")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 14
Role of Urinary Beta 2 Microglobulin and Kidney Injury Molecule-1 in Predicting Kidney Function at One Year Following Acute Kidney Injury
Authors Puthiyottil D, Priyamvada PS , Kumar MN , Chellappan A, Zachariah B, Parameswaran S
Received 12 May 2021
Accepted for publication 17 June 2021
Published 5 July 2021 Volume 2021:14 Pages 225—234
DOI https://doi.org/10.2147/IJNRD.S319933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pravin Singhal
Dhanin Puthiyottil,1 PS Priyamvada,1 Mattewada Naveen Kumar,1 Anand Chellappan,1 Bobby Zachariah,2 Sreejith Parameswaran1
1Department of Nephrology, Jawaharlal Institute of Postgraduate Medical Education& Research, Puducherry, 605006, India; 2Department of Biochemistry, Jawaharlal Institute of Postgraduate Medical Education& Research, Puducherry, 605006, India
Correspondence: PS Priyamvada
Department of Nephrology, Jawaharlal Institute of Postgraduate Medical Education& Research, Puducherry, 605006, India
Email [email protected]
Background: There is only limited information on the utility of urinary biomarkers in predicting long-term kidney function following acute kidney injury (AKI). The current study assessed whether urinary beta 2 microglobulin/creatinine (B2M/creat) and kidney injury molecule-1/creatinine (KIM-1/creat) ratios, measured in the early recovery phase of AKI, are predictive of kidney function at one year.
Methods: This is a prospective study done in a tertiary care centre in South India, from March 2017 to December 2018. Adult patients who survived an episode of AKI were followed up for one year (n=125). B2M/creat and KIM-1/creat ratio were measured at two weeks and three months following AKI.
Results: In the AKI survivors, the B2M/creat ratio at 2 weeks [18.3mg/g (IQR 2.3, 52.9)] and KIM-1/creat ratio [1.1 μg/g (IQR 0.5, 4.0) at two weeks were higher compared to healthy controls [B2M/creat ratio 0.35 mg/g (0.17,0.58) and KIM-1/creat ratio 0.40 μg/g (0.23,1.00); P=< 0.001]. After adjusting for covariates, the eGFR and urinary B2M/creat ratio at two weeks following AKI were predictive of eGFR at one year (P< 0.001). KIM-1/ creat ratios were not predictive of eGFR at one year. A urinary B2M/creat ratio of 10.85 at two weeks following AKI had an 85.5% sensitivity (95% CI 74, 93) and 64.3% (95% CI 53, 75) specificity to predict CKD at one year. An eGFR cutoff of 60 mL/min/1.73 m2 at two weeks had a sensitivity of 81.8% (95% CI 69, 90) and specificity of 71.4% (95% CI 60, 81) for predicting CKD. The presence of either one criteria (urinary B2M/creat ratio > 10.85 (mg/g) or eGFR < 60 mL at two weeks) had a sensitivity of 100% (95% CI 94%, 100%) in predicting CKD at one year.
Conclusion: An eGFR < 60 mL/min/1.73m2 and elevated urinary B2M/creat ratio at two weeks following AKI is predictive of low eGFR at one year. Urinary KIM-1/creat ratios do not predict CKD progression.
Keywords: acute kidney injury, biomarkers, acute tubular necrosis, chronic kidney disease
Introduction
Acute kidney injury (AKI) is a significant public health concern, showing a steadily increasing prevalence in the last few decades.1 AKI outcomes depend on multiple factors, including the aetiology, comorbidities, critical illness, stage of AKI, and patient age. Patients who recover from an AKI episode have a long-term risk of developing sequelae like chronic kidney disease (CKD) and end-stage renal disease (ESRD).2–4 In India, the approximate age-standardised rates for CKD is 9529 cases per million population.5 Despite having a high burden of AKI, it is unclear what proportion of CKDs are secondary to AKI. AKI to CKD transition most often results from an incomplete recovery followed by gradual kidney function loss in the long term. Additional, repetitive, severe damage of previously healthy nephrons might significantly impact AKI to CKD transition.6,7 Most of the data on AKI to CKD transition originates from the developed countries, where patients are older with risk factors including CKD, diabetes and systemic hypertension, which makes them vulnerable to AKI and the subsequent progression to CKD. Early identification of patients with an increased likelihood of CKD progression is essential in risk stratification and planning a long-term follow-up. Creatinine-based eGFR measurements might not be sensitive enough to detect minimal derangements in tubular function.8 Predictive algorithms based on age and comorbidities might be of limited use in the developing world, where AKI often develops in previously healthy individuals, who are at least two decades younger than the AKI patients in the developed world.9–11
The last two decades witnessed the validation of multiple biomarkers for the early diagnosis of AKI. Many novel biomarkers surpassed serum creatinine in AKI diagnosis, and many of them correlated well with short-term outcomes. Most biomarkers are upregulated either by tubular injury or tubular inflammation and remain elevated until the injury/inflammation resolves. Hypothetically, elevated urinary biomarkers might identify patients with ongoing tubular injury or inflammation following AKI, translating to a higher risk of CKD progression. However, the role of biomarkers in predicting AKI to CKD transition remains minimal. Kidney injury molecule-1 (KIM −1) is upregulated by proximal tubular epithelial injury and has already been validated as a marker for AKI. Recently, a few cross-sectional studies have reported elevated urinary KIM-1 levels in patients with documented CKD.12,13 Another recent research has shown that baseline KIM-1 levels in the plasma are predictive of future glomerular function decline in non-proteinuric individuals with diabetes.14 Similarly, higher tissue expression of KIM-1 was associated with a faster decline in eGFR in patients with diabetic nephropathy.15 It is unclear whether KIM-1 levels in the early recovery phase of AKI correlate with long-term renal outcomes.
