Back to Journals » Infection and Drug Resistance » Volume 19
Root Cause Analysis for Outbreaks of Carbapenem-Resistant Acinetobacter baumannii and Pseudomonas aeruginosa in a Pediatric Intensive Care Unit: A Retrospective Study
Authors Peng W, Hao Y, Ding H, Wang Z, Tan K, Tan L
Received 14 February 2026
Accepted for publication 3 May 2026
Published 22 May 2026 Volume 2026:19 598824
DOI https://doi.org/10.2147/IDR.S598824
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemant Joshi
Weijun Peng, Youhua Hao, Honghui Ding, Zhenling Wang, Kun Tan, Li Tan
Department of Hospital Infection Control, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China
Correspondence: Li Tan, Email [email protected] Kun Tan, Email [email protected]
Objective: Children in the pediatric intensive care unit (PICU) are inherently susceptible to multidrug-resistant (MDR) bacterial infections due to physiological vulnerabilities and clinical management-related factors. Such infections are prone to outbreaks and confer substantial harm. This study aims to investigate the etiologies of carbapenem-resistant Acinetobacter baumannii (CRAB) and carbapenem-resistant Pseudomonas aeruginosa (CRPA) infection outbreaks in the PICU and develop targeted prevention and control strategies using the root cause analysis (RCA) approach.
Methods: A retrospective analysis was conducted on five cases (n=5) of MDR infection clusters admitted to the PICU of a large comprehensive hospital from January to February 2024. RCA was applied to identify underlying causes, develop targeted interventions, and evaluate their effectiveness.
Results: From 31 January to 18 February 2024, four CRAB strains and three CRPA strains were detected among five patients (n = 5). Environmental sampling (145 specimens) revealed CRAB in four sites (crane tower, handwashing basin wall, healthcare workers’ hands, and PDA devices) and CRPA in two sites (fiberoptic bronchoscopes and healthcare workers’ hands). Post-intervention, no further MDR clusters were observed in 2024, indicating effective control.
Conclusion: RCA facilitates systematic identification of root causes for MDR outbreaks, enabling targeted interventions to curb transmission and strengthen infection control practices.
Keywords: root cause analysis, pediatric intensive care unit, multidrug-resistant bacteria, carbapenem-resistant Acinetobacter baumannii, carbapenem-resistant Pseudomonas aeruginosa, outbreak
Introduction
Children admitted to the Pediatric Intensive Care Unit (PICU) are particularly vulnerable to multidrug-resistant (MDR) bacterial infections due to severe underlying conditions, immature immune systems, frequent invasive procedures, and extensive antibiotic exposure.1,2 Among these pathogens, carbapenem-resistant Acinetobacter baumannii (CRAB) and carbapenem-resistant Pseudomonas aeruginosa (CRPA) represent the most clinically significant MDR Gram-negative organisms within PICU. These pathogens are associated with life-threatening conditions including lower respiratory tract infections, bloodstream infections, and disseminated disease. Their extensive resistance profiles drastically limit therapeutic options for critically ill pediatric patients, consequently elevating mortality risks and escalating healthcare expenditures.3,4 CRAB demonstrates exceptional environmental persistence, whereas CRPA transmission frequently correlates with contaminated medical equipment and aqueous reservoirs. Both organisms disseminate efficiently via healthcare workers’ hands, fomites, and environmental surfaces, often precipitating nosocomial clusters and outbreaks that impose substantial clinical burdens and operational challenges on healthcare systems.5
Root Cause Analysis (RCA) is a structured, retrospective approach to investigating adverse events, aiming to identify fundamental causes and implement preventive measures. This method focuses on exploring fundamental and systemic causes rather than simply attributing problems to individuals. By revealing potential management loopholes and process deficiencies, it helps formulate targeted and sustainable interventions to prevent the recurrence of similar incidents.6 Accordingly, RCA has been increasingly applied in the investigation and control of nosocomial infection outbreaks in recent years. It can assist medical institutions in identifying key transmission links, optimizing infection prevention and control protocols, and effectively blocking pathogen transmission.7,8 However, studies that apply a complete RCA framework specifically to the investigation and control of concurrent outbreaks of CRAB and CRPA in PICU remain relatively limited.
This study used RCA to explore the causes of CRAB and CRPA infection outbreaks in the PICU. Targeted interventions were implemented to block pathogen transmission and prevent recurrence. We aimed to provide practical references for the investigation and control of MDR outbreaks in clinical practice.
