")
Back to Journals » International Journal of General Medicine » Volume 16
Roles of Gut Microbiota in Alcoholic Liver Disease
Authors Zhang D , Liu Z, Bai F
Received 6 May 2023
Accepted for publication 10 August 2023
Published 23 August 2023 Volume 2023:16 Pages 3735—3746
DOI https://doi.org/10.2147/IJGM.S420195
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Hyam Leffert
Daya Zhang,1,* ZhengJin Liu,2,* Feihu Bai2,3
1Graduate School, Hainan Medical University, Haikou, People’s Republic of China; 2Department of Gastroenterology, The Second Affiliated Hospital of Hainan Medical University, Haikou, People’s Republic of China; 3The Gastroenterology Clinical Medical Center of Hainan Province, Haikou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Feihu Bai, Chief Physician and Professor of Department of Gastroenterology, The Second Affiliated Hospital of Hainan Medical University, Yehai Avenue, #368, Longhua District, Haikou, Hainan Province, 570216, People’s Republic of China, Tel +86-18995181963, Fax +86898-66809168, Email [email protected]
Abstract: Alcoholic liver disease (ALD)—one of the most common liver diseases — involves a wide range of disorders, including asymptomatic hepatic steatosis, alcoholic hepatitis (AH), liver fibrosis, and cirrhosis. Alcohol consumption induces a weakened gut barrier and changes in the composition of the gut microbiota. The presence of CYP2E1 and its elevated levels in the gastrointestinal tract after alcohol exposure lead to elevated levels of ROS and acetaldehyde, inducing inflammation and oxidative damage in the gut. At the same time, the influx of harmful molecules such as the bacterial endotoxin LPS and peptidogly from gut dysbiosis can induce intestinal inflammation and oxidative damage, further compromising the intestinal mucosal barrier. In this process, various oxidative stress-mediated post-translational modifications (PTMs) play an important role in the integrity of the barrier, eg, the presence of acetaldehyde will result in the sustained phosphorylation of several paracellular proteins (occludin and zona occludens-1), which can lead to intestinal leakage. Eventually, persistent oxidative stress, LPS infiltration and hepatocyte damage through the enterohepatic circulation will lead to hepatic stellate cell activation and hepatic fibrosis. In addition, probiotics, prebiotics, synbiotics, fecal microbial transplantation (FMT), bioengineered bacteria, gut-restricted FXR agonists and others are promising therapeutic approaches that can alter gut microbiota composition to improve ALD. In the future, there will be new challenges to study the interactions between the genetics of individuals with ALD and their gut microbiome, to provide personalized interventions targeting the gut-liver axis, and to develop better techniques to measure microbial communities and metabolites in the body.
Keywords: alcoholic liver disease, gut dysbiosis, modulators
Introduction
With socioeconomic development, lifestyle changes, and increased social openness, alcohol abuse, alcohol dependence, and alcoholism have become one of the most serious public health problems worldwide. In 2016, it was reported that 32.5% of the world’s population drinks alcohol, of which 1.5 billion are male drinkers and 900 million are female consumers.1 However, alcohol consumption varies from one country to another.2 In the same year, alcohol ranked seventh among risk factors for disability or death and was the leading risk factor for dangerous diseases in people aged 15–49 years.1 Alcoholic liver disease (ALD) is the most widespread type of chronic liver disease globally. ALD can be classified as mild alcoholic liver disease, alcoholic hepatic steatosis, alcoholic hepatitis, alcoholic liver fibrosis, and alcoholic liver cirrhosis.3 In 2017, alcohol-related liver cirrhosis and cancer accounted for 1% of all deaths, and this is expected to increase in the future.1,4 The prevalence of ALD in Asia has increased significantly from 3.82% in 2000–2010 to 6.62% in 2011–2020, and ALD is expected to be the leading cause of chronic liver disease in Asia.5 China is currently the second largest alcohol consumer worldwide.6,7 Alcohol has also become the second leading cause of liver injury after viral hepatitis.8 A Chinese survey has shown that the drinking rate of adult residents in Liaoning Province is 35.30%, while the drinking rate, hazardous drinking rate, and harmful drinking rate of residents in Tongzhou District of Beijing were 45.29, 3.63, and 4.03% respectively.9,10
The pathogenesis of ALD has not been fully elucidated. Current studies mainly evaluate the direct toxic effects of ethanol and its metabolites on the liver, oxidative stress, lipid metabolism, autophagy, genetics, gender, non-coding RNAs, and the gut microbiome. Early stages of ALD are not often accompanied by obvious symptoms. Traditional biochemical testing methods are less sensitive, and histopathological testing is invasive. Currently, no effective drugs are approved for the treatment of patients with ALD.11 Although abstinence from alcohol is the basic treatment for all stages of ALD, patient compliance is poor. When the disease progresses to advanced stages, liver transplantation is the only effective treatment. End-stage liver disease not only causes physical and mental burdens to patients and their families but also causes great socioeconomic pressure.12
ALD has several unmet clinical needs and challenges, including noninvasive screening methods for disease diagnosis and prognostic assessment, development of therapeutic targets, and selection criteria for liver transplant patients. This review summarizes the relationship between gut dysbiosis and ALD to provide new strategies for the treatment of ALD.
Gut Microbiome
The gut microbiota contains numerous bacteria, archaea, fungi, and viruses. The number of bacteria in the gut is similar to that of human cells.13,14 Although the human microbiome has a genome of over 3 million genes, it is far more complex than the human genome.13,14 Thickobacterium and Bacillus are the two most dominant bacterial phyla in the gut, accounting for almost 90% of all bacteria; the former includes over 200 different genera (eg, Lactobacillus, Bacillus, Clostridium, and Enterococcus).15 Approximately 85% of bacteria (such as Lactobacillus and Bifidobacterium) are commensal organisms, while the rest (such as Clostridium and Clostridium) may be pathogenic.16 Studies have confirmed that normal gut microbiota not only participates in the digestion, decomposition, synthesis, and absorption of substances in the intestinal lumen, provides nutritional support to intestinal mucosal cells, and maintains normal physiological functions of the body but also resists the colonization and growth of foreign bacteria, activates the intestinal immune system, and constitutes an intestinal mucosal barrier together with intact intestinal mucosal epithelial cells.