Many proteins like urinary beta 2 microglobulin (B2M) and enzymes are filtered by glomeruli and subsequently reabsorbed in the proximal tubule. Serum B2M is independent of muscle mass and starts rising early in kidney failure. Because of these properties, serum B2M has been proposed as a candidate marker to assess kidney function in AKI and CKD.16 Tubular injury leads to decreased reabsorption of B2M and tubular enzymes, leading to elevated urinary concentrations. These markers may act as a functional marker of tubular damage or fibrosis.17 In rat models, urinary B2M is reported to increase early in the course of nephrotoxic AKI and return to the control range during the recovery phase.16 Urinary B2M is also reported to be elevated in snake-envenomed individuals, despite a return of eGFR to normal ranges.18 There is an unmet need for a sensitive biomarker that would aid in early identification and risk stratification of patients at risk of progression. We assessed whether elevated urinary beta 2 microglobulin/creatinine (B2M/creat) and Kidney Injury Molecule-1/creatinine (KIM-1/creat) measured in the early recovery phase of AKI (two weeks after discharge) are predictive of low eGFR at the end of one year.
Materials and Methods
The recruitment period was from March 2017 to December 2018, with a follow-up duration of one year. A total of 145 patients were enrolled, and 125 completed all three scheduled follow-up visits. Ethical approval was obtained, and informed consent was obtained from all participants before recruitment. The data of 125 patients who completed all three follow-ups were analysed. Also, a sensitivity analysis was done after including the ten deaths during the study period.
Inclusion and Exclusion Criteria
All patients aged >18 years, surviving an episode of AKI during the study period were enrolled, subject to the exclusion criteria and informed consent. Patients with pre-existing CKD (eGFR< 60 mL/min/1.73m2, urine albumin excretion >30 mg/day or urine protein ≥ + on urine dipstick), glomerular disease, renovascular, or interstitial disease were excluded. Patients who were not having any baseline eGFR value were excluded if the ultra-sonogram showed kidney size less than nine cm, loss of corticomedullary differentiation, and cysts in the kidney. Metastatic malignancies with limited life expectancy and plasma cell dyscrasias were excluded. Patients with obstructive uropathy as the cause of current AKI were enrolled if there was a documented normal creatinine in the preceding three months. Sample collections were deferred in patients with active urinary infections during the follow-up visits. However, none of the participants had UTI at the time of sample collection.
All participants were called up for follow-up visits at two weeks, three months, and one year after discharge from the hospital. The demographic parameters, biochemical parameters, disease severity scores, and clinical details of AKI were recorded at initial hospitalisation. During the follow-up visits scheduled at two weeks, three months and one-year post-discharge, eGFR was assessed using CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) creatinine-based equation. Urine samples were collected during the first and second visits for B2M and KIM-1. Participants were instructed to hand over 10 mL of freshly voided urine to the laboratory within 10 minutes of voiding. The samples were centrifuged at 5000 rpm for two minutes, aliquoted and transferred to a −80 degree freezer immediately and kept frozen for analysis later. Serum and urine creatinine were measured by Jaffe’s kinetic method traceable to IDMS, using Beckman Coulter kits adapted to Beckman Coulter AU5811 Clinical Chemistry Analyser. Internal quality control was performed with every batch of samples, covering the clinical ranges using materials supplied by Biorad. The urinary B2M was assessed by Enzyme-Linked Immunosorbent Assay (ELISA) kits provided by Cal biotech Inc. (El Cajon, CA, USA), and KIM-1 was evaluated by ELISA kits provided by Wuhan Fine Biotech Co.Ltd (China). The intraassay coefficients of variations were less than 10%. We also ascertained the average values for KIM-1/creat and B2M/creat in a control population comprising 39 healthy non-diabetic, non-hypertensive, and non-proteinuric individuals having eGFR >60 mL/min/1.73 m2. The urine samples KIM-1 and B2M were collected in the same manner described for AKI patients.
Case Definitions
AKI was defined according to KDIGO 2012 guidelines. Community acquired AKI (CAAKI) was defined as AKI on admission or developing within 48 hours of entry to the hospital. Hospital acquired (HAAKI) was defined as AKI occurring after 48 hours of hospitalisation. For patients with CAAKI, any eGFR value within three months of the onset of current illness was taken as a baseline. For HAAKI patients, the eGFR on admission was considered as baseline. Major adverse kidney endpoints at one year were defined as death within one year or CKD.
Statistical Analysis
All categorical variables were expressed as frequencies and percentages. Continuous variables were expressed as mean with 95% confidence intervals (95% CI) or median with interquartile range (IQR), based on the normality of distribution. The continuous variables between independent groups were compared by the Student’s t-test or Mann Whitney U-test. A Chi-square test was used to compare the categorical variables. Paired t-test and repeated measures ANOVA were used to assess the temporal changes in kidney function and biomarkers. The values were log-transformed for comparison for Urinary KIM-1/creat and B2M/creat, which were not normally distributed. A linear regression model was created to assess the independent predictors of eGFR at one year. Logistic regression was done to identify predictors of major adverse kidney endpoints. Receiver operating characteristics (ROC) curves were constructed to determine the utility of B2M and eGFR to predict CKD. A linear mixed-effects model was used to analyse the changes in eGFR among the subgroups. All statistical analysis was carried out at a 5% significance level, and a P-value <0.05 was considered significant. IBM SPSS Statistics for Windows, Version 26.0, IBM Corp, IL, USA, was used for analysing the data.
Results
A total number of 145 patients were recruited, and 125 patients completed all three follow-up visits. There were ten deaths from recruitment till the last follow-up at one year. Another ten patients were lost to follow-up after the first sample collection.
