double-C loop platform in combination with hydrophobic and hydrophilic acrylic intraocular lens materials. J Cataract Refract Surg. 2015;41(7):1490–1502. doi:10.1016/j.jcrs.2014.10.042
8. Remón L, Cabeza-Gil I, Calvo B, Poyales F, Garzón N. Biomechanical stability of three intraocular lenses with different haptic designs: in silico and in vivo evaluation. J Refract Surg. 2020;36(9):617–624. doi:10.3928/1081597X-20200713-02
9. Miyake T, Kamiya K, Amano R, Iida Y, Tsunehiro S, Shimizu K. Long-term clinical outcomes of toric intraocular lens implantation in cataract cases with preexisting astigmatism. J Cataract Refract Surg. 2014;40:1654–1660. doi:10.1016/j.jcrs.2014.01.044
10. Zhu X, He W, Zhang K, Lu Y. Factors influencing 1-year rotational stability of AcrySof Toric intraocular lenses. Br J Ophthalmol. 2016;100:263–268. doi:10.1136/bjophthalmol-2015-306656
11. ISO N. 11979-7. Ophthalmic implants — intraocular lenses — part 7: clinical investigations; 2018. Available from: https://www.iso.org/standard/69038.html.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Refractive and Visual Outcomes of a Monofocal Non-Constant Aberration Aspheric Intraocular Lens
Hernández-Martínez A, Díaz-del-Rio MA, Ruiz-Santos M, Ruiz-Mesa R, Tañá-Rivero P
Clinical Ophthalmology 2022, 16:2521-2530
Published Date: 10 August 2022
The REVIVE Study: Long Term Outcomes of a Novel Non-Diffractive Extended Vision IOL versus Monofocal Control IOL
Shafer BM, McCabe C, Reiser H, Newsom TH, Berdahl J
Clinical Ophthalmology 2022, 16:3945-3950
Published Date: 28 November 2022
Rotational Stability After Implantation of an Aspheric Toric Monofocal IOL with a Double C-Loop Haptic Design in Normal and High Axial Lengths
Ang RET, Tañá-Rivero P, Pastor-Pascual F, Stodulka P, Slovak M, Tetz M, Fischinger I, Cazal J, Gessa M, Ibarz-Barberá M, Holland D, Groneberg T
Clinical Ophthalmology 2025, 19:2393-2403
Published Date: 19 July 2025
Visual and Refractive Outcomes After Implantation of an Isofocal Optic-Design Intraocular Lens with Double C-Loop Haptics in Japanese Eyes
Akahoshi T
Clinical Ophthalmology 2025, 19:2453-2462
Published Date: 29 July 2025
Clinical Outcomes of a Multicenter Study Following Implantation of an Isofocal Optic IOL with Double C-Loop Haptics
Daya S, Akahoshi T, Bosc C, Mouchel R, Chassain C, Van Acker E, Di Maria A, Fogagnolo P
Clinical Ophthalmology 2025, 19:3121-3131
Published Date: 2 September 2025