Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Roles and Responsibilities in the Transition to Working Independently: A Qualitative Study of Recently Graduated Radiographers’ Perspectives in Australia
Authors Makanjee CR ![]() , Zhang J, Bergh AM
, Zhang J, Bergh AM
Received 10 April 2023
Accepted for publication 11 July 2023
Published 28 August 2023 Volume 2023:16 Pages 2471—2483
DOI https://doi.org/10.2147/JMDH.S416510
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Chandra R Makanjee,1 Julie Zhang,2 Anne-Marie Bergh3
1Department of Medical Radiation Sciences (MI), University of Canberra, Bruce, Australian Capital Territory, Australia; 2Division of Diagnostic Radiology, Princess Alexandra Hospital, Brisbane, Queensland, Australia; 3Research Centre for Maternal, Fetal, Newborn and Child Health Care Strategies, Faculty of Health Sciences, University of Pretoria, Pretoria, South Africa
Correspondence: Julie Zhang, Division of Diagnostic Radiology, Princess Alexandra Hospital, Brisbane, Queensland, Australia, Tel +61 7 3176 2971, Email [email protected]
Background: Medical imaging features along the entire healthcare continuum and is known for its fast-paced technological evolution which enables it to keep up with the demands of the healthcare system to provide safe, quality services. The overall efficacy and efficiency of the system depends on practitioners’ clinical competence, achieved through professional education and continuous professional development. Recent studies have revealed concerns regarding newly graduated healthcare professionals’ preparedness and readiness to handle actual practice.
Methods: We conducted qualitative face-to-face and telephonic interviews with a convenient and purposive sample of 23 participants consisting of recently graduated radiographers (n=14), radiography students (n=5) and supervising radiographers (n=4) in Australia. Verbatim transcriptions were analyzed inductively to identify themes pertaining to perspectives and experiences of the work readiness of novice radiographers.
Results: The findings of our study suggest that the workplace immersion and transitioning of recently graduated radiographers into their professional roles requires a process of experiential learning and honing of knowledge and skills if they are to function efficiently and independently in a team-oriented workplace. Radiographic services are spread across various levels of care and are an integral part of the organizational structure of a healthcare system. Maladaptive transitions to the workplace may be the result of low self-confidence, a lack of support, uncertainty in inter-collegial interactions, or unrealistic performance expectations. The overarching themes of communication and interaction emerged clearly as recently graduated radiographers navigated the four roles of coordinator, collaborator, mediator, and advocate.
Conclusion: The application of radiographic skills is embedded in a workplace culture of communication and safety. Transitioning to independent practice takes place in a complex, multifaceted environment and is accompanied by internal and external expectations. Because each workplace has a unique context, system and culture, no novice radiographic professional can ever be fully prepared through pre-service training and workplace induction.
Keywords: radiography, safety culture, work readiness, multidisciplinary teamwork, experiential learning, professional development
Introduction
Medical imaging is an integral part of the entire healthcare continuum, featuring in wellness and screening, early diagnosis, treatment selection, and follow-up.1 The diagnostic information adds multidimensional value in terms of clinical benefit (patient empowerment) and clinical management, including organizational and economic efficiencies with a public health benefit.2 Teamwork is an essential requirement for better quality care and patient safety.3,4 Rosen and colleagues associate team competency with team training as a strategy to improve outcomes at different levels: individual (eg attitudes), team (eg efficiency), and organization (eg safety culture).5
In this context, radiographers contribute by maintaining professional competency, while applying best practice principles in an effective, safe and timely manner.6 One inherent professional capability is the ability to adapt their practice to suit their increasing responsibilities without compromising patient care and safety.7 The clinical competence achieved through the professional education of healthcare practitioners contributes to the overall effectiveness of a healthcare system.8 According to Mariño et al, preparedness for practice includes adequate technical skills, clinical knowledge, and the attributes necessary to practice in the profession – the ability to communicate and interact appropriately with patients and colleagues from different professions within the context of the ethical and legal expectations of the healthcare system.9
There have been concerns about newly graduated healthcare professionals’ preparedness and readiness to handle actual practice.10 A challenge is to develop a safety and quality mindset among novice practitioners through practical guidance during several short series of practical experiences in the course of their training.11 Harrison suggests a multidimensional model of practice readiness depicting capabilities in four domains – personal, clinical, professional and industry readiness.10 Chipere et al recommend that the workplace culture for new graduates should encourage integration, personal growth, and retention of new staff.12 Each hospital has its own culture and each hospital unit, such as diagnostic medical imaging, may have its own micro-culture. Therefore, workplace culture differs significantly not only between hospitals but also within the same institution.5 In a letter from 9 November 2022 to the Discipline Head of the University of Canberra, the Medical Radiation Practice Accreditation Committee emphasized the importance of exposing students to varied workplace experiences, including high-pressure work settings that could be daunting to navigate (eg emergency, theatre, or critical settings).
At the time of conceptualizing this study, we found very few studies on the perceptions and experiences of recently graduated radiographers (RGRs) in an integrated healthcare medical imaging service. In this study we attempted to gain insights into the following questions: What are RGRs’ perspectives on work readiness and what are their experiences in achieving safe medical imaging examination procedures and quality outcomes in multidisciplinary, team-oriented workplaces in Australia?
Methodology
Study Design
We selected a qualitative inductive research design to explore how radiographers’ initial workplace experiences are shaped through interactions with individual members of a multidisciplinary team in an institution rendering medical imaging services. The focus was on RGRs, complemented by the perspectives of radiography students and supervisors on this issue.