Among the 125 with complete follow-up, pre-existing comorbid conditions (hypertension, stroke, diabetes, and coronary artery disease) were present in 39 patients. The baseline characteristics of the cohort are given in Table 1. The baseline eGFR was available for 73 persons. None of the patients had any documented AKI before the current admission.
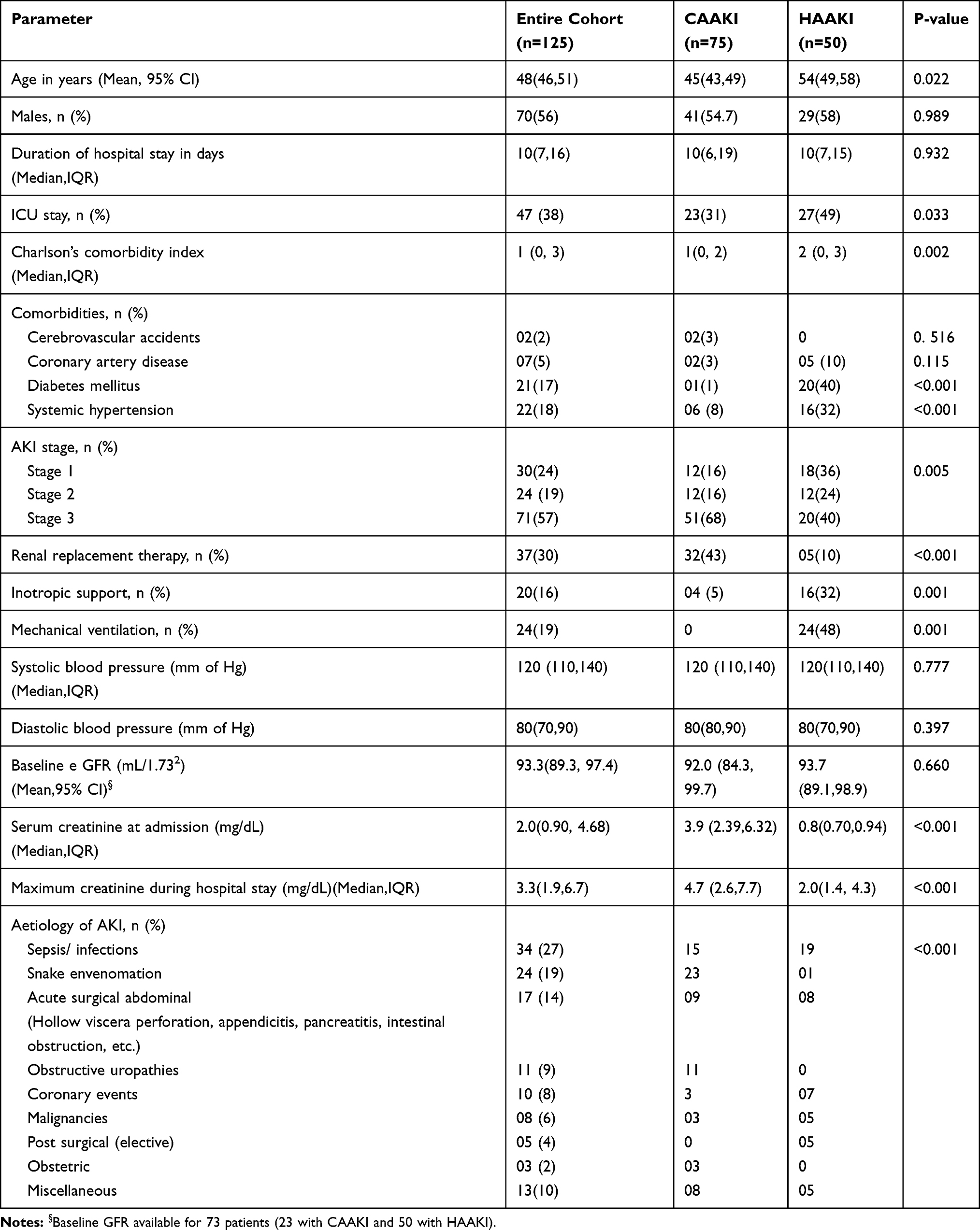 |
Table 1 Baseline Characteristics of the Study Cohort |
Urinary Biomarkers and Kidney Function on Follow-Up
The B2M/creat ratio at 2 weeks [18.3 (IQR 2.3, 52.9)] and at 3 months post AKI [11.3 (IQR 1.2,25.1)] and KIM-1/creat ratio [1.1 (IQR 0.5, 4.0) at two weeks and 2.1 (IQR 0.9,4.0) at 3 months] were higher compared to healthy controls [B2M/creat ratio 0.35 (0.17,0.58) and KIM-1/creat ratio 0.40 (0.23,1.00); P=<0.001]. At the end of one year, 55 patients (44%) progressed to CKD. The CKD stage at the end of one-year follow-up is given in Table 2.