Methods
Study Population
The study was conducted in the PICU of a large comprehensive hospital in Wuhan, China. Five clustered cases of MDR infections occurring between 31 January and 18 February 2024, were included. The study was approved by the Ethics Committee of Tongji Hospital (TJ-IRB202410013). Given the retrospective nature of the study, the requirement for written informed consent was waived by the Ethics Committee. Strict confidentiality was maintained for all patient data, and all personal identifiers were protected to ensure privacy. The verbal informed consent procedure obtained from the legal guardians of pediatric patients was also reviewed and approved by the Ethics Committee. All research procedures were conducted in accordance with the Declaration of Helsinki.
Epidemiological Investigation
A retrospective analysis was performed, with data retrieved from the Xinglin Hospital Infection Real-time Monitoring System, Hospital Information System (HIS), and Laboratory Information Management System (LIS), and supplemented by on-site verification. The collected data encompassed four core dimensions: demographic characteristics (age and sex) of participants; clinical profiles including admission diagnoses, invasive procedures performed, and antimicrobial administration details; microbiological findings covering specimen types, pathogen identification results, and antimicrobial susceptibility test outcomes; and clinical outcomes (treatment efficacy and prognosis).
Environmental Sampling and Microbiological Testing
The hospital infection control department conducted environmental hygiene monitoring of the PICU. The high-touch surfaces (bed rails, monitors, infusion pumps, handwashing basins), healthcare workers’ hands, medical equipment (fiberoptic bronchoscopes, ventilator components), air and water sources, etc., are sampled with reference to the corresponding norms, and then inoculated on ordinary nutrient agar dishes to detect the number of bacterial colonies. For detection of MDR, samples were inoculated onto CHROMagar selective media for CRAB and carbapenem-resistant Klebsiella pneumoniae (CRKP). Since Pseudomonas aeruginosa can grow on this selective medium and a dedicated selective medium for CRPA was not available in our laboratory, we used the above CRAB/CRKP medium for CRPA screening to ensure comprehensive detection of the three major carbapenem-resistant Gram-negative pathogens. All samples were inoculated within 4 hours after sampling and incubated at 36±1°C for 48 hours. Target colonies were screened according to colony morphology, and culture-positive specimens were identified using the VITEK 2-Compact fully automatic microbiological identifier (bioMérieux, France). Antimicrobial susceptibility testing was performed using the Kirby–Bauer disk diffusion method, with results interpreted according to CLSI 2014 guidelines.9
Root Cause Analysis
The RCA team was a multidisciplinary group consisting of infectious disease physicians, microbiologists, infection control specialists, ward medical staff, medical and nursing department managers, and logistics staff. All members received standardized RCA training. The RCA team constructed a timeline and investigated from the dimensions of “person–machine–material–method–environment”. Discrepancies with MDR prevention and control protocols were defined as direct causes. Direct causes were analyzed stepwise to determine root causes, presented in a fishbone diagram (Figure 1). The 5W1H framework (What, Why, Who, When, Where, How) was used to structure the RCA and intervention design.
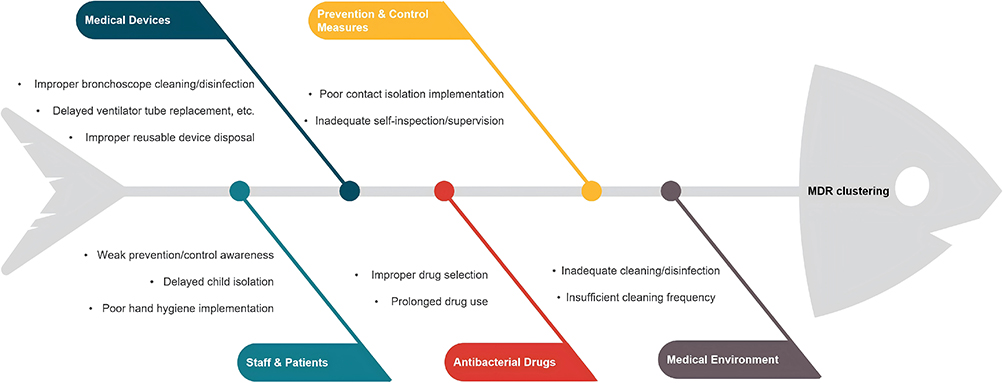 |
Figure 1 Fishbone diagram of root cause analysis (RCA) for CRAB and CRPA clustered infection outbreaks in the PICU. Root causes were systematically analyzed in accordance with the standard framework (Staff & Patients, Medical Devices, Antibacterial Drugs, Prevention & Control Measures, Medical Environment), so as to identify root causes of MDR bacterial clustering transmission. |
Statistical Analysis
Categorical variables are presented as frequencies and percentages. This study mainly adopted descriptive statistics. The limited number of outbreak cases restricted statistical power, which is common and understandable in investigations of single infectious disease outbreaks. This limitation is clearly stated in the Discussion section.