Participants and Sampling Strategies
The study comprised individual interviews with 23 members of three different participant groups: 14 RGRs, five student radiographers (STs) and four supervising radiographers (SRs). The purposive sample of RGRs included participants employed in the public and private sectors. Within each of these sectors, a convenience sample of participants were approached to participate in an interview. The inclusion criterion for RGR participants was professional workplace experience not exceeding two years to allow for varying context-dependent learning experiences. A convenience sample was selected for the STs, with the inclusion criterion that they had to be in their final year of study. Sampling for SR participants was purposive to include different numbers of years of experience as practitioners and clinical supervisors.
The study participants (RGRs and SRs) were recruited from public and private medical imaging departments and practices in Queensland (QLD), New South Wales, and the Australian Capital Territory (ACT) in Australia. Student participants were recruited from universities in the ACT and QLD.
Data Collection
After a potential participant had been contacted by the first or second author to confirm availability for voluntary participation in an individual interview, an information leaflet about the study was sent to the participant and a date was set for the interview. The first two authors conducted all the semi-structured, in-depth interviews between October 2020 and February 2021. The interview guide contained several probing questions, including the following: work experiences in the immediate workplace setting; relevant experiences beyond the immediate workplace; and enablers and barriers when conducting medical imaging examinations in the workplace.
The individual interviews were planned in a specific chronological order. The first interviews were conducted with the student radiographers (n=5) to serve as background and provide a sense of learner perceptions and authentic experiences of the real workplace environment during the students’ practical placement. This was followed by interviews with the RGRs (n=14) to elicit perspectives on and experiences of their new professional role. Their work experience ranged between 3 months and 2 years. Lastly, the four interviews with supervising radiographers aimed to get their perspectives on RGRs’ transition from being students to being qualified radiographers.
Ten interviews were conducted face-to-face at a neutral location that ensured confidentiality and privacy: one with an SR, four with RGRs and five with STs. The remaining RGRs (n=10) and the SRs (n=3) were interviewed by telephone. Interviews lasted between 15 and 53 minutes and were audio-recorded digitally with the consent of the participants.
Data Analysis
The audio-recordings of all interviews were transcribed verbatim. We conducted traditional qualitative content analysis as described by Hsieh and Shannon.13 The result of this type of content analysis is usually a description of lived experiences or the development of a descriptive framework of the phenomenon under investigation. After each interview, the first two authors conducted iterative readings of the transcripts to obtain a sense of the overall content of the data. Key concepts and phrases that stood out during reading were manually highlighted. Code development, memo writing, and category pattern identification were done independently. Most of the codes and categories developed during this phase by the two analysts showed similarities. Discrepancies in interpretation were discussed until consensus was reached. Subsequent rounds of interpretation focused on identifying preliminary themes and subthemes. The process of data collection and analysis took place concurrently until the analysis yielded no new themes, at which point data saturation was assumed to have been achieved14 and no further interviews were conducted. The third author did a second independent analysis using NVivo 9 software to verify the feasibility of the interpretation emanating from the first rounds of analysis and to suggest further adaptations.
Rigor
Measures to ensure the trustworthiness of the study are described in terms of the following criteria: credibility; transferability; dependability; and confirmability.15 Credibility was established through activities such as a five-month period of data collection and simultaneous preliminary data analysis until data saturation was reached. The preliminary interpretations were presented to 15 participants from all three groups to confirm the feasibility of the interpretations (RGR, n=10; ST, n=3; SR, n=2). This constituted a form of member checking. Peer debriefing between the two primary data analysts and the independent verification of the feasibility of the interpretations by an external analyst also enhanced credibility. The findings discussed below include verbatim quotations from participants to illustrate interpretation points.
The expectation is that the findings may be transferable to similar training programs and settings in which RGRs start their careers. This expectation was reinforced by the interpretation framework described in the findings and the direct quotations or rich descriptions that highlight the context of the study. Dependability was supported by the audit trail kept by the second author throughout the study process. Investigator triangulation was attained through two independent data analyses, while the radiography groups (RGRs, students and supervisors) constituted three different data sources that enabled data triangulation.
The documents generated throughout data collection, interpretation, and analysis – the interview transcripts, communications on the data collection and recruitment process, field notes made during interviews and reflective notes – enabled a deeper engagement with the data. In addition, the varied backgrounds of the researchers (an academic radiographer, a practicing radiographer and a qualitative research specialist) minimized subjectivity and contributed to the confirmability of the study.
Ethical Considerations
The Human Research Ethics Committee at the University of Canberra approved the study (HREC-4751). For the face-to-face interviews, written informed consent was obtained from each participant who had agreed to take part in the study and verbal audio-recorded consent was obtained for the telephonic interviews. Before the start of each interview the participant was informed in detail about the purpose, processes and requirements of the study as set out in the information leaflet. The researcher seeking consent also discussed the benefits of the study and emphasized that participation was voluntary and that the participants had the right to withdraw at any time. Participants were assured that confidentiality would be maintained, that each interview would receive a coded identification number and that information in transcripts and study reports would be anonymized to protect participant and workplace identity.
Results
The main expectation about work readiness that emerged from all study participants’ narratives was that RGRs should be able to work independently and feel confident that they have the necessary skills to do the task at hand.