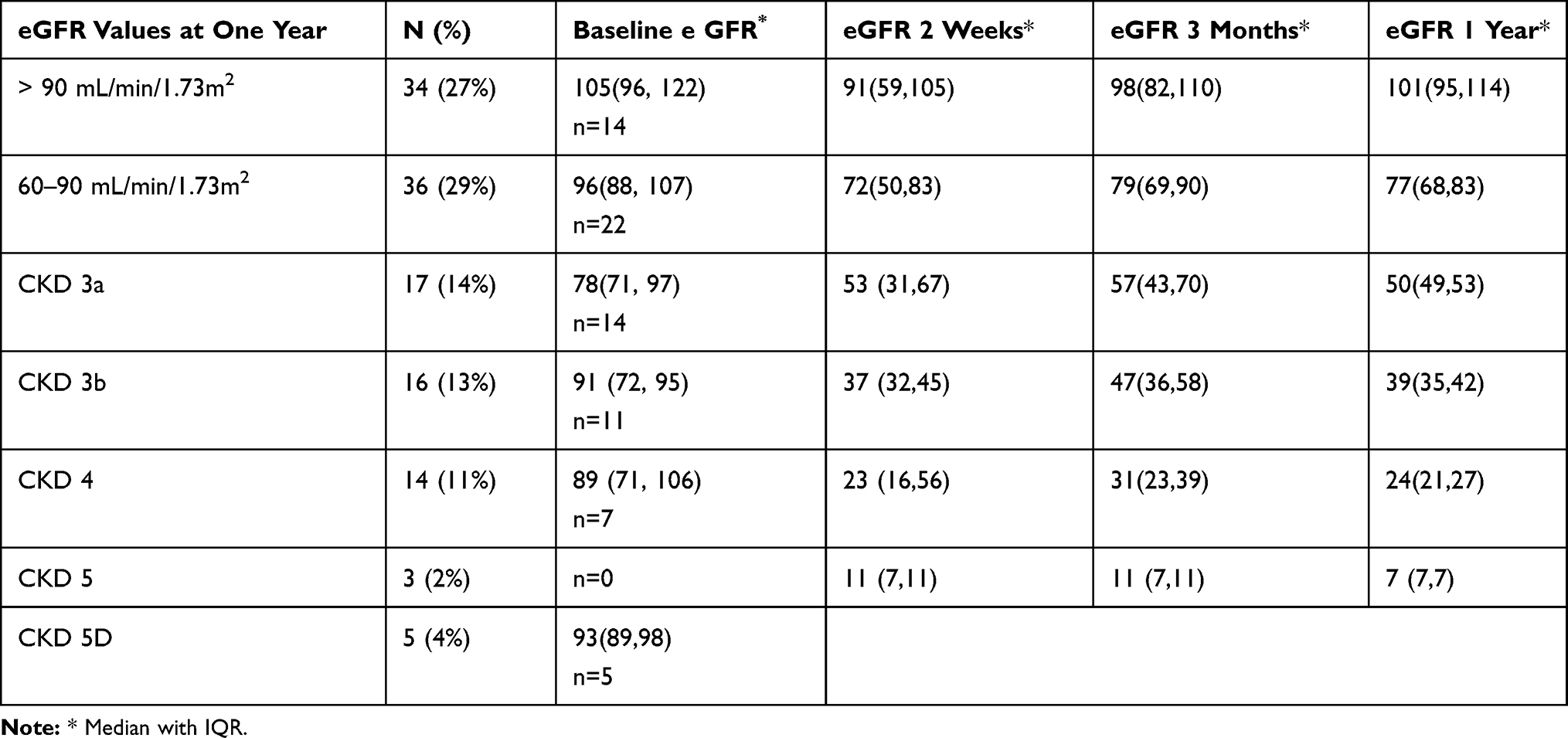 |
Table 2 eGFR Categories at the End of One Year |
Older age, presence of HAAKI and comorbid conditions like diabetes and hypertension were associated with CKD progression. Those who developed CKD had a lower eGFR and higher B2M/creat ratio at two weeks and three months. The KIM-1 /creat ratios were comparable (Table 3). A linear regression model was created to assess the predictors of eGFR at one year. The variables with a P-value of <0.100 were incorporated into the model. Age, AKI type, ICU admissions, comorbidities, new-onset proteinuria, KIM-1/creat ratio, B2M/creat ratio at two weeks and baseline eGFR were included in the model. Only eGFR at two weeks (P<0.001) and B2M/creat ratio (P <0.001) were found to be significant predictors of eGFR at one year (R2=0.687)). The timing of the first urine sample collection from diagnosis of AKI or the no: of days spent in hospital before the HAAKI diagnosis did not influence the eGFR at one year. A second model with the parameters mentioned above and the timing of the first urine sample collection, and the number of days spent in the hospital before the HAAKI diagnosis showed similar results with an R2 of 0.689.