Results
Outbreak Identification
Between January 31 and February 18, 2024, five patients tested positive for MDR bacteria: four with CRAB and three with CRPA (one patient had concurrent CRAB and CRPA), and the antimicrobial susceptibility profiles of the same type of bacteria detected in different patients are completely consistent. All cases were classified as Hospital Acquired Infections (HAI) except one suspected colonization, which was classified as a Class II medical safety adverse event, defined as an event that has caused actual harm or potential risk to patients and requires intervention to prevent adverse outcomes. Clinical details are summarized in Table 1.
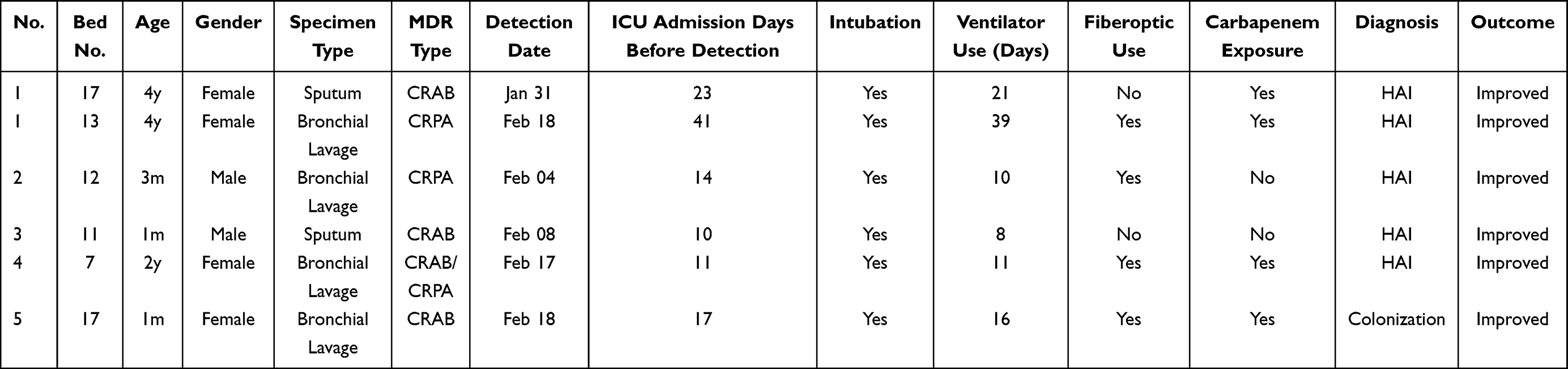 |
Table 1 Clinical Characteristics of 5 Patients with MDR Infections in PICU |
Epidemiological Investigation
Population Distribution
Among the five patients with detected MDR, 2 are boys and 3 are girls, with a mean age of 1.28 years. All five patients had been hospitalized in the PICU for over 10 days prior to MDR detection; 4 had undergone fiberoptic bronchoscopy, and 3 had received carbapenem antibiotics before detection. All patients were discharged after treatment.
Temporal Distribution
The first CRAB case was detected on January 31, 2024, followed by CRPA on February 4, 2024, with sporadic cases until February 17, 2024 (Figure 2).