The various biological functions of the liver are related to the normal gut microbiota. Bile acids secreted by the liver can inhibit pathogenic bacteria in the gut and regulate the balance of gut microbiota. Additionally, gut microbiota metabolites can participate in the metabolism of fats, proteins, sugars, vitamins, and hormones by the liver through enterohepatic circulation. All imbalances or alterations in the taxonomic composition and/or function of the gut microbiota are referred to as “dysbiosis”.17 Currently, various studies have demonstrated that changes in the gut microbiota are associated with diabetes,18 Alzheimer’s disease,19 obesity,20 nephropathy,21 autism,22 polycystic ovary syndrome,23 amyotrophic lateral sclerosis,24 childhood malnutrition,25 premature aging,26 tumors,27 inflammatory bowel disease,28 irritable bowel syndrome,29 and celiac disease.30 Recent studies have shown that liver diseases are closely associated with gut dysbiosis, including chronic viral infections, non-alcoholic fatty liver disease, ALD, and hepatocellular carcinoma.31,32 The liver receives most of the blood from the gut through the portal vein and is, therefore, most exposed to potential bacterial products or metabolites such as lipopolysaccharides, peptidoglycan, short-chain fatty acids, and bile acids.33 Bacterial products or metabolites can activate Kupffer cells, neutrophils, hepatocytes, sinusoidal endothelial cells, and stellate cells, promoting the release of inflammatory mediators (tumor necrosis factor alpha (TNF-α) and interleukin 6 (IL-6)), leading to liver injury and disease.33
The Effect of Alcohol on the Number and Composition of Gut Microbiota
Diets with much fat or sugar can affect the composition of the gut microbiota.34 Excessive alcohol consumption can lead to a predominance of pathogenic bacteria. Mutlu et al35 demonstrated that the ileum and colon of rats gavaged with alcohol daily for 10 weeks showed dysbiosis. It was found that alcohol promoted the growth of Gram-negative bacteria such as the Aspergillus phylum in the gut, thereby reducing the number of anaerobic bacteria such as Bifidobacterium.36 Compared with healthy controls, alcoholics had more Gram-negative anaerobic and aerobic bacteria in their jejunal fluid.37 In the ALD group, the incidence of small intestinal bacterial overgrowth was almost three times higher than that in non-alcoholic controls.38 Alcoholic hepatitis patients have an elevated proportion of cytolytic-positive fecal enterococci, which correlates with the severity and mortality of liver disease.39 In addition to bacteria, the role of gut fungi has attracted considerable attention. Compared with non-alcoholic controls, alcoholics had a lower abundance and diversity of fungal species.40,41 Candida albicans and its exotoxin candidin were found to exacerbate ethanol-induced ALD, which is associated with increased mortality.42 Table 1 summarizes the studies that observed changes in the gut microbiota of ALD patients.
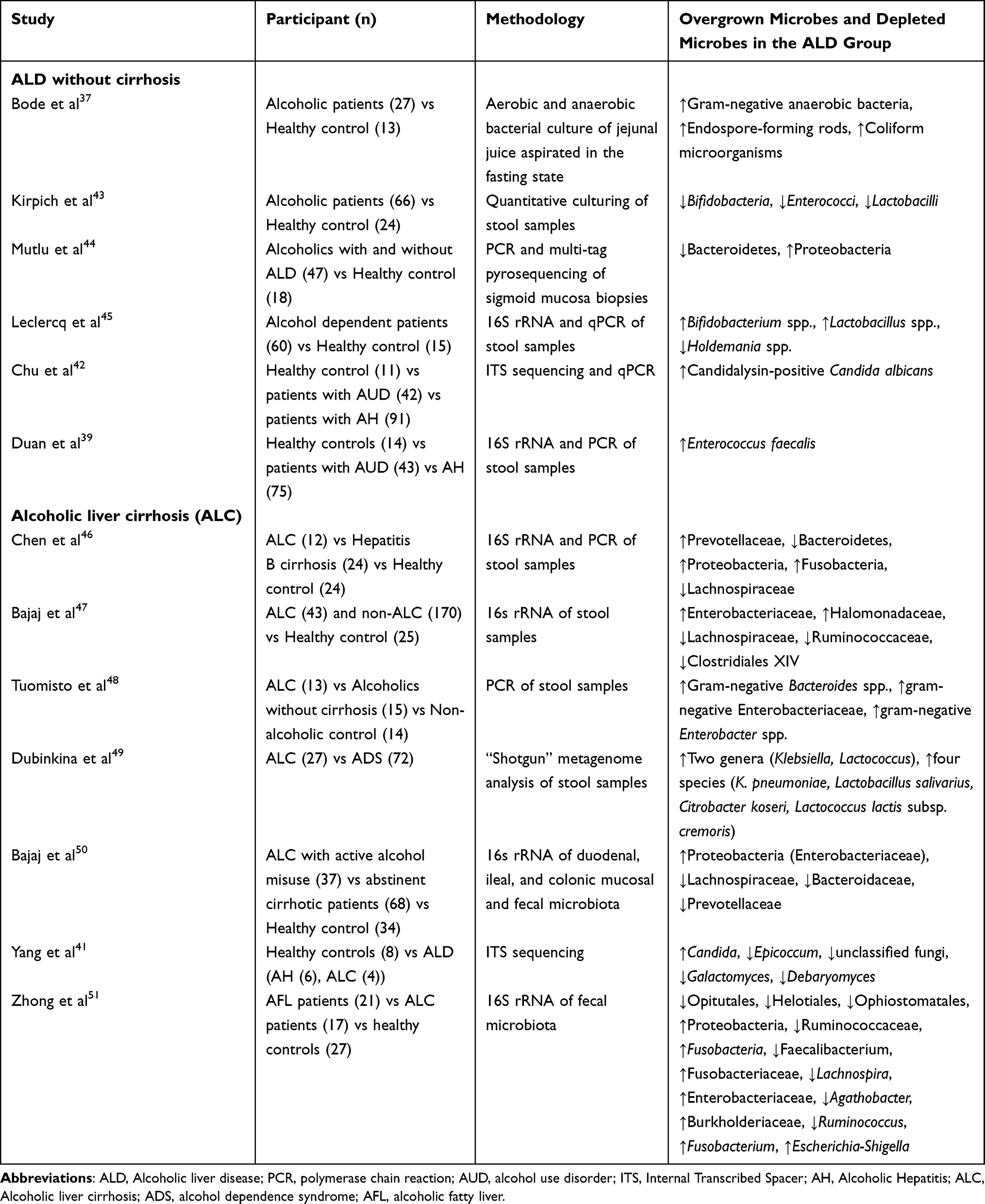 |
Table 1 Studies That Assessed Changes in the Gut Microbiota in ALD Patients |
Numerous animal experiments have confirmed the importance of gut microbiota and their metabolites in ALD. Visapää et al52 used ciprofloxacin in a rat model of ALD and found that the concentration of acetaldehyde in the gut lumen and portal blood was greatly reduced, confirming the role of the gut microbiota in alcohol metabolism. Llopis et al53 used humanized mice and found that the gut microbiota modified the susceptibility of individuals to ALD. In another study, fecal microbes from alcohol-tolerant mice were transplanted into alcohol-sensitive mice, which showed tolerance to alcohol.54
However, the mechanisms by which ethanol alters microbial composition are not known. During alcohol consumption, alcohol is rapidly absorbed by diffusion, mainly in the upper gastrointestinal tract. The effects of alcohol on the distal small intestine and colon arise mainly from the circulation balance between the lumen of the gastrointestinal tract and the vascular space. Little is known about how relatively small concentrations of ethanol in the large intestine cause profound changes in the fecal microbiota.55 Recent studies have shown that ethanol is not directly metabolized by the gut microbiota and that ethanol-related changes in the gut microbiota are a side effect of elevated acetate levels in humans.56
Mechanisms of Alcohol-Induced Intestinal Damage Through Oxidative Stress, Leading to Leaky Gut and Endotoxemia
Typically, intestinal monolayers form tightly connected barriers with various proteins, forming intestinal tight junctions (TJ), adherens junctions (AJ), and bridging particles.57 This barrier keeps microorganisms in the intestinal lumen away from blood flow, while also allowing luminal nutrients to enter the portal vein, thus ensuring a useful, nontoxic blood supply to the recipient organ.58 Disruption of the gut barrier is an important factor in the pathogenesis of ALD, and the main mechanisms are related to alcohol and its metabolite acetaldehyde, impaired small bowel motility,59 changes in gastric acid secretion,60 dysfunction of gut mucosal epithelial cells,61 and increased lipopolysaccharides from enterobacteria. This paragraph will place special emphasis on the mechanisms and effects of gut ecological dysbiosis and alcohol exposure on the intestinal barrier, particularly on increased intestinal permeability. Alcohol and acetaldehyde can cause mucus erosion and ulceration, alter the glycosylation of the protective mucus layer, and increase intestinal permeability.62 Alcohol can be absorbed in the duodenum and jejunum.63 After entering the monolayer by simple diffusion from the mucus layer, ethanol is either metabolized in the barrier or continues to diffuse into the circulation for delivery to various body sites.63 Importantly, ADH is more highly expressed and active in both the small and large intestine compared to ALDH, suggesting a greater accumulation of reactive acetaldehyde than acetate in the monolayer following alcohol metabolism.64 In addition, the presence of CYP2E1 and its elevated levels in the