I don’t get to fall back on anyone else now. It’s all up to me. That’s probably the main thing. … Confidence feeds into that as well. (RGR8)
Unlike students, fully-fledged radiographers were expected to undertake additional responsibilities:
Not so much the work, but more so the responsibility. That’s different. You’ve got a lot more on your shoulders. Try not to screw up. (RGR1)
Challenges facing RGRs entailed integrating two different skill sets and three different roles in ways that cannot be achieved in a university training program – “Nothing is textbook, it’s all different” (SR3). The focus of the radiography curriculum is the development of radiographic imaging skills that would ensure patient safety and quality images. These skills are applicable to the role of the radiographer as technician and to a certain extent as team member. The other skill set pertains to generic, “interchangeable skills” (RGR3) for effective functioning in the system in the role of coordinator, collaborator, mediator and advocate, but also as team member beyond the medical imaging department and across different departments and entities. The overarching theme is that of communication and interaction across the system. Figure 1 illustrates the integration of these roles and the skills expected of the RGRs.
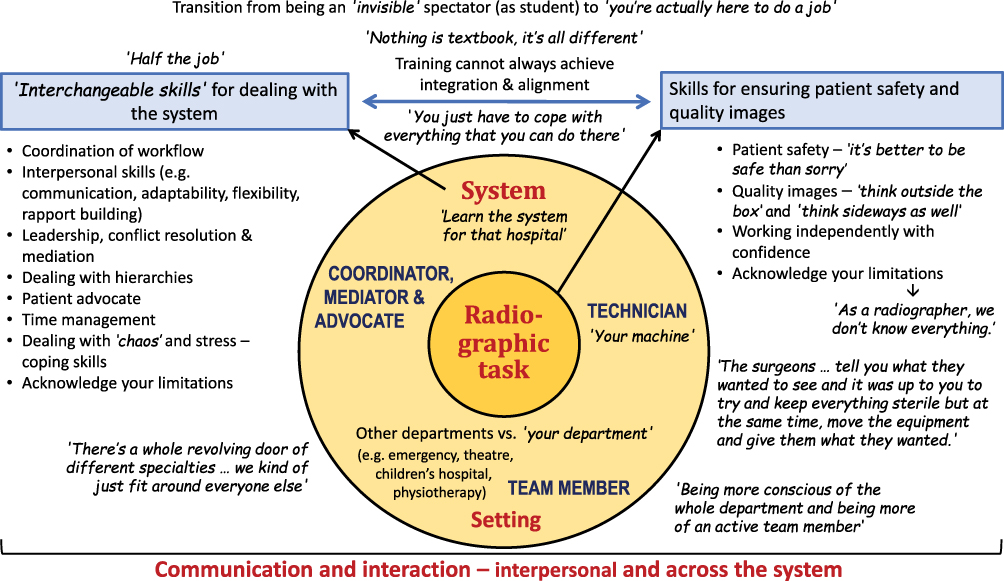 |
Figure 1 Skills, roles and responsibilities expected of newly graduated radiographers. The dark yellow centre circle represents the core duty of radiographers. The lighter yellow outer circle represents the interconnectedness of the environments they practice in and their associated roles; often bridging gaps between patients, multidisciplinary team members and the overarching healthcare system. On the white outer edges, multiple skills and examples relating to communication and interaction are given to add context and meaning. |
Skills for Ensuring Patient Safety and Quality Images
The Technician – “Technical Radiographic Skills”
A common thread running through the interviews is that the radiographer as technician had “to really pay attention to what’s happening” (RGR6) in order to make appropriate decisions and judgements on the quality of images without compromising patient safety.
I tried really hard … every x-ray I’d take. I would try and decide if it was diagnostic or not, if I would repeat it and develop a threshold for what I was happy sending through. (RGR12)
One participant referred to the fact that radiographers can become complacent:
Often radiographers get very used to reading “PA hand” and just do it. … There’s a lot of situations where unnecessary things are done because people aren’t critically thinking about what’s needed for that indication. … There’s a level of thinking for yourself and making your own decisions. (RGR7)
A supervising radiographer had the following expectations of novice radiographers:
To be able to take x-rays and from looking at those x-rays they can decide whether they should proceed with extra views or whether those views that they have taken already answered the clinical question. … But, in terms of CT [computed tomography] … I don’t have high expectations. As long as they are willing to learn, I think that is the most important thing to start off as a graduate. They need to be enthusiastic about what they are doing. (SR1)
Another golden thread regarding radiographers’ technical skills is that “as a radiographer, we don’t know everything” (SR3). Awareness of one’s own capabilities and knowledge-and-skills gaps is important if one is to avoid mistakes – “just ask questions. Even if you ask the same question over and over again” (RGR1). Building confidence or finding reassurance comes through self-motivation – “You’ve got to tell yourself, you have learnt all this; you can get there, and you can do it” (SR3). The following is how one participant described the unfamiliarity of a new workplace or situation:
No matter how much you know, it’s still, ‘I know all this, but I don’t know this.’ You work through and go, ‘No, I do know this. It’s just a different machine or a slightly different set up … it might not be perfect … I’ve just learnt it in a different way.’ (SR3)
Lastly, RGRs found themselves in complex situations with simultaneous events taking place where they had to perform a balancing act by being accountable for patient and staff safety while looking after their equipment. This is how one participant described such events:
We’ve had cases where you’re trying to get a chest x-ray and the patient crashes. So they’re trying to start CPR [cardiopulmonary resuscitation] and you’re like, ‘No, no, no! I need to get that board out. … That board is worth more than my life. My boss is gonna kill me if I don’t get that out.’ … There was a case where the patient got shocked when they were on the board and then that ruined the whole system. … You just have to really … look after your equipment but also, you’re swinging heavy, pushing the big hand, swishing the C-arm around, … the mobile. … Be aware you’re also injuring your colleagues while you’re trying to help save the patient’s life. (RGR6)
The Radiographic Team Member – “You Actually Have a Bit of a Voice Because You’ve Been Involved”
As a technician, a radiographer is also dependent on teamwork with colleagues for the safe performance of certain radiographic tasks, especially when it is difficult to do certain examinations on one’s own. An example would be doing a mobile chest x-ray for a suspected case of coronavirus disease (COVID):
You need to talk about which role you want to be in. Do you want to be the clean radiographer or the dirty radiographer? Also, if you’re the clean radiographer, you have to tell the dirty radiographer where to position the board; whether it’s high enough or low enough (RGR9). (Note: The ‘clean radiographer’ operates the equipment and the ‘dirty radiographer’ has contact with the patient.)