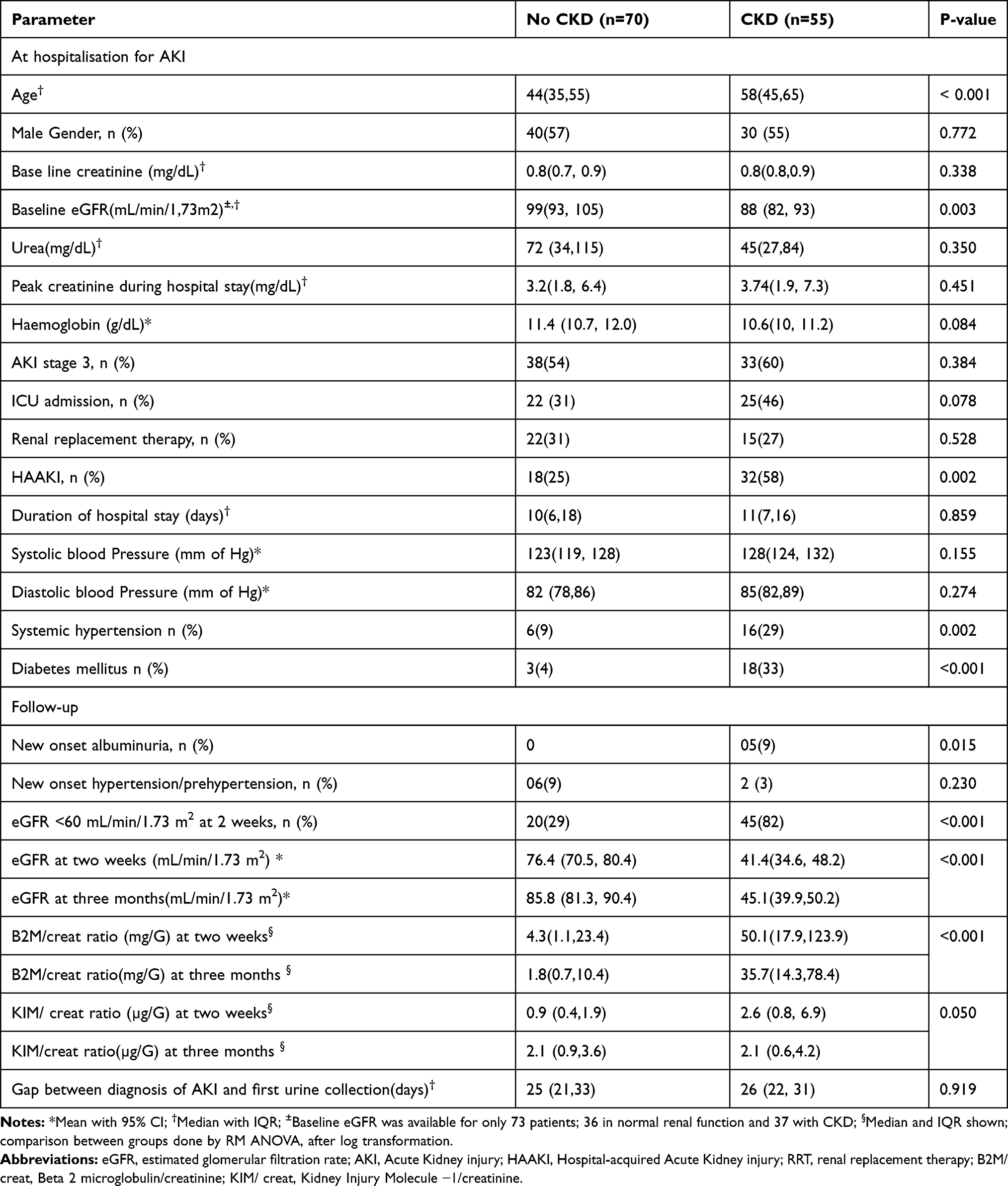 |
Table 3 Characteristics of Patients with and without CKD at the End of One-Year Follow-Up |
The AUC for eGFR at two weeks to predict CKD at one year was 0.855 (0.791, 0.920; Figure 1A). The AUC for B2M at two weeks to predict CKD at the end of one year was 0.796 (95% CI 0.717 −0.875; Figure 1B). From the ROC, a urinary B2M/creat ratio value of 10.85 would result in higher sensitivity and lesser specificity in predicting CKD at one year (Table 4). A linear mixed model adjusted for age and baseline eGFR showed that those with Urinary B2M/creat ratio >10.85 had lower eGFR trajectories throughout the year (Table 5). The median duration of the urine sample collection from the onset of AKI was similar in the high (25 days, IQR 22,30.3), and low urinary B2M/creat groups (25 days, IQR 21,31); P = 0.935.
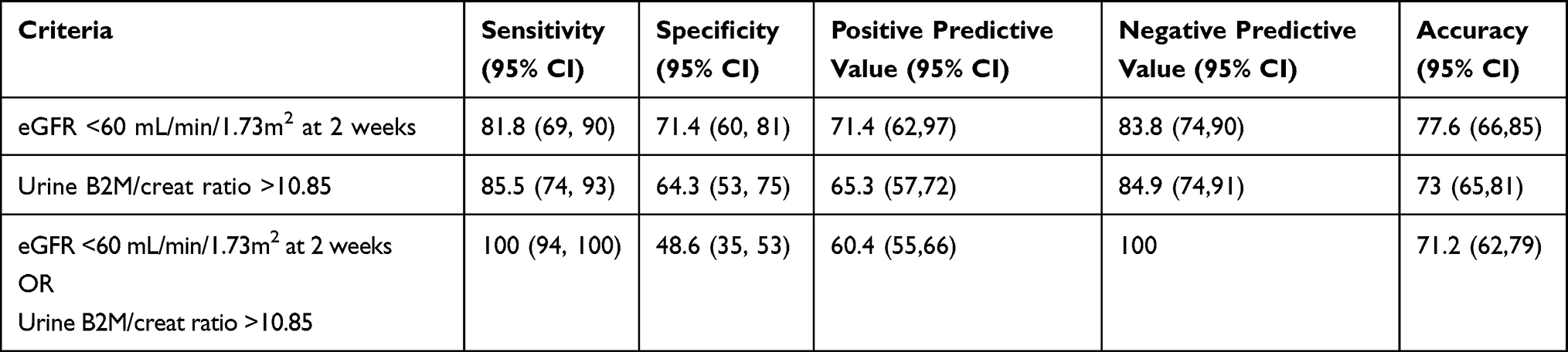 |
Table 4 Sensitivity and Specificity of Various Criteria for Predicting CKD |
 |
Table 5 eGFR Trajectories Across Subjects with Urinary B2M/Creat Ratio >10.85 and <10.85 at Two Weeks |
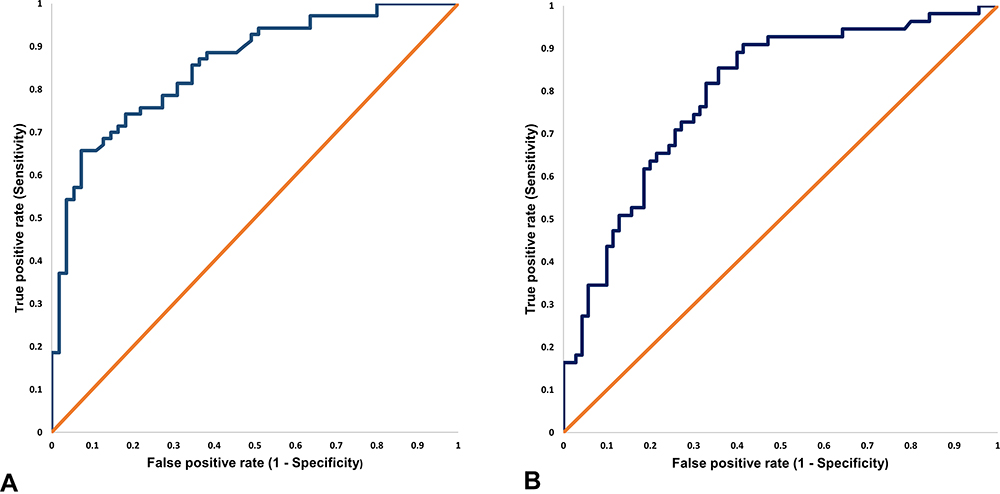 |
Figure 1 (A) eGFR at 2 weeks and CKD status at one year (AUC 0.855). (B) B2M/creat ratio at two weeks and CKD at one year (AUC 0.796). |
We did a sensitivity analysis, including the ten patients who died during the study period. Five deaths happened between 2 weeks to three months, and the remaining five occurred between 3 months to one year. The results are summarised in Supplementary Table 1. After adjustments for covariates, e GFR at two weeks (P<0.001) and urinary B2M/creat were significant predictors of adverse kidney outcomes. The ROC curves for B2M at two weeks to predict major adverse kidney endpoints showed an AUC of 0.754 (95% CI 0.672, 0.835). The AUC for eGFR at two weeks to predict major adverse kidney endpoints at one year was 0.860 (0.799, 0.921).
Discussion
In the current study, we found that elevated urinary B2M/creat ratio, but not KIM-1/creat in the early recovery phase, is associated with a lower eGFR at one year. B2M is a protein discovered in 1964 in the urine of patients having Wilson’s disease and cadmium poisoning. It is a 100 amino acid protein secreted by all nucleated cells at a constant rate. B2M is filtered by the glomerulus and reabsorbed, and catabolised by proximal renal tubules. The urinary concentration of B2M is below 360μg/L in healthy adults. Tubular injury may result in reduced reabsorption and elevated levels of B2M in the urine. The data on the predictive utility of B2M in predicting renal outcomes is emerging. Serum B2M shows a good correlation with Cystatin C and creatinine; eGFR estimations in adults using the CKD-EPI B2M equations have been already validated. The lack of daily fluctuations and independence of race, age, and sex makes this molecule explored further as a potential marker of e GFR.16 B2M has also been evaluated as a marker of tubular injury. A few population-based studies showed that urine β2m levels could be used to diagnose tubular toxicity by heavy metals, lithium, tenofovir, aminoglycosides, and sepsis.16 Serum B2M has been proposed as an independent marker of severity of AKI and its outcomes in children and individuals with intracerebral bleeds.19,20 Urine B2M has been reported to remain elevated in almost half of the patients who recover from AKI resulting from snake envenomation.18
Recently, many novel biomarkers are reported to help early diagnosis, risk stratification, and prediction of the in-hospital outcome of AKI.21 Data from the TRIBE-AKI cohort demonstrated that elevated biomarkers in the immediate perioperative period confer a high mortality risk up to 3 years.22 In the Sapphire study, the product of Tissue inhibitor of metalloproteinases 2 (TIMP-2) and Insulin-like growth factor binding protein 7 (IGFBP7) measured early in critical illness settings identified patients with increased risk for renal replacement therapy and mortality over the next nine months.23