gastrointestinal tract after alcohol exposure due to low levels of ALDH2 expression in the gut65–67 lead to elevated levels of ROS and acetaldehyde, inducing inflammation and oxidative damage in the gut and liver.68,69 Alcohol and acetaldehyde activate the expression of toll-like receptor 4 (TLR4) on gut mucosal cell membranes and protein kinase C activity, thereby inhibiting the expression of cell tight junction-related connexins such as occludin and zona occludens-1.70,71 Studies have reported that alcohol can reduce the secretion of regenerating insulin lectin (REG3) in gut epithelial cells, leading to the parasitization of harmful bacteria in the intestinal mucosa.72–74 At the same time, the resulting dysbiosis of the intestinal ecology alters intestinal metabolism and the influx of harmful molecules such as the bacterial endotoxin LPS and peptidoglycan can induce intestinal inflammation and oxidative damage, further compromising the intestinal mucosal barrier.58 In this process, various oxidative stress-mediated post-translational modifications (PTMs) play an important role in the integrity of the barrier, eg, the presence of acetaldehyde will result in the sustained phosphorylation of several paracellular proteins.75 Continued damage to the barrier can lead to leaky gut, which subsequently leads to a localized immune response in the gut, increased levels of harmful gut-derived compounds (eg, lipopolysaccharides (LPS), peptidoglycans, exosomes, etc.) entering the circulation, resulting in endotoxemia, and more.
Interaction Among Gut Dysbiosis, Intestinal Barrier Dysfunction, and ALD
Alcohol may act as the initiator of liver damage. After the impairment of the intestinal mucosal barrier, translocation of harmful components such as bacteria, bacterial DNA, bacterial peptidoglycan, bacterial flagellin, and endotoxin further contributes to the development and progression of ALD.
Intrinsic immune cells of the liver, Kupffer cell, activation through specific receptors such as toll-like receptors (TLRs) mediated by LPS and oxidative stress driven by metabolism of the ethanol by hepatic CYP2E1 and from activated NOXs, increases large amounts of the pro-inflammatory effect of cytokines such as IL-1, IL-6, TNFα, leukotrienes, platelet-activating factor, oxygen radicals, nitric oxide, nitrous oxide, etc., causing multi-organ failure and secondary liver injury, cirrhosis, hepatocellular carcinoma, or liver failure.52,76–78 Eventually, sustained oxidative stress, LPS infiltration, and hepatocyte damage will lead to hepatic stellate cell activation, resulting in hepatic fibrosis and sustained liver injury.79–81 The pathophysiology of ALD is shown in Figure 1.
 |
Figure 1 Pathogenesis and treatment of alcoholic liver disease. Alcohol consumption induces a weakened gut barrier and changes in the composition of the gut microbiota. The elevated CYP2E1 levels in the gastrointestinal tract after alcohol exposure lead to elevated levels of ROS and acetaldehyde, inducing intestinal inflammation and oxidative damage in the gut. The influx of harmful molecules such as the bacterial endotoxin LPS and peptidogly from gut dysbiosis can also induce inflammation and oxidative damage, further compromising the intestinal mucosal barrier. In this process, various oxidative stress-mediated post-translational modifications (PTMs) play an important role in the integrity of the barrier, eg, the presence of acetaldehyde will result in the sustained phosphorylation of several paracellular proteins (occludin and zona occludens-1), which can lead to intestinal leakage. Eventually, persistent oxidative stress, LPS infiltration and hepatocyte damage through the enterohepatic circulation will lead to hepatic stellate cell activation, hepatic fibrosis and hepatic cirrhosis. |
Intervention of the Gut Microbiota
Recently, there has been a surge in research on whether patients with ALD can be treated with probiotics, prebiotics, synbiotics, fecal microbial transplantation (FMT), bioengineered bacteria, gut-restricted FXR agonists and others by modulating gut microbiota via different mechanisms (Figure 1, Table 2).
 |
Table 2 Clinical Trials Targeting the Intestinal Microbiome in ALD Disease |
Probiotics, Prebiotics, and Synbiotics
The World Health Organization defines probiotics as “living microorganisms that are beneficial to the health of the host”.62 Lactobacillus and Bifidobacterium can fight pathogenic bacteria by promoting the growth of the intestinal epithelium and modulating the host immune system.93–95 In 1994, it was found that feeding Lactobacillus strains that survived in the gastrointestinal tract reduced endotoxemia and liver damage in a rat model of ALD.96 Lactobacillus rhamnosus (LGG) was the first probiotic to be tested in a rodent model of ALD and was effective in leaky gut and liver inflammation.97,98 Muciniphila can also reduce ethanol-induced liver injury.99 While probiotics are safe in healthy individuals, caution is needed in certain patients, including premature infants, the elderly, and patients with low immune function, short bowel syndrome, central venous catheters, or heart diseases.100 Clinical trials have shown that probiotics are associated with bacteremia, endocarditis, gastrointestinal toxicity, and the transfer of antibiotic resistance in the gastrointestinal flora.100
Prebiotics can promote the growth and activity of specific or minority microbiota in the host’s gut.101 In alcohol-fed mice, pectin restored intestinal cupped cell function, increased the growth of anthropoid genera, and prevented liver injury.54,102
Synbiotics, a combination of probiotics and prebiotics, are complex carbohydrates in the gastrointestinal tract that are not digested and metabolized by the pancreas and intestinal enzymes, and show advantages in the treatment of ALD.103–105
Probiotics, prebiotics, and synbiotics may slow the progression of ALD; however, the dose, form, and regimen warrant further exploration. In addition, modulation of the gut microbiome may be transient, with recovery observed for only a few weeks to months. Nonetheless, longitudinal and long-term studies are still needed to determine better regimens.