Furthermore, teamwork involves having an enquiring approach – “What do you think this means?” (SR3) – and embracing feedback from colleagues on alternative approaches to completing a task:
You must be open to telling others what you’re planning to do and your reasons for doing that. When others give you feedback, you should be open. They might have a better idea, a better approach and you should be open to that. (RGR10)
Participants’ approaches varied in terms of how they used the existing departmental team culture to find an icebreaker or topic which could engage others’ interest and attention. Examples would be preparing a presentation or voicing “any concerns or new protocols or anything like that” (RGR9). One participant related how she became an acknowledged radiography team member – “She actually knows stuff about stuff” (RGR6) – when she was requested to prepare a poster on a particular view that some radiographers had not mastered correctly.
Generic Skills – “Those Interchangeable Skills”
Transitioning from being a student to being a fully-fledged radiographer can be like being thrown in at the deep end in an unfamiliar environment – “There’s your department and … your machine, go for it!” (SR3). In addition to being a technician with “your machine”, special skills are needed to adapt to the situation and to patients – “So you’ve got to know your work, know how to adapt, be able to relate to the people and be able to ask if you are not sure. … You have got to be able to think sideways as well” (SR3).
And then … plain old adaptability; like just being thrown into something and going, ‘Okay, how do I problem-solve my way out of this?’ Going back to basics and going, ‘Look, if I can do this, from there I can work this out.’ (RGR11)
Novice radiographers also came to realize that they had to be ready to perform many other tasks in an environment that sometimes appeared quite chaotic. For navigating the work environment, they felt they needed skills such as:
The ability to access certain systems or structures or people that you can get help from. Having that capability to ask work colleagues or having programs to help you improve that’s already set in place. … another important factor in work readiness. (RGR1)
Some participants referred to the skills radiographers acquire during their student placements, whereas others mentioned skills picked up in other work situations before they became radiographers – “A lot of those skills are transferable” (RGR1):
I guess it’s mainly a lot to do with placement again. That’s where I could build on my skills. That’s where I even got feedback in some of the weak links that I had. … Just be open-minded. … clinical experience is important. (SR1)
I put so much Kmart [department store] stuff into my statement responses to job interviews. There’s heaps of time management I got from there, talking skills, problem solving skills, conflict resolution. (RGR11)
Mastering the Systems and Structures
An initial challenge for RGRs was the realization that within an institutional context it was “not just I’m going to x-ray this patient right now” (RGR12). Participants echoed the importance of context-specific knowledge and skills in understanding the functioning of the system, “how everything sort of worked together; you would have had to learn the system for that hospital” (SR2). Novice professionals also had to learn to perform administrative tasks efficiently, as described by a supervisor:
Especially … [in a] private hospital, there is so much clerical work. You’re not just always scanning. You have to be able to consent the patient properly, … to assign or register the work properly. If you don’t do those steps, that can delay reporting because you’ve missed out on something. So, as they graduate, if they could pick up the clerical skills … that’s a really good head start. (SR2)
One participant related her experience of an inter-professional program for new graduates: “I don’t think you realize how much it helps just to have some people around the hospital that you know that are outside of your department” (RGR9). Another skill developed through mastering the system and its structures is the ability to “get to know the routine of who is in charge of what” (RGR10) and anticipate what should be done:
You just have to do whatever the doctor tells you. … Try to be a little bit pre-emptive. I find it more challenging to work in ED [emergency department] where there’s doctors and nurses. You have to know when and where to find who. (RGR10)
Finally, hierarchical structures, the associated professional boundaries and roles, and interpersonal relationships could affect the operation of the system. This is how one supervisor described a situation regarding ranks within a radiology department:
the radiologist, sonographers and other technical people (radiographers, CT radiographers), clerical people and then clinical assistant. The important thing is for all people within that hierarchy, nobody to think they’re better than the other person. It needs to be a team of equal standing. Once you get somebody saying, ‘They’re just a clinical assistant’ or ‘They’re just a nurse’ or whatever, that’s when things can fall down.’ (SR4)
The Coordinator – “Things Change All the Time”
In addition to learning organizational functions and pathways, participants also referred to leadership and management capabilities and interaction with a diverse range of staff members – answering phone calls, organizing patients to come through, calling for the wardies [porters], talking to the nurses in emergency about getting patients across, having a wider understanding of the department (RGR12).