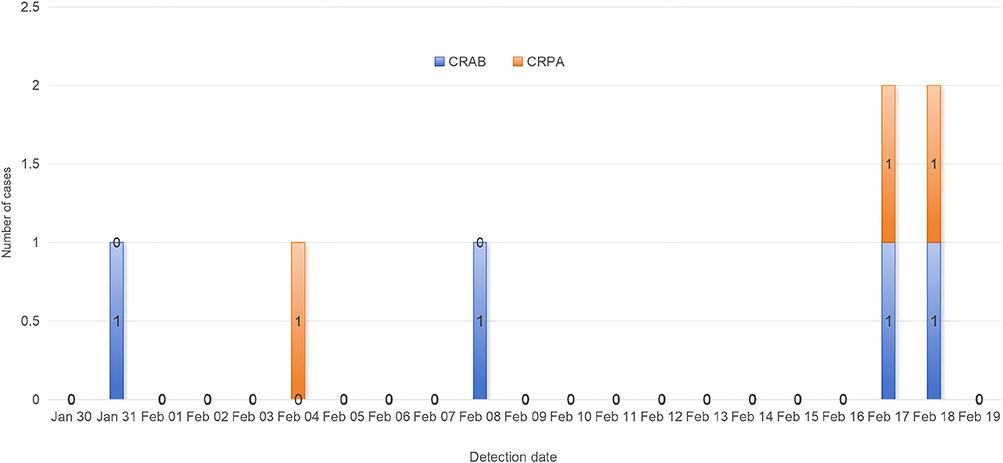 |
Figure 2 Temporal distribution of CRAB and CRPA detection cases during the outbreak investigation period (January 31 to February 18, 2024). Blue bars represent CRAB positive cases, Orange bars represent CRPA positive cases. The vertical axis indicates the number of daily detected cases. |
Spatial Distribution
CRAB cases were dispersed, while CRPA cases clustered in adjacent beds (Figure 3).
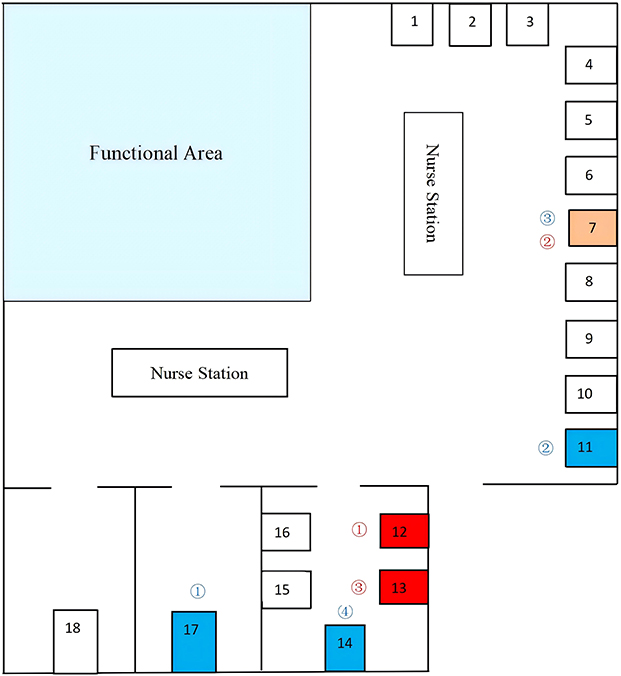 |
Figure 3 Blue marking for patients with CRAB detection, red marking for patients with CRPA detection; Orange marking for double detection; of which, bed 17 and bed 13 are the same patient was detected at different time points: after CRAB became negative, it was transferred to bed 13 and then CRPA was detected; blue ①~④ is the order of CRAB detection, and red ①~③ is the order of CRPA detection. |
Device Association
Four patients underwent fiberoptic bronchoscopy. Shared bronchoscopes showed CRPA in rinsing fluid, with matching antimicrobial profiles.
Environmental Hygiene Testing
Environmental hygiene sampling was carried out on February 21,2024, and of 145 environmental samples, 4 (2.76%) tested positive for CRAB and 2 (1.38%) for CRPA (Table 2). Contaminated sites included: CRAB: Crane tower (20.0%), Personal Digital Assistant (PDA, 20.0%), handwashing basin wall (12.5%), healthcare workers’ hands (10.0%); CRPA: Fiberoptic bronchoscopes (25.0%), healthcare workers’ hands (10.0%).