FMT
Maintenance of normal gut flora is not the responsibility of one or two dominant gut bacteria.43 FMT in healthy individuals may play a better role in ALD. FMT can be traced back to the Eastern Jin Dynasty when Ge Hong documented the use of fecal fluid to treat patients with food poisoning and diarrhea in “Post-Elbow Prescription”.106 In 1958, Eiseman et al107 completed effective treatment of FMT in patients with severe pseudomembranous colitis. The potential role of FMT in regulating the gut microbiota in ulcerative colitis and gastrointestinal and non-gastrointestinal diseases is strongly emphasized.108–111 Bajaj et al112 used FMT and broad-spectrum antibiotics to treat recurrent hepatic encephalopathy. Xu et al113 treated a patient with cirrhosis and spontaneous bacterial peritonitis using FMT based on conventional therapy, which showed significant improvement in the general condition. A few studies have investigated the effect of FMT in ALD patients. Patients with severe AH who were not eligible for glucocorticoid therapy received FMT for 7 days and showed significant improvement in liver disease severity and survival.89 It was reported that liver function, hepatic encephalopathy, and Model for End-Stage Liver Disease (MELD) scores of a 38-year-old patient with corticosteroid-refractory severe AH who consecutively received FMT for 1 week had improved.91 Washed microbiota transplantation (WMT) — a full process technique based on an intelligent fecal bacteria isolation system and strict quality control of the associated rinsing and transplantation routes — is a new stage in the development of FMT with greater safety. A prospective study showed that complete enteral nutrition combined with WMT improved the nutritional status and induced clinical remission in malnourished Crohn’s disease patients.114 Currently, personalized and precise WMT that matches the patient and preserves autologous flora has been proposed.
Bioengineered Bacteria and Bacteriophages
Bioengineered bacteria that secrete beneficial metabolites is a new approach to precision medicine. Lactobacillus producing indole-3-acetic acid (IAA) reduced the severity of ALD.61 Precise editing of cytolytic fecal enterobacteria in fecal colonized sterile mice from patients with AH using phages reduced the severity of ethanol-induced liver in mice.39 Bioengineered bacteria or phages have not been tested in clinical settings and large multicenter clinical trials are needed to determine their beneficial effects in humans.
Precision Medicine Approaches Targeting the Intestinal Microbiome
A recent study115 showed that blocking bile acid excretion into the intestine or silencing the bile acid receptor, farnesoid X receptor (FXR), promoted bacterial overgrowth in the small intestine and increased intestinal wall permeability and bacterial translocation, as well as systemic and local inflammation in the liver. Therapeutic targets should be devoted to the study of anti-lipopolysaccharide antibodies or TLR4 inhibitors to block liver damage from intestinal inflammatory factors in the future. Another new area of interest may be miR155 inhibitors. Intestinal permeability and endotoxin and inflammatory factor levels were alleviated in miR155-deficient ALD mice.116
Other Treatments for Modulation of the Gut Microbiota
Natural products and phytochemicals act through various pathways, such as modulating the intestinal microbiota, improving redox responses, and being anti-inflammatory. Supplementation with lychee pulp extract upregulated the expression of intestinal tight junction proteins, antimicrobial proteins, and mucin in ALD mice and increased the relative abundance of Lactobacillus spp., Acetobacter spp., Actinobacteria phylum, and Corynebacterium spp. while decreasing serum endotoxin levels.117 Tang et al reported that oatmeal supplementation for 12 weeks maintained tight junctions and colonic mucosal integrity by preventing alcohol-induced leaky gut in rats.118 Natural products and related phytochemicals are ideal candidates against ALD, which warrants validation using clinical trials.
Modern studies have found that herbal medicines also exert therapeutic effects by adjusting the intestinal flora. Liu et al119 found that Lycium barbarum extract restored the growth of bifidobacteria and lactobacilli and adjusted the imbalance of the intestinal flora. Research has shown that the alcoholic extract of Ocimum sanctum can regulate the intestinal flora, protect the intestinal mucosa, and reduce the level of endotoxin leakage and the degree of alcoholic liver damage in rats.120,121
Conclusions
Alcohol causes changes in the gut microbiota and weakens the gut barrier. Persistent oxidative stress, LPS infiltration and hepatocyte damage through the enterohepatic circulation will lead to hepatic stellate cell activation and hepatic fibrosis leading to the development and exacerbation of ALD. Probiotics, prebiotics, synbiotics, FMT, bioengineered bacteria, gut-restricted FXR agonists and others are promising therapeutic approaches that can alter gut microbiota composition to improve ALD. In the future, there will be new challenges to study the interactions between the genetics of individuals with ALD and their gut microbiome, to provide personalized interventions targeting the gut-liver axis, and to develop better techniques to measure microbial communities and metabolites in the body.
Main Concepts and Learning Points
- Alcohol causes changes in the gut microbiota and weakens the gut barrier.
- Persistent oxidative stress, LPS infiltration and hepatocyte damage through the enterohepatic circulation will lead to hepatic stellate cell activation and hepatic fibrosis leading to the development and exacerbation of ALD.
- Probiotics, prebiotics, synbiotics, FMT, bioengineered bacteria, gut-restricted FXR agonists and others can improve ALD.
- This will be a new challenge to study the interactions between the genetics of individuals with ALD and their gut microbiome, to provide personalized interventions targeting the gut-liver axis, and to develop better techniques to measure microbial communities and metabolites in the body.
Author Contributions
All authors made a significant contribution to the work reported in terms of the conception, study design, execution, acquisition of data, analysis and interpretation. They took part in drafting, revising or reviewing the article; gave final approval of the final manuscript to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This work was supported by Hainan Provincial Health Industry Research Project (22A200078), Hainan Provincial Postgraduate Innovation Research Project (Qhyb2022-133), the specific research fund of The Innovation Platform for Academicians of Hainan Province (YSPTZX202313), and Hainan Province Clinical Medical Center (No. 2021818).
Disclosure
The authors declare that they have no competing interests.
References
1. GBD 2016 Alcohol Collaborators. Alcohol use and burden for 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2018;392(10152):1015–1035. doi:10.1016/S0140-6736(18)31310-2
2. World Health Organization. Global status report on alcohol and health 2014. Geneva, Switzerland: WHO; 2014. Available from: https://www.who.int/publications-detail-redirect/global-status-report-on-alcohol-and-health-2014.
3. Singal AK, Bataller R, Ahn J, Kamath PS, Shah VH. ACG clinical guideline: alcoholic liver disease. Am J Gastroenterol. 2018;113(2):175–194. doi:10.1038/ajg.2017.469
4. Asrani SK, Mellinger J, Arab JP, Shah VH. Reducing the global burden of alcohol-associated liver disease: a blueprint for action. Hepatology. 2021;73(5):2039–2050. doi:10.1002/hep.31583
5. Xu HQ, Xiao P, Zhang FY, Liu T, Gao YH. Epidemic characteristics of alcohol-related liver disease in Asia from 2000 to 2020: a systematic review and meta-analysis. Liver Int. 2022;42(9):1991–1998. doi:10.1111/liv.15312
6. Xie YD. More and more harmful drinkers in patients with liver disease. Ganboshi. 2021;(1):47–48. Chinese.
7. Wu Y, Li YR, Yang YX, Yin JZ, Feng YM. Current status of research on the pathogenesis of alcoholic liver disease. J Clin Hepatobiliary Dis. 2020;36(12):2822–2825. Chinese.
8. Liu Y, Su L. Guidelines for the primary care of alcoholic liver disease (2019). J Clin Hepatobiliary Dis. 2021;37(1):36–40. Chinese.