Essential coordination skills included the ability to manage time, workflow and throughput, and to prioritize tasks. Activities involving these skills could initially be quite stressful:
… time management is a big one. … you just have to know how to work in a logical and sequential manner. So, it’s one of those skills that if you develop then that’s where … it sort of makes the workflow a lot easier. … A majority [of new graduates], I would say, are still sort of grasping that skill of working logically, what’s right to do, what’s wrong to do; it just comes with time. (SR2)
Additionally, finding the correct pace to suit particular situations entailed being flexible and adapting to the work patterns of others:
The main thing is finding each person’s different flow and how they work and trying to conform to what they’re like. For example, if they do things really fast, trying to get people ready a lot faster …. Or, if people work slower and one at a time, take your time and get everything done. (RGR8)
The Mediator and Advocate – “If You’re Not Really in This to Help the Patient, Then I Do Not Know What You are Doing”
The role of the radiographer as mediator and advocate takes different forms. It is situational and dependent on the context and the characteristics of the professional team. Against the backdrop of patient safety, problem solving and the nurturing of interpersonal interactions and relations emerged from participants’ narratives as two leading skills that are of importance in their role as mediator and advocate in the professional team. They were “not just button pushers” (RGR2), but bridged knowledge gaps, mediated requests and thought “outside the box” (SR3). Through proactive thinking, they advocated not only for patient safety but also for patient comfort:
And in a hospital situation … you’re just all working together. But, we’re always the one to advocate for the patient. ‘Do we need to do all these x-rays? We don’t want too much radiation.’ … It’s all that sort of discussion that I think happens organically … If we notice anything on an x-ray, … or [are] unsure about something, also bring it to the attention of the radiologist so the patient can have further imaging while they’re there or be directed to the right place post x-ray; to a hospital for fracture reduction or back to their GP [general practitioner]. (SR2)
Participants referred to their mediating role between doctor and patient as “sort of go between the two” (SR3) to make decisions on the best way to do an examination and get the appropriate answers:
Most of our responsibility is care of the patient. And of course, we’re dealing with radiation, so you’ve got to care for them in that way too, not just in getting the views. Making it as pleasant an experience as you can and getting an answer for them and … for the doctor as well … Talk to your patient. Seem on their side. … Look at the situation, assess it, do it safely. (SR3)
Radiographers also found themselves in a mediating role between other professionals to promote the best patient outcome:
So, it’s kind of a conflict resolution. … You got two doctors arguing with each other, you got to decide what’s more important. Have those skills to not only calm the situation down between the two doctors but try and get the perfect solution for the betterment of the patient. (RGR2)
The Interdepartmental Collaborator – “There’s a Whole Revolving Door of Different Specialties … We Kind of Just Fit Around Everyone Else”
RGRs have to work collaboratively and differently from the way they were used to as students:
As the student, you’re a little bit invisible to the wider team because people are like, ‘Oh, you’re just there to observe.’ Now it’s, ‘You’re actually here to do a job. Come on.’ (RGR12)
In addition, mutual respect and maintaining professional boundaries are important when collaborating on an imaging examination in different situations:
You’re working one-on-one with speech pathologists, so it’s important to ask them what their plan is before you see the patient. Help prep the patient but let them run the examination and always checking in with what projection they want or what frame. (RGR13)
RGRs also referred to the challenge of learning how to work as a member of a multidisciplinary team – “Where I’m at, there are so many different modalities and people specializing in different things; so, to be a good team member is important” (RGR14). Team leadership promoted role certainty because “your team leader is calling the shots and you’re just working around everyone else as much as you can” (RGR6). The team situations could range from a neonatal unit to a theatre:
I’ve done a lot in public with theatre and neonatal. Especially with the neonatal you were very much part of the neonatal team. … go to all their briefing sessions on what the babies were up to, what their treatment was going to be, where you’d fit into that. And you had to work in with the pediatricians and the physios that were treating the bubs, and the nurses and all the interventional care, even down to helping the patients when there was a problem with the power supply. You’d be pulled into – as you were part of the team working there – to come in and lend a hand … Theatre was the same. The surgeons … tell you what they wanted to see, and it was up to you to try and keep everything sterile but at the same time, move the equipment and give them what they wanted. (SR3)
Another participant described the satisfaction of having a unique role, especially in emergency teams:
ED [Emergency department] is its own different ball game. … A whole different team you’re working with. You’re actually working with consultant ED doctors, reg[istrar] doctors; you’re getting phone calls from ICU [intensive care unit], phone calls from the ward. It can be quite hectic at times; it is a very rewarding job. You never get bored. … You’re not doing the same thing every day. … The skills are tightly tailored. It’s a highly niche skill set … I think it’s what’s enjoyable … Not something most people can do. (RGR2)
Through their efforts to be good interdisciplinary collaborators, RGRs felt like disrupters: “Do you mind if I put my machine here? Do you mind if I do this or that? You feel like you’re being annoying” (RGR7). However, they found a safe haven in their own department:
At the end of the day, we’re most of the time like a disruption. … You’re only ever really in charge once [the patients] come back to your domain. Once they’re in our CT room or our fluoro room, then … you’re in charge and the nurse is following your directions. But until that point, it’s always the other way around. (RGR11)
Respectful collaboration expanded to embrace all staff categories and clients, for example “at the children’s hospital I worked a lot with carers and parents in the roles of carers for their children” (RGR7). Where there was a large team (which may not be the case in all practices), team members included “lots of MIAs [medical imaging assistants] and wardies and those sorts of auxiliary staff” (RGR7).
Communication and Interaction
The application of radiographic and generic skills was embedded in a workplace culture of communication – “You can make anything go as long as you can communicate with your patient and other staff around you” (RGR11). Communication could take the form of interpersonal interaction or communication across the system.