The information on the utility of biomarkers after an apparent recovery of AKI in identifying AKI to CKD transition is sparse. Theoretically, the urinary biomarkers might remain elevated as long as the tubular injury persists. Data from the FRAIL-AKI cohort reported elevated urinary biomarkers Interleukin (IL-18) and KIM-1 in children who developed AKI following cardiopulmonary bypass, despite having normal eGFR.22 This urinary biomarker production represents continuing inflammatory pathophysiology within the kidney, despite the return of GFR to normal ranges.24 Another study among paediatric cardiac surgery cohorts demonstrated higher urinary Neutrophil gelatinase-associated lipocalin (NGAL) levels on follow-up. However, the elevated biomarkers failed to show any association with CKD.25 These biomarkers are surrogates of subclinical tubular injury, which creatinine-based tests cannot pick up. The follow-up period for these two studies was seven years and five years, respectively, which might not be sufficient for CKD development. Those children with elevated biomarkers are likely to be potential candidates who might develop CKD later in life. In adult snake envenomed patients, despite an eGFR recovery, the urinary B2M levels remain persistently elevated even at six months, suggesting a potential role of B2M as an early marker for persistent tubular dysfunction.18 To the best of our knowledge, no other published studies have looked into the trends and utility of biomarkers following a recovery from AKI in the adult population. A multicentre study evaluating the prognostic and diagnostic utility of blood and urine biomarkers following AKI is underway.26
Even though KIM-1 levels in the follow-up cohort were higher than healthy controls, there was no statistically significant association between KIM-1 levels and adverse renal outcomes at one year. These observations are similar to the data from the TRIBE AKI cohort.22 Similar findings were reported from animal models looking into the temporal trends in biomarker concentrations at different time points following AKI. After ischemic reperfusion injury in rats, the serum and urine levels of KIM-1 peaked at the acute phase, followed by a gradual decrease over time. On the other hand, markers like NGAL increased continuously from AKI to the chronic stage.27 These data suggest that KIM-1 might be an inferior marker to monitor the progression of AKI to CKD. Molecules like IL-18 and KIM-1 are upregulated by tubular injury and might remain elevated as long as the tubular injury persists. The transition from AKI to CKD is characterised by maladaptive repair and incomplete resolution, leading to kidney structure and function loss. The maladaptive response includes myofibroblast activation and deposition of extracellular matrix, tubular damage and fibrosis. During this phase of epithelial to mesenchymal transition, the KIM-1 level may come down, as it needs an injured proximal convoluted tubular (PCT) epithelial cell for its production. Functional markers like urinary B2M levels are dependent on tubular resorption. In scenarios where tubular resorption is impaired – either due to tubular injury or fibrosis – the levels might remain elevated. These differences might account for the inferior performance of KIM-1. Data from patients with early CKD also shows a subpar performance for KIM-1.28 On the other hand, elevated KIM-1 levels in diabetic kidney disease might represent ongoing proximal tubular damage induced by hyperglycaemia and proteinuria.14,15
In the current study, eGFR less than <60 mL at two weeks appears to have a better specificity but less sensitivity for identifying CKD at one year. In contrast, elevated urinary B2M/creat is more sensitive, albeit less specific in predicting renal dysfunction at one year. The presence of either elevated urinary B2M/creat or low eGFR improves sensitivity and negative predictive value to 100%. Combining both GFR and B2M would help identify patients who are at high risk of progression. Especially in resource-poor settings where extended serial follow-up is challenging, the combined criteria can potentially be used for early risk stratification. We believe that the low specificity of B2M/creat is due to the limited follow-up period. Those with high urinary B2M/creat showed a lower eGFR right from two weeks; those patients might progress to CKD if followed up for a more extended period.