9. Li X, Luan DC, Ren S, et al. A study on the drinking behavior of residents over 18 years old in Liaoning Province from 2010 to 2012. Chine J Preventive Med 2020;21(1):16–21. Chinese.
10. Pi JT, Wang C, Zhang JM, et al. Epidemiological survey on alcohol consumption and alcoholic liver disease among permanent residents in Tongzhou District, Beijing. J Chronic Dis 2022;23(5):712–716. Chinese.
11. Hyun J, Han J, Lee C, Yoon M, Jung Y. Pathophysiological aspects of alcohol metabolism in the liver. Int J Mol Sci. 2021;22(11):5717. doi:10.3390/ijms22115717
12. Shah ND, Ventura-Cots M, Abraldes JG, et al. Alcohol-related liver disease is rarely detected at early stages compared with liver diseases of other etiologies worldwide. Clin Gastroenterol Hepatol. 2019;17(11):2320–2329.e12. doi:10.1016/j.cgh.2019.01.026
13. Sender R, Fuchs S, Milo R. Are we really vastly outnumbered? Revisiting the ratio of bacterial to host cells in humans. Cell. 2016;164(3):337–340. doi:10.1016/j.cell.2016.01.013
14. Sender R, Fuchs S, Milo R. Revised estimates for the number of human and bacteria cells in the body. PLoS Biol. 2016;14(8):e1002533. doi:10.1371/journal.pbio.1002533
15. Eckburg PB, Bik EM, Bernstein CN, et al. Diversity of the human intestinal microbial flora. Science. 2005;308(5728):1635–1638. doi:10.1126/science.1110591
16. Vassallo G, Mirijello A, Ferrulli A, et al. Review article: alcohol and gut microbiota- the possible role of gut microbiota modulation in the treatment of alcoholic liver disease. Aliment Pharm Ther. 2015;41:917–927. doi:10.1111/apt.13164
17. Bajaj JS. Alcohol, liver disease and the gut microbiota. Nat Rev Gastroenterol Hepatol. 2019;16:235–246. doi:10.1038/s41575-018-0099-1
18. Zheng SJ, Luo Y, Xiao JH. The impact of intestinal microorganisms and their metabolites on type 1 diabetes mellitus. Diabetes Metab Syndr Obes. 2022;15:1123–1139. doi:10.2147/DMSO.S355749
19. Wang F, Gu YZ, Xu C, et al. Transplantation of fecal microbiota from APP/PS1 mice and Alzheimer’s disease patients enhanced endoplasmic reticulum stress in the cerebral cortex of wild-type mice. Front Aging Neurosci. 2022;14:858130. doi:10.3389/fnagi.2022.858130
20. Barber TM, Valsamakis G, Mastorakos G, et al. Dietary influences on the microbiota-gut-brain axis. Int J Mol Sci. 2021;22(7):3502. doi:10.3390/ijms22073502
21. Chou YT, Kan WC, Shiao CC. Acute kidney injury and gut dysbiosis: a narrative review focus on pathophysiology and treatment. Int J Mol Sci. 2022;23(7):3658. doi:10.3390/ijms23073658
22. Sharon G, Cruz NJ, Kang DW, et al. Human gut microbiota from autism spectrum disorder promote behavioral symptoms in mice. Cell. 2019;177(6):1600–1618.e17. doi:10.1016/j.cell.2019.05.004
23. Qi XY, Yun CY, Sun LL, et al. Gut microbiota-bile acid-interleukin-22 axis orchestrates polycystic ovary syndrome. Nat Med. 2019;25(8):1225–1233. doi:10.1038/s41591-019-0509-0
24. Blacher E, Bashiardes S, Shapiro H, et al. Potential roles of gut microbiome and metabolites in modulating ALS in mice. Nature. 2019;572(7770):474–480. doi:10.1038/s41586-019-1443-5
25. Gehrig JL, Venkatesh S, Chang HW, et al. Effects of microbiota- directed foods in gnotobiotic animals and undernourished children. Science. 2019;365(6449):eaau4732. doi:10.1126/science.aau4732
26. Bárcena C, Valdés-Mas R, Mayoral P, et al. Healthspan and lifespan extension by fecal microbiota transplantation into progeroid mice. Nat Med. 2019;25(8):1234–1242. doi:10.1038/s41591-019-0504-5
27. Li Y, Tinoco R, Elmén L, et al. Gut microbiota dependent anti tumor immunity restricts melanoma growth in Rnf5-/- mice. Nat Commun. 2019;10(1):1492. doi:10.1038/s41467-019-09525-y
28. Hold GL, Smith M, Grange C, Watt ER, El-Omar EM, Mukhopadhya I. Role of the gut microbiota in inflammatory bowel disease pathogenesis: what have we learnt in the past 10 years? World J Gastroenterol. 2014;20:1192–1210. doi:10.3748/wjg.v20.i5.1192
29. Kassinen A, Krogius-Kurikka L, Mäkivuokko H, et al. The fecal microbiota of irritable bowel syndrome patients differs significantly from that of healthy subjects. Gastroenterology. 2007;133:24–33. doi:10.1053/j.gastro.2007.04.005
30. Nadal I, Donant E, Ribes-Koninckx C, Calabuig M, Sanz Y. Imbalance in the composition of the duodenal microbiota of children with coeliac disease. J Med Microbiol. 2007;56:1669–1674. doi:10.1099/jmm.0.47410-0
31. Lechner S, Yee M, Limketkai BN, Pham EA. Fecal microbiota transplantation for chronic liver diseases: current understanding and future direction. Dig Dis Sci. 2020;65(3):897–905. doi:10.1007/s10620-020-06100-0
32. Patel D, Sharma D, Mandal P. Gut microbiota: target for modulation of gut-liver-adipose tissue axis in ethanol-induced liver disease. Mediators Inflamm. 2022;2022:4230599. doi:10.1155/2022/4230599
33. Milosevic I, Vujovic A, Barac A, et al. Gut-liver axis, gut microbiota, and its modulation in the management of liver diseases: a review of the literature. Int J Mol Sci. 2019;20(2):395. doi:10.3390/ijms20020395
34. David LA, Maurice CF, Carmody RN, et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature. 2014;505(7484):559–563. doi:10.1038/nature12820
35. Mutlu E, Keshavarzian A, Engen P, Forsyth CB, Sikaroodi M, Gillevet P. Intestinal dysbiosis: a possible mechanism of alcohol-induced endotoxemia and alcoholic steatohepatitis in rats. Alcohol Clin Exp Res. 2009;33:1836–1846. doi:10.1111/j.1530-0277.2009.01022.x
36. Inokuchi S, Tsukamoto H, Park E, Liu ZX, Brenner DA, Seki E. Toll-like receptor 4 mediates alcohol-induced steatohepatitis through bone marrow-derived and endogenous liver cells in mice. Alcohol Clin Exp Res. 2011;35(8):1509–1518. doi:10.1111/j.1530-0277.2011.01487.x
37. Bode JC, Bode C, Heidelbach R, Dürr HK, Martini GA. Jejunal microflora in patients with chronic alcohol abuse. Hepatogastroenterology. 1984;31(1):30–34.
38. Bode C, Kolepke R, Schäfer K, Bode JC. Breath hydrogen excretion in patients with alcoholic liver disease-evidence of small intestinal bacterial overgrowth. Z Gastroenterol. 1993;31(1):3–7.