Interpersonal Communication
Across the board, participants referred to the importance of communication and interpersonal skills – “the most important thing is people skills” (RGR8). One participant said:
By nature [of] this job you have to be a person who is quite good with interpersonal skills since we are dealing with patients all the time. If you don’t have those good interpersonal skills, you don’t have those communication skills with your patients, but also your peers. And I just think it’s inherent as a radiographer. (RGR2)
The communication behavior of colleagues towards patients and radiographers was a source of frustration to RGRs:
I get frustrated when I see people speak to a patient abruptly because we’re running out of time. I think that you being curt with that person is going to save four seconds and that’s really not worth it. (RGR11)
Some of them [the radiologists] can give the – especially the new staff – quite a bit of trouble. … I’m saying someone should tell some of them their way of approaching radiographers is not helping us do our job. (RGR10)
Regarding interprofessional communication, many participants considered a vital part of a novice’s work to be “open … and asking questions” (RGR6). One supervisor expressed this as follows:
Communicate with doctors, even if they’re all different levels. You know what it’s like, it can be quite: ‘Do they want to hear from me? I just do this bit of the job.’ … They want to know what you thought of it. You’re not going to give the full answer; they are, but they still want your take on it, on what you thought. (SR3)
Participants also referred to the occasional lack of cooperation from doctors:
When you ask questions … sometimes they expect you to know the answer already or they don’t really give you a very clear or definitive answer. You end up being more confused. There is a doctor who works at XXX … She’s not trained to be nasty or anything, that’s just her temperament but it doesn’t help us do our work. (RGR10)
Communication Across the System
Interdisciplinary interaction included two types of communication that reflect on the functioning of the system. One was communication via the request form and the other was communication about radiation safety – “As a student, we really didn’t prepare for that as much because your supervisor would be the one talking to those people” (RGR5).
RGRs emphasized the importance of clear instructions from colleagues ordering an examination. They mentioned “request forms … that have been pretty dodgy” (RGR14) and “handwriting being difficult to read” (RGR13) – “I find [the request forms] vary a lot from place to place based on how they’re written, what’s acceptable and what doctors will write” (RGR7). Ambiguities should be followed up so that the radiographer can interpret the request correctly:
If it’s a request form and the doctor’s written something wrong, and you don’t double check with them, you might end up x-raying the wrong side or the wrong body part. (RGR8)
Even communication with reception staff was necessary from time to time, because they scheduled the x-rays, but
… they don’t have the background knowledge of anatomy. It’s like trying to communicate with them [on the request] … they might [have] written in the notes that there is a supracondylar humerus fracture, they order a humerus, but we all know that that’s an elbow. (RGR6)
Participants also referred to the fact that doctors consult them about getting their request right:
Radiologists, other doctors in the area will often come and ask our advice about what they should be ordering. … I ordered this, and you did this, can you explain why? And physios and that too. It’s a huge multidisciplinary effort; just daily life there. (RGR6)
Patient safety has already been referred to as part of the role of the radiographer as advocate for patient safety. Radiographers also learn to become educators on radiation safety for other members of the multidisciplinary team:
For example, you’re doing mobile work and you need to be able to communicate with nurses so they’re fully understanding when you’re taking an exposure. That they have an idea of radiation safety, and if not, it’s the radiographer’s responsibility to educate the nursing staff. Dealing with theatres as well and understanding responsibility and what theatre staff and what surgeons need at any particular time. Particularly in a large hospital, there’s a lot of interdisciplinary interactions. (SR4)
Discussion
Harrison describes practice readiness as a complex, multidimensional construct where skills required for readiness go beyond discipline-specific professional competencies.10 The findings of our study suggest that the immersion and transitioning of RGRs into their professional role in their workplace environment requires an expanded conceptualization of their roles and responsibilities. Radiographic services are spread across various levels of care and interwoven with the context and organizational structures and functions that could impact individual RGRs with regard to the following: accountability; confidence; decision making; judgement calls; organizational learning; leadership actions; respectful work environment; professional development; work process; effective safety communication; non-punitive response; error reporting; and teamwork.5,6,16 This entails going through a process of experiential learning and honing knowledge-and-skills to function efficiently and independently in a team-oriented workplace.
RGRs found themselves in the deep end as they navigated the various processes of the integrated system when leading and managing various potentially conflictual situations related to imaging services. This led to an awareness and realization that the complex nature of the medical imaging processes and procedures requires the development of “interchangeable skills” through critical thinking, enquiring, experience, flexibility, feedback and reflection when there is doubt.3,17–20 All these traits are important to prevent errors or harm to patients and professional colleagues. With a systems approach, uncertainty and improvement can be managed through key strategies for targeting avoidable errors, for example effective teamwork and communication, institutionalizing a culture of safety, providing patient-centered care, and using evidence-based practice.19,21
Radiography is a complex, technical, highly structured and production-oriented discipline that is constantly evolving to keep up with the demands of the health system.22 Radiographers must therefore continuously expand and adapt their practice to align with their increasing responsibilities and learn new ways to communicate and work with individuals in broader healthcare teams.7 Because of team diversity and dynamics, there is no “one size fits all” framework for teamwork.23
The quality of request orders may well impact on the quality of a novice radiographer’s work with regard to decisions concerning patient positioning, imaging projections, exposure parameters and dose optimization, which could affect the selection of imaging protocols for patient safety and the accuracy of image interpretation and radiology reports.24,25 In addition to drawing on prior experience and knowledge through reflection, study participants valued an efficiently and effectively functioning team following the standard care processes needed for sound medical imaging outcomes for patients without compromising staff and patient safety.24,26 Participants also shared examples that illustrated the importance of coordinating activities, communicating through collaboration, and endeavouring to participate in negotiation and shared decision making.24,25,27 Interpersonal and professional relations were developed by building rapport and engaging with the team both within the radiography department and beyond.28 According to Chipere et al, positive interpersonal interactions are the cornerstone of creating a workplace where RGRs feel comfortable about broadening their experience and sense of empowerment.12
Healthcare organizations consist of a variety of healthcare professionals working in several interconnected teams that strive to provide safe and consistent care.29 Examples shared in our study alluded to radiographers feeling subservient and subordinate to the medical professionals.27 The inherent hierarchical nature and structure based on professional identities and rankings are inevitable, especially for the newcomers. The value of non-professional staff was acknowledged on the basis of their knowledge, skills, role and responsibilities.29 Central to this are the RGRs’ advocacy, mediating and collaborative roles in coordinating medical imaging processes and procedures to prevent adverse events.