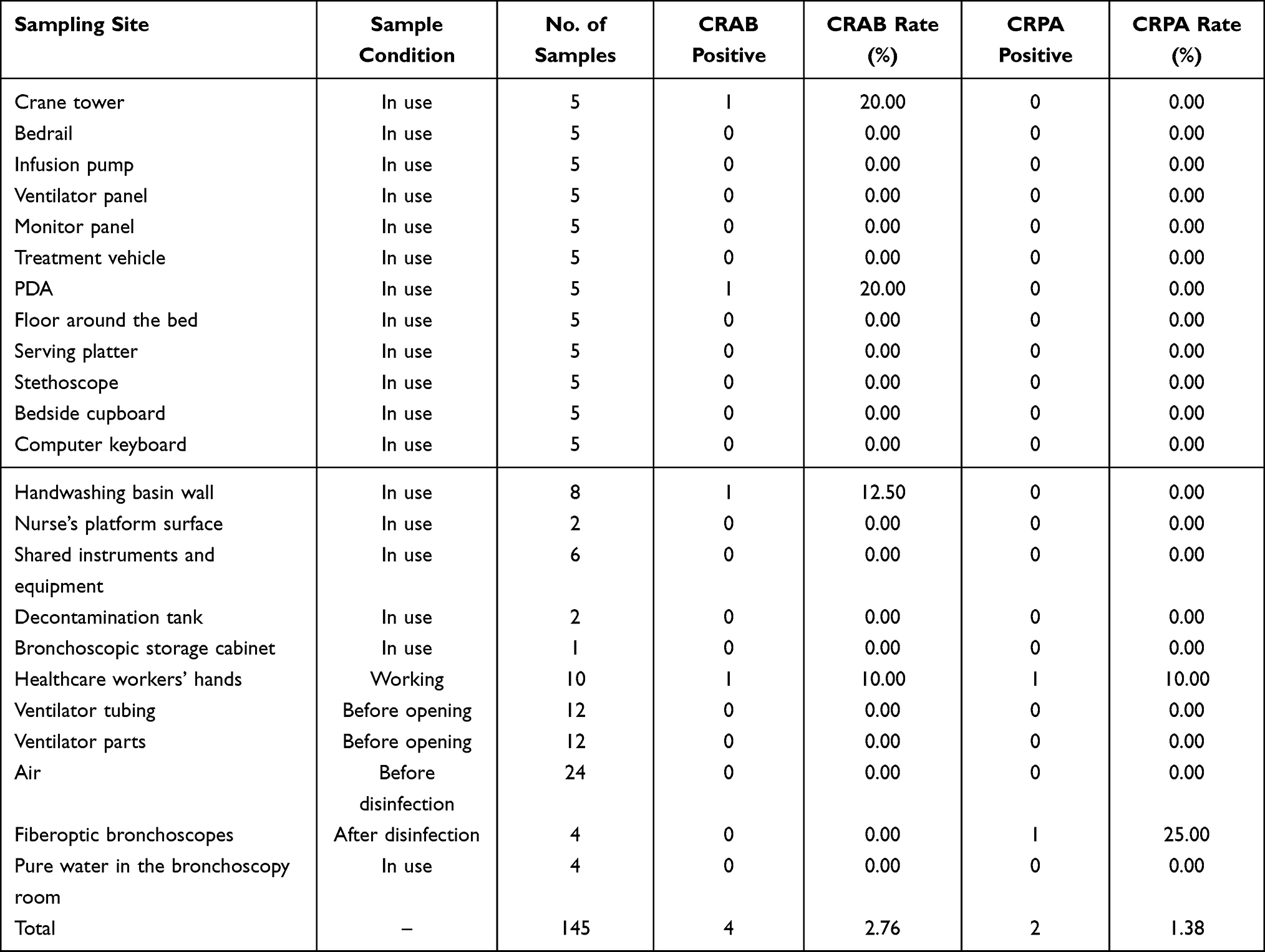 |
Table 2 Environmental Surveillance Results in the PICU |
Interventions and Outcomes
Based on RCA findings, targeted interventions were formulated by the 5W1H principle, as summarized below:
Enhanced Isolation
Cluster patients in dedicated isolation wards, and the bedside isolation measures are strictly implemented; MDR-infected patients are strictly under the care of specialists; restrict visitor access, and the medical staff entering and exiting the ward are strictly implementing the contact and isolation measures.
Hand Hygiene and Training
Mandatory education on MDR transmission for medical staff; real-time supervision of hand hygiene compliance.
Environmental Disinfection
Quaternary ammonium wipes for high-touch surfaces and strictly “one wipe per surface”; cleaning staff using 500 mg/L chlorine for patient zones; 1,000 mg/L chlorine for handwashing basins; and the air-conditioning vents are cleaned and disinfected by the property staff.
Equipment Management
Strictly implement the process of cleaning and disinfection of fibrilloscopes, and then send four fibrilloscopes to the Disinfection and Supply Center for sterilisation and treatment before fixing one fibrilloscope for the exclusive use of MDR patients, and replace the disinfectant from glutaraldehyde to o-phthalaldehyde (OPA). Contact the ventilator manufacturer to clean and sterilise the relevant intraventilator tubes of positively detected patients.
Antimicrobial Stewardship
Pharmacy-led prescription reviews were performed, and an approval mechanism for special-grade and restricted antibiotics was adopted to standardize and appropriately restrict carbapenem use in the PICU.