39. Duan Y, Llorente C, Lang S, et al. Bacteriophage targeting of gut bacterium attenuates alcoholic liver disease. Nature. 2019;575(7783):505–511. doi:10.1038/s41586-019-1742-x
40. Sun SS, Wang K, Sun L, et al. Therapeutic manipulation of gut microbiota by polysaccharides of Wolfiporia cocos reveals the contribution of the gut fungi-induced PGE2 to alcoholic hepatic steatosis. Gut Microbes. 2020;12(1):1830693. doi:10.1080/19490976.2020.1830693
41. Yang AM, Inamine T, Hochrath K, et al. Intestinal fungi contribute to development of alcoholic liver disease. J Clin Invest. 2017;127:2829–2841. doi:10.1172/JCI90562
42. Chu HK, Duan Y, Lang SJ, et al. The Candida albicans exotoxin candidalysin promotes alcohol-associated liver disease. J Hepatol. 2020;72:391–400. doi:10.1016/j.jhep.2019.09.029
43. Kirpich IA, Solovieva NV, Leikhter SN, et al. Probiotics restore bowel flora and improve liver enzymes in human alcohol-induced liver injury: a pilot study. Alcohol. 2008;42(8):675–682. doi:10.1016/j.alcohol.2008.08.006
44. Mutlu EA, Gillevet PM, Rangwala H, et al. Colonic microbiome is altered in alcoholism. Am J Physiol Gastrointest Liver Physiol. 2012;302:G966–G978. doi:10.1152/ajpgi.00380.2011
45. Leclercq S, Matamoros S, Cani PD, et al. Intestinal permeability, gut-bacterial dysbiosis, and behavioral markers of alcohol-dependence severity. Proc Natl Acad Sci U S A. 2014;111:E4485–E4493. doi:10.1073/pnas.1415174111
46. Chen YF, Yang FL, Lu HF, et al. Characterization of fecal microbial communities in patients with liver cirrhosis. Hepatology. 2011;54:562–572. doi:10.1002/hep.24423
47. Bajaj JS, Heuman DM, Hylemon PB, et al. Altered profile of human gut microbiome is associated with cirrhosis and its complications. J Hepatol. 2014;60:940–947. doi:10.1016/j.jhep.2013.12.019
48. Tuomisto S, Pessi T, Collin P, Vuento R, Aittoniemi J, Karhunen PJ. Changes in gut bacterial populations and their translocation into liver and ascites in alcoholic liver cirrhotics. BMC Gastroenterol. 2014;14:40. doi:10.1186/1471-230X-14-40
49. Dubinkina VB, Tyakht AV, Odintsova VY, et al. Links of gut microbiota composition with alcohol dependence syndrome and alcoholic liver disease. Microbiome. 2017;5:141. doi:10.1186/s40168-017-0359-2
50. Bajaj JS, Kakiyama G, Zhao D, et al. Continued alcohol misuse in human cirrhosis is associated with an impaired gut-liver axis. Alcohol Clin Exp Res. 2017;41:1857–1865. doi:10.1111/acer.13498
51. Zhong XD, Cui P, Jiang JJ, et al. Streptococcus, the predominant bacterium to predict the severity of liver injury in alcoholic liver disease. Front Cell Infect Microbiol. 2021;11:649060. doi:10.3389/fcimb.2021.649060
52. Visapää JP, Jokelainen K, Nosova T, Salaspuro M. Inhibition of intracolonic acetaldehyde production and alcoholic fermentation in rats by ciprofloxacin. Alcohol Clin Exp Res. 1998;22(5):1161–1164.
53. Llopis M, Cassard AM, Wrzosek L, et al. Intestinal microbiota contributes to individual susceptibility to alcoholic liver disease. Gut. 2016;65(5):830–839. doi:10.1136/gutjnl-2015-310585
54. Ferrere G, Wrzosek L, Cailleux F, et al. Fecal microbiota manipulation prevents dysbiosis and alcohol-induced liver injury in mice. J Hepatol. 2017;66(4):806–815. doi:10.1016/j.jhep.2016.11.008
55. Halsted CH, Robles EA, Mezey E. Distribution of ethanol in the human gastrointestinal tract. Am J Clin Nutr. 1973;26:831–834. doi:10.1093/ajcn/26.8.831
56. Martino C, Zaramela LS, Gao B, et al. Acetate reprograms gut microbiota during alcohol consumption. Nat Commun. 2022;13(1):4630. doi:10.1038/s41467-022-31973-2
57. Odenwald MA, Turner JR. The intestinal epithelial barrier: a therapeutic target? Nat Rev Gastroenterol Hepatol. 2017;14(1):9–21. doi:10.1038/nrgastro.2016.169
58. Bishehsari F, Magno E, Swanson G, et al. Alcohol and gut-derived inflammation. Alcohol Res. 2017;38(2):163–171.
59. Bode C, Bode JC. Alcohol’s role in gastrointestinal tract disorders. Alcohol Health Res World. 1997;21(1):76–83.
60. Liu Y, Yu XJ, Zhao JX, Zhang H, Zhai QX, Chen W. The role of MUC2 mucin in intestinal homeostasis and the impact of dietary components on MUC2 expression. Int J Biol Macromol. 2020;164:884–891. doi:10.1016/j.ijbiomac.2020.07.191
61. Hendrikx T, Duan Y, Wang YH, et al. Bacteria engineered to produce IL-22 in intestine induce expression of REG3G to reduce ethanol-induced liver disease in mice. Gut. 2019;68(8):1504–1515. doi:10.1136/gutjnl-2018-317232
62. Grewal RK, Mahmood A. Ethanol induced changes in glycosylation of mucins in rat intestine. Ann Gastroenterol. 2009;22:178–183.