The overall effectiveness of a healthcare team or system is partly dependent on the pre-service education of its practitioners.8 Maladaptive transitions to the workplace can occur because of lack of support and confidence, uncertainty in inter-collegial interactions, or unrealistic performance expectations.30 In our study, participants related how they learned about the organizational context, its characteristics and functioning, and about how to integrate the knowledge and skills acquired through their training into a stressful working environment requiring quality service and safe patient care. These actions included prioritization of tasks, time management, administration and leadership, dealing with complex interactions, and adapting communication styles and strategies.31,32 A common thread in participant perspectives was the recognition that no one could know everything and that the improvement of knowledge and skills was a gradual process.
Study Strengths and Limitations
To the best of our knowledge, this is the first study to include three radiographer populations (RGRs, students and supervisors). The semi-structured interviews yielded rich information and detailed experiences – particularly in the context of multidisciplinary teamwork and the Australian healthcare system – that allowed us to understand the day-to-day experiences and challenges faced by RGRs. These insights could assist with creating written workplace guidelines and clear expectations that could facilitate the immersion of RGRs as they transition to working independently. Embedding more health systems content and functioning into the pre-service practicum units could enhance learning about organizations and workplace culture.
Due to the qualitative nature of the study, the findings are not generalizable to all radiographic settings in Australia or to all novice radiographers. However, readers working in other public and private settings may be able to identify with some of the topics discussed in this paper. Although the focus of the study was on RGRs, the findings could have been enhanced or expanded if similar numbers of students and supervisors had been included. The study was conducted during the coronavirus pandemic and logistical constraints made it difficult to recruit a bigger sample of these two groups.
Conclusion
This study provided insights into the readiness and preparedness of RGRs for the roles and responsibilities awaiting them in the real workplace environment. It demonstrated the complex nature of transitioning from student to fully-fledged radiographer in an integrated environment that is in constant flux and embodies the radiographers’ own expectations and those of the supervisors and other members of multidisciplinary teams. Regardless of the radiographer’s practical experience and competency in performing radiographic tasks, it must be remembered that each workplace has its own context, system and culture that requires continuous social positioning, new learning, and adaptation of skills. Hence, no one can ever be fully ready and prepared through their pre-service training or their initial workplace induction. Individuals have to be open and receptive and learn to “try not to be a hero and do it yourself” (RGR3).
Abbreviations
CT, computed tomography; ED, emergency department; RGR, recently graduated radiographer; SR, supervising radiographer; ST, student radiographer.
Ethics Approval and Informed Consent
The study was approved by the Human Research Ethics Committee at the University of Canberra (HREC-4751) and all participants signed an informed consent form or gave audio-recorded verbal consent. The participants’ informed consent included publication of anonymized responses.
Acknowledgments
We would like to thank all the study participants who willingly shared their perspectives and experiences related to the work readiness of recently graduated radiographers.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was self-funded.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bercovich E, Javitt MC. Medical imaging: from roentgen to the digital revolution, and beyond. Rambam Maimonides Med J. 2018;9(4):e0034. doi:10.5041/RMMJ.10355
2. Wurcel V, Cicchetti A, Garrison L, et al. The value of diagnostic information in personalised healthcare: a comprehensive concept to facilitate bringing this technology into healthcare systems. Public Health Genomics. 2019;22(1–2):8–15. doi:10.1159/000501832
3. Tlili MA, Aouicha W, Rejeb MB, et al. Assessing patient safety culture in 18 Tunisian adult intensive care units and determination of its associated factors: a multi-center study. J Crit Care. 2020;1(56):208–214. doi:10.1016/j.jcrc.2020.01.001
4. Farokhzadian J, Dehghan Nayeri N, Borhani F. The long way ahead to achieve an effective patient safety culture: challenges perceived by nurses. BMC Health Serv Res. 2018;181:654. doi:10.1186/s12913-018-3467-1
5. Rosen MA, DiazGranados D, Dietz AS, et al. Teamwork in healthcare: key discoveries enabling safer, high-quality care. Am Psychol. 2018;734:433–450. doi:10.1037/amp0000298
6. Karami A, Farokhzadian J, Foroughameri G. Nurses’ professional competency and organizational commitment: is it important for human resource management? PLoS One. 2017;1211:e0187863. doi:10.1371/journal.pone.0187863
7. Larsson W, Lundberg N, Hillergård K. Use your good judgement – radiographers’ knowledge in image production work. Radiography. 2009;153:e11–e21. doi:10.1016/j.radi.2008.09.003
8. Adams EJ, Adamson BJ, Poulos A. An insight into the students’ perspective of a nuclear medicine clinical education program. Radiographer. 2004;513:111–116. doi:10.1002/j.2051-3909.2004.tb00008.x
9. Mariño R, Delany C, Manton D, et al. Preparedness for practice of newly qualified dental professionals in Australia - educator, employer, and consumer perspectives. BMC Med Educ. 2022;396. doi:10.1186/s12909-022-03476-7
10. Harrison HC. New graduate registered nurse practice readiness for Australian healthcare contexts: a collective instrumental case study. PhD thesis. Townsville, Australia: Nursing and Midwifery, James Cook University; 2018. Available from: https://researchonline.jcu.edu.au/56555/1/JCU_56555-harrison-2018-thesis.pdf.