Strengths and Limitations
The study involved systematic measurements of urine biomarkers at two time points and kidney function at three time points in patients with AKI. Patients with pre-existing CKD were excluded. Patients with glomerular, renovascular, and tubulointerstitial diseases, which would affect the B2M levels, were excluded. The biomarker levels were compared with values from the control population. Conditions like haematological malignancies and infections, which might lead to elevations of B2M, were also excluded. Patients were discharged at the treating physician’s discretion; there is some heterogeneity in sample collection timing. The sample collection was scheduled at two weeks and three months following discharge. However, this does not seem to have affected the B2M/creat ratios or the eGFR at one year. The median duration of sampling was not different among the various subgroups (CKD vs no CKD, high vs low urinary B2M/creat ratio, CAAKI vs HAAKI).
There are potential limitations on the use of urinary B2M as a biomarker for risk stratification. Urinary B2M levels depend on serum concentration, glomerular filtration, and tubular secretion. The utility might be limited in conditions like myeloma and urinary infections. In the circumstances like cortical necrosis and renal infarctions, the filtered load of B2M might decrease, leading to spuriously low urinary B2M despite renal dysfunction. Similarly, in severe renal failure, the levels may be spuriously low because of sharp reductions in GFR. The study is underpowered for subgroup analysis; hence, could not assess the relationship between the aetiology of renal failure, biomarker levels, and progression to CKD. The study intended to recruit only AKI patients without a prior history of CKD. However, only 73 patients had a documented eGFR before the development of AKI. In a developing country like India, people seldom get a periodic medical evaluation. For those without documented eGFR, a normal kidney ultrasound and absence of proteinuria was mandatory for recruitment. It might not be possible to rule out pre-existing CKD completely by this approach. Other limitations include a relatively short follow-up period, small sample size, high dropout rates, and less proportion of patients with earlier AKI stages. Kidney biopsy data were not available in patients who progressed to CKD.
Conclusions
Urinary B2M/creat ratio at two weeks has a higher sensitivity, whereas eGFR <60 mL/min/1.73 m2 at two weeks have a higher specificity in predicting CKD at one year. The presence of either one of these criteria improves the sensitivity to 100%. Those with elevated urinary B2M/creat ratio at two weeks showed lower eGFR trajectories. Urinary B2M/creat ratio at two weeks can be used as a potential marker to identify patients at risk of progression, in conjunction with the eGFR at 2 weeks. Urinary KIM-1/creat ratios do not help in predicting CKD progression.