63. Elamin EE, Masclee AA, Dekker J, Jonkers DM. Ethanol metabolism and its effects on the intestinal epithelial barrier. Nutr Rev. 2013;71(7):483–499. doi:10.1111/nure.12027
64. Chiang CP, Wu CW, Lee SP, et al. Expression pattern, ethanol-metabolizing activities, and cellular localization of alcohol and aldehyde dehydrogenases in human small intestine. Alcohol Clin Exp Res. 2012;36(12):2047–2058. doi:10.1111/j.1530-0277.2012.01836.x
65. Roberts BJ, Shoaf SE, Jeong KS, Song BJ. Induction of CYP2E1 in liver, kidney, brain and intestine during chronic ethanol administration and withdrawal: evidence that CYP2E1 possesses a rapid phase half-life of 6 hours or less. Biochem Biophys Res Commun. 1994;205(2):1064–1071. doi:10.1006/bbrc.1994.2774
66. Cho YE, Song BJ. Pomegranate prevents binge alcohol-induced gut leakiness and hepatic inflammation by suppressing oxidative and nitrative stress. Redox Biol. 2018;18:266–278. doi:10.1016/j.redox.2018.07.012
67. Cho YE, Yu LR, Abdelmegeed MA, Yoo SH, Song BJ. Apoptosis of enterocytes and nitration of junctional complex proteins promote alcohol-induced gut leakiness and liver injury. J Hepatol. 2018;69(1):142–153. doi:10.1016/j.jhep.2018.02.005
68. Salaspuro M. Bacteriocolonic pathway for ethanol oxidation: characteristics and implications. Ann Med. 1996;28(3):195–200. doi:10.3109/07853899609033120
69. Koivisto T, Salaspuro M. Aldehyde dehydrogenases of the rat colon: comparison with other tissues of the alimentary tract and the liver. Alcohol Clin Exp Res. 1996;20(3):551–555. doi:10.1111/j.1530-0277.1996.tb01091.x
70. Kourkoumpetis T, Sood G. Pathogenesis of alcoholic liver disease: an update. Clin Liver Dis. 2019;23(1):71–80. doi:10.1016/j.cld.2018.09.006
71. Uesugi T, Froh M, Arteel GE, Bradford BU, Thurman RG. Toll-like receptor 4 is involved in the mechanism of early alcohol-induced liver injury in mice. Hepatology. 2001;34(1):101–108. doi:10.1053/jhep.2001.25350
72. Wang LR, Fouts DE, Stärkel P, et al. Intestinal REG3 lectins protect against alcoholic steatohepatitis by reducing mucosa-associated microbiota and preventing bacterial translocation. Cell Host Microbe. 2016;19(2):227–239. doi:10.1016/j.chom.2016.01.003
73. Xie GX, Zhong W, Zheng XJ, et al. Chronic ethanol consumption alters mammalian gastrointestinal content metabolites. J Proteome Res. 2013;12:3297–3306. doi:10.1021/pr400362z
74. Chen P, Stärkel P, Turner JR, Ho SB, Schnabl B. Dysbiosis-induced intestinal inflammation activates tumor necrosis factor receptor I and mediates alcoholic liver disease in mice. Hepatology. 2015;61:883–894. doi:10.1002/hep.2748
75. Atkinson KJ, Rao RK. Role of protein tyrosine phosphorylation in acetaldehyde-induced disruption of epithelial tight junctions. Am J Physiol Gastrointest Liver Physiol. 2001;280(6):G1280–G1288. doi:10.1152/ajpgi.2001.280.6.G1280
76. Singh R, Bullard J, Kalra M, et al. Status of bacterial colonization, toll-like receptor expression and nuclear factor-kappa B activation in normal and diseased human livers. Clin Immunol. 2011;138(1):41–49. doi:10.1016/j.clim.2010.09.006
77. Roh YS, Zhang B, Loomba R, Seki E. TLR2 and TLR9 contribute to alcohol-mediated liver injury through induction of CXCL1 and neutrophil infiltration. Am J Physiol Gastrointest Liver Physiol. 2015;309(1):G30–G41. doi:10.1152/ajpgi.00031.2015
78. Hritz I, Mandrekar P, Velayudham A, et al. The critical role of toll-like receptor (TLR) 4 in alcoholic liver disease is independent of the common TLR adapter MyD88. Hepatology. 2008;48(4):1224–1231. doi:10.1002/hep.22470
79. Cubero FJ, Nieto N. Arachidonic acid stimulates TNFα production in Kupffer cells via a reactive oxygen species-pERK1/2-Egr1-dependent mechanism. Am J Physiol Gastrointest Liver Physiol. 2012;303(2):G228–G239. doi:10.1152/ajpgi.00465.2011
80. Yamashina S, Takei Y, Ikejima K, et al. Ethanol-induced sensitization to endotoxin in Kupffer cells is dependent upon oxidative stress. Alcohol Clin Exp Res. 2005;29(12 Suppl):246S–50S. doi:10.1097/01.alc.0000191128.54871.40
81. Shi H, Dong L, Dang X, et al. Effect of chlorogenic acid on LPS-induced proinflammatory signaling in hepatic stellate cells. Inflamm Res. 2013;62(6):581–587. doi:10.1007/s00011-013-0610-7
82. Loguercio C, Federico A, Tuccillo C, et al. Beneficial effects of a probiotic VSL#3 on parameters of liver dysfunction in chronic liver diseases. J Clin Gastroenterol. 2005;39(6):540–543. doi:10.1097/01.mcg.0000165671.25272.0f
83. Gupta H, Kim SH, Kim SK, Han SH, Kwon HC, Suk KT. Beneficial shifts in gut microbiota by Lacticaseibacillus rhamnosus R0011 and Lactobacillus helveticus R0052 in alcoholic hepatitis. Microorganisms. 2022;10(7):1474. doi:10.3390/microorganisms10071474
84. Stadlbauer V, Mookerjee RP, Hodges S, Wright GAK, Davies NA, Jalan R. Effect of probiotic treatment on deranged neutrophil function and cytokine responses in patients with compensated alcoholic cirrhosis. J Hepatol. 2008;48:945–951. doi:10.1016/j.jhep.2008.02.015
85. Amadieu C, Maccioni L, Leclercq S, et al. Liver alterations are not improved by inulin supplementation in alcohol use disorder patients during alcohol withdrawal: a pilot randomized, double-blind, placebo-controlled study. EBioMedicine. 2022;80:104033. doi:10.1016/j.ebiom.2022.104033
86. Loguercio C, De Simone T, Federico A, et al. Gut-liver axis: a new point of attack to treat chronic liver damage? Am J Gastroenterol. 2002;97(8):2144–2146. doi:10.1111/j.1572-0241.2002.05942.x
87. Bode C, Schäfer C, Fukui H, Bode JC. Effect of treatment with paromomycin on endotoxemia in patients with alcoholic liver disease-a double-blind, placebo-controlled trial. Alcohol Clin Exp Res. 1997;21(8):1367–1373.