11. Murray MA. Linking patient safety to clinical practice: the insight of new graduate registered nurses. PhD thesis. Perth, Australia: School of Nursing and Midwifery, Murdoch University; 2019. Available from: https://researchrepository.murdoch.edu.au/id/eprint/50613/1/Murray20191.pdf.
12. Chipere TG, Motaung T, Nkosi B. Structuring improved work environments for newly-qualified radiographers. rThree approaches to qualitative content analysis. Qual Health Res. 2005;159:1277–1288. doi:10.1177/1049732305276687
13. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qualit Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
14. Bowen GA. Naturalistic inquiry and the saturation concept: a research note. Qual Res. 2008;81:137–152. doi:10.1177/1468794107085301
15. Lincoln S, Guba EG. Naturalistic Inquiry. Newbury Park: Sage Publications; 1985.
16. Moore QT. Determinants of overall perception of radiation safety among radiologic technologists. Radiol Technol. 2021;931:8–24.
17. Larsson K. Understanding and teaching critical thinking—A new approach. Int J Educ Res. 2017;184:32–42. doi:10.1016/j.ijer.2017.05.004
18. Barak M, Levenberg A. Flexible thinking in learning: an individual differences measure for learning in technology-enhanced environments. Comput Educ. 2016;99:39–52. doi:10.1016/j.compedu.2016.04.003
19. Cole P, Hallard R, Broughton J, et al. Developing the radiation protection safety culture in the UK. J Radiol Prot. 2014;342:469–484. doi:10.1088/0952-4746/34/2/46
20. Baumann A, Hunsberger M, Crea-Arsenio M, Akhtar-Danesh N. Policy to practice: investment in transitioning new graduate nurses to the workplace. J Nurs Manag. 2018;264:373–381. doi:10.1111/jonm.12540
21. Simsekler MCE, Qazi A, Alalami MA, Ellahham S, Ozonoff A. Evaluation of patient safety culture using a random forest algorithm. Reliab Eng Syst. 2020;204:107186. doi:10.1016/j.ress.2020.107186
22. Lundberg N IT in healthcare - artefacts, infrastructures and medical practices. Doctoral dissertation Gothenburg Studies in Informatics, Report 17. Göteborg, Sweden: Department of Informatics, School of Economics and Commercial Law, Göteborg University; 2000. Available from: https://gupea.ub.gu.se/bitstream/handle/2077/905/gupea_2077_905_1.pdf?sequence=1&isAllowed=y.
23. MacNaughton K, Chreim S, Bourgeault IL. Role construction and boundaries in interprofessional primary health care teams: a qualitative study. BMC Health Serv Res. 2013;13:486. doi:10.1002/j.2051-3909.2004.tb00008.x
24. European Society of Radiology (ESR). European Federation of Radiographer Societies (EFRS). Patient safety in medical imaging: a joint paper of the European Society of Radiology (ESR) and the European Federation of Radiographer Societies (EFRS). Insights Imaging. 2019;101:45. doi:10.1186/s13244-13019-10721-y
25. Chilanga CC, Olerud HM, Lysdahl KB. Radiographers’ actions and challenges when confronted with inappropriate radiology referrals. Eur Radiol. 2022;326:4210–4217. doi:10.1007/s00330-021-08470-z
26. Hughes RG. Nurses at the “sharp end” of patient care In: Hughes RG, editor. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Rockville, MD: Agency for Healthcare Research and Quality US.; 2008. Available from. https://www.ncbi.nlm.nih.gov/books/NBK2672/.
27. Naylor S, Ferris C, Burton M. Exploring the transition from student to practitioner in diagnostic radiography. Radiography. 2016;222:131–136. doi:10.1016/j.radi.2015.09.006
28. Fatahi N, Kustrimovic M, Elden H. Non-medical radiography staff experiences in inter-professional communication: a Swedish qualitative focus group interview study. J Multidiscip Healthc. 2020;13:393–401. doi:10.2147/JMDH.S231442
29. Ratnapalan S, Uleryk E. Organizational learning in health care organizations. Systems. 2014;21:24–33. doi:10.3390/systems2010024
30. Wakefield E. Is your graduate nurse suffering from transition shock? J Perioper Nurs. 2018;311:47–50. doi:10.3316/informit.474537270039300
31. Janićijević N. The mutual impact of organizational culture and structure. Econ Ann. 2013;58198:35–60. doi:10.1016/j.jmir.2017.02.071
32. Morley L, Cashell A. Collaboration in health care. J Med Imaging Radiat Sci. 2017;482:207–216. doi:10.1016/j.jmir.2017.1002.1071
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.