After the implementation of the above measures, the implementation status and effectiveness of each measure were continuously tracked. From February 21 to March 6, there were no new patients with multidrug-resistant (MDR) bacterial infections in the PICU, and the outbreak was terminated. By December 31, 2024, no MDR clustering events had occurred in the PICU, confirming that the intervention and control measures were effective.
Discussion
Our key findings confirm RCA’s value in managing PICU MDR outbreaks. A cluster of 5 CRAB/CRPA HAI/colonization cases (Jan 31–Feb 18, 2024) involved transmission via healthcare workers’ hands, poorly reprocessed bronchoscopes, and high-touch surfaces. Targeted interventions rapidly halted the outbreak with no 2024 recurrence, highlighting RCA’s role in addressing infection control gaps.
Consistent with previous studies,10,11 reinforcing standard infection prevention and control measures (eg., hand hygiene, contact isolation, environmental cleaning and disinfection) proved critical for controlling MDR spread in the PICU. Healthcare workers’ hands are well-documented as a major vector for cross-transmission of MDR bacteria in ICUs,12 and improved hand hygiene compliance significantly reduces transmission risk via contaminated hands. Environmental surfaces in ICUs are another important medium for transient and cross-transmission of MDR bacteria, as their physicochemical properties allow pathogens such as CRAB to survive for days to months.10 Intensive cleaning and disinfection of these surfaces effectively reduces environmental pathogen load, thereby decreasing MDR colonization and spread.13 Early single-room or centralized isolation of MDR patients with dedicated nursing care further interrupts transmission chains,14,15 and these standardized preventive measures are both effective and cost-effective for MDR control.16 Their effectiveness in our PICU may be attributed to the relatively low baseline MDR prevalence.17
Fiberoptic bronchoscopy is widely used clinically for treating lung infections, as it facilitates the timely removal of infectious agents, improves lung ventilation, and reduces inflammation.18,19 However, our study identified fiberoptic bronchoscopes as a critical transmission vector, with CRPA detected in disinfected devices—consistent with reports of inadequate reprocessing enabling cross-infection.20,21 Switching to OPA (a more effective disinfectant for endoscopes) and designating dedicated bronchoscopes for MDR patients eliminated this risk, highlighting the need for rigorous reprocessing protocols and dedicated equipment for high-risk patients.
CRAB was also detected on the walls of bedside handwashing basins, suggesting that contaminated handwashing facilities may serve as MDR transmission vectors. Consistent with relevant studies and guidelines,22,23 this finding supports the need to strengthen disinfection of handwashing sinks or remove unnecessary sinks in critical care settings. Additionally, irrational antimicrobial use is a well-established root cause of MDR infections. Several studies have shown that CRPA is highly likely to be induced by carbapenem use (eg., meropenem) in PICU patients, and the benefits of meropenem administration may not outweigh the risk of inducing CRPA.24,25 Clinicians should therefore exercise caution when prescribing carbapenems in the PICU.
Determining the cause of an outbreak is one of the most difficult aspects of the investigation and disposition of previous hospital infection outbreaks, and often the source cannot be identified even until the outbreak is over. Conventional epidemiological investigations are often limited by the level of the investigator and are unable to comprehensively and accurately reveal the cause of the outbreak, and some studies have shown that less than half of the outbreaks have found the source of the outbreak.26 Through the application of root cause analysis, the root cause of adverse events such as similar nosocomial outbreaks can be identified in a timely and comprehensive manner with the help of a multidisciplinary team and scientific methods, so that the proliferation of outbreaks can be controlled as soon as possible, and the risk of the reoccurrence of such events can be effectively reduced,27,28 which is crucial for the investigation and disposal of outbreaks.
Despite its contributions, this study has several limitations. First, it employed a single-center design, which may limit the generalizability of findings to other PICU with different patient populations, resource availability, or infection control practices. Second, whole-genome sequencing (WGS) was not performed to confirm the genetic relatedness of clinical and environmental isolates, which would have strengthened causal links between environmental contamination and patient infections.29 Third, no quantitative data on healthcare worker compliance with infection control measures (eg., hand hygiene adherence rates pre- and post-intervention) were collected, making it difficult to directly link changes in compliance to outbreak control. Fourth, only one round of environmental sampling was conducted on February 21, 2024, which may not reflect the dynamic changes in environmental contamination during the entire outbreak. Fifth, this study mainly used descriptive statistics, and the limited number of cases (n=5) restricted statistical power. Although these constraints are common and understandable in outbreak investigations, they should be noted as limitations.