88. Kalambokis GN, Mouzaki A, Rodi M, et al. Rifaximin improves systemic hemodynamics and renal function in patients with alcohol-related cirrhosis and ascites. Clin Gastroenterol Hepatol. 2012;10(7):815–818. doi:10.1016/j.cgh.2012.02.025
89. Philips CA, Pande A, Shasthry SM, et al. Healthy donor fecal microbiota transplantation in steroid-ineligible severe alcoholic hepatitis: a pilot study. Clin Gastroenterol Hepatol. 2017;15(4):600–602. doi:10.1016/j.cgh.2016.10.029
90. Philips CA, Phadke N, Ganesan K, Ranade S, Augustine P. Cortico-steroids, nutrition, pentoxifylline, or fecal microbiota transplantation for severe alcoholic hepatitis. Indian J Gastroenterol. 2018;37(3):215–225. doi:10.1007/s12664-018-0859-4
91. Philips CA, Phadke N, Ganesan K, Augustine P. Healthy donor faecal transplant for corticosteroid non-responsive severe alcoholic hepatitis. BMJ Case Rep. 2017;2017:bcr2017222310. doi:10.1136/bcr-2017-222310
92. Sharma A, Roy A, Premkumar M, et al. Fecal microbiota transplantation in alcohol-associated acute-on-chronic liver failure: an open-label clinical trial. Hepatol Int. 2022;16(2):433–446. doi:10.1007/s12072-022-10312-z
93. Yan F, Cao HW, Cover TL, Whitehead R, Washington MK, Polk DB. Soluble proteins produced by probiotic bacteria regulate intestinal epithelial cell survival and growth. Gastroenterology. 2007;132:562–575. doi:10.1053/j.gastro.2006.11.022
94. Saulnier DM, Spinler JK, Gibson GR, Versalovic J. Mechanisms of probiosis and prebiosis: considerations for enhanced functional foods. Curr Opin Biotechnol. 2009;20:135–141. doi:10.1016/j.copbio.2009.01.002
95. Jones SE, Versalovic J. Probiotic Lactobacillus reuteri biofilms produce antimicrobial and anti-inflammatory factors. BMC Microbiol. 2009;9:35. doi:10.1186/1471-2180-9-35
96. Nanji AA, Khettry U, Sadrzadeh SM. Lactobacillus feeding reduces endotoxemia and severity of experimental alcoholic liver (disease). Proc Soc Exp Biol Med. 1994;205(3):243–247. doi:10.3181/00379727-205-43703
97. Forsyth CB, Farhadi A, Jakate SM, Tang YM, Shaikh M, Keshavarzian A. Lactobacillus GG treatment ameliorates alcohol-induced intestinal oxidative stress, gut leakiness, and liver injury in a rat model of alcoholic steatohepatitis. Alcohol. 2009;43:163–172. doi:10.1016/j.alcohol.2008.12.009
98. Nanji AA, Khettry U, Sadrzadeh SMH. Lactobacillus feeding reduces endotoxemia and severity of experimental alcoholic liver (disease). Proc Soc Exp Biol Med. 1994;205:243–246. doi:10.3181/00379727-205-43703
99. Grander C, Adolph TE, Wieser V, et al. Recovery of ethanol-induced Akkermansia muciniphila depletion ameliorates alcoholic liver disease. Gut. 2018;67(5):891–901. doi:10.1136/gutjnl-2016-313432
100. Snydman DR. The safety of probiotics. Clin Infect Dis. 2008;46(Suppl. 2):S104–S111, S144–S151. doi:10.1086/523331
101. Sarin K, Pande A, Schnabl B. Microbiome as a therapeutic target in alcohol-related liver disease. J Hepatol. 2019;70(2):260–272. doi:10.1016/j.jhep.2018.10.019
102. Wrzosek L, Ciocan D, Hugot C, et al. Microbiota tryptophan metabolism induces aryl hydrocarbon receptor activation and improves alcohol-induced liver injury. Gut. 2021;70(7):1299–1308. doi:10.1136/gutjnl-2020-321565
103. Floch MH. The role of prebiotics and probiotics in gastrointestinal disease. Gastroenterol Clin North Am. 2018;47(1):179–191. doi:10.1016/j.gtc.2017.09.011
104. Raso GM, Simeoli R, Iacono A, et al. Meli effects of a Lactobacillus paracasei B21060 based synbiotic on steatosis, insulin signaling and toll-like receptor expression in rats fed a high-fat diet. J Nutr Biochem. 2014;25(1):81–90. doi:10.1016/j.jnutbio.2013.09.006
105. Kassaian N, Aminorroaya A, Feizi A, Jafari P, Amini M. The effects of probiotic and synbiotic supplementation on metabolic syndrome indices in adults at risk of type 2 diabetes: study protocol for a randomized controlled trial. Trials. 2017;18(1):148. doi:10.1186/s13063-017-1885-8
106. Zhang FM, Luo WS, Shi Y, Fan ZN, Ji GZ. Should we standardize the 1700-year-old fecal microbiota transplantation? Am J Gastroenterol. 2012;107:1755–1756. doi:10.1038/ajg.2012.251
107. Eiseman B, Silen W, Bascom GS, Kauvar AJ. Fecal enema as an adjunct in the treatment of pseudomembranous enterocolitis. Surgery. 1958;44(5):854–859.
108. Xu Z, Liu ZX, Dong XG, et al. Fecal microbiota transplantation from healthy donors reduced alcohol-induced anxiety and depression in an animal model of chronic alcohol exposure. Chin J Physiol. 2018;61(6):360–371. doi:10.4077/CJP.2018.BAH633
109. Tian ZH, Liu J, Liao MY, et al. Beneficial effects of fecal microbiota transplantation on ulcerative colitis in mice. Dig Dis Sci. 2016;61(8):2262–2271. doi:10.1007/s10620-016-4060-2
110. Konturek PC, Haziri D, Brzozowski T, et al. Emerging role of fecal microbiota therapy in the treatment of gastrointestinal and extra-gastrointestinal diseases. J Physiol Pharmacol. 2015;66(4):483–491.
111. Yanira G, Bibbò S, Gasbarrini A, Cammarota G. Therapeutic modulation of gut microbiota: current clinical applications and future perspectives. Curr Drug Targets. 2014;15(8):762–770. doi:10.2174/1389450115666140606111402
112. Bajaj JS, Kassam Z, Fagan A, et al. Fecal microbiota transplant from a rational stool donor improves hepatic encephalopathy: a randomized clinical trial. Hepatology. 2017;66(6):1727–1738. doi:10.1002/hep.29306
113. Xu YH, Song CF, Zhou ZJ, et al. Clinical efficacy of fecal bacteria transplantation in the treatment of cirrhosis combined with bacterial spontaneous peritonitis. J Mudanjiang Med College. 2017;38(1):56–57.
114. Xiang LY, Yu Y, Ding X, et al. Exclusive enteral nutrition plus immediate vs. delayed washed microbiota transplantation in Crohn’s disease with malnutrition: a randomized pilot study. Front Med. 2021;8:666062. doi:10.3389/fmed.2021.666062
115. Kalman RS, Goldberg DS. The role of obeticholic acid in gut bacterial translocation and inflammation. Gastroenterology. 2016;151(4):759–761. doi:10.1053/j.gastro.2016.08.035
116. Lippai D, Bala S, Catalano D, Kodys K, Szabo G. MicroRNA-155 deficiency prevents alcohol-induced serum endotoxin increase and small bowel inflammation in mice. Alcohol Clin Exp Res. 2014;38:2217–2224. doi:10.1111/acer.12483
117. Xiao J, Zhang RF, Zhou QY, et al. Lychee (Litchi chinensis Sonn.) pulp phenolic extract provides protection against alcoholic liver injury in mice by alleviating intestinal microbiota dysbiosis, intestinal barrier dysfunction, and liver inflammation. J Agric Food Chem. 2017;65(44):9675–9684. doi:10.1021/acs.jafc.7b03791
118. Tang YM, Forsyth CB, Banan A, Fields JZ, Keshavarzian A. Oats supplementation prevents alcohol-induced gut leakiness in rats by preventing alcohol-induced oxidative tissue damage. J Pharmacol Exp Ther. 2009;329(3):952–958. doi:10.1124/jpet.108.148643
119. Liu YT, Xu W, Xin Y, et al. The adjustment effect of Lycium barbarum extract on the imbalance of intestinal flora in mice. Natural Products Res Dev. 2015;27(7):1270–1272.
120. Tan M, Zhang H, Wang JW. Preliminary investigation on the protective effect and mechanism of Wu Yao on acute alcoholic liver injury. J Anhui Med Univ. 2015;50(12):1773–1775.
121. Dong Y, Qiu P, Zhao LS, et al. Metabolomics study of the hepatoprotective effect of Phellinus igniarius in chronic ethanol- induced liver injury mice using UPLC-Q/TOF-MS combined with ingenuity pathway analysis. Phytomedicine 2020;74:152697. doi:10.1016/j.phymed.2018.09.232
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.