Compliance with Ethical Standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of Indian Council of Medical Research and JIPMER, Puducherry at which the studies were conducted (IEC approval no: JIP/IEC/2017/185,468) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cerdá J, Lameire N, Eggers P, et al. Epidemiology of acute kidney injury. Clin J Am Soc Nephrol. 2008;3(3):881–886. doi:10.2215/CJN.04961107
2. Hsu RK, Hsu CY. The role of acute kidney injury in chronic kidney disease. Semin Nephrol. 2016;36(4):283–292. doi:10.1016/j.semnephrol.2016.05.005
3. Okusa MD, Chertow GM, Portilla D. The nexus of acute kidney injury, chronic kidney disease, and world kidney day 2009. Clin J Am Soc Nephrol. 2009;4(3):520–522. doi:10.2215/CJN.06711208
4. Chawla LS, Kimmel PL. Acute kidney injury and chronic kidney disease: an integrated clinical syndrome. Kidney Int. 2012;82(5):516–524. doi:10.1038/ki.2012.208
5. Bikbov B, Purcell CA, Levey AS, et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2020;395(10225):709–733. doi:10.1016/S0140-6736(20)30045-3
6. He L, Wei Q, Liu J, et al. AKI on CKD: heightened injury, suppressed repair, and the underlying mechanisms. Kidney Int. 2017;92(5):1071–1083. doi:10.1016/j.kint.2017.06.030
7. Venkatachalam MA, Weinberg JM, Kriz W, Bidani AK. Failed tubule recovery, AKI-CKD transition, and kidney disease progression. J Am Soc Nephrol. 2015;26(8):1765–1776. doi:10.1681/ASN.2015010006
8. Vanmassenhove J, Vanholder R, Lameire N. Points of concern in post acute kidney injury management. Nephron. 2018;138(2):92–103. doi:10.1159/000484146
9. Hodgson LE, Sarnowski A, Roderick PJ, Dimitrov BD, Venn RM, Forni LG. Systematic review of prognostic prediction models for acute kidney injury (AKI) in general hospital populations. BMJ Open. 2017;7(9):e016591. doi:10.1136/bmjopen-2017-016591
10. James MT, Pannu N, Hemmelgarn BR, et al. Derivation and external validation of prediction models for advanced chronic kidney disease following acute kidney injury. JAMA - J Am Med Assoc. 2017;318(18):1787–1797. doi:10.1001/jama.2017.16326
11. Lee BJ, Hsu CY, Parikh R, et al. Predicting renal recovery after dialysis-requiring acute kidney injury. Kidney Int Rep. 2019;4(4):571–581. doi:10.1016/j.ekir.2019.01.015
12. Lim AI, Tang SCW, Lai KN, Leung JCK. Kidney injury molecule-1: more than just an injury marker of tubular epithelial cells? J Cell Physiol. 2013;228(5):917–924. doi:10.1002/jcp.24267
13. Tian L, Shao X, Xie Y, et al. Kidney injury molecule-1 is elevated in nephropathy and mediates macrophage activation via the Mapk signalling pathway. Cell Physiol Biochem. 2017;41(2):769–783. doi:10.1159/000458737
14. Nowak N, Skupien J, Niewczas MA, et al. Increased plasma kidney injury molecule-1 suggests early progressive renal decline in non-proteinuric patients with type 1 diabetes. Kidney Int. 2016;89(2):459–467. doi:10.1038/ki.2015.314
15. Hwang S, Park J, Kim J, et al. Tissue expression of tubular injury markers is associated with renal function decline in diabetic nephropathy. J Diabetes Complications. 2017;31(12):1704–1709. doi:10.1016/j.jdiacomp.2017.08.009
16. Argyropoulos CP, Chen SS, Ng YH, et al. Rediscovering beta-2 microglobulin as a biomarker across the spectrum of kidney diseases. Front Med. 2017;4. doi:10.3389/fmed.2017.00073
17. Coca SG, Parikh CR. Urinary biomarkers for acute kidney injury: perspectives on translation. Clin J Am Soc Nephrol. 2008;3(2):481–490. doi:10.2215/CJN.03520807
18. Jaswanth C, Priyamvada PS, Zachariah B, Haridasan S, Parameswaran S, Swaminathan RP. Short-term changes in urine beta 2 microglobulin following recovery of acute kidney injury resulting from snake envenomation. Kidney Int Rep. 2019;4(5):667–673. doi:10.1016/j.ekir.2019.01.016
19. Wang R, Hu H, Hu S, He H, Shui H, Bahous SA. β2-microglobulin is an independent indicator of acute kidney injury and outcomes in patients with intracerebral hemorrhage. Med. 2020;99(8). doi:10.1097/MD.0000000000019212
20. Barton KT, Kakajiwala A, Dietzen DJ, Goss CW, Gu H, Dharnidharka VR. Using the newer kidney disease: improving global outcomes criteria, beta-2-microglobulin levels associate with severity of acute kidney injury. Clin Kidney J. 2018;11(6):797–802. doi:10.1093/ckj/sfy056
21. Devarajan P. Biomarkers for the early detection of acute kidney injury. Curr Opin Pediatr. 2011;23(2):194–200. doi:10.1097/MOP.0b013e328343f4dd
22. Coca SG, Garg AX, Thiessen-Philbrook H, et al. Urinary biomarkers of AKI and mortality 3 years after cardiac surgery. J Am Soc Nephrol. 2014;25(5):1063–1071. doi:10.1681/ASN.2013070742
23. Koyner JL, Shaw AD, Chawla LS, et al. Tissue inhibitor metalloproteinase-2 (TIMP-2) IGF-binding protein-7 (IGFBP7) levels are associated with adverse long-term outcomes in patients with AKI. J Am Soc Nephrol. 2015;26(7):1747–1754. doi:10.1681/ASN.2014060556
24. Cooper DS, Claes D, Goldstein SL, et al. Follow-up renal assessment of injury long-term after acute kidney injury (FRAIL-AKI). Clin J Am Soc Nephrol. 2016;11(1):21–29. doi:10.2215/CJN.04240415
25. Greenberg JH, Devarajan P, Thiessen-Philbrook HR, Krawczeski C, Parikh CR, Zappitelli M. Kidney injury biomarkers 5 years after AKI due to pediatric cardiac surgery. Pediatr Nephrol. 2018;33(6):1069–1077. doi:10.1007/s00467-018-3888-4
26. Go AS, Parikh CR, Ikizler TA, et al. The assessment, serial evaluation, and subsequent sequelae of acute kidney injury (ASSESS-AKI) study: design and methods. BMC Nephrol. 2010;11(1). doi:10.1186/1471-2369-11-22
27. Dong Y, Zhang Q, Wen J, et al. Ischemic duration and frequency determines AKI-to-CKD progression monitored by dynamic changes of tubular biomarkers in IRI mice. Front Physiol. 2019;10. doi:10.3389/fphys.2019.00153
28. Bhavsar NA, Köttgen A, Coresh J, Astor BC. Neutrophil gelatinase-associated lipocalin (NGAL) and kidney injury molecule 1 (KIM-1) as predictors of incident CKD stage 3: the atherosclerosis risk in communities (ARIC) study. Am J Kidney Dis. 2012;60(2):233–240. doi:10.1053/j.ajkd.2012.02.336
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.