Conclusion
RCA facilitates systematic identification of root causes for CRAB and CRPA outbreaks in the PICU, enabling targeted interventions to curb transmission and strengthen infection control practices. Although this study is limited by its single-center design and small sample size, the RCA approach shows broad applicability and practical value in the investigation and control of MDR bacterial outbreaks, and can provide a useful reference for infection control management in similar pediatric intensive care settings.
Funding
Hubei Provincial Natural Science Foundation Project: Mechanism Study on the Influence of Hospital Infection Prevention and Control Behavior Model Based on Human Factors Engineering on Execution Efficiency (Grant No. 2023AFB132); Soft Science Research Project of Tongji Hospital: Study on the Construction of Hospital Infection Risk Management System (No. 3).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Havan M, Kendirli T, Parlar ÖT, et al. Clinical management of a pandrug-resistant OXA-48 Klebsiella pneumoniae infection in the pediatric intensive care unit. Microb Drug Resist. 2023;29(6):256–10. doi:10.1089/mdr.2022.0247
2. Bazaid AS, Aldarhami A, Bokhary NA, et al. Prevalence and risk factors associated with drug resistant bacteria in neonatal and pediatric intensive care units: a retrospective study in Saudi Arabia. Medicine. 2023;102(42):e35638. doi:10.1097/MD.0000000000035638
3. Zhang Y, Xu G, Miao F, et al. Insights into the epidemiology, risk factors, and clinical outcomes of carbapenem-resistant Acinetobacter baumannii infections in critically ill children. Front Public Health. 2023;11:1282413. doi:10.3389/fpubh.2023.1282413
4. Huang W, Wei X, Xu G, et al. Carbapenem-resistant Pseudomonas aeruginosa infections in critically ill children: prevalence, risk factors, and impact on outcome in a large tertiary pediatric hospital of China. Front Public Health. 2023;11:1088262. doi:10.3389/fpubh.2023.1088262
5. Wang X, Du Z, Huang W, et al. Outbreak of multidrug-resistant Acinetobacter baumannii ST208 producing OXA-23-like carbapenemase in a Children’s Hospital in Shanghai, China. Microb Drug Resist. 2021;27(6):816–822. doi:10.1089/mdr.2019.0232
6. Singh G, Patel RH, Vaqar S, et al. Root cause analysis and medical error prevention. In: StatPearls. Internet. StatPearls Publishing; 2024.
7. Jiang S, Yi L, Chen Y, et al. Optimizing sterilization packaging through root cause analysis: an exploration into sealing defects of paper-plastic pouches. Med Sci Monit. 2023;29:e940342. doi:10.12659/MSM.940342
8. Troelsen FS, Sorensen HT, Pedersen L, et al. Root-cause analysis of 762 Danish post-colonoscopy colorectal cancer patients. Clin Gastroenterol Hepatol. 2023;21(12):3160–3169. doi:10.1016/j.cgh.2023.03.034
9. Humphries R, Bobenchik AM, Hindler JA, et al. Overview of changes to the clinical and laboratory standards institute performance standards for antimicrobial susceptibility testing, M100, 31st edition. J Clin Microbiol. 2021;59(12):e21321. doi:10.1128/JCM.00213-21
10. Karampatakis T, Tsergouli K, Roilides E. Infection control measures against multidrug-resistant Gram-negative bacteria in children and neonates. Future Microbiol. 2023;18(11):751–765. doi:10.2217/fmb-2023-0072
11. Kim D, Lee H, Choi J-S, et al. The changes in epidemiology of imipenem-resistant Acinetobacter baumannii bacteremia in a pediatric intensive care unit for 17 years. J Korean Med Sci. 2022;37(24):e196. doi:10.3346/jkms.2022.37.e196
12. Gajic I, Jovicevic M, Milic M, et al. Clinical and molecular characteristics of OXA-72-producing Acinetobacter baumannii ST636 outbreak at a neonatal intensive care unit in Serbia. J Hosp Infect. 2021;112:54–60. doi:10.1016/j.jhin.2021.02.023
13. Thatrimontrichai A, Pannaraj PS, Janjindamai W, et al. Intervention to reduce carbapenem-resistant Acinetobacter baumannii in a neonatal intensive care unit. Infect Control Hosp Epidemiol. 2020;41(6):710–715. doi:10.1017/ice.2020.35
14. Tomczyk S, Zanichelli V, Grayson ML, et al. Control of carbapenem-resistant enterobacteriaceae, Acinetobacter baumannii, and Pseudomonas aeruginosa in healthcare facilities: a systematic review and reanalysis of quasi-experimental studies. Clin Infect Dis. 2019;68(5):873–884. doi:10.1093/cid/ciy752
15. Yin L, He L, Miao J, et al. Actively surveillance and appropriate patients placements’ contact isolation dramatically decreased Carbapenem-resistant Enterobacteriaceae infection and colonization in pediatric patients in China. J Hosp Infect. 2020;104(Suppl 1):S124–S130.
16. Seesahai J, Church PT, Asztalos E, et al. Neonates with Maternal Colonization of Carbapenemase-Producing, Carbapenem-Resistant Enterobacteriaceae: A Mini-Review and a Suggested Guide for Preventing Neonatal Infection. Children. 2021;8(5):412. doi:10.3390/children8050412
17. Kim B, Kim K, Yoon J-S. Nosocomial Acinetobacter baumannii infection in children in adult versus pediatric intensive care units. Pediatr Int. 2020;62(4):451–458. doi:10.1111/ped.14133
18. Liang Y, Jiang X, Ma L, et al. Diagnostic value and safety of ultrathin bronchoscope and endobronchial ultrasonography with a guide sheath combined with rapid on-site evaluation system for peripheral pulmonary infectious diseases. Minerva Surg. 2023;78(1):37–44. doi:10.23736/S2724-5691.22.09597-1
19. Eom JS, Park S, Jang H, et al. Bronchial washing using a thin versus a thick bronchoscope to diagnose pulmonary tuberculosis: a randomized trial. Clin Infect Dis. 2023;76(2):238–244. doi:10.1093/cid/ciac789
20. Guy M, Vanhems P, Dananche C, et al. Outbreak of pulmonary Pseudomonas aeruginosa and Stenotrophomonas maltophilia infections related to contaminated bronchoscope suction valves, Lyon, France, 2014. Euro Surveill. 2016;21(28):16–00798. doi:10.2807/1560-7917.ES.2016.21.28.30286
21. Mehta AC, Muscarella LF. Bronchoscope-related “superbug” infections. Infect Chest. 2020;157(2):454–469. doi:10.1016/j.chest.2019.08.003
22. Zeng M, Xia J, Zong Z, et al. Guidelines for the diagnosis, treatment, prevention and control of infections caused by carbapenem-resistant gram-negative bacilli. J Microbiol Immunol Infect. 2023;56(4):653–671. doi:10.1016/j.jmii.2023.01.017
23. Low JM, Chan M, Low JL, et al. The impact of sink removal and other water-free interventions in intensive care units on water-borne healthcare-associated infections: a systematic review. J Hosp Infect. 2024;150:61–71. doi:10.1016/j.jhin.2024.05.012
24. Lutsar I, Chazallon C, Trafojer U, et al. Meropenem vs standard of care for treatment of neonatal late onset sepsis (NeoMero1): a randomised controlled trial. PLoS One. 2020;15(3):e0229380. doi:10.1371/journal.pone.0229380
25. Romandini A, Pani A, Schenardi PA, et al. Antibiotic Resistance in Pediatric Infections: Global Emerging Threats, Predicting the Near Future. Antibiotics. 2021;10(4):376. doi:10.3390/antibiotics10040376
26. Dramowski A, Aucamp M, Bekker A, et al. Infectious disease exposures and outbreaks at a South African neonatal unit with review of neonatal outbreak epidemiology in Africa. Int J Infect Dis. 2017;57:79–85. doi:10.1016/j.ijid.2017.01.026
27. Lakbala P, Bordbar N, Fakhri Y. Root cause analysis and strategies for reducing falls among inpatients in healthcare facilities: a narrative review. Health Sci Rep. 2024;7(7):e2216. doi:10.1002/hsr2.2216
28. Lee J-Y, Huang C-H, Sie Y-A, et al. Applying the human factors analysis and classification system within root cause analysis to prevent medical errors and enhancing patient safety culture: insights from a medical center. Int J Qual Health Care. 2025;37(1):czad007. doi:10.1093/intqhc/mzaf009
29. Gramatniece A, Silamikelis I, Zahare I, et al. Control of Acinetobacter baumannii outbreak in the neonatal intensive care unit in Latvia: whole-genome sequencing powered investigation and closure of the ward. Antimicrob Resist Infect Control. 2019;8(1):84. doi:10.1186/s13756-019-0537-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.